Embed Size (px)
Citation preview
7/17/17
1
ForensicMarijuana:TheScienceofMedical
Cannabinoids
Dr.MerrillNortonPharm.D.,D.Ph.,ICCDP-DClinicalAssociateProfessorofAddictionPharmacyPractice
News MoreAmericansareusingmarijuana,accordingtoanewgovernmentreport.About8.4percentofAmericansages12andolderwerecurrentusersofmarijuanalastyear,upfrom7.5percentin2013.Thepercentageofteensages12to17whosmoke,drinkoruseprescriptionnarcoticsnonmedicallyhasfallen,HealthDayreports.
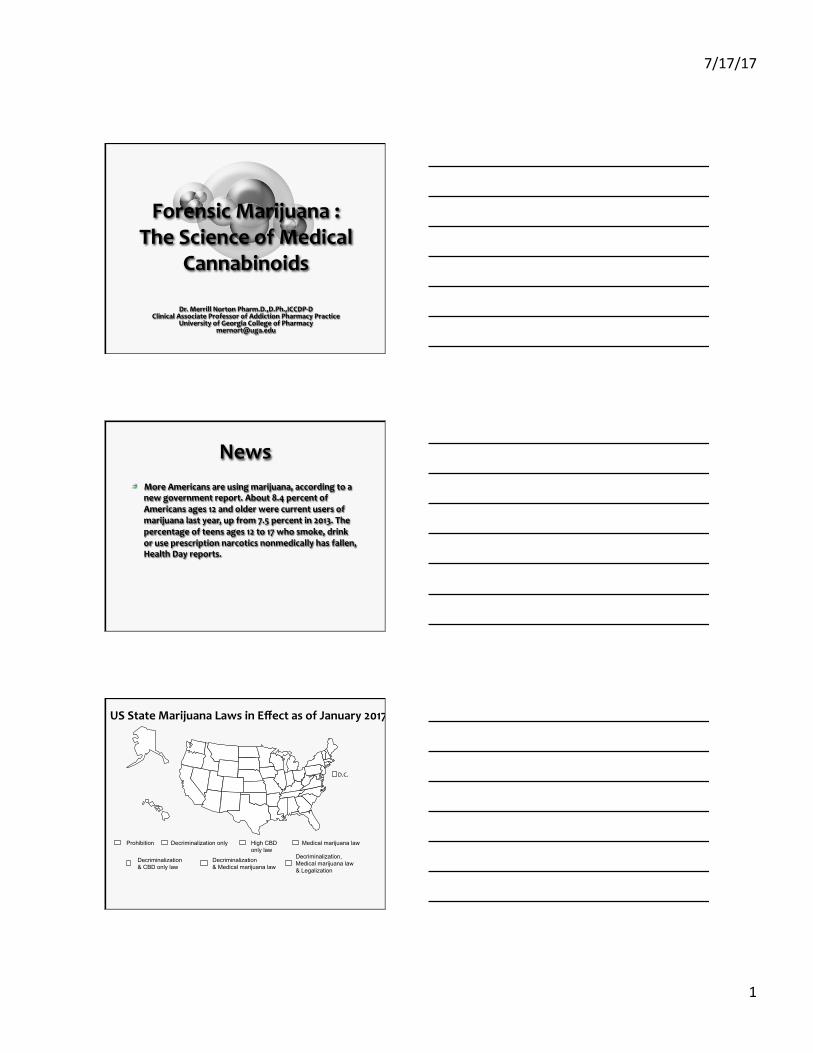
D.C.
Medical marijuana law Decriminalization only
Decriminalization & Medical marijuana law
Decriminalization, Medical marijuana law & Legalization
Decriminalization & CBD only law
High CBD only law
Prohibition
USStateMarijuanaLawsinEffectasofJanuary2017
7/17/17
2
1. Alzheimer'sDisease2. Anorexia3. Arnold-Chiarimalforma9on4. Arthri9s5. Ataxia6. Cachexia7. Cancer8. Cardiopulmonaryrespiratorysyndrome9. Causalgia10. Cervicaldystonia11. Crohn'sdisease12. Decompensatedcirrhosis13. Dystonia14. Epilepsy15. Fibromyalgia16. Glaucoma17. Hepa99sC18. HIV/AIDS19. Hun9ngton’sdisease20. Hydrocephalus21. Inflammatoryautoimmune-mediatedarthri9s22. Inflammatoryboweldisease(IBS)23. Inflammatorydemyelina9ngpolyneuropathy24. Inters99alcys99s25. LouGehrig’sdisease(amyotrophiclateralsclerosis,
ALS)
26. Lupus27. Migraines28. Mul9pleSclerosis29. Musclespasms30. Musculardystrophy31. Myastheniagravis32. Myoclonus33. Nail-patellasyndrome34. Nauseaorvomi9ng35. Neurofibromatosis36. Neuropathy37. Pain38. Pancrea99s39. Parkinson'sdisease40. Peripheralneuropathy41. Post-trauma9cstressdisorder(PTSD)42. Reflexsympathe9cdystrophy43. Residuallimbpainfromamputa9on44. Seizuredisorders45. Sjogren'ssyndrome46. Spas9city47. Spinalcorddamagewithintractablespas9city48. Syringomyelia49. Terminalillness50. Toureae’ssyndrome51. Trauma9cbraininjury
51MedicalCondi9onsForWhichMarijuanaIsApprovedbyaState
Sources:MarijuanaPolicyProject,2014.KeyAspectsofStateandD.C.MedicalMarijuanaLaws,fromNa9onalConferenceofStateLegislatures,“StateMedicalMarijuanaLaws,”www.ncsl.org.;Rahn,B.,2014.QualifyingCondi9onsforMedicalMarijuanabyState,www.Leafly.com
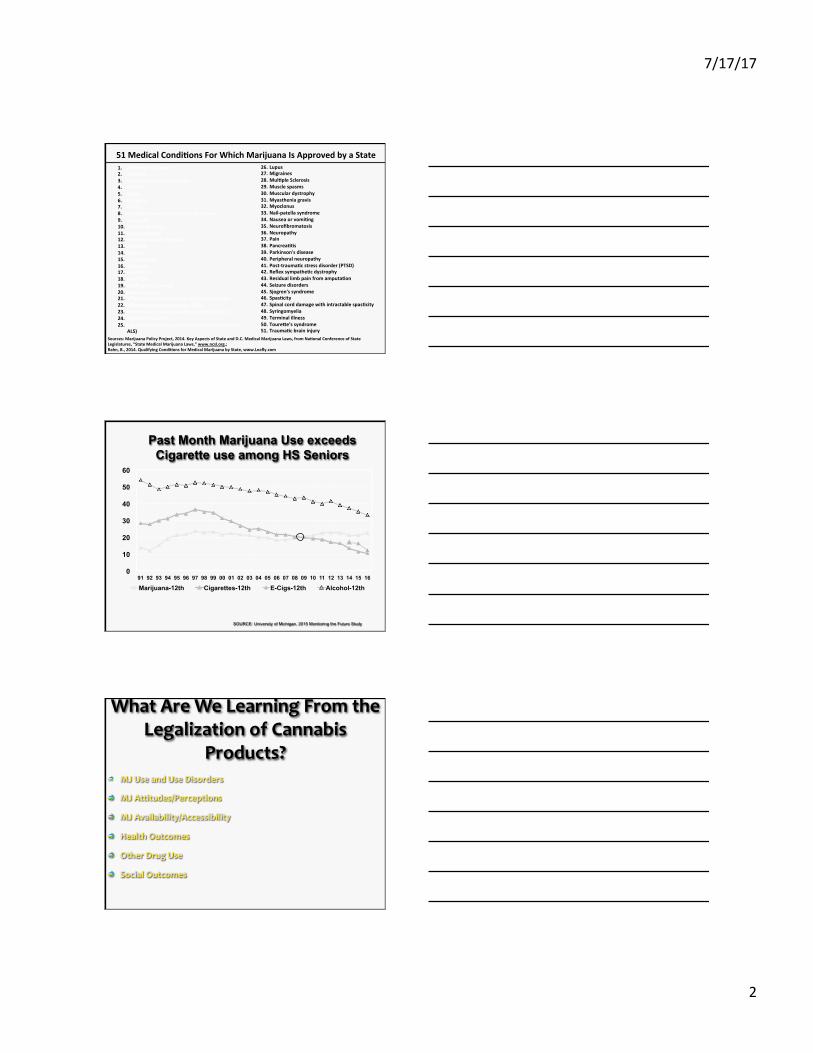
Past Month Marijuana Use exceeds Cigarette use among HS Seniors
0
10
20
30
40
50
60
91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16
Marijuana-12th Cigarettes-12th E-Cigs-12th Alcohol-12th
SOURCE: University of Michigan, 2015 Monitoring the Future Study
WhatAreWeLearningFromtheLegalizationofCannabis
Products? MJUseandUseDisorders
MJAttitudes/Perceptions
MJAvailability/Accessibility
HealthOutcomes
OtherDrugUse
SocialOutcomes
7/17/17
3
MJUseandUseDisorders(1) USE:
Adolescents-MJuseremainedconsistentwhileuseofotherdrugs,alcoholandtobaccodeclined
Adults-IncreasesinMJusebetween2001and2013 ParentcurrentMJuseincreasedlikelihoodofchildpastyearMJuse
CannabisUseDisorders: DensityofdispensariesrelatedtohigherratesofMJabuseanddependence
BUT:80%medicalMJpatientsusedailywithoutcannabisusedisordersymptoms
MJUseandUseDisorders(2)
Producttypesandmethods: MMJconsumersusedifferentlythanrecreationalconsumers Smokingisstillpredominantmethodinyouth,butMMJstatesmorelikelytoconsumeinfoodorotherwaysthannon-MMJstates
SocialmediaissourceofinformationaboutnovelformsofMJ–e.g.YouTubevideosofdabbing
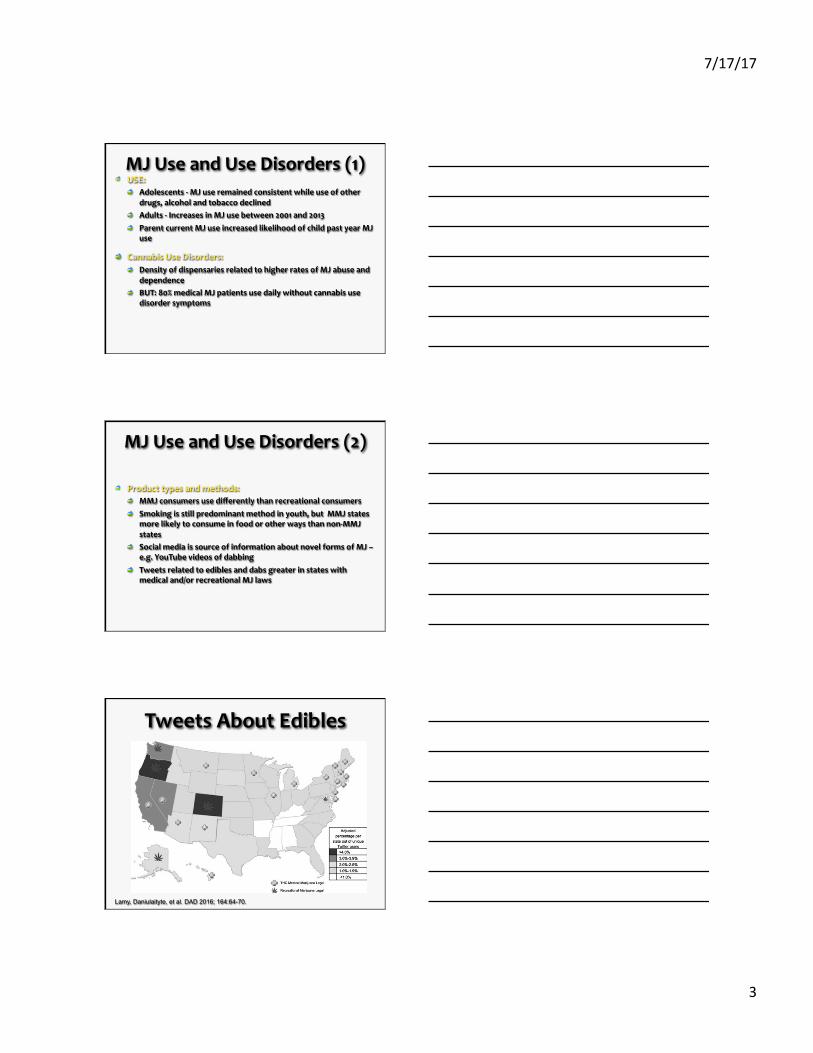
Tweetsrelatedtoediblesanddabsgreaterinstateswithmedicaland/orrecreationalMJlaws
TweetsAboutEdibles
Lamy, Daniulaityte, et al. DAD 2016; 164:64-70.
