Embed Size (px)
Citation preview

1
9th EVIDENCE–BASED CLINICAL PRACTICE WORKSHOP
For Clinical Decision Making and Health Management
IDENTIFY – APPRAISE – INTERPRET– ELABORATE – IMPLEMENT
AMIL LIFESCIENCE
Suzana Alves da Silva Peter Wyer
Rio de Janeiro, 2015

83
Section IV DEVELOPING$POLICIES$AND$RECOMMENDATIONS$USING$GRADE$

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
84
20 THE GRADE APPROACH FOR DEVELOPING RECOMMENDATIONS
The User’s Guides To The Medical Literature: A Manual for Evidence -Based Clinical Practice, second edit ion. 22.4:679-702.
20.1 OBJECTIVES
! To demonstrate how to assess the quality of evidence available to answer each relevant question.
! To demonstrate how to develop strength of recommendation. ! To discuss the relationship between quality of evidence and strength of recommendation.
There may be strong recommendation in the presence of evidence of low quality?
20.2 ELABORATION OF WELL STRUCTURED CLINICAL QUESTIONS AND IDENTIFICATION OF THE RELEVANT OUTCOMES
The formulation of structured questions should consider the perspectives of all stakeholders involved in the policy. These issues must clearly state the population of interest of the guideline, interventions and their alternatives, as well as relevant outcomes for the patient population and for the health system.
20.3 SYSTEMATIC REVIEW OF LITERATURE
The systematic review should be performed for each structured question that was drafted and selected as relevant by the guideline development team, with clear criteria on what types of studies to include or not in the review. More information on the methods of preparation of a systematic review can be found in the Cochrane Handbook.
20.4 HOW TO ASSESS THE QUALITY OF THE EVIDENCE?
A avaliação da quality of evidence diz respeito a avaliação do conjunto de evidências encontradas32 capazes de responder as questões estruturadas que foram formuladas. Os aspectos que devem ser considerados nesta avaliação estão descritos na Table 9. A quantificação da magnitude e precision dos Results, o gradiente dose-resposta, bem como a presença de confundidores que poderiam amenizar o benefício da intervention podem aumentar a quality of evidence.
Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
85
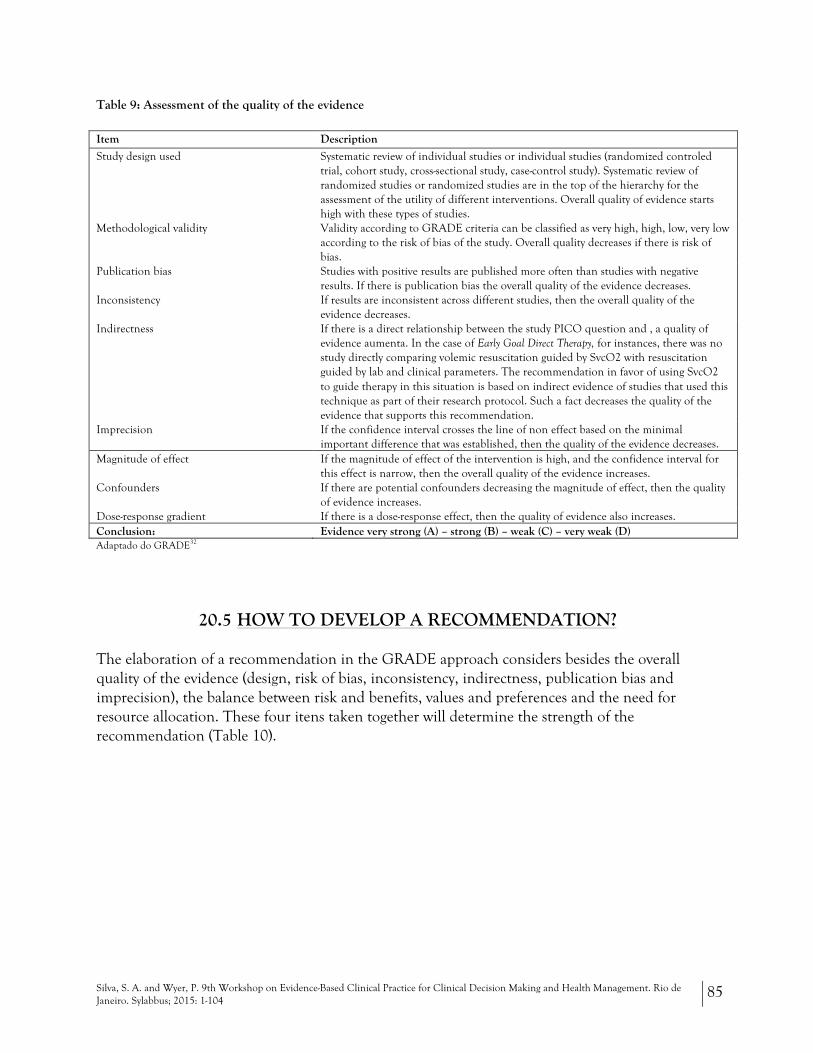
Table 9: Assessment of the quality of the evidence
Item Description
Study design used Systematic review of individual studies or individual studies (randomized controled trial, cohort study, cross-sectional study, case-control study). Systematic review of randomized studies or randomized studies are in the top of the hierarchy for the assessment of the utility of different interventions. Overall quality of evidence starts high with these types of studies.
Methodological validity Validity according to GRADE criteria can be classified as very high, high, low, very low according to the risk of bias of the study. Overall quality decreases if there is risk of bias.
Publication bias Studies with positive results are published more often than studies with negative results. If there is publication bias the overall quality of the evidence decreases.
Inconsistency If results are inconsistent across different studies, then the overall quality of the evidence decreases.
Indirectness If there is a direct relationship between the study PICO question and , a quality of evidence aumenta. In the case of Early Goal Direct Therapy, for instances, there was no study directly comparing volemic resuscitation guided by SvcO2 with resuscitation guided by lab and clinical parameters. The recommendation in favor of using SvcO2 to guide therapy in this situation is based on indirect evidence of studies that used this technique as part of their research protocol. Such a fact decreases the quality of the evidence that supports this recommendation.
Imprecision If the confidence interval crosses the line of non effect based on the minimal important difference that was established, then the quality of the evidence decreases.
Magnitude of effect If the magnitude of effect of the intervention is high, and the confidence interval for this effect is narrow, then the overall quality of the evidence increases.
Confounders If there are potential confounders decreasing the magnitude of effect, then the quality of evidence increases.
Dose-response gradient If there is a dose-response effect, then the quality of evidence also increases. Conclusion: Evidence very strong (A) – strong (B) – weak (C) – very weak (D) Adaptado do GRADE32
20.5 HOW TO DEVELOP A RECOMMENDATION?
The elaboration of a recommendation in the GRADE approach considers besides the overall quality of the evidence (design, risk of bias, inconsistency, indirectness, publication bias and imprecision), the balance between risk and benefits, values and preferences and the need for resource allocation. These four itens taken together will determine the strength of the recommendation (Table 10).

