Embed Size (px)
Citation preview

Formal Analysis, Policy Formulation, andEnd-Stage Renal Disease
April 1981
NTIS order #PB81-209769

Library of Congress Catalog Card Number 80-600161
For sale by the Superintendent of Documents,U.S. Government Printing Office, Washington, D.C. 20402

Foreword
This case study is one ofassessment, The ImplicationsThat assessment analyzes the
17 studies comprising Background Paper #2 for OTA’sof Cost-Effectiveness Analysis of Medical Technology.feasibility, implications, and value of using cost-effec-
tiveness and cost-benefit analysis (CEA/CBA) in health care decisionmaking. The ma-jor, policy-oriented report of the assessment was published in August 1980. In additionto Background Paper #2, there are four other background papers being published inconjunction with the assessment: 1) a document which addresses methodologicalissues and reviews the CEA/CBA literature, published in September 1980; 2) a casestudy of the efficacy and cost-effectiveness of psychotherapy, published in October1980; 3) a case study of four common diagnostic X-ray procedures, to be published insummer 1981; and 4) a review of international experience in managing medical tech-nology, published in October 1980. Another related report was published inSeptember of 1979: A Review of Selected Federal Vaccine and Immunization Policies.
The case studies in Background Paper #2; Case Studies of Medical Technologiesare being published individually. They were commissioned by OTA both to provideinformation on the specific technologies and to gain lessons that could be applied tothe broader policy aspects of the use of CEA/CBA. Several of the studies were specifi-cally requested by the Senate Committee on Finance.
Drafts of each case study were reviewed by OTA staff; by members of the ad-visory panel to the overall assessment, chaired by Dr. John Hogness; by members ofthe Health Program Advisory Committee, chaired by Dr. Frederick Robbins; and bynumerous other experts in clinical medicine, health policy, Government, and econom-ics. We are grateful for their assistance. However, responsibility for the case studies re-mains with the authors.
JOHN H. GIBBONSDirector
111

Advisory Panel on The Implications ofCost-Effectiveness Analysis of Medical Technology
John R. Hogness, Panel ChairmanPresident, Association of Academic Health Centers
Stuart H. Altman Sheldon LeonardDean ManagerFlorence Heller School Regulatory AffairsBrandeis University General Electric Co.
James L. BenningtonChairmanDepartment of Anatomic Pathology and
Clinical LaboratoriesChildrens Hospital of San Francisco
John D. ChaseAssociate Dean for Clinical AffairsUniversity of Washington School of Medicine
Joseph FletcherVisiting ScholarMedical EthicsSchool of MedicineUniversity of Virginia
Clark C. HavighurstProfessor of LawSchool of LawDuke University
Barbara J. McNeilDepartment of RadiologyPeter Bent Brigham Hospital
Robert H. MoserExecutive Vice PresidentAmerican College of Physicians
Frederick MostellerChairmanDepartment of BiostatisticsHarvard University
Robert M. SigmondAdvisor on Hospital AffairsBlue Cross and Blue Shield Associations
Jane Sisk WillemsVA ScholarVeterans Administration

OTA Staff for Background Paper #2
Joyce C. Lashof, Assistant Director, OTAHealth and Life Sciences Division
H. David Banta, Health Program Manager
Clyde J. Behney, Project DirectorKerry Britten Kemp, * Editor
Virginia Cwalina, Research AssistantShirley Ann Gayheart, Secretary
Nancy L. Kenney, SecretaryMartha Finney, * Assistant Editor
Other Contributing Staff
Bryan R. Luce Lawrence Miike Michael A. RiddioughLeonard Saxe Chester Strobel*
OTA Publishing Staff
John C. Holmes, Publishing Officer
John Bergling* Kathie S. Boss Debra M. Datcher
Patricia A. Dyson* Mary Harvey* Joe Henson
● OTA contract personnel

Preface
This case study is one of 17 topics being is-sued that comprise Background Paper #2 to theOTA project on the Implicatiom of Cost-Effec-tiveness Analysis of Medical Technology. * Theoverall project was requested by the SenateCommittee on Labor and Human Resources. Inall, 19 case studies of technological applicationswere commissioned as part of that project.Three of the 19 were specifically requested bythe Senate Committee on Finance: psychother-apy, which was issued separately as Back-ground Paper #3; diagnostic X-ray, which willbe issued as Background Paper #.5; and respira-tory therapies, which will be included as part ofthis series. The other 16 case studies were se-lected by OTA staff.
In order to select those 16 case studies, OTA,in consultation with the advisory panel to theoverall project, developed a set of selectioncriteria. Those criteria were designed to ensurethat
●
●
●
●
●
●
●
as a group the case studies would provide:
examples of types of technologies by func-tion (preventive, diagnostic, therapeutic,and rehabilitative);examples of types of technologies by physi-cal nature (drugs, devices, and procedures);examples of technologies in different stagesof development and diffusion (new, emerg-ing, and established);examples from different areas of medicine(such as general medical practice, pedi-atrics, radiology, and surgery );examples addressing medical problems thatare important because of their high fre-quency or significant impacts (such ascost );examples of technologies with associatedhigh costs either because of high volume(for low-cost technologies) or high individ-al costs;examples that could provide informativematerial relating to the broader policy andmethodological issues of cost-effectivenessor cost-benefit analysis (CEA/ CBA); and
examples with sufficient evaluable litera-ture.
On the basis of these criteria and recommen-dations by panel members and other experts,OTA staff selected the other case studies. These16 plus the respiratory therapy case study re-quested by the Finance Committee make up the17 studies in this background paper.
All case studies were commissioned by OTAand performed under contract by experts in aca-demia. They are authored studies. OTA sub-jected each case study to an extensive reviewprocess. Initial drafts of cases were reviewed byOTA staff and by members of the advisorypanel to the project. Comments were providedto authors, along with OTA’s suggestions forrevisions. Subsequent drafts were sent by OTAto numerous experts for review and comment.Each case was seen by at least 20, and some by40 or more, outside reviewers. These reviewerswere from relevant Government agencies, pro-fessional societies, consumer and public interestgroups, medical practice, and academic med-icine. Academicians such as economists and de-cision analysts also reviewed the cases. In all,over 400 separate individuals or organizationsreviewed one or more case studies. Although allthese reviewers cannot be acknowledged indi-vidually OTA is very grateful for- their com-ments and advice. In addition, the authors ofthe case studies themselves often sent drafts toreviewers and incorporated their comments.
These case studies are authored workscommissioned by OTA. The authors are re-sponsible for the conclusions of their spe-cific case study. These cases are not state-ments of official OTA position. OTA doesnot make recommendations or endorse par-ticular technologies. During the variousstages of the review and revision process,therefore, OTA encouraged the authors to present balanced information and to recog-nize divergent points of view. In two cases,OTA decided that in order to more fullypresent divergent views on particular tech-nologies a commentary should be added tothe case study. Thus, following the case

studies on gastrointestinal endoscopy andon the Keyes technique for periodontal dis-ease, commentaries from experts in the ap-propriate health care specialty have beenincluded, followed by responses from theauthors.
The case studies were selected and designed tofulfill two functions. The first, and primary,purpose was to provide OTA with specific in-formation that could be used in formulatinggeneral conclusions regarding the feasibility andimplications of applying CEA/CBA in healthcare. By examining the 19 cases as a group andlooking for common problems or strengths inthe techniques of CEA/CBA, OTA was able tobetter analyze the potential contribution thatthese techniques might make to the managementof medical technologies and health care costsand quality. The second function of the caseswas to provide useful information on the spe-cific technologies covered. However, this wasnot the major intent of the cases, and theyshould not be regarded as complete and defini-tive studies of the individual technologies. Inmany instances the case studies do represent ex-cellent reviews of the literature pertaining to thespecific technologies and as such can stand ontheir own as a useful contribution to the field. Ingeneral, though, the design and the fundinglevels of these case studies was such that theyshould be read primarily in the context of theoverall OTA project on CEA/CBA in healthcare.
Some of the case studies are formal CEAs orCBAs; most are not. Some are primarily con-cerned with analysis of costs; others are moreconcerned with analysis of efficacy or effec-tiveness. Some, such as the study on end-stagerenal disease, examine the role that formalanalysis of costs and benefits can play in policyformulation. Others, such as the one on breastcancer surgery, illustrate how influences otherthan costs can determine the patterns of use of atechnology. In other words, each looks at eval-uation of the costs and the benefits of medicaltechnologies from a slightly different perspec-
tive. The reader is encouraged to read this studyin the context of the overall assessment’s objec-tives in order to gain a feeling for the potentialrole that CEA/CBA can or cannot play in healthcare and to better understand the difficulties andcomplexities involved in applying CEA/CBA tospecific medical technologies.
The 17 case studies comprising BackgroundPaper #2 short titles and their authors are:
Artificial Heart: Deborah P. Lubeck and John P.Bunker
Automated Multichannel Chemistry Analyzers:Milton C. Weinstein and Laurie A. Pearlman
Bone Marrow Transplants: Stuart O. Schweitz-er and C. C. Scalzi
Breast Cancer Surgery: Karen Schachter andDuncan Neuhauser
Cardiac Radionuclide Imaging: William B.Stason and Eric Fortess
Cervical Cancer Screening: Bryan R. LuceCimetidine and Peptic Ulcer Disease: Harvey V.
Fineberg and Laurie A. PearlmanColon Cancer Screening: David M. EddyCT Scanning: Judith L. WagnerElective Hysterectomy: Carol Korenbrot, Ann
B. Flood, Michael Higgins, Noralou Roos,and John P. Bunker
End-Stage Renal Disease: Richard A. RettigGastrointestinal Endoscopy: Jonathan A. Show-
stack and Steven A. SchroederNeonatal Intensive Care: Peter Budetti, Peggy
McManus, Nancy Barrand, and Lu AnnHeinen
Nurse Practitioners: Lauren LeRoy and SharonSolkowitz
Orthopedic Joint Prosthetic Implants: Judith D.Bentkover and Philip G. Drew
Periodontal Disease Interventions: Richard M.Scheffler and Sheldon Rovin
Selected Respiratory Therapies: Richard M.Scheffler and Morgan Delaney
These studies will be available for sale by theSuperintendent of Documents, U.S. Govern-ment Printing Office, Washington, D.C. 20401.Call OTA’s Publishing Office (224-8996) foravailability and ordering information.

Case Study #1
Formal Analysis, Policy Formulation,and End-Stage Renal Disease
Richard A. Rettig, Ph. D.The Rand Corp.
Santa Monica, Calif.
AUTHOR’S ACKNOWLEDGMENTS
The author thanks the following individuals for helpful comments on an earlierdraft: Robert W. Berliner, M. D.; Benjamin T. Burton, Ph. D.; Nancy Boucot Cum-mings, M. D.; William de Cesare, M. D.; Joseph L. de la Puente; Richard B. Freeman,M. D.; Carl W. Gottschalk, M. D.; Thomas J. Kennedy, Jr., M. D.; Herbert E. Klar-man, Ph. D.; Irving J. Lewis; Charles L. Plante; George E. Schreiner, M. D.; DonaldW. Seldin, M. D.; and WiIliam H. Stewart, M.D. Remaining errors of fact are the re-sponsibility of the author. Interpretations, of course, are wholly the author’s respon-sibility.

