Embed Size (px)
Citation preview

Bull. Org. mond. Sane 1960, 22, 469-484Bull. Wld Hlth Org.
Food-borne Infections and Intoxications in Europe*Dr H. P. R. SEELIGER 1
Any attempt to evaluate the prevalence of food-borne diseases in Europe is fraughtwith difficulty, partly because in some countries such diseases, if reported, are not clearlydesignated as food-borne, and partly because of the variety in terminology and methods ofclassification.
Nevertheless, it is apparent that, although certain food-borne infections have decreasedin prevalence, others have increased during the past decade. This increase has been shownto be related in some countries to the import of certain foodstuffs andfodder from tropicaland subtropical regions and has resulted in a general spread of Salmonella infections bya wide variety of serotypes. Food-borne intoxications are predominantly caused by theingestion of the toxins elaborated by the growth of Staphylococcus aureus in food and byspore-forming bacilli. Botulism is now rare in Europe.
While the recent increase in the prevalence of these diseases calls for strict supervisionoffoodproducts and improved measures of ensuringfood hygiene, the efficacy ofsuch stepsas may be taken will depend on close co-operation between public health and veterinarypublic health authorities.
HISTORY AND GENERAL REMARKS
The knowledge of food-borne infections andmtoxications in Europe dates back to the early daysof medical bacteriology when it became apparentthat such dread diseases as typhoid fever, para-typhoid fever and dysentery could frequently betraced to the consumption of food contaminatedwith enteropathogenic bacteria.
Besides direct-contact and water-borne infections,various foodstuffs-either contaminated directly (bycarriers, etc.) or indirectly (by flies, etc.) with theprimary human pathogens, Salmonella typhi, Salm.paratyphi A and B and those of the Shigella group-were incriminated as vehicles of infection of theseclassical anthroponoses. The microbes causingscarlet fever and diphtheria were also occasionallyfound to be spread by contaminated food.
In addition to such micro-organisms of strictlyhuman origin, several animal pathogens known tocause zoonoses in a variety of wild and domesticanimals were recognized as important agents of
* Modified version of a paper submitted to the EuropeanTechnical Conference on Food-borne Infections and Intoxi-cations, held in February 1959 under the auspices of theWHO Regional Office for Europe.
1 Privatdozent in Medical Microbiology and Head of theNational Salmonella Centre, Institute of Hygiene, Universityof Bonn, Federal Republic of Germany
human food-borne infections. This, for instance, istrue of all salmonelloses with the exception of thesepticaemic and enteric fevers due to the above-mentioned organisms whose natural host is thehuman being. Other dangerous diseases like Maltafever, Bang's disease and tuberculosis are also quiteoften food-borne. The same occasionally applies totularaemia, listeriosis and other zoonoses.A third group of bacterial food-borne illness in
man is represented by several more or less dangerousintoxications. Such toxicoses are provoked by theingestion, often of minute amounts, of powerfulexotoxins elaborated by saprophytic soil bacteriaand by parasitic human microbes in certain typesof food under favourable conditions. A well-knownexample of the saprophytic toxicoses is botulism,with its high fatality rate. Food-poisoning due tostaphylococcal enterotoxins, Clostridium welchii andother toxogenic bacteria has only been shown to bea major problem during the past two decades follow-ing the elucidation of the etiology of " non-specific"food-poisoning.
CLASSIFICATION AND TERMINOLOGY
Before discussing the subject in detail, the ter-minology of bacterial food-borne diseases requirescomment, for it is a rather complex problem. Invarious languages the term " bacterial food poison-
874 -469-

H. P. R. SEELIGER
ing" (intoxication alimentaire, toxi-infection ali-mnentaire, bakterielle Nahrungsmittelvergiftung, etc.)is used. It is sometimes applied in its true sense,meaning food-borne intoxication. But it is fre-quently used in a general manner to describe alltypes of food-borne disease, including typicalinfections by human and animal pathogens.One of the main reasons for this has been the
extreme difficulty experienced by many physiciansin establishing a rapid and reliable clinical diagnosis.This is mainly due to the complexity and overlappingof clinical symptoms.Only during the past decade has the medical
profession made any considerable progress indifferential diagnosis based on the symptomatologyof certain food-borne bacterial diseases. This mustbe attributed to the invaluable support given to thephysician by the bacteriological laboratory. Onthe basis of laboratory findings it is now possible tocorrelate clinical entities with certain etiologicalagents. Where this practice has been followed theso-called " non-specific" cases of food-poisoninghave decreased in number and have been replacedmore and more by " specific " terms in which theetiology is related to typical clinical syndromes.Today, designations like " salmonellosis ", " staphy-lococcal food-poisoning ", " Clostridium welchiifood-poisoning ", " Bacillus cereuis food-poisoning ",etc. have found general recognition and are beingused with increasing frequency.
Several other infectious diseases, such as typhoidfever, paratyphoid fever, dysentery, coli-enteritis etc.,are not classified as food-borne diseases, though ina number of instances they are certainly food-borne.Owing to the variable period of incubation, theorigin of the infection is quite often obscure andonly in a certain proportion of episodes is it estab-lished by subsequent epidemiological investigations.It seems logical that such infections should beclassified under their proper name. This, however,ought not to prevent the public health officer frommaking careful inquiries as to the source of infection.Establishment of the chain of infection is of con-siderable importance in the control of these diseases,which may be subdivided according to their modeof transmission. Thus the term typhoid fever wouldbe used in the general classification, and in the sub-division the proportion of water-borne, food-borne,contact and other types of infection would beindicated. This procedure would facilitate judge-ment as to the predominant route of transmissionin certain areas.
The general designation " food-borne infection"seems to be most useful when it is restricted toclinically apparent or inapparent infections causedpredominantly by micro-organisms, or almostexclusively transmitted by directly or indirectly con-taminated food.Only if the food-borne nature of the illness is
diagnosed or suspected by the attending physiciancan further steps be taken by the public healthauthorities to prove or disprove the presumptivediagnosis of bacterial food-poisoning and to replacethis general term by the etiological designation.
In practice this would mean that wherever clinicaland circumstantial evidence points to food as thecause of an infection or intoxication, the disease willbe classified by the clinician as food-borne. Wherethe onset, symptoms, clinical course etc. are typical,he may at least have grounds for suspecting aparticular etiological agent.
In many acute infections, particularly in thosecaused by salmonellae, signs of intoxication prevailat the beginning of the illness and symptoms of trueinfection-fever, etc.-follow later.
Other medical designations, such as vomiting,vomiting and diarrhoea, enteritis, colitis, gastro-enteritis, etc., are merely descriptive and are irrelevantto the mode of transmission.
In short, the general trend is to use etiologicalterms in the classification of bacterial food-bornediseases instead of merely descriptive clinical desig-nations.From the standpoint of the epidemiologist and
of the public health officer it is imperative that thephysician use a classification (quite apart from hisclinical diagnosis) which points to the possiblesource. Doctors should therefore be encouragedto include important epidemiological features in theclassification of diseases.
It should be mentioned that this method ofclassification was not used in the 1955 revision ofthe International Classification of Diseases (WorldHealth Organization, 1957). For instance, somebacterial food-borne diseases with predominantintestinal involvement may be found classified underinfectious diseases commonly arising in the intestinaltract (040-049). These, which exclude enteritis(571, 764) and diarrhoea (571, 764, 785.6), are asfollows:040 Typhoid fever041 Paratyphoid fever042 Other Salmonella infections043 Cholera
470

