Embed Size (px)
Citation preview

Fortress and Frontier in American Health Care
Robert F. Graboyes
MERCATUS RESEARCH

Copyright © 2014 by Robert F. Graboyes and the Mercatus Center at George Mason University
Release: October 2014
ABSTRACT
America’s health care policy debate has long been framed as Left versus Right, Democrat versus Republican, federal versus state, and public versus private. This paper offers an alternative demarcation: Fortress versus Frontier. Health care is mostly in the Fortress, meaning that public policy focuses on protecting patients from risks and providers from competitors. Information technology (IT) is mostly on the Frontier, meaning that all Americans—even industry out-siders like Steve Jobs and Mark Zuckerberg—have been free to experiment and innovate with computers, telecommunications, and the Internet despite enor-mous risks to personal finances, privacy, safety, health, and well-being. The Fortress discourages creative destruction and disruptive innovation, and the Frontier tolerates both. Health care provision and innovation generally require official sanction; meanwhile, costs have risen. IT innovators have not needed permission to create and have thus been able to tap into serendipitous genius; the result has been plummeting costs. This paper suggests some potential pol-icy actions to shift health care from Fortress to Frontier, and toward a goal of producing better health for more people at lower cost on a continuous basis.
JEL codes: D83, I11, I18, J44, L26, O31, O33
Keywords: innovation, health, technology, technological change, risk, risk-averse, insurance, protectionism, health outcomes
Robert F. Graboyes. “Fortress and Frontier in American Health Care.” Mercatus Research, Mercatus Center at George Mason University, Arlington, VA, October 2014. http://mercatus.org/publication/fortress-and-frontier-american-health-care.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
3
America has engaged in a Sisyphean health care debate for decades, and the discussion today tends to be mind-numbingly repetitious.1 Since World War II, the debate has focused on the percentage of
Americans who have health insurance cards. The political Left has pursued the European-Canadian ideal of universal coverage—a health care system financed or operated by the government, with every resident eligible for some pack-age of services, defined and altered by the government over time. The political Right has been reactive—sometimes downplaying the desirability of universal coverage2 and other times suggesting more decentralized means of achieving the same end.3
The bitter and persistent debate over the Patient Protection and Affordable Care Act (ACA)4 is the most recent and most visible manifestation of this focus on coverage. But there were similar philosophical arguments over Medicare and Medicaid.5 In each act, coverage—not quality of care or outcome of treatment—was the primary goal.
The debate over coverage (and over related issues concerning how health care providers are paid) has focused attention almost exclusively on the
1. Jason Millman, “The Health-Care Debate Hasn’t Changed in 20 Years, New Clinton Documents Show,” Washington Post, April 18, 2014, http://www.washingtonpost.com/blogs/wonkblog /wp/2014/04/18/the-health-care-debate-hasnt-changed-in-20-years-new-clinton-documents -show/.2. See, for example, Ramesh Ponnuru, “The Misguided Quest for Universal Coverage,” New York Times, April 8, 2009, http://www.nytimes.com/2009/04/09/opinion/09ponnuru.html?_r=0.3. See, for example, Avik Roy, “Transcending Obamacare: A Patient-Centered Plan for Near-Universal Coverage and Permanent Fiscal Solvency” (report, Manhattan Institute, New York, 2014), http://www.manhattan-institute.org/html/mpr_17.htm#.VAI732P0dzs.4. The ACA is composed of the Patient Protection and Affordable Care Act, Pub. L. No. 111-148, 124 Stat. 119 (2010), and the Health Care and Education Reconciliation Act of 2010, Pub. L. No. 111-152, 124 Stat. 1029 (2010).5. For example, in 1961, Ronald Reagan burnished his national reputation as a public policy spokesman through a widely distributed recording, “Ronald Reagan Speaks Out against Socialized Medicine,” available on YouTube at http://www.youtube.com/watch?v=fRdLpem-AAs (10:06, posted by “Restoring the American Dream,” August 1, 2007).

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
4
demand side of health care markets—who pays how much to whom for which currently offered services. The debate underplays questions of supply—how innovation can alter the very nature of the health care delivery system. This paper argues that the most important fact about American health care policy is that Left and Right actually share a detrimental worldview—an excessive aversion to risk and a deference to medical insiders—and that this consensus slows the rate of technological progress in health care.
Section I characterizes this consensus view as the “Fortress” and its opposite as the “Frontier.” The Fortress is an institutional environment that aims to obviate risk and protect established producers (insiders) against com-petition from newcomers (outsiders). The Frontier, in contrast, tolerates risk and allows outsiders to compete against established insiders. The Fortress, in other words, disdains economist Joseph Schumpeter’s notion of cre-ative destruction6 and Harvard business professor Clayton Christensen’s idea of disruptive innovation.7 The Fortress-Frontier divide does not correspond neatly with the more familiar partisan or ideological divides. Framing health care policy issues in this way opens the door for a more productive national health care discussion and for uncon-ventional policy alliances.
Section II describes the Frontier via accounts of out-side innovators. The characters include a Hollywood actress who revolutionized warfare and encryption, an unheralded doctor who pioneered stem-cell therapy in a small-town hospital, a carpenter and puppet-maker who invented func-tional prosthetic hands costing one-thousandth the price of professionally made devices (aided by an evolutionary biologist who started a worldwide consortium of amateur prosthetists), and college students who devised a low-cost treatment for clubfoot.
6. Joseph A. Schumpeter, Capitalism, Socialism, and Democracy, 3rd ed. (New York: Harper, 1950).7. Joseph L. Bower and Clayton M. Christensen, “Disruptive Technologies: Catching the Wave,” Harvard Business Review 73, no. 1 (January–February 1995): 43–53.
“Left and Right actually share a detrimental worldview—an excessive aversion to risk and a deference to medical insiders.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
5
Section III describes the nature of the Fortress, also illustrated by a series of anecdotes. The characters in this section include an early-20th-century edu-cation reformer and a terminally ill rodeo enthusiast.
Section IV discusses how this focus on innovation can help break the logjam that has long divided Left from Right on health care. That would be to shift attention away from how to divvy up today’s costly services and toward the more fundamental question of how we can produce better health through less costly means.
Finally, Section V provides a menu of obstacles to innovation, along with some solutions that have been offered to surmount those obstacles. This sec-tion outlines a set of policies that could shift portions of health care from the Fortress to the Frontier—generating better health at lower cost for more people on a continuous basis.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
6
I. TWO WORLDVIEWS: FORTRESS AND FRONTIER
Trying to preemptively plan for every hypothetical worst-case scenario means the best-case scenarios will never come about.
—Adam Thierer
Since World War II, technological advances—a large proportion emanat-ing from America—have dramatically changed life on earth.8 A child in a third-world village might now carry a smartphone that, in the words
of one analyst, “would have been the most powerful computer in the world in 1985.”9 This computer can take pictures, play music and games, provide weather reports, translate text from one language to another, facilitate medi-cal care, and much more. In no time and at little cost, the child can email or telephone or Skype a loved one on the other side of the world.10
Tellingly, this device is such an astounding departure from the past that science fiction writers working just a few years before its appearance failed to imagine anything like it.11 And even more tellingly, the key names in smart-phone development came out of nowhere—not out of the blue-chip telecom-munications companies of the time. A Canadian colleague likes to tell how a man once came into his office carrying an ungainly-looking box that, the man explained, would soon combine a portable telephone with web brows-ing, email, music, and other services. Why, my friend wondered, would any-one want such a thing? The visitor, it turned out, was a founding partner at Research in Motion, and the device was a prototype BlackBerry.