7/17/17
4
MJAttitudesandPerceptions
MMJlawsnotassociatedwithincreasesinMMJstates,howeverlegislationmaymorebroadlyimpactperceptionsofharm
Evenamongparentusers,strongoppositiontoteenuse
0
20
40
60
75 77 79 81 83 85 87 89 91 93 95 97 99 01 03 05 07 09 11 13 15
Past Year Use Perceived Risk
SOURCE: University of Michigan, 2016 Monitoring the Future Study
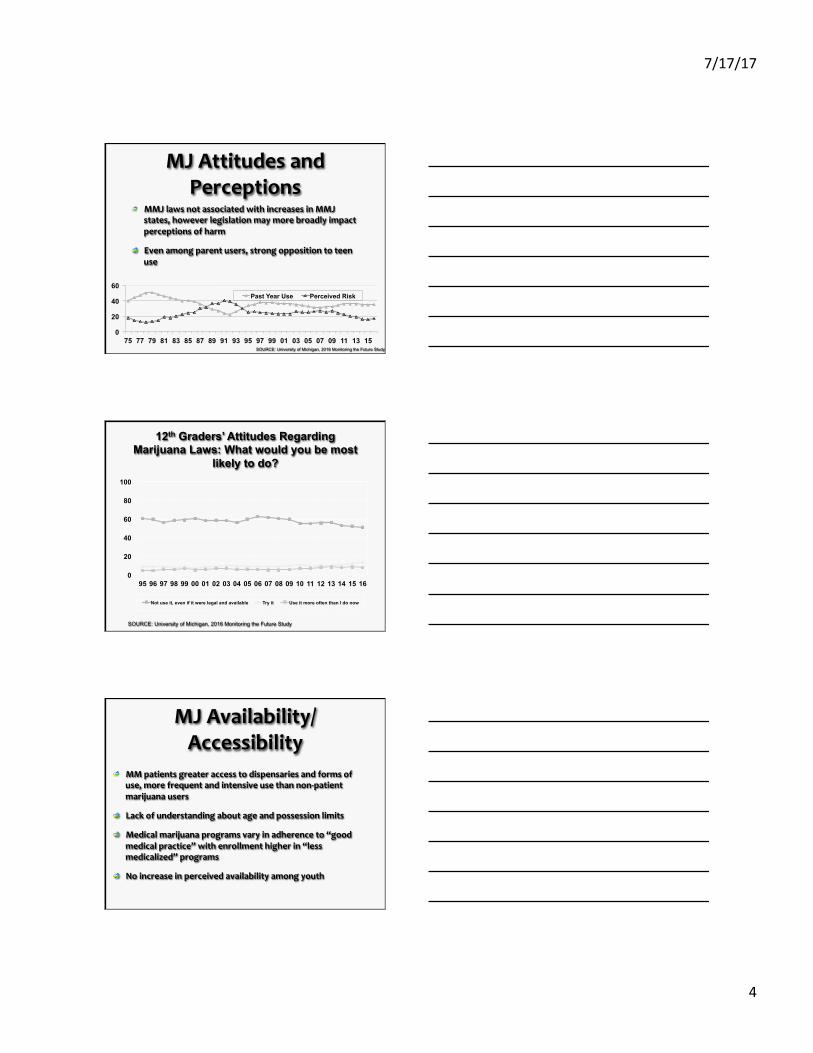
12th Graders’ Attitudes Regarding Marijuana Laws: What would you be most
likely to do?
0
20
40
60
80
100
95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16
Not use it, even if it were legal and available Try it Use it more often than I do now
SOURCE: University of Michigan, 2016 Monitoring the Future Study
MJAvailability/Accessibility
MMpatientsgreateraccesstodispensariesandformsofuse,morefrequentandintensiveusethannon-patientmarijuanausers
Lackofunderstandingaboutageandpossessionlimits
Medicalmarijuanaprogramsvaryinadherenceto“goodmedicalpractice”withenrollmenthigherin“lessmedicalized”programs
Noincreaseinperceivedavailabilityamongyouth
7/17/17
5
HealthOutcomes
IncreaseinMJdependenthospitaldischargesandpoisoncentercalls
MedicalMJpatientsreportedreasonsforMJuseassleep,anxiety,pain
PersistentMJuseinyoungadulthoodpositivelyassociatedwithgeneralizedanxietydisorder,substanceuse(incl.alcoholandtobacco)disorders
OtherDrugUse Alcohol:
Evidenceofbothsubstitutionandcomplementarity Concurrentusemorecommonamongrecreationalusersandsomewhatrareamongmedicalusers
Tobacco: TeensmokingpredictedlaterMJuse
RxOpioids: Trendstowardslessmisuseofprescriptionopioids
SocialOutcomes Densityofdispensariesrelatedtohigherviolentandpropertycrime,childneglectandabuse
EarlyadolescentuseofMJassociatedwithlowereducationandeconomicoutcomes
Driving/ridingafterMJusecommoninunderageMJ-usingcollegestudents
7/17/17
6
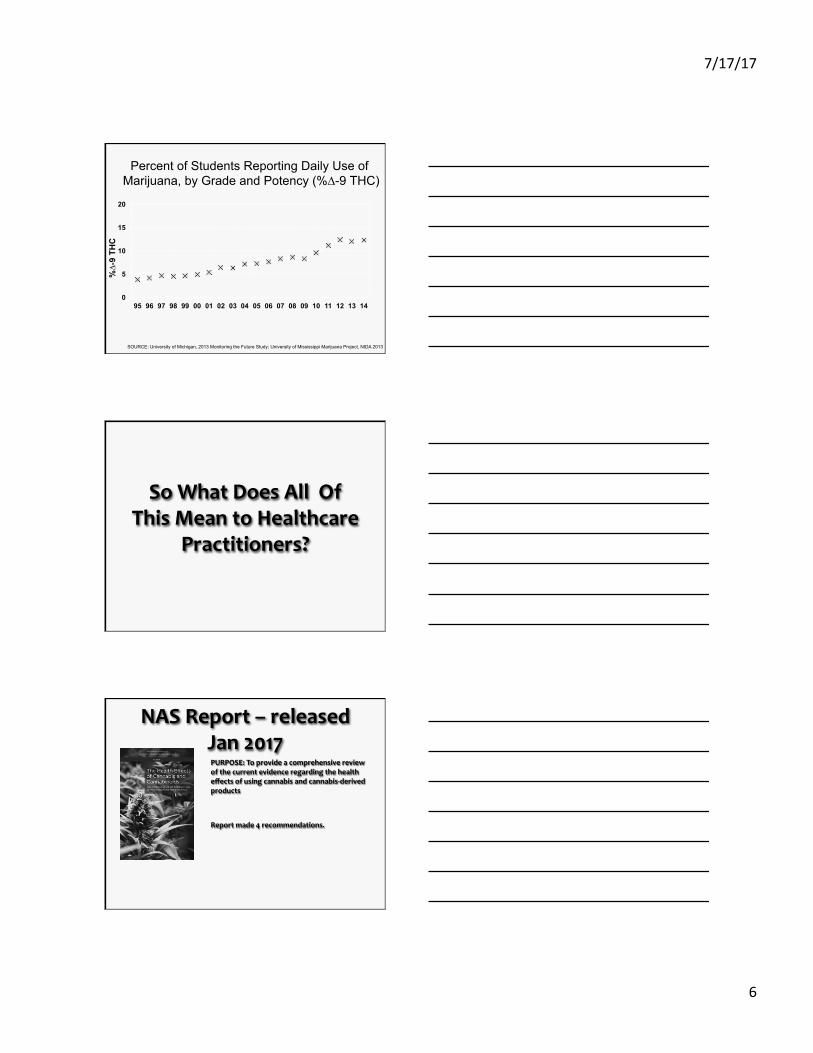
Percent of Students Reporting Daily Use of Marijuana, by Grade and Potency (%∆-9 THC)
0
5
10
15
20
95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14
%∆-
9 TH
C
SOURCE: University of Michigan, 2013 Monitoring the Future Study; University of Mississippi Marijuana Project, NIDA 2013
SoWhatDoesAllOfThisMeantoHealthcare
Practitioners?
NASReport–releasedJan2017
PURPOSE:Toprovideacomprehensivereviewofthecurrentevidenceregardingthehealtheffectsofusingcannabisandcannabis-derivedproducts
Reportmade4recommendations.
7/17/17
7
1.AddressResearchGaps
Examinehealtheffectsofcannabisinat-riskorunder-researchedpopulations(e.g.youth,elderly,pregnant/breastfeedingwomen)
Determinebenefits&harmsassociatedwithunderstudiedMJproducts(e.g.edibles,topicals)
Investigateeconomicimpactofrecreational/medicalMJusonhealthcaresystems,healthinsuranceproviders,&patients
2.ImproveResearchQuality
Developminimumdatasetforobservational&clinicalstudies,standardsforresearchmethods&designs,guidelinesfordatacollectionmethods
AdaptexistingresearchreportingstandardstoneedsofMJresearch
Developuniformterminologyforclinical&epidemiologicalMJresearch
Developstandardized&evidence-basedquestionbanksforclinicalresearch&publichealthsurveillancetools
3.ImproveSurveillanceCapacity
Developquestionbanksonbeneficial&harmfuleffectsoftherapeutic&recreationalMJuse&incorporatethemintomajorpublichealthsurveyssuchasNHANES,NHIS,BRFSS,NSDUH,YRBS,NVSS,MEPS,NSFG
StrategiesforsurveillanceofharmfuleffectsofMJfortherapeuticuse
Developnoveldiagnostictechnologiesforrapid,accurate,non-invasiveassessmentofMJexposure&impairment.

7/17/17
8
4.AddressResearchBarriers
Proposestrategiesforexpandingaccesstoresearch-gradeMJ
Identifynontraditionalfundingsources&mechanismstosupportcomprehensivenationalMJresearchagenda
Investigatestrategiesforimprovingquality,diversity,&externalvalidityofresearch-gradeMJproducts
PhysicianPrescribingBackground
TheHealthEffectsofCannabisandCannabinoids:TheCurrentStateofEvidenceandRecommendationsforResearch
440pages|6x9|PAPERBACK
ISBN978-0-309-45304-2|DOI:10.17226/24625
CommitteeontheHealthEffectsofMarijuana:AnEvidenceReviewandResearchAgenda;BoardonPopulationHealthandPublicHealthPractice;HealthandMedicineDivision;NationalAcademiesofSciences,Engineering,andMedicine
TheHealthEffectsofCannabisandCannabinoids:TheCurrentStateofEvidenceandRecommendations
forResearch(2017)
TheNationalAcademiesofSciences,Engineering,andMedicine(theNationalAcademies)willappointanadhoccommitteetodevelopacomprehensive,in-depthreviewofexistingevidenceregardingthehealtheffectsofusingmarijuanaand/oritsconstituents.
Thecommitteewilldevelopaconsensusreportwithtwoprimarysections:(1)asectionofthereportwillsummarizewhatcanbedeterminedaboutthehealtheffectsofmarijuanauseand,(2)asectionofthereportwillsummarizepotentialtherapeuticusesofmarijuana.
7/17/17
9
The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and
Recommendations for Research (2017)
Aftercarefulconsideration,thecommitteechosenottoattempttoreviewbasic,non-humanresearchinordertoattempttobolsterevidenceforidentifiedhealthoutcomesfromcannabisexposure.
Giventhemethodologicvariationinthestudiesreviewed,aswellaspotentialdeficienciesinstudydesignandexecution,thecommitteefocuseditsattentionandenergyonidentifyinghighqualitystudieswiththebestinformationandlowestriskofbiasasthewaytoensurethatreportfindingsandconclusionswereasinformativeandrelevantaspossible.
The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and
Recommendations for Research (2017)
Exposuremeasurementisalwaysanadditionalconcernwhenevaluatingcomprehensivereviewsofobservationalstudies.
Assessmentofcannabisexposureisparticularlychallengingbecauseofitsillegalstatus(inmostsettings)andtherelianceonself-report.Inherentdifficultiesinaccuratelyassessingtheexposureintermsofdose,specifictypeofcannabisproductused,modeofintake,duration,frequency,andothervariablesresultinthevariabilityindefinitionsusedtooperationalizecannabisexposure.
Riskofpolysubstanceuse
GUIDELINESONPRESCRIBINGMARIJUANA
TheFederationofStateMedicalBoards(September2016)recommendationssetforthsomebasicgroundrulesfordoctorswhochoosetoprescribeormakeareferralformedicalmarijuana:
•Thedoctorshouldadheretocurrentstandsofpracticeandcomplywithstatelaws,rulesandregulations,whichmayspecifyconditionsforwhichapatientmayquality.
•Thedoctor’sofficeshouldnotbelocatedatamarijuanadispensaryorcultivationcenter.Thedoctorshouldnotreceivefinancialcompensationfromorholdafinancialinterestinmarijuana-relatedbusinessesorbeaffiliatedwiththeminanyway.
•Thephysicianshouldnotusemarijuanaeithermedicinallyorrecreationallywhileactivelyengagedinthepracticeofmedicine.
Fitzgerald,S.NationalBoardOffersGuidanceforDoctorsPrescribingMedicalMarijuana,NeurologyToday;September22,2016
7/17/17
10
GUIDELINESONPRESCRIBINGMARIJUANA
Therecommendationsalsofocusonspecificsoftheofficevisit:
Thereshouldbeanestablisheddoctor-patientrelationshipbeforethedoctorconsiderstheuseofmedicalmarijuana.
•Thedoctorshoulddoaphysicalexamandgatherhealthhistory,includingdocumentationofprevioustherapiesusedbythepatientandinformationonanypersonalorfamilyhistoryofsubstanceabuse,mentalillnessorpsychoticdisorders.
Thediagnosisshouldjustifytheconsiderationofmedicalmarijuana.
Fitzgerald,S.NationalBoardOffersGuidanceforDoctorsPrescribingMedicalMarijuana,NeurologyToday;September22,2016
GUIDELINESONPRESCRIBINGMARIJUANA
•Thedoctorshouldreviewothertreatmentoptions.Theknownbenefitsandrisksofmarijuanashouldbepresented,alongwiththewarningthat,unlikewithFDA-approveddrugs,thereisvariabilityandlackofstandardizationinmarijuanapreparation.
•Ifthemedicalmarijuanaischosen,aspecifictreatmentplanforalimitedperiodoftimeshouldbeagreedon,withdetailsdocumentedinthemedicalrecord.Thedoctorshouldinstructthepatientnottodriveoroperateheavymachinerywhileusingmarijuana.
•Thepatientshouldbeseenforfollow-upvisitstomonitorforefficacyandsideeffectsofmedicalmarijuana.
•Patientswithahistoryofmentalhealthproblems,substanceabuseoraddictionshouldbereferredforfurtherevaluationasneeded.
Fitzgerald,S.NationalBoardOffersGuidanceforDoctorsPrescribingMedicalMarijuana,NeurologyToday;September22,2016
WillIGetArrestedforPrescribing(Recommending)MedicalCannabinoids?
In2013,theJusticeDepartmentdeclaredU.S.attorneyswouldnolongerpursueactionsagainstphysiciansforrecommendingmedicalmarijuanainstateswhereithasbeenmadelegal,arulingsupportedbytheAmericanCollegeofPhysicians…….
Thismaychange…………
7/17/17
11
WhatShouldAPrescriberKnowAboutMedicalCannabinoids?
Terms Pharmacokinetics–whatthebodydoestoadrug.Referstothemovementofadruginto,through,andoutofthebody
ADME(Absorption,Distribution,Metabolism,andElimination)
Absorption–aftertakingadrug,itmustcrossoneormorebiologicalmembranesbeforeitreachesthesystemiccirculation. Exception:DrugsadministeredIVenterthesystemiccirculationdirectly
–noabsorptionstep.
