Embed Size (px)
Citation preview
Systemic Therapy & Biologicsfor
PSORIASIS
Chang Choong ChorConsultant DermatologistCC Chang Skin Specialist @ Gleneagles Kuala Lumpur
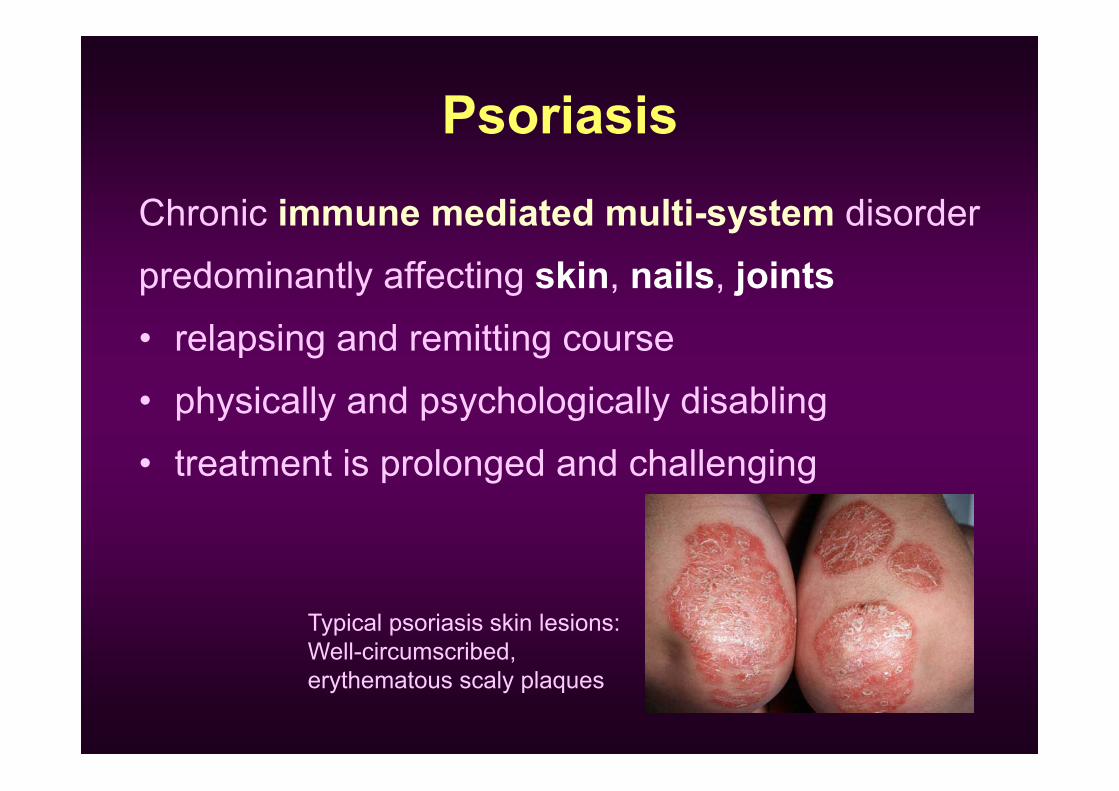
PsoriasisChronic immune mediated multi-system disorderpredominantly affecting skin, nails, joints• relapsing and remitting course• physically and psychologically disabling• treatment is prolonged and challenging
Typical psoriasis skin lesions: Well-circumscribed, erythematous scaly plaques
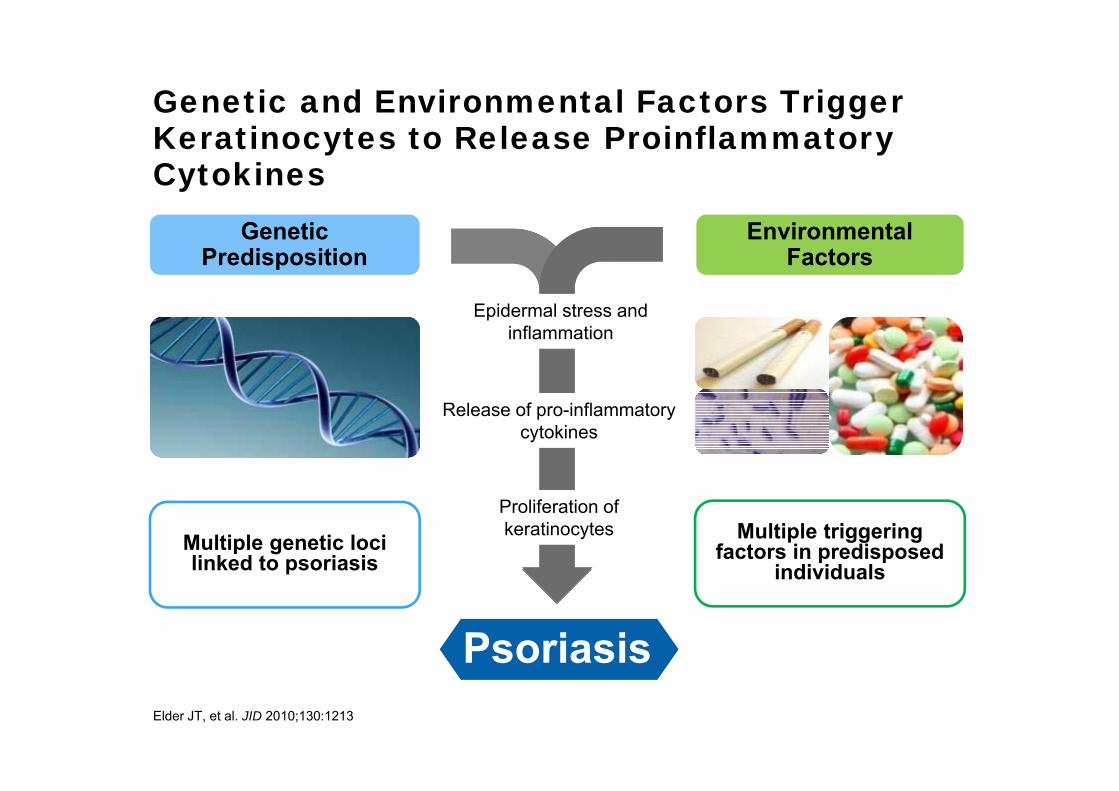
Genetic and Environmental Factors Trigger Keratinocytes to Release ProinflammatoryCytokines
Psoriasis
Environmental Factors
Genetic Predisposition
Release of pro-inflammatory cytokines
Multiple triggering factors in predisposed
individualsMultiple genetic loci linked to psoriasis
Epidermal stress and inflammation
Proliferation of keratinocytes