Contents
PageIntroduction. , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
The ESRD Patient Population. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Formal Analysis Literature Pertaining to ESRD . . . . . . . . . . . . . . . . . . . . . . . . . . .
Formal Analysis and ESRD Policy Formulation . . . . . . . . . . . . . . . . . . . . . . . . . . .Report of the Committee on Chronic Kidney Disease . . . . . . . . . . . . . . . . . . .Kidney Disease Program Analysis: A Report to the Surgeon General . . . . . . .The Policy and Eureaucratic Contexts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Policy and Program Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table No.1. Age Distribution of Dialysis Patients and
Programs, March 1960-March 1967 . . . .2. Age Distribution of Dialysis Patients and
March 1963-March 1967. . . . . . . . . . . . .
Deaths in PHS-Supported
Deaths in VA
3. Patients Alive on Dialysis in the United States, 1970-764. Total Kidney Transplants Worldwide by Year, 1967-765. Medicare ESRD Patient Population, 1973-78 . . . . . . . .6. Predicted Caseload in Patient Years of Dialysis Under Varying Levelsof
Expected Cases of Chronic UremiaTransplantation, 3968-77 . . . . . . .
and Differing Amounts of. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7. Increased Life-Years and Costs per Additional Life-Year by Means ofTreatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8. Total Estimated Federal and Non-Federal Patient Care Costs of a NationalDialysis and Transplantation Program
9. HEW Cost Summary . . . . . . . . . . . . .10. Program Benefits . . . . . . . . . . . . . . . .
FIGURE
3
4
6
66
111820
22
23
Page
4
4555
10
11
121415
Figure No. Page1. Effect of the Advancing State of the Art on Future Program Composition . . . . . 16

Case Study #1:
Formal Analysis, Policy Formulation,and End-Stage Renal Disease
Richard A. Rettig, Ph. D.The Rand Corp.
Santa Monica, Calif.
INTRODUCTION
The past two decades have witnessed increas-ing use of formal analysis in Federal Govern-ment policymaking. Most strongly identifiedwith the Department of Defense in the early1960’s (8,15,16), formal analysis has now beenextended to all areas of domestic public policy,including health (35,36). The use of formal anal-ysis has also been extended from policymakingto program evaluation (44). In this case study,we analyze two instances of the use of formalanalysis in the formulation of Federal Govern-ment policy for end-stage renal disease (ESRD).
The term formal analysis, as used in thisstudy, refers to any explicitly analytical meansof systematically examining the social costs andbenefits of alternative policies for the purpose ofchoosing a preferred alternative in light of an apriori normative decision rule. Included arecost-benefit analysis (CBA), cost-effectivenessanalysis (CEA), risk-benefit analysis, technol-ogy assessment, and other comparable means ofanalysis used in decisionmaking.
Much attention is given in the literature aboutformal analysis for policymaking to the generaltechniques and limits of analysis (23,30) or theresults and implications of particular studies. Ofcritical importance, as well, however, are the in-stitutional factors encouraging or inhibiting theuse of formal analysis in policymaking. Theseinstitutional factors are a major concern of thiscase study.
This case study examines two instances of theuse of formal analysis in the formulation of Fed-eral Government policies toward ESRD.1 Its fo-cus is on the work of two committees, whose re-ports were an integral part of the ESRD policyformulation process in 1966 and 1967: 1) theGottschalk committee, advisory to the U.S. Bu-reau of the Budget (BOB), and 2) the Burtoncommittee, internal to the Public Health Service(PHS). Several questions are addressed. Whatfactors gave rise to the demand for formal anal-ysis within the policy process? What were thepurposes of and constraints on the analyses?What did the analyses conclude? How were theresults of these analyses used? What general les-sons can be drawn from this experience?
Background information about ESRD is pre-sented in the first section below. The subsequentsection contains a review of the literature per-taining to ESRD, emphasizing the two majoranalytical studies—the Gottschalk report andthe Burton report—which were pertinent to thepolicy formulation process. The role that thosetwo studies played in that process is then ex-amined in the next section. In the final section,we develop our conclusions.
‘The general evolutlon of Federal policy in the area ot ESRD hasbeen analyzed elsewhere (32, 33).

THE ESRD PATlENT POPULATION
Treatment of ESRD by hemodialysis began inearly 1960. By early 1967, according to esti-mates prepared by an advisory committee toBOB, approximately 750 to 1,000 patients hadbeen treated by dialysis (31).
Data on patients treated in PHS-supporteddialysis programs from March 1960 to March1967 are presented in table 1. These data indi-cate that roughly 90 percent of these patientswere distributed across the four age groups from15 to 54 years. They also show an overall mor-tality rate for these patients of 17 percent, withconsiderable variation in the mortality rates forspecific age groups.
Table 2 presents similar data for patientsreceiving dialysis in Veterans Administration(VA) hospitals from March 1963 through March1967. By comparison with the PHS data in table1, the data on these patients reveal a slightly
higher patient mortality rate, fewer younger pa-tients, and fewer elderly patients.
Time series data on dialysis began to be col-lected in 1970. Data from the National DialysisRegistry 2 are presented in table 3. These datashow: 1) the proportion of women in the totalpatient population increased from 32 percent in1970 to 40 percent in 1976; 2) the average ageclimbed steadily for both in-center and home di-alysis patients; and 3) the proportion of homepatients to total dialysis patients climbed to ap-
‘The National Dialysis Registry was managed by the ResearchTriangle Institute from 1967 through 1976, under contract to theNational Institutes of Health (NIH). The National Dialysis Regis-try was known to underreport the total U.S. dialysis population,because participation in the Registry was voluntary. Since the au-thorization of the medicare ESRD program in late 1972 created theexpectation that both the National Dialysis Registry and the Hu-man Renal Transplant Registry would be merged into a single sys-tem, it can be assumed that underreporting was exacerbated from1974 onward.
Table 1 .—Age Distribution of Dialysis Patients and Deaths inPHS-Supported Programs, March 1960-March 1967
-.P e r c e n t N u m b e r - Percent
Age group All patients total patients deceased deceased
Under 15 . . . . . . . . 3 - ‘-1 .2- 0 0.0-15-24 ., ., ., 42 17.0 7 16.725-34 ., 69 27.9 9 13.035-44 . . . . . . . . . 61 24.7 7 11.445-54 ... 52 21.1 13 25.055-64 . . . . . . . . . 18 7.3 5 27.8Over 65 . . . . . . 2 0.8 1 50.0
Total . . ... . . 247 ‘1 00.0 ‘42-” ‘- ‘ - 1-7,0
SOURCE Report of the Committee on Chronic Kidney Disease. September 1967
Table 2.—Age Distribution of Dialysis Patients and Deaths in VA HospitalsMarch 1963-March 1967
Percent Number P e r c e n t -
Age group All patients total patients deceased deceasedU n d e r 1 5 ,
—-0 0.0 0 0.0 ‘-
15-24 . . . . . . 8 3.5 2 25.025-34 . . . ... 54 23.4 9 16.735-44 . . ., 99 42.8 18 18.245-54 ., ., . . 62 26.8 14 22,65 5 - 6 4 . , . . . . . . 8 3.5 4 50.0Over 65 . . . 0 0.0 0 0.0
Total ., ., . . . 231 100.0 47 20,3
SOURCE Report of the Committee on Chronic Kidney Disease September 1967

Reportdated Jan. 1
1970.. .1 9 7 1 . . . , .1 9 7 2 , . 1 9 7 3 .1 9 7 41975 . . .1976 . .
Table 3.— Patients Alive on Dialysis in the United States, 1970-76
Total numberof patients alive
2,3983,4634,9817,498
10,30613,41717,063
Numberof men
1,6212,2563,2124,7416.3348,231
10,156
Numberof women
7621,1841,7512,6963,8715,0986,783
Number in Average age
home program In center patients Home patients
844 39 411,361 40 422,001 42 432,703 44 453,402 44 433,814 45 444,076 46 45
SOURCE Research Triangle Institute National Dialysis Registry, Final Report. August 1976
proximately 40 percent in 1971 and 1972, anddeclined steadily thereafter to 24 percent in 1976(4). (By 1979, home dialysis patients accountedfor approximately 13 percent of the total dialy-sis patient population. )
Worldwide data on kidney transplants fromthe early 1950’s through May 1, 1976, areshown in table 4. Based on the Human Renal
Transplant Registry, ’ these data show a fairlystable number of transplants being performed inthe United States since 1972 (l).
Table 4.— Total Kidney Transplants Worldwide by Year, 1967-76’
1953-66 1967 1968 1969 1970 1971 1972 1973 1974 1975 1976 Total
U n i t e d S t a t e s 1,146 462 702 872 1,139 1,676 2,232 2,417 2.218 2,399 438 15,701Canada 93 64 83 83 126 200 165 211 177 72 – 1,274Australia (to 4/30/75) 55 95 128 203 203 263 242 292 317 115 — 1,913Other count r ies . 426 211 332 381 524 778 862 925 994 787 — 6,220
Total 1 , 7 2 0 8 3 2 1,245 1.539 1,992 2,917 3,501 3,845 3,706 3,373 438 25,108
a I nc I udes al I t ransp I ants recorded u p to Ma, 1 19 ?6Tc)Ial trdnsplanl~ 25108Total re[ I p lents 22261
S O U R C E Amerlc dn Colleqe 01 Ptl’/\lctan~ Na! lundl Insf!tljte, ~f Healt II Orqan Trdns~)lant Rey(>tr! Mdk IVP,} L,/PIIe( 7976
Medicare coverage for ESRD treatment byboth dialysis and transplantation has beenavailable for more than 90 percent of the U.S.population since July 1, 1973. The number ofpatients in the medicare ESRD program from itsinception in 1973 through 1978 is shown in table5. The proportion of patients 65 years old andabove in the medicare ESRD patient populationhas increased from 5 percent in 1974 to basically20 percent in 1977 and 1978.
The establishment of a data system for pro-viding accurate, consistent, and timely data onESRD patients has proved to be an extremelydifficult task (32). The single Medicare Registry,which was to have combined both the NationalDialysis and Human Renal Transplant Regis-tries, existed briefly from 1975 through 1978 asa contractor-managed system, and it issued re-ports only in December 1976. The management
contract for that Registry was terminated in1978, and responsibility for the ESRD MedicalInformation System was transferred from theBureau of Quality Assurance of PHS to theMedicare Bureau of the Health Care FinancingAdministration (HCFA). The new system beganto issue reports in 1979.
Table 5 .—Medicare ESRD Patient Population1973-78
End of calender year Total number of patients
July 1, 1973a ., 11,0001973. , . : 14$0001974 ..., . . . . 23,0001 9 7 5 . 31,0001976 : , : : : ., . . 38,0001977 44.0001978 50,000
‘1 nce~) t Ion of proq ram
SOURCE Of fire of F[nanc{dl and Acli~arlal Anal, SIS DI\ islon of Mec!(care CrJstEstimates Health Care FIndn(Incj A!mnl\trat(on March 1979