Distribution–thepassageofdrugmoleculesfrombloodtotissues.
Metabolism–chemicallychangingdrugcomponentsintometabolites.
Excretion–thepassageofmoleculesfromthebloodtotheoutsideofthebodythroughurine,bile,orotherroutes.
Terms Bioavailability–amountofdrugabsorbedcomparedtothedrugdose. Example:afractionofthedosemaybemetabolizedduringtheearlypassagethroughthegastrointestinaltractorliver.
HalfLife–amountoftimerequiredfortheconcentrationoramountofdruginthebodytobereducedby50%.
Cmax–peakconcentrationofdrug.
Pharmacodynamics–thestudyoftheactionoreffectsofdrugsonthebody.

7/17/17
12
Psychoactive(Personal)vsNon-Psychoactive(Medical)
Cannabinoids
Delta-9-THC“PSYCHOACTIVE”
CBD“NOTPSYCHOACTIVE”
AreYouFamiliarWithTHCMedicationsYouCan
Prescribe?
Marinol(Dronabinol) Chemicallyas(6aR-trans)-6a,7,8,10a-tetrahydro-6,6,9-trimethyl-3-pentyl-6H-dibenzo[b,d]pyran-1-ol.
Issyntheticdelta-9-tetrahydrocannabinol(delta-9-THC)**
Availableinroundsoftgelationcapsulesin2.5mg,5mg,or10mgcapsules
Pharmacodynamics:primarilycentralsympathomimeticactivity
Onset:0.5-1.0hours
Peak:2-4hours
Duration:4-6hourswithappetitestimulationlastingupto24hoursafteradministration
7/17/17
13
Marinol(Dronabinol) Pharmacokinetics
AbsorptionandDistribution:95%absorbedaftersingledosebutonly10-20%reachessystemiccirculation,largevolume(Vd)ofdistributionduetohighlipidsolubility
Metabolism:Undergoesfirstpasshepaticmetabolism,yieldingbothactiveandinactivemetabolites.Primarymetaboliteis11-OH-delta-9-THCwhichconcentrationspeakat0.5to4hoursafteroraldosing-clearanceaverageis0.2L/kgbutvariesanddeclinesoverseveraldays.
Elimination:initialhalflifeis4hoursandterminalhalflifeis25-36hours-duetolargeVd,Marinolisexcretedatlowlevelsforprolongedperiodsoftime.Excretedinfecesandurine(lowlevelsofMarinoldetectedinurineafter5weeks).
Syndros(Dronabinol)OralSolution
FDAApprovedin1985
OralSolution5mg/ml
Syndrosisacannabinoidindicatedinadultsforthetreatmentof:anorexiaassociatedwithweightlossinpatientswithAIDS(1);andnauseaandvomitingassociatedwithcancerchemotherapyinpatientswhohavefailedtorespondadequatelytoconventionalantiemetictreatments.
Dosing:Calibratedoralsyringewith5mgSyndrosmax-ifmorethan5mgnecessarymustgiveindivideddoseswith6-8ouncesofwater
Updated2016Guideslines:Startingdoseof2.1mgorallytwicedaily,onehourbeforelunchanddinner.
ADEs:Dizziness,Euphoria,ParanoidReaction,AbnormalThinking,AbdominalPain,Nausea,andVomiting
FDACenterWatch2016
OtherTHCMedicationsBeingConsideredforFDAApprovalSativex(THCandCBD)-OromucosalsprayformulationusedforthetreatmentofmoderatetoseverespasticityofMS
Epidiolex(CBD)-isplant-derivedCBD,indevelopmentforthetreatmentofanumberofrarepediatricepilepsydisorders
7/17/17
14
SoWhatIsAlloftheControversyAboutPrescribingTHC/CBD
Medications?
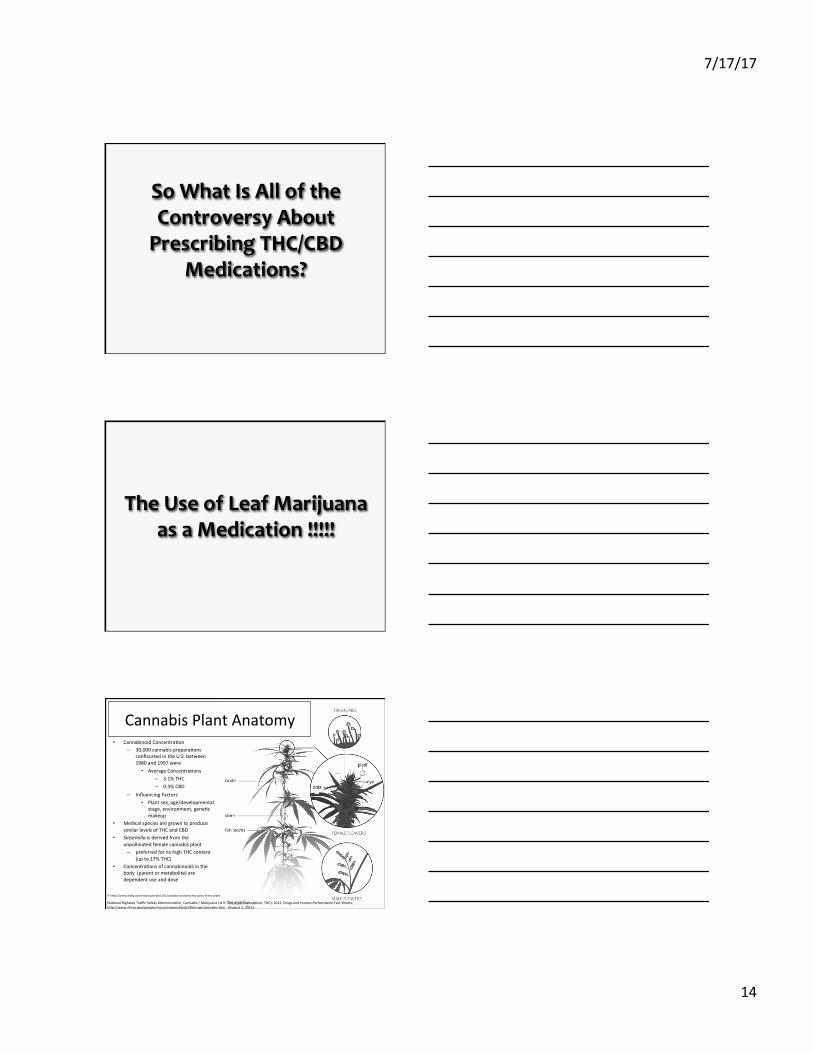
TheUseofLeafMarijuanaasaMedication!!!!!
• CannabinoidConcentra8on– 30,000cannabisprepara8ons
confiscatedintheU.S.between1980and1997were
• AverageConcentra8ons– 3.1%THC– 0.3%CBD
– InfluencingFactors• Plantsex,age/developmental
stage,environment,gene8cmakeup
• MedicalspeciesaregrowntoproducesimilarlevelsofTHCandCBD
• Sinsemillaisderivedfromtheunpollinatedfemalecannabisplant
– preferredforitshighTHCcontent(upto17%THC)
• Concentra8onsofcannabinoidsinthebody(parentormetabolite)aredependentuseanddose
CannabisPlantAnatomy
P:hYps://www.leafly.com/news/cannabis-101/cannabis-anatomy-the-parts-of-the-plant
Na8onalHighwayTrafficSafetyAdministra8on,Cannabis/Marijuana(Δ9-Tetrahydrocannabinol,THC),2012,DrugsandHumanPerformanceFactSheets,hYp://www.nhtsa.gov/people/injury/research/job185drugs/cannabis.htm,(August3,2015)

7/17/17
15
Classifying Marijuana • Marijuana produces some excitatory effects but it
is not generally regarded as a stimulant.
• Marijuana produces sedative effects, but a person faces no risk of slipping into a coma or dying.
• Marijuana produces mild analgesic effects (pain relief), but it is not related pharmacologically to opiates like drugs.
• Marijuana produces hallucinations at high doses, but its structure does not resemble LSD or any other drug formally categorized as hallucinogen.
Chemistry was established over 100 years ago by two chemists, the Smith Brothers. 50 cannabinoid-based compounds, with 4 major cannabinoids in the plant: • 2 isomers, a trans-delta-9-THC and a delta-8-THC • A cannabidiol [CBD] (the 2nd most abundant psychoactive
ingredient after THC) • A cannabinol is a decomposition product of THC that
accumulates as cannabis samples age. After ingestion, delta-9 is converted in the liver to 11-Hydroxy THC which is equally as potent and active.
Ë Delta-9-tetrahydrocannabinol (THC) is the active ingredient of marijuana
major metabolites OH-THC (11-delta-9-THC) and THC-COOH (11-nor-delta-9-THC-carboxylic acid, inactive)
Levo is the more active isomer
O
OH
11-OH-THC (active) THC
7/17/17
16
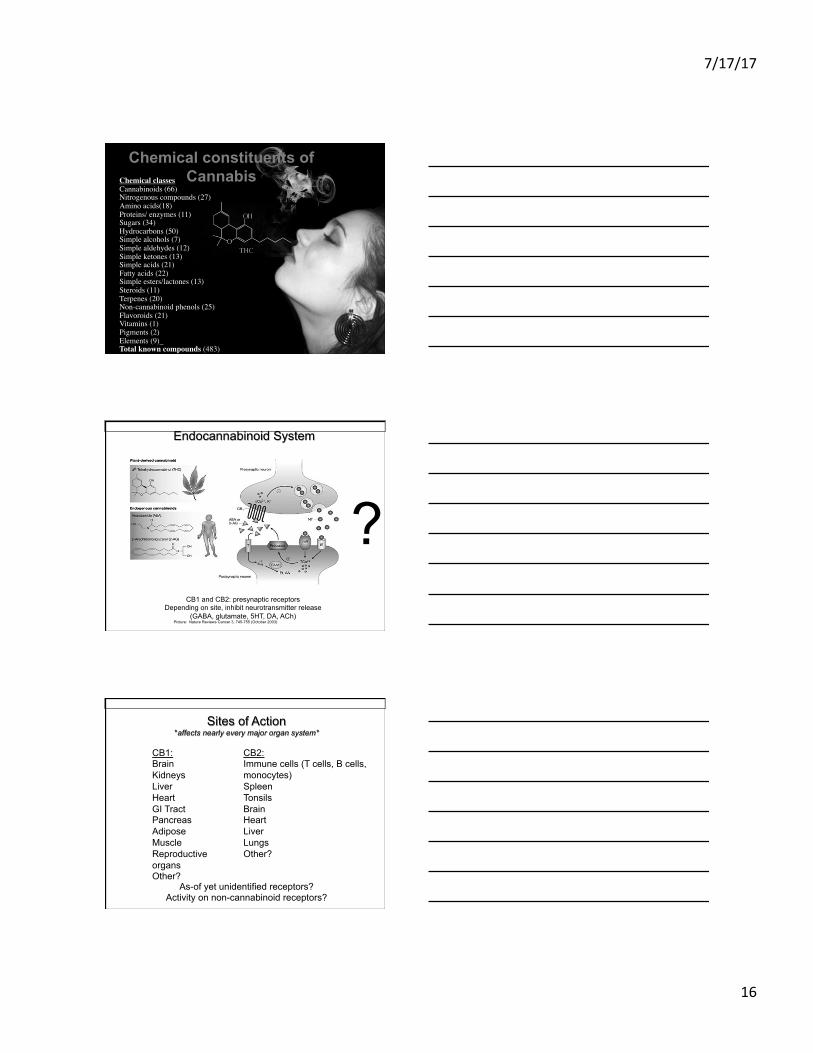
Chemical constituents of Cannabis Chemical classes
Cannabinoids (66)Nitrogenous compounds (27)Amino acids(18)Proteins/ enzymes (11)Sugars (34)Hydrocarbons (50)Simple alcohols (7)Simple aldehydes (12)Simple ketones (13)Simple acids (21)Fatty acids (22)Simple esters/lactones (13)Steroids (11)Terpenes (20)Non-cannabinoid phenols (25)Flavoroids (21)Vitamins (1)Pigments (2)Elements (9) Total known compounds (483)
Picture: Nature Reviews Cancer 3, 745-755 (October 2003)
CB1 and CB2: presynaptic receptors Depending on site, inhibit neurotransmitter release
(GABA, glutamate, 5HT, DA, ACh)
?
Endocannabinoid System
Sites of Action *affects nearly every major organ system*
As-of yet unidentified receptors? Activity on non-cannabinoid receptors?
CB2: Immune cells (T cells, B cells, monocytes) Spleen Tonsils Brain Heart Liver Lungs Other?
CB1: Brain Kidneys Liver Heart GI Tract Pancreas Adipose Muscle Reproductive organs Other?