Elder JT, et al. JID 2010;130:1213
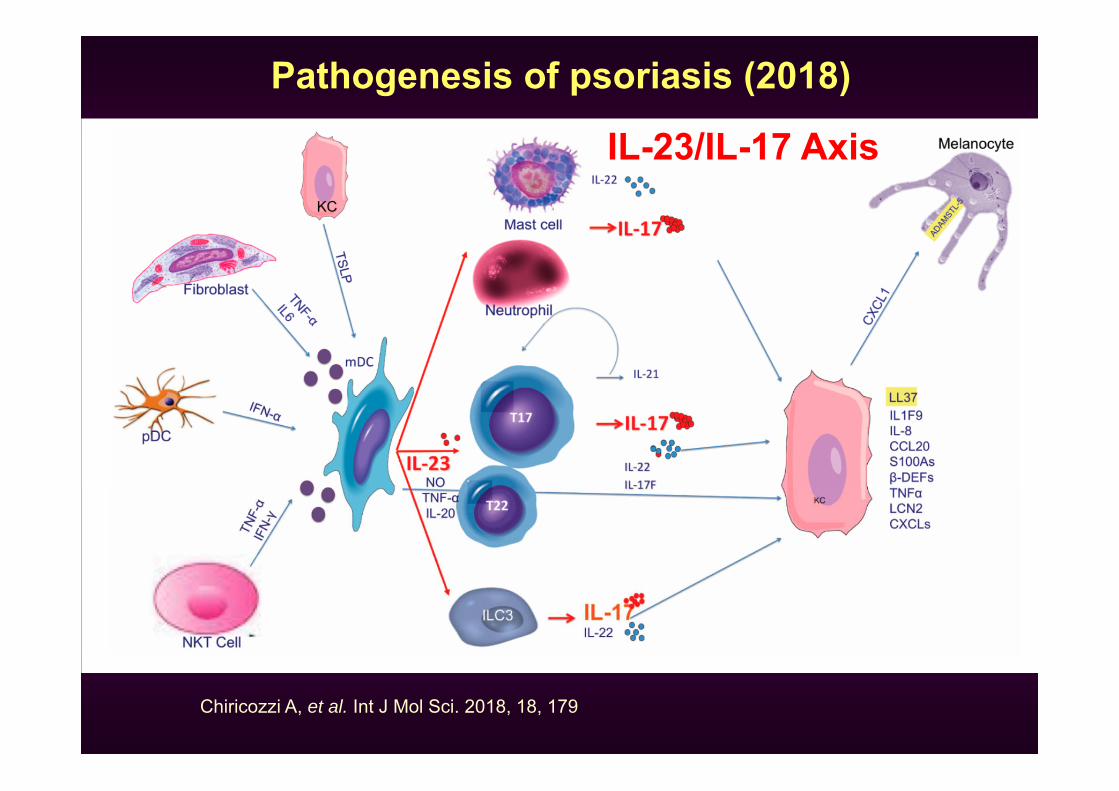
Chiricozzi A, et al. Int J Mol Sci. 2018, 18, 179
Pathogenesis of psoriasis (2018)
IL-23/IL-17 Axis
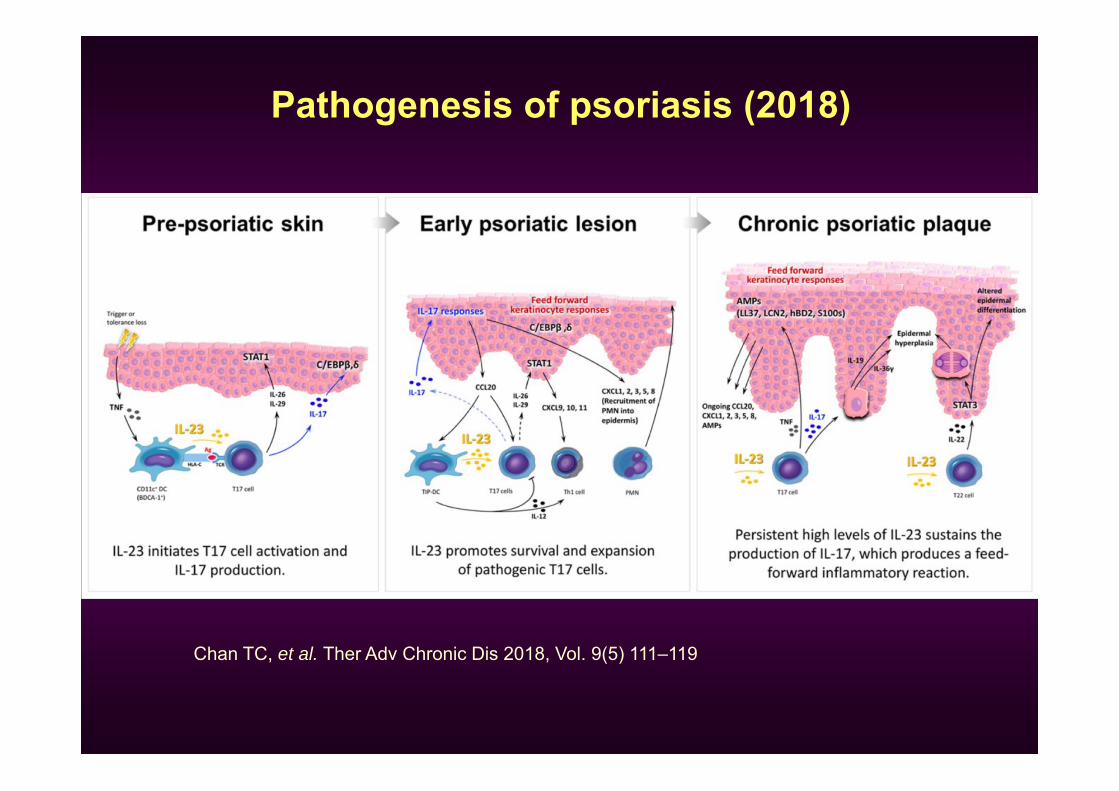
Pathogenesis of psoriasis (2018)
Chan TC, et al. Ther Adv Chronic Dis 2018, Vol. 9(5) 111–119
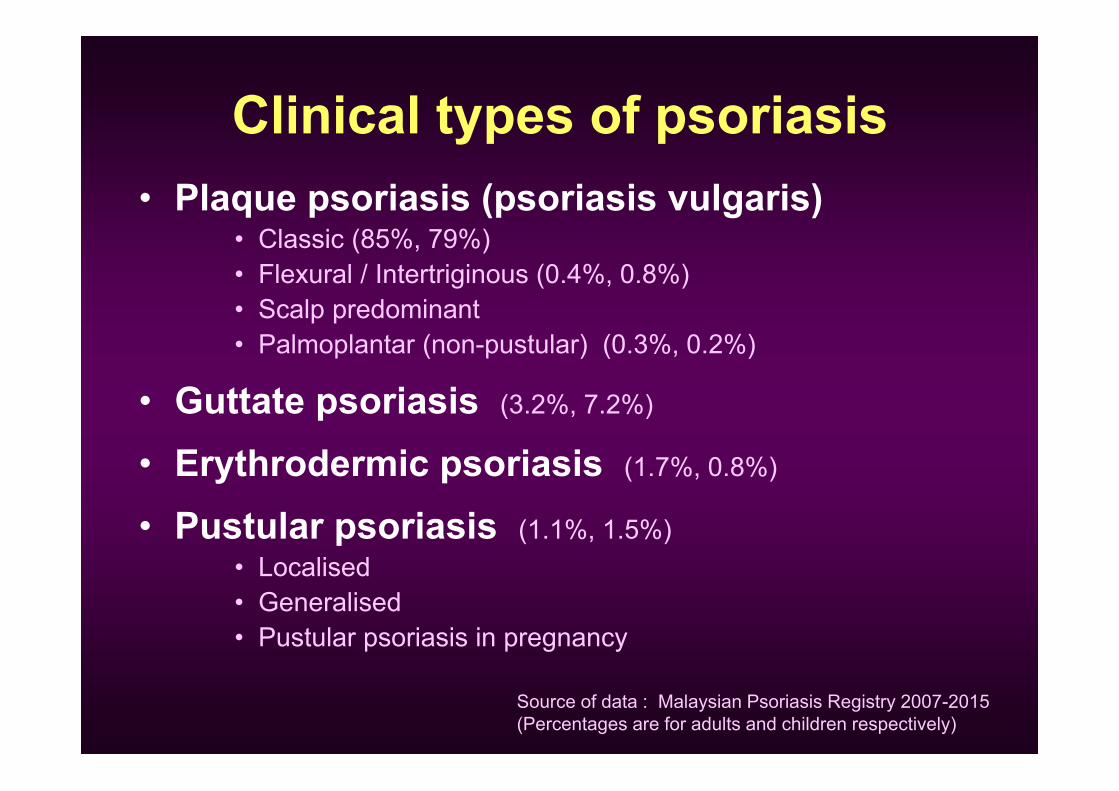
Clinical types of psoriasis• Plaque psoriasis (psoriasis vulgaris)
• Classic (85%, 79%)• Flexural / Intertriginous (0.4%, 0.8%)• Scalp predominant• Palmoplantar (non-pustular) (0.3%, 0.2%)
• Guttate psoriasis (3.2%, 7.2%)
• Erythrodermic psoriasis (1.7%, 0.8%)
• Pustular psoriasis (1.1%, 1.5%)• Localised• Generalised• Pustular psoriasis in pregnancy
Source of data : Malaysian Psoriasis Registry 2007-2015(Percentages are for adults and children respectively)
Malaysian Psoriasis Registry 2007-2015
http://www.acrm.org.my/dermreg/mpr.php