A pertinent quotation is often attributed to Henry Ford: “If I had asked people what they wanted, they would have said faster horses.”12 The idea is
8. Marti Trewe, “U.S. Dominates List of Top 9 Most Innovative Nations,” American Genius, December 19, 2011, http://agbeat.com/entrepreneur/top-9-most-innovative-countries-list-dominated-by-u-s/.9. Horace Dediu, quoted in Charles Arthur, “How the Smartphone Is Killing the PC,” The Guardian, June 5, 2011, http://www.theguardian.com/technology/2011/jun/05/smartphones-killing-pc.10. Compare this with the 1980s, when I traveled extensively in sub-Saharan Africa for a major inter-national bank. I was able to make a call to the United States perhaps once a week, briefly, expensively, and after considerable time waiting for a connection. It was next to impossible to get US news reports less than three or four days old.11. In Stanley Kubrick’s 2001: A Space Odyssey (1968), HAL, the sentient computer at the heart of the film, is enormous. On the Pan Am flight to the moon, there are no laptops or personal digital assis-tants, so it is a pen—not a computer—that drifts away in weightlessness.12. Writing for the Harvard Business Review, Patrick Vlaskovits asserts there is no evidence that Ford actually made the statement, though the sentiment seems spot-on. Vlaskovits, “Henry Ford, Innovation, and That ‘Faster Horse’ Quote,” Harvard Business Review Blog Network, August 29, 2011, http://blogs.hbr.org/2011/08/henry-ford-never-said-the-fast/.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
7
that very few of us perceive the great innovations that are just around the cor-ner. And going a step further, it is unproductive or even counterproductive to assign the task of anticipating future innovations to a particular individual or group. This is one problem with assuming that a government agency or an established company can efficiently and effectively serve as the designated identifier of innovations.
BlackBerry, which made widespread mobile computing a reality, did not originate at AT&T, Western Electric, ITT, or Stromberg-Carlson. It originated with a couple of engineering students backed by some venture capitalists. World-changing innovations usually come from obscure people in unexpected places. There is no reason to imagine that the spark of genius that led to the BlackBerry would have occurred within the organization of, say, Western Electric. In fact, the BlackBerry was a mortal threat to the likes of Western Electric, undermining its structure of prior investments. Had a Western Electric researcher thought up the idea of the BlackBerry, he might well have kept it to himself—or been told to do so. More innocently, though, established insiders are notoriously poor at foreseeing innovation. As author Matt Ridley notes,
That is why Apple, not IBM, perfected the personal computer, why the Wright brothers, not the French army, invented pow-ered flight, why Jonas Salk, not the British National Health Service, invented a polio vaccine, why Amazon, not the Post Office, invented one-click ordering and why a Finnish lumber-supply company, not a national telephone monopoly, became the world leader in mobile telephony.13
In recent decades, industry after industry has undergone a reinvention similar to that of telecommunications. Standardized containers revolution-ized shipping, trucking, and freight rail.14 This change, highly counterintuitive at its outset, created vast amounts of wealth, much of which accrued to ordi-nary consumers—including those at the lowest wage levels. The information technology that made the third-world child’s cell phone possible also revo-lutionized distribution, ushering in just-in-time inventory management and one-click Internet shopping.
13. Matt Ridley, The Rational Optimist: How Prosperity Evolves (New York: HarperCollins, 2010), 261.14. For a description of the development and impact of the shipping container, see David Goldhill, Catastrophic Care: Why Everything We Think We Know about Health Care Is Wrong (New York: Vintage Books, 2013), 285–89.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
8
Harvard business professors Joseph Bower and Clayton Christensen call this process “disruptive innovation”—technological change driven by those outside the industry’s mainstream—that replaces complex products with sim-ple ones, yields massive price decreases, and leads to previously unthinkable quality increases (perhaps in ways unimagined by the innovators).15
In The Innovator’s Prescription: A Disruptive Solution for Health Care, Christensen and his coauthors Jerome Grossman and Jason Hwang argue that health care remained anomalous during this period of rapid innovation.16 To be sure, there were astounding technological developments in health care, but the innovation was, in Christensen’s terms, “sustaining” rather than “disruptive.”
Sustaining innovation brings evolutionary change to an existing market. Disruptive innovation brings revolutionary change that creates new markets altogether. Unlike disruptive innovation, sustaining innovation generally arises from established insiders and increases costs.17
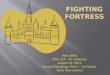
For example, in primary care, a sustaining innovation might be adding new and better equipment to a physician’s office. A disruptive innovation would be starting a telemedicine practice such as Doctor on Demand, which provides consultations via cell phone or iPad.18 A consultation with this practice currently costs $40—comparable to the cost of an office visit. From the patient’s perspective, however, there are substantial savings in terms of nonmonetary costs: travel time, waiting time, child care, missed work, the unpleasantness of getting out of bed while sick. The former innovation improves an existing market. The latter creates a new market.
Another example, explored later in depth, is the supply of prosthetic hands and arms. Sustaining innovations are those that improve the quality of professionally made prosthetics, such as the myoelectric bebionic3, which costs $25,000–$30,000.19 The disruptive innovation in that space is the 3-D printed hand, costing only a few dollars in materials and requiring perhaps six hours of assembly time by a volunteer (and even less time with newer
15. Bower and Christensen, “Disruptive Technologies.”16. Clayton M. Christensen, Jerome H. Grossman, and Jason Hwang, The Innovator’s Prescription: A Disruptive Solution for Health Care (New York: McGraw-Hill, 2009). The authors argue that we have frozen health care into a pair of century-old business models—the general hospital and the physician practice.17. For a survey of some disruptive innovations, see the summary of Jason Hwang’s ideas in John Converse Townsend, “Disruptive Innovation: A Prescription for Better Health Care,” Forbes, April 23, 2013, http://www.forbes.com/sites/ashoka/2013/04/23/disruptive-innovation-a-prescription -for-better-health-care/.18. Doctor on Demand website, accessed August 30, 2014, http://www.doctorondemand.com/.19. RSL Steeper bebionic website, accessed August 30, 2014, http://bebionic.com/.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
9
models). While the latter is in some ways inferior to the former, it is finan-cially accessible to far more people, including victims of war in Sudan and Sierra Leone.20
In many industries, America has frequently served as the locus of the ini-tial flash of disruption. US institutions (laws, regulations, professional norms, and societal attitudes) have been uniquely supportive of outsiders with ideas.21 To a considerable degree, health care has been the exception. America’s 75-year debate over health care has an ironic twist. Liberals and conservatives both per-ceive America’s health care economy as far more freewheeling than Europe’s. One side sees that as a bad thing and the other a good thing. But, observed
20. Mick Ebeling, “How a 3-D Printed Arm Gave Hope to Boy Maimed in Bomb Blast,” CNN, March 19, 2014, http://www.cnn.com/2014/03/19/opinion/3d-print-arm-daniel/.21. “Institutions are the rules of the game in a society or, more formally, are the humanly devised constraints that shape human interaction.” Douglass C. North, Institutions, Institutional Change and Economic Performance (Cambridge: Cambridge University Press, 1990), 3.
Revolutionizing primary care: Telemedicine can expand care and bring down costs, especially in underserved com-munities like rural areas, inner cities, and Hispanic enclaves. Doctor on Demand, whose mobile app interface is shown here, offers medical examinations nationwide via tablet or smartphone for $40 (as of 2014). Credit: Doctor on Demand.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
10
closely, the US health care system is not really Frontier America; rather, it differs only incrementally from Fortress Europe (or Fortress Canada).22
This paper explores America’s impediments to disruptive innovation—the absence of which the American economy can ill afford. Health care expen-ditures will soon exceed 20 percent of the US economy23 and are projected to strain the federal budget through all or most of the 21st century.24 David Goldhill, a television network CEO and health care expert, estimated that a young employee in his marketing department would spend around 50 percent of her lifetime earnings on health care, including insurance premiums, cost-sharing, out-of-pocket expenditures, and taxes devoted to health care ends.25
Over the past 75 years, America’s health care debate has focused almost entirely on the demand side of the consumer and labor markets: Who pays how much to whom for which services? Stereotyping a bit, the Left has argued for tighter regulation and shifting the locus of control from the states to the federal government and from the private sector to the public sector. The Right has argued for looser regulation and shifting the locus of control from the federal government to the states and from the public sector to the private sector.