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
86
Table 10: Clinical consideration for the strength of recommendation on the GRADE approach.
Considerations in favor of Considerations against Conclusion Quality of the evidence Many high quality randomised trials
have shown the benefit of inhaled steroids in asthma
Only case series have examined the utility of pleurodesis in pneumothorax
A, B, C or D?
Do the benefits overcome risks?
Aspirin in myocardial infarction reduces mortality with minimal toxicity, inconvenience, and cost
Warfarin in low risk patients with atrial fibrillation results in small stroke reduction but increased bleeding risk and substantial inconvenience
Yes Maybe Maybe not No
Patients values and preferences are in accordance to the recommendation?
Young patients with lymphoma will invariably place a higher value on the life prolonging effects of chemotherapy than on treatment toxicity
Older patients with lymphoma may not place a higher value on the life prolonging effects of chemotherapy than on treatment toxicity
Yes Maybe Maybe not No
Resources allocation are clearly justifiable?
The low cost of aspirin as prophylaxis against stroke in patients with transient ischemic attacks
The high cost of clopidogrel and of combination dipyridamole and aspirin as prophylaxis against stroke in patients with transient ischaemic attacks
Yes Maybe Maybe not No
Recommendation: In favor of? Against?
Strength of recommendation: Strong? Weak?
Adapted from GRADE30
The establishment of the strength of recommendation is a complex process and should not be done by one or two individuals but by a board composed of at least specialists, methodologists and clinicians, with all holding the summary of the body of the evidence that has been selected and analyzed in a systematic way by the guideline development group. Consensus should also be made in a transparent and systematic way using a validated process such as Delphi.
In the GRADE approach the summary of evidence is produced by the guideline development group in a table format by using the GRADEpro tool. (http://www.gradeworkinggroup.org/toolbox/index.htm)
More information on the method of developing a guideline and making recommendations can be obtained at the Institute of Medicine's report on "Guidelines We Can Trust". These items are all available under "Supplements" in the SIMPLE. Website.
Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
87
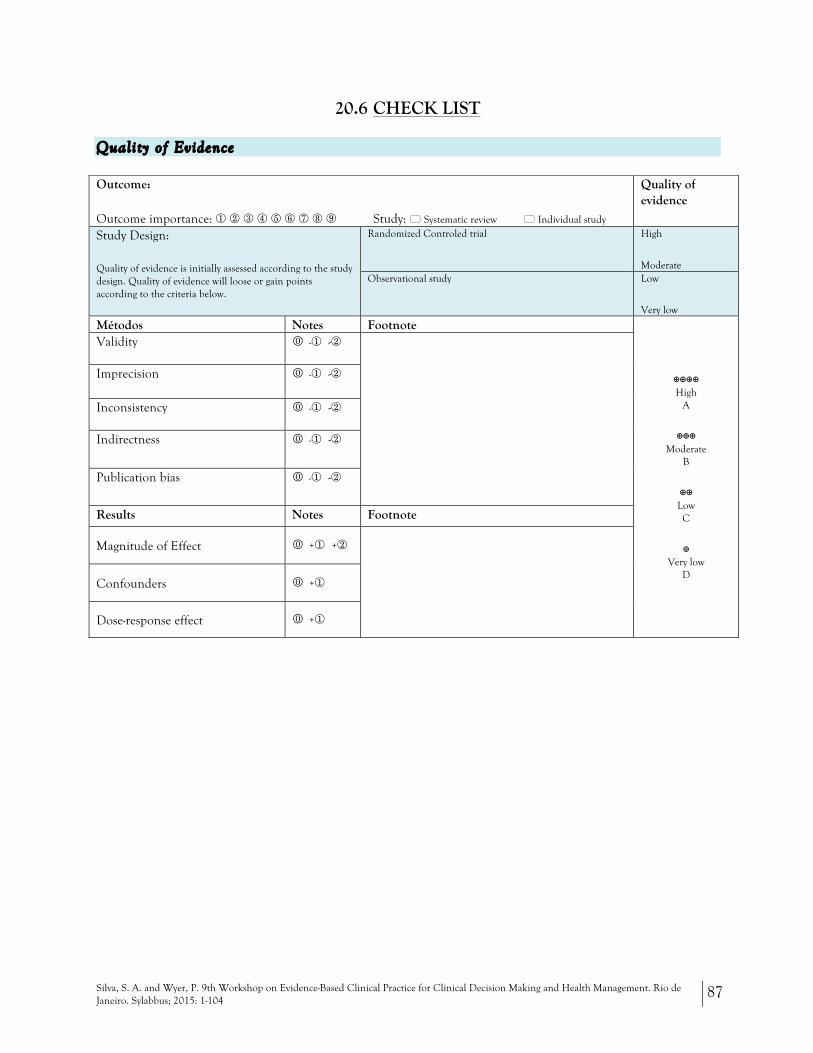
20.6 CHECK LIST
Quality of Evidence
Outcome:
Outcome importance: ① ② ③ ④ ⑤ ⑥ ⑦ ⑧ ⑨ Study: ! Systematic review ! Individual study
Quality of evidence
Study Design:
Quality of evidence is initially assessed according to the study design. Quality of evidence will loose or gain points according to the criteria below.
Randomized Controled trial
High
Moderate Observational study Low
Very low
Métodos Notes Footnote
⊕⊕⊕⊕ High
A
⊕⊕⊕ Moderate
B
⊕⊕ Low C
⊕ Very low
D
Validity 0 -① -②
Imprecision 0 -① -②
Inconsistency 0 -① -②
Indirectness 0 -① -②
Publication bias 0 -① -②
Results Notes Footnote
Magnitude of Effect 0 +① +②
Confounders 0 +①
Dose-response effect 0 +①

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
88
Strength of recommendation
Factor Comment Strength of recommendation
Balance between desirable and undesirable effects
The larger the difference between the desirable and undesirable effects, the higher the likelihood that a strong recommendation is warranted. The narrower the gradient, the higher the likelihood that a weak recommendation is warranted
Strong recommendation in favor of the intervention
!!
Weak recommendation in favor of the intervention
!?
Weak recommendation against
"?
Strong recommendation against
""
Quality of evidence
The higher the quality of evidence, the higher the likelihood that a strong recommendation is warranted
Values and preferences
The more values and preferences vary, or the greater the uncertainty in values and preferences, the higher the likelihood that a weak recommendation is warranted
Resources allocation
The higher the costs of an intervention—that is, the greater the resources consumed—the lower the likelihood that a strong recommendation is warranted