7/17/17
17
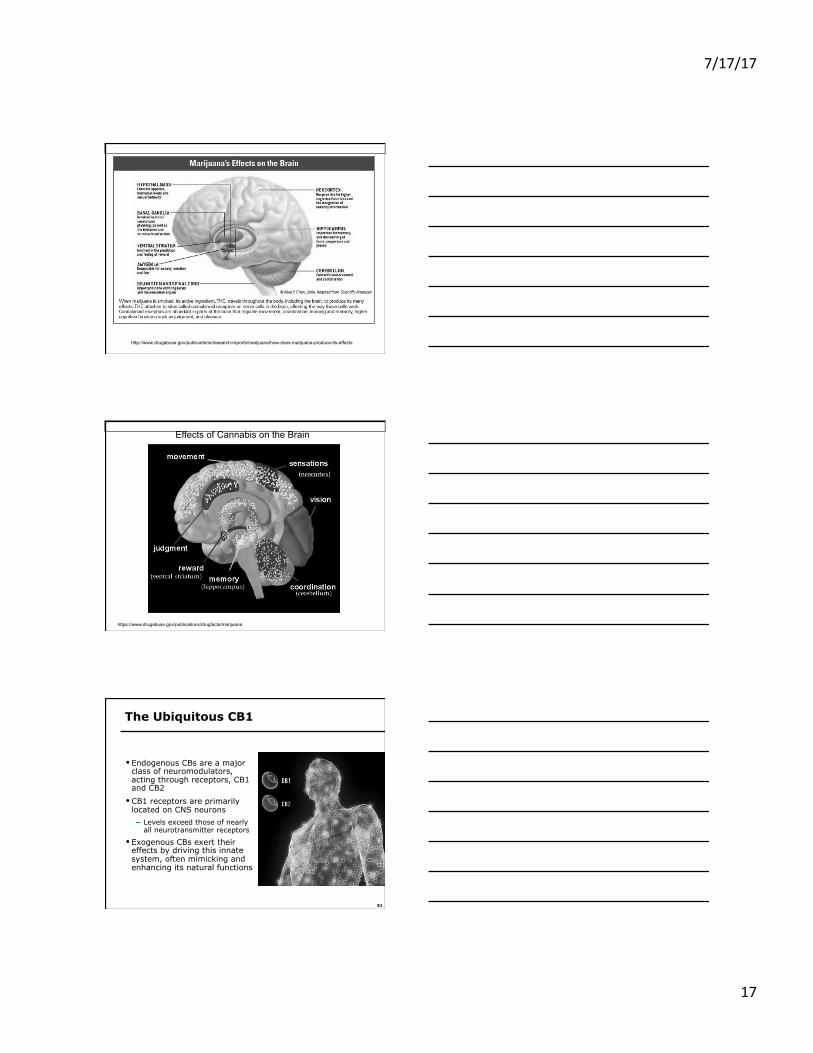
http://www.drugabuse.gov/publications/research-reports/marijuana/how-does-marijuana-produce-its-effects
Effects of Cannabis on the Brain
https://www.drugabuse.gov/publications/drugfacts/marijuana
51
The Ubiquitous CB1
• Endogenous CBs are a major class of neuromodulators, acting through receptors, CB1 and CB2
• CB1 receptors are primarily located on CNS neurons
Levels exceed those of nearly all neurotransmitter receptors
• Exogenous CBs exert their effects by driving this innate system, often mimicking and enhancing its natural functions
7/17/17
18
52
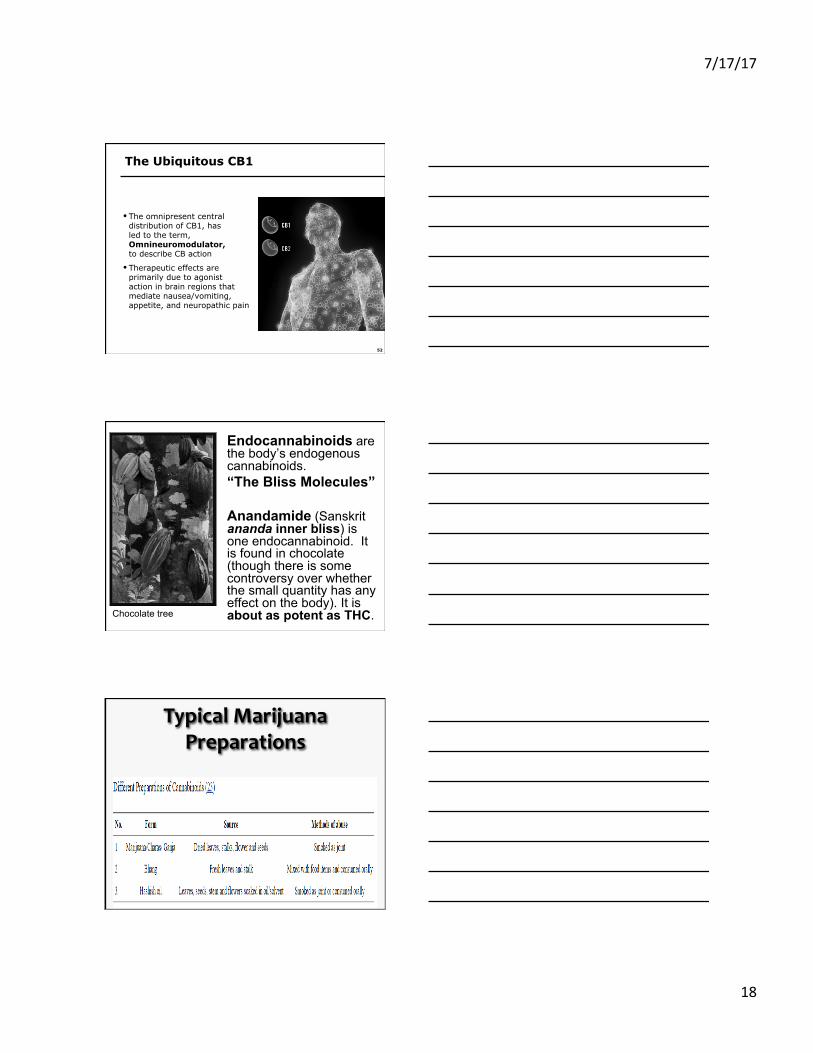
The Ubiquitous CB1
• The omnipresent central distribution of CB1, has led to the term, Omnineuromodulator, to describe CB action
• Therapeutic effects are primarily due to agonist action in brain regions that mediate nausea/vomiting, appetite, and neuropathic pain
Endocannabinoids are the body’s endogenous cannabinoids. “The Bliss Molecules” Anandamide (Sanskrit ananda inner bliss) is one endocannabinoid. It is found in chocolate (though there is some controversy over whether the small quantity has any effect on the body). It is about as potent as THC. Chocolate tree
TypicalMarijuanaPreparations
7/17/17
19
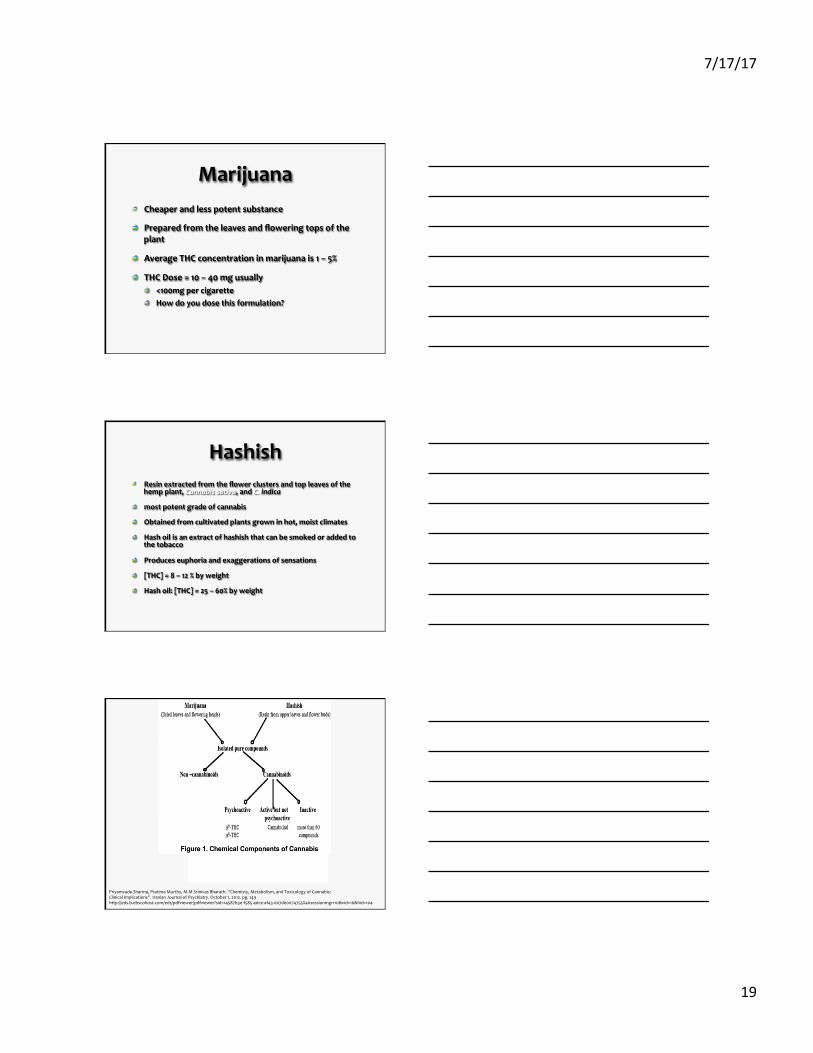
Marijuana Cheaperandlesspotentsubstance
Preparedfromtheleavesandfloweringtopsoftheplant
AverageTHCconcentrationinmarijuanais1–5%
THCDose=10–40mgusually <100mgpercigarette Howdoyoudosethisformulation?
Hashish Resinextractedfromtheflowerclustersandtopleavesofthehempplant,Cannabissativa,andC.indica
mostpotentgradeofcannabis
Obtainedfromcultivatedplantsgrowninhot,moistclimates
Hashoilisanextractofhashishthatcanbesmokedoraddedtothetobacco
Produceseuphoriaandexaggerationsofsensations
[THC]=8–12%byweight
Hashoil:[THC]=25–60%byweight
PriyamvadaSharma,PratimaMurthy,M.MSrinivasBharath.“Chemisty,Metabolism,andToxicologyofCannabis:ClinicalImplications”.IranianJournalofPsychiatry.October1,2012.pg.149http://eds.b.ebscohost.com/eds/pdfviewer/pdfviewer?sid=14587b3e-f585-4dce-af43-007de0074755%40sessionmgr110&vid=16&hid=104
7/17/17
20
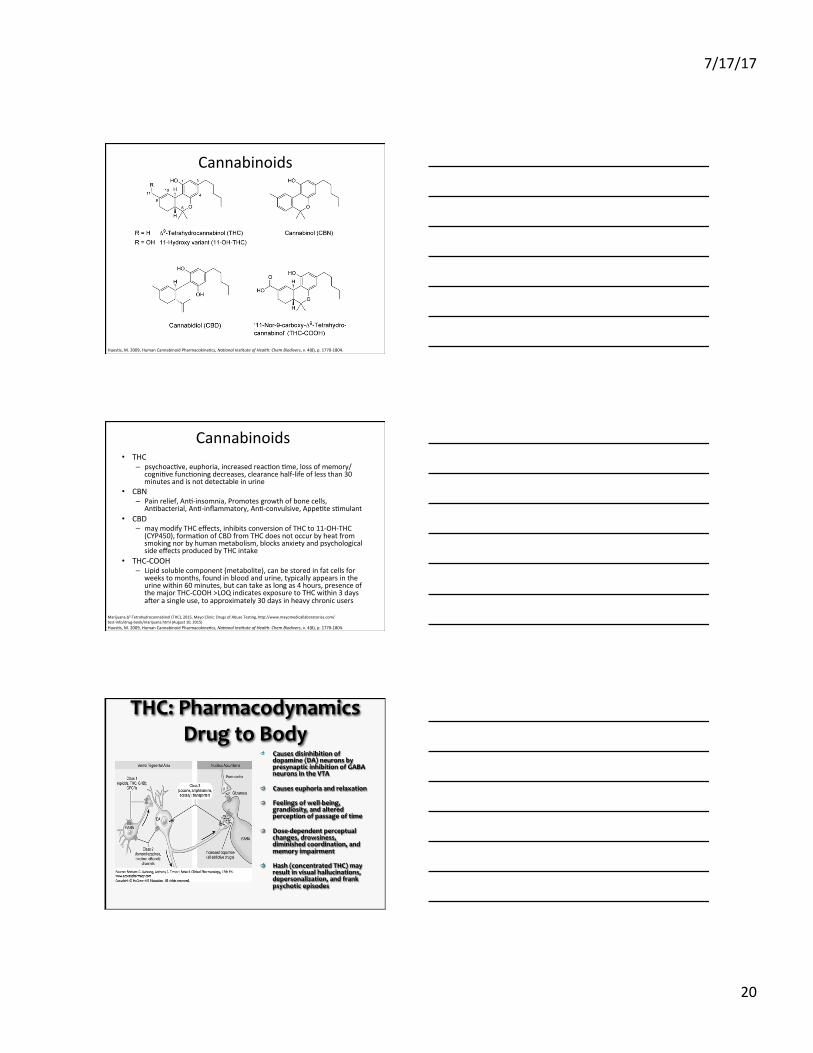
Cannabinoids
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
Cannabinoids• THC
– psychoac8ve,euphoria,increasedreac8on8me,lossofmemory/cogni8vefunc8oningdecreases,clearancehalf-lifeoflessthan30minutesandisnotdetectableinurine
• CBN– Painrelief,An8-insomnia,Promotesgrowthofbonecells,
An8bacterial,An8-inflammatory,An8-convulsive,Appe8tes8mulant• CBD
– maymodifyTHCeffects,inhibitsconversionofTHCto11-OH-THC(CYP450),forma8onofCBDfromTHCdoesnotoccurbyheatfromsmokingnorbyhumanmetabolism,blocksanxietyandpsychologicalsideeffectsproducedbyTHCintake
• THC-COOH– Lipidsolublecomponent(metabolite),canbestoredinfatcellsfor
weekstomonths,foundinbloodandurine,typicallyappearsintheurinewithin60minutes,butcantakeaslongas4hours,presenceofthemajorTHC-COOH>LOQindicatesexposuretoTHCwithin3daysaeerasingleuse,toapproximately30daysinheavychronicusers
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
MarijuanaΔ9-Tetrahydrocannabinol(THC),2015,MayoClinic:DrugsofAbuseTes8ng,hYp://www.mayomedicallaboratories.com/test-info/drug-book/marijuana.html(August10,2015)
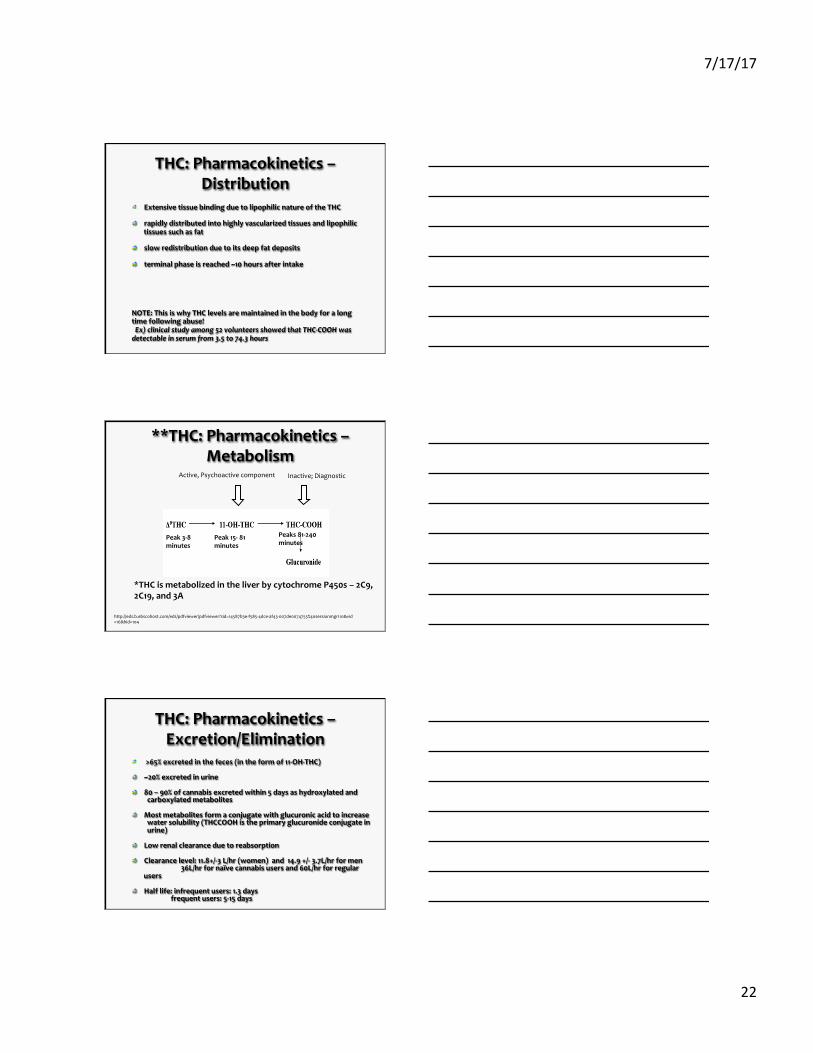
THC:PharmacodynamicsDrugtoBody
Causesdisinhibitionofdopamine(DA)neuronsbypresynapticinhibitionofGABAneuronsintheVTA
Causeseuphoriaandrelaxation
Feelingsofwell-being,grandiosity,andalteredperceptionofpassageoftime
Dose-dependentperceptualchanges,drowsiness,diminishedcoordination,andmemoryimpairment
Hash(concentratedTHC)mayresultinvisualhallucinations,depersonalization,andfrankpsychoticepisodes
7/17/17
21
THC:Pharmacodynamics
apartialagonistatbothCB1&2receptors,hasactivityatnon-CBreceptorsandothertargets,andisresponsibleforthepsychoactiveeffectsofcannabisthroughitsactionsattheCB1receptor.