These divisions are not trivial, but both sides fail to address the most important issues. The debate over American health care policy is akin to a family squabbling over whether to pay for household purchases with cash or credit—while never discussing what to buy. Cash versus credit is not a trivial choice; the payment mechanism has some influence over spending habits. But it pales in comparison with the choice of what will be supplied.
Inside, Outside, Destruct, and Disrupt
The decades-long partisan fight over American health care policy reached a high plateau in 2010 with the passage of the ACA. In 2014, rancor continues unabated at the federal and state levels. Yet then, as now, the most important
22. John C. Goodman, Priceless: Curing the Healthcare Crisis (Oakland, CA: Independent Institute, 2012), 91–93. Goodman argues that the US health care system differs relatively little from the Canadian and Western European systems.23. This projection from the Centers for Medicare & Medicaid Services pegs health care at 19.9 per-cent of GDP in 2022: “National Health Expenditure Projections 2012–2022,” accessed October 9, 2014, http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports /NationalHealthExpendData/downloads/proj2012.pdf.24. See Charles P. Blahous, “Will the Recent Slowdown in Health Care Cost Growth Improve Medicare’s Financing Outlook?” (Mercatus Research, Mercatus Center at George Mason University, Arlington, VA, January 14, 2014), http://mercatus.org/publication/will-recent-slowdown-health -care-cost-growth-improve-medicare-s-financing-outlook.25. Goldhill, Catastrophic Care, chapter 2.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
11
debate concerning American health care is, “How open should the health care system be to innovation by outsid-ers?” or, equivalently, “How risk-averse should we be, and how much deference should we confer on established insiders?”26
The shorthand form for this question is “Fortress or Frontier?” Later sections will define these two terms more fully, but in brief, the Frontier is an environment in which risk-taking is tolerated and outsiders are free to challenge established insiders. The Fortress, in contrast, discourages risk-taking and protects insiders from challenges by out-siders. I argue that American policymakers of most politi-cal, ideological, and philosophical stripes tilt toward the Fortress viewpoint, thereby discouraging technological and managerial innovations that could benefit both our health and our wealth.27
The current debate over health care has not for the most part been one of Fortress versus Frontier. Rather, it has been over which type of Fortress is most desirable. Should the shape of health care be determined by insiders in the federal government, or insiders in state governments and in private entities, such as medical specialty organiza-tions, hospitals, and insurers?
We can explain the Fortress-Frontier divide in terms of Schumpeter’s “creative destruction” and Christensen’s “disruptive innovation.” Creative destruction is the notion that innovation and economic growth emerge from the failure and collapse and purposeful destruction of old eco-nomic organizations, which are then replaced by more efficient organizations. Montgomery Ward and Sears Roebuck give way to Kmart and Wal-Mart; Pan Am falls
26. In the area of technological innovation, public policy scholar Adam Thierer describes a struggle between the “precautionary principle” and “permissionless innovation.” Thierer, Permissionless Innovation: The Continuing Case for Comprehensive Technological Freedom (Arlington, VA: Mercatus Center at George Mason University, 2014).27. A good discussion of the reasons why policymakers tend to reward incumbents can be found in Bruce Yandle, “Bootleggers and Baptists: The Education of a Regulatory Economist,” Regulation: AEI Journal on Government and Society, May–June 1983, 12–16.
“The Frontier is an environment in which risk-taking is tolerated and outsiders are free to challenge established insiders.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
12
and Southwest rises.28 In health care, creative destruction could consist of a newer hospital putting an older one out of business, or out-of-state physicians moving into a community to supplant locally trained physicians.
The concept of disruptive innovation is related to creative destruction and describes the replacement of old modes of production, including both physical technologies and managerial structures, by newer modes. The big-box Kmart and Wal-Mart give way to the online Amazon.com; mainframe comput-ers give way to laptops and smartphones. Hand-loaded ships give way to crane-loaded container ships. Business travel faces competition from GoToMeeting.
But Schumpeter’s and Christensen’s terms describe processes, while the Frontier described here is more an institutional environment or philosophi-cal worldview that encourages those processes. The Frontier is a cause, while creative destruction and disruptive innovation are effects. Conversely, the Fortress is an institution or philosophy that impedes creative destruction and disruptive innovation. The Fortress tends more to preserve the institutional status quo and promote sustaining innovation—innovation from established institutions. Sustaining innovation tends to increase costs and build on estab-lished producers and products. Disruptive innovation creates entirely new markets and shatters established producers and products. We now live in a decades-old era of disruptive innovation in many fields—though for the most part not in health care.
The most striking (or strikingly obvious) example of disruptive innova-tion is in data processing. In 1965, computers were all room-sized mainframes; they often cost millions of dollars. There were relatively few of them, they were mostly owned by elite organizations, and their workings were distant from the lives of most Americans. In 1965, a disruptive innovator, the Digital Equipment Corporation (DEC), changed the world by offering the first minicomputer—the podium-sized PDP-8—for $18,000. Great companies like Honeywell and Sperry lost their dominant role in the computer world. IBM survived by rein-venting itself, and that transformation is still frequently studied because it is almost unique in business history.29
An essential prerequisite for disruptive innovation is relative ease of entry into the market by outsiders—those who are not credentialed and those
28. See also Virginia Postrel, The Future and Its Enemies: The Growing Conflict over Creativity, Enterprise, and Progress (New York: Touchstone, 1998). Postrel defines two worldviews—stasis vs. dynamism—that are similar to the Fortress and the Frontier. She launches a broadside against the notion that centralized experts should determine the course of technology.29. Christensen, Grossman, and Hwang describe the mainframe-to-mini transition in the introduc-tion to Innovator’s Prescription.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
13
who have not come up through the ranks. A notable example is the rise and fall of DEC. DEC was the computer industry’s great disruptor in 1965—an out-of-nowhere firm that brought down world leaders in the computer industry. Within a decade, DEC itself began its slide into oblivion as Bill Gates, Steve Jobs, and others developed microcomputers.
In the 1980s, cell phones began proliferating, but they were toys of the rich well into the 1990s—symbols of status among the higher ranks of Wall Street executives. Not many years later, billions of cell phones filled pockets around the world—including those in the poorest villages of the developing world. As mentioned earlier, when a third-world villager carries an iPhone, he has in his hand a computer more powerful than any computer on earth in 1985—for one-ten-thousandth or so of the cost—even without figuring in inflation.
Summing up, the Frontier encourages creative destruction and disruptive innovation. Undreamed-of products arise and old, revered ones vanish. New production processes sweep away old ones. This is a place where unknown innovators in garages destroy titans of industry. The Frontier celebrates and rewards risk, and there is a brutal egalitarianism to the creative process.
In contrast, the Fortress discourages creative destruction and disrup-tive innovation. Insiders are protected from competition by government or by private organizations (such as insurers and medical societies) acting in quasi-governmental fashion. In the Fortress, insiders preserve the existing order. Innovation comes from well-established, credentialed insiders who, it is pre-sumed, have the wisdom and motives and competence to identify opportunities for innovation.
Often, Fortress entities fail to recognize the Frontier until it threat-ens their own businesses. IBM founder Thomas Watson said in 1943 that total world demand for computers was around five machines. Christensen, Grossman, and Hwang note that incumbent producers often underestimate the speed with which upstart competitors can overtake them. “But then the world flips suddenly, crippling the established companies.”30 They cite the speed with which the tiny digital camera market wiped out or badly damaged Polaroid, Agfa, Fuji, and Kodak.
In any country, health care will have both Fortress and Frontier elements. A country may tend toward one direction or another, but there are always lacu-nae of the other present. Literally and metaphorically, one can build a fortress on the frontier. The questions concern both the magnitude and the particulars of the split—how much of the health care sector should be within the Fortress
30. Christensen, Grossman, and Hwang, Innovator’s Prescription, 250.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
14
and how much left to the Frontier. And there is nothing intrinsic to medicine that preordains that it should be more Fortress than other industries. As the fol-lowing discussion suggests, the lines between Fortress and Frontier can be fluid.