89
Section V IMPLEMENTATION
Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
90
21 GUIDELINES
The User’s Guides To The Medical Literature: A Manual for Evidence -Based Clinical Practice, second edit ion. 21:597-618 / 22.4:679-702
21.1 OBJECTIVES
! To demonstrate how to critically appraise a practice guideline. ! To demonstrate how to interpret its results. ! To demonstrate how to apply its results for decision making.
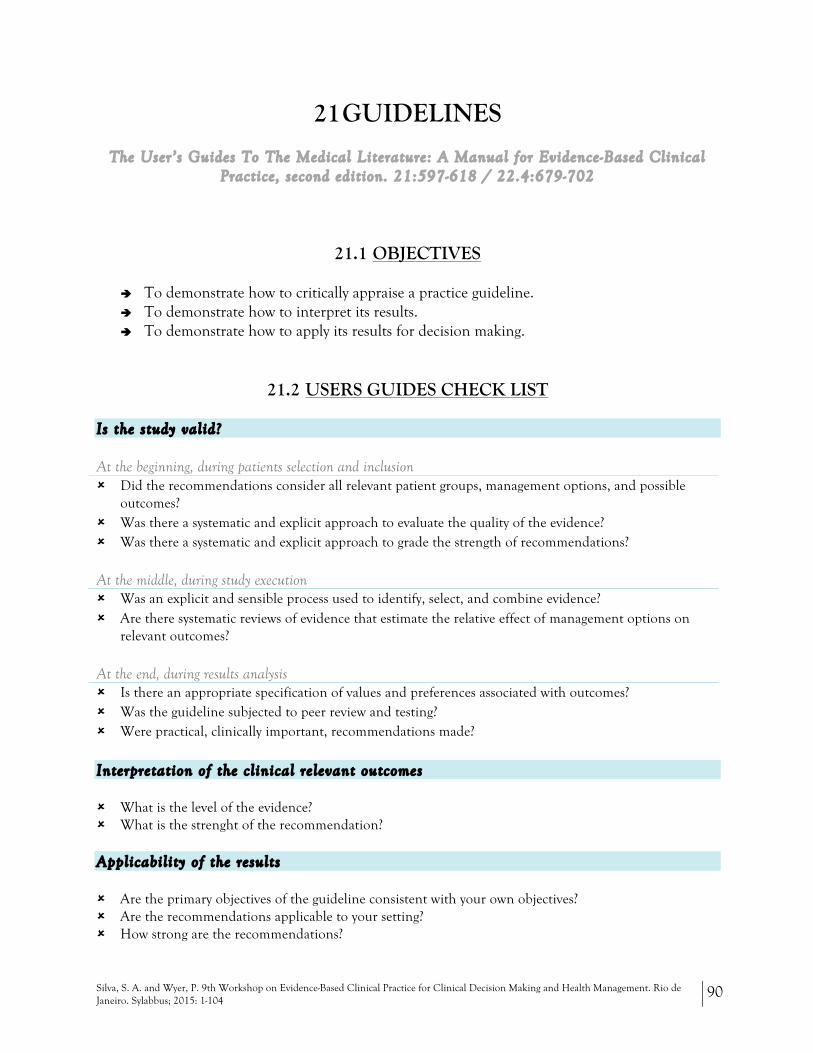
21.2 USERS GUIDES CHECK LIST
Is the study valid?
At the beginning, during patients selection and inclusion # Did the recommendations consider all relevant patient groups, management options, and possible
outcomes? # Was there a systematic and explicit approach to evaluate the quality of the evidence? # Was there a systematic and explicit approach to grade the strength of recommendations?
At the middle, during study execution # Was an explicit and sensible process used to identify, select, and combine evidence? # Are there systematic reviews of evidence that estimate the relative effect of management options on
relevant outcomes?
At the end, during results analysis # Is there an appropriate specification of values and preferences associated with outcomes? # Was the guideline subjected to peer review and testing? # Were practical, clinically important, recommendations made?
Interpretation of the c l inical re levant outcomes
# What is the level of the evidence? # What is the strenght of the recommendation?
Applicabi l i ty of the results
# Are the primary objectives of the guideline consistent with your own objectives? # Are the recommendations applicable to your setting? # How strong are the recommendations?
Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
91
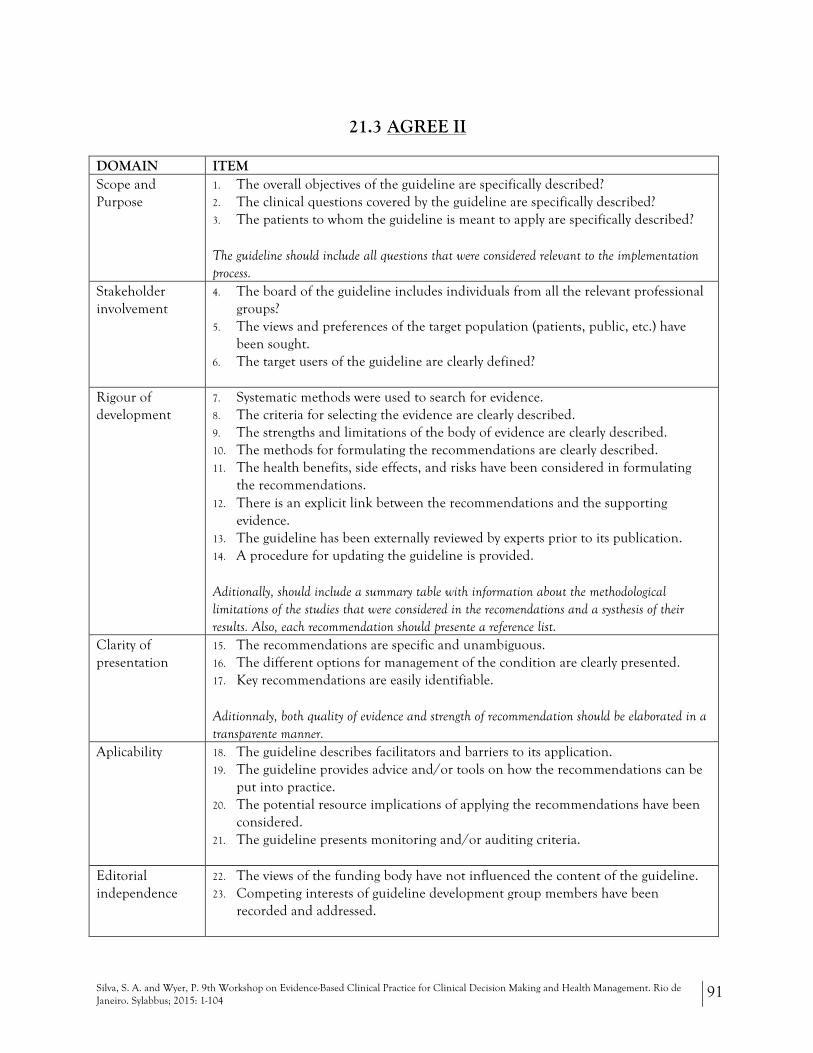
21.3 AGREE II
DOMAIN ITEM Scope and Purpose
1. The overall objectives of the guideline are specifically described? 2. The clinical questions covered by the guideline are specifically described? 3. The patients to whom the guideline is meant to apply are specifically described?
The guideline should include all questions that were considered relevant to the implementation process.
Stakeholder involvement
4. The board of the guideline includes individuals from all the relevant professional groups?
5. The views and preferences of the target population (patients, public, etc.) have been sought.
6. The target users of the guideline are clearly defined?
Rigour of development
7. Systematic methods were used to search for evidence. 8. The criteria for selecting the evidence are clearly described. 9. The strengths and limitations of the body of evidence are clearly described. 10. The methods for formulating the recommendations are clearly described. 11. The health benefits, side effects, and risks have been considered in formulating
the recommendations. 12. There is an explicit link between the recommendations and the supporting
evidence. 13. The guideline has been externally reviewed by experts prior to its publication. 14. A procedure for updating the guideline is provided.
Aditionally, should include a summary table with information about the methodological limitations of the studies that were considered in the recomendations and a systhesis of their results. Also, each recommendation should presente a reference list.
Clarity of presentation
15. The recommendations are specific and unambiguous. 16. The different options for management of the condition are clearly presented. 17. Key recommendations are easily identifiable.
Aditionnaly, both quality of evidence and strength of recommendation should be elaborated in a transparente manner.
Aplicability 18. The guideline describes facilitators and barriers to its application. 19. The guideline provides advice and/or tools on how the recommendations can be
put into practice. 20. The potential resource implications of applying the recommendations have been
considered. 21. The guideline presents monitoring and/or auditing criteria.
Editorial independence
22. The views of the funding body have not influenced the content of the guideline. 23. Competing interests of guideline development group members have been
recorded and addressed.
Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
92
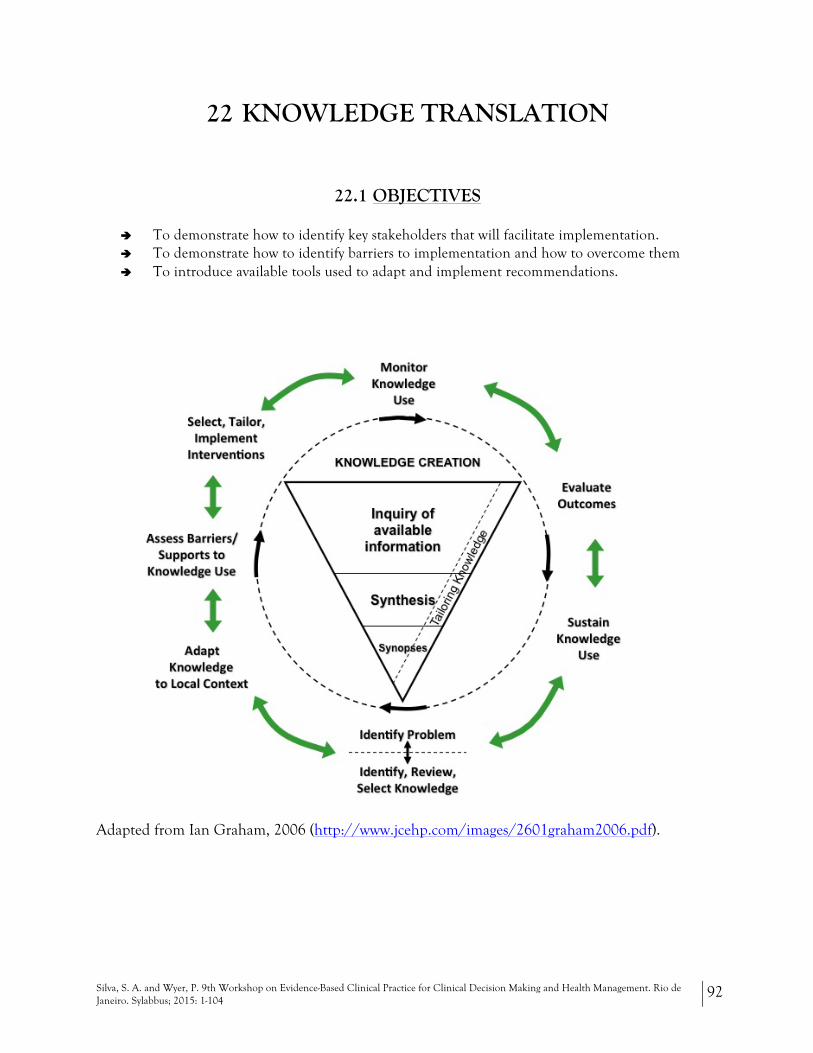
22 KNOWLEDGE TRANSLATION
22.1 OBJECTIVES
! To demonstrate how to identify key stakeholders that will facilitate implementation. ! To demonstrate how to identify barriers to implementation and how to overcome them ! To introduce available tools used to adapt and implement recommendations.
Adapted from Ian Graham, 2006 (http://www.jcehp.com/images/2601graham2006.pdf).