FORMAL ANALYSIS LITERATURE
In 1967, two reports were published whichconstitute the primary formal analyses pertain-ing to ESRD. One of these reports, often knownas the Gottschalk report,4 was the work of anexpert advisory committee to BOB (31 ). Theother report, known as the Burton report, 5 wasthe work of a PHS task force which reported tothe U.S. Surgeon General (17). Work on theGottschalk report was begun in mid-1966 andcompleted “1 year later. The Burton report wasprepared in 4 months in 1967. The two reportswere released together in November 1967, at apress release called by PHS.
A derivative literature is associated with eachreport. Herbert Klarman, an economist whoserved on the Gottschalk committee, subse-quently wrote abou: that committee’s effort inseveral articles (18,19,20). Similarly, RobertGrosse briefly discussed the Burton report to theSurgeon General in several papers describingthe Health, Education, and Welfare (HEW) pro-gram analyses in health done in the 1965-67period (1 1, 12, 13).
A set of analyses on kidney disease was per-formed by Research Triangle Institute} (RTI).
PERTAINING TO ESRD
RTI’s initial report to the Kidney Disease Con-trol Program of PHS was prepared under a con-tract effective June 27, “1966 (14). A subsequentpaper set forth the methodology for conductingbenefit-cost analysis of kidney disease (10). Thefull report on work performed under RTI’s con-tract was published later in 1968 (21). All thiswork was either supported by or derived fromthe Burton committee’s efforts.
Several other formal analyses have also beendone. Pliskin, for instance, developed a healthindex for the selection of chronic renal diseasepatients (27) and a methodology for projectingneeded hemodialysis beds (28). Barnes pre-sented a simplified model of treating patients onchronic hospital dialysis, chronic home dialysis,living donor transplantation, and cadaver do-nor transplantation (2). Recently, Stange andSumner have compared expected life-yearsgained from and costs of treatment by center di-alysis, home dialysis, and transplantation (41).
In addition, there area few other brief formalanalyses that attempt to compare the costs andeffectiveness of the several means of treatmentfor ESRD. These add little that is new by way ofdata, methodology, or results to the literaturecited above, however, and since the focus of thepresent study is on the institutional factors in-fluencing the use of formal analysis, attention isdirected mainly to the Gottschalk and Burtonreports respectively.
FORMAL ANALYSIS AND ESRD POLICY FORMULATION
In the more than 15 years during which Fed- Report to the Surgeon General (the Burton re-eral policy toward ESRD has developed, cost port) (17). These reports stimulated furtheranalyses have always been central to policy for- analyses and also provided guidance to action.mulation. But only on one occasion have otherforms of analysis been integral to the policy Report of the Committeeprocess. In 1966 and 1967, two efforts were on Chronic Kidney Diseasemade to apply CEA to kidney disease. Thereports that resulted have already been men- The need for a review of Federal policies andtioned: 1) Report of the Committee on Chronic programs related to ESRD was forcefully under-Kidney Disease to BOB (the Gottschalk report) lined for BOB by several events in 1965 and(31), and 2) Kidney Disease Program Analysis: early 1966. First, VA submitted a budget request

to BOB for construction funds to create dialysisunits in a number of VA hospitals and for addi-tional funds to staff these units. VA’s requestprompted BOB to ask the Office of Science andTechnology about the possibility of an externalreview of the VA dialysis program. That Officeagreed that such a review would be useful, buturged that it include all Federal Government ef-forts in ESRD.
The attractiveness of such a review was re-inforced when NBC News, on November 28,1965, presented a l-hour television documen-tary, “Who Shall Live?” (26). Narrated by Ed-win Newman, that program dramatically con-trasted the lack of funds for dying individualsneeding dialysis treatment to the hundreds ofmillions of dollars being spent for exploration ofouter space and major weapons systems. New-man concluded the program by observing:“What is wrong is that a medical miracle hasbeen achieved and we refuse to face its implica-tions. We continue to argue over where themoney is coming from—and we have the mon-ey. ” Representative Melvin Laird (R., Wis. ),then ranking Republican member of the Houseappropriations subcommittee for HEW, wasquoted: “We’re spending billions of dollars toget to the moon, and it seems to me that thesehuman problems, which we have right here onearth, need to be solved. ” BOB, the Office ofScience and Technology, and the White Houseall recognized that public pressures for moreFederal funding of dialysis were building.
The expansion of dialysis-related activitieswas being actively promoted within PHS. Dr.James Kimmey, chief of PHS’s Renal DiseaseActivity Branch, Division of Chronic Diseases,supported by certain congressional and medicalallies, was advocating a dialysis program thatwould grow to an eventual level of $150 millionannually. In March 1966, however, BOB staffdiscovered that Kimmey’s plan had not consid-ered either the VA program or the offsetting ef-fects of providing transplants to some patients,although it did acknowledge that some dialysispatients would die (24). The need for a Govern-ment-wide review seemed increasingly clear.
In early 1966, therefore, BOB organized anadvisory committee of outside experts to review
Federal activities in dialysis. Dr. Carl Gott-schalk, University of North Carolina, agreed tochair the committee and helped select the mem-bers from medicine, science, and ethics; BOBselected Klarman and Gerald Rosenthal, theeconomists. 6 The Gottschalk committee metseven times from July 1966 through May 1967,and submitted its report (31) to CharlesSchultze, BOB director, in September 1967; thereport was released to the public in Novemberof the same year.
Central to any analysis is its purpose. BOB’scharge to the Gottschalk committee was not ful-ly articulated at the outset, but instead evolvedover several months. Two concerns were fore-most to BOB. One was national policy makers’substantial interest at that time in realizing clin-ical payoff from the Nation’s large and continu-ing investment in biomedical research. That in-terest was dramatized on June 27, 1966, whenPresident Lyndon B. Johnson called the Directorof the National Institutes of Health (NIH) andthe directors of the individual institutes of NIHto the White House to ask pointedly about thepractical benefits the Nation was receiving fromNIH-supported biomedical research (42).
BOB’s second concern was to involve itselfearly in decisionmaking about new medical pro-grams, especially those having major resourceimplications, so that policies could be shapedfrom a national perspective. Within BOB, Irv-ing Lewis, Chief of the Health and Welfare Divi-sion, recalls: “We were very troubled by the VArequest. There was a VA program, there was aPHS program, but there was no national ap-proach to the problem” (22). The advisory com-mittee of experts was convened to help BOBdevelop a national approach to ESRD.
h l e m b t ’ r e n l n l l t t{e t hat f~~)fl (lr~anlzt’li n t’rt’ I )r lit!nard Anl(~>. I>u At’ l] n I t’(’r~l t \ I ~r I t’t~ I \ ~\’ 131 u(’m It ~ \ n Ii’ t’ r~l t \ ~~tl’t’nn~t’lvanl~ I)r \~’lllitlnl A [;rt’~’nt’ ( rll~~’r>it \ t~t 1<(~( ht’>tt’r])r [ {t,rbt,rt Kldrman l,)hn~ l+t)pkln~ IInlt(rs[t \ 1 )r l(Ihn > ~’]I<jr]<jn lln]i,t,r~]t~ t)t (- .Illt{)rnla S.]n [.r.inc IW {) [)r (;t,rald l<ow,n-t h a t l}rclndt’]~ L lnltt’r~ll \ t)w a r hl I<ut’bhauwn 1~(’1’i’~’1~~’l’llmpt(~n, Ly(}ns, and Ca tes, New York, Dr C,e[~rge E. Sch rel nerG(Jrgetown Unl\’ers]ty, and I>r. D(~naId W’ Selciin Unr\ft>rsitv (ltTexa\, Dallas. The advl~(~rs to the c(>mmlt tee were Dr Robert \\’Berllner, Natl(~nal Heart In\t]tutt’ [>r Bernard Greenberg Unl\fer-\I t ~’ (}I Nor-t h C-a rol ln~ and Dr Arnold S Nash, Llnr ~’er~l t y (ltN’orth C~r(~llna T h e BOEl pr(lte>~l(~nal ~upp(~rtlng the c(lmmlttt’c’wa~ Plerrc S [’almtr h e rcp(~rted to I r v i n g I l.ew’1~ Ch]et (~fIKIU s Ht’alt h ancj \3’elf art, [l(t’l+i(~n

BOB expressed its two primary concerns atthe Gottschalk committee’s initial meeting inJuly 1966, but clear definition of the committee’smission came later. The committee’s Octobermeeting involved conversations with visiting
foreign physicians attending the InternationalCongress on Nephrology. In November, thegroup visited Dr. Belding H. Scribner, a pioneerin treating kidney failure by hemodialysis, inSeattle to learn about home dialysis and talk topatients. Not until the December meeting, how-ever, did BOB’s charge to the committee comeinto sharp focus.
Some on the committee wished to conduct aCBA addressing the relative priority “of in-vesting resources in treatment of chronic kidneydisease as against other needs in the health field”(37). One suggestion was to convene a group ofhealth generalists to consider alternative claimson resources. A majority of those on the com-mittee, however, held that determination ofpriorities rested with the Surgeon General, theSecretary of HEW, the BOB Director, and thePresident. Irving Lewis, responding to an in-quiry from his BOB staff, concurred: “I thinkthis is right. They should, however, give prior-ities within kidney disease.”7
The Gottschalk committee’s report, conse-quently, focused on those individuals withchronic kidney failure who required treatmentby hemodialysis or kidney transplantation (31).These two forms of treatment, it said, “are nowavailable as fruits of research and developmentprograms and are life-saving.” Though by nomeans optimal, these treatments could add asignificant number of years to the lives of in-dividuals “now dying because these treatmentforms are not generally available. ” The cost-effectiveness section of the Gottschalk reportelaborated the reasons for not doing CBA, orweighing the funds used for treating chronickidney failure against alternative uses of re-sources. The basic problem with CBA, it noted,was placing a value on human life. Further-more, the report said, “in the absence of over-whelming costs (as reflected by an appreciable
‘Klarman recalls that he and R(wenthal spent much time in 1967attempting, wlth(~ut success, t[~ prepare a CBA,
fraction of the GNP), ” treatment for ESRDshould be made universally available (31):
The reasons for this decision are the irrever-sibilit y of the decision not to do so, as far as anindividual is concerned; the existence for thefirst time of a technology capable of prolonging
the lives of persons otherwise doomed to anearly death; the relative youth of these persons;the prospects of further improvements in tech-nology; and the fact that patients are known andidentifiable, not members of a statistical distri-bution, enhances the community’s interest indoing somethin g in their behalf.
The committee’s CEA took as it point ofdeparture the committee’s conclusion andrecommendation that treatment be provided toall in medical need of it.
The Gottschalk report also dealt with theissue of prevention versus treatment. In trans-mitting the report to BOB Director Schultze,Gottschalk wrote (31):
Prevention is obviously preferable to treat-ment of disease. Unfortunately, knowledge con-cerning the causes and prevention of end-stagekidney disease is limited and this is an area inwhich an expanded research effort is required.Furthermore, even if a completely successfulmethod of prevention is developed it will haveno significant impact on the numbers of peopledying from end-stage kidney disease for manyyears. Therefore, the Committee recommends anational treatment program aimed at providingchronic dialysis and/or transplantation for all ofthe American population for whom it is medical-ly indicated.
The conclusions of the committee’s reportwere the following: 1) the high cost of ESRDtreatment required Federal financial assistance;8
2) ESRD treatment should be universally avail-able, not arbitrarily provided, say, to veterans,but denied to nonveterans; and 3) the Federalcommitment to ESRD treatment necessarily hadto be a continuing one. The Gottschalk commit-tee also concluded that continuing medical re-search into the causes of kidney disease and
‘This conclusion was based on written and oral testim{~ny re-ceived by the committee tr(~m LOUIS Reed, %clal Security Admln-istra tion, and from representatives of all major health insuranceplans.

