Embed Size (px)
Citation preview

[DOCKET NO. 91N-0450]
GUIDELINE FOR QUALITY ASSURANCE IN BLOOD ESTABLISHMENTS
July 11, 1995
For further information about this document, contact:
Center for Biologics Evaluation and Research (HFM-635) Food and Drug Administration 1401 Rockville Pike Rockville, MD 20852-1448 301-594-3074
Submit written comments on this document to:
Dockets Management Branch (HFA-305) Food and Drug Administration Rm. 1-23 12420 Parklawn Dr. Rockville, MD 20857
Submit requests for single copies of this document to:
Congressional and Consumer Affairs Branch (HFM-12) Food and Drug Administration 1401 Rockville Pike Rockville, MD 20852-1448 301-594-1800 FAX 301-594-1938
Comments and requests should be identified with the docket number found in brackets at the heading of this document.

TABLE OF CONTENTS
PURPOSE . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
SCOPE . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . 2
QUALITY CONTROL/ASSURANCE PROGRAM . . . . . . . . . . . . . . 3
QUALITY ASSURANCE FUNCTION . . . . . . . . . . . . . . . . . 3 Reporting Responsibilities . . . . . . . . . . . . . . . 4
QUALITY CONTROL/ASSURANCE UNIT RESPONSIBILITIES . . . . . . 5 Standard Operating Procedures (SOPs) . . . . . . . . . . 5 Training and Education . . . . . . . . . . . . . . . . . 6 Competency Evaluation . . . . . . . . . . . . . . . . . 7 Proficiency Testing . . . . . . . . . . . . . . . . . . 7 Validation . . . . . . . . . . . . . . . . . . . . . . . 8 Equipment . . . . . . . . . . . . . . . . . . . . . . . 8 Error/Accident Reports, Complaints, and Adverse
Reactions . . . . . . . . . . . . . . . . . . . . . 8 Records Management . . . . . . . . . . . . . . . . . . . 9 Lot Release Procedures . . . . . . . . . . . . . . . . . 9 Quality Assurance Audits . . . . . . . . . . . . . . . . 10
APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . 12
GLOSSARY . . . . . . . . . . . . . . . . . . . . . . . . . . 32
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . 34 Health and Human Services References . . . . . . . . . . 34 General References . . . . . . . . . . . . . . . . . . . 34

QUALITY ASSURANCE IN BLOOD ESTABLISHMENTS
PURPOSE
The purpose of this guideline is to assist manufacturers of blood and blood components, including blood banks, transfusion services, and plasmapheresis centers, in developing a quality assurance (QA) program in their effort to be consistent with recognized principles of quality assurance and current good manufacturing practice (CGMP).
SCOPE
This guideline provides general information on procedures and practices and may be useful to blood establishments in developing and administering a QA program. Because the Food and Drug Administration (FDA) is in the process of revising 21 CFR 10.90(b), this document is not being issued under the authority of 21 CFR 10.90(b), and the document, although called a guideline, does not bind the agency and does not create or confer any rights, privileges, or benefits for or on any person. Blood establishments may follow the guideline or may choose to use alternative procedures not provided in the guideline. If a blood establishment chooses to use alternative procedures, the establishment may wish to discuss the matter further with the agency to prevent expenditure of resources on activities that may be unacceptable to the FDA.
Blood and blood components applicable to the prevention, treatment, or cure of human diseases or injuries are biological products subject to regulation pursuant to Section 351 of the Public Health Service (PHS) Act [42 U.S.C. 262]. Similarly, blood and blood components intended for use in the diagnosis, cure, mitigation, treatment, or prevention of diseases in humans are drugs as defined in Section 201(g) of the Federal Food, Drug, and Cosmetic (FD&C) Act [21 U.S.C. 321(g)]. Section 501 (a)(2)(B) of the FD&C Act states, in part, that a drug shall be deemed to be adulterated if "the methods used in, or the facilities or controls used for, its manufacture, processing, packing, and holding do not conform to or are not operated or administered in conformity with current good manufacturing practice to assure that such drug meets the requirements" of the FD&C Act. Because blood and blood components are drugs under the FD&C Act, the Current Good Manufacturing Practice regulations in 21 CFR, Parts 210 and 211 are applicable. In addition, FDA has issued CGMP
1

regulations for blood and blood components in 21 CFR, Part 606.
This guideline is intended to be used in conjunction with the applicable federal standards in 21 CFR, Parts 600 through 680 and Parts 210 and 211. Section 210.2 provides that the regulations in Parts 210 through 226 and 600 through 680 are considered to supplement, not supersede, each other. Where it is impossible to comply with the applicable regulations in both Parts 210 through 226 and Parts 600 through 680, the regulations specifically applicable to the product shall apply and supersede the more general regulations. Some examples of 21 CFR, Parts 210 and 211 and Parts 600 through 680 supplementing each other are set forth in Appendix A. This guideline may be amended periodically as needed.
Blood establishments should be aware that under the Clinical Laboratory Improvement Amendments of 1988 (CLIA), establishments performing laboratory testing, including blood banks, transfusion services, and plasmapheresis centers, must also comply with applicable regulations in 42 CFR, Part 493. These regulations, generally effective September 1, 1992, establish standards for laboratory personnel, quality control, proficiency testing, patient test management, and QA based on test complexity and patient risk factors.
INTRODUCTION
It is generally believed that the United States has one of the safest blood supplies in the world. This is due in large part to the development and implementation of standards for donor suitability and product quality. Since 1983, many significant developments have occurred including the implementation of new tests and donor suitability criteria. In addition, the FDA has intensified its oversight of blood establishments and has documented the release of unsuitable blood and blood components in a number of situations due to deficiencies from established standards.
These findings may be related to several factors: (1) the increase in the number of tests performed (increased testing increases the opportunity for errors and contributes to the complexity of the operation), (2) the increasing use of complex advanced technology in testing procedures and equipment including computerized systems, (3) a shortage of appropriately trained health care and laboratory personnel,
2

and (4) the need for more sophisticated process and system control procedures in blood establishments, including procedures for training and supervising existing personnel.
In a memorandum dated April 6, 1988, FDA's Center for Biologics Evaluation and Research (CBER) requested that blood establishments review procedures and employee training programs to determine the adequacy of safeguards to prevent the release of unsuitable blood products. CBER issued a memorandum on March 20, 1991, notifying blood establishments of the increasing number of product recalls due to errors and accidents in manufacturing. CBER described examples of the types of errors and accidents that have resulted in the release of unsuitable products. In addition, CBER reminded establishments of the reporting requirement for errors and accidents and the need for follow-up investigation.
To ensure the continued safety of the nation's blood supply, it is essential that blood establishments implement effective control over manufacturing processes and systems. FDA believes that this can be accomplished by each blood establishment developing a well planned, written, and managed QA program designed to recognize and prevent the causes of recurrent deficiencies in blood establishment performance. The goals of QA are to significantly decrease errors, ensure the credibility of test results, implement effective manufacturing process and system controls, and ensure continued product safety and quality. QA includes measures to prevent, detect, investigate, assess, and correct errors. The emphasis is on preventing errors rather than detecting them retrospectively.
Implementing a QA program requires a commitment of time and resources. The design and scope of a QA program depend on the size and complexity of manufacturing operations performed by the establishment. The potential public health consequences require that all establishments, regardless of size, invest in QA.
QUALITY CONTROL/ASSURANCE PROGRAM
A QA program is a system designed and implemented to ensure that manufacturing is consistently performed in such a way as to yield a product of consistent quality. QA is the sum of activities planned and performed to provide confidence that
3
all systems and their elements that influence the quality of the product are functioning as expected and relied upon.
There are several dimensions to QA including quality control (QC) procedures and current good manufacturing practice. Adequate quality control procedures are an element of conformity with CGMP and include the routine on-line or in-process monitoring of manufacturing procedures [See 21 CFR 211.22(a), 211.100(a), 606.140(b)]. Other dimensions of QA relevant to the control of production include standards for personnel, facilities, procedures, equipment, testing, and recordkeeping activities.
QUALITY ASSURANCE FUNCTION
A quality control unit having the responsibility and authority to ensure product quality is required by 21 CFR 211.22(a). In the pharmaceutical industry, the group performing this function often has been titled the Quality Control Unit. With the evolution of the concept of QA during the past 20 years, the group responsible for oversight of all activities relating to product quality (including quality control) often has been titled the Quality Assurance Unit. Subsequently, in practice, the term quality control often has been considered by many as limited to describing the component of a QA program that includes the activities and controls used to determine the accuracy of the establishment's equipment and operations in manufacturing (i.e., on-line or in-process testing) and product release. Irrespective of the title of the person or persons performing QA duties, a quality assurance function should be established.
Although the term "quality assurance" is not used in 21 CFR, Parts 210 and 211 and Parts 600 through 680, these regulations clearly require a program of activities to control the manufacturing process to prevent the release of unsuitable products. For purposes of clarity, this document uses the term "quality assurance" to describe the actions, planned and performed, to provide confidence that all systems and elements that influence the quality of the product are working as expected. The person or group of persons who perform this function will be referred to as the QC/QA Unit. The terms "quality control" and "quality assurance" will be defined as stated above and in the glossary.
4

The QC/QA Unit should coordinate, monitor, and facilitate all QA activities. The QC/QA Unit may include one or more individuals dedicated solely to QA functions or individuals who also perform other tasks in the establishment. In the latter situation, however, individuals should not have final oversight of their own work [See 21 CFR 606.100(c), 211.194]. In a small firm, it may be feasible for one individual to function as the QC/QA Unit. That person has the responsibility for implementing controls and reviewing results of manufacturing to ensure that product quality standards are met.
Reporting Responsibilities A QC/QA Unit should report to management or its designee. In licensed firms, this unit should report to the Responsible Head who is the individual designated in the establishment license application to represent the firm in its regulatory activities with CBER [See 21 CFR 600.10(a)] or his/her designee. In unlicensed firms, the QC/QA Unit should report to a "designated qualified person" [See 21 CFR 606.20(a)] or his/her designee.
The Responsible Head or the designated qualified person is required to exercise control over the establishment in regard to all matters related to compliance with FDA requirements including the FD&C Act and the PHS Act, and should have the authority to implement corrective action when necessary. These individuals are responsible for ensuring corrective action has been taken. The Responsible Head or designated qualified person is also responsible for ensuring that personnel are appropriately assigned and trained to accomplish their duties [See 21 CFR 211.25, 600.10, 606.20].
The QC/QA Unit reports independently from production to management. The QC/QA Unit should ensure that production personnel follow CGMP. When necessary, the QC/QA Unit should have the authority to stop production and/or release of product.
QUALITY CONTROL/ASSURANCE UNIT RESPONSIBILITIES
The responsibilities of a QC/QA Unit in blood establishments should include, but are not limited to, the following areas:
Standard Operating Procedures (SOPs) [See 21 CFR 211.100, 606.65(e), 606.100]
5