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
93
22.2 KNOWLEDGE TRANSLATION/EVIDENCE-BASED QUALITY IMPROVEMENT
Background
Two perspectives pertain to the interface between care coordination and improvement in clinical settings and the process through which knowledge gleaned from clinical research is assimilated into practice. Looking at the issue from the perspective of researchers seeking realization of the fruits of their toil, Glasziou and Haynes estimated that as few as 20% of effective interventions may actually reach patients.1 Changing clinician behavior to ensure implementation of the best evidence into practice is challenging. The evidence pipeline is a visual tool (variously adapted by Lang, Haynes and others) that demonstrates the knowledge translation cycle.2 The first stage is getting the evidence straight. This involves all of the principles of critical appraisal and evidence synthesis. Through the next three stages, the results and conclusions obtained through excellent clinical research are characteristically dissipated; most of the potential benefits fail to reach the patient. A well-planned project that addresses the barriers and facilitators at each of these stages will ensure more complete and/or systematic uptake of the recommended practice.
A great deal of literature has been devoted to the issue of implementation of specific interventions, such as sepsis pathways, clinical prediction rules and even entire practice guidelines.3 The perspective that is most pertinent when the objective of an effort is to develop or increase the utilization of specific intervention, decision tool or guideline is represented as a ‘knowledge to action’ cycle and may be considered to be the ‘knowledge translation’ (KT) mode. 4
A second perspective related to the incorporation of clinical evidence into practice may be better described as ‘evidence-based quality improvement.’ 5 In this case, the impulse comes not from the perceived need to implement a specific intervention or guideline, but rather to improve care in a particular clinical area and setting and develop indicators that allow an evaluation of the evidence implementation program. This mode, which might be considered to reflect more of a ‘practice-based’ perspective, is perhaps closer to the premises and orientation of the TEACH program. A QI model that incorporated evidence-based principles within it, developed by Wright et al, 6 contributed substantially to the TEACH design.
The principles summarized below apply commonly to both the KT and the ‘evidence based QI’ modes.
Steps to Change Behavior to Implement Evidence into Practice (modified from7)
1. Start with a manageable problem and specify an achievable goal – plan to develop a formal proposal including all components
2. Key ingredients: Teamwork and leadership 3. Do an environmental scan 4. Identify gaps in care – document deviation from ideal practice or variability in practice 5. Understand current behavior 6. Understand relevant evidence on effectiveness of uptake strategies in this area 7. Map your intervention strategy and care plan in detail 8. Create a data collection system 9. Decide how to report results to your target audience 10. Select and introduce behavior change strategies 11. Reevaluate performance and modify behavior as necessary 12. Plan for sustainability