Fortress Becomes Frontier: ARPANET to Google
The Internet began as Fortress and flourished as Frontier. The original Internet, the ARPANET, was a project of ARPA (the Advanced Research Projects Agency of the United States Department of Defense) and was limited to a relatively small core of high-level researchers and defense officials. The ARPANET was tightly constrained, and its original strictures assured that it could not have become today’s Internet. In a 1982 handbook, the Massachusetts Institute of Technology warned students against misuse of the network:
It is considered illegal to use the ARPAnet for anything which is not in direct support of Government business. . . .
Sending electronic mail over the ARPAnet for commer-cial profit or political purposes is both anti-social and illegal. By sending such messages, you can offend many people, and it is possible to get MIT in serious trouble with the Government agencies which manage the ARPAnet.31
The Internet that so altered human society emerged when it was opened to outsiders who were free to develop their own applications and add them to the platform. But this very freedom tends to frighten people who see the Internet as a place of risk and mob rule. Commenting on the Heartbleed secu-rity vulnerability, one Washington Post reporter remarked on the “terrifying” nature of the Internet: “It is inherently chaotic, built by multitudes and con-tinuously tweaked, with nobody in charge of it all.”32
Millions of websites and apps populate today’s Internet. Most fail to attract any appreciable following. A relatively small number—Google, Amazon, Facebook, Wikipedia, Twitter, and so on—attract billions of users, changing
31. Christopher C. Stacy, “Getting Started Computing at the AI Lab” (Working Paper 235, Massachusetts Institute of Technology, Artificial Intelligence Laboratory, September 7, 1982), 9, available at http://www.academia.edu/1416892/Getting_Started_Computing_at_the_AI_Lab.32. Craig Timberg, “Heartbleed Bug Puts the Chaotic Nature of the Internet under the Magnifying Glass,” Washington Post, April 9, 2014, http://www.washingtonpost.com/business/technology /heartbleed-bug-puts-the-chaotic-nature-of-the-internet-under-the-magnifying-glass/2014/04/09 /00f7064c-c00b-11e3-bcec-b71ee10e9bc3_story.html.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
15
world society to an unprecedented degree. Anyone who grew up in this era will understand that the life-changing websites and apps did not come from a Federal Department of Apps (FDA?). Nor did they generally come from well-established private entities. Nor, most likely, could they have.
The Obama administration claimed that HealthCare.gov would be the Travelocity.com or Amazon.com of health insurance.33 But Travelocity and Amazon were not risk-averse productions staged by established elites and given a monopoly over innovation. Very likely, a government-anointed travel or retail site would have been a rolling disaster like HealthCare.gov. Instead, each of these successful sites was the winner of a great race by countless now-forgotten (and generally never-remembered) competitors.
Fortress Remains Fortress: NASA to Nay-Say
In 1957, the United States could not manage to place even a small satellite in orbit, and Americans cringed at the nightly sight of Sputnik I passing overhead. Twelve years later, NASA landed two men on the surface of the moon and brought them safely home again. Add to that the planetary probes, the Hubble Space Telescope, and other projects, and NASA must be regarded as one of the most innovative organizations in history. Yet its critics note that NASA had a burst of unparalleled innovation and then settled into a long period of relative lethargy. Aviation designer Burt Rutan, a leading NASA critic (he refers to the agency as “Nay-Say”), speculates that the Cold War concerns of the 1950s and ’60s created a short-lived culture in which NASA employees put aside their self-interest for the good of the agency and the country—a culture that could not be sustained beyond a relatively brief window in time.
In 2010, Rutan’s company, Scaled Composites, won the $10 million Ansari XPrize by launching one vehicle on two separate suborbital flights within a period of two weeks. He has partnered with investor Richard Branson to form Virgin Galactic, which aims to provide the world’s first regularly scheduled tourist flights to space. Though the effort is well along, it has not yet succeeded. If it doesn’t, there are other private ventures—Elon Musk’s SpaceX, Jeff Bezos’s Blue Origin, and more—close on Rutan’s heels.
In a 2004 Wired article, Rutan predicted that private enterprise will suc-ceed where government planning has failed:
33. Jonathan Cohn, “Healthcare.gov Is Not Amazon.com: Should We Care?,” New Republic, December 4, 2013, http://www.newrepublic.com/article/115815/why-healthcaregov-not -amazoncom-should-we-care.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
16
For nearly half a century, the government has held a monopoly on manned space exploration. Quite predictably, this approach has not served us well. NASA is clinging blindly to an embarrassingly expensive and dangerous space shuttle program that should have been scrapped years ago. . . . In the open market, entrepreneurs and space hobbyists will do in a decade what NASA couldn’t do in 46 years: provide safe, reliable trips to the heavens for the cost of a Caribbean cruise.34
Rutan was overly optimistic on the timeline, but the private projects are already bearing fruit. The Wikipedia article “List of Private Spaceflight Companies” gives an idea of the magnitude of this nascent industry.35 A YouTube video of SpaceX’s Grasshopper vehicle36 or Rutan’s SpaceShipTwo37 hints at how different their approaches are from NASA’s reliance on single-use, disposable ballistic missiles.
In his article, Rutan noted that NASA’s response to the Columbia disaster was to withdraw into a no-risk policy—consigning astronauts to low-orbit mis-sions that preclude most of what is interesting about space travel. Rutan noted that he needed no government resources to achieve suborbital space travel:
The technology of SpaceShipOne is relatively simple and inex-pensive. The hardware is almost entirely reusable. In fact, the only parts subject to real wear and tear are the bearings in the landing gear, which can be easily and cheaply replaced. The spacecraft can theoretically take off and land from any airport. You don’t need a launchpad or an expensive base facility—just a 9,000-foot stretch of runway. With simplicity comes safety. . . . It’s time for NASA to get out of manned space travel and con-centrate on its core strength: basic research and development of space technologies.38
34. Burt Rutan, as told to Joseph Portera, “After the X Prize,” Wired, December 2004, http://archive .wired.com/wired/archive/12.12/rutan.html.35. Wikipedia, s.v. “List of Private Spaceflight Companies,” last modified September 28, 2014, http://en.wikipedia.org/wiki/List_of_private_spaceflight_companies.36. “Grasshopper 744m Test: Single Camera (Hexacopter),” YouTube video, 1:36, posted by “SpaceX,” October 12, 2013, https://www.youtube.com/watch?v=9ZDkItO-0a4.37. “SpaceShipTwo—First Rocket-Powered, Supersonic Test Flight,” YouTube video, 1:56, posted by “Virgin Galactic,” April 30, 2013, https://www.youtube.com/watch?v=M1GiAOzKz4k.38. Rutan, “After the X Prize.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
17
These stories of innovation in space exploration highlight an interesting contrast. In health care, the Obama administration has pursued a bureaucracy-heavy, top-down approach, and the result thus far has been disastrous. In con-trast, more than any of its predecessors, the Obama administration has opened the way for private entrepreneurs to take the helm in space flight. It did so by shifting the federal bureaucracy into a more hands-off stance and, to a great extent, getting out of the way of entrepreneurs like Rutan and Bezos and Musk.39
NASA was a remarkable government innovation, but it stagnated when the government maintained the agency’s monopoly for too long, allowing its goals to grow diffuse. The disruptive innovators now just getting started are creating new markets including, but not limited to, space tourism.
39. Rand Simberg, “Government Should Butt Out of Space Race,” USA Today, January 15, 2014, http://www.usatoday.com/story/opinion/2014/01/15/nasa-bush-space-exploration-column /4495785/.