QA activities relevant to SOPs include:
(1) Determining that SOPs exist for all manufacturing procedures including, but not limited to, testing, and that SOPs accurately describe and define the procedure, including a statement of what the procedure is intended to accomplish. The actual content of the SOPs may be the responsibility of the production units [See Federal Register, Volume 43, No. 190, Sept. 29, 1978, pp. 45014, 45032].
(2) Reviewing and ensuring written approval of all SOPs prior to implementation and confirming that SOPs comply with all applicable statutory and regulatory requirements. Additionally, prior to the implementation of each SOP, the QC/QA unit ensures that the following items are written and in place:
(a) procedures to establish validation protocols to ensure that methods and processes accomplish their intended purpose;
(b) identification of personnel responsible for performing each procedure;
(c) procedures for training and certifying individuals identified in (b);
(d) responsibilities of supervisors for oversight of the performance of all procedures;
(e) methods for periodic proficiency testing; (f) methods for periodic competency evaluation of the
individuals performing each procedure; (g) methods for evaluating the performance of each
procedure during QA audits; (h) designation of each procedure as a critical or non
critical control point (as defined in the glossary); and
(i) instructions for records maintenance consistent with requirements for recordkeeping.
(3) Maintaining an index of all SOPs, a master copy, and an archive of obsolete SOPs.
(4) Ensuring that the SOP content is reviewed to assess impact on other systems and their functions.
6
(5) Ensuring that each employee is provided with, and has ongoing access to, the necessary SOPs to perform assigned duties.
(6) Ensuring that validation protocols are designed prospectively, performed and evaluated, and that written validation reports are prepared. Validation of a process already in use may be based upon accumulated production, testing, and control data.
(7) Ensuring that modifications or changes in SOPs are appropriately documented including the rationale for the change. Ensuring that revised or new methods and processes are validated and do not create an adverse impact elsewhere in the system or operation. Changes in SOPs should be made in accordance with a written procedure and be formally approved before implementation.
(8) Ensuring that SOPs for all QC/QA unit activities exist and define the QC/QA unit's responsibility for performing SOP review, approval, or authorization or, if appropriate, ensuring review, approval, or authorization has been performed.
(9) Ensuring pertinent SOPs are promptly updated to reflect changes in manufacturer's directions for use and all SOPs and manufacturing records are reviewed at least annually.
Training and Education The QC/QA Unit should assist in developing, reviewing, and ensuring the approval of training and educational programs for all personnel [See 21 CFR 211.25]. Training should include the following programs:
New employee orientation, CGMP training, SOP training, Technical training, Supervisory training, Managerial training, QA training, Computerized system training, and Continuing education and training.
7

The QC/QA Unit should be aware of factors that indicate a need for training or retraining. Information regarding the need for such training may be derived from management observations, proficiency test results, competency evaluations, technical changes, error/accident reports, complaints, QA audits, and problems discovered at critical control points identified in each system within the establishment's total operation. Thresholds for implementing retraining programs should be established.
Competency Evaluation To ensure that all staff are trained and maintain their competency to perform all assigned tasks, the QC/QA Unit should implement a formal regular competency evaluation program. A competency evaluation program should evaluate theoretical and practical knowledge of procedures including, but not limited to, the following:
(1) Direct observations of performance of routine and quality control procedures including, as applicable, donor suitability, sample handling, processing, testing, labeling, and instrument preventive maintenance;
(2) Monitoring the recording and reporting of test results by reviewing work sheets, quality control records, preventive maintenance records, and other records and entries (both manual and automated);
(3) Written tests to assess problem solving skills, knowledge of SOPs, and theory; and
(4) Assessment of performance using internal blind specimens and external proficiency test specimens.
Minimum acceptable scores, performance, and remedial measures to correct inadequate performance on competency evaluations should be documented and retained in personnel records. Evaluation summaries provide useful information to correct individual or group performance problems.
Proficiency Testing Proficiency tests are commonly one part of the QA program for testing laboratories. In addition to the facility's standard review of proficiency test results, the QC/QA Unit should also review, evaluate, and monitor the proficiency testing program
8
to ensure the adequate evaluation of test methods and equipment and competency of personnel performing testing.
Blood establishment proficiency testing procedures should ensure that proficiency samples are tested by all personnel normally performing routine testing, using routine test equipment, during routine test runs. Blood establishments should provide for proficiency testing of back-up or alternate test methods, e.g., manual procedures or "stat" tests. Procedures should ensure accurate, reliable, and prompt test results.
Supervisors, management, and the QC/QA unit should review and evaluate proficiency test results. Additionally, the QC/QA Unit should analyze results for trends or patterns to identify specific problems. There should be a written plan for remedial action in the case of unsuccessful proficiency test performance.
Other quality control procedures may be useful in monitoring laboratory performance. These include statistical reviews of unknown and control sample results, comparisons of initial and repeat test values, and results of the same test performed by different methods or at different sites.
Validation The FDA has provided general guidance in its Guideline on General Principles of Process Validation (May, 1987) which should be referenced to determine the validation principles applicable to an individual establishment's systems and processes. The QC/QA unit should ensure that adequate validation procedures have been performed. Complaints, errors, accidents, and problems at critical control points should be reviewed to determine the need for revalidation or revision of validation procedures.
Equipment Equipment installation qualification is performed to establish "confidence that process equipment and ancillary systems are capable of consistently operating within established limits and tolerances" [Guideline on General Principles of Process Validation (May, 1987)]. The QC/QA Unit should ensure that procedures are in place for equipment qualification, process validation, and revalidation after repairs to ensure the proper function of all equipment. Appropriate records of the
9

results of validation testing should be reviewed and maintained.
There should be written procedures for equipment qualification, validation, maintenance, and monitoring. Additionally, there should be schedules for equipment monitoring, calibration, and maintenance sufficient to ensure that performance is according to specifications. Equipment monitoring procedures should include evaluation of consequences of malfunctioning or out-of-calibration equipment. Computer systems used in manufacturing are equipment subject to 21 CFR 211.68 and 606.60.
Error/Accident Reports, Complaints, and Adverse Reactions The QA program should provide assurance that procedures are in place and exactly followed for the review, evaluation, investigation, and correction of manufacturing errors and accidents. There should also be a system to ensure timely reporting to CBER of errors and accidents that may affect the safety, purity, identity or quality of blood products [See 21 CFR 600.14]. QA procedures should ensure that all complaints regarding product quality are investigated to determine whether the complaint is related to an error or accident in manufacturing. Investigative procedures should include provisions for review to determine whether the complaint represents an adverse reaction. Donor or recipient adverse reactions may be life-threatening, permanently disabling, or fatal. Procedures should be in place to ensure that donor and recipient adverse reactions are thoroughly investigated and completely documented. Fatalities must be reported to CBER in accordance with 21 CFR 606.170(b). The QC/QA Unit should ensure that product recalls and market withdrawals are handled according to established procedures and guidelines [See 21 CFR, Part 7].
Procedures should be in place to ensure transfusion reactions are investigated. A program should be in place to train patient care staff to recognize symptoms of adverse reactions so that appropriate intervention can be taken. Procedures should include review of manufacturing procedures when bacterial contamination of the product is suspected. Possible bacterial contamination should be reported to the blood collection facility.
An essential element of QA is feedback into the QA system of knowledge acquired through investigations of complaints,
10

error/accident incidents, and adverse reactions. If there is no investigation of complaints, error/accidents, or adverse reactions, factors contributing to the problems cannot be identified and corrected. Errors or accidents in manufacturing may be identified either by employees in the course of routine activities or by supervisors during record review. The QC/QA Unit should assess all errors that occur during manufacturing, including those identified before products are released. The QC/QA Unit should receive copies of error/accident reports and ensure appropriate follow-up actions have been taken. There should be procedures for initiating and completing all corrective actions. Corrective actions may include system or process redesign, retraining, and procedural changes.
Records Management The QC/QA Unit should approve or ensure approval of all recordkeeping systems (manual and automated). Electronic or computerized recordkeeping systems should be properly validated [See 21 CFR 211.68]. QA procedures should be implemented to ensure that required records [See 21 CFR 606.160] are reviewed as necessary to ensure the accurate and complete history of all work performed. Portions of the review may be performed at appropriate periods during or after blood collecting, processing, compatibility testing, and storing [See 21 CFR 606.100(c)].
Lot Release Procedures Each component, as defined in 21 CFR 606.3(c), (e.g., Red Blood Cells, Platelets, Plasma, or Cryoprecipitated AHF) prepared from a unit of whole blood represents one lot of product and bears a lot number, which is often the unit number assigned at the time of collection. QA procedures should be implemented to ensure that records are reviewed for accuracy, completeness, and compliance with established standards. A second person should review each significant step in each process associated with every component prior to release [See 21 CFR 606.100(c), 211.194(a)(7)&(8)]. QA procedures should be in place to ensure that any lot discrepancies or failure of a lot or unit to meet its specifications are thoroughly investigated.
Labeling control procedures should be appropriate to the system and equipment. If automated labeling equipment retains information that could be erroneously printed during subsequent use, strict control procedures to prevent this
11
should be implemented [See 21 CFR 211.125]. There should be written procedures designed and followed to ensure that correct labels, labeling, and packaging material are used for drug products [See 21 CFR 211.130].
Blood and blood components are labeled at various stages in the manufacturing process. At collection, products may be labeled as to the type of product the facility anticipates manufacturing. Products may be labeled as to blood group and expiration date at a later point in the manufacturing process. Products may be converted from one product type to another (e.g., Fresh Frozen Plasma to Recovered Plasma, Whole Blood to Red Blood Cells) and subsequently relabeled. Relabeling of blood products due to conversion to another product must undergo the same control procedures and have the same records maintained as the initial labeling operation.
At each stage in the manufacturing process where labeling occurs, there should be process controls that ensure correct labels have been applied. Prior to release, the completely labeled product should be reviewed. Control procedures for final label review should include review of applicable production records and a record of verification by a second individual to ensure products have been properly labeled, e.g., donor classification, blood group, expiration date, and product name. When proper control procedures for labeling are followed, labeling errors are minimized.
Quality Assurance Audits A QA audit is one mechanism for evaluating the effectiveness of the total QA system. Comprehensive audits should be conducted periodically in accordance with written procedures [See 21 CFR 211.180(e)]. A comprehensive audit should consist of review of a statistically significant number of records. A focused audit may be necessary when quality problems have been identified, or to monitor, more effectively, a particularly critical area. However, isolated audits restricted to one area may not detect system-wide problems. The QC/QA Unit's written procedures for a focused audit should be flexible enough to allow for additional audits without requiring changes in SOPs.
Audit procedures will vary in complexity depending on the size of the establishment and the specific processes under review. Individuals conducting audits should possess sufficient knowledge, training, and experience to identify problems in
12

the specific processes under review. The auditor or audit team should not be responsible for performing the procedures being audited. In situations in which an external audit program is used, the QC/QA unit is responsible for assuring that the audit meets the needs of the establishment and is consistent with 21 CFR 211.180(e). The annual review required by 21 CFR 211.180(e) is not viewed as a QA audit, and records of these reviews must be available during FDA inspections.
There should be a written report documenting audit procedures and results. Procedures should include a plan for the Responsible Head or designated qualified person and other appropriate responsible officials to review and evaluate the results of the audit. The purpose of the review and evaluation is to ensure that responsible individuals are aware of problems, and corrective action is implemented. Audit reports should be retained for a period consistent with product record retention requirements.
QA audits should be structured using a systems approach. Major systems of a blood manufacturing operation are identified in Tables 1-8, Appendix B. The systems which may comprise blood establishment operations and that should be audited should include, at a minimum, the following:
Quality Control/Assurance; Donor Suitability; Blood Collection; Component Manufacturing; Product Testing; Storage and Distribution; Lot Release; and Computer.
Each system may function independently or collectively with other systems. The critical control points in each system refer to areas that may affect the safety and quality of the product if key elements are not performed or functioning correctly. The key elements are individual steps in each critical control point. QA audits should evaluate critical control points and key elements in each system. Examples of critical control points and associated key elements are included in Tables 1-8, Appendix B. Each establishment should customize its audit for its own systems.
13