FOOD-BORNE INFECTIONS AND INTOXICATIONS IN EUROPE
044045046
BrucellosisBacillary dysenteryAmoebiasis
047 Other protozoal dysentery048 Unspecified forms of dysentery049 Food-poisoning (subdivided into staphylo-
coccal, botulism and unspecified).
Some descriptively classified diseases can befound under:
543 Gastritis and duodenitis571 Gastro-enteritis and colitis, except ulcerative,
age 4 weeks and over
785.6 Diarrhoea, age 2 years and over.
Both for epidemiological reasons and for theapplication of preventive measures, it is essential tosubdivide bacterial food-borne diseases accordingto their etiology. When food-borne infections andfood-borne intoxications are classified separately,several etiological terms would have their placeunder each heading.The use of the general term " bacterial food-
poisoning" may be accepted if applied in a generalmanner, as in the United Kingdom, Switzerland, theFederal Republic of Germany and other countries.
Cases and outbreaks the etiology of which cannotbe identified are usually classified as " non-specific "
in the sense that their true nature remains obscure.Some workers have suggested a more detailed systemof classification.
However, where the etiology can be established,the proper etiological designation should be applied.The advantages of such a procedure are obvious.
In England and Wales, where this system of classifi-cation has been used for several years, it is easy toestimate not only prevalence but also the proportionof the various pathogenic agents, their relativefrequency and their epidemiological importance.This is illustrated in Table 1, taken from a technicalworking paper and from reports issued by theCentral Public Health Laboratory at Colindale,London.
In most other countries this subdivision has notyet come into general use though it is employed bycertain health departments and municipal and Statebacteriological laboratories.
In the following, the term bacterial food-poisoningwill, unless otherwise stated, be restricted to therecognized intoxications, i.e., to bacterial food-borne diseases which are not transmitted directlyfrom man to man or from man to animal, and whichare characterized by toxic symptoms. The remaining
AND
Presumedcausal agent 1953
Salmonellae 3 114
Staphylococci 132
Cl. welchii 25
Other 6
Chemical 0
Unknown
Total
2 000
5 227
WALES, 1953-56
Year
1954
3 508
127
48
9
2
2 322
6016
1955 1956 Total
5 269 4 323 16 214
138 131 528
90 77 240
13 16 44
4 3 9
3 447
8961
3 163 10 932
7 713 27 967
bacterial food-borne diseases will be discussed underthe term food-bornie infections even when they are
reported under bacterial food-poisoning in many
official statistics.
NOTIFICATION
Compulsory notification of bacterial food-poison-ing is not yet generally practised in Europeancountries. Official reporting was introduced many
years ago in Germany, and in England and Walesbefore the Second World War. In Switzerlandofficial reporting started in 1952, while in many
other countries no official system of notificationexists, e.g., in Norway. This, however, does notmean that the public health authorities in thosecountries are not interested in the problem. In fact,in some countries, Norway, for instance, the Statelaboratories collect sufficient information on bacterialfood-poisoning and from this are able to estimate itsprevalence very well (S. Hauge personal communi-cation, 1959). In other countries, the more severe
contagious and infectious diseases are still of suchimportance as to arouse the main interest of thepublic health services.
In recent years experience in some countries,particularly during and since the Second WorldWar, has shown that the older methods of notifyingand reporting bacterial food-poisoning are insuffi-cient and need improvement. For instance, inEngland and Wales, new regulations came into forcein 1949 (Cockburn, 1955), greatly improving the
TABLE 1FOOD-POISONING INCIDENTS IN ENGLAND
471

H. P. R. SEELIGER
previous notification system. As this procedurehas now proved its value over a period of ten yearsit may be summarized briefly.
Private physicians must notify all cases of sus-pected food-poisoning to Medical Officers ofHealth who, in turn, not only carry out the necessaryinvestigations in collaboration with authorizedlaboratories, but also submit these reports forcentral registration. This applies to all those diseaseswhich are apparently due to the ingestion of infectedor contaminated food.
Furthermore, the Medical Officer of Healthreports all sporadic and epidemic outbreaks offood-poisoning to the Ministry of Health, whilethe public health laboratories and the majority ofthe hospital laboratories forward their findings tothe Central Public Health Laboratory Service.Wherever possible, the physician should report
the kind of food believed to be responsible for theincident of suspected food-poisoning.
In some countries,.such as France, there is anobligatory system for group outbreaks or epidemicsonly, but not for sporadic cases.
It should, however, be borne in mind that com-pulsory notification does not mean that all casesor outbreaks are reported. Generally, only thesevere cases come to the attention of the publichealth service. The less severe are usually notreported. Therefore, the available data-even inthose countries where official reporting is practisedmust be evaluated with caution.Whether incidents of bacterial food-poisoning are
reported depends not only on the existence of anofficial reporting procedure but mainly on thewillingness of doctors to co-operate in notifyingthe public health authorities. It should be realizedthat official notification may have numerous conse-quences, both personal and economic, greatlyinfluencing the patient's future attitude towards hisphysician. Mild symptoms and rapid recoveryfurther explain (at least in many cases) why officialreports probably represent only a fraction of thetrue incidents. This subject will be further discussedbelow under the heading " Validity of Data " (seepage 475).
FACTORS INFLUENCING BACTERIAL FOOD-BORNEDISEASE
Human illness due to consumption of food con-taining pathogenic bacteria or toxins-partly theresult of bacterial contamination, partly the result
of the primary presence of pathogens in the foodand partly the effect of poisonous products-is notrestricted to those European countries where hygieneand sanitation are still undeveloped. It is quitecommon in those countries, too, which are knownto have a high standard of living, good sanitationand personal hygiene.Food-borne diseases have always been present
in under-developed countries but, owing to the highprevalence of other severe diseases, they were usuallyconsidered of minor importance. The more thefatal diseases are brought under control, the greateris the interest focussed on other forms of illness.This certainly also applies to the food-borne infec-tions -and intoxications.
Bacterial food-borne disease has likewise been atypical concomitant and sequel of wars, devastations,natural catastrophes and periods of famine andstarvation all over Europe, very few areas excepted.One only has to recall the innumerable cases ofdysentery, typhoid and paratyphoid fever whichoccurred in Europe during and following the Firstand Second World Wars, as well as the occurrenceof botulism and gangrene of the bowel, the last twobeing mostly due to the unsatisfactory preparationand canning of food which thereby becomes con-taminated. It has almost been forgotten that at thebeginning of the First World War cholera was stilla menace to the soldiers fighting in the east andsouth-east of the European continent.The enormous movements of people, sometimes
actual migrations involving millions of soldiers,prisoners, and refugees, widely dispersed the existingpre-war endemo-epidemic foci of enteric fevers anddysentery (e.g., Shiga dysentery). This resulted inthe spread of countless carriers of these dangeroushuman pathogens all over Europe. Poor hygiene,crowded quarters, low standards of living, the in-creased chance of contamination of perishable food,insufficient supervision and control by the publichealth services, lack of remedies and of hospitalfacilities affected the epidemiological picture andled to post-war epidemics of typhoid and paraty-phoid fevers and of bacterial dysentery in manyparts of Europe. The number of cases can only beestimated, as no valid statistics exist for a number ofyears. It has been calculated that several millions ofEuropeans were stricken by food-borne entericinfections during the period between 1940 and 1950.The tremendous importance of the endemo-
epidemic, highly contagious food-borne infectionsand of other types of bacterial food-poisoning
472