Markets beyond the earth: As NASA’s space program fades, entrepreneurs such as Burt Rutan, Jeff Bezos, and Elon Musk compete to change the direction of space flight. Here, Rutan (third from left) and associates celebrate their $10 million Ansari XPrize after successfully launching two manned suborbital flights. Credit: Gene Blevins/Corbis.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
18
Settling In: The Gates of the Fortress
Bruce Yandle, a scholar with the Mercatus Center at George Mason University, famously coined the term “bootleggers and Baptists” to describe a particular type of symbiotic relationship.40 Bootleggers earn more money if alcohol is illegal, so they support efforts by Baptists to outlaw liquor. Thus arises a strange-bedfellows alliance of sincere antialcohol forces and purvey-ors of illegal alcohol. In health care, the problem may be more of bootlegging Baptists—medical industry insiders who believe that market restrictions are genuinely in the interests of patients, and are pleased that such restrictions will coincidentally increase their incomes and their control over health care.
A recent op-ed illustrates this duality. In the column, Bill Crounse, Microsoft’s chief medical officer, decries “cavalier talk” about disruptive inno-vation as follows:
Imagine for a minute that you are a hospital executive, a doctor, a nurse or other clinician and you hear people who work outside your industry talking about disrupting or destructing it. . . . There you are doing the best you can to make it through each day keep-ing your hospital or practice economically sound, dealing with the barrage of patients at your door, staying one step ahead of ever-increasing rules, regulations and rising costs, while those who’ve never worked a day in your world tell you they are going to disrupt and/or destroy it. . . . I don’t imagine my colleagues who work at Microsoft (or Google, or Apple, or Amazon) would appreciate being told by a hospital administrator or a doctor that they knew better how to run a tech company, or what ails the tech industry.41
Crounse seems perfectly sincere. But the irony is that he works for Microsoft, whose founder, Bill Gates, made tens of billions of dollars by being the risk-taking outsider who disrupted the computer industry. No doubt the employees at the now-long-gone Digital Equipment Corporation did their best to make it through each day, keep the company financially sound, stay one step ahead of
40. Yandle, “Bootleggers and Baptists,” 12. There is a new bootleggers and Baptists book: Adam Smith and Bruce Yandle, Bootleggers & Baptists: How Economic Forces and Moral Persuasion Interact to Shape Regulatory Politics (Washington, DC: Cato Institute, 2014).41. Bill Crounse, “Why the Creative Destruction of Healthcare May Not Be Such a Good Idea,” Health Care Blog, March 18, 2014, http://thehealthcareblog.com/blog/tag/disruption/.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
19
the rules and costs. And then Gates, the college dropout who had never been a part of DEC’s world, helped propel the company into oblivion.
The story doesn’t end there, of course. There is good reason to be thankful for all that Microsoft has done—and the same goes for many companies with similar stories, such as Google, Apple, and Amazon.com. One can argue that Gates and other information technology (IT) entrepreneurs have indirectly saved an enormous number of lives. They have done so by setting into motion the lower-quality to larger-quantity to vastly-improved-quality sequence of events in computers. This technological change made it possible to save lives and relieve suffering in previously unimaginable ways: OnStar, dynamic sta-tioning of ambulances, wireless biometric telemetry, nationwide 911 capability, more efficient allocation of medical resources (e.g., just-in-time inventory), and on and on and on.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
20
II. FRONTIER TALES
Innovation is like a bush fire that burns brightly for a short time, then dies down before flaring up somewhere else.
—Matt Ridley, The Rational Optimist
The most important thing to understand about disruptive innovation is that it often comes (perhaps usually comes) from strange and unex-pected places. The following four stories illustrate this notion.
Actress and Composer: The Unexpected Provenance of EncryptionModern Wi-Fi and GPS devices rely on an encryption technique called frequency-hopping spread spectrum, in which the signal is sent over a sequence of different frequencies rather than just one. The idea originated early in the 20th century, but it was made practical for military usage by a pair of inventors during World War II. The first of these inventors was, astonishingly, actress Hedy Lamarr.42 Lamarr had been married to a Nazi-sympathizing Austrian weapons dealer whom she grew to hate. He often brought her to his busi-ness meetings, apparently to show off his trophy wife. Expected to sit silently, Lamarr listened carefully to the conversations. By the time she left Europe she had secretly acquired a world-class expertise in high-tech weaponry. In the United States she developed the idea of spread-spectrum technology as a way of preventing the Nazis from jamming the signals directing the US Navy’s radio-controlled torpedoes.
She needed some help rendering her idea practical, and turned to a friend, George Antheil, a symphonic composer who was prominent for a time on the Paris arts scene. Lamarr and Antheil had to devise a method for syn-chronizing the frequency-hopping on the transmitting and receiving ends of the signal. Antheil recalled that in the 1920s he had written a musical work in which 16 pianos were synchronized by means of piano rolls.43 He suggested that this technique could be adapted to radio-controlled torpedoes. Lamarr and Antheil developed the necessary process and successfully patented it. Though US forces didn’t use the technology during World War II, they eventually used
42. Lamarr’s invention is described in Fleming Meeks, “I Guess They Just Take and Forget about a Person,” Forbes, May 14, 1990, 136–38.43. The piece was written for Fernand Léger’s film Ballet Mécanique (1924).

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
21
it during the Cuban Missile Crisis in 1962 to prevent the Soviets from jamming their communications.
Needless to say, the government, established war contractors, and uni-versities are not likely to have selected a Hollywood actress and an avant-garde symphonic composer to devise a key component of naval weaponry. But this story is not an isolated case. Disruptive innovation almost always comes from unexpected sources.
In 2014, Lamarr and Antheil were inducted into the National Inventors
Innovation from unexpected people: When permitted, innovation emerges from unforeseen places. During World War II, actress Hedy Lamarr (pictured) and composer George Antheil invented a technology to prevent Axis powers from jamming the US Navy’s radio-controlled torpedoes. Their patent, shown here, contributed to GPS, Bluetooth, and other important technologies. Credits: Bettmann/Corbis (left) and US Patent & Trademark Office (right).

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
22
Hall of Fame.44 Their invention evolved into the encryption methods used today in Bluetooth and other consumer electronic devices.
Small-Town Doctor, Big-Time Discovery
Milton Ende, MD, grew up with my mother in Petersburg, Virginia, and was an astoundingly fine diagnostician. When my aunt with chronic health problems became critically ill, he asked a question no one over the years had thought to ask: “Has anyone ever tested her for multiple sclerosis?” They hadn’t, until his quick mind inferred that key diagnosis in an instant.
In the early 1960s, Ende wondered why infants rarely contracted can-cers. He and his brother Norman, also an MD, thought that perhaps something in infants’ blood inhibited cancer growth—and they wanted to test whether transplanting blood from infants to cancer sufferers might have therapeutic benefits. Ethically, they couldn’t extract blood from infants for this purpose,
44. “Inductees,” National Inventors Hall of Fame website, accessed July 28, 2014, http://invent.org /inductees/.
Innovation in unexpected places: Milton Ende (left), collaborating with his brother Norman (right), performed the earliest stem-cell transplants for cancer treatment. Working in an obscure small-town hospital, the brothers obtained little funding and their findings were routinely rejected by major medical journals. Recognition came very late in their lives. Credit: Courtesy Norman Ende, MD.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
23
but they realized they could use infant blood cells from the umbilical cords (and later placentas) of newborns. Cord blood, we now know, is rich in stem cells.
The brothers transplanted cord blood into cancer sufferers whose cases were deemed hopeless and who volunteered for the experiment. These experi-ments cured no one, but some patients exhibited temporary and at times sub-stantial and prolonged improvement—enough to give the doctors hope that they were on to something.
Funders and major medical journals routinely rejected the Endes’ work, so in 1972, they reported their first findings in a regional publication, the Virginia Medical Monthly.45 In medicine, credentialism is real, and sometimes a real prob-lem. During the first few years after 2000 some finally recognized the impor-tance of the Endes’ work, describing them as the earliest of all pioneers in stem-cell therapy.46 While the Endes never received their full measure of recognition, other pioneers gave rise to a vast array of stem-cell research and therapies.