APPENDICES
14

Appendix A. Examples of 21 CFR, Parts 210 through 211 and Parts 600 through 680 Supplementing Each Other.
The CGMP regulations for drugs are useful in ensuring the quality of blood and blood products, and implementing these regulations is both feasible and practical. The CGMP regulations in 21 CFR 211 are general and suitable for all finished pharmaceuticals, and flexible to permit innovation. These regulations provide some flexibility to manufacturers to select the methods and processes most suitable for the products and operations of the individual firms. Notwithstanding such flexibility, manufacturers must, of course, create and implement procedures that are sufficient to accomplish all objectives of the CGMP regulations. In those few cases where precise procedures are set forth in the CGMP regulations, individuals believing that alternative mechanisms may also be acceptable are invited to request approval to use an alternative procedure pursuant to 21 CFR 640.120.
The term "lot" is defined for biological products in 21 CFR 600.3(x). This same term is also defined in 21 CFR 210.3(b)(10). The term "batch" is defined in 21 CFR 210.3(b)(2) as a specific quantity of a drug or other material that is intended to have uniform character and quality, within specified limits, and is produced according to a single manufacturing order during the same cycle of manufacture. For purposes of good manufacturing practice, a unit of whole blood or each of its components collected for transfusion or further manufacturing is both a lot and a batch. Testing for a single unit of blood may be performed as part of a run consisting of testing many other units of blood at the same time. In situations where testing (or other manufacturing) records include the results of more than one unit in a single record, signatures need only be written on the record as a whole rather than next to the results of each unit.
The regulations in 21 CFR, Parts 210 through 226, and 600 through 680 are considered to supplement, not supersede, each other, unless the regulations explicitly provide otherwise. In the event that it is impossible to comply with all applicable regulations in both 21 CFR, Parts 600 through 680 and Parts 200 through 211, the regulations specifically applicable to the drug in question shall supersede the more general regulations. The following charts provide examples of 21 CFR, Part 211 and Parts 600 through 680 supplementing each other. The highlighted text in 21 CFR 211, CGMP
15

for Finished Pharmaceutical, identifies additional standards of CGMP that are also applicable to blood and blood components.
16

CURRENT GOOD MANUFACTURING PRACTICE SPECIFIC FOR
BLOOD AND BLOOD COMPONENTS
CURRENT GOOD MANUFACTURING PRACTICE FOR
FINISHED PHARMACEUTICAL (INCLUDES BLOOD AND BLOOD COMPONENTS)
The biologic regulations describe requirements for record review, product quality control, laboratory controls, equipment controls, and SOPs for quality control, but do not explicitly refer to a QC/QA Unit. The Part 211 CGMPs specify that a person or group of persons will be responsible for performing these functions [21 CFR 211.22]
Comprehensive audit record review may consist of review of a sample of records that are representative of product production. A review of every complaint, recall, and product failure must be performed.
211.22 (a) There shall be a quality control unit that shall have the responsibility and authority to approve or reject all components, drug product containers, closures, in-process material, packaging material, labeling, and drug products, and the authority to review production records to assure that no errors have occurred or, if errors have occurred, that they have been fully investigated.
(c) The quality control unit shall have the responsibility for approving or rejecting all procedures or specifications impacting on the identity, strength, quality, and purity of the drug product.
(d) The responsibilities and procedures applicable to the quality control unit shall be in writing; such written procedures shall be followed.
211.180(e) Written records required by this part shall be maintained so that data therein can be used for evaluating, at least annually, the quality standards of each drug product to determine the need for changes in drug product specifications or manufacturing or control procedures. Written procedures shall be established and followed for such evaluations and shall include provisions for: (1) A review of every batch, whether approved or rejected, and, where applicable, records associated with the batch. (2) A review of complaints, recalls, returned or salvaged drug products, and investigations conducted under 211.192 for each drug product.
606.100(b) 211.100 Written standard operating procedures (a) There shall be written procedures for production and shall be maintained and shall include process control designed to assure that the drug products all steps to be followed in the have the identity, strength, quality, and purity they purport collection, processing, compatibility or are represented to possess. Such procedures shall include testing, storage and distribution of all requirements in this subpart. These written procedures, blood and blood components for including any changes, shall be drafted, reviewed, and homologous transfusion, autologous approved by the appropriate organizational units and reviewed transfusion and further manufacturing and approved by the quality control unit. purposes. Such procedures shall be (b) Written production and process control procedures shall available to the personnel for use in be followed in the execution of the various production and the areas where the procedures are process control functions and shall be documented at the time performed unless this is impractical. of performance. Any deviation from the written procedure
should be recorded and justified.
17

CURRENT GOOD MANUFACTURING PRACTICE SPECIFIC FOR
BLOOD AND BLOOD COMPONENTS
606.100(c) All records pertinent to the lot or unit maintained pursuant to these regulations (i.e., Parts 600 through 680) shall be reviewed before the release or distribution of a lot or unit of final product. The review or portions of the review may be performed at appropriate periods during or after blood collecting, processing, compatibility testing and storing. A thorough investigation, including the conclusions and follow-up, of any unexplained discrepancy or the failure of a lot or unit to meet any of its specifications shall be made and recorded.
Record review specified in 211.192 may be performed by the QC/QA unit which is comprised of one or more individuals dedicated solely to QA functions or individuals who also perform other tasks in the establishment. In the latter situation, however, individuals should not have final oversight of their own work.
There should be SOPs describing product release procedures in emergency situations.
Documentation of review of suitability of results included in in-process and laboratory testing records may consist of the signatures of the individual performing the procedure and the individual reviewing the records on the record as a whole rather than next to the results that pertain to the individual unit. Appropriate SOPs should be in place identifying individuals responsible for review and the criteria for review.
CURRENT GOOD MANUFACTURING PRACTICE FOR
FINISHED PHARMACEUTICAL (INCLUDES BLOOD AND BLOOD COMPONENTS)
211.192 All drug product production and control records, including those for packaging and labeling, shall be reviewed by the quality control unit to determine compliance with all established, approved written procedures before a batch is released or distributed. Any unexplained discrepancy... or the failure of a batch or any of its components to meet any of its specifications shall be thoroughly investigated, whether or not the batch has already been distributed. The investigation shall extend to other batches of the same drug product and other drug products that may have been associated with the specific failure or discrepancy. A written record of the investigation shall be made and shall include the conclusions and follow-up.
211.194(a) Laboratory records shall include complete data derived from all tests necessary to assure compliance with established specifications and standards including examinations and assays, as follows: (7) The initials or signature of the person who performs each test and the date(s) the tests were performed. (8) The initials or signature of a second person showing that the original records have been reviewed for accuracy, completeness, and compliance with established standards.
18

CURRENT GOOD MANUFACTURING CURRENT GOOD MANUFACTURING PRACTICE SPECIFIC FOR PRACTICE FOR
BLOOD AND BLOOD COMPONENTS FINISHED PHARMACEUTICAL (INCLUDES BLOOD AND BLOOD COMPONENTS)
211.115 (a) Written procedures shall be established and followed prescribing a system for reprocessing batches that do not conform to standards or specifications and the steps to be taken to insure that the reprocessed batches will conform with all established standards, specifications, and characteristics. (b) Reprocessing shall not be performed without the review and approval of the quality control unit.
19

CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
606.20(b) The personnel responsible for the collection, processing, compatibility testing, storage or distribution of blood or blood components shall be adequate in number, educational background, training and experience, including professional training as necessary, or combination thereof, to assure competent performance of their assigned functions, and to ensure that the final product has the safety, purity, potency, identity and effectiveness it purports or is represented to possess. All personnel shall have capabilities commensurate with their assigned functions, a thorough understanding of the procedures or control operations they perform, the necessary training or experience, and adequate information concerning the application of pertinent functions of this part to their respective functions.
211.25(a) Each person engaged in the manufacture, processing, packing or holding shall have education, training, and experience, or any combination thereof, to enable that person to perform the assigned functions. Training shall be in the particular operations that the employee performs and in current good manufacturing practice (including the current good manufacturing practice regulations in this chapter and written procedures required by these regulations) as they relate to the employee's functions. Training in current good manufacturing practice shall be conducted by qualified individuals on a continuing basis and with sufficient frequency to assure that employees remain familiar with CGMP requirements applicable to them. (b) Each person responsible for supervising the manufacture, processing, packing, or holding of a drug product shall have the education, training, and experience or any combination thereof, to perform assigned functions in such a manner as to provide assurance that the drug product has the safety, identity, strength, quality, and purity that it purports or is represented to possess. (c) There shall be an adequate number of qualified personnel to perform and supervise the manufacture, processing, packing or holding of each drug product.
20
CURRENT GOOD MANUFACTURING PRACTICE
SPECIFIC FOR BLOOD AND BLOOD COMPONENTS
CURRENT GOOD MANUFACTURING PRACTICE FOR
FINISHED PHARMACEUTICALS (INCLUDES BLOOD AND BLOOD COMPONENTS)
606.20(c) 211.28 Persons whose presence can (a) Personnel engaged in the manufacture, processing, packing, or adversely affect the safety and holding of a drug product shall wear clean clothing appropriate for purity of the products shall be the duties they perform. Protective apparel, such as head, face, and excluded from areas where the arm covering, shall be worn as necessary to protect drug products from collection, processing, contamination. compatibility testing, storage (b) Personnel shall practice good sanitation and health habits. or distribution of blood or (c) Only personnel authorized by supervisory personnel shall enter blood components is conducted. those areas of the buildings and facilities designated as limited In the Federal Register [40 FR access. 53534 Nov. 18, 1975], the (d) Any person shown at any time (either by medical examination or Commissioner stated that the supervisory observation) to have apparent illness or open lesions that intent of this regulation is to may adversely affect the safety or quality of drug products shall be also exclude from the excluded from direct contact with components, drug products processing area persons who may containers, closures, in-process materials, and drug products until distract the attention of the the condition is corrected or determined by competent medical personnel from the performance personnel not to jeopardize the safety or quality of drug products. of their duties and persons who All personnel shall be instructed to report to supervisory personnel by their very presence in the any health conditions that may have an adverse effect on drug processing area are capable of products. affecting the safety and purity of the product (e.g., persons moving from testing areas to the processing area without taking the necessary precautions.
The role of the Responsible Head in ensuring that personnel are appropriately trained and qualified for their duties is described in 606.10 and 606.20.
211.34 Consultants advising on the manufacture, processing, packing, or holding of drug products shall have sufficient education, training, and experience, or any combination thereof, to advise on the subject for which they are retained. Records shall be maintained stating the name, address, and qualifications of any consultants and the type of service they provide.
606.40(b) describes requirements for adequate ventilation. 211.46 describes ventilation control procedures in more detail.
211.46 (b) Equipment for adequate control over air pressure, micro-organisms, dust, humidity and temperature shall be provided when appropriate for the manufacture, processing, packing, or holding of a drug product. (c) Air filtration systems, including prefilters and particulate matter air filters, shall be used when appropriate on air supplies to production areas. If air is recirculated to production areas, measures shall be taken to control recirculation of dust from production. In areas where air contamination occurs during production, there shall be adequate exhaust systems or other systems adequate to control contaminants.
21

CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
211.48 (a) Potable water shall be supplied under continuous positive pressure in a plumbing system free of defects that could contribute contamination to any drug product... (b) Drains shall be of adequate size and, where connected directly to a sewer, shall be provided with an air break or other mechanical device to prevent back-siphonage.
22

CURRENT GOOD MANUFACTURING PRACTICE
SPECIFIC FOR BLOOD AND BLOOD COMPONENTS
CURRENT GOOD MANUFACTURING PRACTICE FOR
FINISHED PHARMACEUTICALS (INCLUDES BLOOD AND BLOOD COMPONENTS)
21 CFR 606.40(c) 211.52 describes adequate, clean, and Adequate facilities shall be provided, including hot and cold water, convenient hand washing soap or detergent, air dryers or single service towels, and clean facilities for personnel. toilet facilities easily accessible to working areas.
211.68 (a) Automatic, mechanical, or electronic equipment or other types of equipment including computers, or related systems that will perform a function satisfactorily, may be used in the manufacture, processing, packing, and holding of a drug product. If such equipment is so used, it shall be calibrated, inspected, or checked according to a written program designed to assure proper performance. Written records of those calibration checks and inspections shall be maintained.
(b) Appropriate controls shall be exercised over computer or related systems to assure that changes in master production records or other records are instituted only by authorized personnel. Input to and output from the computer or related system of formulas or other records or data shall be checked for accuracy. The degree and frequency of input/output verification shall be based on the complexity and reliability of the computer or related system. A backup file of data entered into the system shall be maintained except where certain data, such as calculations performed in connection with laboratory analysis, are eliminated by computerization or other automated processes. Hard copy or alternative systems, such as duplicates, tapes, microfilm designed to assure that backup data are exact and complete and that it is secure from alteration, inadvertent erasures, or loss shall be maintained.
606.40(d) 211.56 Provide safe and sanitary (a) Any building used in the manufacture, processing, packing, or disposal for the following: holding of a drug product shall be maintained in a clean and sanitary (1) Trash and items used during condition. Any such building shall be free of infestation by rodents, the collection, processing and birds,insects and other vermin (other than laboratory animals). Trash compatibility testing of blood and organic waste matter shall be held and disposed of in a timely and and blood products. sanitary manner. (2) Blood and blood components not suitable for use or distribution.
23
606.60
CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
(a) Equipment used in the collection, processing, compatibility testing, storage and distribution of blood and blood components shall be maintained in a clean and orderly manner and located so as to facilitate cleaning and maintenance. The equipment shall be observed, standardized and calibrated on a regularly scheduled basis as prescribed in the SOP and shall perform in the manner for which it was designed so as to assure compliance with the official requirements prescribed in this chapter for blood and blood products.
606.100(b)(15) requires that SOPs include schedules and procedures for equipment maintenance and calibration.
211.67 (b) Written procedures shall be established and followed for cleaning and maintenance of equipment, including utensils, used in the manufacture, processing, packing, or holding of a drug product. These procedures shall include, but are not necessarily limited to, the following: (1) Assignment of responsibility for cleaning and maintaining equipment; (2) Maintenance and cleaning schedules, including, where appropriate, sanitizing schedules; (3) A description in sufficient detail of the methods, equipment, and materials used in cleaning and maintenance operations, and the methods of disassembling equipment as necessary to assure proper cleaning and maintenance; ... (5) Protection of clean equipment from contamination prior to use; (6) Inspection of equipment for cleanliness immediately before use. (c) Records shall be kept of maintenance, cleaning, sanitizing, and inspection as specified in 211.180 and 211.182.
211.105 (b) Major equipment shall be identified by a distinctive identification number or code that shall be recorded in the batch production record to show specific equipment used in the manufacture of each batch of a drug product. In cases where only one particular type of equipment exists in a manufacturing facility, the name of the equipment may be used in lieu of a distinctive number or code.
24

606.120
CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
606.100(b)(16) requires that written SOPs include labeling procedures and safeguards to avoid labeling mixups.
(b) The labeling operation shall include the following controls: (1) Labels shall be held upon receipt, pending review and proofing against an approved final copy, to ensure accuracy regarding identity, content, and conformity with the approved copy.
211.122 (a) There shall be written procedures describing in sufficient detail the receipt, identification, storage, handling, sampling, examination, and/or testing of labeling and packaging materials; such written procedures shall be followed. Labeling and packaging materials shall be representatively sampled, and examined or tested upon receipt and before use in packaging or labeling of a drug product. (b) Any labeling or packaging materials meeting appropriate written specifications may be approved and released for use. Any labeling or packaging that does not meet such specifications shall be rejected to prevent their use in operations for which they are unsuitable. (c) Records shall be maintained for each shipment received of each different labeling and packaging material indicating receipt, examination or testing and whether accepted or not ...
25
606.120
CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
606.100(b)(16) requires that written SOPs include labeling procedures and safeguards to avoid labeling mixups.
(b) The labeling operation shall include the following controls: (2) Each type of label representing different products shall be stored and maintained in a manner to prevent mixups, and stocks of obsolete labels shall be destroyed. (3) All necessary checks in labeling shall be utilized to prevent errors in translating test results.
Label control procedures should be appropriate to control the specific labeling process or equipment. Procedures to reconcile labels should be performed if automated labeling equipment retains labeling information from previous runs that could be erroneously printed during the next use.
Packaging is addressed in Part 606 CGMPs in 606.65(a), pyrogen free container, 606.65(b), visual inspection, 606.100(b)(13), procedures to relate unit to donor, and 640.1(c), final container.
211.125 (a) Strict control shall be exercised over labeling issued for use in drug product labeling operations. (b) Labeling materials issued for a batch shall be carefully examined for identity and conformity to the labeling specified in the master or batch production records. (c) Procedures shall be utilized to reconcile the quantities of labeling issued, used, and returned, and shall require evaluation of discrepancies found between the quantity of drug product finished and the quantity of labeling issued when such discrepancies are outside narrow preset limits based on historical operating data. Such discrepancies shall be investigated in accordance with 211.192. (d) All excess labels bearing lot or control numbers shall be destroyed. (e) Returned labeling shall be maintained and stored in a manner to prevent mixups and provide proper identification. (f) Procedures shall be written describing in sufficient detail the control procedures employed for the issuance of labeling; such written procedures shall be followed.
211.130 There shall be written procedures designed to assure that correct labels, labeling, and packaging materials are used for drug products; such written procedures shall be followed. These procedures shall incorporate the following features: (a) Prevention of mixups and cross-contamination by physical or spacial separation from operations on other drug products. (b) Identification of the drug product with a lot or control number that permits determination of the history of the manufacture and control of the batch. (c) Examination of packaging and labeling materials for suitability and correctness before packaging operations, and documentation of such examination in the batch production record. (d) Inspection of the packaging and labeling facilities immediately before use to assure that all drug products have been removed from previous operations. Inspection shall also be made to assure that packaging and labeling materials not suitable for subsequent operations have been removed. Results of inspection shall be documented in the batch production records.
211.134 (a) Packaged and labeled products shall be examined during finishing operations to provide assurance that containers and packages in the lot have the correct label. (b) A representative sample of units shall be collected at the completion of finishing operations and shall be visually examined for correct labeling. (c) Results of these examinations shall be recorded in the batch production or control record.
26
CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
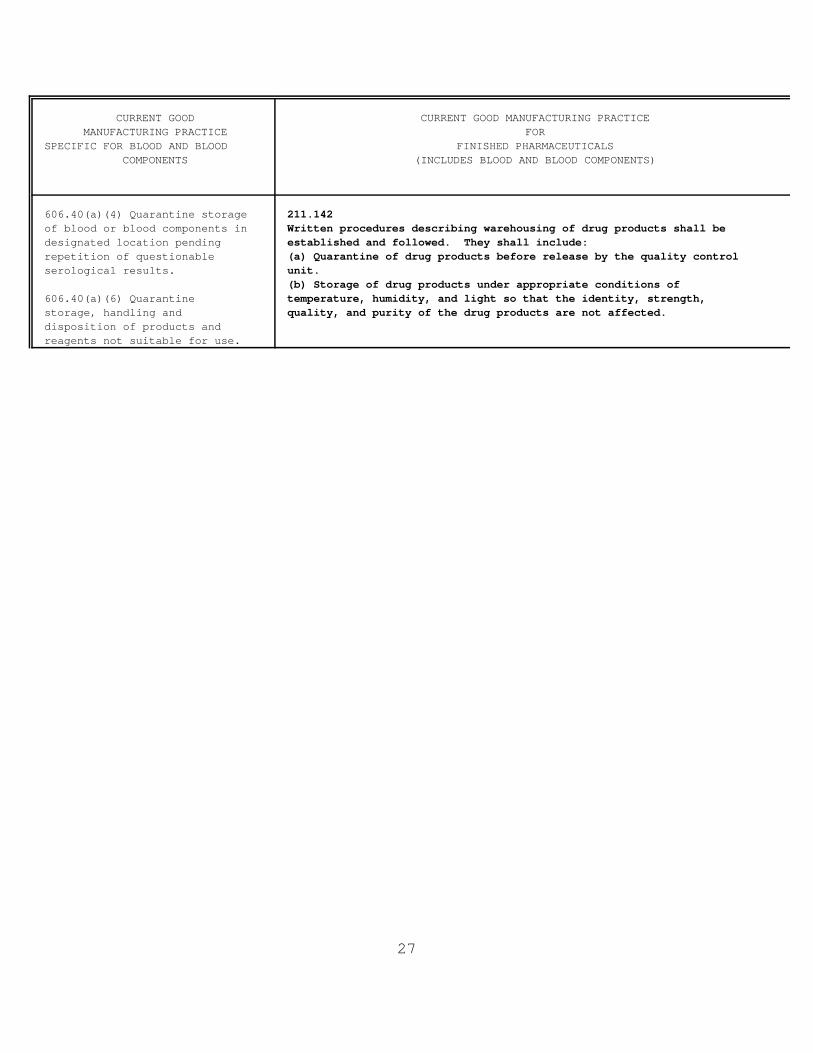
606.40(a)(4) Quarantine storage of blood or blood components in designated location pending repetition of questionable serological results.
606.40(a)(6) Quarantine storage, handling and disposition of products and reagents not suitable for use.
211.142 Written procedures describing warehousing of drug products shall be established and followed. They shall include: (a) Quarantine of drug products before release by the quality control unit. (b) Storage of drug products under appropriate conditions of temperature, humidity, and light so that the identity, strength, quality, and purity of the drug products are not affected.
27

CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
Specifications and standards for blood, blood components, and products for further manufacture are outlined in the 600s.
606.140 Laboratory control procedures shall include: (a) The establishment of scientifically sound and appropriate specifications, standards and test procedures to assure that blood and blood components are safe, pure and potent and effective. (b) Adequate provisions for monitoring the reliability, accuracy, precision and performance of laboratory test procedures and instruments. (c) Adequate identification and handling of all test samples so that they relate to the specific unit of product being tested, or to its donor, or to the specific recipient, where applicable.
606.60 (b) Equipment that shall be observed, standardized and calibrated with at least the following frequency, include but are not limited to: ...
211.160 (a) The establishment of any specifications, standards, sampling plans, test procedures, or other laboratory control mechanisms required by this subpart, including any change in such specifications, standards, sampling plans, test procedures, or other laboratory control mechanisms, shall be drafted by the appropriate organizational unit and reviewed and approved by the quality control unit. The requirements in this subpart shall be followed and shall be documented at the time of performance. Any deviation from the written specifications, standards, sampling plans, test procedures, or other laboratory control mechanisms shall be recorded and justified. (b) Laboratory controls shall include the establishment of scientifically sound and appropriate specifications, standards, sampling plans, and test procedures designed to assure that components, drug product containers, closures, in-process materials, labeling, and drug products conform to appropriate standards of identity, strength, quality, and purity. Laboratory controls shall include: (1) Determination of conformance to appropriate written specifications for the acceptance of each lot within each shipment of components, drug product containers, closures, and labeling used in the manufacture, processing, packing, or holding of drug products. The specifications shall include a description of the sampling and testing procedures used. Samples shall be representative and adequately identified. Such procedures shall also require appropriate retesting of any component, drug product container, or closure that is subject to deterioration... (4) The calibration of instruments, apparatus, gauges, and recording devices at suitable intervals in accordance with an established written program containing specific directions, schedules, limits for accuracy and precision, and provisions for remedial action in the event accuracy and/or precision limits are not met. Instruments, apparatus, gauges, and recording devices not meeting established specifications shall not be used.
28

CURRENT GOOD MANUFACTURING PRACTICE
SPECIFIC FOR BLOOD AND BLOOD COMPONENTS
CURRENT GOOD MANUFACTURING PRACTICE FOR
FINISHED PHARMACEUTICALS (INCLUDES BLOOD AND BLOOD COMPONENTS)
Required and recommended viral marker testing, quality control testing, and other product testing combined with testing requirements outlined in an establishment's SOP are product specifications. Acceptance criteria are determined from product specifications.
211.165 (a) For each batch of drug product, there shall be appropriate laboratory determination of satisfactory conformance to final specifications for the drug product... (d) Acceptance criteria for the sampling and testing conducted by the quality control unit shall be adequate to assure that batches of drug products meet each appropriate specification and appropriate statistical quality control criteria as a condition for their approval and release. The statistical quality control criteria shall include appropriate acceptance levels and/or appropriate rejection levels. (e) The accuracy, sensitivity, specificity, and reproducibility of test methods employed by the firm shall be established and documented... (f) Drug products failing to meet established standards or specifications and any other relevant quality control criteria shall be rejected. Reprocessing may be performed. Prior to acceptance and use, reprocessed material must meet appropriate standards, specifications, and any other relevant criteria.
606.120(a)(1) Labels shall be 211.184 held upon receipt, pending (d) Documentation of the examination and review of labels and labeling review and proofing against an for conformity with established specifications in accord with approved final copy, to ensure 211.122(c) and 211.130(c). accuracy regarding identity, content, and conformity with the approved copy.
606.160(b)(2)(v) provides for maintaining records of labeling, including the initials of the person responsible.
Master production and control records should include the signatures required in 211.186(a).
211.186 (a) To assure uniformity from batch to batch, master production and control records for each drug product, including each batch size thereof, shall be prepared, dated, and signed (full signature, handwritten) by one person and independently checked, dated, and signed by a second person. The preparation of master production and control records shall be described in a written procedure and such procedure shall be followed.
29
CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
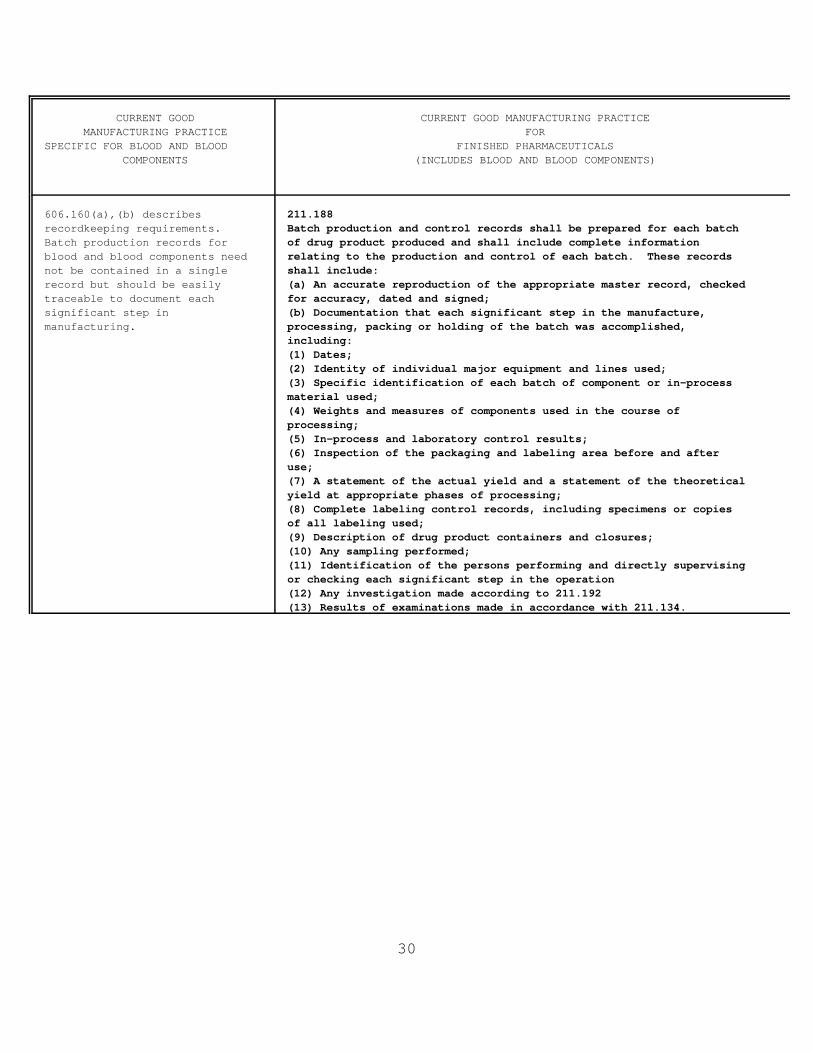
606.160(a),(b) describes recordkeeping requirements. Batch production records for blood and blood components need not be contained in a single record but should be easily traceable to document each significant step in manufacturing.
211.188 Batch production and control records shall be prepared for each batch of drug product produced and shall include complete information relating to the production and control of each batch. These records shall include: (a) An accurate reproduction of the appropriate master record, checked for accuracy, dated and signed; (b) Documentation that each significant step in the manufacture, processing, packing or holding of the batch was accomplished, including: (1) Dates; (2) Identity of individual major equipment and lines used; (3) Specific identification of each batch of component or in-process material used; (4) Weights and measures of components used in the course of processing; (5) In-process and laboratory control results; (6) Inspection of the packaging and labeling area before and after use; (7) A statement of the actual yield and a statement of the theoretical yield at appropriate phases of processing; (8) Complete labeling control records, including specimens or copies of all labeling used; (9) Description of drug product containers and closures; (10) Any sampling performed; (11) Identification of the persons performing and directly supervising or checking each significant step in the operation (12) Any investigation made according to 211.192 (13) Results of examinations made in accordance with 211.134.
30