smokingrouteorbyvaporization:centralnervoussystemandphysiologicaleffectsoccurwithinminutes
Thepsychotropiceffector"high"occursmuchmorequicklybythesmokingthanbytheoralroute
Physiologicaleffectsincluderapidchangesinheartrateanddiastolicbloodpressure,conjunctivalsuffusion,drymouthandthroat,vasodilatation,anddecreasedrespiratoryrate
THC-PharmacokineticsBodytoDrug–Absorption
A.Inhalation/Smoking
90%ofTHCinbloodcirculatesinplasmaandrestsinRBCs
Delta-9-THCisdetectableinplasmawithinsecondsafterthefirstpuff
Peakplasmaconcentrationattainedwithin3–10minutes
Bioavailabilityvariesaccordingtodepthofinhalation,puffduration,andbreath-hold
systemicbioavailabilityis~23–27%forheavyusersand10–14%foroccasionalusers
MaximumTHCplasmaconcentrationisobserved8minutesafteronsetofsmoking
Delta-9-THCplasmaconcentrationrapidlydecreasesto1–4ng/mLwithin3–4hours
THC:Pharmacokinetics–Absorption
B.OralIngestion
relativelyslowersystemicabsorption:1to2hoursbutcanbedelayedbyafewhours
extensivelivermetabolismreducesoralbioavailabilityofTHCby4–12%
maximumTHCplasmaconcentration4.4011ng/mLfor20mgand2.7–6.3ng/mLfor15mg
7/17/17
22
THC:Pharmacokinetics–Distribution
ExtensivetissuebindingduetolipophilicnatureoftheTHC
rapidlydistributedintohighlyvascularizedtissuesandlipophilictissuessuchasfat
slowredistributionduetoitsdeepfatdeposits
terminalphaseisreached~10hoursafterintake
NOTE:ThisiswhyTHClevelsaremaintainedinthebodyforalongtimefollowingabuse!Ex)clinicalstudyamong52volunteersshowedthatTHC-COOHwasdetectableinserumfrom3.5to74.3hours
**THC:Pharmacokinetics–Metabolism
Active,Psychoactivecomponent Inactive;Diagnostic
*THCismetabolizedintheliverbycytochromeP450s–2C9,2C19,and3A
http://eds.b.ebscohost.com/eds/pdfviewer/pdfviewer?sid=14587b3e-f585-4dce-af43-007de0074755%40sessionmgr110&vid=16&hid=104
Peak3-8minutes
Peak15-81minutes
Peaks81-240minutes
THC:Pharmacokinetics–Excretion/Elimination
>65%excretedinthefeces(intheformof11-OH-THC)
~20%excretedinurine
80–90%ofcannabisexcretedwithin5daysashydroxylatedandcarboxylatedmetabolites
Mostmetabolitesformaconjugatewithglucuronicacidtoincreasewatersolubility(THCCOOHistheprimaryglucuronideconjugateinurine)
Lowrenalclearanceduetoreabsorption Clearancelevel:11.8+/-3L/hr(women)and14.9+/-3.7L/hrformen36L/hrfornaïvecannabisusersand60L/hrforregularusers
Halflife:infrequentusers:1.3daysfrequentusers:5-15days
7/17/17
23
AdverseDrugEffectsofLeafMarijuana
Psychological Effects
Ø Euphoria Ø Relaxation
Ø Altered time and space perception
Ø Lack of concentration
Ø Impaired memory/learning
Ø Mood changes Ø Disorientation
Ø Sense of well-being
Ø Drowsiness
Physiological effects
Ø Tachycardia Ø Reddened conjuctiva
Ø Dry mouth and throat
Ø Increased appetite
Ø Vasodilation
Ø Bronchodilation Ø Decreased respiratory rate
7/17/17
24
Duration of Effects on Driving
Ø Effects from smoking are felt within minutes Ø Effects reach their peak in 10-30 minutes
Ø Most users experience a “high” that last about 2-3 hours
Ø Most behavioral and physiological effects last 3-6 hours after drug use
Ø Researchers have shown that some residual effects may last up to 24 hours
Ø Psychomotor impairment can persist after the perceived high has dissipated
Drug Interactions
Ø Marijuana combined with stimulants (cocaine, amphetamines, etc.) can lead to increased hypertension, tachycardia and possible cardiotoxicity
Ø Depressants (Benzodiazepines, barbiturates, muscle relaxants, etc.) can increase drowsiness and CNS depression
Ø Marijuana used in combination with ethanol leads to additive effects
Ø Marijuana and ethanol use makes the user more likely to be a traffic safety risk than when consumed alone
How much should a person use to get 25 mg of THC? • 20% THC • Net weight 1/8 oz or
3.5 gm
• Single serving 50 mg
http://onehumanbeing.com/the_mmj_project/2009/03/granddaddy-purple-at-cclb/
http://bothcollective.com/page/6/?app-download=windowsphone
7/17/17
25
ButIsTHCToxic???
• 2009studyfromAmericanScien9stontherela9vetoxicityofrecrea9onaldrugsshowedthatusingonly109mesthe"effec9ve"doseofalcoholcouldbefatal,whereasmorethan1,0009mestheeffec9vedoseofmarijuanawouldhavetobeusedtobepossiblyfatal.
• ThetoxicdoseofTHCina65kgadultwouldbe8.45kg.
Dr.MerrillNorton,Pharm.D.,D.Ph.,ICCDP-DandCaitlinPayne,ResearchAssistant 73
ButisTHCToxic???• Thetachycardiaalmostinvariablyproducedinacute
intoxica9on,combinedwiththesensoryaltera9onsandincreasedtremorcommonlyreported,probablycontributetotheaffec9vecomponentsofthesereac9ons.CNSandrespiratorydepressionarenotedwithhighdoses,whichinsevereoverdosemaybelife-threatening(Rosencrantz,1983).Theseeffectsare,ofcourse,moredangeroustothosewithpre-exis9ngcardiacirregulari9es.Becauseofthelargeeffec9vetolethaldosera9oinhumans(probablyinexcessof1:1000innon-tolerantusers)theriskofexperiencingseveretoxiceffectsofcannabisislimitedbytheaversivepsychotropiceffectsofhighdoses,whichusuallyleadtocessa9onofusebeforetheonsetofdangerousphysicalconsequences.
Dr.MerrillNorton,Pharm.D.,D.Ph.,ICCDP-DandCaitlinPayne,ResearchAssistant 74
ModifyingConcentra8ons• Why
– SeekingbeYerhigh– MoreTHCandlessCBD
• CBDlimtspsychoac8veeffectsofTHC• terpenes,delayormodulatetheonsetofeffectsofcannabinoids
– an8-inflammatoryterpenesthatprotectthelungsfromirrita8on
• What– HoneyOil,Wax,HashOil
• How– UsingburningtechniquesandsolventstoridplantandplantresinsofCBD
– pureTHCprepara8onsmaybethepresenceofresidualsolvents(e.g.,ethanol)thatareneededtosolubilizethes8ckypureTHC
Na8onalHighwayTrafficSafetyAdministra8on,Cannabis/Marijuana(Δ9-Tetrahydrocannabinol,THC),2012,DrugsandHumanPerformanceFactSheets,hYp://www.nhtsa.gov/people/injury/research/job185drugs/cannabis.htm,(August3,2015)
DeBacker,B.,Maebe,K.,Verstraete,A.,Charlier,C.,2012,Evolu8onoftheContentofTHCandOtherMajorCannabinoidsinDrug-TypeCannabisCumngsandSeedlingsDuringGrowthofPlants,JournalofForensicSciences,v.57(4)
7/17/17
26
EvolvingCannabisAdministra9on• What?
– Newroutes• Why?
– Providemoredirectdelivery
• Considera9ons:
– Mathema9calmodelshavebeendevelopedtoes9matethe9meofmarijuanaexposurewithina95%confidenceintervalbasedonbloodconcentra9ons
– Marijuanahasbeenshowntoimpairperformanceondrivingsimulatortasksandonopenandcloseddrivingcoursesforuptoapproximately3hours
Na8onalHighwayTrafficSafetyAdministra8on,Cannabis/Marijuana(Δ9-Tetrahydrocannabinol,THC),2012,DrugsandHumanPerformanceFactSheets,hYp://www.nhtsa.gov/people/injury/research/job185drugs/cannabis.htm,(August3,2015)
MedicalMarijuanaStandards
What is in medical cannabis?