means of prevention was needed, though it didnot consider this issue at any length.
The recommendations that followed fromthese conclusions dealt with the supply of anddemand for ESRD treatment, and the manage-ment of Federal efforts in this area. On the sup-ply side, the Gottschalk committee recom-mended Federal investment in establishing com-prehensive kidney centers and satellite com-munity dialysis units, as well as in traininghealth professionals to staff such facilities. Onthe demand side, its recommendation was toprovide for patient care financing by amendingtitle XVIII (medicare) of the Social Security Act.Specifically, the committee recommended enact-ing the Johnson administration’s p e n d i n g
amendment to extend medicare coverage to thedisabled under 65 years of age and redefiningdisabled to include those with kidney failureeven though they might continue to work as aresult of treatment. On Federal management, itsuggested “an appropriate mechanism” for coor-dinating governmental efforts.
The formal analysis in the committee’s reportincluded sections on treatment by hemodialysisand by transplantation, a discussion of the in-cidence and prevalence of chronic kidney fail-ure, a projection of treatment needs, and CEAitself (31). The hemodialysis section addressedpatient selection criteria. Ideal candidates forhemodialysis were then thought to be personsbetween 15 and 45 years of age, the upper agelimit was expected to rise, however, and foranalytical purposes, the committee used a 54-year upper age limit. Vascular diseases as med-ical conditions limiting treatment were brieflydiscussed, as were the limits of dialyzingchildren. It was also noted that the degree ofrehabilitation of dialysis patients varied widely;existing data were of little use on the matter. Itwas expected that psychosocial problems of pa-tients adapting to dialysis would increase asselection criteria were relaxed.
PHS and VA data were analyzed for some in-dication of mortality. Later in the analysis, pro-jections would be based on 15-percent mortalityof a dialysis population cohort in its first year,and a 10-percent mortality in each successive
year. ’ Costs for 16 center dialysis programsranged from $10,000 to $21,000 per patient peryear. Five home dialysis programs had costsranging from $3,750 to $9,800 per year.
The section on transplantation outlined astrong case for that treatment relative to dial-ysis. The report noted an important shift overtime in organ donor source—from identicaltwins to close blood relatives to nonliving (ca-daver) donors. Cadaver organs, it said, were be-coming the most important source of organs,owing in part to high success rates with them.
Worldwide mortality data from the HumanRenal Transplant Registry, however, showedthat survival rates declined with the shift fromidentical twins to siblings to parents to un-related living donors to cadavers (25). The bestl-year survival rate for cadaver kidneys was 38percent. The report concluded that these world-wide data were of little predictive value, how-ever, since they included the early experimentalstage of transplantation. The report used onlydata for the 2 most recent years, broken downby large and small transplantation centers.These data showed l-year kidney survival ratesof 65 percent for sibling donors and 39 percentfor cadavers transplanted in large centers, re-sults deemed “noteworthy” and “very encour-aging. ”
The committee’s optimism about the future ofrenal transplantation was based on two subsetsof data from the Human Renal Transplant Reg-istry. The first excluded all deaths save those re-sulting from uncontrollable rejection: 3-yearsurvival rates for siblings and parents were 70percent and over 60 percent for cadavers. Thesecond set included deaths from rejection andinfection: l-year survival rates were 66 percentfrom close relatives and 54 percent from cadav-er kidneys. The committee’s report found it “im-pressive” that projections for fifth year survivalfor all cadaver kidneys, “if technical failures anddeaths due to causes other than infection or re-jection are excluded, ” were 40 percent. The fu-
by Bernard Greenberg.detailed survivorship

10 . Background Paper #2: Case Studies of Medical Technologies
ture prospects for transplantation, the reportsuggested, were the following (31):
From the subsets it is possible to extrapolatewhat might be expected from continuing experi-ence and excellent management with existingmethods of treatment, i.e., between 65 percentand 75 percent l-year survival for a closely
related donor, between 40 percent and 50 per-cent survival for a cadaver donor. Additionalknown factors expected to improve the resultsfurther are (a) selection of antigenically compati-ble donors, (b) improved immunosuppression,and (c) the induction of specific immunologictolerance.
Several features about these projections forkidney survival deserve mention. First, no esti-mates of the magnitude of the shift from livingto cadaver donors were given in its report; norwere different projections developed for differ-ent degrees of shift. Second, the two subsets ofRegistry data on which the projections werebased were not published. Finally, it was neverclearly indicated how the assumptions based onthese data subsets were used in the later CEA.
These matters are important because the op-timism about transplantation, based on experttestimony heard by the committee, was neverfully realized. One-year survival for cadavertransplants subsequently reached 55 percent in1970 and then declined slightly (1,43). At thetime of the committee’s report, there were fewwho questioned the assumption that successwith transplantation would improve with time.
Reported costs for transplantation from fourcenters ranged from $10,000 to $22,000, in-cluding preoperative and postoperative dialysiscosts. One center reported an average cost of$13,300 for its 46 most recent transplants, andthe Gottschalk committee judged that as the“most valid estimate. ”10
The report contained a long section on inci-dence and prevalence of chronic kidney failure.Noting the absence of any periodic reporting onthis disease, the Gottschalk committee devel-oped two estimates of the potential dialysiscases for 1964, and from these derived an upperlimit, lower limit, and most probable annual di-alysis caseload. Mortality estimates were de-rived from actual data on dialysis: 15 percentmortality in the first year; 10 percent for eachsuccessive year. The kidney transplant failurerate was estimated to be 50 percent annually forthe first 2 years and 5 percent each year there-after. Projections of the dialysis caseload for thedecade from 1968 through 1977 were made onthe basis of varying levels of chronic kidney fail-ure and varying numbers of patients trans-planted. These projections are shown in table 6.If one compares the 1977 dialysis caseload formaximum level of transplantation and lowestlevel of total cases (29,201) with that for notransplantation and the maximum number of di-alysis cases (53,633), it is obvious that projec-
IOKlarman developed this estimate during a visit to Dr. David
Hume, one of the kidney transplant pioneers, at the Medical Col-lege of Virginia in Richmond.
Table 6.—Predicted Caseload in Patient Years of Dialysis Under Varying Levels of Expected Casesof Chronic Uremia and Differing Amounts of Transplantation, 1968-77
—Probable number Maximum number
No transplantation, and of transplantations, and of transplantations, andnumber of cases is: number of cases is: number of cases is:
Most MostYear Lower
Mostprobable Upper Lower probable Upper Lower probable Upper
1968 . . . . . . 5,530 6,436 7,541 – 5 , 3 5 4—
6,261 7,365 5,333 6,2391969 . . . . . . 10,470
7,34412,187 14,279 9,982 11,698 13,790 9,914 11,636 13,722
1970 . . . . . . 15,038 17,503 20,506 14,158 16,624 19,626 14,037 16,503 19,5061971 . . . . . . 19,265 22,423 26,269 17,914 21,071 24,917 17,588 20,747 24,5921972 . . . . . . 23,191 26,994 31,624 21,293 25,096 29,727 20,584 24,3871973 ....., 26,847 31,252
29,01736,611 24,325 28,728 34,088 23,141 27,544
1974, . . . . . 30,265 35,22932,905
41,272 27,016 31,979 38,021 25,300 30,2631975 . . . . . . 33,468
36,30538,956 45,638 29,367 34,856 41,538 27,043 32,532 39,213
1976 . . . . . . 36,482 42,463 49,747 31,382 37,363 44,648 28,354 34,334 41,6201 9 7 7 . . . , 39,332 45,779 53,633 33,053 39,498 47,351 29,201 35,649 43,505
— — — . . — — - — — — .SOURCE Report O( the Corrrrrr/ffee on Chronic Kfdney Dsease, September 1967

tions vary substantially as a consequence oftheir underlying assumptions. Such wide varia-tion can obviously affect planning for facilities,if program decisions are to be based on the pro-jections.
The heart of the Gottschalk report’s CEA wasa comparison of the expected life-years addedby transplantation and by dialysis with thepredicted costs of each. The critical assumptionsfor transplantation were the 50-percent kidneysurvival at the end of 2 years and a 5-percentannual failure rate thereafter. On the basis ofthese assumptions, transplantation led to an ex-pected 17 additional life years (13.3 from trans-plantation and 3.9 from dialysis before and aftera transplantation). Dialysis, on the other hand,based on a 15-percent first year mortality andlo-percent for each successive year, led to an ex-pected 9 additional life-years.
The present value costs of 17 years of addi-tional life from transplantation were calculatedto be $44,500. The comparable present valuecosts of 9 additional life-years from dialysiswere calculated to be $104,000 for center dialy-sis and $38,000 for home dialysis; if there were a50-50 split between the two, the average esti-mated cost for dialysis would be $71,000. (Thepresent value estimates were based on 4- and 5-percent discount rates, respectively, for centerand home dialysis. )
The results of the comparison are presented intable 7. An adjustment for quality of life wasmade for transplantation based on the observa-tion that an additional year of life from a suc-cessful transplantation is much better (1.25
Table 7.— Increased Life-Years and Costs perAdditional Life-Year by Means of Treatment
Life-years costModality cost gained per year
D i a l y s i sCenter. . . . . . $104,000 9 $11,600Home. ... . . . 38,000 9 4,200A v e r a g e . . . . 71,000 9 7,900TransplantationUnadjusted. . . . . . 44,500 17 2,600Adjusted for quality. 44,500 20.5 2,200
—S O U R C E Report 01 fhe Commlltee on Chronic Kldr7ey f)(sease September
1967
times better) than an additional life-year fromdialysis.
The conclusions of the Gottschalk report’sCEA, not surprisingly, were these: 1) The max-imum transplantation course was a better wayto increase life expectancy for a given cost; 2)the value of a home dialysis program did notdiffer much from that of transplantation, em-phasizing the proportion of transplantationcosts attributable to dialysis; and 3) any shift inthe dialysis population away from center dialy-sis and toward home dialysis offered substantialeconomic gain.
The committee’s recommendation, therefore,was for a national treatment program aimed atbuilding adequate treatment capacity and pay-ing patient bills. Within that policy, the com-mittee said, transplantation should be encour-aged to the maximum extent possible, and homedialysis should be encouraged over centerdialysis,
The estimated total costs, including both Fed-eral and non-Federal funds, for the patient careportion of the national dialysis and trans-plantation program recommended by the Gott-schalk committee were $40 million (low) and$49 million (probable) for fiscal 1970, the firstyear, and $157 million (low) and $205 million(probable) for fiscal 1974, the fifth year. Thecommittee’s table summarizing the cost esti-mates is reproduced as table 8. Estimates fortotal patients treated by both dialysis andtransplantation were 3,662 in the first year and18,500 in the fifth. The estimated costs to theFederal Government, from fiscal years 1969through 1975, for construction or renovation,initial equipment, operating subsidy, and train-ing personnel for kidney centers and communitydialysis units, respectively, were $29 million,$22 million, $30 million, $30 million, $22 mil-lion, $23 million, and $15 million.
Kidney Disease Program Analysis:A Report to the Surgeon General
In the early 1960’s, under Defense SecretaryRobert McNamara, CEA was introduced intonational security decisionmaking with a flour-ish. In 1965, Henry S. Rowen left his position as