606.170
CURRENT GOOD CURRENT GOOD MANUFACTURING PRACTICE MANUFACTURING PRACTICE FOR
SPECIFIC FOR BLOOD AND BLOOD FINISHED PHARMACEUTICALS COMPONENTS (INCLUDES BLOOD AND BLOOD COMPONENTS)
(a) Records shall be maintained of any reports of complaints of adverse reactions regarding each unit of blood or blood product arising as a result of blood collection or transfusion. A thorough investigation of each reported adverse reaction shall be made. A written report of the investigation of adverse reactions, including conclusions and follow-up, shall be prepared and maintained as part of the record for that lot or unit of final product by the collecting or transfusing facility. When it is determined that the product was at fault in causing a transfusion reaction, copies of all such written reports shall be forwarded to and maintained by the manufacturer or collecting facility.(b) When a complication of blood collection or transfusion is confirmed to be fatal, theDirector, Office of Compliance, Center for Biologics Evaluation and Research, shall be notified by telephone or telegraph as soon as possible; a writtenreport of the investigation shall be submitted to the Director, Office of Compliance, Center for Biologics Evaluation and Research, within 7 days after the fatality by the collecting facility in the event of a donor reaction, or by the facility that performed the compatibility tests in the event of a transfusion reaction.
211.198 (a) Written procedures describing the handling of all written and oral complaints regarding a drug product shall be established and followed. Such procedures shall include provisions for review by the quality control unit, of any complaint involving the possible failure of a drug product to meet any of its specifications and, for such drug products, a determination as to the need for an investigation in accordance with 211.192. Such procedures shall include provisions for review to determine whether the complaint represents a serious and unexpected adverse drug experience which is required to be reported to the Food and Drug Administration in accordance with 310.305 of this chapter. (b) A written record of each complaint shall be maintained in a file designated for drug product complaints. The file regarding such drug product complaints shall be maintained at the establishment where the drug product involved manufactured, processed, or packed, or such file may be maintained at another facility if the written records in such files are readily available for inspection at that other facility. Written records involving a drug product shall be maintained until at least 1 year after the expiration date of the drug product, or 1 year after the date that the complaint was received, whichever is longer. In the case of certain OTC drug products lacking expiration dating because they meet the criteria for exemption under 211.137, such written records shall be maintained for 3 years after distribution of the drug product. (1) The written record shall include the following information, where known; the name and strength of the drug product, lot number, name of complainant, nature of complaint, and reply to complainant. (2) Where an investigation under 211.192 is conducted, the written record shall include the findings of the investigation and follow-up. The record or copy of the record of the investigation shall be maintained at the establishment where the investigation occurred in accordance with 211.180(c). (3) Where an investigation under 211.192 is not conducted, the written record shall include the reason that an investigation was found not to be necessary and the name of the responsible person making such a determination.
31
Appendix B. TABLES OF SYSTEMS
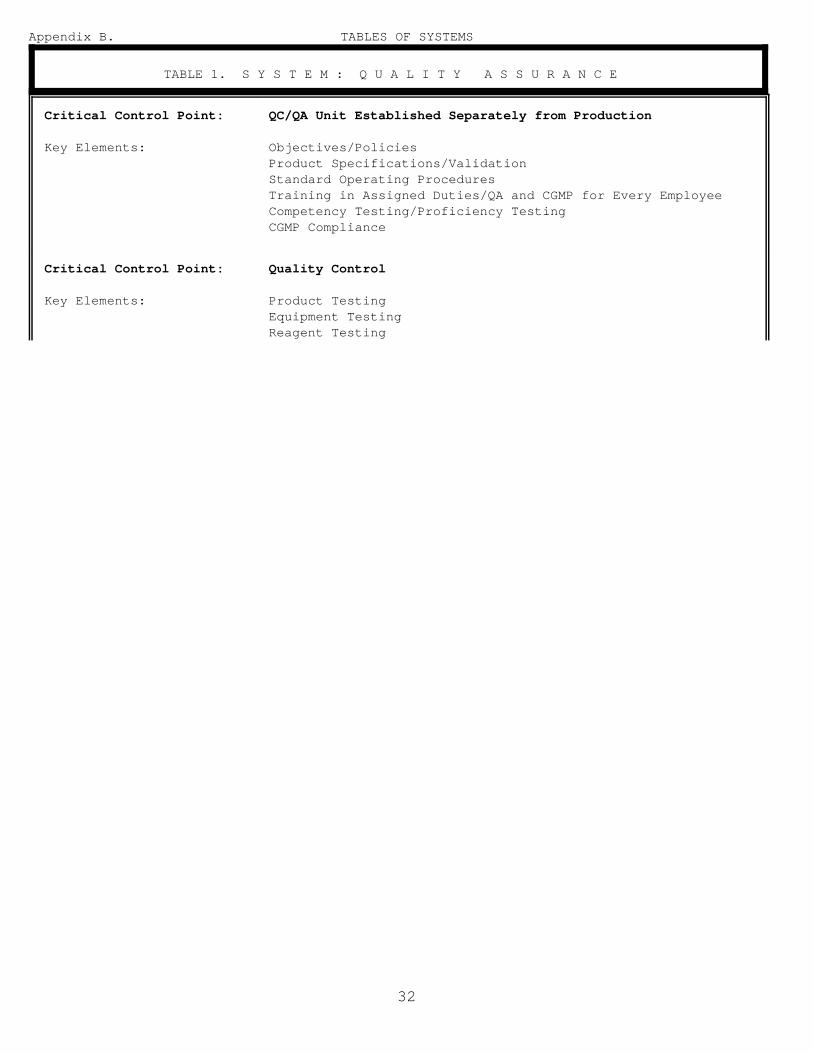
TABLE 1. S Y S T E M : Q U A L I T Y A S S U R A N C E
Critical Control Point: QC/QA Unit Established Separately from Production
Key Elements: Objectives/Policies Product Specifications/Validation Standard Operating Procedures Training in Assigned Duties/QA and CGMP for Every Employee Competency Testing/Proficiency Testing CGMP Compliance
Critical Control Point: Quality Control
Key Elements: Product Testing Equipment Testing Reagent Testing
32

Critical Control Point: QA Audits
Key Elements: Systems Working Separately and Collectively Thresholds (Limits) Alert Levels/Action Levels Written Audit Reports Report Evaluation/Data Analysis Feedback Corrective Action/Follow-up Investigation
Critical Control Point: Complaints/Defects/Adverse Reaction Report Evaluation
Key Elements: Procedures Include Cause/Effect Evaluation Error and Accident Reports Laboratory Error Reports Donor Callbacks (Post Donation Information) User Complaints Post Transfusion Disease/Other Adverse Reactions Timely Evaluations Follow-up Investigation/Problem Resolution
Critical Control Point: Information Flow
Key Elements: Regular Review of Manufacturer's Instructions for Use to Identify Changes and Incorporate Changes in SOPs
Procedures to Issue New/Remove Old SOPs Changes Provided to Actual Users All Shifts/BackUp Personnel Included FDA Letters to Those Who Need to Know Managers Receive Accurate/Timely Information
Critical Control Point: Equipment Maintenance/Repair
Key Elements: Qualification/Acceptance Testing Preventative Maintenance Routine/Scheduled Maintenance Maintenance Records Qualification/Validation After Repair Repair Records
33
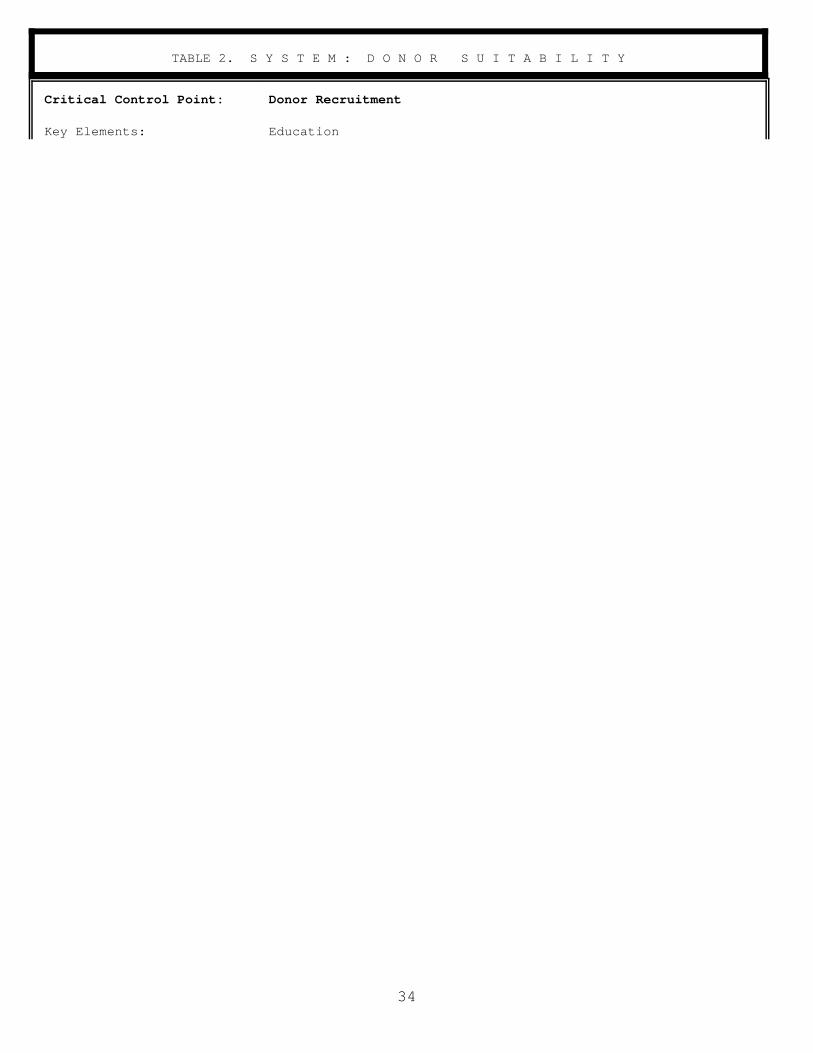
TABLE 2. S Y S T E M : D O N O R S U I T A B I L I T Y
Critical Control Point: Donor Recruitment
Key Elements: Education
34

Critical Control Point:
Key Elements:
Donor Registration
Accurate Information Provided by the Donor Accurate Information Entered in Record Files Certainty of Identifiers/Permanently Effective Method to Prevent Known Unsuitable Donors from Donating (
E x a m p l e : U s e o f D o n o r D e f e r r a l R e g i s t r y a t t h e t i m e o f r e g i s t r
35
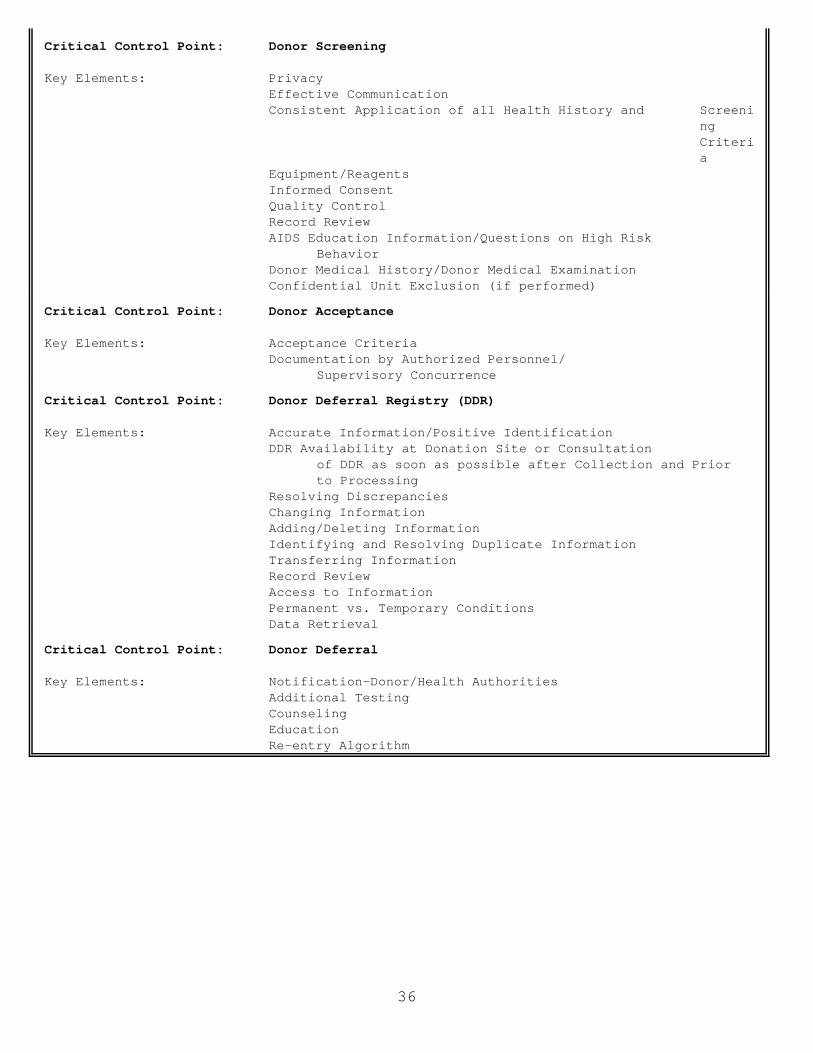
Critical Control Point: Donor Screening
Key Elements: Privacy Effective Communication Consistent Application of all Health History and Screeni
ng Criteri a
Equipment/Reagents Informed Consent Quality Control Record Review AIDS Education Information/Questions on High Risk
Behavior Donor Medical History/Donor Medical Examination Confidential Unit Exclusion (if performed)
Critical Control Point: Donor Acceptance
Key Elements: Acceptance Criteria Documentation by Authorized Personnel/
Supervisory Concurrence
Critical Control Point: Donor Deferral Registry (DDR)
Key Elements: Accurate Information/Positive Identification DDR Availability at Donation Site or Consultation
of DDR as soon as possible after Collection and Prior to Processing
Resolving Discrepancies Changing Information Adding/Deleting Information Identifying and Resolving Duplicate Information Transferring Information Record Review Access to Information Permanent vs. Temporary Conditions Data Retrieval
Critical Control Point: Donor Deferral
Key Elements: Notification-Donor/Health Authorities Additional Testing Counseling Education Re-entry Algorithm
36