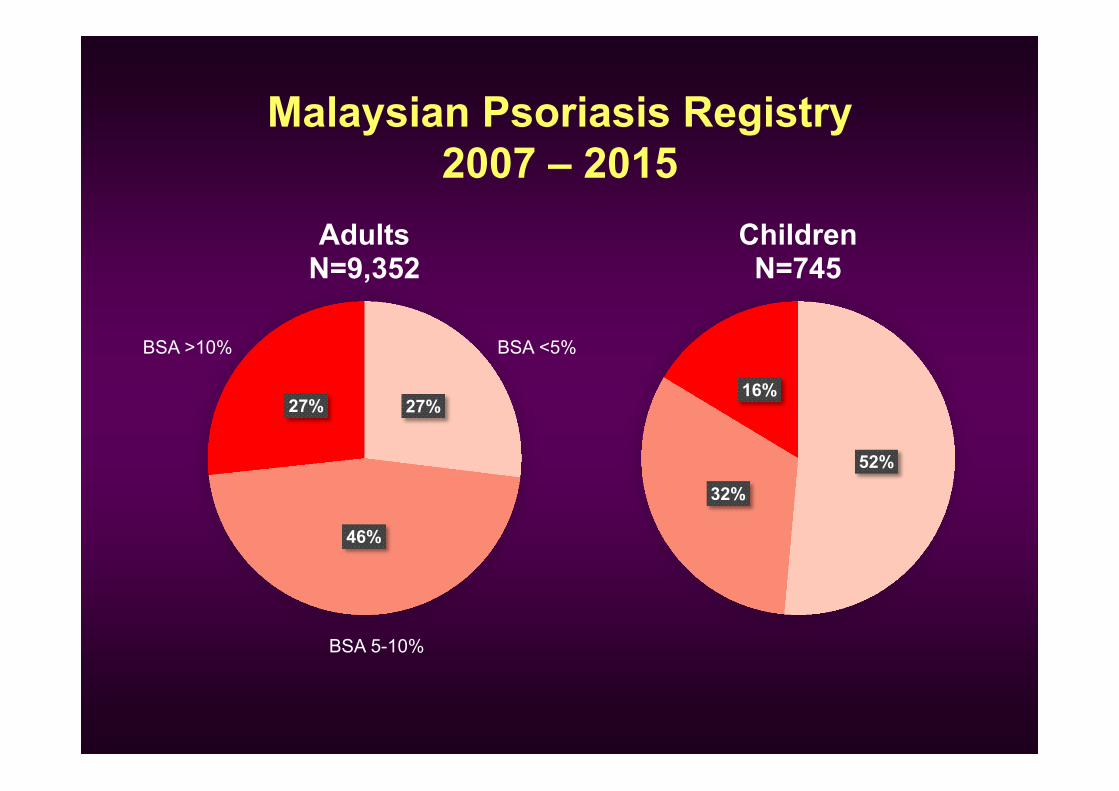
52%
32%
16%
ChildrenN=745
27%
46%
27%
AdultsN=9,352
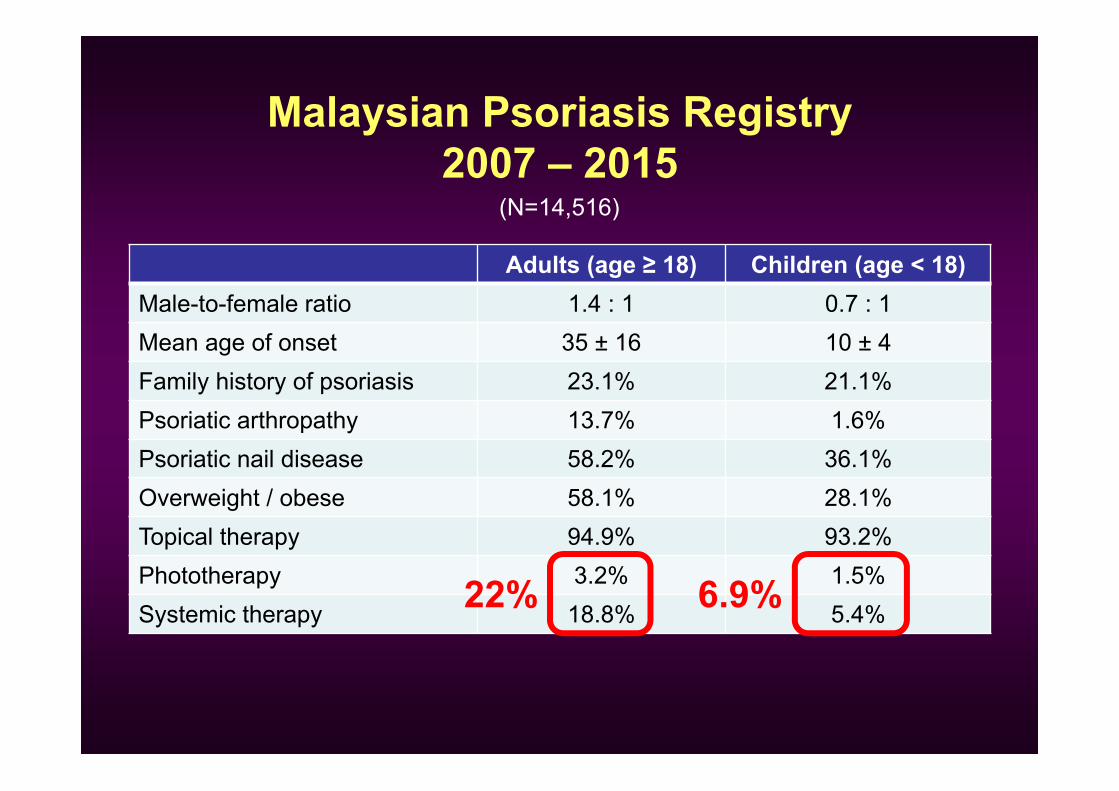
Malaysian Psoriasis Registry2007 – 2015
BSA <5%
BSA 5-10%
BSA >10%
Malaysian Psoriasis Registry2007 – 2015
Adults (age ≥ 18) Children (age < 18)Male-to-female ratio 1.4 : 1 0.7 : 1Mean age of onset 35 ± 16 10 ± 4Family history of psoriasis 23.1% 21.1%Psoriatic arthropathy 13.7% 1.6%Psoriatic nail disease 58.2% 36.1%Overweight / obese 58.1% 28.1%Topical therapy 94.9% 93.2%Phototherapy 3.2% 1.5%Systemic therapy 18.8% 5.4%
(N=14,516)
22% 6.9%
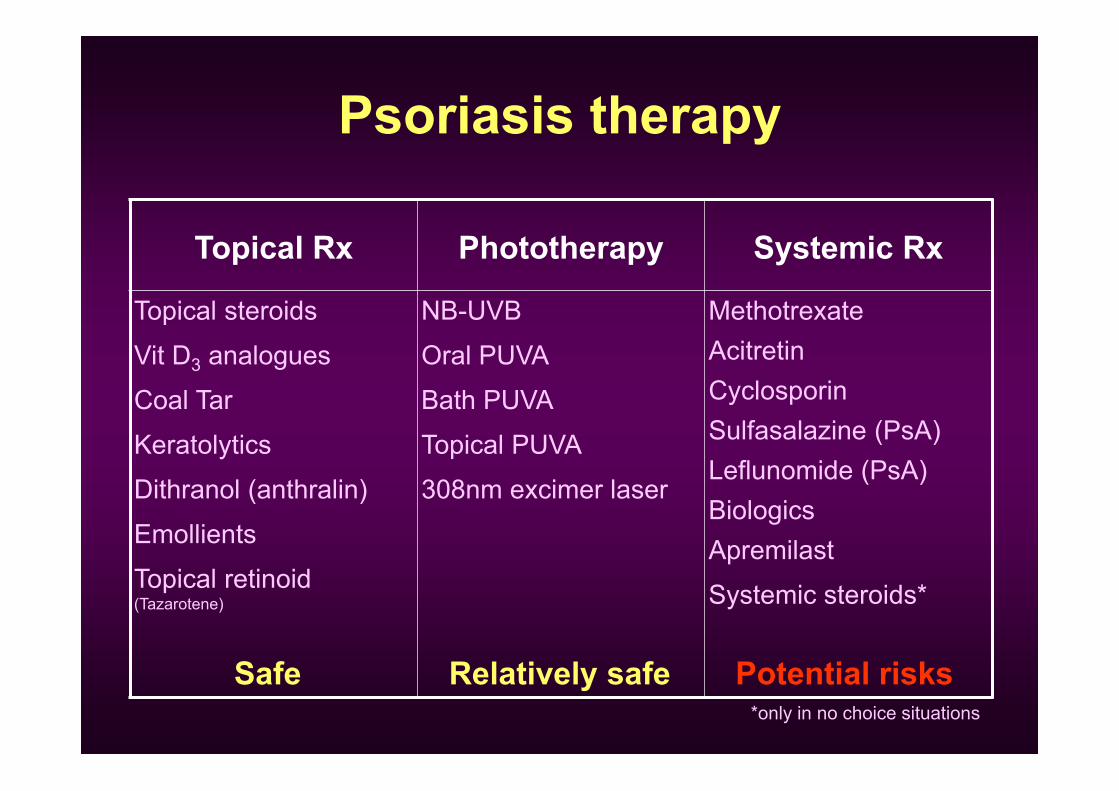
Psoriasis therapy
Topical Rx Phototherapy Systemic Rx
Topical steroidsVit D3 analoguesCoal TarKeratolyticsDithranol (anthralin)EmollientsTopical retinoid(Tazarotene)
NB-UVBOral PUVABath PUVATopical PUVA308nm excimer laser