FOOD-BORNE INFECTIONS AND INTOXICATIONS IN EUROPE
stimulated extensive control measures by the publichealth and veterinary public health authorities.Their joint efforts have been rewarded by consider-able success with regard to the suppression andprevention of some of the most dangerous food-borne diseases and in a general improvement infood hygiene. This is well illustrated by the steadydecrease of the severe forms of shigellosis (Shigadysentery) as well as of typhoid and paratyphoidfever in most European countries since 1946-47.
However, the promising results obtained so farby the conquest or suppression of some food-borneenteric fevers and of tuberculosis due to bovinetubercle bacilli do not justify the conclusion that theproblem has been solved. Typhoid and paratyphoidfevers have by no means disappeared, and 2860 freshinfections due to Salmonella paratyphi B werereported from the Federal Republic of Germanyin 1956, many of them food-borne. The danger topublic health that still exists has been exemplifiedby two large-scale food-borne outbreaks of typhoidfever in the Federal Republic.Although the improvement in general living
conditions and in food hygiene in most Europeancountries has led to a diminution in the incidence ofdangerous food-borne diseases, it is interesting tonote that the incidence of gastro-enteritis and relateddiseases, including bacterial food-poisoning in ageneral sense, has not just remained stationaryduring the past decade, but has shown a definitetendency to increase. Such observations are notconfined to countries that suffered directly duringthe war. They extend beyond their frontiers tocountries where food and culinary hygiene arehighly developed and in which the incidence ofmalignant food-borne enteric fevers has dropped toa low figure. This has been illustrated by severallarge outbreaks of food-borne infections caused bysalmonellae in Sweden and Switzerland during recentyears.
INCREASED INCIDENCE OF FOOD-POISONING AND FOOD-
BORNE INFECTIONS AND FACTORS RESPONSIBLE
A steadily increasing number of published reportsfrom most European countries record numeroussporadic or epidemic occurrences of disease ob-viously connected with the ingestion of pathogenicorganisms or their toxic products.The high incidence of bacterial food-borne
diseases was first recognized by American workersin the USA. Besides the well-known Salmonella
infections, intoxications caused by staphylococcaland other bacterial poisons were found to be veryfrequent. For 1944 alone the number of cases ofstaphylococcal gastro-enteritis was estimated to runbetween half a million and one million (Feig, 1950).During the period immediately prior to the
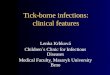
arrival of the Allied Forces in the Second WorldWar, and thereafter, mass infections and intoxica-tions occurred in Western Europe among soldiersand civilians to a hitherto unknown extent. Manyoutbreaks were caused by the ingestion of food-stuffs containing different species of Salmonellaknown to have their natural habitat in animals.Only a few of these species, such as Salm. typhi-murium, had played an important role during thepre-war years; others had been reported rarely ornot at all. It soon became apparent that various eggproducts, dried and otherwise preserved, harbouredlive Salmonella species, thereby creating a newhealth hazard of great importance (see the accom-panying figure).
Furthermore, increasing evidence was obtainedthat common human parasites, Staphylococcusaureus in particular, played as great a role in Europeas in the USA, as the causes of bacterial food-poisoning. In addition, new agents in bacterialfood intoxications were identified. Among theseClostridium welchii and Bacillus cereus deservespecial mention.
OUTBREAKS OF SALMONELLA FOOD-POISONINGIN ENGLAND AND WALES, 1923-44
Reproduc3d from Great Britain, Medical Research Council (1947)by p3rmis3ion of the Controller, Her Majesty's Stationery Office
473

H. P. R. SEELIGER
There is no doubt that an increase in the numberof food infections and of cases of so-called food-poisoning have occurred in many areas of Europe.The increase is real, and not merely an apparent risebrought about by better diagnostic facilities. Ofcourse, improved and refined diagnostic techniques(see, for instance, International Association of FoodSanitarians, 1957; Dack, 1956; Hobbs, 1953; Hobbset al., 1953; Mossel, 1958) have facilitated theinvestigation of etiological factors and led withgrowing frequency to their elucidation.
It is noteworthy that in some cases the highincidence of food-borne diseases in hygienicallyprogressive countries has recently been shown tobe directly related to the volume of certain food-stuffs and fodder imported from tropical or sub-tropical regions. The significance of such materialsdestined for human and animal consumptionwithout further treatment as a reservoir for patho-genic organisms has been appreciated for a longtime, but the potential dangers have not been fullyrecognized. Incidentally, the presence of Salmonellaspecies in Chinese dried egg yolk was establishedas early as 1931. The small volume of importationprior to 1942, however, created no serious concernor hazard. The real danger was detected only whenmass imports increased the chances of contaminationand infection. The correctness of these conclusionsis proved not only by the outbreaks mentionedabove during the war and post-war years, but alsoby identical observations in the Federal Republic ofGermany following the restoration of trade commu-nications in 1948.Even more important than the imports of con-
taminated egg products were the quantities of im-ported fish-, blood- and bone-meal from tropicalcountries. This type of animal food was found tocontain a tremendous number of Salmonella species.A glance at German import statistics shows, however,that the origin of these products was the decisivefactor, and not the quantity alone. For instance,between 75 000 and 132 000 tons of fodder ofanimal origin were imported into Germany annuallyduring the period from 1926 to 1936 with no seriousconsequences, except a few sporadic cases or smallepidemics which might have been caused by con-taminated foodstuffs. The reason for this low rateof infection apparently was that usually not morethan 3% of this type of animal food was importedfrom tropical countries. The remainder came fromScandinavia, Great Britain, Canada, etc. Between1949 and 1958 the import of fish-, blood- and bone-
meal in the German Federal Republic alone rosefrom 13 000 tons to more than 100 000 tons annually.During this period more than 30% originated fromtropical areas, Angola in particular. These 300%contained enough enteropathogens, Salmonella espe-cially, to create a public health hazard of the utmostimportance. There is sufficient evidence that theseobservations and conclusions are valid for manyEuropean countries, and not for Germany alone.
It must be realized that neither the food andfodder import dealers and industries nor thoseresponsible for the preparation of food within thefamily circle or on a wider scale have had anyawareness of this change in the epidemiologicalsituation.Great changes are taking place in the living and
eating habits of large parts of the European popula-tion. One such change has been the increased con-sumption of perishable foods, such as cream-containing cakes and ice-cream. Another is that,contrary to pre-war customs, almost a third of thepopulation of western and northern Europe noweat at least one meal per day, often more, awayfrom home in canteens, cafetarias and restaurants.Yet another example is the meals service for school-children which it is compulsory to provide in severalcountries. As early as 1942 the public health hazardinvolved in the war-conditioned trend to mass-feeding was under careful review (Trub & Wund-ram, 1942).Lack of knowledge of the potential dangers,
increased consumption of perishable food, inade-quate preparation and preservation processes,insufficient storage, large-scale catering, and con-tinued importation of infected or contaminatedbasic or raw materials must be regarded as amongthe most important factors responsible for the pre-sent high incidence of human illness due to infectedfoodstuffs.Food-borne infections due to salmonellae and
intoxications have occurred in the past, too. Butthey were usually restricted to single persons or tosmall groups such as families. Major outbreakswere confined to persons living in barracks, camps,prisons, hospitals or mental institutions, where theyobtained their food from a central kitchen. Withthe changes that have since occurred in living andeating conditions the risk of acquiring a bacterialfood-borne disease has increased considerably.Added to the factors favouring food-borne
diseases are the problems of latent infection ofcattle and poultry stock due to ingestion of infected
474