TABLE 3. S Y S T E M : B L O O D C O L L E C T I O N
Critical Control Point: Blood, Component, Source Plasma Collection
Key Elements: Identification of Donor, Containers, Pilot Samples,
Verification that Donor corresponds to Container, Pilot Sample, Components, Records
Arm Preparation Equipment/Supplies/IV Solutions Collection Set/Container Type Donor Adverse Reactions Overbleeding/Underbleeding Product Specifications Automated Collection Multiple Component Harvesting Volume of Product Retained/Returned to Donor Material Defects Procedural Errors Record Review
Compone nts, Records
Critical Control Point: Donor Immunization Program
Key Elements: Antigen Safety, Purity, and Potency Antigen Selection and Administration/Schedules/Doses Donor Antibody Production and Evaluation Product Specifications for Labeled Use/Discard Disposition of Low Titer or Other Unsuitable
Product Donor Medical Record Review Adverse Reactions Product Record Review
37

TABLE 4. S Y S T E M : C O M P O N E N T M A N U F A C T U R I N G
Critical Control Point: Component Preparation
Key Elements: Acceptance Criteria for Source Blood Product (e.g., prolong ed bleeds, suitabl e donors, etc.)
Preparation Time/Temperature/Equipment/Weight or Volume Assignment of Expiration Date Anticoagulant/Additive Solution/Container Sterile Connection Device/Pooling Apparatus/Other Devices Record Review Quality Control (Including Sampling Size) Disposition of All Products Shipping, Holding Temperature Conditions of Centrifugation Identification of Personnel/Equipment
Critical Control Point: Labeling-Manual
Key Elements: Label Acceptance Review Prior to Use Product Specific Expiration Date Assignment Verification of Correct Labeling Records of Labeling Operations
Critical Control Point: Labeling-Computerized
Key Elements: Bar Coding Label Control, Reconciliation On-Line Printing Devices On Demand/Batch Printing
Critical Control Point: Quarantine
Key Elements: Location of Product-Untested, Repeat Test Pending, Biohazardous, Not Meeting Specifications, Unsuitable for Transfusion, Autologous, Directed
Processing Record Review/Review by Second Person Destruction or Other Disposition/Records Equipment
Critical Control Point: Sterile Connecting Device
Key Elements: Integrity of Weld "Like Tubing"
38
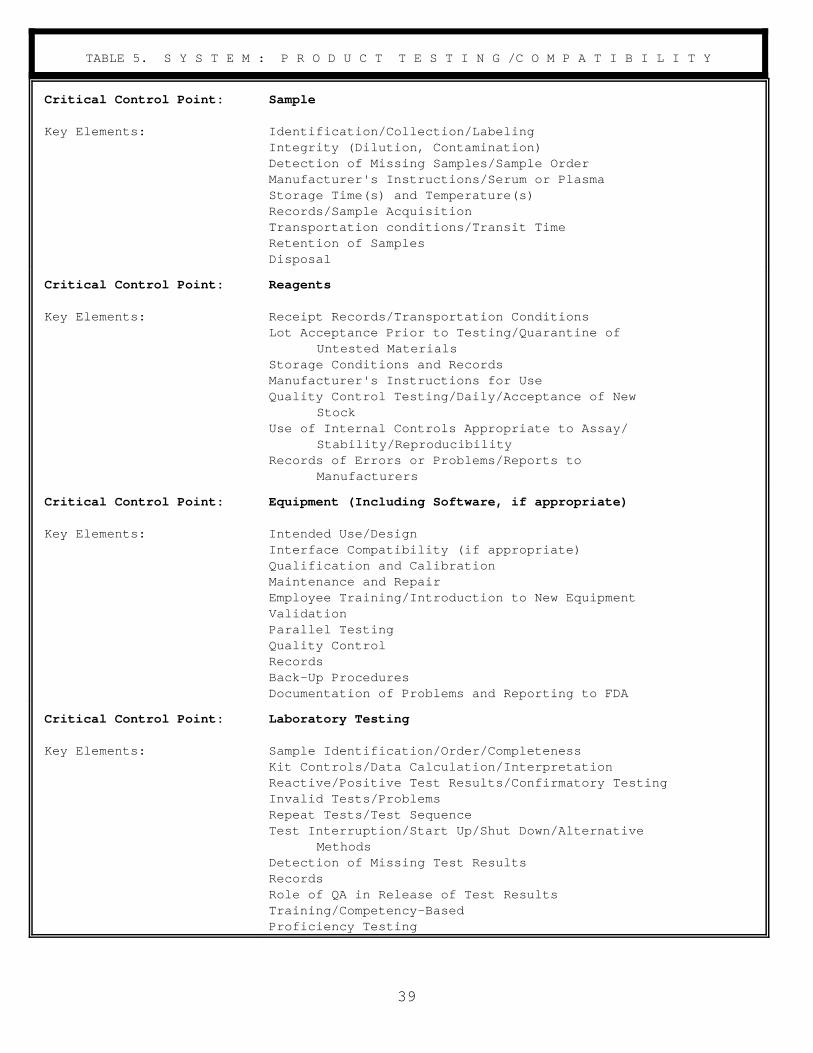
TABLE 5. S Y S T E M : P R O D U C T T E S T I N G /C O M P A T I B I L I T Y
Critical Control Point:
Key Elements:
Critical Control Point:
Key Elements:
Critical Control Point:
Key Elements:
Critical Control Point:
Key Elements:
Sample
Identification/Collection/Labeling Integrity (Dilution, Contamination) Detection of Missing Samples/Sample Order Manufacturer's Instructions/Serum or Plasma Storage Time(s) and Temperature(s) Records/Sample Acquisition Transportation conditions/Transit Time Retention of Samples Disposal
Reagents
Receipt Records/Transportation Conditions Lot Acceptance Prior to Testing/Quarantine of
Untested Materials Storage Conditions and Records Manufacturer's Instructions for Use Quality Control Testing/Daily/Acceptance of New
Stock Use of Internal Controls Appropriate to Assay/
Stability/Reproducibility Records of Errors or Problems/Reports to
Manufacturers
Equipment (Including Software, if appropriate)
Intended Use/Design Interface Compatibility (if appropriate) Qualification and Calibration Maintenance and Repair Employee Training/Introduction to New Equipment Validation Parallel Testing Quality Control Records Back-Up Procedures Documentation of Problems and Reporting to FDA
Laboratory Testing
Sample Identification/Order/Completeness Kit Controls/Data Calculation/Interpretation Reactive/Positive Test Results/Confirmatory Testing Invalid Tests/Problems Repeat Tests/Test Sequence Test Interruption/Start Up/Shut Down/Alternative
Methods Detection of Missing Test Results Records Role of QA in Release of Test Results Training/Competency-Based Proficiency Testing
39

TABLE 6. S Y S T E M : L O T R E L E A S E
Critical Control Point: Verification of Purported Labeling Claims
Key Elements: Record Review : All Testing, required and recommended, was performed according to manufacturer's instructions and SOP, and the results are acceptable for release
Record Review: All Quality Control was performed, and results were within acceptable limits
Record Review: All Manufacturing Records verified and approved by designated, responsible personnel prior to the release of every component
Record Review: Correct Expiration Date Assigned
Documentation of All Review
Critical Control Point: Donor Suitability
Key Elements: Record Review Deferral Registry
40
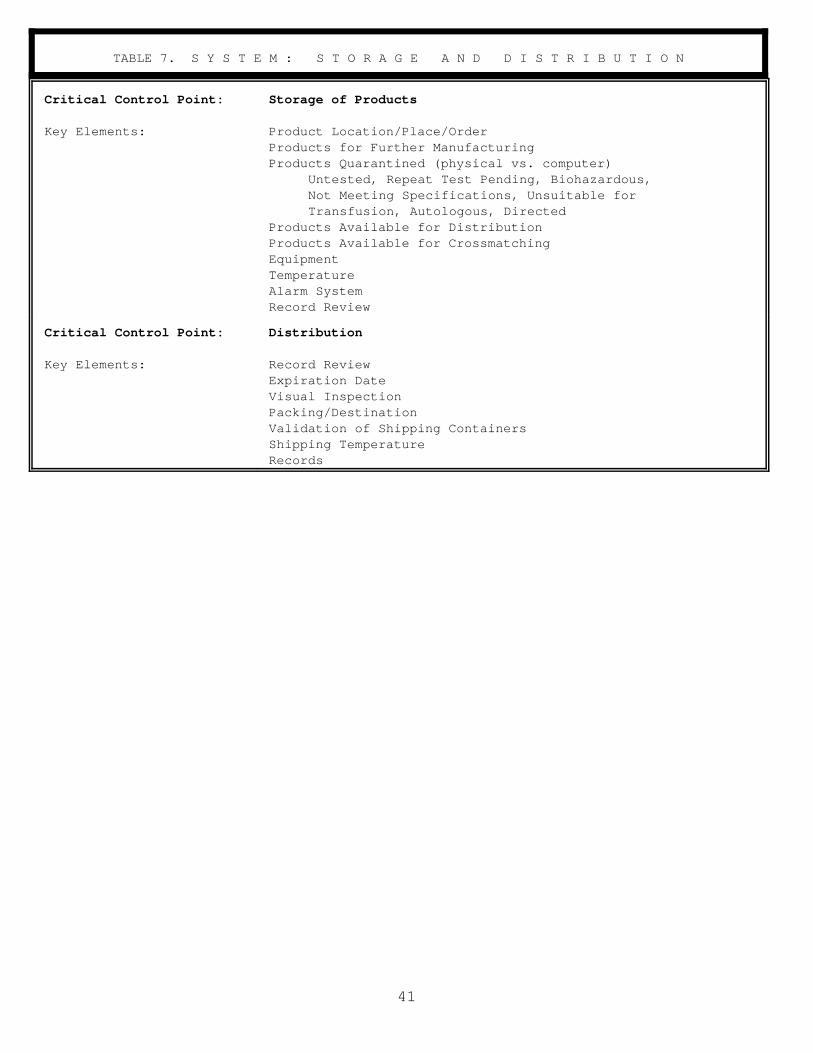
TABLE 7. S Y S T E M : S T O R A G E A N D D I S T R I B U T I O N
Critical Control Point: Storage of Products
Key Elements: Product Location/Place/Order Products for Further Manufacturing Products Quarantined (physical vs. computer)
Untested, Repeat Test Pending, Biohazardous, Not Meeting Specifications, Unsuitable for Transfusion, Autologous, Directed
Products Available for Distribution Products Available for Crossmatching Equipment Temperature Alarm System Record Review
Critical Control Point: Distribution
Key Elements: Record Review Expiration Date Visual Inspection Packing/Destination Validation of Shipping Containers Shipping Temperature Records
41