MethotrexateAcitretinCyclosporinSulfasalazine (PsA)Leflunomide (PsA)BiologicsApremilastSystemic steroids*
Safe Relatively safe Potential risks*only in no choice situations
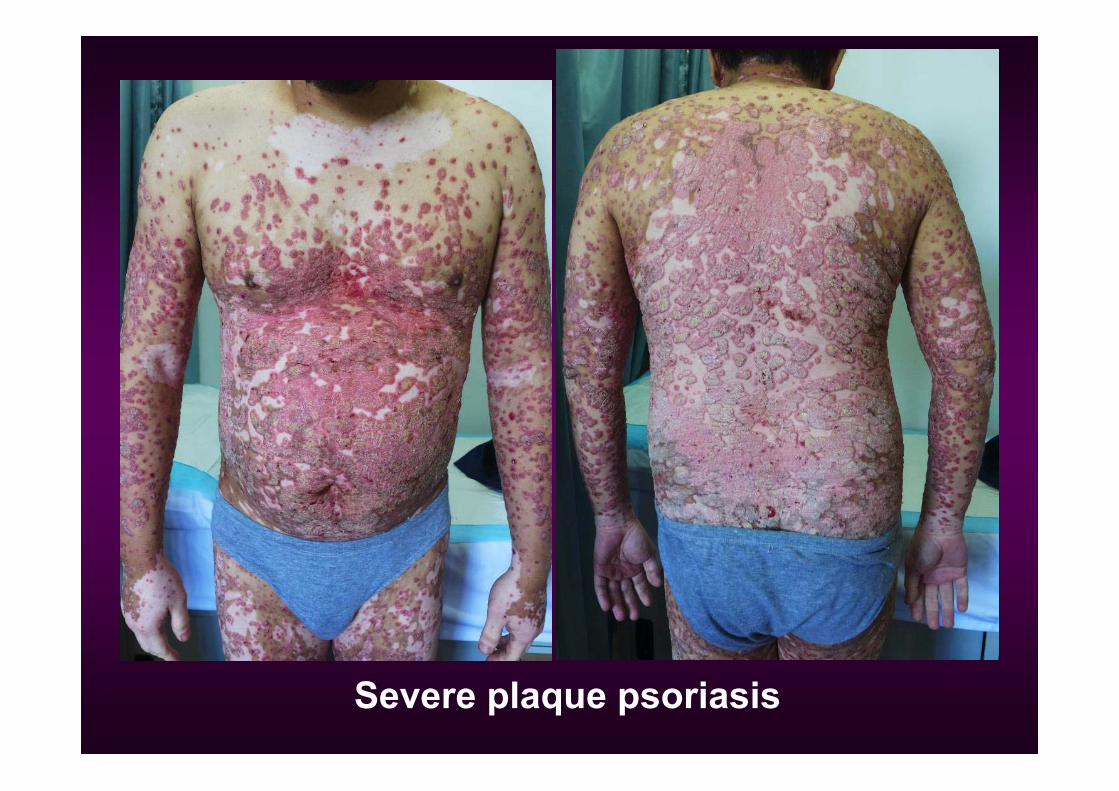
Severe plaque psoriasis
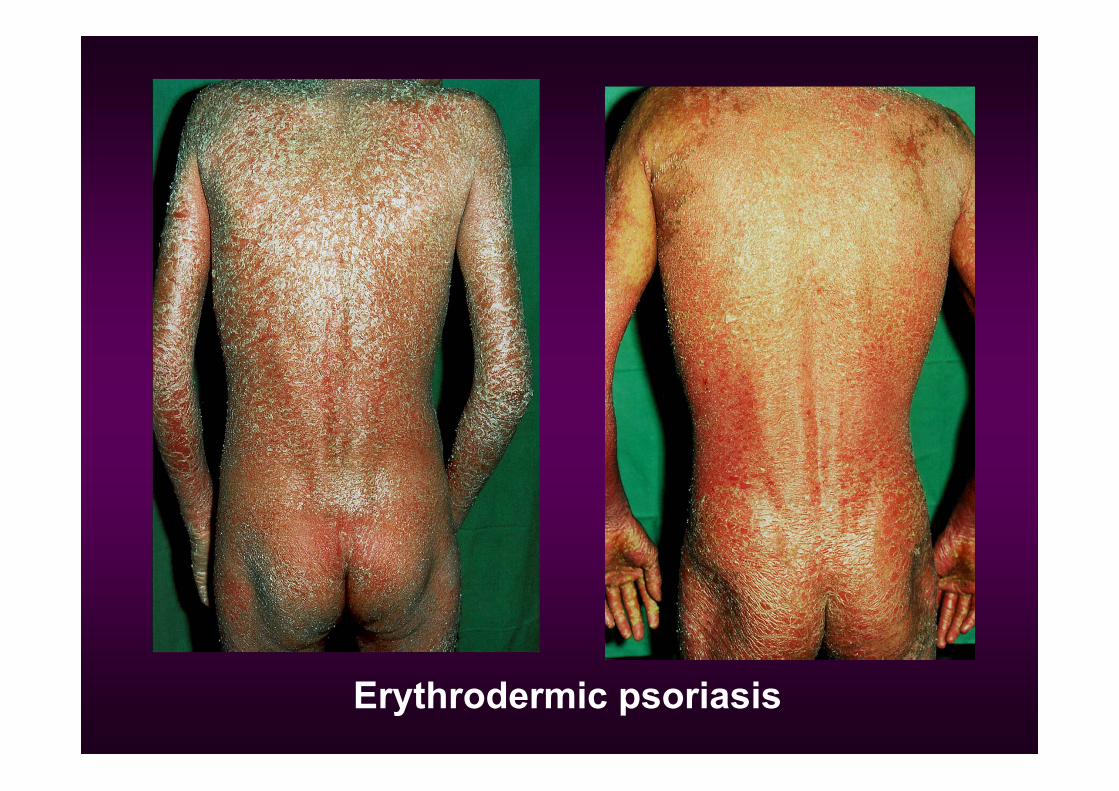
Erythrodermic psoriasis
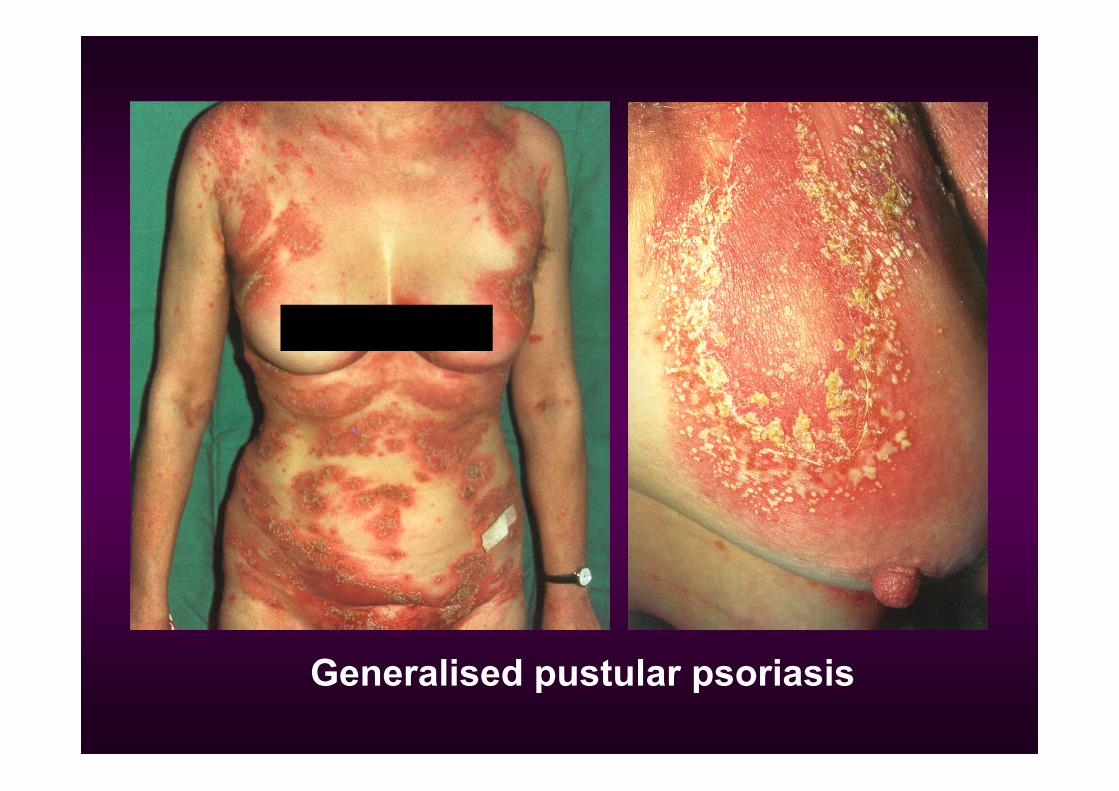
Generalised pustular psoriasis
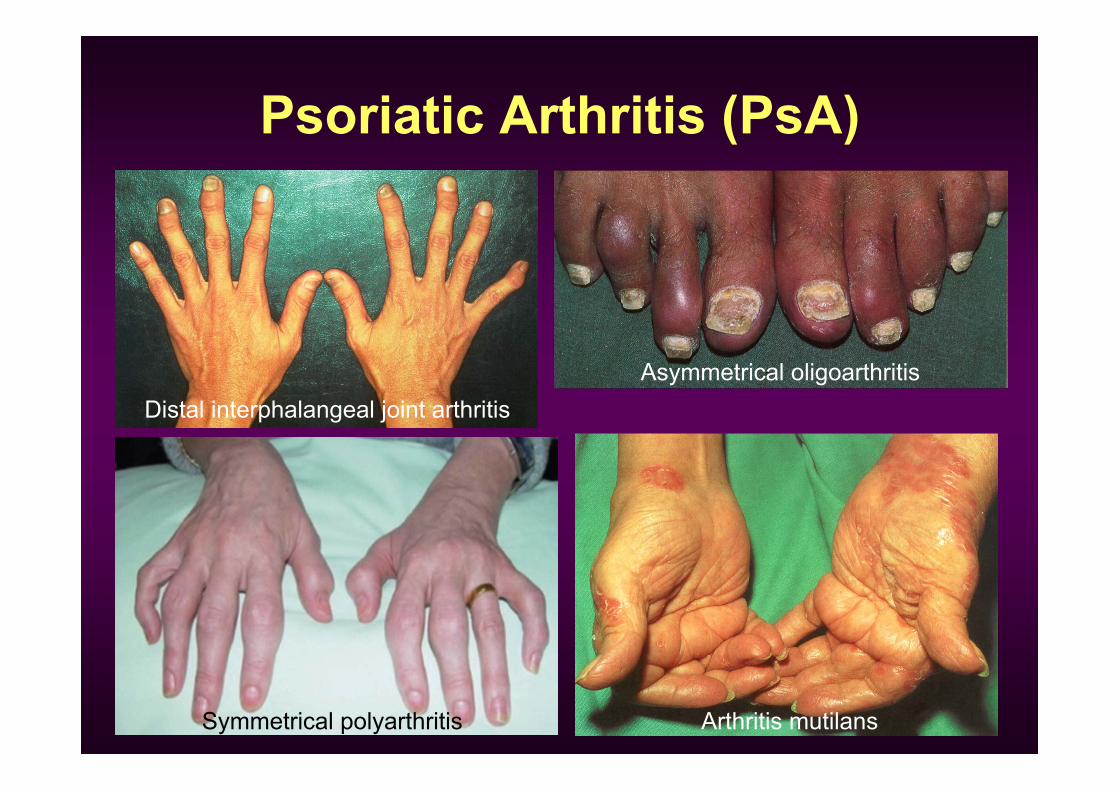
Psoriatic Arthritis (PsA)
Distal interphalangeal joint arthritis
Symmetrical polyarthritis
Asymmetrical oligoarthritis
Arthritis mutilans
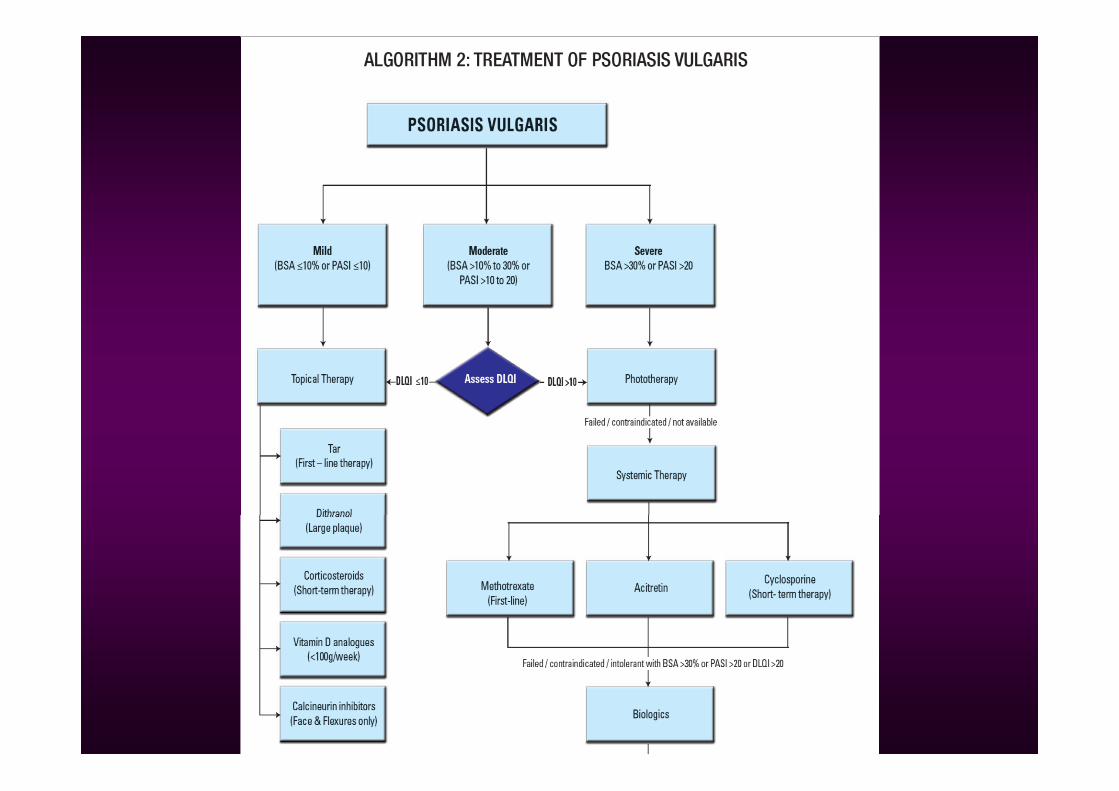
Systemic therapy• Should be considered in patients with
– Moderate and severe plaque psoriasis– Psoriatic arthritis– Erythrodermic psoriasis– Pustular psoriasis
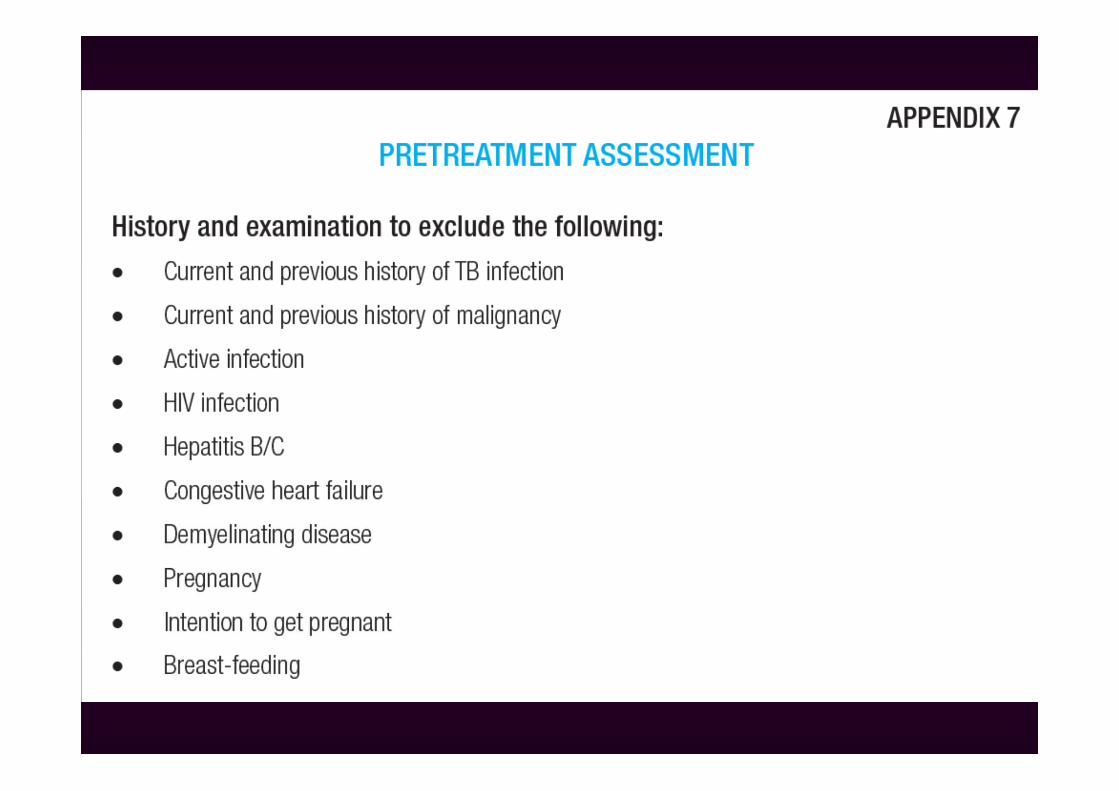
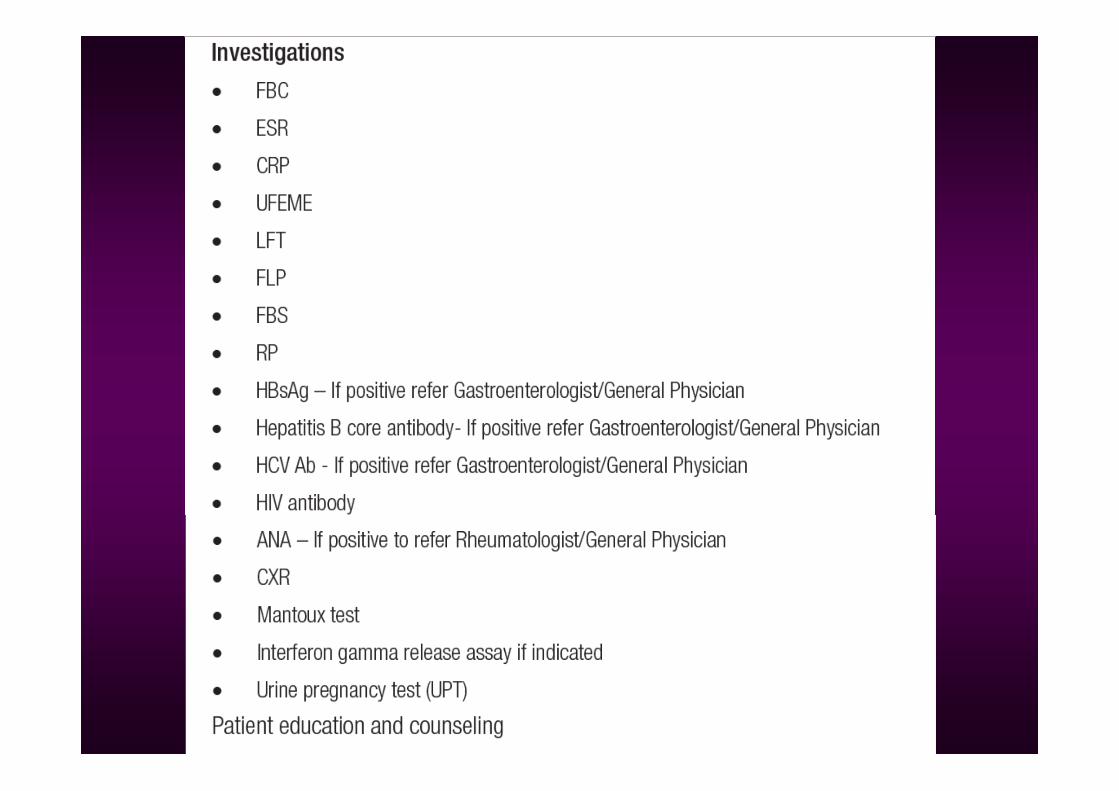
• Patient counselling: indication, options, risks• Pre-treatment assessment• Baseline and regular monitoring