www.fullspectrumlabs.com Accessed 07/18/2011
7/17/17
27
Recent Clinical Trials of Cannabinoids for the Treatment of CNS Disorders
Disorder Target Symptoms Therapeutic Cannabinoid
Clinical Outcome
Multiple Sclerosis Spasticity Oral THC, CBD In progress Neurogenic pain Sublingual THC, CBD Phase II trial in progress Bladder dysfunction Sublingual THC, CBD Phase II trial in progress
Parkinsons’s disease Dystonia Nabilone No effect Dyskinesia Nabilone ↓ Dyskinesia Tremor Δ9-THC No effect
Cancer Pain Sublingual THC, CBD Phase III trial in progress
Postoperative pain Pain IM levonantradol ↓ pain, but less effective than existing therapies
Croxford, JL. CNS Drugs 2003; 17(3) CBD = cannabidiol
THC = tetrahydrocannabinol
Recent Clinical Trials of Cannabinoids for the Treatment of CNS Disorders (cont’d)
Disorder Target Symptoms Therapeutic Cannabinoid
Clinical Outcome
Spinal cord injury Pain Sublingual THC, CBD
Phase II trial in progress
GI tract pain Pain THC ↓ Morphine requirement
Traumatic Brain Injury / Stroke
Neurodegeneration IV dexanabinol (HU-211)
↓ Intracranial pressure, ↓ mortality, phase III trial in progress
Neurodegeneration CBD In progress
HIV wasting syndrome
Appetite loss, nausea Smoked cannabis In progress
Appetite loss, nausea Dronabinol ↑ appetite, ↓ nausea
Tourette’s syndrome Behavioural disorders THC undetermined
Croxford, JL. CNS Drugs 2003; 17(3)
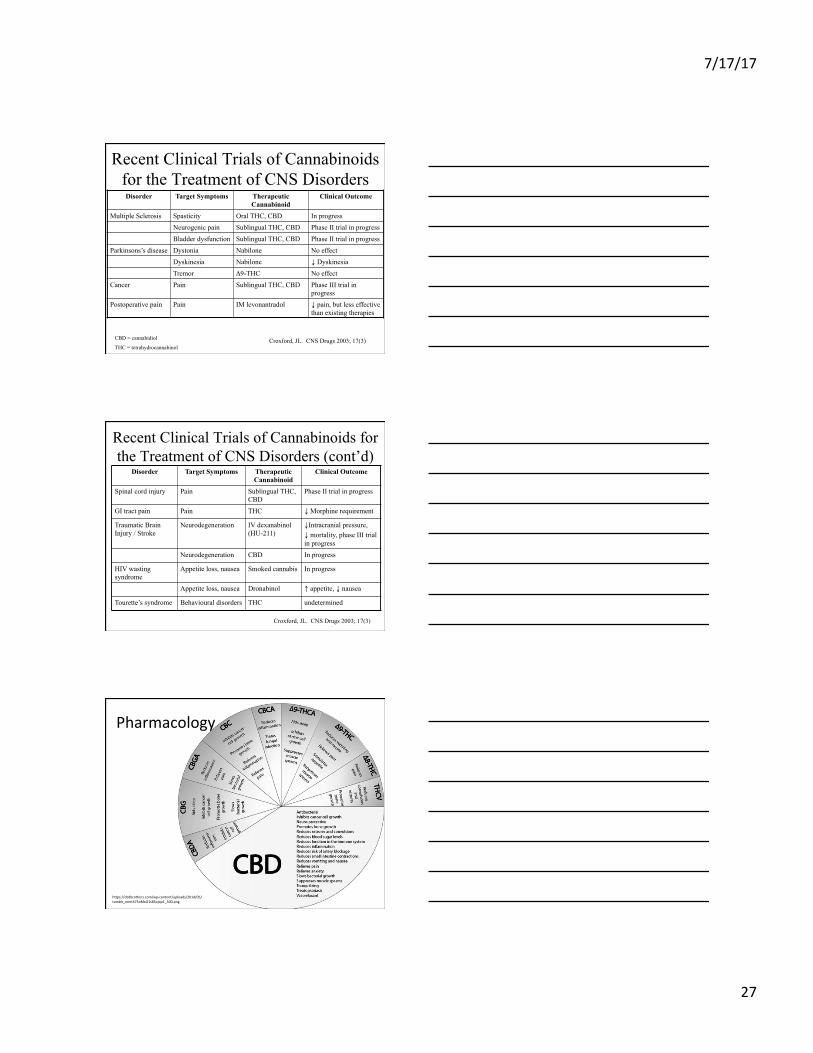
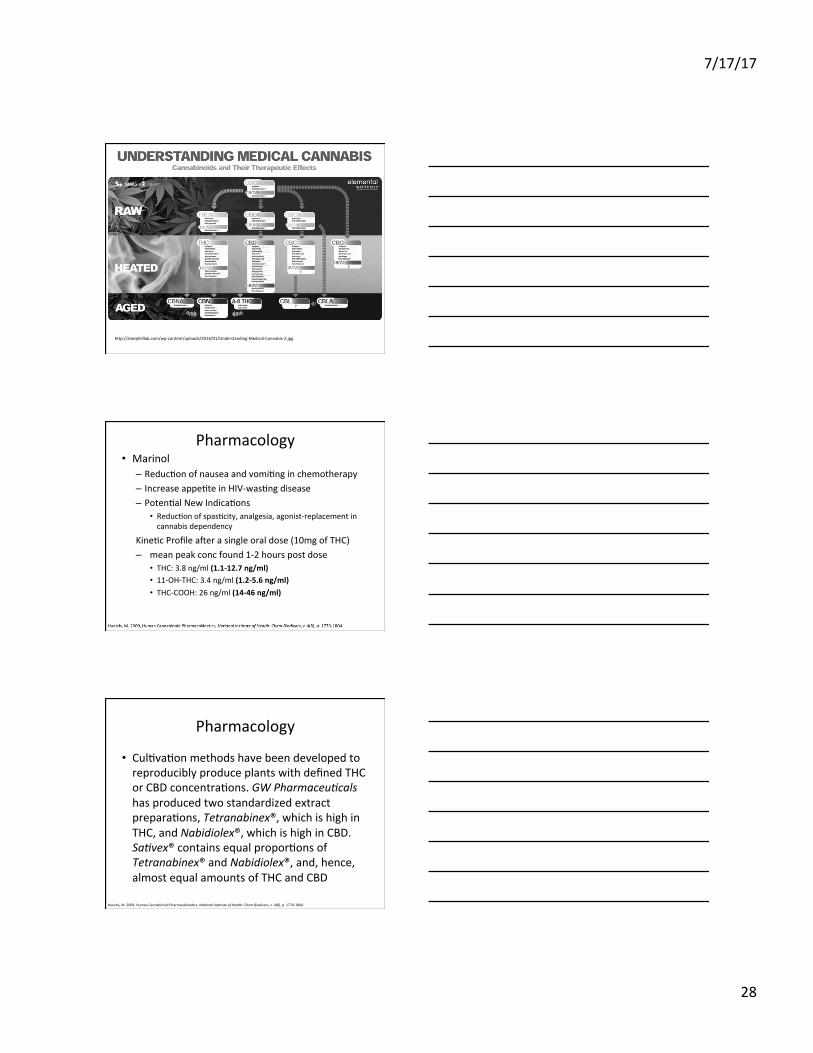
Pharmacology
hYps://cbdbrothers.com/wp-content/uploads/2014/05/tumblr_mmt475oMxO1s85ojqo1_500.png
7/17/17
28
hYp://steephilllab.com/wp-content/uploads/2014/01/Understanding-Medical-Cannabis-2.jpg
Pharmacology• Marinol
– Reduc8onofnauseaandvomi8nginchemotherapy– Increaseappe8teinHIV-was8ngdisease– Poten8alNewIndica8ons
• Reduc8onofspas8city,analgesia,agonist-replacementincannabisdependency
Kine8cProfileaeerasingleoraldose(10mgofTHC)– meanpeakconcfound1-2hourspostdose
• THC:3.8ng/ml(1.1-12.7ng/ml)• 11-OH-THC:3.4ng/ml(1.2-5.6ng/ml)• THC-COOH:26ng/ml(14-46ng/ml)
Pharmacology
• Cul8va8onmethodshavebeendevelopedtoreproduciblyproduceplantswithdefinedTHCorCBDconcentra8ons.GWPharmaceu+calshasproducedtwostandardizedextractprepara8ons,Tetranabinex®,whichishighinTHC,andNabidiolex®,whichishighinCBD.Sa+vex®containsequalpropor8onsofTetranabinex®andNabidiolex®,and,hence,almostequalamountsofTHCandCBD
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
7/17/17
29
DrugInterac8ons• S8mulants
– Cocaine,Amphetamines,etc• increasedhypertension• tachycardia• cardiotoxicity.
• Depressants– Benzodiazepines,Barbiturates,Ethanol,Opioids,An8histamines,musclerelaxants,etc.
• increasedrowsiness• CNSdepression
• Alcohol• greaterimpairment• decreasesinfunc8on• lesslikelytoreactappropriately• increasedreac8on8mes
Na8onalHighwayTrafficSafetyAdministra8on,Cannabis/Marijuana(Δ9-Tetrahydrocannabinol,THC),2012,DrugsandHumanPerformanceFactSheets,hYp://www.nhtsa.gov/people/injury/research/job185drugs/cannabis.htm,(August3,2015)
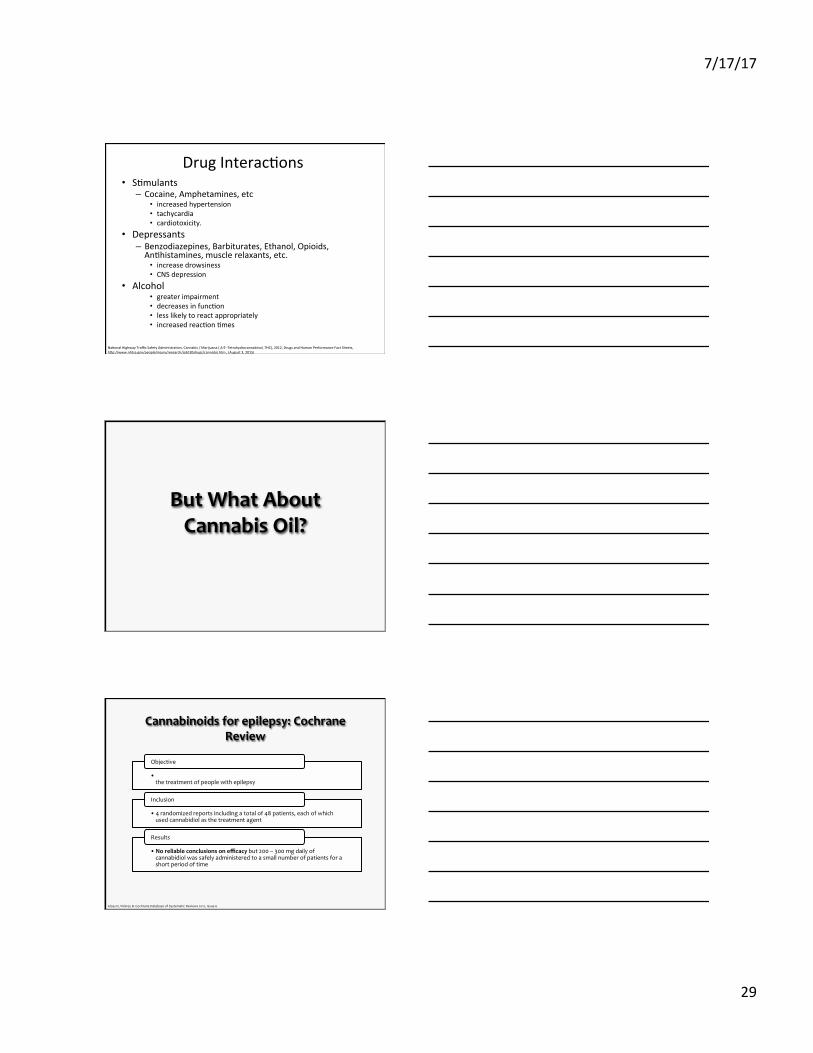
ButWhatAboutCannabisOil?
• Assesstheefficacyofmarijuana,oroneofmarijuana’sconstituentsinthetreatmentofpeoplewithepilepsy
Objective
• 4randomizedreportsincludingatotalof48patients,eachofwhichusedcannabidiolasthetreatmentagent
Inclusion
• Noreliableconclusionsonefficacybut200–300mgdailyofcannabidiolwassafelyadministeredtoasmallnumberofpatientsforashortperiodoftime
Results
Cannabinoidsforepilepsy:CochraneReview
GlossD,VickreyB.CochraneDatabaseofSystematicReviews2012,Issue6

7/17/17
30
AmericanAcademyofNeurology
Concludethat“forpatientswithepilepsy,dataareinsufficienttosupportorrefutetheefficacyofcannabinoidsforreducingseizurefrequency”
ThereisNOTsufficientevidencetoprescribeCBDorrecommendself-treatmentwithsmokedmarijuana
KoppelBSetal.Neurology2014;82:1556-1563
Anecdotalcasesofchildrensuccessfullytreatedwith
medicalmarijuana(CBD
enrichedpreparations)
Prominentinternetand
nationalmediaattention
Beliefthattreatmentsderivedfrom
naturalproductsaresaferormore
effectiveiscommonandpotentiallydangerous
Whyareparentsusingcannabis?