In-center dialysis
Cost/ - ‘EstimatedPatients patient Costa
Fiscal year treated year ( $ 0 0 0 , 0 0 0 ).1970Low estimate 1,456 $10,000 $15Probable . . . 1,456 “14,000 201971Low estimate 2,194 “ 0,000 22Probable . . 2,194 14,000 311972Low estimate 3,731 10,000 37Probable 3,731 14,000 527973Low estimate 5,878 10,000 59Probable 5,8781974Low estimate 7,575Probable 7,5751975Low estimate 8,925P r o b a b l e 8,925
aRounded to nearest m(lllon
4,000 82
0,000 764,000 106
0,000 894,000 125
Home dialysis Transplantations Total program
Cost/ Estimated Cost/ Estimated EstimatedPatients patient cost a Patients trans- Costa Patients cost a
treated ‘ year ($000,000) treated plant ($000,000)l treated ($000,000)— .
1,4561,456
2,1942,194
3,7313,731
5,8795,879
7,5767,576
8,9268,926
$4,000 $17 750 $10,000 $ 85,000 19 750 13,000 10
4,000 16 1,250 10,000 135,000 18 1,250 13,000 16
4,000 30 1,750 10,000 185.000 34 1,750 13,000 23
4,000 45 2,550 10,000 265,000 51 2,550
4,000 47 3.3505,000 55 3,350
4,000 49 4,1505,000 58 4,150
3,000 33
3,6623,662
5,6385,638
9,2129,212
4,3074,307
0,000 34 18,5013,000 44 18,501
0,000 42 22,0013,000 54 22,001
$4049
5165
85109
130166
157205
180237
bBa~ed on ~pp c ~ables do ~n(j 41 Ex,:lu[je5 ~atlent ~edr5 of dla IySl~ rleeded for [ransplanfs (table d 1 I because the COSt of th(s dtalysls IS Included In the cost per traOS
plantation For 197375 the numl)er of pal,enl years o! dlalysls for new cases orglnatlng (n these years have been deducted because they are capability rather than requlrements they have beer replaced by mo>l probable number of new pal (ents need)ng d(alys{s (table 40) translated to patlenl years by using 925 percent the firstyear 872 percenl second y~ar dn(i 876 percent thlr(j y ear
cFrom table 3dlncludes ,n[tlal home dlalys(s e(lulpn)ent dnd Ira(n(ng costs of $lIJ 000 for new pat(~nts on home d(alys(s 1970 $,11 ‘2 rn!(l(on 1971 $74 mllllon 1972 $154 fnltllorl
1973 $21 5 mill ton 1974$17 ml Ijon 1975 $135 m[ll Ion Assumes that equ lpment provided for home d(alyws patients who have d(ed or been transplanted WIII bemade aval I able for new pat Ients :,larl I ng on home d{aly S(S
SOURCE Reporl of ffie Cornrn/(/e? on Ctrrorr/c K/drrev D/sease September 1977
Deputy Assistant Secretary of Defense for Sys-tems Analysis to become the Assistant Directorof BOB. In that position, aided by a formal dec-laration from President Lyndon B. Johnson, hepromoted the use of CBA and CEA throughoutthe domestic agencies of the Federal Govern-ment. Also in 1965, John Gardner became theSecretary of HEW and took a number of steps toincrease his control over the far-flung HEWbureaucracy. One step was to create the posi-tion of Assistant Secretary for Planning andEvaluation to do for HEW what the systemsanalysts had done for the Defense Department.The f irst occupant of that post , Will iamGorham, came from the Pentagon. Early in1966, Gorham and his staff sought to promotethe use of CEA and CBA in HEW (34).
In response to these developments at HEW,the U.S. Surgeon General, William H. Stewart,in March 1967 established health program anal-ysis groups to address disease control issuesrelated to air pollution, cancer, health care
facilities, kidney disease, manpower, and nar-cotic addiction.11 For each issue, these groupswere to discuss: 1) goals and objectives andways of measuring them; 2) alternative ap-proaches to the same objectives; 3) the cost “ofreaching various points on the continuum of ob-jectives by means of alternative approaches;”and 4) assumptions underlying conclusions, theuncertainties affecting the estimates, and theissues not resolvable at that time. Each alter-native approach was to consider “the relativemix of research, prevention, and control. ” Theprogram analysis groups were to complete theirwork by May 30, 1967, and the resulting reportswere to guide the development of the HEW’s1969-1973 5-year program and financial plan, aswell as the fiscal 1969 budget and legislativeproposals (9).
‘ A l~be l)r~~~r,]m Nlemt)rdndum ~)n St’!c’c ted I)Iwase ~ontro]”l’r(lgrdm~, drafted I }rt’c~r c’c]rllc’r, w<i~ c I ted ds dn cxcrc iw t () gal nt’xpc>r]enc e I n ~ppl yi ng t] n.] I y’ t ]ca 1 met h(d~ t () t hl~ \t ULIII L)} d lwawcon t rol progrc] ms.

The kidney disease program analysis group,chaired by Dr. Benjamin T. Burton, was com-posed of individuals from various parts ofPHS.12 Its charge from the Surgeon General wasa general one given to all the program groups.The kidney disease group, therefore, translatedthis general guidance into a charge to perform“a logical analysis of programs leading to asolution or amelioration of the problem of kid-ney disease” (17). The group identified tradi-tional disease control mechanisms for such atask as prevention, diagnostic and therapeutictechniques, laboratory and clinical research,manpower training, public education, and theconstruction of specialized facilities. It made theassumption that no “single program componentwould lead to a major reduction in the nationalkidney disease problem, ” so a mix of ap-proaches would have to be employed. It furtherassumed that “unlimited Federal funds” werenot available for any given disease problem,such as kidney disease; therefore, “a rationalbalance” had to be struck between various ap-proaches “to derive maximum benefits from anycurrent or possibly extended future Federal ef-forts. ” These controlling assumptions affectedthe definition of the problem for analysis, theanalysis itself, and the implications of theanalysis.
The Burton report to the Surgeon General(17) was organized into six chapters: the sum-mary of the report and chapters dealing suc-cessively with the major types of kidney disease;current kidney disease control programs, bothFederal and non-Federal; research methods; theprogram analysis; and the cost of treating all pa-tients with chronic kidney failure.
The Burton group’s analysis was based on abreakdown of kidney disease into four primarytypes:
1. infectious diseases,2. hypersensitivity diseases,3. diseases associated with hypertension,
and4. end-stage disease.
The progression of each of the first three typeswas to the same functional equivalent—end-stage—where irreversible deterioration of kid-ney function had proceeded so far that un-treated individuals would die.
Each of the four types of kidney disease wasanalyzed in terms of four hypothetical pro-grams, delineated by time, funding level, andstate of clinical practice. The four different pro-grams were described as follows (17):13
1.
2.
3.
4.
hypothetical program at the current HEWexpenditure level (essentially $47 million),based on the current state of the art;hypothetical program at an intermediateHEW expenditure level (roughly 21/2 timesthe current level), based on the currentstate of the art;hypothetical program at an acceleratedHEW expenditure level (roughly six timesthe current level), based on the currentstate of the art; andhypothetical program for fiscal year 1975,at “an accelerated HEW expenditure level(roughly six times the current level), basedon the expected advanced state of the artin 1975.
Within each of the resulting 16 analyses, atten-tion was given to “a rational mix of programcomponents” —prevention, diagnosis and treat-ment, research, training, and facilities. Thefourth program, it should be noted, was basedon numerous assumptions about scientific andclinical progress by 1975; it is highly sensitive tothose assumptions and consequently its projec-tions are not discussed below.
‘ ‘Freemdn recd]]~ that the intermediate’ prqectlons were c]oseto redl number~ and the ‘ decelerated project l(~ns were t(~tdl]vILkd]L?eLi

14 . Background Paper #2: Case Studies of Medical Technologies
The estimated annual costs to HEW are lion, and $813 million. (All cost figures are inshown in table 9 below. The totals for each of constant 1966 dollars. )the four resource levels, respectively, are $47million, $117 million, $290 million, and $293 Short- and long-term benefits from these vari-million. The corresponding total annual nation- ous expenditure levels were estimated. Short-al costs including HEW costs (not shown in the term benefits were calculated for reductions intable) are $241 million, $333 million, $526 mil- annual mortality, number of new cases, and
Table 9 .— HEW Cost Summary (in thousands of dollars)
Program level Infectious Hypersensitivity Hypertensive End-stage cost Percent—Current expenditure Ievelb
Diagnosis, prevention, treatment:Prevent ion (including education
and administration) . . . . . . . . . . . $3,803 $1,500 $4,000 $9,303 19.920/.Diagnosis and treatment. . . . . . . . . —
—— — $7,240 7,240 15.50

days of morbidity. Long-term benefits werecalculated in terms of eventual annual reductionin number of cases reaching ESRD. Long-term,though never specified, is essentially the 20thyear of program effort. For ESRD, only short-term mortality reduction is shown, since that isall that is possible. The calculated benefits areshown in table 10.
What conclusions are to be drawn from theBurton study? First, additional resources inprevention beyond current levels promised littleadditional benefit in reduced deaths and rathermodest additional benefits in reduced preva-lence and morbidity. Second, the prevention ofhypertension offered an important means for
reduction of deaths from ESRD. Third, only thedirect treatment of ESRD offered the best pro-spect for reducing deaths from that type ofkidney disease. Although the Burton reportitself nowhere reaches these conclusions in socrisp a fashion, careful perusal of table 10 pro-vides the basis for these inferences.
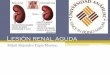
Actually, the Burton report itself gives an im-pression somewhat at variance with the afore-mentioned conclusions. Figure 3 of the report,reproduced as figure 1, discusses the changing“state of the art” due to advances from scientificresearch. The clear implication is that betterknowledge about preventing and treating pri-mary kidney disease would cut deeply into the
Table 10.—Program Benefits
Total
Benefits by kidney disease category— —Program level Infectious Hypersensitivity Hypertensive— End-stage
Current expenditure /eve/b
Short-term benefit-reductionsMortality. ., . . . . . . . . . . . . . .Prevalence . . . . . . . . . . . . .Morbid days . . . . . . . . . . . . . .
Long-term benefit-reductionsAnnual . . . . . . . . . . . . . . . . . .Cumulative. . . . . . . . . . . . . .
Intermediate expenditure levelb
Short-term benefit-reductionsMortality. . . . . . . . . . . . . . . .Prevalence ... ... . . . . . . .Morbid days. . . . . . . . . . . . . .
Long-term benefit-reductionsAnnual . . . . . . . . . . . . . . . .Cumulative. . . . . . . . . . . . . . .
Accelerated expenditure levelb
Short-term benefit-reductionsMortality. ., . . . . . . . . .Prevalence . . . . . . . . ...Morbid days . . . . . . . . . . . .
Long-term benefit-reductionsAnnual . . . . . . . . . . . . . . . . . .Cumulative. . . . . . . . . . . . . . .
Accelerated expenditure levelc
Short-term benefit-reductionsMortality. . . . . . . . . . . . . . . . .Prevalence . . . . . . . . .
70 deaths3,231,260 cases
15,962,420 days
610 deaths 2,190 deaths27,000 cases
1,802,000 days
690 deaths 3,560 deaths3,258,260 cases
17,764,420 days
6,080 deaths112,410 deaths
1,750 deaths25,850 deaths
4,330 deaths86,560 deaths
70 deaths3,243,860 cases
16,273,640 days
610 deaths 2,270 deaths39,880 cases
2,056,820 days
1,560 deaths—
4,510 deaths3,278.740 cases
18,330,460 days
6,590 deaths122,490 deaths
1,770 deaths26,190 deaths
4,820 deaths96,300 deaths
70 deaths3,292,860 cases
17,483,880 days
610 deaths 2,380 deaths42,750 cases
2,311,340 days
7,675 deaths—
10,735 deaths3.335,610 cases
19,795,220 days
6,690 deaths123,780 deaths
4,820 deaths96,300 deaths
1,870 deaths27,480 deaths
9,300 deaths289.690 cases
80 deaths5,630,720 cases
770 deaths62.250 cases
27,399 deaths 37,549 deaths5,991,723 cases
34,253,290 days
21,090 deaths586,160 deaths
.
Morbid days . . . . . . . . . . . . . . 26,064,430 days 2,610,000 days 5,578,860 daysLong-term benefit-reductions
Annual . . . . . . . . . 4,125 deaths 8,610 deaths 9,480 deathsCumulative. . . . . . . . . . . 76,500 deaths 320,000 deaths 189,660 deaths
Short term benefits – reduction In annual mortal~ty, etc when piograrn-ls fully op-e-ra~lveLong term annual benefits—evenlual annual reduction [n number of cases reachtng end stage kidney diseaseLong-term cumulative benef!ts– sum total of long term annual benefitsaRenal disease associated wrth hwertens(onbcurrenl state of the artcAdvanced state of the art
SOURCE Kfdrrey D/sease Program Analysls A Reporf 10 the Surgeon General (Washington D C DHEW JLIIY 19671