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
94
Three areas summarize the focus of such an endeavor:
! Identify key stakeholders who will facilitate implementation strategies ! Understand current behavior: Identification of barriers to and facilitators of evidence uptake ! Develop an evidence implementation plan: Select and introduce behavior change strategies
The leadership attributes of change agents help to select the appropriate stake holder representatives (Six sigma black belt change agents).7
! Work well independently and in groups ! Remain calm under pressure ! Anticipate problems and act immediately ! Respect colleagues and are respected by the team ! Inspire others ! Delegate tasks to others and coordinate efforts ! Understand abilities and limitations of colleagues ! Show genuine concern for others for what they need and want ! Accept criticism well ! Want improvement
Choosing Change Strategies
! Prioritize barriers into those potentially amenable to change ! Professional interventions (CME, audit and feedback) ! Financial interventions ! Organizational interventions (expanded roles for nurses, NPs) ! Regulatory interventions (professional credentialing)
The Cochrane Effective Practice and Organization of Care Reviews Group under the authorship of Grimshaw, Shirran and Thomas, completed a summary of 41 systematic reviews of hundreds of original studies testing the effects of different behavior change strategies on clinician behavior and patient outcome.10 The review concludes that active strategies (workshops) are more effective than passive strategies (handing out an educational leaflet).
However, this has been revised by a more recent review of 235 studies of guideline dissemination and implementation strategies done by the same lead author.11 This paper suggests that most methods tested for changing clinician behavior have a very modest effect. The above literature suggests that the best methods for practitioner education for practice change include manual or computerized prompts, distributing educational material, audit and feedback and multiple concurrent strategies.
A final point relevant to the TEACH process: evidence based skills come into play in the context of a practice-based ‘evidence based quality improvement’ approach in two ways. Firstly they enable a QI project to efficiently tap into the best and most current evidence pertaining to the content of care in the designated clinical area and setting. Secondly, they pertain to the process of locating and assimilating evidence pertaining to the process of care in analogous settings.

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
95
Bibliografia:
1. Glasziou P, Haynes B. The paths from research to improved health outcomes. ACP JC. 2005;142(2):A8-10 2. Lang ES, Wyer PC, Haynes RB. Knowledge Translation: Closing the Evidence-to-Practice Gap. Ann
Emerg Med. 2007;49:355-363. 3. Harrison MB, Legare F, Graham ID, et al. Adapting Clinical Practice Guidelines to Local Context and
Assessing Barriers to Their Use. CMAJ 2010;182:E78-E84. 4. Strauss SE, Holroyd-Leduc J. Knowledge-to-action Cycle. Evidence Based Med 2008;13:98-100. 5. Shojania KG, Grimshaw JM. Evidence-based Quality Improvement: The State of the Science. Health
Affairs 2005;24:138-150. 6. Wright SW, Trott A, Lindsell CJ, Smith C, Gibler WB. Creating a System to Facilitate Translation of
Evidence Into Standardized Clinical Practice: A Preliminary Report. Ann Emerg Med. 2008;51:80-86. 7. Cook DJ, Wall RJ, Foy R, et al. Changing Behavior to Apply Best Evidence in Practice. In: Users’ Guides
to the Medical Literature: A Manual for Evidence-Based Clinical Practice, 2nd Edition, Guyatt G, et al Editors. , New York, NY: The McGraw-Hill Companies, Inc, 2008; Chapter 22.7, P.721-742
8. Hogan DL, Logan JThe Ottawa Model of Research Use: a guide to clinical innovation in the NICU. Clin Nurse Spec. 2004 Sep-Oct;18(5):255-61
9. Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, Rubin HR. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999 Oct 20;282(15):1458-65.
10. Grimshaw JM, Shirran L, Thomas R, et al. Changing provider behavior: an overview of systematic reviews of interventions. Med Care. 2001;39(8) (suppl 2):112-45.
11. Grimshaw JM, Thomas RE, MacLennan G, et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technology Assess. 2004;8(6):iii-iv, 1-72.

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
96
22.3 CASE SCENARIO
Early Goal Direct Therapy for Sepsis Protocol
You are the head of the emergency department and have been approached by representatives of the quality improvement committee of the hospital. As a result of two recent sepsis related deaths, in which the diagnosis and hence the treatment was delayed, they have performed a survey and have determined that the in-hospital mortality rate for patients admitted with sepsis has been higher than expected. They are asking for an institution wide review of sepsis care for the purpose of improving outcomes in this area. Working with the director of the intensive care unit and several other stake holders in the facility, including nursing administration, you have agreed that there have been several studies looking at early goal directed therapy for sepsis, which have shown a benefit to patients. There is currently no structured protocol in your facility to address the acute sepsis care. You, working with others on your provisional pathway committee proceed to review the evidence and develop an evidence-based guideline for how to manage these patients in your hospital.
You previously presented the systematic review by Jones, et al in journal club last year, and have been frustrated to see that there has been little change in practice. We know that time is of the essence in the management of trauma and acute myocardial infarction, and there is now substantial evidence that timely and appropriate care provided to patients with sepsis reduces mortality. Nonetheless, these patients are often not targeted to receive aggressive care in the ED. Lack of timely care results in increased mortality and increased costs.
You are very interested in why evidence that clearly demonstrates a benefit to the patients does not change behavior in the department or your institution. You believe there is an urgent need and agree to be the physician lead on this project.
Enclosures
1. Didactic handout for knowledge translation 2. Cook DJ, Wall RJ, Foy R, et al. Changing Behavior to Apply Best Evidence in Practice. In: Users’ Guides to the
Medical Literature: A Manual for Evidence-Based Clinical Practice, 2nd Edition, Guyatt G, et al Editors. , New York, NY: The McGraw-Hill Companies, Inc, 2008; Chapter 22.7, P.721-742.
3. Jones AE, Brown MD, Trzeciak S, et al . The Effect of quantitative resuscitation strategy on mortality in patients with sepsis: A meta-analysis. Crit Care Med 2008;36:2734-39. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2737059/?tool=pubmed
4. Rivers, Nguyen, Havstad et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001;345:1368-77. http://content.nejm.org/cgi/content/abstract/345/19/1368