FOOD-BORNE INFECTIONS AND INTOXICATIONS IN EUROPE
fodder without clinical symptoms. The large-scaleinfestation of domestic animals with enteropathogensresults in the transmission of infectious agents tothe meat-processing plants and abattoirs, to but-cher's shops and kitchens. Moreover, rivers andlakes may become contaminated through infectiouswaste and excreta. Pastures may be infected byfloods, aquatic animals may ingest the pathogensand then aquatic animals may, in turn, be eatenby gulls etc. Thus the vicious circle of infection iscompleted.
Infected raw materials and food are responsiblealso for active infections and the development ofcarriers among food-handlers. Pathogenic organismsmay thus be transmitted to food-handlers and thenfrom the excreta of the food-handlers to foodproducts, utensils, towels and so forth. The sourcesand possibilities of food contamination with patho-gens are therefore numerous and the epidemio-logical consequences obvious.The increase of food-borne diseases in Europe is
also closely connected with international travel.Tens of thousands of travellers from tropical andsubtropical countries arrive in Europe every month,some harbouring and excreting human pathogenstransmissible by fiod. During the greater part of theyear millions of European tourists, particularlyfrom the north, west and central parts, move to thesouth and adjacent areas where-despite all effortshygienic conditions do not always correspond tomodern requirements.
Relatively high carrier rates, especially amongthe poor; bad latrine facilities; polluted watersupplies; the large numbers of flies, predominantvectors of enteric disease; unsafe methods of hand-ling, preparing and storing food in combinationwith the climatic conditions and high averagetemperatures which favour the survival of pathogensand their multiplication are regarded as the mainreasons for the intestinal disorders of varyingseverity and duration from which many visitors tosouthern Europe suffer. Not infrequently theyreturn sick or become sick shortly after their return,especially from enteric fevers with a prolongedincubation period.What is often attributed to intolerance of certain
foods, olive oil in particular, is in fact often the con-sequence of a bacterial food-borne infection orintoxication. Of course, various other factors,intolerance of food included, do have their part insuch disturbances.
Small eating places often advertise (not only in
the south) that their food is prepared with a maxi-mum of hygiene. Unfortunately, however, many ofthese advertisements are in marked contrast toreality. There may be plenty of goodwill, but thisis made ineffective by insufficient knowledge ofhygienic requirements. Moreover, culinary hygienein warm countries is not inexpensive, and thereforefrequently not compatible with cheap food.
In large restaurants and hotels, sometimes famousfor their good cuisine, the risk of acquiring food-borne diseases is also high. There may be adequatefacilities for the preparation of safe food, but theyare often not used. Moreover, the type of foodserved in these places-pies, hors-d'oeuvres, creams,etc. are more susceptible to infection by micro-organisms and their subsequent multiplication thanthe simple food prepared in the small places. Suchperishable foodstuffs are also used for the decorationof other food which involves increased handlingand risks. The experienced observer-usually follow-ing his own experience of the sequels of eating hors-d'aeuvres, sweets etc.-can study at such places howpractically every newly arrived guest is stricken bysome intestinal disorder within a few days.The native population of the southern European
countries is by no means spared from food-bornediseases. The official statistics usually give noindication of the incidence of enteric fevers anddysentery in these areas. The figures for bacterialdysentery, particularly, are often incredibly low.Apparently the indigenous population in many areasacquires immunity against dangerous enteric feversand locally prevalent types of bacterial dysenteryduring the first two decades of life, often in earlychildhood. But these people suffer from otherintestinal disturbances and food-poisoning, too. Infact, such attacks are regarded as normal during thewarm season.Although the occurrence of Salmonella in endemic
areas is often a local problem, the spread becomesepidemiologically important as soon as human andanimal food products from such places are exportedto other areas, where they may be encountered bya non-immune population.Any reduction of food-borne diseases in these
countries would benefit not only the tourists, butalso the inhabitants themselves.
VALIDITY OF DATA
Although a general increase of food-borne infec-tions and intoxications is evident from publications
475

H. P. R. SEELIGER
and reports, only data of limited accuracy regardingthe real prevalence are available.As stated above, this is largely due to the confusion
created by the poor diagnostic terminology in which,according to Feig (1950), unrelated syndromesappear as synonymous, and related syndromes areoften classified independently. Another importantreason is that modern knowledge of the variouskinds of bacterial food-poisoning is still restrictedto a small number of physicians, public healthofficers and veterinary public health officers andtheir auxiliary personnel.
Sporadic cases of food-poisoning and food-borneinfections frequently do not come to the attentionof the public health authorities. Even larger out-breaks with classical symptoms are often erroneouslydiagnosed as " non-specific ", or regarded as infec-tions of unknown nature caused by viruses, etc.One such outbreak involving a great number ofpersons at a large factory in a western German citywas thus reported in the newspapers as a possiblenew virus disease, before careful investigationsperformed by the local public health authoritiesestablished that the epidemic was due to a Salmonellareading food-borne infection.As a rule, only major outbreaks are thoroughly
investigated. Owing to the severity of the clinicalcourse and the improved diagnostic facilities, food-borne infections caused by Salmonella species aremore frequently recognized and reported in Europethan bacterial food-poisoning of staphylococcal orClostridium welchii origin. Therefore, figures andestimates of the latter two are far lower than in theUSA, for example. Whether the differences are realor only apparent remains to be ascertained.
There is sufficient evidence that the overwhelmingmajority of food-borne infections and intoxicationsare not reflected in official statistics. At the presenttime, even a rough estimation or approximation ofthe actual figures is hardly possible, except in a fewinstances. Figures concerning botulism may beconsidered reliable, as the disease is easily recog-nized owing to the severe clinical picture. Butunfortunately botulism usually is not reportedseparately from other forms of bacterial food-poisoning.
Lastly, it should not be forgotten that even incountries with good reporting and sufficient labo-ratory facilities-for instance, England and Wales-more than 40% of incidents of reported food-borne disease remain obscure etiologically (Cock-burn & Vernon, 1957), though this may be due in
part to lack of special investigation of incidents.Of the outbreaks which could be investigated bylaboratories at the right time, only 12% could notbe identified. In the Land of North-Rhine-West-phalia out of 26 epidemic incidents which werereported, 19 were cleared up during 1946 and 1950(Trub & Reploh, 1954). There is no doubt thatthese 26 reported incidents represented but a minutefraction of the real figures.
All these points must be kept in mind when theprevalence of bacterial food-borne disease is dis-cussed.
FOOD-BORNE INFECTIONS IN EUROPE
Enterobacteriaceae
Typhoid and paratyphoid fever. Official figuresdemonstrate that both diseases have graduallyreached pre-war levels. Occasional epidemics,mostly food-borne, have disturbed this tendency.The prevalence of these epidemiologically relatedtrue anthroponoses is different for different coun-tries, and may even differ within the same country.In West Germany and West Berlin, for example,there is a higher rate of paratyphoid B infection thanin Central Germany and East Berlin, where-incontrast to the rest of the country-typhoid fever isstill predominant. Available statistics give noevidence of the percentage of these diseases due tofood-borne infections.One remarkable example of paratyphoid B fever
needs some comment: proved infections due to aphage type of Salmonella paratyphi B hitherto notknown to occur in Europe, could be traced to theimportation of Chinese frozen whole egg, fromwhich that particular phage type was isolated repeat-edly in England and Germany. As frozen wholeeggs are used extensively in baking (those respon-sible being unaware of the possible dangers involved)it is obvious that enteric fevers might easily be spread,before efficient control measures could be applied.
Other Salmonella infections. During the past tenyears members of the Salmonella group have beenresponsible for the majority of sporadic and epidemicincidents of food-borne infections in the northern,central and western areas of Europe.
In contrast to the causative organisms of typhoidand paratyphoid fevers, which are often directlytransmitted by man, the main reservoir of otherSalmonella species is in animals, with only occasionalhuman carriers. Poultry, poultry products and
476