CilioMRetal.Epilepsia.2014.55(6):787-790
Charlotte§ CharlotteisalittlegirlfromColorado
withDravetsyndrome
§ Frequentboutsoffebrileandafebrilestatusepilepticus
§ Failedmultiplemedications:Levetiracetam,oxcarbazepine,topiramate,zonisamide,valproate,clobazam,clonazepam,anddiazepam
§ At5yearsofage,hadsignificantcognitiveandmotordelays,requiredafeedingtube,andneededfullassistancewithactivitiesofdailyliving
§ 50generalizedtonic-clonicseizuresperday
http://www.cnn.com/2013/08/07/health/charlotte-child-medical-marijuana/
7/17/17
31
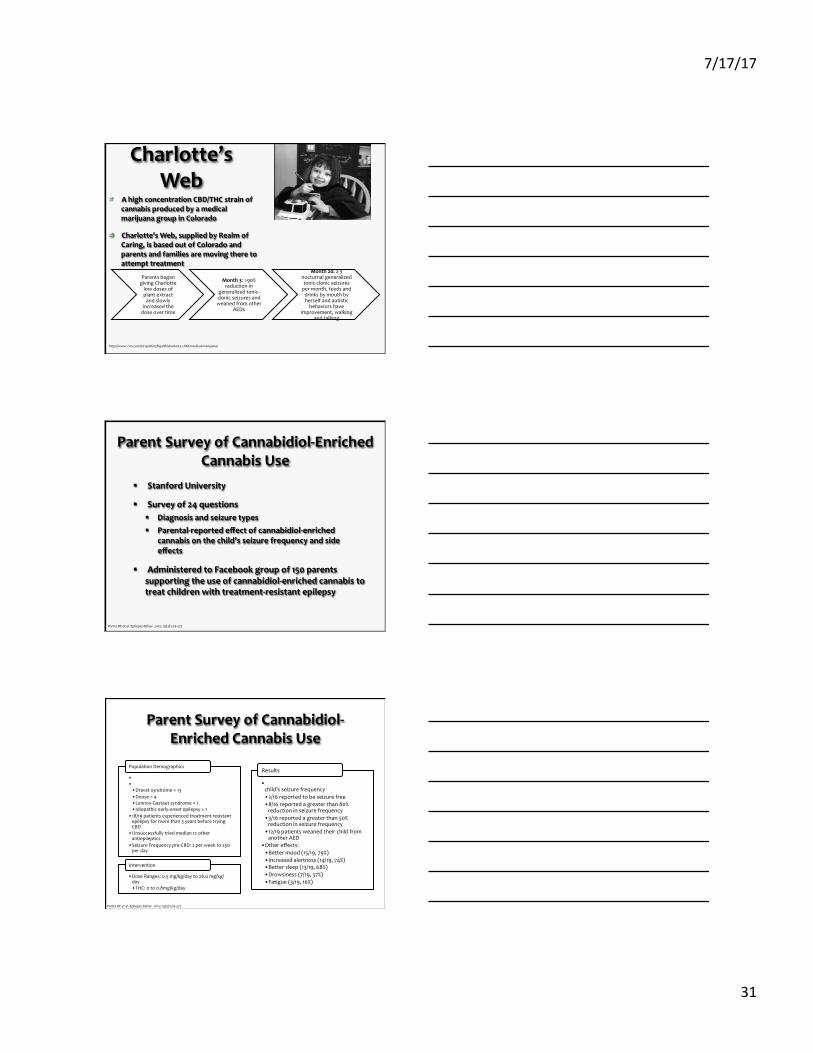
Charlotte’sWeb
AhighconcentrationCBD/THCstrainofcannabisproducedbyamedicalmarijuanagroupinColorado
Charlotte’sWeb,suppliedbyRealmofCaring,isbasedoutofColoradoandparentsandfamiliesaremovingtheretoattempttreatment
ParentsbegangivingCharlottelowdosesofplantextractandslowly
increasedthedoseovertime
Month3:>90%reductionin
generalizedtonic-clonicseizuresandweanedfromother
AEDs
Month20:2-3nocturnalgeneralizedtonic-clonicseizurespermonth,feedsanddrinksbymouthbyherselfandautisticbehaviorshave
improvement,walkingandtalking
http://www.cnn.com/2013/08/07/health/charlotte-child-medical-marijuana/
ParentSurveyofCannabidiol-EnrichedCannabisUse
§ StanfordUniversity
§ Surveyof24questions§ Diagnosisandseizuretypes§ Parental-reportedeffectofcannabidiol-enriched
cannabisonthechild’sseizurefrequencyandsideeffects
§ AdministeredtoFacebookgroupof150parentssupportingtheuseofcannabidiol-enrichedcannabistotreatchildrenwithtreatment-resistantepilepsy
PorterBEetal.EpilepsyBehav.2013;29(3):574-577
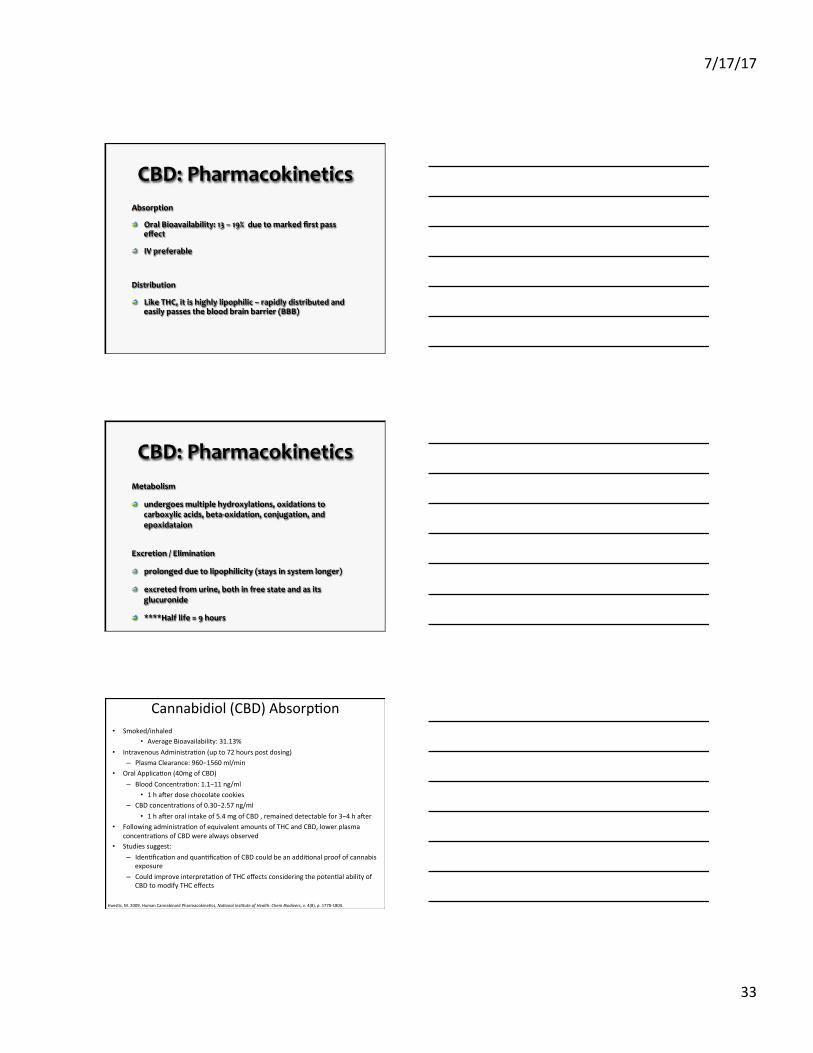
ParentSurveyofCannabidiol-EnrichedCannabisUse
PorterBEetal.EpilepsyBehav.2013;29(3):574-577
• Agerange:2–16yearsold• SeizureTypes:• Dravetsyndrome=13• Doose=4• Lennox-Gastautsyndrome=1• Idiopathicearly-onsetepilepsy=1
• 18/19patientsexperiencedtreatmentresistantepilepsyformorethan3yearsbeforetryingCBD
• Unsuccessfullytriedmedian12otherantiepileptics
• SeizureFrequencypre-CBD:2perweekto250perday
PopulationDemographics
• DoseRanges:0.5mg/kg/dayto28.6mg/kg/day• THC:0to0.8mg/kg/day
Intervention
• 16/19(84%)reportedareductionintheirchild’sseizurefrequency• 2/16reportedtobeseizurefree• 8/16reportedagreaterthan80%reductioninseizurefrequency
• 3/16reportedagreaterthan50%reductioninseizurefrequency
• 12/19patientsweanedtheirchildfromanotherAED
• Othereffects:• Bettermood(15/19,79%)• Increasedalertness(14/19,74%)• Bettersleep(13/19,68%)• Drowsiness(7/19,37%)• Fatigue(3/19,16%)
Results

7/17/17
32
Cannabidiol:CBD
Cannabinoids
Delta-9-THC“ACTIVE”CBD“INACTIVE
Cannabidiol (CBD) versus THC • THC and CBD molecules present in largest amounts in cannabis.
Most recognized and studied. • Classed as phytocannabinoids (as opposed to endocannabinoids
and cannabinoids that are manufactured artificially), both CBD and THC interact with specific cells in our brains.
• THC – Psychoactive cannabinoid, THC is responsible for the “high” from smoking marijuana so production and usage are strictly regulated (even in WA, OR, CO and AK).
• CBD – naturally occurring cannabinoid, and the second most abundant molecule in Cannabis plant.
• CBD is legal and safe to consume, yet has long been in the shadow of THC.
CBD:Pharmacodynamics
LacksdetectablepsychoactivityanddoesnotappeartobindtoeitherCB1orCB2receptorsatphysiologicallymeaningfulconcentrations.
Affectstheactivityofasignificantnumberofothertargetsincludingionchannels,receptors,andenzymes.
Mayhaveanti-inflammatory,analgesic,anti-nausea,anti-emetic,anti-psychotic,anti-ischemic,anxiolytic,andanti-epileptiformeffects.
7/17/17
33
CBD:PharmacokineticsAbsorption
OralBioavailability:13–19%duetomarkedfirstpasseffect
IVpreferable
Distribution
LikeTHC,itishighlylipophilic–rapidlydistributedandeasilypassesthebloodbrainbarrier(BBB)
CBD:PharmacokineticsMetabolism
undergoesmultiplehydroxylations,oxidationstocarboxylicacids,beta-oxidation,conjugation,andepoxidataion
Excretion/Elimination
prolongedduetolipophilicity(staysinsystemlonger)
excretedfromurine,bothinfreestateandasitsglucuronide
****Halflife=9hours
Cannabidiol(CBD)Absorp8on• Smoked/inhaled
• AverageBioavailability:31.13%• IntravenousAdministra8on(upto72hourspostdosing)
– PlasmaClearance:960−1560ml/min• OralApplica8on(40mgofCBD)
– BloodConcentra8on:1.1−11ng/ml• 1haeerdosechocolatecookies
– CBDconcentra8onsof0.30−2.57ng/ml• 1haeeroralintakeof5.4mgofCBD,remaineddetectablefor3−4haeer
• Followingadministra8onofequivalentamountsofTHCandCBD,lowerplasmaconcentra8onsofCBDwerealwaysobserved
• Studiessuggest: – Iden8fica8onandquan8fica8onofCBDcouldbeanaddi8onalproofofcannabis
exposure– Couldimproveinterpreta8onofTHCeffectsconsideringthepoten8alabilityof
CBDtomodifyTHCeffects
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
7/17/17
34
Cannabidiol(CBD)Metabolism• Significantfirst-passeffect
– UnlikeTHC,alargepropor8onisexcretedunchangedinthefeces• Co-administra8onofCBDwithTHCdidnotsignificantlyimpactTHCorTHC
metabolitekine8cs,including:– thetotalclearance,– volumeofdistribu8on– terminalelimina8onhalf-lives
• CBDonlypar8allyinhibitedthehydroxyla8onofTHCto11-OH-THCcatalyzedbyCYP2C– Studybasedonconcentra8onvs8mecurves,ra8osofmax.average
concentra8ons,andAUCvaluesof:• 11-OH-THC/THC• THC-COOH/THC• THC-COOH/11-OH-THC
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
CannabisElimina8on• 5dayspostdose:80−90%ofTHCisexcreted
– 65%isexcretedinthefeces• Primaryfecalmetabolite:11-OH-THC
– 20%beingeliminatedintheurine• primaryurinarymetabolite:acid-linkedTHC-COOHglucuronideconjugate
• Urineconcentra8ondropsrapidlyun8lreachingaconcentra8onof20−50ng/ml,thenbeginsdecreaseatamuchslowerrate
• Longterminalhalf-lifeofTHCinplasma– Reportedtobegreaterthan4.1dinchroniccannabisusers
• MeanplasmaTHC-COOHelimina8onhalf-lives:– FrequentUsers:5.2±0.8– InfrequentUsers:6.2±6.7d
• However,nosignificantpharmacokine8cdifferencesbetweenchronicandoccasionalusershavebeensubstan8ated
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
PharmacodynamicsofOtherCannabinoids
Δ8-THC(anisomerofΔ9-THC):partialagonistatbothCBreceptorsandsharesrelativelysimilarefficacyandpotencywithΔ9-THC.Morepotentanti-emeticthanΔ9-THC.
Cannabinol(aproductofΔ9-THCoxidation):has10%oftheactivityofΔ9-THC.Appearstohavesomepossibleimmunosuppressiveproperties.
Cannabigerol:partialCB1/2receptoragonist.Mayhavesomeanti-inflammatoryandanalgesicproperties.Itmayalsoblock5-HT1Areceptorsandactasanα2-adrenoceptoragonist.
Tetrahydrocannabivarin:actsasaCB1receptorantagonistandCB2receptorpartialagonist.Itmayhaveanti-epileptiform/anti-convulsantproperties.
7/17/17
35
Pharmacology(2015)
• Cul9va9onmethodshavebeendevelopedtoreproduciblyproduceplantswithdefinedTHCorCBDconcentra9ons.GWPharmaceu,calshasproducedtwostandardizedextractprepara9ons,Tetranabinex®,whichishighinTHC,andNabidiolex®,whichishighinCBD.Sa,vex®containsequalpropor9onsofTetranabinex®andNabidiolex®,and,hence,almostequalamountsofTHCandCBD
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
DifferentRoutesofAdministrationandthe
EffectonPlasmaConcentrations
A. IntravenousRoute
B. OralRoute
C. Vaporization/Inhalation
D. Dabbing
IntravenousRoute-Researchprimarily
HowCannabisCausesParanoia:UsingtheIntravenousAdministrationof∆9-Tetrahydrocannabinol(THC)toIdentifyKeyCognitiveMechanismsLeadingtoParanoiaDanielFreeman*,1,GrahamDunn2,RobinM.Murray3,NicoleEvans1,RachelLister1,AngusAntley1,MelSlater4,5,BeataGodlewska1,RobertCornish6,JonathanWilliams7,MartinaDiSimplicio8,ArtemisIgoumenou9,RudolfBrenneisen10,ElizabethM.
Tunbridge1,PaulJ.Harrison1,CatherineJ.Harmer1,PhilipCowen1andPaulD.Morrison3+
7/17/17
36
Edibles
Edibles• Gela9ncapsules,glycocholate,sesameoil:improvedbioavailability
– Considerablevaria9onsinpeakconcentra9onsandratesofabsorp9on
» Occurredevenwhenadministerinthesamevehiclemorethanonce
– SesameOilbasedAdministra9on» OralTHCbioavailability:10-20%
• Meningested20mg• Womeningested15mg
» PlasmaPeakat4-6hours,butwereconsideredoveres9matedbecauseofradioac9velabelingnotbeingsubjecttoonlyTHCandextendingtoitsmetabolites
Dr.MerrillNorton,Pharm.D.,D.Ph.,ICCDP-DandCaitlinPayne,ResearchAssistant 107
OralAdministration–ClinicalStudyExample
ingestionofbrowniescontainingalowdoseofΔ9-THC(9mgTHC/brownie)àmeanpeakplasmaΔ9-THClevelsof5ng/mL
IngestionofbrowniescontainingahighdoseofΔ9-THC(~13mgΔ9-THC/brownie)àmeanpeakplasmaΔ9-THClevelsof6to9ng/mL
NOTE:only10–20%oftheadministereddoseentersbloodstreamduetoextensivefirstpasseffect
7/17/17
37
Inhala8onandSmoking• Absorp8on
– Rapidandefficientdeliveryfromlungstobrain– ExposingdrugeffectstoCNS(abusepoten8al)– Slightlylowerpeakconcentra8onsthatIVadministeredTHC– Bioavailability:2-56%
• Duetovariabilityinsmokingdynamics/ability– Number,dura8on,spacingbetweenpuffs,hold8me,inhala8onvolume,smokingtopography,and
expecta8on– Forma8onof11-OH-THCandTHC-COOHoccurredlaterandwithmuchlowerconcentra8ons
• TechniqueandStudyDesign– THCdisposi8onfollowedfor7daysaeersmokingasinglecannabiscigareYecontaining1.75%or3.55%THC
• ImmediatelyfollowingfirstcigareYepuff– MeanTHCconc1.75%(16mg):7.0+/-8.1ng/ml– MeanTHCconc3.55%(34mg):18.1+/-12.0ng/ml
• Peakconcoccurredat9minutespriortostoppingsmokingat9.8minutes– PeakTHCconc1.75%(16mg):84.3ng/ml(range50-129)– PeakTHCconc3.55%(34mg):162.2ng/ml(range76-267)
• Within2hoursofcessa8onalllevelsfellbelow5ng/ml• Dosedetec8on(levelabove0.5ng/ml)
– 1.75%(16mg):3to12hours– 3.55%(34mg):6to27hours
• Thoughtsonsafety/delivery– AllsubjectsusinghashishbasedcigareYesexperiencedhigherTHCconcentra8onsinplasma– THCconcentra8onstypicallypeakduringtheactofsmoking,whilepeak11-OHTHCconcentra8onsoccurapproximately
9-23minutesaeerthestartofsmokingHues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
Vaping• Absorp8on
– vaporizersreportedtheonsetofeffectsmorerapidlywithpureTHC(mean2.5min)thanherbalcannabis(mean6.5min)
– vaporizerresultedinhigherplasmaconcentra8onsofTHCcomparedtosmokedmarijuanaat30and60minateachstrength
• Technique– hea8ngcannabistoatemperaturebetween180and2001C,itispossibleto
vaporizethecannabinoidsthatresideonthetrichomesonthesurfaceofcannabisflowersandleaves,whileavoidingcombus8on
• Thoughtonsafety/delivery– vola8zescomponentssuchasTHC,CBD,andterpenes,butwithsignificant
reduc8onofpyroly8cbyproducts– releasesubstan8al– amountsoftheTHCwhileproducingnomeasurableamountsofthebenzene,
toluene,andnaphthalene,whicharegeneratedwhenmarijuanaissmoked– vaporizertoinhalesomeformofpureTHC(likelydissolvedinalcoholor
anothersolvent)
Hazekamp,A.,Ware,M.,Muller-Vahl,K.,Abrams,D.,Grotenhermen,F.,2013,Themedicinaluseofcannabisandcannabinoids--aninterna8onalcross-sec8onalsurveyonadministra8onforms,JournalofPsychoac8veDrugs,45(3),p.199-210
Vaporization-clinicalstudyexample
32Adultcannabissmokersdrankplaceboorlow-dosealcohol10minbeforeinhaling500mgplacebo,low-dose(2.9%)THC,orhigh-dose(6.7%)THCvaporizedcannabis.