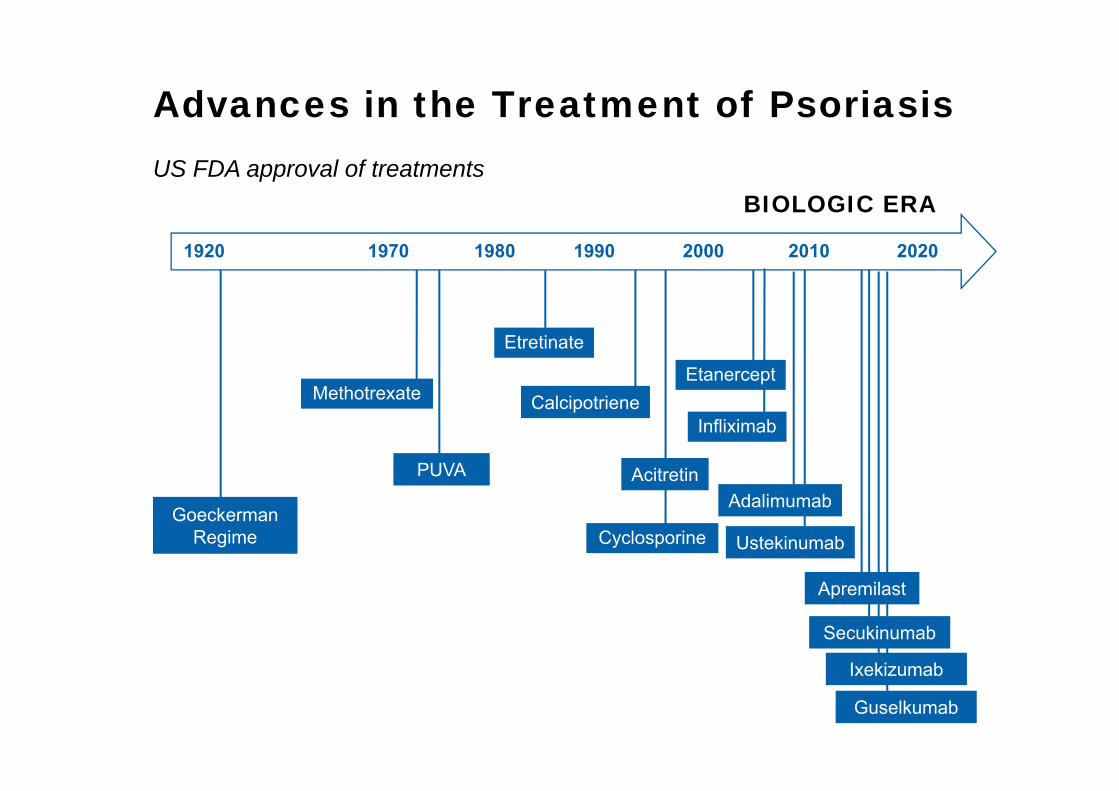
Advances in the Treatment of PsoriasisUS FDA approval of treatments
GoeckermanRegime
Methotrexate
Ustekinumab
Etretinate
Cyclosporine
Calcipotriene
1920 1970 1990 2000 2020
AcitretinPUVAAdalimumab
Infliximab
Etanercept
20101980
Secukinumab
Apremilast
Ixekizumab
Guselkumab
BIOLOGIC ERA
Systemic agentsConventional systemic agents
– Methotrexate (Pso, PsA)– Acitretin (Pso)– Cyclosporin (Pso)– Sulfasalazine (PsA)– Leflunomide (PsA)– Systemic steroids (Pso, PsA)
BiologicsOthers
– Apremilast (Pso, PsA)– Tofacitinib (PsA, Pso)
Factors to considerPatient factors
– Age– Co-morbidities
• CKD, hepatitis, HIV, etc
– Pregnancy– Previous treatment– Financial status
Disease factors– Type of psoriasis– Presence of PsA
Drug factors– Availability– Cost of drug + monitoring– Onset of action– Frequency of dosing– Tolerability– Long term safety– Drug interaction