Treat menend-stagekidneydisease
Preventionandtreatmentprimarykidneydiseases
of
I I Dialysis .
SOURCE. Program A Surgeon Genera/ (Washington D C DHEW July 1967)
need to treat ESRD. That this development has scientific advance in analyzing the costs andnot come to pass by 1980 (as the Gottschalk re- benefits of medical care.port’s optimism about transplantation has alsofailed to materialize) should be a reminder to all The final chapter of the Burton report dealtabout the dangers of relying on “inevitable” with the cost of treating all patients threatened

by end-stage kidney failure, either by dialysis ortransplantation. Though this issue was not partof the original charge to the group, the reportargued, it was a logical corollary of the previousanalysis. The policy question was stated in thereport in the following way (17):
In any consideration of possible programs forthe amelioration of the kidney disease problem,the overall expense of treating all patientsthreatened with a uremic death regardless of thepossible costs, for humanitarian reasons, repre-sents one extreme in a broad spectrum of possi-ble programs. It should therefore be ascertainedto serve as a maximal benchmark for any inten-sive attempt at program analysis or planning.
Unlike the Gottschalk committee, which tooktreatment as its point of origin, the Burton com-mittee took it as one extreme in the range ofpossible programs.
The Burton committee assumed that 50,000patients were vulnerable to ESRD year afteryear, of whom 10,000 could be treated by “con-servative management” (primarily dietary con-t rol). Of the remaining patients, 11,000 werecandidates for transplantation, 2,000 ideal can-didates, and another 9,000 satisfactory. Theassumption was made, therefore, that 29,000new patients were available for and would beplaced on dialysis each year.
Estimated annual outcomes for transplanta-tion among the ideal candidates were that 80percent would be “cured,” 10 percent would failand be placed on dialysis, and 10 percent woulddie; the corresponding values for satisfactorycandidates were 30, 30, and 40. For the dialysispatients, it was estimated that 50 percent woulddie in the first year, and there would be a 90-percent survival rate for those remaining in eachsuccessive year.
Costs for the first 15 years of the programwere estimated by the Burton committee using“present cost” figures of $16,000 for a transplantoperation and $15,000 per year for dialysistreatment. (No home dialysis was projected. )
. .]
‘A tuture c (wt’ pr<)]cc tl~~n, U+ I ng $12,000 t ( ~r eac h t ra n~pla n tand !3 10,000 tor d ld ] y~l \ p~’r ~rea r wa~ a I S( ) m~de, on the a i~u m p-t I{ln that c ott~ WIC)U Id dcc 1 I nt, ot,er t I mt~ t t-()117 I nc r(,d ~td et t )( It,nc I(,\
I n prov Id I ng treat men t
Based on first and successive year cohorts of40,000 patients, the projected costs were:
1st year $611 million 40,000 patients5th year $1,044 mill ion 102,000 patients
15th year $2,702 million 179,000 patients
Having laid out a program for treating allthose vulnerable to kidney failure and havingdeveloped the corresponding cost estimates, theBurton report then limited the domain of appli-cability of its analysis. It noted that “supply”constraints of trained personnel and facilitieswould limit the rate of program buildup. Moresignificantly, it reduced the “demand” substan-tially from 40,000 vulnerable to an annualcohort of 8,000 to 10,000 individuals ideallysuited for dialysis and transplantation.
Finally, on the penultimate page of the Burtoncommittee’s report to the Surgeon General, itwas noted that (17):
With this general framework in mind andutilizing the elements and computations in Sec-tion V of Chapter 5, it is possible to arrive atpractical and feasible predictions concerning thecost of such a program and the overall numberof patients that could be accommodated by i tduring each of the first few years, the number ofpatients who are likely to- graduate from thisprogram permanently each year because of suc-cessful transplantation, the number of individ-uals who would have to be maintained perma-nently with the aid of chronic dialysis, and thenumber of new patients which such a programcould accommodate each year.
Having calculated costs for the much less likely40,000-patient annual cohort, however, the re-port stopped abruptly without making any cal-culations for the smaller, more probable, 8,000 -to 1(),000-patient cohort!
Overall, the Burton committee report had anumber of problems, some of which were stylis-tic. First, there was a somewhat naive belief in“decisions based upon a thorough, dispassion-ate, and logical analysis” and in the possibilityof allocating resources “on the basis of logicalpriorities. ” Second, the 16 different scenariosmake the analysis entirely too complex to be ofmuch use by policy makers. Third, each scenariois highly complex in its own right, built uponnumerous assumptions about the clinical feasi-

bility of the various components or forms of in-tervention, the appropriate “mix” of compo-nents, and the relative shares of Federal andnon-Federal funds. Fourth, the narrative tendstoward a repetitious presentation of calculationsbased on certain assumptions, justified by rela-tively little description of clinical feasibility, andoften supported only by citations to “best esti-mate” or “informed medical judgment .“
The Policy and Bureaucratic ContextsThe Gottschalk and Burton committees
worked at approximately the same time; theyaddressed similar subject matter; and their re-ports were issued simultaneously. It is worth-while to compare and contrast the two commit-tees, and their respective reports, and the policyand bureaucratic contexts in which they oper-ated.
The two committees differed in their initialstimulus and central purpose. The Gottschalkcommittee was a direct response to the existenceof expensive, lifesaving therapies developedlargely from publicly financed medical researchand to the mounting pressures to make thosetreatments available to the general public. Thatcommittee was not asked to address the ques-tion of whether treatment for ESRD should beprovided relative to alternative uses of re-sources; it was asked how such treatmentshould be made available if the basic policychoice was to go forward.
The Burton committee arose from the generaleffort within HEW to use program budgeting,systems analysis, and CBA for allocating re-sources to major programs. In general, the com-missioned studies were undertaken in order toprovide guidance for HEW’s 5-year programand financial plan and for fiscal year 1969 budg-et and legislative proposals. An attachment to amemorandum from Secretary Gardner stated,“Of particular importance this year is the ques-tion of kidney diseases. The future of Federalsupport for hemodialysis, transplantation, andprevention needs decisions based on thoroughanalysis” (29). No further clarification of pur-pose was given to the committee, nor did anysubsequent interaction occur between the com-mittee and the Surgeon General, the Assistant
Secretary for Health, and the Assistant Secre-tary for Planning and Evaluation which mighthave sharpened the focus of the committee’sstudy.
The two committees differed in composition.The Gottschalk committee’s members and con-sultants included three renal physiologists, twonephrologists, an immunologist, a transplantsurgeon, a psychiatrist, two economists, a law-yer, a biostatistian, and a professor of ethics.These people came primarily from universities,and especially academic medicine, but also fromGovernment and the private practice of law.The Burton committee’s members and consult-ants included one nephrologist, the director ofthe National Institute of Arthritis and MetabolicDiseases’ (NIAMD) artificial kidney program,the director of the National Institute of Allergyand Infectious Diseases’ transplant immunologyprogram, two professionals from the PHS kid-ney disease control program, several other PHSofficials, and three operations analysts. Mem-bers were drawn exclusively from the Govern-ment, consultants from a nonprofit researchfirm, Scientific and clinical competence wasgreater on the Gottschalk committee.
The duration of the two committees differedsubstantially. The Gottschalk committee metfirst in mid-1966 and a total of seven times overthe next year. A draft report was circulated forcomment in the summer of 1967 and a final re-port was presented to the Director of BOB thatSeptember. The Burton committee met initiallyin late March 1967. Its final report was trans-mitted to the Surgeon General in late July, only4 months later.
In substantive terms, the reports generallyagreed about the value of research, differedsomewhat on the value of prevention, and dif-fered greatly on the treatment of ESRD. TheGottschalk committee concluded that “continu-ing and expanded research in the fields of trans-plantation immunity, organ procurement andstorage, and dialysis is essential for optimal de-velopment of these methods of treatment” (31).The Burton committee, less directly but morefrequently supported research as critical to deal-ing with kidney disease. It tended to go beyonda limited endorsement, however, and suggested

that research was likely to generate substantialfuture reductions in deaths from ESRD.
On prevention, the Gottschalk committee de-clared that a screening program for pyelone-phritis, glomerulonephritis, and polycystic kid-ney disease made very little sense. The Burtoncommittee essentially said the same thing, butcouched its findings in language which obscuredthat conclusion. The Burton committee did,however, emphasize the prospective benefits inreduced deaths from ESRD due to prevention ofhypertension, a matter on which the Gottschalkcommit tee was silent.
It was on the issue of treatment for ESRD,however, that the two committees divergedmost sharply. The Gottschalk committee usedthe treatment of ESRD as its point of departure.That committee focused exclusively on patientswho were dying from chronic kidney failure,hence candidates for treatment by hemodialysisor transplantation. The two forms of therapy,its report declared, were “sufficiently well ad-vanced today to warrant launching a nationalprogram” (31). For the Burton committee, bycontrast, a universal treatment program repre-sented one “extreme” of policy possibilities, the“maximal benchmark” of how far the Govern-ment might go.
The Gottschalk committee estimated 3,662patients in the first year of a treatment program,increasing to 18,500 in the fifth year. The cor-responding costs were $40 million to $49 millionfor the first year, and $157 million to $205million in the fifth. Cost estimates were basedon the assumption that half of all dialysis pati -nts were treated at home at an annual cost of$4,000 (low estimate) or 5,000 (probable esti-mate). The estimated annual costs for centerdialysis ranged from $10,000 (low estimate) to$14,000 (probable estimate). Roughly 20 per-cent of the total beneficiary population, i t wasestimated, would receive a transplant, the costsof which ranged from $10,000 to $13,000. Esti-mates about the patient population ( table 8) ex-plicitly assumed that growth would be con-strained by available facilities.
The Burton committee established the costs ofa treatment program for 40,000 first-year pa-
tients at $611 million, and of a f i f th-yearpopulation of 102,000 at slightly more than $1billion (in 1967 dollars). In fact, as noted above,the committee’s report to the Surgeon Generalindicated that an annual cohort of only 8,000 to10,000 individuals would be serious candidatesfor a treatment program “in the near future”(17). Neither patient population nor associatedcost estimates for this most likely annual patientcohort were developed in the report, however,so the astronomical cost estimates based on theunlikely 40,000 annual patient cohort stood byimplication as the committee’s contribution tothe policy discussion.
These discrepancies between the Gottschalkand Burton committee reports might have beenunimportant t save for the circumstances of theirrelease to the public. Initially, BOB had plannedto keep the Gottschalk committee’s report secretand present it only to the BOB Director. Newsof the committee and its work leaked out to thepress, however, resulting in some publicity inApril 1967 and the certainty that the final reportcould not remain secret (38). But BOB itself,confronted with the fiscal implications of a na-tional ESRD treatment program, and increas-ingly feeling the effect of Vietnam war demandson funds for the Great Society programs,walked away from the Gottschalk committee’sreport.
BOB’s retreat from the Gottschalk report wasmanifested in several ways. Dr. Burton recallsthat BOB was unwilling to publish the report,and he authorized payment for publication of.500 copies out of the budget of NIAMD’s arti-ficial kidney program. The cover of the reportcarried only the title and date, Report of theCommittee on Chronic Renal Disease, Septem-ber 1967. Inside was a transmittal letter fromDr. Carl Gottschalk to BOB Director CharlesSchultze, but no official acknowledgment ofreceipt by the Director. Finally, the manner ofthe report’s release revealed BOB’s desire to putdistance between itself and the report from itscommit tee of experts.
The Burton report to the Surgeon Generalwas completed in late July, the Gottschalkreport to BOB in mid-September. The political