Could the Endes’ experiment occur today? Physicians have told me almost certainly not. Whatever their considerable virtues, institutional review boards would likely be an obstacle. Fears of malpractice litigation would likely dissuade most physicians from such experimentation, and the US Food and Drug Administration (FDA) is more active in proscribing novel practices nowadays.47 Administrative burdens have shifted physicians from solo prac-tices (such as Milton Ende’s) into group practices that would likely be more wary of experimentation. One cardiologist with whom I spoke reminisced about grassroots innovation in his field 40 years ago. At that time a burst of new surgical procedures emerged via improvisation and experimentation—almost on the fly.
Recently, singer John Mellencamp described how a doctor improvised a radical surgical technique to save Mellencamp’s life after he was born with severe spina bifida.48 Similarly, Frank Jobe, an orthopedic surgeon, devised a
45. Ende and Ende, “Hematopoietic Transplantation by Means of Fetal (Cord) Blood: A New Method,” Virginia Medical Monthly 99, no. 3 (March 1972): 276–79.46. Virginia Commonwealth University Office of Government Relations, news release about Milton and Norman Ende, October 2001, http://www.govrel.vcu.edu/news/Releases/2001/oct/bios.htm. For more information on the Ende brothers’ experiments, see Virginia C. Hughes, “Cord Blood Transplantation: Hallmarks of the 20th Century,” Laboratory Medicine 31, no. 12 (December 2000): 672–78, http://labmed.ascpjournals.org/content/31/12/672.full.pdf.47. In a paper coauthored with scholar Dina Gould Halme, former FDA commissioner David A. Kessler notes that work with stem cells requires the submission of an investigational new drug appli-cation to the FDA before human studies can begin. Halme and Kessler, “FDA Regulations of Stem-Cell-Based Therapies,” New England Journal of Medicine 355 (October 19, 2006): 1730.48. Sean Woods, “John Mellencamp’s Life Advice,” Men’s Journal, March 2014, http://www .mensjournal.com/magazine/john-mellencamps-life-advice-20140219.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
24
radical elbow reconstruction now widely performed on baseball players. The procedure, known as the “Tommy John surgery,” is named for the first baseball player whose career it saved.49
3-D Printing: Hands across the Water
Leon is a Massachusetts boy in his early teens, born with no fingers on his left hand. Prosthetics are expensive and cumbersome—costing perhaps $25,000–$80,000. The cost often hits patients in the form of thousands of dollars of deductibles, copays, and caps. Leon’s father, Paul McCarthy, was determined to find a less-expensive alternative.
Searching the Internet, McCarthy discovered the serendipitous collabo-ration of Richard Van As, Ivan Owen, and Yolandi Dippenaar. In South Africa, Van As, a woodworker, had accidentally cut off two fingers and mangled two others. In Washington State, Owen, a puppet-maker, was known as a skilled builder of puppet hands. Dippenaar, also South African, gave birth to a child, Liam, with no fingers on his dominant right hand.
On the web, Van As saw Owen’s work, and the two collaborated to pro-duce inexpensive but workable prosthetics using 3-D printers. Dippenaar caught wind of their work and recruited them to create a hand for five-year-old Liam—one whose fingers could respond to the movement of muscles in his arm. While Van As had originally sought only to construct a hand for himself, Dippenaar’s request led him to pursue a larger goal.
Scouring the Internet, McCarthy learned of this new technology and found Owen’s posted manufacturing instructions. Using an inexpensive 3-D printer, he and Leon manufactured a hand costing somewhere in the $10 to $50 range. With his bright green hand, Leon can pick up pencils, hold a water bot-tle, and ride a bicycle. If he breaks or outgrows it, $10–$50 will buy another.50
Meanwhile, in Kansas, 16-year-old Mason Wilde had been sidelined from football by repeated concussions. Searching for a new activity to occupy his time, he learned of Van As and Owen’s printed hand; it happened Wilde knew a
49. Mike Dodd, “Tommy John Surgery: Pitcher’s Best Friend,” USA Today, July 28, 2003, http://usa today30.usatoday.com/sports/baseball/2003-07-28-cover-tommy-john_x.htm.50. “Boy Gets Prosthetic Hand Made by 3-D Printer,” YouTube video, 2:55, posted by “CBS Evening News,” October 28, 2013, http://www.youtube.com/watch?v=FGSo_I86_lQ. For a moving description of the development of the 3-D printed hand, see “MakerBot and Robohand: 3D Printing Mechanical Hands,” YouTube video, 10:11, posted by “makerbot,” May 8, 2013, https://www.youtube.com /watch?v=WT3772yhr0o.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
25
younger child, Matthew, who was missing the fingers on one hand. In his spare time, Wilde constructed a mechanical hand for Matthew.51
At the Rochester Institute of Technology (RIT), Jonathan Schull is “a biological psychologist, entrepreneur, community organizer, and director of RIT’s Center for Student Innovation.”52 Schull became involved with the 3-D hand project and ultimately founded e-Nable,53 a Google+ and Facebook net-work that has attracted (at the point I write this) more than 1,200 individuals in need of prosthetic hands or interested in building them.54 Thanks to this
51. Mará Rose Williams, “Kansas Teen Uses 3-D Printer to Make Hand for Boy,” Kansas City Star, January 31, 2014, http://www.kansascity.com/news/local/article337980/Kansas-teen-uses-3-D -printer-to-make-hand-for-boy.html.52. Jonathan Schull’s biography, Idea Connection Systems website, accessed October 9, 2014, http://www.innovating.com/innovation-speakers-bureau/speakers/jon-schull/. 53. e-Nable website, accessed August 10, 2014, http://enablingthefuture.org/.54. e-Nable Facebook page, accessed August 10, 2014, https://www.facebook.com/enableorganization.
Genius from crowds: An FDA-approved prosthetic hand can cost $40,000. In 2013, an injured carpenter and a puppet-maker 10,000 miles away invented a functional 3-D printed hand costing between $10 and $50. A worldwide crowd of amateurs has driven a stunning developmental process to improve these hands. This process provides a window onto the future of health care innovation. Credit: Katarina Price Photography.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
26
network of amateurs, as time passes, the hands have evolved to become more aesthetically pleasing, facile, and—in some cases—unconventional. One father, for example, designed his son’s hand to have opposable thumbs at either end to aid in grasping. The boy is now known by schoolmates as “Cool Hand Luke.”55
So a woodworker, a puppet-maker, the families of disabled children, a sidelined high school athlete, his younger friend, an academic polymath, and a thousand others scattered around the globe became critical links in an expand-ing network of tinkerers and inventors. With open-source technologies, net-work members improve the design of these prosthetics, little by little. Even the children being fitted for the hands have contributed, devising some radical design features. It’s exactly the process we see with Internet apps—strokes of genius from unexpected places. Notice that this process did not come from the titans of medicine, manufacturing, or government, nor would it have. No panel of experts appointed Van As and Owen to develop the printed hand. And we’ll never know how many tinkerers tried and failed to do something similar.
For now, the FDA is not an impediment to the printed hand. Schull noted in a conversation with me that mechanical hands given away for free are not subject to FDA approval at present.56 If any of the components were motorized, if the prosthetic were a leg, or if builders sold the prosthetics rather than giving them away, they would be subject to the FDA’s long and expensive deliberative processes.57 This need for permission can effectively block products from ever reaching the market.