FOOD-BORNE INFECTIONS AND INTOXICATIONS IN EUROPE
cattle are the most significant for human infections.Apart from endemic infection in herds usually dueto Salm. typhimurium, Salm. dublin and Salm.enteritidis in cattle, Salm. gallinarum-pullorum inpoultry, and a variety of other types in ducks-theimportation of infected animals or their productsfrom eastern and south-eastern Europe into thecentral and western part was formerly one of thesources of human salmonellosis. In recent yearssuch imports have again caused several outbreaks ofSalmonella infections due to Salm. newport, Salm.cholerae-suis, and other species which are frequentin swine.
It is certain that the importation of infected foddermaterials such as fish-, bone-, blood- or whale-mealhas become largely responsible for the latent Sal-monella infections of European livestock. In Den-mark, where the danger apparently was appreciatedfirst (Muller, 1952), it proved largely possible totake appropriate and successful preventive measures.In the Netherlands and the United Kingdom valuablecontributions were made with regard to the controland prevention of fodder- and food-borne salmonel-loses (Hobbs, 1957; Mossel, 1958). In the FederalRepublic of Germany, during 1957 and 1958,legislative measures had to be taken in order todiminish at least the continuous importation ofcertain fodder and food products.Even if urgent measures, such as the pasteuriza-
tion of all products containing salmonellae, wereadopted generally, it would still take some time toalter the situation in view of the enormous quantitiesof material in stock, and the difficulties of findingand eradicating carriers amongst cattle, swine andpoultry. Apart from the fact that animal carriersmostly appear to be quite healthy and that theirmeat passes the usual inspections without beingsuspected or condemned, the clinically inapparentinfections are difficult to trace. Consumption ofbacon, ham and sausage meats contaminateddirectly or indirectly with Salmonella species ofobviously non-European origin has resulted in large-scale outbreaks with thousands of infections. Oneepidemic with more than 6000 cases due to a Salm.bareilly infection was caused by camembert cheese(Bonitz, 1953). This cheese was apparently contami-nated by a healthy human carrier of Salm. bareillywho lived on a farm where swine were fed withbatches of fish-meal known to contain Salm.bareilly. The chain of infection is often so complexthat reconstruction of the path of transmission isimpossible.
Another important epidemiological factor is theinfection of egg products by Salmonella. The roleplayed by ducks' eggs in food-borne infections iswell known. Hens' eggs may also be incriminatedin a number of incidents. The significance of driedegg powder was first appreciated during the SecondWorld War (Great Britain, Medical Research Coun-cil, 1947). This was confirmed after 1950 by English,Dutch and German investigators. In the FederalRepublic of Germany and in Great Britain severaloutbreaks were traced to this source of infection.It has already been mentioned that Chinese eggpowder was found to contain Salmonella as earlyas in 1931 (Knorr, 1931). Frozen whole egg andcrystalline egg albumen may be even more importantepidemiologically.The pasteurization of egg products, during or
immediately after production, or perhaps on arrivalin the importing country, would be most desirable.But it appears to be impracticable owing to thesubstantial deterioration in quality that it causes,especially to frozen whole egg and dried egg yolk.Crystalline egg albumen is one of the few egg pro-ducts which can be pasteurized without any majorloss of quality. The subject has been carefullyreviewed in an extensive monograph by Brooks &Taylor (1955).
Routine examination of imported egg products,unfortunately, does not ensure the safety of theconsumer, as was noticed during some outbreaks in1957 in the Federal Republic of Germany, for nolaboratory service can hope to examine a high enoughproportion of the total imports to be able to saywith assurance that only negative shipments passfor human consumption.
Fortunately, not all salmonellae pathogenic toanimals or transmitted by animal products are ofthe same order of pathogenicity to man. Severalspecies, such as Salm. abortus-ovis, Salm. typhi-suisand Salm. gallinarum-pullorum, very rarely, if at all,cause human illness. However, infections due toSalm. gallinarum-pullorum have been reported in afew instances.Not all Salmonella species found so far in imported
fodder have been re-isolated from human or latentanimal infections. In the Federal Republic ofGermany from 1955 until 1957 only about 75 %of such species had been found in human excreta.The same holds true for isolation from Europeananimals. This may indicate that some strains oftropical Salmonella will not easily adapt themselvesto hosts in non-tropical areas. It has been suspected
477

H. P. R. SEELIGER
that the animal may serve as some kind of a screenfor these enteropathogens. Other species, however,have obviously settled down successfully and havebecome endemic for more than three years. Salni.blockley is a typical example. Whether such eventsare merely accidental or the expression of a variablehost specificity remains to be seen (Seeliger, 1957,1958).A few figures may be cited to illustrate the in-
cidence of food-borne Salmonella infections. InEngland and France during 1956 out of 7710 reportedoutbreaks of bacterial food-borne disease salmonellaewere found to be the cause in 4323 instances. Inthese countries the total figure of Salmonella isola-tions from human beings rose from 1997 in 1949-50to 2347 in 1951-52, 4432 in 1953-54 and 6505 in1955-56.No less impressive are the figures reported from
the Federal German Republic, including WestBerlin, where fairly complete data are available forthe years 1956 and 1957. This may be seen fromTable 2, based on data in Seeliger (1958b, 1959).The corresponding figures for reported cases of
bacterial food-poisoning (which include most Sal-nuonella infections) are, according to the GermanFederal Office of Statistics: for 1955, 7.6 per100000; for 1956, 8.9 per 100000; and for 1957,5.3 per 100000.During the same period, the following reports
were received on paratyphoid fever (which alsoincludes some severe infections due to other Sal-mnonella species): for 1955, 7.1 per 100 000; for 1956,5.7 per 100 000; for 1957, 4.9 per 100 000 (which isonly 0.1 per 100 000 higher than the pre-war figurefor Germany with the 1938 boundaries). From thisone may conclude with due caution that, after thecontinued increase since 1950, a slight decline inSalmonella infections was observed for the firsttime in the Federal Republic as a whole during 1957.This, however, does not apply to all localities. Atseveral places the figures were definitely higher thanduring the preceding years.
Altogether, more than 150 different species ofSalmonella have been identified in Federal Germanyand West Berlin since 1950-the first year of in-creased prevalence-from human, animal, food,fodder, sewage, river water and other sources. Thisrepresents more than 25°/ of all Salmonella speciesrecognized by the Kauffmann-White Schema. Therewas a conspicuous concordance of the species ofhuman, animal, food, fodder and other origin, withthe limitations stated above.
TABLE 2PRIMARY ISOLATIONS OF SALMONELLA SPECIES FROM
HUMAN SOURCES IN THE FEDERAL REPUBLICOF GERMANY, INCLUDING WEST BERLIN, IN 1956 AND 1957
1956 1957
Total 9 926 8186
Numberofspeciesisolated(except Salm. typhi) 86 88
Salm. paratyphi B, total
Salm. typhimurium, total
Other species, total
3 099
2610
4217
2 649
1 919
3 618
Among the great diversity of Salmonella speciesisolated in the central, western and northern partsof Europe, Salm. typhimurium is predominant. Itcauses more than 30% of all incidents. In Swedenand England bacterial phage-typing has been em-ployed with very gratifying results to elucidateextremely complex problems of epidemiology andepizootiology (Lilleengen, 1948; Anderson & Stone,1955).Comparable data from the German Democratic
Republic are available through the public healthauthorities and from various reports (e.g., Meyer-Oschatz, 1957) up to 1957. They likewise show atrend of increasing prevalence of human salmonel-loses as regards both actual incidents and the sero-logical species isolated.The sharp rise in the incidence of salmonellosis
can easily be gauged by comparing the above datawith a summary report covering findings in pre-warGermany from 1933 to 1939: then only 18 differentspecies, most of them single isolations, were identi-fied.
Unfortunately, detailed data are not availablefrom various European countries, particularly inthe south. According to some unpublished reports,the total figures and numbers of Salmonella speciesisolated seem to be rather low compared with thefindings cited before. Certainly more accurate infor-mation is needed before any conclusions can bedrawn.From the foregoing it is obvious that successful
control and prevention require close co-operation,nationally and internationally, on the part of bothpublic health and veterinary public health services.They need the support and the understanding ofimport merchants and experts in the national
478