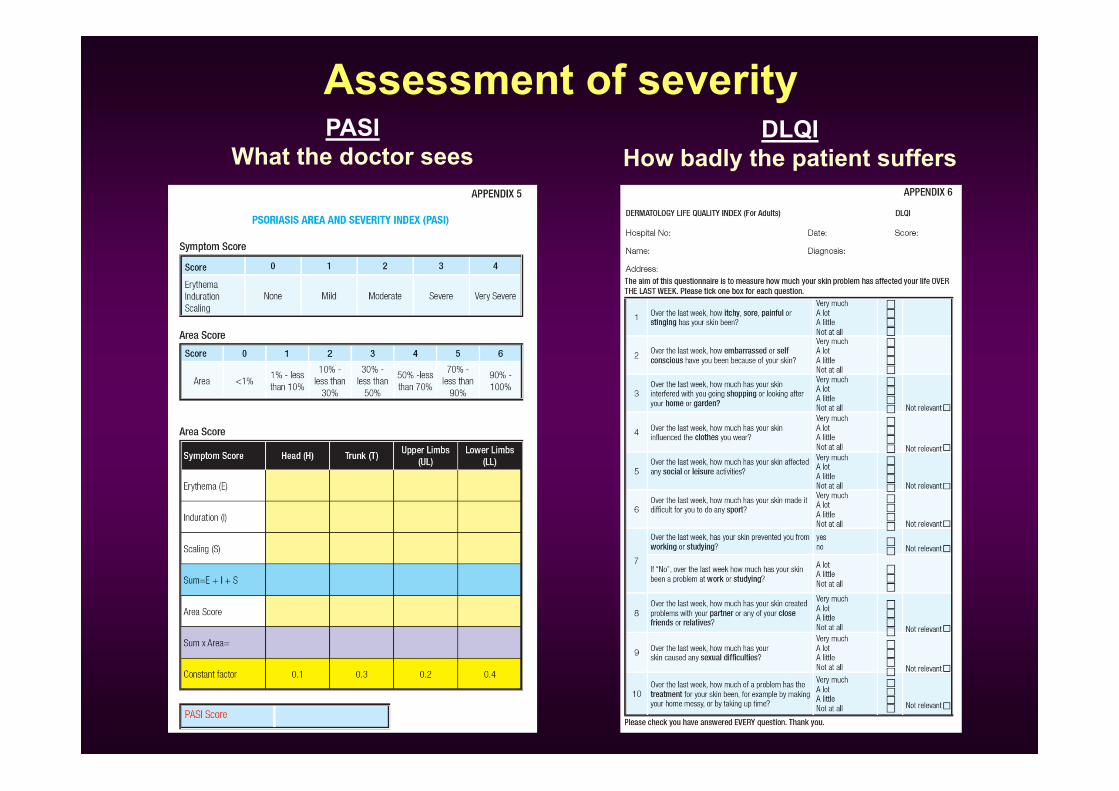
Assessment of severityPASI
What the doctor seesDLQI
How badly the patient suffers
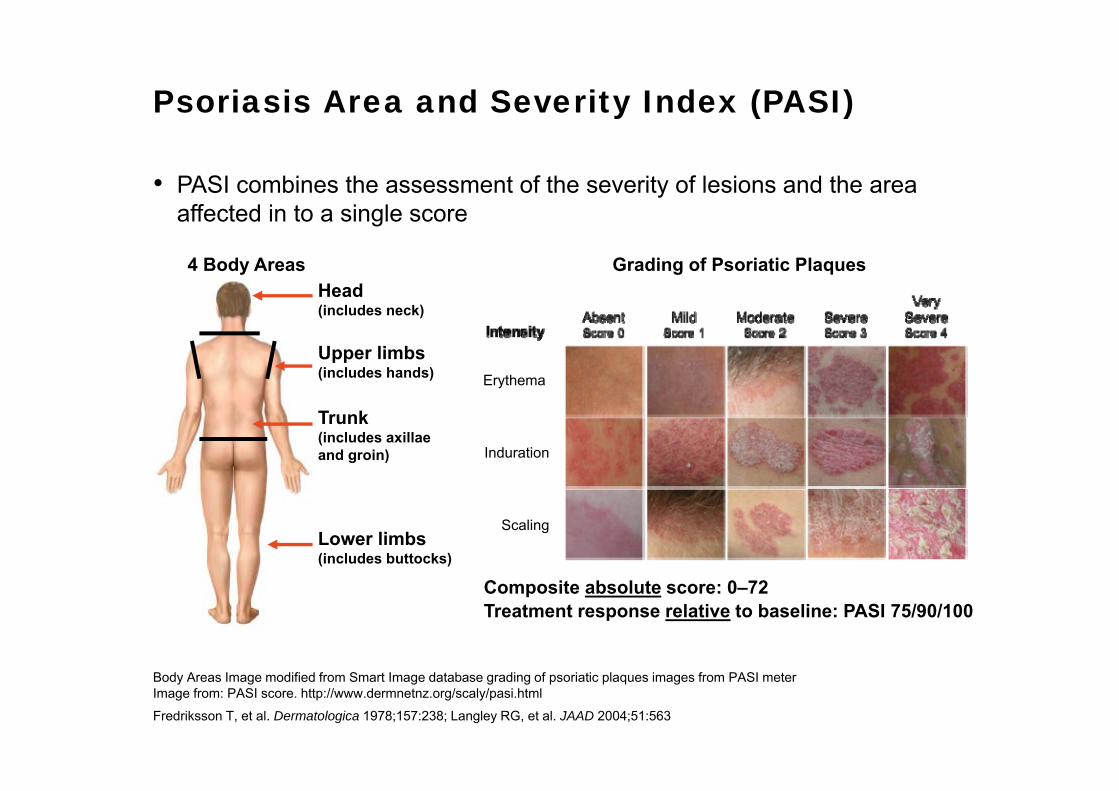
Psoriasis Area and Severity Index (PASI)
• PASI combines the assessment of the severity of lesions and the area affected in to a single score
Head (includes neck)
4 Body Areas Grading of Psoriatic Plaques
Upper limbs (includes hands)
Trunk (includes axillae and groin)
Lower limbs (includes buttocks)
Composite absolute score: 0–72Treatment response relative to baseline: PASI 75/90/100
Erythema
Induration
Scaling
Body Areas Image modified from Smart Image database grading of psoriatic plaques images from PASI meterImage from: PASI score. http://www.dermnetnz.org/scaly/pasi.htmlFredriksson T, et al. Dermatologica 1978;157:238; Langley RG, et al. JAAD 2004;51:563
Body Surface Area (BSA)