question became how to release these reports ina way to minimize public pressures for an ex-panded ESRD treatment program. A “low key”approach was agreed on, and strategy was co-ordinated between Joseph Califano on the WhiteHouse staff, BOB Director Schultze, and HEWSecretary John Gardner (3). The two reportswere released simultaneously at a PHS pressconference on November 3, 1967.
The press conference itself engendered somehard feelings. Dr. Gottschalk was notified of thepress conference by telephone in Chapel Hill,N. C., only 12 hours before it was scheduled,and he was unable to attend. Dr. Robert Ber-liner, then intramural research director of theNational Heart Institute, and technically an “ad-viser” to the Gottschalk committee, was presentto represent the expert committee. Since BOBhad refused to take any position on the Gott-schalk report, however, Berliner was unable tomake other than perfunctory comments aboutit. Dr. Burton, on the other hand, was underfewer inhibitions regarding the report from hiscommittee. The reporter who covered the storyfor Medical World News wrote that the featureof the briefing was not the report of the BudgetBureau’s expert committee, but the PHS reportto the Surgeon General which emphasized re-search on preventing kidney disease rather thantreating it. Dr. Burton reportedly called theGottschalk committee report “shortsighted.” “Inthe long run, ” he was quoted as saying, “wewant to get rid of the infectious mechanismsleading to kidney disease” (6). ”
Policy and Program Effects
What were the policy and program effects ofthese two formal analyses? The Burton reporthad little direct effect on PHS policies or pro-grams in kidney disease. For one thing, the Sur-geon General’s charge precluded the studygroup’s making any recommendations. In gen-eral, the Burton report reinforced NIH researchprograms related to dialysis and transplantationand supported PHS efforts in prevention. Itcountered, to some degree, the pressures from
‘‘Burton recalls speahlng ot Immunological” mechanl>rn~ In con-nection with glomerulonephrlt” i~
within the PHS kidney disease control programto promote a greatly expanded treatment pro-gram.
The Burton report was well received by Wil-liam Gorham, the HEW Assistant Secretary forPlanning and Evaluation, by Dr. Alice Rivlin,his deputy, and by Dr. Philip R. Lee, the Assist-ant Secretary for Health. Others in HEW wereless responsive. Dr. Burton recalls briefing Sec-retary Gardner on the study for 11/2 hours short-ly before the Secretary’s resignation in early1968 and receiving only a noncommittal “Thankyou very much” in return. Robert Grosse, aneconomist involved in HEW’s effort to improveresource allocation by using formal analysis,described the kidne y disease group’s workfavorably but uncriticall y in several papers(11,12,13).
One effect of the Burton report, noted above,was to engender hard feelings among somemembers of the Gottschalk committee and thosein the medical community who were favorablydisposed to the Gottschalk report’s recommen-dations. These hard feelings arose from thebelief that the Burton study group, by its im-plicit attack on a national treatment programand by the circumstances surrounding the pub-lic release of the two reports, had sought tosabotage the report of the Gottschalk commit-tee.
Three factors contributed to this impressionof sabotage. First, the reasons behind the PHSstudy were never clear. Why study kidney dis-ease when it was known that a BOB committeewas at work on the subject, many reasoned, ifnot to prevent PHS from being outflanked on anissue of some importance to it? PHS was not en-tirely clear on this point. It recognized that thereal policy problem was the treatment issue, butdid not address this matter directly in the chargeto the study group. The PHS study group,moreover, acknowledged that the cost of a na-tional dialysis and transplantation treatmentprogram was beyond its charge, but neverthe-less chose to conclude its report on that subject.The purposes and motives of PHS were thuscalled into question.

Second, BOB’s motives and behavior in walk-ing away from the report by its committee of ex-perts were not widely understood. Irving Lewisrecalls the occasion when Dr. Gottschalkbriefed BOB Director Schultze on the report:Schultze praised the work of the committee andits report, but said that resources for newdomestic initiatives were increasingly scarce as aresult of the impact of the Vietnam war (22).BOB, consequently, sought to dampen the im-pact of the Gottschalk committee’s report in theways described above.
Finally, hard feelings arose from the absenceof communication between the two committees.Interaction between the two groups did occurthrough several formal and informal means, butthese were limited in scope and duration. Asingle meeting of the two committees in thespring of 1977 would have clarified for eachother their respective missions and perhapswould have facilitated a more clearly under-stood division of labor.
The Gottschalk committee and its report rec-ommending a national ESRD treatment pro-gram had greater effects than the Burton com-mittee and its report, because the Gottschalkcommittee was a group with high status inacademic medicine, and advisory to BOB in theExecutive Office of the President. The commit-tee’s effects were of four kinds. The first was toneutralize opposition to dialysis and transplan-tation within the academic medical researchcommunity by making clear that these therapieswere established and not experimental and byconvincing the community that the patient load,and thus the economic burden, was predictable.Dr. George Schreiner recalls that representa-tives of foreign countries who testified at thecommittee’s second meeting, held at the sametime as the International Congress of Nephrol-ogy, all reported that the incidence of good dial-ysis candidates each year was in the range of 56to 58 patients per million population. Certainpredictabilities existed. The committee’s work,Schreiner remembers, “gave a much broadervista to the scientific types like Gottschalk,Seldin, and Berliner” (40).
The converse effect of the Gottschalk commit-tee’s work was to sanction the work of clinicians
who were treating patients. Controversy existedthroughout the early 1960’s about whether dial-ysis and transplantation, especially the former,were experimental or established treatment. Thereport of the Gottschalk committee declaredthat dialysis and transplantation were “capableof prolonging life” and were “sufficiently well-advanced today to warrant launching a nationalprogram, ” The impact of this declaration wassummarized several years ago by one prominentclinician in this way: “It was not until 1967 andthe Gottschalk report that you had for the firsttime an expression of national opinion that dial-ysis and cadaveric transplantation were ther-apy” (39).
The third effect of the Gottschalk report wason the VA’s renal program, which had precipi-tated the formation of the committee. There wascreated within VA a home dialysis programwhich came to dialyze a significant portion ofthe veteran dialysis patients. A secondary effecton VA was to encourage the development of itstransplantation program in a select number ofVA hospitals and to encourage the advocacy oftransplantation programs within the PHS pro-gram as well.
The question arises about the effect of theGottschalk report on subsequent legislation,especially upon the extension of medicare cover-age to ESRD through the inclusion of section2991 in Public Law 92-603, the Social SecurityAmendments of 1972. After the committee’sreport, several bills that incorporated the re-port’s recommendations were proposed in Con-gress, but none was enacted. In 1970, the heartdisease, cancer, and stroke legislation wasamended to include kidney disease, the only leg-islative enactment on the subject occurring be-fore Public Law 92-603.
Dr. George Schreiner, member of the Gott-schalk committee, served as president of the Na-tional Kidney Foundation from 1969 through1971. In that capacity, and aided by CharlesPlante r Washington representative of the foun-dation, Schreiner used the report, in his words,“as a two-by-four to get the mule’s attention. ” Innumerous one-on-one discussions with individ-ual members of Congress and their staff, theGottschalk report was cited as evidence of the

importance of treating ESRD. That report,therefore, helped clinicians advocating a treat-ment financing effort. Schreiner was emphatic,however, that legislation would never have oc-curred because of the report (40).
Within the Bureau of Health Insurance of theSocial Security Administration, Irwin Wolk-stein, Deputy Director for Program Policy,remembers reading the Gottschalk report andtalking about it with Klarman. The Bureau ofHealth Insurance as an organization, however,had deep reservations about extending healthinsurance coverage on a categorical diseasebasis. The Gottschalk report per se generated noadvocates for its recommendation within medi-care (45). Neither the staff of the House Waysand Means Committee nor the Senate FinanceCommittee had read the report at the time of the1972 legislation.
The 1972 legislation, however, did extendmedicare coverage to those with ESRD underthe general extension of coverage to the dis-abled. In this respect, the statute was consistent
CONCLUSIONS
What general conclusions can be drawn fromthis study about the use of formal analysis inpolicy formulation? First, policy toward ESRDwas always governed by two rudimentary factsconcerning treatment for ESRD: Such treatmentwas costly and lifesaving. These facts were un-changed by analysis; nor did analysis alterperceptions of what policy ought to be. Someshrank from the large cost implications of a na-tional treatment program: How can we affordsuch an expensive effort for so few? Othersreacted to the benefits: How can we withholdlifesaving therapy simply because people lackthe means to pay for it? Analysis did not alterthe fact that the policy issue was a basic politicalchoice between scarcity on the one hand, andthe priceless value of life on the other (s).
Second, it is important to recognize that ex-pectations of progress infuse practically all do-mains of science and technology, including
medicine, Indeed, in this analysis, we witness
with the Gottschalk report’s recommendation.The statute and implementing regulations forthe medicare renal program differed in two re-spects, however, from major recommendationsof the report. First, whereas the Gottschalkcommittee recommended a strong emphasis onhome dialysis, the medicare program inadver-tently introduced disincentives to that form oftreatment (32). Second, the report recom-mended a Federal investment in the “supply”side of treatment facilities and trained medicalprofessionals. In 1972, though the needs on thesupply side were less than those 5 years earlier,no consideration was given to this Federalassistance, and the statute focused exclusively
on augmenting the “demand” side by financingpatient care.
In summary, the Gottschalk committee reporthad little direct effect on the 1972 resolution ofthe policy question of financing patient care.The effects on the scientific and clinical com-munities, of course, may have indirectly in-fluenced the subsequent course of events.
several instances of underlying optimism aboutprobable developments in medical research andpractice. The Gottschalk committee was overlyoptimistic about transplantation, the Burtoncommittee about research and prevention. Ifanalysis is based on limited and inadequatedata, as it usually is at the early stages of policyformulation, it is then quite difficult to separaterealistic from overly optimistic expectationsabout the future. A critical review of basicassumptions by experts not involved in theanalytical effort may be the best corrective tothis source of bias.
Third, formal analysis on allocating resourcesfor lifesaving therapy cannot be done in secret.Though the original intention of BOB was tosecure expert judgment from the Gottschalkcommittee on a confidential basis, leaks to thepress, the resultant publicity about a “secret” ef-fort, and congressional inquiries eventually
forced the analyses to be released (7). PHS, on