FOOD-BORNE INFECTIONS AND INTOXICATIONS IN EUROPE
economy as the complex epidemiology and epizoo-tiology of the food-borne Salmonella infections hasfar-reaching consequences for international trade,national economy and agriculture.
Shigellosis. Shigellosis is still prevalent throughoutEurope. For the most part, Shigella infections arecaused by members of the Sh. flexneri subgroup andby Sh. sonnei. Many infections are food-borne inthe sense that the organisms are transmitted byfoodstuffs infected directly or indirectly. While Sal-monella and Shigella strains seem to be spread byfood in a haphazard manner, Sh. sonnei apparentlyis not. Out of the large number of infections due tothis organism, practically none of them was foundto be food-borne in England and Wales. Again itmust be stressed that neither the official statisticsnor the bacteriological reports allow any conclusionas to the number of incidents caused or the partplayed by food-borne infections. As the causativeorganisms are strictly parasites of man and theprimates, control and prevention are chiefly restrictedto the normal public health authorities. It may beassumed that shigellosis occurs more frequently inthe southern, south-eastern and eastern areas ofEurope. This however, is not always supported byofficial statistics (Rodenwaldt & Jusatz, 1950-57).
Other enterobacterioses. The role played by otherenterobacteriaceae and related organisms such asAlkaligenes, Aeromonas, Pseudomonas, etc., in food-borne infections is uncertain. As they constitutepart of the normal faecal bacteria it is extremelydifficult to evaluate their part in intestinal infections.Moreover, many of these organisms live as sapro-phytes outside the body and are found as commensalsand contaminants of various kinds of food. Underfavourable conditions they easily multiply and causespoilage. The presence of Escherichia coli in waterand foodstuffs has long been regarded as definiteproof of recent faecal contamination. Only duringthe past ten years has it been discovered that severalserotypes are pathogenic to man. Clinical infectionsof the small intestine are quite frequent among thenewborn, particularly in children's hospitals andsimilar institutions where they have become moreimportant than the Shigella infections so frequentlyobserved in the past. Clinical infections among theolder age-groups seem to be rarer, although this hasnot yet been fully investigated. The proportion offood-borne E. coli infections is probably variable,as in the case of shigellosis and other enterobacte-rioses. Some reports indicate that enteropathogenic
E. coli types may be transmitted from animal hoststo the human being. Neither the importance of thisnor the route of infection is known.
It is possible that certain serotypes of othergroups such as Hafnia, Providencia, Klebsiella andProteus may also be enteropathogenic for man,while others are not. The situation may be similarto that arising with the pathogenicity of the variousSalmonella and Arizona species (Taylor, 1958).Among these organisms of doubtful pathogenicity,
Proteus has been incriminated as a cause of food-borne infections (Dack, 1956; Moser, 1953).The obscurity of the causal relationship of many
enterobacteriaceae and related species with food-borne infections renders well-planned and carefulinvestigations imperative in order to approach theproblem successfully.Another point should also be stressed. Even if a
few salmonellae or other enterobacteriaceae maybe harmless from the clinical point of view, theynevertheless indicate faecal contamination of humanfood. Apart from the epidemiological and clinicalimplications, any type of food can be rejected foraesthetic reasons where gross faecal contaminationis found.
Food-borne infections due to other bacteria
It is generally acknowledged that bovine tuber-culosis is responsible for human infections. Theseare chiefly conveyed by infected milk and milkproducts. The proportion of bovine infectionsamong the human tuberculosis cases is still understudy. It obviously is more prevalent among youngchildren in rural areas than in urban areas whereonly pasteurized milk is available. Bovine infectionsin man have become very rare in those countrieswhere eradication of bovine tuberculosis in cattleis near to completion or in rapid progress (WHO/FAO Seminar on Zoonoses, 1953). In the FederalRepublic of Germany it has been reported that almost75 % of the cattle are now free from tuberculosis.
Certain forms of human pasteurellosis, especiallydue to Pasteurella pseudotuberculosis, may likewisebe food-borne. This is borne out by the fact thatthe primary localization is usually found in thedigestive tract, particularly in the mesenteric glands.So far its epidemiology and prevalence are stillobscure.Another important zoonosis causing food-borne
infections is brucellosis. In the Mediterranean areait is estimated that approximately 50% of thehuman cases of brucellosis are caused solely or
479

H. P. R. SEELIGER
partially by the consumption of infected food,chiefly milk and milk products (WHO/FAO Seminaron Zoonoses, 1953). Whether these estimates applyto other parts of Europe remains to be investigated.Apart from Bang's disease, which has been endemicand enzootic in all European cattle-raising countries,Malta fever has found its way from the south andsouth-western parts of the continent to centralEurope, where an increasing number of animal andhuman infections have been reported since 1948.As infections due to Brucella abortus are still pre-valent in many herds all over Europe, the potentialdanger on the one hand to the consumer of non-pasteurized milk, cheese and other products andon the other of animal losses to the farmer makesthe eradication of brucellosis in cattle an urgentproblem.
Tularaemia has become enzootic over extensiveareas of Europe (Rodenwaldt & Jusatz, 1950-57).This has resulted in several sporadic and epidemichurman infections. So far, no food-borne case dueto ingestion of infected meat has come to the author'sattention. It has been proved, however, that thecausative organisms can be transmitted to man byinfected hare's meat. In the incidents in questioninfection was apparently induced through smallwounds during handling of the infected food.Among the " newer " diseases that may be trans-
mitted by originally infected food, chiefly by non-pasteurized milk, is listeriosis. Relatively little isknown of the epidemiology, epizootiology andnatural reservoir of its causative organism, Listeriamonocytogenes. In several instances human infec-tions have been traced to the consumption of rawmilk from infected cattle and goats. Eggs and meatmay also have some importance in the transmissionof the disease. With more than 500 human casesobserved during the past decade in Europe, listeriosisrequires special attention (Seeliger, 1958a).Although infections due to Erysepilothrix rhusio-
pathiae transmitted by animal products occuroccasionally in human beings, the danger seems tobe small.
In conclusion it should once more be emphasizedthat close collaboration of the public health andveterinary public health authorities is indispensablefor the control and prevention of the food-bornezoonoses. It has become clear that these diseasesrepresent not only a professional hazard for thosewho handle and take care of animals or their pro-ducts, but in some instances an even greater dangerfor the majority of people who come into indirect
contact with animals via infected or contaminatedfood. There is plenty of work to be done to diminishexisting dangers to public health caused by food-borne infections of human and animal origin.
FOOD-BORNE INTOXICATIONS(BACTERIAL FOOD-POISONING) IN EUROPE
BotulismThis malignant form of bacterial food-poisoning
has been discussed extensively by competent authors(Meyers, 1928; Dack, 1956). Its distribution isworld-wide, but fatality rates differ. In Europe, forinstance, fatality has been reported to be muchlower than in the USA, apparently owing to theprevalence of less toxogenic Clostridium botulinumtypes in the soil. In Europe type B is prevalent.Several outbreaks were reported during the post-war period up to 1948. They were exclusively dueto poor methods of home-canning and preservationof susceptible food. Typical instances have been thesmall outbreaks in the Federal Republic of Germanydue to sour-fried-herring, a northern dish; to home-made liver-sausage; and to several kinds of home-preserved " sterilized " vegetables.
In Norway some recent outbreaks of type Bbotulism were caused by cured meat and ham(Skulberg, 1957, 1958), while in Denmark outbreaksof type E botulism could be traced to marinatedherring (Pedersen, 1953).Owing to lack of proteolytic properties, intoxi-
cated food may not show any obvious sign ofspoilage.
In official medical statistics and in the lists ofcauses of death, botulism is not separated fromother food-borne infections in most Europeancountries. It is not possible, therefore, to give anyreliable information on its prevalence. From thereports and literature available, it seems thatbotulism is almost non-existent in the western andcentral parts of Europe at the present time.
Staphylococcal .food-intoxicationFollowing the detection of staphylococcal entero-
toxin as a cause of human food-poisoning (Dack,1947, 1956; Jordan & Burrows, 1934a), numerousreports have presented evidence that staphylococcalfood-intoxication is one of the relatively prevalentforms of bacterial food-borne disease.The extent of food-poisoning due to the pyogenic
staphylococci is still underestimated. It was notappreciated in Europe until the end of the Second
480