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
97
22.3.1 Part I : Identication of the key stakeholders that wil l faci l i tate implementation strategies
Key Ingredients: teamwork and leadership
Pick leaders who are change agents as suggested by the leadership attributes of Black Belts in the Six Sigma method.
Include someone with biostatistics skills early in the planning stages to help ensure your design and data collection are appropriate.
Action Current process Proposed new process Department Responsible for Action
Stakeholder Responsible person
Early identification of sepsis
Patients triaged per CTAS
Increase triage awareness ED ED clinical resource nurse
Patients picked up in department once they deteriorate
Increased education for recognition of sepsis
ED nurse educator Physician rounds coordinator
Timely delivery of antibiotics
Physician choice and order entry
New information system triggers and reminders
Information technology
EDIS representative Hospital IT programmer
Certain antibiotics mixed only in pharmacy
All first line sepsis antibiotics to be stored in ED
Pharmacy ED pharmacist Hospital pharmacist
Nursing administration as ordered
System for direct order communication and implementation
ED Charge nurse Emergency physician
Choice of appropriate antibiotics
Physician choice and order entry
Establish guidelines for suspected source
ED Internal Medicine Intensive Care
Director CQI Infectious Disease Specialists Intensivists
Identification of most likely source
Diagnostic Imaging Radiologist
Early fluid resuscitation
Physician enters orders Flagging of fluid bolus orders Direct communication
ED EDIS rep Charge nurse Emergency physician
Hemodynamic monitoring
Intermittent blood pressure
In septic shock commence central line insertion for CVP measurement
Emergency Department
Emergency physician Emergency Nurse
Intermittent lactate at physician discretion
Regular lactate levels at specified intervals
Lab Medicine Director of laboratory medicine
If vasopressors are indicated then arterial line
Vasopressor support
At treating physician discretion
Standardized choice of vasopressor Implement EDIS order set
Intensive care Emergency Department
Intensivist Emergency physician
Data collection No monitoring Monitor quality of implementation
Epidemiology Biostatician
Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
98
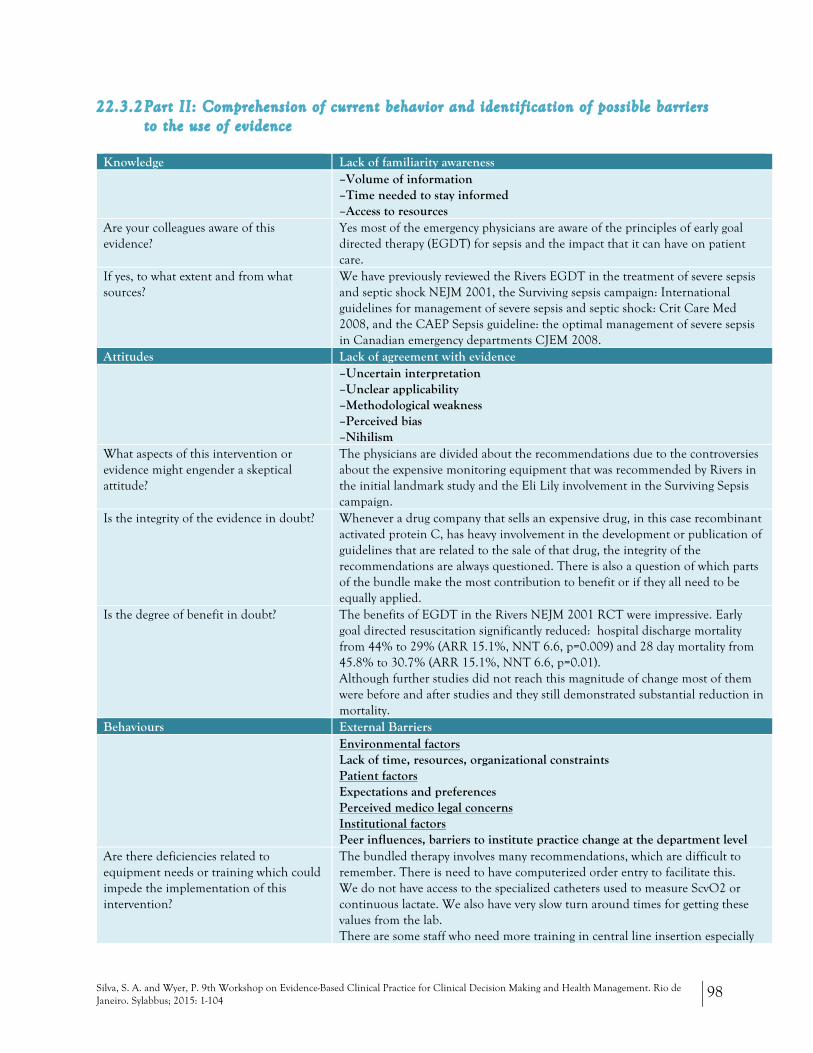
22.3.2 Part II: Comprehension of current behavior and identif ication of possible barriers to the use of evidence
Knowledge Lack of familiarity awareness –Volume of information
–Time needed to stay informed –Access to resources
Are your colleagues aware of this evidence?
Yes most of the emergency physicians are aware of the principles of early goal directed therapy (EGDT) for sepsis and the impact that it can have on patient care.
If yes, to what extent and from what sources?
We have previously reviewed the Rivers EGDT in the treatment of severe sepsis and septic shock NEJM 2001, the Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: Crit Care Med 2008, and the CAEP Sepsis guideline: the optimal management of severe sepsis in Canadian emergency departments CJEM 2008.
Attitudes Lack of agreement with evidence –Uncertain interpretation
–Unclear applicability –Methodological weakness –Perceived bias –Nihilism
What aspects of this intervention or evidence might engender a skeptical attitude?
The physicians are divided about the recommendations due to the controversies about the expensive monitoring equipment that was recommended by Rivers in the initial landmark study and the Eli Lily involvement in the Surviving Sepsis campaign.
Is the integrity of the evidence in doubt?
Whenever a drug company that sells an expensive drug, in this case recombinant activated protein C, has heavy involvement in the development or publication of guidelines that are related to the sale of that drug, the integrity of the recommendations are always questioned. There is also a question of which parts of the bundle make the most contribution to benefit or if they all need to be equally applied.
Is the degree of benefit in doubt?
The benefits of EGDT in the Rivers NEJM 2001 RCT were impressive. Early goal directed resuscitation significantly reduced: hospital discharge mortality from 44% to 29% (ARR 15.1%, NNT 6.6, p=0.009) and 28 day mortality from 45.8% to 30.7% (ARR 15.1%, NNT 6.6, p=0.01). Although further studies did not reach this magnitude of change most of them were before and after studies and they still demonstrated substantial reduction in mortality.
Behaviours External Barriers Environmental factors
Lack of time, resources, organizational constraints Patient factors Expectations and preferences Perceived medico legal concerns Institutional factors Peer influences, barriers to institute practice change at the department level
Are there deficiencies related to equipment needs or training which could impede the implementation of this intervention?
The bundled therapy involves many recommendations, which are difficult to remember. There is need to have computerized order entry to facilitate this. We do not have access to the specialized catheters used to measure ScvO2 or continuous lactate. We also have very slow turn around times for getting these values from the lab. There are some staff who need more training in central line insertion especially

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
99
ultrasound guided The antibiotics required are not all stocked in the department. The RNs will need some training in using the different vasopressors recommended. The most commonly used vasopressor in the department is dopamine.
Are there negative repercussions that could emerge as a result of this intervention (i.e. costs, medico legal issues, generating more work)
22.3.3 Part III: Development of an strategy for evidence implementation.
Knowledge What methods exist for disseminating this evidence as well as an implementation plan or protocol to relevant parties?
Need to use multiple strategies, as it is not practical to get the entire department to attend training events. To review the evidence and sort out the controversies around the monitoring devices and the surviving sepsis campaign conduct a dedicated journal club. Send out a Google doc PowerPoint presentation prior to the meeting with stimulus questions. Following the workshop send a follow up questionnaire to reinforce the learning.
For the implementation plan design a poster to outline the algorithm and post it in the resuscitation area. Place the entire protocol with a copy of the poster as well on the website.
Develop an email campaign “Sepsis One Minute at a Time” with short snappers explaining the rationale behind each step in the algorithm.
Who best to present the evidence and the implementation plan in a way that maximizes impact?
Need to select opinion leaders in the group who can influence the team. Respected, knowledgeable RNs and MDs will conduct the various teaching sessions and design the website. We will also ask for guest appearances from ICU and Infectious Diseases to attend for support and advice.
Atitudes How would you generate a culture of improvement and innovation around this project?
Use actual inputs from the two mortality cases in the scenario, patient and staff concerns or incident reports to address a real need for change. Use the evidence from the papers reviewed to demonstrate the size of the impact that we could have on mortality if we do what we do better and work as a team. There is nothing new here just improving our performance for the benefit of the patient.
Who should be involved in the development of this project?
Emergency department CQI team, consisting of lead physician, lead RN, support from ED director, nurse manager, and CQI leader.
Clinical Resource Nurse, Nurse Educators, Pharmacy, Information Technology, Infectious Disease specialist, Intensivist, Radiology, Laboratory Medicine. See Part II above.
How do you motivate involvement?
Make it easier to accomplish by providing order sets, checklists and better access to labs and equipment.
Standardization also makes things easier for the RN’s as they know what to expect.