Bloodandplasmaconcentrationswereobtainedbeforeandupto8.3hafteringestion
“ControlledCannabisVaporizerAdministration:BloodandPlasmaCannabinoidswithandwithoutAlcohol”RebecaL.Hartman,TimothyL.Brown,GaryMilavetz,AndrewSpurgin,DavidA.Gorelick,GaryGaffneyandMarilynA.Huestis.ClinicalChemistry.June2015vol61no.6p.850-869.
http://www.clinchem.org.proxy-remote.galib.uga.edu/content/61/6/850.full
7/17/17
38
Dabbing Inhalationofaconcentratedtetrahydrocannabinol(THC)productcreatedthroughbutaneextraction
Blasting-passbutanethroughasteelorglasstubepackedwithdriedcannabistrimmings-THCandotherhydrophobiccompoundsintheplant’strichomesdissolveintothebutane-butane-THCsolutionleavesthetubethroughfilterandiscollectedinadishortray-butaneevaporatesandleavesresinsthatcanhaveTHCconcentrationupto80%
SoWhatIstheProblemWithMedicalMarijuana
ForPrescribers?
7/17/17
39
NewTypesofConcentrates
• Kief• WaterHash• CO2Oil• ButaneHashOil(BHO)• Rosin
Concentra9on:Kief• Alsoknownasdrysieve(some9mes“drysip”)hash,kiefisthe
simplestofconcentrates.Kiefiscomposedofthetrichomes(thecrystallinestructurescoa9ngtheoutsidesurfaceoftheflowers)brokenawayfromthedriedplantmaterial,usuallyviaspecializedfilteringscreensandalialeelbowgrease.Kiefisgenerallyconsideredalower-qualityextract,butsometop-flightextractorscanproduceanextremelycleanandflavorfulproductusingthismethod.THCcontentcanrangefrom20percentto60percent.Thisprocessatitshighestlevelyieldsnothingbutthelargest,mostperfecttrichomeglandheadsandnoneoftheglandstems,plantmaaer,etc.thatgenerallycloudsthequicker,lower-qualitykiefextrac9ons.WhileitiscertainlyavailableinColoradodispensaries,comparedtothreeyearsago,itismuchhardertofindbecauseoftheprevalenceofsolventextractsandthelowreturnthatitprovidestocommercialgrowers.
DeBacker,B.,Maebe,K.,Verstraete,A.,Charlier,C.,2012,Evolu8onoftheContentofTHCandOtherMajorCannabinoidsinDrug-TypeCannabisCumngsandSeedlingsDuringGrowthofPlants,JournalofForensicSciences,v.57(4)
ConcentratesofWaterHash• Therearevarioustechniquesusedintheproduc9onofwaterhash,and
theresul9ngproductshavemanyforms(bubblehash,solventlesswax,icewax,amongothers).Thebasicprincipleisthis:plantmaterial(eitherdryorfresh-frozengenerally)ismixedwithcoldwaterandice,thenagitatedmanuallyormechanicallyinordertobreakoffthenow-brialetrichomeheads.Thissolu9onisthenfilteredthroughspecifically-sizedscreenstoremoveanythingundesirable,leavingbehindarela9velypurefinishedproductthattypicallytestsbetween50percentand80percentTHC.Themostcommonwaythatwaterhashisextractedisusingaseriesofmicroscreenfabricbags(generallyreferredtoas“bubblebags”)whichremovevariousgradesofproductaccordingtothesizeofpar9clestheyallowthrough.
7/17/17
40
ConcentratesofCO2Oil
• Thisvarietyofextractiscreatedusingcarbondioxidecompressedathighpressuresun8litbecomeswhatisknownasa“supercri8calfluid,”whichthenisabletostriptheessen8aloilsofthecannabisplantmuchlikehydrocarbonsolvents.CO2oilisgenerallyaloose,orange-8ntedoilthatcanbeeitherclearoropaquedependinguponthefinishingprocessesusedaeerextrac8on,andTHCcontenttestsbetween50percentand75percent.Theappealofthismethodformanyisthatitisnon-flammableandcontainsnochemicalsolvents.ThemachinesrequiredtodoCO2extrac8onsatanykindofcommercialscalecancosthundredsofthousandsofdollars.
ConcentratesofButaneHashOil(BHO)
• Perhapsthemostcommontypeofextractonthemarket,BHOhasavarietyofnames(wax,shaYer,crumble,oil,errl,honeycomb,moonrock,nectar,etc.)butlikewaterhash,thebasicprinciplesofextrac8onarethesameacrossallofthem,withthevaria8onsinappearanceandtexturemostlycominginfinishingprocesses.Tomakeabutaneconcentrate,butaneispressurizedinavesselandwashedoverplantmaterial(usuallydry,butsome8mesfresh-frozen—moreonthatbelow),thentheresul8ngsolu8oniscollected.Thehashmakermustremoveanyresidualsolventfromthissolu8on,sothenextstepgenerallyisapplyingheat(butanehasalowboilingpoint)andvacuum(whichlowerstheboilingpointfurther)inordertomakethisprocesseasierandfasterwhileretainingthehighestamountofflavorfulterpenesandcannabinoidsinthefinishedproduct.BHOgenerallytestsbetween60percentand90percentTHC,makingitperhapsthestrongestconcentrateonthemainstreammarket.
ConcentratesofRosin• ThenewestandhoYesttypeofextractonthescenerightnow,rosinisextractedfromeitherdriedbuds,trim,orlower-gradewaterhash/kief.Whatisuniqueaboutrosinisthatitcanbemadewithnothingmorethanastandardhairstraightener,parchmentpaperandsomehand-appliedpressure.Whenthematerialissmashedandheatedquicklybetweentheparchmentsheets,itextrudessomeoftheessen8aloilspresentintheplant,resul8nginagoldenshaYeroroil-likeextractthatlookssimilartopressedhigh-qualitywaterhashorevensolvent-extractedshaYer.Rosinisafairlyrecentdevelopment,soitsavailabilityindispensariesiss8llsomewhatlimited,asisdataaboutitspotency;butearlyreportsonsomerosinextractshaveshowednumbersbetween50percentand70percentTHC,similartothatofhigh-qualitywaterhash.
7/17/17
41
Inhala9onandSmoking• Absorp9on
– Rapidandefficientdeliveryfromlungstobrain– ExposingdrugeffectstoCNS(abusepoten9al)– Slightlylowerpeakconcentra9onsthatIVadministeredTHC– Bioavailability:2-56%
• Duetovariabilityinsmokingdynamics/ability– Number,dura9on,spacingbetweenpuffs,hold9me,inhala9onvolume,smokingtopography,andexpecta9on
– Forma9onof11-OH-THCandTHC-COOHoccurredlaterandwithmuchlowerconcentra9ons
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
ColoradoMarijuanaAnalysis–March2015
Denverlabanalyzedmorethan600samplesofbudprovidedbycertifiedgrowersandsellers
averageTHClevelwas18.7%,andsomeretailpotcontained30%THCormore
Littleornocannabidiol(CBD)—theaverageCBDamount:0.1% Recall:CBDlacksdetectablepsychoactivityandinsteadhas
anti-inflammatory,analgesic,anti-nausea,anti-emetic,anti-psychotic,anti-ischemic,anxiolytic,andanti-epileptiformeffects–the“medical”inmedicalmarijuana.
OtherAdministra9ons• Routes
– Oromucosal• Sa,vex®isadministeredsublinguallytoavoidfirst-passmetabolismbytheliver.Sa,vex®is
approvedinCanadaforthetreatmentofneuropathicpainassociatedwithmul9plesclerosis,andinthreeEuropeancountriesforanumberofindica9ons.
– Rectal• THC-hemisuccinateprovidedthehighestbioavailabilityof13.5%(Marinolsuppository)• bioavailabilityoftherectalroutewasapproximatelytwicethatoftheoralroute• THCdidnotaccumulateinthebloodfollowing10−15mgdailydoses• administra9onof2.5−5mgofTHCproducedmaximumplasmaconcentra9onsof1.1−4.1ng/ml
within2−8h.– Transcutaneous
• meansteady-stateplasmaconcentra9onofΔ8-THCwas4.4ng/mlwithin1.4h,andwasmaintainedforatleast48h
• Permeabili9esofCBDandCBNwerefoundtobe10-foldhigherthanforΔ8-THC• Lowabusepoten9alduetoslowdeliveryofTHCtothebrain
– Intravenous• THCproducedschizophrenia-likeposi9veandnega9vesymptomsandeuphoria,andaltered
aspectsofcogni9vefunc9on– Acuteparanoia,panic,hypotension,withdrawal,behaviorandcogni9vedefects
(endogenouspsychosis)
Hues8s,M.2009,HumanCannabinoidPharmacokine8cs,Na+onalIns+tuteofHealth:ChemBiodivers,v.4(8),p.1770-1804.
7/17/17
42
124
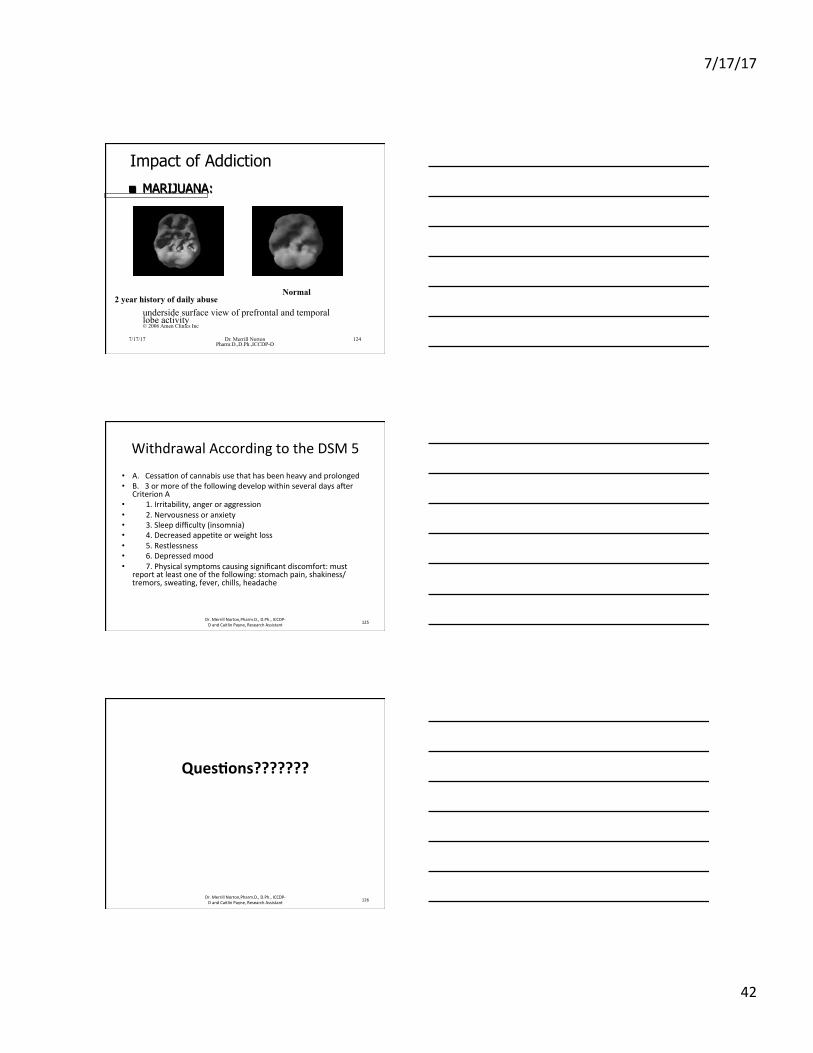
Impact of Addiction
■ MARIJUANA:
16 y.o. 2 year history of daily abuse
underside surface view of prefrontal and temporal lobe activity © 2006 Amen Clinics Inc
Normal
7/17/17 Dr. Merrill Norton Pharm.D.,D.Ph.,ICCDP-D
WithdrawalAccordingtotheDSM5
• A.Cessa8onofcannabisusethathasbeenheavyandprolonged• B.3ormoreofthefollowingdevelopwithinseveraldaysaeer
CriterionA• 1.Irritability,angeroraggression• 2.Nervousnessoranxiety• 3.Sleepdifficulty(insomnia)• 4.Decreasedappe8teorweightloss• 5.Restlessness• 6.Depressedmood• 7.Physicalsymptomscausingsignificantdiscomfort:must
reportatleastoneofthefollowing:stomachpain,shakiness/tremors,swea8ng,fever,chills,headache
125Dr.MerrillNorton,Pharm.D.,D.Ph.,ICCDP-DandCaitlinPayne,ResearchAssistant
Ques9ons???????
Dr.MerrillNorton,Pharm.D.,D.Ph.,ICCDP-DandCaitlinPayne,ResearchAssistant 126





