FOOD-BORNE INFECTIONS AND INTOXICATIONS IN EUROPE 481
World War that this food-intoxication played suchan important role. In the USA, between 1945 and1947, 926 outbreaks were reported, involvingapproximately 50000 individuals. Of these out-breaks 80% were caused by enterotoxins of haemo-lytic staphylococci. This amounts to four times thenumber of food-borne infections due to salmonellaeduring the same period. As already pointed out, ithas been estimated that in 1944 from half a millionto a million persons were affected by staphylococcalfood-poisoning in the USA. This should in no waybe interpreted as due to any particular sensitivityin the American population to staphylococcalenterotoxin, as was at first thought by some. Theingestion of foodstuffs containing staphylococcalpoison by American soldiers and European em-ployees during 194748 produced severe outbreakswith identical results in both groups.Whether the figures reported in the USA apply
to European conditions is uncertain. In Englandand France, for example, the percentage of staphylo-coccal food-poisoning was far lower, amountingto about a hundredth of the cases of food-borneinfections due to salmonellae in 1956 (Cockburn; 1Cockburn & Vernon, 1957). Meat and meat pro-ducts, milk, cheese and certain types of sweets andpastry were found to be mostly involved in theseincidents (Cockburn; 1 Cockburn & Vernon, 1957;Hobbs, 1953; Ritchie et al., 1947).For several years now an increasing number of
reports has been received of similar events in theFederal German Republic, in southern countrieslike Italy (Sicily) and Portugal (Da Fonte, 1950;Moser & Mumme, 1954; Spano, 1956), and inCzechoslovakia (Sedlak, 1950). It is quite probablethat many other outbreaks have occurred but havenot been reported or even recognized as due tostaphylococci.The causal organisms, certain types of Staphylo-
coccus aureus, are transmitted directly from infectedindividuals to food or by means of contaminatedfood utensils. They produce, under favourableconditions, a specific toxin, particularly in substratesrich in albumen, with or without the presence ofsugar (cream, bread pudding, ice-cream, glaze, ham,meat dishes, sandwiches, sausage, cheese and milk).Keeping these products for a few hours at room orbody temperature encourages the rapid multiplica-
1 Cockburn, C. W., Epidemiology offood-borne diseaseswith special reference to England and Wales (unpublishedworking document of the WHO Regional Office for Europe,EURO/88.2/6)
tion of the organisms and the development of theenterotoxin. Batches of dried milk with high staphy-lococcal content were responsible for repeatedsevere outbreaks among schoolchildren in England.At first the outbreaks were unexplained, but theystopped when dried milk free of staphylococci wasemployed in the preparation of school meals(Anderson & Stone, 1955).
Bacteriophage-typing is essential in the investiga-tion of staphylococcal food-poisoning because some50% of the human population carry Staph. aureus.
It should be noted that the presence of Staph.aureus in raw milk destined for human consumption(Grade A milk) has been observed quite frequentlyby the author. But the hazard to public health isusually not considered very high.
Prevention of staphylococcal food-poisoning islargely a technical kitchen problem and will not bediscussed in detail in this connexion. There is generalagreement that rapid refrigeration of those food-stuffs that can be frozen is the best means of pre-venting possible outbreaks of this type of food-poisoning. The measures to be taken, however,will be understood by the people involved only whenthe medical profession collects enough material toconvince the public of the health hazard involved.At the present time, many doctors are not evenaware of the fact that " staphylococcal food-poison-ing" exists as a disease.
Streptococcalfood-poisoning
Apart from the occasional food-borne transmis-sion of pyogenic streptococci resulting in humaninfections, such as scarlet fever, sore throat and soforth, streptococci have been incriminated as acause of true food-poisoning (Jordan & Burrows,1934b). As only very few reports are available onthis subject, it is not yet possible to evaluate itsincidence or importance.
Food-poisoning due to spore-forming bacilli (exceptClostridium botulinum)
Food-borne intoxications due to a particularheat-resistant anaerobic bacillus, belonging to thegas-gangrene-producing Clostridium welchii, arebeing reported with increasing frequency. One ofthe first reported incidents was recognized in Ger-many before the Second World War (Zeuner, 1938)and possibly even earlier. Later on, several out-breaks were observed in England, France, Norway,Germany and elsewhere.

482 H. P. R. SEELIGER
Poisoning is mostly caused by meat and saucesprepared in canteens and kept in large containersat temperatures which allow the multiplication ofthe organisms, and then eaten the next day withoutfurther thorough heating. Milk likewise has beenincriminated in several instances (Buttiaux &Beerens, 1953). In fact, enumeration of heat-resistant C. welchii has been suggested as a valuablecriterion for the initial contamination of milksamples (Buttiaux & Beerens, 1953). The entero-toxic effect seems to be associated with the bacterialcells and is not present in filtrates without organisms.Pressure-cooking with rapid cooling and so forthare simple and effective measures. The rapidcooling of large containers, however, may presenttechnical problems. This entity seems to be etio-logically related to a disease called intestinal gan-grene (Darmbrand), which was observed in northernGermany after the last war.The actual incidence of C. welchii food-poisoning
is not known. According to reports available fromEngland and France, proved incidents have repre-sented quite a variable proportion of all food-poisoning incidents. Sometimes they have amountedto only a tenth of the reported cases of staphylo--coccal food poisoning and sometimes the propor-tion has been higher (Cockburn; 1 Cockburn &Vernon, 1957, 1958; Dack, 1956). In Norway, C.welchii food-poisoning is definitely more prevalentthan staphylococcal food-intoxication. In Germanythis type of disease has been diagnosed at a fewplaces where its symptomatology and bacteriologywere known. In the light of findings in Hamburg
and Bonn, one would be inclined to believe thatthis type of food-poisoning is much more frequentthan would appear from official reports and therelevant literature (Linzenmeier, 1956; Moser, 1953;Seeliger, 1956).Another type of food-poisoning is ascribed to
Bacillus cereus, an aerobic spore-forming soilorganism. Several large outbreaks were studied inNorway and Denmark with some 800 cases reported(Christiansen et al., 1951; Hauge, 1955). Otherincidents were observed in Sweden (Hauge, 1955)and the Netherlands (Clarenburg & Kampel-macher, 1957). Starch-containing foodstuffs suchas vanilla sauce, yellow pudding and sour potatomash have been incriminated. This type of food iscompatible with the frequent occurrence of B. cereusin starch, flour and potatoes. Experience showsthat intoxication will not ozcur unless the numberof organisms is at least in the order 107 per gram.More studies are necessary in order to estimate theprevalence and importance of B. cereus food-poisoning.From the foregoing it must be concluded that the
increasing incidence of bacterial food-borne infec-tions and intoxications demands closer supervisionof food products and better food hygiene, thecareful instruction of producers and consumersin the dangers involved, improved culinary hygieneand, most urgent of all, legal measures to forestallthe continuous spreading of pathogenic organismsin food products. All this requires better co-operation and collaboration between the publichealth and veterinary public health authorities.
RI-SUMt
Des rapports de plus en plus nombreux signalent enEurope des infections, epidemiques ou sporadiques, enrelation avec la consommation d'aliments contenant desgermes pathogenes ou leurs toxines. L'accroissement dela frequence de ces infections est reel. I1 n'est pas dfiseulement a de meilleurs diagnostics ou a des declarationsplus fideles. Diverses circonstances l'expliquent: laguerre et ses sequelles, la consommation grandissantede produits pour I'alimentation humaine ou animale,importes de regions oui les prescriptions d'hygiene sontpeu rigoureuses ou inappliquees, le nombre croissant de
1 Cockburn, W. C., Epidemiology of food-borne diseaseswith special reference to England and Wales (unpublishedworking document of the WHO Regional Office for Europe,EURO/88.2/6)
produits tropicaux consommes en Europe, l'habitudequi se generalise dans tous les secteurs de la population,en particulier chez les travailleurs manuels et les ecoliers,de prendre au moins un repas hors du foyer, au res-taurant, en cantine, etc., le developpement du tourismequi fait affluer les habitants de pays oui l'hygiene est laplus developpee vers les pays du sud, oui elle l'est moins.Du reste, les pays oui l'hygiene alimentaire et culinaireest d'un niveau eleve ne sont pas a l'abri de ces infections,les diverses epidemies qui s'y sont declarees ces dernieresannees en temoignent.
L'auteur analyse la situation telle qu'elle se presenteen Europe. I1 passe en revue les divers facteurs quiempechent que l'on s'en fasse une ide exacte: differencesdans le systeme de notification d'un pays A I'autre, impre-