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
100
Monitor performance and give specific and timely feedback.
Release antibiotics the to the department, so that ID and Pharmacy consultation is not required.
How would you seek out the resources that could support the development of this initiative?
Get assistance from the medical education program and the nurse educators for development of the presentations, Google doc and email campaign. Seek hospital media and communications support to create the poster.
Meet with laboratory medicine to engage them in the necessity to improve lab turn around times.
Behaviours What modality (ies) would you choose to maximize the effect of an action plan (e.g. develop a protocol, change requisitions, pre-printed orders, develop an electronic resource)?
Develop a protocol, design a poster, upload protocol to website. Create EDIS order sets to provide inclusion and exclusion criteria reminders, to automatically trigger appropriate laboratory, diagnostic and monitoring orders.
Create EDIS order sets with recommendations for fluid therapy, antibiotics, vasopressors and blood products.
Design a flow sheet for monitoring vitals signs, recurrent labs and fluids administered.
Develop quality indicators that can be easily pulled from the EDIS to monitor implementation plan.
How would you recruit the resources that might be necessary (time / monetary / manpower) to implement this action plan?
Meet with Clinical Department Head, Administrative Director, Chief of Staff, Director of Laboratory Medicine and Information Technology to obtain support from their departments.
Get funding through the medical education budget for a resident project to help with biostatistics and information technology demand
What equipment and training are required to implement this plan?
No new equipment will be required, as we will do intermittent monitoring of lactate and ScvO2.
The most intensive training will be geared to the early recognition of sepsis to get these patients entered into the pathway.
We will be using some new teaching technologies with Google docs, which may require an orientation.
The remainder of the training will focus on the explanation of the somewhat complicated treatment algorithm
What methods would you employ to identify eligible patients?
Need to increase awareness in triage by teaching the SIRs criteria and ensuring that it is recognized.
Have more direct communication between nurses and physicians once SIRs criteria are met, much like ECG is always presented directly to MD to read once it is completed. Unfortunately, there is no easily identifiable marker of sepsis.
How would you promote and market this protocol in a manner that can maximize buy-in and success?
Emphasize how we can have a major impact on patient outcomes by working together as a team. The approach to these patients is currently chaotic and variable. Implementing this protocol will get everyone on the same page, moving in the same direction and will make our work easier.
Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
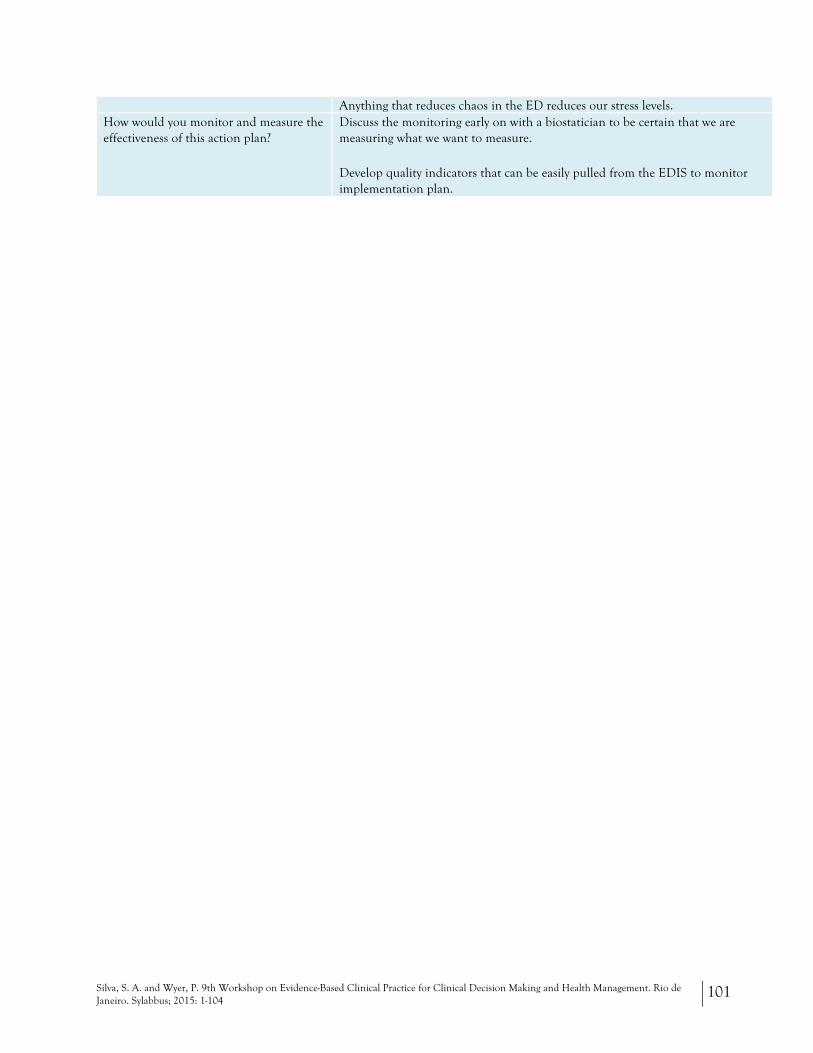
101
Anything that reduces chaos in the ED reduces our stress levels. How would you monitor and measure the effectiveness of this action plan?
Discuss the monitoring early on with a biostatician to be certain that we are measuring what we want to measure.
Develop quality indicators that can be easily pulled from the EDIS to monitor implementation plan.