• Measurement of involved BSA is estimated by the patient’s handprint (one full palm and fingers = 1% BSA) – Head and Neck = 10% (10 handprints)
– Upper extremities = 20% (20 handprints)
– Trunk (axillae and groin) = 30% (30 handprints)
– Lower extremities (buttocks) = 40% (40 handprints)
– Total BSA = 100% (100 handprints)
Finlay AY. BJD 2005;152:861
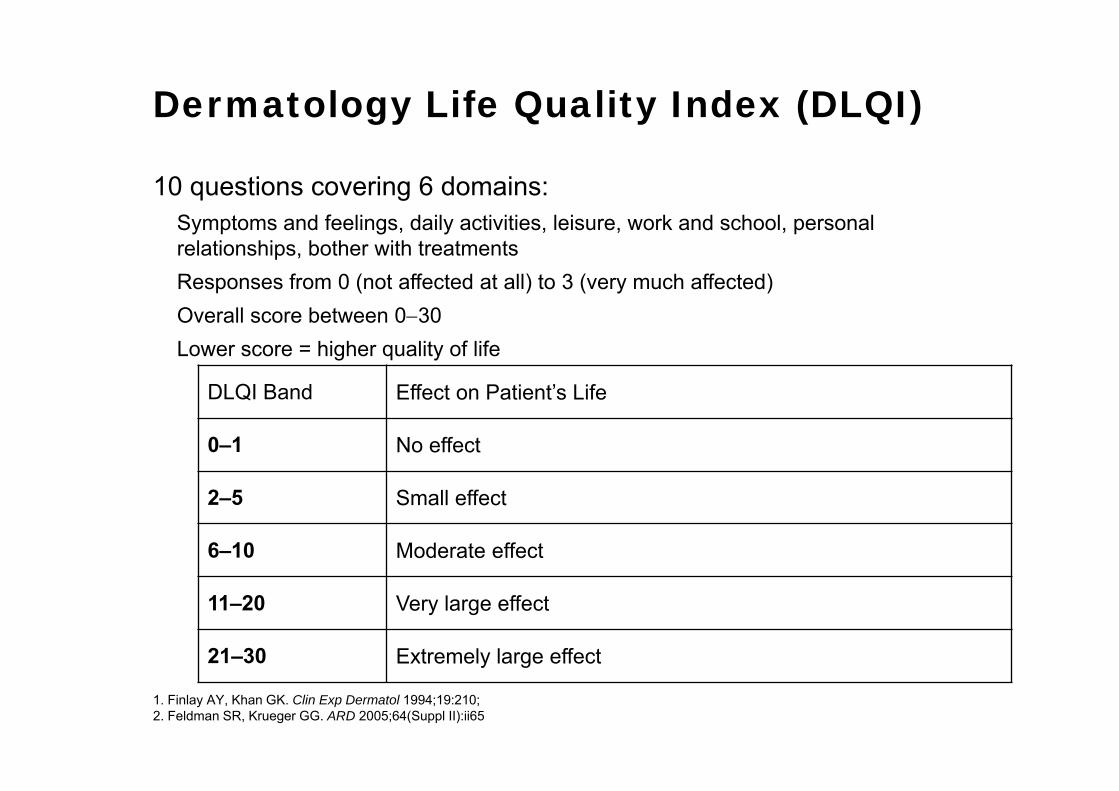
Dermatology Life Quality Index (DLQI)
10 questions covering 6 domains:Symptoms and feelings, daily activities, leisure, work and school, personal relationships, bother with treatmentsResponses from 0 (not affected at all) to 3 (very much affected) Overall score between 030Lower score = higher quality of life
1. Finlay AY, Khan GK. Clin Exp Dermatol 1994;19:210;2. Feldman SR, Krueger GG. ARD 2005;64(Suppl II):ii65
DLQI Band Effect on Patient’s Life
0–1 No effect
2–5 Small effect
6–10 Moderate effect