FOOD-BORNE INFECTIONS AND INTOXICATIONS IN EUROPE 483
cision de la terminologie et varietes des methodes declassification. On peut cependant faire quelques consta-tations generales:
D'apres les statistiques dont on peut faire etat, lagrande majorite des infections d'origine alimentaire sontattribuables aux Salmonella.
Outre les especes endemiques connues, on en a isoledes centaines d'autres dont beaucoup etaient pour ainsidire inconnues en Europe jusqu'a maintenant. L'atten-tion a donc e appel6e sur de nouvelles sources d'in-fection, decelees principalement dans les produits impor-tes en provenance de differents pays tropicaux ou sub-tropicaux. Les examens bacteriologiques ont revele parexemple que certains produits A base d'ceufs deshydratesou surgeles, et les tourteaux de farine de poisson, d'os,et de sang, renfermaient parfois un nombre impression-nant d'especes de Salmonella, souvent identiques A cellesqui avaient 6te isolees dans des prelevements patholo-giques pris sur l'homme. En outre, les memes types ontete isoles chez les animaux domestiques, en particulierchez les animaux de boucherie.
Outre les salmonelloses, les shigelloses dues en parti-culier a Shigella sonnei sevissent toujours en Europe.Toutes cependant ne semblent pas avoir une originealimentaire.
Contrairement aux infections, les intoxications d'ori-gine alimentaire sont produites surtout par l'ingestionde toxines elaborees par la croissance de Staphylococcusaureus dans les aliments. La prophylaxie des intoxicationsalimentaires dues aux staphylocoques est surtout unequestion de technique culinaire. On s'accorde en generalA reconnaitre que la refrigeration rapide de ceux descomestibles qui peuvent etre congeles est le meilleurmoyen preventif. Le phago-typage est une mesure indis-
pensable dans l'analyse des intoxications alimentairesdues aux staphylocoques; en effet, cette technique estsouvent la seule qui permette de remonter a la source del'infection.Un autre type d'intoxication alimentaire est provoque
par les bacilles sporogenes. Le botulisme est pour ainsidire inexistant en Europe, oii l'on ne rencontre plus quedes cas sporadiques. Les maladies dues a l'ingestion debacilles anaerobies particulierement resistants a la cha-leur et appartenant au groupe de Clostridium welchiisemblent presenter une plus grande importance, commeon l'a observe en Angleterre, en France, en Norvege eten Allemagne. Les intoxications de ce type sont liees leplus souvent a la consommation de viandes et de saucespreparees dans des cantines et conservees dans de grandsrecipients a des temperatures qui favorisent la multipli-cation du germe. Il semble que le nombre des accidentsqui lui sont imputables soit bien inferieur a celui desintoxications staphylococciques.Parmi les bacilles aerobies sporogenes, Bacillus cereus
a et incrimine en Norvege, au Danemark, en Suede,aux Pays-Bas et recemment en Hongrie. Il ressort desdonnees disponibles que l'intoxication se produit seule-ment si le nombre des micro-organismes ing6res est enmoyenne de l'ordre de 107 par g. Le r6le etiologique dece bacille est encore discute.La recrudescence des toxi-infections d'origine alimen-
taire impose un contr6le plus etroit et une ameliorationde l'hygiene des denrees alimentaires. Tourefois, l'effi-cacite des mesures prises, quelle qu'en soit la nature,dependra de la collaboration etroite des autorites desante publique et de sante publique veterinaire, quidevront etre armees de tous les moyens reglementairesn6cessaires.
REFERENCES
Anderson, P. H. & Stone, D. M. (1955) J. Hyg. (Lond.),53, 387
Bonitz, K. (1953) Dtsch. med. Wschr., 78, 1412Brooks, J. & Taylor, D. J. (1955) Eggs and egg products,London, HMSO
Buttiaux, R. & Beerens, T. H. (1953) Rev. Path. comp.,No. 652, 1448
Christiansen, O., Koch, S. 0. & Madelung, P. (1951)Nord. Med., 3, 194
Clarenburg, A. & Kampelmacher, E. H. (1957) Voeding,18, 381
Cockburn, C. W. & Vernon, E. (1957) Monthly Bull.Minist. Hlth Lab. Serv., 16, 233
Cockburn, C. W. & Vernon, E. (1958) Monthly Bull.Minist. Hlth Lab. Serv., 17, 252
Dack, G. M. (1947) Amer. J. publ. Hlth, 37, 360Dack, G. M. (1956) Food poisoning, 3rd ed., Chicago,
University of Chicago Press
Da Fonte, A. J. (1950) Bol. Serv. Saiude pibl. (Lisboa),2, 87
Feig, M. (1950) Amer. J. publ. Hlth, 40, 1372Great Britain, Medical Research Council (1947) The
bacteriology of spray-dried egg with particular refe-rence to food poisoning, London, HMSO (Spec. Rep.Ser. med. Res. Coun. (Lond.), No. 260)
Hauge, S. (1955) J. appl. Bact., 18, 591Hobbs, B. C. (1953) Food poisoning and food hygiene,London, Arnold
Hobbs, B. C. (1957) Sanitarian, 66, 95Hobbs, B. C., Smith, M. E., Oakley, C. L., Warrack,G. H. & Cruikshank, J. (1953) J. Hyg. (Lond.), 51,75
Jordan, E. 0. & Burrows, W. (1934a) Amer. J. Hyg.,20, 604
Jordan, E. 0. & Burrows, W. (1934b) J. infect. Dis.,55, 363
4

484 H. P. R. SEELIGER
Knorr, M. (1931) Arch. Hyg. (Ber.), 105, 237Lilleengen, K. (1948) Acta path. microbiol. scand.,
Suppl. 77Linzenmeier, G. (1956) 65ff. Gesundh.-Dienst., 17, 708Meyer, K. F. (1938) Botulismus. In: Kolle, W., Kraus, R.& Uhlenhuth, P. Handbuch der pathogenen Mikro-organismen, 3rd ed., Jena, vol. 4, p. 1269
Meyer-Oschatz, W. (1957) J. Hyg. Epid. Microbiol., 1,190
Moser, L. (1953) Dtsch. med. Wschr., 78, 1762Moser, L. & Mumme, C. (1954) Munch. med. Wschr.,
96, 226Mossel, A. A. (1958) Zbl. Bakt., L Abt. Orig., 172, 69Miller, J. (1952) Nord. Vet.-Med., 4, 290Pedersen, H. 0. (1953) Nord. Vet.-Med., 5, 700Ritchie, J. M., Murray, D. & Holgate, M. (1947) Lancet,
2, 256Rodenwaldt, E. & Jusatz, H. J. (1950-57) World atlasof epidemiology, Hamburg, Falk Verlag
Sedlag, J. (1950) eas. L.k. ces., 89, 795
Seeliger, H. P. R. (1956) Dtsch. med. Wschr., 81, 1419(In English in Germ. med. Monthly, 1957, 2, 86)
Seeliger, H. P. R. (1958a) Listeriose, 2nd ed., Leipzig, BarthSeeliger, H. P. R. (1958b) Zbl. Bakt. L, Abt. Ref., 169,303Seeliger, H. P. R. (1959) Zbl. Bakt. I., Abt. Orig., 174,
327Skulberg, A. (1957) Nord. hyg. T., 27, 263Skulberg, A. (1958) Nord. hyg. T., 28, 133Spano, C. (1956) Igiene San. pubbl., 11, 485Taylor, J. (1958) Sem. Hop. Paris, 6, 893Trub, C. L. P. & Reploh, H. (1954) Arch. Hyg. (Berl.),
138, 98Triub, C. L. P. & Wundram, G. (1942) Ver6ff. Volks-
gesundh.-Dienst., 56, 480WHO/FAO Seminar on Zoonoses (1953) Advances in
the control of zoonoses, Geneva (World Health Organ-ization: Monograph Series, No. 19)
World Health Organization (1957) Manual of the Inter-national Statistical Classification of Diseases, Injuries,and Causes of Death,... 1955 revision, Geneva