Approval issues are likely to become more acute, since 3-D printers also have the capacity to use biological materials in place of plastic. There has already been progress using the printers to produce replacement organs58—and there are already moves afoot to ban the use of such technologies.59
55. e-Nable Facebook photo, accessed October 9, 2014, https://www.facebook.com /enableorganization/photos/a.563360593741733.1073741830.554753701269089/678836695527455 /?type=1.56. See Robert F. Graboyes, “Innovation Is the Key to Health Care Reform,” Reason.com, July 1, 2014, http://reason.com/archives/2014/07/01/innovation-is-the-key-to-health-care-ref/.57. Information on FDA device approval procedures can be found at “PMA Approvals,” US Food and Drug Administration website, last modified October 2, 2014, http://www.fda.gov/medicaldevices /productsandmedicalprocedures/deviceapprovalsandclearances/pmaapprovals/default.htm. The FDA did report positively on 3-D printed hands in Steven K. Pollack and James Coburn, “FDA Goes 3-D,” FDA Voice, August 15, 2013, http://blogs.fda.gov/fdavoice/index.php/2013/08/fda-goes-3-d/.58. Catherine Jewell, “3-D Printing and the Future of Stuff,” WIPO Magazine (World Intellectual Property Organization), April 2013, http://www.wipo.int/wipo_magazine/en/2013/02/article _0004.html.59. Gartner Inc., “Gartner Says Uses of 3D Printing Will Ignite Major Debate on Ethics and Regulation,” news release, January 29, 2014, http://www.gartner.com/newsroom/id/2658315.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
27
Extreme Affordability: Miracle Brace
Each year, hundreds of thousands of children worldwide are born with clubfoot—a condition in which the feet turn inward. Untreated, clubfoot is debilitating and can imperil a person’s ability to lead a normal life and earn a living. In the United States, treatments are often highly labor-intensive, requiring dedicated work by therapists and parents. Another treatment is a metal brace costing $300–$700.
Many children with clubfoot, however, are born in developing countries. In such cases skilled therapists are hard to come by and the children’s parents may lack money and time to deal with the disability. With this in mind, a charity called Miraclefeet approached students in a Stanford University class on “extreme affordability.” Two students, Jeff Yang and Ian Connolly, consulted with Brazilian doctors to design a plastic brace that can be pro-duced on a 3-D printer for less than $20. In addition to its low cost, the brace is easy to use and is designed to look like a toy, in contrast to the cold-looking metal braces used in the United States.60
Note the disruptive nature of this product. The $20 printed brace costs between one-fifteenth and one-thirty-fifth the price of metal braces sold in the United States. The product appears to be less therapy-intensive than other methods commonly used in the United States, thereby diminishing the flow of revenue to health care profession-als. As of January 2014, the inventors were planning to seek FDA approval so the device could be distributed in the United States.61
60. Joseph Flaherty, “Stanford Whizzes Develop an Astoundingly Cheap Fix for Clubfoot,” Wired, January 14, 2014, http://www.wired.com /design/2014/01/curing-kids-style-design-thinking/; “Extreme Design for Extreme Affordability,” Stanford University website, accessed August 10, 2014, http://extreme.stanford.edu/projects/miraclefeet-brace.61. Tom Fowler, “Stanford Students Develop a Cheap Fix for Clubfoot,” Medgadget, January 21, 2014, http://www.medgadget.com/2014/01 /stanford-students-develop-a-cheap-fix-for-clubfoot-video.html.
“The $20 printed brace costs between one-fifteenth and one-thirty-fifth the price of metal braces sold in the United States.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
28
Science and Technology: Cousins, Not Siblings
The above anecdotes illustrate how innovation often comes from strange places. As we will see in section III, since the early 20th century, health care has been one of the more insular industries in America. In health care, inno-vation has tended to come from expected places—from highly credentialed insiders. In his seminal book on the American medical profession, The Social Transformation of American Medicine, Paul Starr writes,
The dominance of the medical profession . . . goes consider-ably beyond [its] rational foundation. Its authority spills over its clinical boundaries into arenas of moral and political action for which medical judgment is only partially relevant and often incompletely equipped. Moreover, the profession has been able to turn its authority into social privilege, economic power, and political influence. In the distribution of rewards from medi-cine, the medical profession, as the highest-paid occupation in our society, receives a radically disproportionate share. Until recently, it has exercised dominant control over the markets and organizations in medicine that affect its interests. And over the politics, policies, and programs that govern the system, the profession’s interests have also tended to prevail. At all these levels, from individual relations to the state, the pattern has been one of professional sovereignty.62
Matt Ridley writes, “Much as I love science for its own sake, I find it hard to argue that discovery necessarily precedes invention and that most new practical applications flow from the minting of esoteric insights by natural philosophers.”63 Ridley argues that the relationship between innovation and patents is especially loose—that patents often lead to no innovation and that at other times, innovation proceeds apace without patents. He calls innovation “a semidirected, groping, bumbling process of trial and error by clever, dexter-ous professionals with a vague but gradually clearer notion of the processes at work. . . . It is what happens today in the garages and cafés of Silicon Valley, but not in the labs of Stanford University.”64
62. Starr, The Social Transformation of American Medicine (New York: Basic Books, 1982).63. Ridley, Rational Optimist, 255.64. Ibid., 257.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
29
Ridley notes the irony in previous criticism of the entrepreneurial atmo-sphere:
Even as late as 1988 dirigistes were still criticising the frag-mented companies of Silicon Valley as “chronically entrepre-neurial” and incapable of long-term investing. This was when Microsoft, Apple, Intel and (later) Dell, Cisco, Yahoo, Google and Facebook—chronically entrepreneurial all, in their garage or bedroom beginnings—were just laying the foundations for their global dominance at the expense of precisely the big com-panies dirigistes admired.65
In other words, science is an excellent gauge and a terrible autopilot. Ridley points out that “of the four men who made the biggest advances in the steam engine—Thomas Newcomen, James Watt, Richard Trevithick and George Stephenson—three were utterly ignorant of scientific theories, and historians disagree about whether the fourth, Watt, derived any influence from theory at all.”66
It is easy to find examples of ultimate insiders incapable of seeing what lay immediately ahead. In the late 1940s, Vannavar Bush—president of MIT, engineer, inventor, and head of the US Office of Scientific Research and Development during World War II—dismissed the possibility of precisely guided intercontinental ballistic missiles.67 Western Union once dismissed the telephone as an impractical novelty.68
Without endorsing their sentiments, it is worth mentioning that some cutting-edge innovators are ambivalent about the virtues of formal higher edu-cation. Some years ago, I personally heard aviation designer Burt Rutan explain how he urged a student to quit engineering school in his third year and come to work for Rutan’s company. Rutan told the student that he would not want to hire him after he finished the degree because, paraphrasing, “In the first three years, they taught you what you can do in engineering. In the fourth year, they will teach you what you cannot do, and I am not interested in hiring someone who knows what cannot be done.” My colleague, Maurice McTigue, a former ambassador from New Zealand to Canada, tells a similar story. Microsoft, he
65. Ibid., 268.66. Ibid., 255.67. G. Harry Stine, Intercontinental Ballistic Missile: The Making of the Weapon That Changed the World (New York: Orion Books, 1991), 107.68. Ridley, Rational Optimist, 261.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
30
says, was recruiting third-year students from the University of Western Ontario for the same reason that Rutan cited. Google’s Laszlo Bock notes that his company has hired a substantial number of non-college graduates: “When you look at people who don’t go to school and make their way in the world, those are exceptional human beings. And we should do everything we can to find those people.”69
To repeat, nothing said here is meant to suggest that higher education, insider status, and expert credentials are negatives. Rather, the lesson is that an infusion of ideas from outside a field of expertise and from outside formal educational channels can be highly beneficial if not essen-tial to the process of innovation.
Sources of Innovation: A Caveat
Arguably, the problem in health care is not that we lack innovation of any type, but rather that we have in place incentives that encourage sustaining innovation and dis-courage disruptive innovation. Ironically, federal inno-vation funding may be a significant obstacle to the sort of innovation this paper associates with the Frontier.
The federal government has a sizable infrastructure for funding innovation. The National Institutes of Health, the National Science Foundation, and other agencies pro-vide large sums of money in the form of innovation grants. The Centers for Medicare & Medicaid Services has an Innovation Center charged with developing “innovative payment and service delivery models to reduce program expenditures . . . while preserving or enhancing the quality of care.”70
These agencies can point to a great many success sto-ries. Without belittling the work they do, it is legitimate to
69. Quoted in Thomas L. Friedman, “How to Get a Job at Google,” New York Times, February 22, 2014, http://mobile.nytimes.com/2014/02/23 /opinion/sunday/friedman-how-to-get-a-job-at-google.html.70. “About the CMS Innovation Center,” Centers for Medicare & Medicaid Services website, accessed October 3, 2014, http://innovation.cms.gov /about/index.html.