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
102
References
1. Tan SY, Uyehara P. William Osler (1849-1919): medical educator and humanist. Singapore medical journal. 2009;50(11):1048-1049.
2. Sackett DL. Teaching critical appraisal. Journal of general internal medicine. 1990;5(3):272. 3. Sackett DL, Wennberg JE. Choosing the best research design for each question. BMJ. 1997;315(7123):1636. 4. Evidence-based medicine. A new approach to teaching the practice of medicine. JAMA : the journal of the
American Medical Association. 1992;268(17):2420-2425. 5. Guyatt G. Evidence-based medicine (Editorial). ACP Journal Club. Annals of Internal Medicine. 1991;114(Suppl.
2):A16. 6. Haynes RB. What kind of evidence is it that Evidence-Based Medicine advocates want health care providers
and consumers to pay attention to? BMC health services research. 2002;2:3. 7. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and
what it isn't. Bmj. 1996;312(7023):71-72. 8. Tanenbaum SJ. What physicians know. The New England journal of medicine. 1993;329(17):1268-1271. 9. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and
what it isn't. 1996. Clinical orthopaedics and related research. 2007;455:3-5. 10. Onate-Ocana LF, Ochoa-Carrillo FJ. The GRADE system for classification of the level of evidence and grade
of recommendations in clinical guideline reports. Cirugia y cirujanos. 2009;77(5):417-419. 11. Schunemann HJ, Best D, Vist G, Oxman AD. Letters, numbers, symbols and words: how to communicate
grades of evidence and recommendations. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2003;169(7):677-680.
12. Glasziou P, Vandenbroucke JP, Chalmers I. Assessing the quality of research. BMJ. 2004;328(7430):39-41. 13. Barbui C, Dua T, van Ommeren M, et al. Challenges in developing evidence-based recommendations using
the GRADE approach: the case of mental, neurological, and substance use disorders. PLoS medicine. 2010;7(8).
14. Owens DK, Lohr KN, Atkins D, et al. AHRQ series paper 5: grading the strength of a body of evidence when comparing medical interventions--agency for healthcare research and quality and the effective health-care program. Journal of clinical epidemiology. 2010;63(5):513-523.
15. Kunz R, Djulbegovic B, Schunemann HJ, Stanulla M, Muti P, Guyatt G. Misconceptions, challenges, uncertainty, and progress in guideline recommendations. Seminars in hematology. 2008;45(3):167-175.
16. Hitt J. Evidence-Based Medicine. THE YEAR IN IDEAS: A TO Z. 2001; http://www.nytimes.com/2001/12/09/magazine/the-year-in-ideas-a-to-z-evidence-based-medicine.html. Accessed Mar 29, 2012.
17. Godlee F. Milestones on the long road to knowledge. BMJ. 2007;334 Suppl 1:s2-3. 18. Sehon SR, Stanley DE. A philosophical analysis of the evidence-based medicine debate. BMC health services
research. 2003;3(1):14. 19. Silva SA, Charon R, Wyer PC. The marriage of evidence and narrative: scientific nurturance within clinical
practice. Journal of evaluation in clinical practice. 2011;17(4):585-593. 20. Silva SA, Wyer P. The Roadmap: a blueprint for evidence literacy within a Scientifically Informed Medical
Practice and LEarning model. Journal of Person Centred Medicine. 2012:In press. 21. Fryback DG, Thornbury JR. The efficacy of diagnostic imaging. Medical decision making : an international
journal of the Society for Medical Decision Making. 1991;11(2):88-94. 22. Silva SA, Wyer PC. The Roadmap: a blueprint for evidence literacy within a Scientifically Informed Medical
Practice and Learning Model. European Journal of Person Centered Healthcare. 2013;3(1):53-68. 23. Hlatky MA, Greenland P, Arnett DK, et al. Criteria for evaluation of novel markers of cardiovascular risk: a
scientific statement from the American Heart Association. Circulation. 2009;119(17):2408-2416.

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
103
24. Methods Guide for Medical Test Reviews. 2010; http://www.effectivehealthcare.ahrq.gov/tasks/sites/ehc/assets/File/methods_guide_for_medical_tests.pdf, 2014.
25. Guidance by type. NICE Guidance 2014; http://www.nice.org.uk/guidance/index.jsp?action=byType, 2014.
26. Schwartz MD, Valdimarsdottir HB, DeMarco TA, et al. Randomized trial of a decision aid for BRCA1/BRCA2 mutation carriers: impact on measures of decision making and satisfaction. Health psychology : official journal of the Division of Health Psychology, American Psychological Association. 2009;28(1):11-19.
27. Saadatmand S, Rutgers EJ, Tollenaar RA, et al. Breast density as indicator for the use of mammography or MRI to screen women with familial risk for breast cancer (FaMRIsc): a multicentre randomized controlled trial. BMC cancer. 2012;12:440.
28. Anderson DR, Kahn SR, Rodger MA, et al. Computed tomographic pulmonary angiography vs ventilation-perfusion lung scanning in patients with suspected pulmonary embolism: a randomized controlled trial. JAMA : the journal of the American Medical Association. 2007;298(23):2743-2753.
29. Hachamovitch R, Hayes SW, Friedman JD, Cohen I, Berman DS. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation. 2003;107(23):2900-2907.
30. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-926.
31. Brozek JL, Akl EA, Compalati E, et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines part 3 of 3. The GRADE approach to developing recommendations. Allergy. 2011;66(5):588-595.
32. Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck-Ytter Y, Schunemann HJ. What is "quality of evidence" and why is it important to clinicians? BMJ. 2008;336(7651):995-998.
33. Conti R, Veenstra DL, Armstrong K, Lesko LJ, Grosse SD. Personalized medicine and genomics: challenges and opportunities in assessing effectiveness, cost-effectiveness, and future research priorities. Medical decision making : an international journal of the Society for Medical Decision Making. 2010;30(3):328-340.
34. Green RC, Roberts JS, Cupples LA, et al. Disclosure of APOE genotype for risk of Alzheimer's disease. The New England journal of medicine. 2009;361(3):245-254.
35. Briel M, Ferreira-Gonzalez I, You JJ, et al. Association between change in high density lipoprotein cholesterol and cardiovascular disease morbidity and mortality: systematic review and meta-regression analysis. BMJ. 2009;338:b92.
36. Charon R. Narrative Medicine: Attention, Representation, Affiliation. Narrative. 2005;13:261-269. 37. Charon R, Wyer P. Narrative evidence based medicine. Lancet. 2008;371(9609):296-297. 38. Epstein RM, Peters E. Beyond Information: Exploring Patient's Preferences. JAMA : the journal of the
American Medical Association. 2009;302:195-197. 39. Freire P. Education for Critical Consciousness. New York: Continuum; 1974. 40. Richardson WS, Wilson MC, Nishikawa J, Hayward RS. The well-built clinical question: a key to evidence-
based decisions. ACP journal club. 1995;123(3):A12-13. 41. Pfisterer M, Buser P, Rickli H, et al. BNP-guided vs symptom-guided heart failure therapy: the Trial of
Intensified vs Standard Medical Therapy in Elderly Patients With Congestive Heart Failure (TIME-CHF) randomized trial. JAMA : the journal of the American Medical Association. 2009;301(4):383-392.
42. Ellis P. Research on the Comparative Effectiveness of Medical Treatments: Issues and Options for an Expanded Federal Role. 2007; http://www.cbo.gov/publication/41655. Accessed April 9, 2012.
43. Haynes B. Clinical Study Categories. 2011; http://www.ncbi.nlm.nih.gov/pubmed/clinical. Accessed April 9, 2012.
44. Pasternak T, Movshon JA, Merigan WH. Creation of direction selectivity in adult strobe-reared cats. Nature. 1981;292(5826):834-836.
45. Pasternak T, Merigan WH, Movshon JA. Motion mechanisms in strobe-reared cats: psychophysical and electrophysical measures. Acta Psychol (Amst). 1981;48(1-3):321-332.

Silva, S. A. and Wyer, P. 9th Workshop on Evidence-Based Clinical Practice for Clinical Decision Making and Health Management. Rio de Janeiro. Sylabbus; 2015: 1-104
104
46. Melvill Jones G, Mandl G, Cynader M, Outerbridge JS. Eye oscillations in strobe reared cats. Brain Res. 1981;209(1):47-60.
47. Mandl G, Melvill Jones G, Cynader M. Adaptability of the vestibulo-ocular reflex to vision reversal in strobe reared cats. Brain Res. 1981;209(1):35-45.
48. Kopans DB. A strobe-sequenced device to facilitate the three-dimensional viewing of cross-sectional images. Radiology. 1980;135(3):780-781.
49. Skinner JS, Smeeth L, Kendall JM, Adams PC, Timmis A. NICE guidance. Chest pain of recent onset: assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin. Heart. 2010;96(12):974-978.





