the other hand, always intended to release theBurton committee’s report, and its intentionsplaced further pressure on BOB to release theGottschalk report. It is the case, however, thatthe Government has substantial discretion inhow it releases reports, and can choose to do soin ways that enhance or diminish the impact ofrecommendations.
Fourth, the absence of major policy action inresponse to the Gottschalk and Burton reportsdoes not mean that these efforts had no impact.Certainly, these reports did raise the conscious-ness of policy makers at the highest levels ofGovernment to the substantial cost implicationsof action, Given that the Vietnam war wasabsorbing increasing proportions of nationalresources at the time, it is not surprising thatnothing happened.16 The effects of greater even-tual policy consequence were those on the sci-entific and clinical communities, includingstrengthening clinician advocacy on behalf oftreatment financing.
Fifth, analysts have their greatest effect whenthey have direct access to key policy makers(23). The expert advisory committee to BOBhad access to the BOB Director, to the Office ofScience and Technology, and to the WhiteHouse. The members of the PHS study group
—‘“~ottschalk recalls that BOB ottlclals told hlm early In the w’ork
()[ the corn m i t tee that the anal ySIS was undertaken, In part, to cre-ate a pol ]cy opt Ion I n the event peace arrived I n Southeast ASla.Lewl~ has no such recollection”.
REFERENCES
1. Advisory Cc~mmittee tt~ the Renal TransplantRegistry t “The 13th Repclrt t~t the Human RenalTransplant Re~istry, ” 7-)”a}lspl(7}lt. Proc, 9(1 ):9,1977.
2. Barnes, B. A., “An Overview of the Treatmentof End-Stage Renal Disease and a Considerationof Sc~me CJI the Consequences, ” in Costs, Risks,and Benefits of Surgery, J. P. Bunker, et al.(eds. ) (New York: Oxford University press,1977),
3. “BOB ~HEW Studies on Kidney Disease, ” mem(~-randum from Charles L. %-hul tze, Directc~r, Bu-reau <~f the Budget, to Jc}seph Califanc~, TheWhite House, Sept. 21, 1967.
had access mainly to the higher officials inHEW. An additional, and closely related, pointis that analysis has its greatest effect when pol-icymakers wish to use it and have access them-selves to instruments that affect policies andprograms. The influence of the Gottschalk com-mittee report, in large measure, was confined toVA, because BOB could influence VA directlythrough the budgetary process and because itconsciously shrank from the report’s larger im-plications.
Finally, it should be noted that analysis donefor purposes of policy formulation is likely to belimited by a number of factors. The statement ofthe problem will control the analysis and its out-comes. Data are likely to be inadequate, espe-cially for issues just coming to policy prom-inence. Assumptions are required on criticalissues. Estimates are based on assumptions andinadequate data. Normative preferences will befound explicitly or implicitly throughout theanalysis. Projections over time are highly sen-sitive to the estimates, assumptions, and data.Uncertainty may inhere in clinical practicewhich cannot be reduced by formal analysis butonly by the increase of scientific knowledge.Given these limitations, the large conclusions offormal analysis are likely to be most importantto policy formulation if the estimates, assump-tions, and data appear to be reasonable. Formalanalysis may augment policymaking; it cannotsubstitute for it,
4. Bryan, F. A., Jr., T)le Natio)~al Dia/,vsis Regis-try: llex~elopr)?e)!t oj a Medical Registry c)~ Pa-tie}lk CI)Z C\lro}zic Dialysis, Fi)lal Report, ][l)IP1967-August 1976 (Research Triangle Park,N. C.: Research Triangle Institute, August 1976).
5. Calabresi, G. , and Bobbitt, P., Trtigic C/?oic~~s(New York: W. W. Norton & Co., 1978).
6. “Capital Rounds, ” M~dical World News, Nov.24, 1967.
7, “Chronic Kidney Disease Report, ” memoran-dum from Joe Laitin, Press Officer, Bureau ofthe Budget, to Charles L. Schultze, Direct(>r,Bureau c~f the Budget, Sept. 22, 1967.
8. Enthc~ven, A. C., and Smith, \U., Elou) Mz/c/~ IS

9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
E)Iough? Shaping the Dcfcrzsc I+~;yrti)u, 1961-69
(NeWY~rk:Harper& Row, 1971).“Establishment Of Health Program AnalysisGroups,” memorandum frc~m the U.S. Surget]nGeneral to Directors, Bureau of Health Man-power, Bureau of Disease Preventic~n and En-vironment tal Con trc~l, National Institutes t~fHealth, Bureau of Health Services, and NationalInstitute of Mental Health, Mar. 15, 1967.Fogel, M. E., and LeSourd, D. A., Desigt/ (>~Kid/re.y Diseuse Cc)~trol Prograt}rs, researchmemorandum (Rese,irch Triangle Park, N. C.:Research Triangle In~titute, February 1978).Grosse, R. N., “Cost-Benefit Analysis in DiseaseControl Programs, ” in Cost-B~~t~c~it A )~tilysis,M. G. Kendall (cd. ) (New York: American El-sevier, 1971).
“Cost-Benefit Analysis of Health Serv-ices, ” A}])]. A})l. Acad. P[)lit. Soc. Sci. 399:89,1972,
, “Prchlems ~~f Resource Allocation i nHealth, ” in I + { blic Expeil(~it~/ rm uird PolicyAnalysis, R. H. Havernan and J. Margolis (eds. )(Chicago: Markham Publishing Co., 1970).HalIan, J. B., et al., 7-IIc Ecot/ot~~ic Cc)sts of Kid-)ley Disease (Researc I Triangle Park, N. C.: Re-search Triangle Institute, October 1967).Hitch, C. J., D~~risio)~-M~lk-i)~g for Defe}lse (Ber-keley, Calif.: University of Calit(Jrnia Press,1965).Hitch, C. J., and McKean, R. N., The Econom-ics of Defense in the Nuclear Age (Cambridge,Mass.: Harvard University Press, 1960).Kid)[ey Diseusc Progwt)I A)lal,ysis: A R~~port tothe SI/Ygeo)/ GeI~eraJ’ ( Washingt[~n, D. C.: De-partment c>f Health, Educatit~n, and Welfare,Ju]y 1967).Klarman, H. E., “ApplicatiI~n of Cc~st-BenefitAnalysis to the Health Services and the SpecialCase of Technologic [innovation, ” l)rt. ), I-fealtllscrz~. 4(2):325, 1974.
“Present Stat .1s of Cost-Benefit Analysis,in the Health Field “ A)tl. J. Pl[hlic Hcalt/I57(1 1): 1948, 1967.Klarman, H. E., et al., “Cost Effectiveness Anal-ysis Applied to the Treatment of Chronic RenalDisease,” Med. Cure 6(1):48, 1968.LeSourd, D. E., et al,, Be}~cfit-Cost A~zalysis ofKidney Dismsc Progra)ns (Washington, D. C.:Department of Health, Education, and Welfare,August 1968).Lewis, 1. J., formerly Chief, Health and WelfareDivision, Bureau of the Budget, telephone inter-view, Nov. 14, 1979.Lincibl~m, C. E. , ard Cc~hen, D. K. , U.~tible
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
K}~ oudedge: Social Scic)lcc a~ld S[)ciul Proble\)rS{~/z~i)z<~ (New Haven, Cc)nn.: Yale UniversityPress, 1979).“Meeting on Renal Llialysis, ” memt~randum forthe file frc~m K. Peltzie, Bureau t]f the Budget,Mar. 9, 1966.Murray, J. E., et al., “Fifth Report of the HumanKidney Transplant Registry, ” Transplantation5(4):752, 1967.NBC News, “Wh(~ Shall Live?” presented Nov.28, 1965.pliskin, J. S., and Beck, C. H., “A Health Indexfor Patient Selection: A Value Function Ap-proach With Applications t(> Chronic Rena] Fail-ure Patients, ” Ma~~agc})IcI~t Sci. 22(9):1009,1976.Pliskin, J. S., et al., “Hemodial ysis—Projec t ingFuture Bed Needs: Deterministic and Probabil-istic Forecasting, C(J/)1. Bio~~lml. Res. 9:317,1976.“Prclgram Analyses f~~r Fiscal Year 1969, ” mem-c~randum tr(~m the Secretary tc~ various HEW of-ficials, Mar. 2, 1967.Quade, E. S. (cd.), A}/alysis for Military Deci-si~>j~s ( Chicagt): Rand McNally & Co., 1964).Rep(lrf of tll~ Co~)~})zittec 0 ) 1 C\lro?lic Kici)~eyDisease, September 1967.Rettig, R. A., l)tl~~~(~)~t~~i?ti?~~ tl~c E~ld-Stage Rc)lalDisease ~rograt)~ of Medicare, R-2505 -HCFA/HEW (Santa Monica, Calif.: RAND Corp., Sep-tember 1980).
“The P~~licy Debate on Patient Care Fi-— — ,nancing for Victims of End-Stage Renal Dis-ease,” Lau) co)?te))~p, Pmbl. 40(4):196, 1976.Riv]in, A. M., “The Planning, Programming,and Budgeting System in the Department ofHealth, Education, and Welfare: Sc~me LessonsFrom Experience, ” i n Plihlic Expc~lditures a)ldPolicy Analysis, R. H. Haveman and J, Margolis(eds. ) (chiCagO: Markham Publishing Co.,1970) .
S,vste}}~atic T/~i)zki}~g for Social Actio~~(Wash~ngt{~n, D. C.: The Brookings Institution,197 1).Schultze, C. L . , TIIe Politics o)[d Eco)lo)~licst~f P1/b/ic S/Jei~di}/g (Washington, D .C. : TheBrookings Institution, 1968).“Scope of the Reporting Being Prepared by theBureau’s Hem{xiialysis Commit tee,” memoran-dum from P. S. Palmer, Bureau of the Budget, toI. J. Lewis, Bureau of the Budget, Dec. 13, 1966.“Secret Panel Weighs U.S. Policy on UremiaTreat merit, ” M e d i c a l W{~r/d NL-WIS 8(1.5):36,
1967.

.
3 9 . Shapirt~, F. L., Minneapt~lisr Minn., i n t e r v i e w , 4 3 .July 29, 1974.
40. Shreiner, G., Gec}rgetc~w’n University, Washing-ton, D. C., telephone interview, Dec. 11, 1979. 44.
41. Stan~e, P. V., and Sumner, A. T., “PredictingTreatment Ccwits and Life Expectancy for End-Stage Renal Disease, ” N. E}Ig. ]. Ma]. 298(7): 45.372, 1978.
42. Strickland, S. P., Politics, ScIe~~cL~, a}~d D)-L~L7L7
Disc~7sP (Cambridge, Mass.: Harvard Universi-ty Press, 1972).
Terasaki, P. I., et al., “Analysis of Yearly Kid-ney Transplant Survival Rates, ” Tra/~sp/uI/t.Prof. 8(2) 139, 1976.Weiss, C. H., Ez~ull[l]ti(7~l Rmmrc/1: Met)lods ~~fAsscssi)?g Progra))l Effrcti~~c}/ess (EnglewoodCliffs, N. J.: Prentice-Hall, 1972).Wolkstein, I., Bureau of Health Insurance, So-cial Security Administration, Baltimore, Md.,interview, Sept. 10, 1973.
.I U S WV EFW MENT I> RINTm G OFFICE 1981 341-F44 1001