TABLE 8. S Y S T E M : C O M P U T E R
Critical Control Point:
Key Elements:
Critical Control Point:
Key Elements:
Critical Control Point:
Key Elements:
Critical Control Point:
Key Elements:
Documentation
Hardware - listing of equipment, installation date serial numbers, maintenance records, electrical and environmental requirements, installation instructions, maintenance schedules and procedures
Software - listing of programs, general program descriptions, program interaction, development,changes, archives, test plans, testing review and evaluation, and implementation date(s)
Validation of Components and systems Personnel/SOPs Training programs, Outlines, and Documentation
Testing the Computer System
Develop and maintain a test database/test plan (SOP) (as appropriate)
Develop and maintain test case protocols to cover normal,exceptional, boundary, stress, and invalid test cases
Perform testing and document results Parallel Testing Define and document evaluation of the test process Document modifications performed as a result of
testing
Implementation
Define and document implementation process Equipment Interface Change Control Approval Process Procedures for Back-up and Restore Procedures for Data Conversion(s) Procedures for Downtime Software Archives (as appropriate) Security/Passwords
Maintenance
Hardware Software for Applications and Operating Systems Change Control Approval Process Archives Procedures for Back-Up and Restore Procedures for Downtime Routine Audits of Data and Systems
Also, please refer to the critical control points Labeling-Computerized, Table 4., Component Manufacturing and Equipment/Software, Table 5., Product Testing.
42

GLOSSARY Action Level: A limit that indicates the need to immediately identify the source of a discrepancy and make the necessary corrections to avoid a compromise in product quality. The QC/QA unit approves and evaluates adherence to this limit.
Alert Level: A limit that a potential problem needs to be identified and corrected but does not indicate that an effect on product quality has resulted. The QC/QA unit approves and evaluates adherence to this limit.
Audit: See Quality Assurance Audit.
Competency Evaluation: An internal process for assessing an individual's ability to perform all assigned tasks. A variety of performance appraisal methods may be used.
Component: (1) That part of a single-donor unit of blood separated by physical or mechanical means [See 21 CFR 606.3(c)]. (2) Any ingredient intended for use in the manufacture of a drug product, including those that may not appear in such drug product [See 21 CFR 210.3(b)(3)]. (3) A piece of equipment or software associated with a computerized system.
Computer Change Control: The process of identifying, evaluating, coordinating, implementing, documenting, and obtaining formal approval of changes in a computerized system or database.
Critical Control Point: A function or an area in a manufacturing process or procedure that failure or loss of control may have an adverse effect on the quality of the finished product and may result in a health risk.
Current Good Manufacturing Practice (CGMP): Methods used in, and the facilities or controls used for, the manufacture, processing, packing, or holding of a drug including, but not limited, to blood products to assure that such product meets the requirements of the FD&C Act as to safety and has the identity and strength, and meets the quality and purity characteristics, which it purports or is represented to possess [See FD&C Act, Sec. 501(a)(2)(B)]. CGMP ensures products are consistently manufactured and controlled by quality standards appropriate to their intended use. It encompasses both manufacturing and quality control/quality assurance procedures.
Key Element: An individual step in a critical control point of the manufacturing process.
Maintenance: Activities such as adjusting, cleaning, modifying, overhauling equipment to assure performance in accordance with requirements. Maintenance to a software system includes, among other things, correcting software errors, adapting software to a new environment, or making enhancements to software.
Manufacture: Blood is produced by the body and requires further processing before it can be safely transfused. The term manufacture is defined, in part, in 21 CFR 600.3(u), as all steps in the propagation or manufacture and preparation of products. The biologics regulations prescribe requirements concerning all aspects of the manufacture of blood even before it is collected from the donor (e.g., donor suitability criteria). Manufacture is also used in the FD&C Act and the PHS Act in direct reference to blood and blood products [40 FR 53532, November 18, 1975].
Parallel Test or Parallel Run. Functional testing performed using two or more different systems simultaneously. This may include comparison of an established system to a new system. (International Standards Organization definition: A test run of a new or an altered data processing system with the same source data that is used in another system; the other system is considered as the standard of comparison.)
Production: The name given to personnel and/or operations involved in manufacturing.
43

Proficiency Testing: An evaluation of "the ability to perform laboratory procedures within acceptable limits of accuracy, through the analysis of unknown specimens distributed at periodic intervals by an external source" (Deboy and Jarboe, 1991).
Program Description: A narrative that describes a computer program's functions and interaction with other programs.
Qualification: Establishing confidence that process equipment, reagents, and ancillary systems are capable of consistently operating within established limits and tolerances. Process performance qualification is intended to establish confidence that the process is effective and reproducible.
Quality: Conformance of a product or process with pre-established specifications or standards.
Quality Assurance (QA): The actions, planned and performed, to provide confidence that all systems and elements that influence the quality of the product are working as expected individually and collectively.
Quality Assurance Audit: A documented, independent inspection and review of manufacturing and associated systems, performed periodically according to written procedures to verify, by examination and evaluation of objective evidence, the degree of compliance with those elements of the QA program under review.
Quality Assurance Program: An organization's comprehensive system for manufacturing safe, effective, and quality products according to regulatory standards. This program includes preventing, detecting, and correcting deficiencies that may compromise product quality.
Quality Control/Assurance (QC/QA) Unit: One or more individuals designated by, and reporting directly to, management with defined authority and responsibility to assure that all quality assurance policies are carried out in the organization.
Quality Control (QC): A component of a QA program that includes the activities and controls used to determine the accuracy and reliability of the establishments' personnel, equipment, reagents, and operations in the manufacturing of blood products including testing and product release.
Specification(s): Physical characteristics and composition, performance characteristics, parameters, requirements, standards, intended functions, behavior, or other characteristics of a product, system, or part of a system (as appropriate).
Test Cases: (as applied to computerized systems)
# Normal: valid data sets are used to produce normal outputs;
# Exceptional: valid data which provide an unusual twist to force the program to react to the unexpected;
# Boundary: data which force the program to evaluate conditions that are of borderline validity or at the boundaries of pre-established alert or action levels for control;
# Stress: data which forces the system to reach its maximum level of performance (during development and in the environment of the user);
# Invalid: data that are not valid; test data should be designed to force a program to prove that it can detect and respond appropriately to invalid input. Examples of invalid test cases may include an
44

invalid donation date, e.g., 02/30/91; an invalid ABO group, e.g., "P"; a negative hemoglobin value; or no data entry.
Test Database: A database containing normal and abnormal values created by copying the production database and adding anomalous data. The test database is used to challenge a computerized system during validation and/or acceptance testing.
Thresholds: Guideline values which are needed in reviewing records to determine the adequacy of performance. These are the acceptable limits for quality to determine when intervention is necessary. Thresholds may be expressed as a number or percentage.
Validation: Establishing documented evidence which provides a high degree of assurance that a specific process will consistently produce a product meeting its predetermined specifications and quality attributes. A process is validated to evaluate the performance of a system with regard to its effectiveness based on intended use.
45

REFERENCES
Health and Human Services References
l. Title 21, Code of Federal Regulations, Parts 210, 211, 600, 606, 610, 640, 660.
2. FDA, Center for Drugs and Biologics and Center for Devices and Radiological Health (CDRH), Guideline on General Principles of Process Validation (May 1987).
3. FDA 91-4179: CDRH, Medical Device Good Manufacturing Practices Manual, 5th Edition (August 1991).
4. FDA Compliance Program Guidance Manual, Blood and Blood Products, 7342.001, 7342.002.
5. FDA Compliance Policy Guide, FDA Access to Results of Quality Assurance Program Audits and Inspections, 7151.02, 1989.
6. FDA Memorandum: April 6, 1988, Control of Unsuitable Blood and Blood Components.
7. FDA Memorandum: March 20, 1991, Deficiencies Relating to the Manufacture of Blood and Blood Components.
8. Federal Register, Volume 43, No. 190, September 29, 1978, Human and Veterinary Drugs, Current Good Manufacturing Practice in Manufacture, Processing, Packing, or Holding, 4501345087.
9. Federal Register, Volume 40, No. 223, November 18, 1975, Human Blood and Blood Products, Collection, Storage and Processing, 53532-53544.
10. Federal Register, Volume 57, No. 40, February 28, 1992, Clinical Laboratory Improvement Amendments of 1988; Final Rule, 7002-7288.
11. FDA, Center for Biologics Evaluation and Research (CBER), Draft Guideline for the Validation of Blood Establishment Computer Systems; Docket No. 93N-0394, October 28, 1993.
General References
Accreditation Manual for Hospitals. 1991. Joint Commission on Accreditation of Healthcare Organizations.
Bartlett, R. Leadership for Quality. 1991. ASM News; 57:15-21.
DeBoy, J. and Jarboe, B. Government-Mandated Cytology Proficiency Testing: Practical, Equitable and Defensible Standards. 1991. ORB; 152-161.
Juran, J. Quality Control Handbook. 1974. McGraw-Hill.
Kritchevsky, S. and Simmons, B. Continuous Quality Improvement: Concepts and Applications for Physician Care. 1991. JAMA; 266:1817-1823.
Melum, M.M. Total Quality Management: Steps to Success. 1990. Hospitals 64(23):42,44.
Milakovich, M.E. Creating a Total Quality Health Care Environment. 1991. Health Care Manage Rev; 16(2):9-20
McLaughlin, C.P. and Kaluzny, A.D. Total Quality Management in Health: Making It Work. 1990. Health Care Manage Rev; 15(3): 7-14.
46

Olso, A. Remmington's Pharmaceutical Sciences. 1980. Control; 16(82):1434-8.
Rosvoll, R., Editor, Accreditation Requirements Manual of the American Association of Blood Banks. 1990. American Association of Blood Banks.
Walker, R., Editor, Technical Manual, 11th Edition. 1993. American Association of Blood Banks.
47