11–20 Very large effect
21–30 Extremely large effect
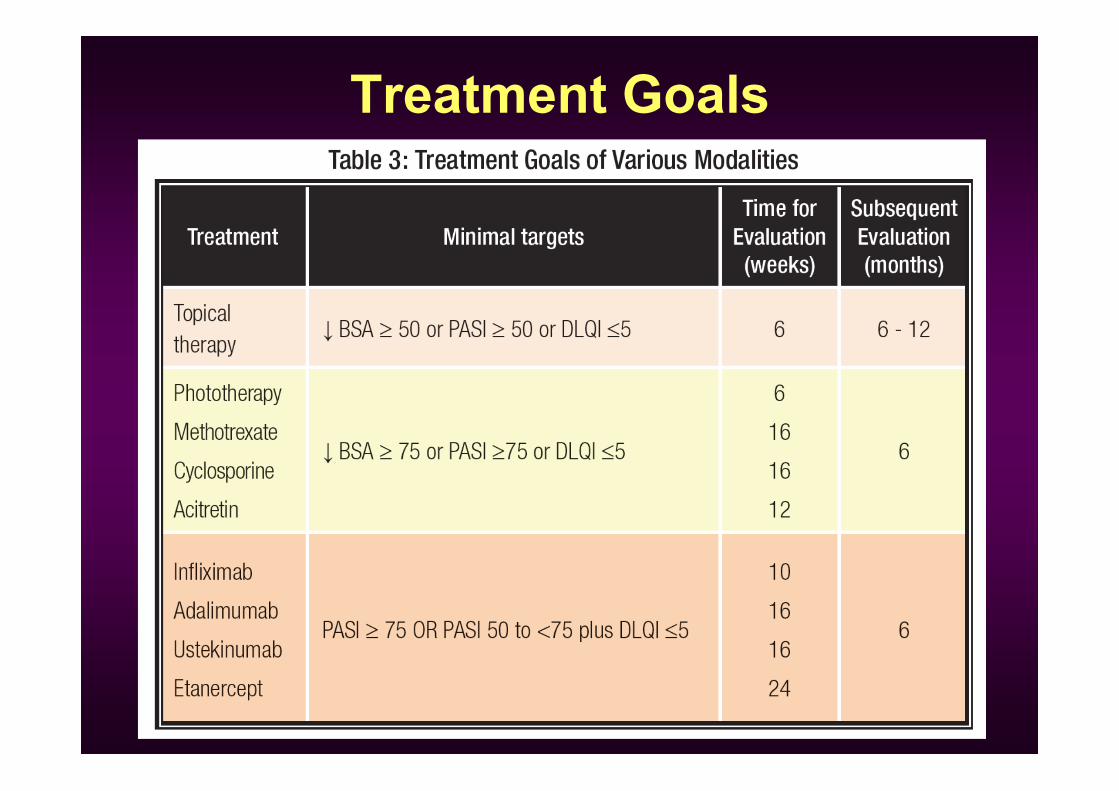
Treatment Goals
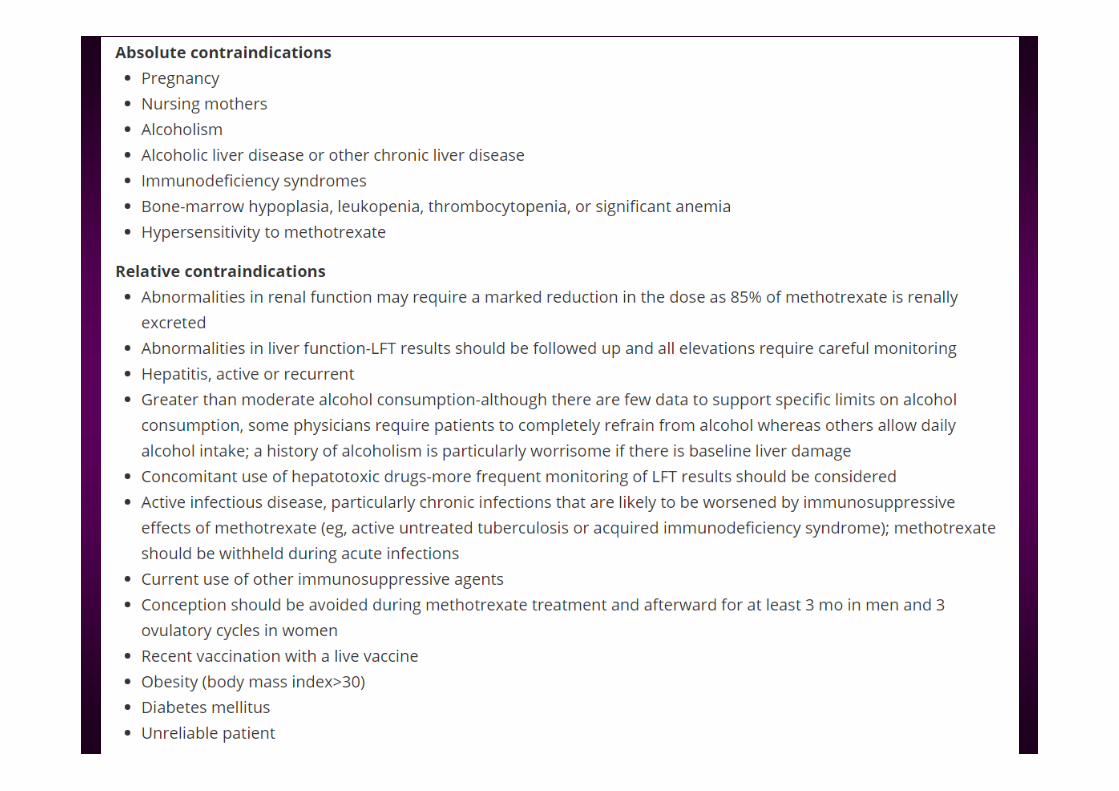
Methotrexate
• First-line systemic treatment for moderate to severe psoriasis
• Inhibit dihydrofolate reductase• Dose: 7.5 – 20 mg/week PO or IM or SC
ONCE WEEKLY DOSING
• Folic acid supplementation recommended
Methotrexate – adverse effects• Gastrointestinal effects
• Nausea, vomiting, diarrhoea, abd pain, GI ulceration
• Liver toxicity• Elevated liver enzymes• Liver fibrosis
– Risk factors: type 2 DM, obesity, NASH, alcohol, hepatitis B or C
• Bone marrow suppression• Risk factors: renal insufficiency, elderly, dosing error, alcohol, drug
interaction, lack of folate supplementation• Monitoring: LFT, procollagen III aminopeptide, Fibroscan, liver
biopsy
• Others: • Malaise, alopecia, photosensitivity, pneumonitis, lung fibrosis