“Ironically, federal innovation funding may be a significant obstacle to the sort of innovation this paper associates with the Frontier.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
31
ask whether we have an excess of public management and funding of innova-tion and whether these funding mechanisms discourage outside innovators. Not all innovation is created equal. Inside innovators could certainly point with pride to the better and better mainframe computers that preceded the micro-computer era. But there is a qualitative difference between the Fortress-driven mainframe innovation and the Frontier-driven microcomputer era. Similarly, while locked in the Fortress, the ARPANET’s slow evolution was a stunning achievement, but it bore little resemblance to the manic innovation we see on today’s web.
In this section, we have seen pathbreaking innovations from unlikely outsiders—Hedy Lamarr’s spread-spectrum technology, Milton Ende’s stem-cell transplants, and Ivan Owen’s prosthetic hands. The question is how likely federal agencies are to fund innovators such as these. The political economy of public grant approvals makes it unlikely. Arguably, the grant review process slants heavily toward applicants with established track records and credentials. Reviewers themselves likely face greater career risk in awarding grants to a Lamarr or an Ende or an Owen than to a well-established industry insider. And thus, the federal grant machine likely encourages incremental innovation—evolutionary rather than revolutionary changes.
Moreover, federal innovation grants could actually discourage radical innovation by giving a competitive advantage (or the threat of such an advan-tage) to safer, slower models. And finally, there are political economy issues to consider. If grant reviewers view applicants as potential future employers, that could bias awards as well.
The central message here is that the source of innovation matters a great deal. This section is mostly caveat and conjecture, merely touching on a topic that deserves a much fuller treatment.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
32
III. A BRIEF HISTORY OF THE FORTRESS
Physicians are not prepared for genomic medicine.
—Eric Topol, The Creative Destruction of Medicine
To better understand the Fortress, this section explores the transfor-mation of American medicine in the 20th century. America’s medical Fortress arguably began with the 1910 Flexner Report. This Progressive
Era report vastly altered medical education and greatly elevated perceptions of the medical profession itself. In the ensuing decades, American health care institutions evolved along similar lines with an aggressive focus on protect-ing the public from treatment risks and protecting providers from competi-tion. These institutions included an enhanced role for the American Medical Association (AMA), the establishment of Blue Cross Blue Shield and other insurers, increased restrictions on providers through state licensing boards, and greater restrictions on drugs and medical devices by the FDA.
Flexner’s Fortress
The foundation of the health care Fortress was laid in the first decade of the 20th century. In 1904, the AMA established the Council on Medical Education, which, in 1908, commissioned the Carnegie Foundation for the Advancement of Teaching to evaluate America’s medical colleges. The foundation hired the Louisville, Kentucky, educator Abraham Flexner to evaluate the nation’s medi-cal schools, and the resulting Flexner Report of 1910 still resonates today.
In 1910, America’s 155 medical schools varied markedly in quality, in ped-agogical methods, and in medical philosophies. The Flexner Report upended American medical education and transformed American medicine. Medical his-torian Edward Halperin gives three reasons: (1) the Flexner Report’s findings were consistent with the progressive politics of its time, (2) the report appeared at what was arguably the first moment in human history when “a random patient with a random disease consulting a doctor chosen at random stands a better than 50/50 chance of benefiting from the encounter,” and (3) history is written by the victors, and the modern medical profession is what remained after Flexner wiped away dissenting pedagogical and philosophical streams.71
71. Edward C. Halperin, “Viewpoint: A Century Later, the Flexner Report Still Has Our Attention,” Association of American Medical Colleges newsroom, accessed August 10, 2014, https://www.aamc .org/newsroom/reporter/march10/45532/viewpoint.html. The quotation is Halperin quoting Harvard physiologist Lawrence Henderson.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
33
The importance of Halperin’s first reason—Flexner coinciding with the Progressive Era—cannot be overestimated. “If the sick are to reap the full ben-efit of recent progress in medicine,” Flexner said, “a more uniformly arduous and expensive medical education is demanded.”72 Flexner wanted medical education to be more exclusive, more standardized, more homogeneous, more centralized, and more expensive. He got his way, and it remains so today.
Flexner unleashed dramatic changes in American medicine. In the wake of his report, half the country’s medical schools were forced to close. Some may well have been low-quality institutions, but many or most were not.73
Flexner demonized for-profit medical schools and, for decades, for-profit schools vanished from the American educational scene. (They have returned, notably in the form of offshore and osteopathic medical schools.) The effect was to greatly constrict the supply of doctors. Medical incomes rose from their modest levels early in the century to the high levels that prevailed until recently and, in some areas (particularly the medical specialties), still remain.74
But quality of students and education is only one part of the Flexner story. Of equal or greater importance is the drive for standardization—for sameness. Competing medical philosophies were no longer to be found in American medical schools. The surviving notion was, and still is, that proper treatment is deterministic—given a set of symptoms (along with other details about the patient), there is one appropriate treatment, and it can be determined by an algorithm. The medical school curriculum was also standardized, so there was little to differentiate one school from another. The assumption that health care is a business was exiled from the medical schools because, in Flexner’s view, “The physician is a social instrument.”75
The Flexner Report also shuttered five of the nation’s seven then-existing African-American medical schools. One reason was that a large por-tion of African-American students attended resource-poor undergraduate
72. Abraham Flexner, “Medical Education in the United States and Canada: A Report to the Carnegie Foundation for the Advancement of Teaching” (report, Carnegie Foundation for the Advancement of Teaching, New York, 1910), 13, available at http://archive.org/stream/medicaleducation00flexiala /medicaleducation00flexiala_djvu.txt.73. As a caveat, this section is concerned primarily with the negative effects of Flexner’s report, and doesn’t discuss how its results may have been beneficial. I will posit here that the costs have consid-erably outweighed the benefits and therefore I will focus on the costs. For a more thorough treat-ment of Flexner, see the excellent account in chapter 3 of Princeton sociologist Paul Starr’s The Social Transformation of American Medicine.74. For a comparison of physician salaries in the United States and elsewhere, see Christopher J. Conover, “Are U.S. Doctors Paid Too Much?,” Forbes, May 28, 2013, http://www.forbes.com/sites /theapothecary/2013/05/28/are-u-s-doctors-paid-too-much/.75. Flexner, “Medical Education,” 154.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
34
colleges that could not provide the courses Flexner believed must be taken before medical school. A nationally standardized medical school curriculum no longer had sufficient flexibility to accommodate such students. The result was a decades-long lack of black doctors to serve black communities.76
Flexner’s Followers
For the better part of a century, Flexner-inspired structures spread throughout the health care industry. Beginning in 1929, Blue Cross (and later Blue Shield) greatly altered the concept of health insurance. Henceforth, health insurance assumed a form different from almost any other type of insurance. It would pay not just for large, unlikely, unanticipated expenses—the traditional role of insurance. Now, health insurance would serve as the conduit of payment even for small, routine, fully anticipated expenses. And perhaps more significantly, Blue Cross marked a shift from cash-upon-diagnosis to reimbursement-upon-treatment. “Health insurance” was now as much a prepayment plan as it was insurance, and every claim paid represented additional provider income.
In 1938, the FDA’s control over pharmaceuticals greatly expanded, as it did again in 1962. In both cases, the proximate cause was a recent drug-related catastrophe. In the first instance, the event was the death of around 100 patients who used tainted sulfonamide drugs. In the second instance, the event was the recent thalidomide disaster in Europe and elsewhere (but not in the United States). Later, medical devices were also brought under the FDA’s purview.
State governments avidly joined in the construction of this medical edi-fice. Agreeing with Flexner’s abhorrence of business in medicine, most states adopted legislation barring or severely restricting the employment of physicians and other medical personnel by entities not owned by medical practitioners. Known collectively as the corporate practice of medicine doctrine, these laws are now largely anachronistic, yet they linger on the books and limit or slow the development of novel organizational structures for health care providers.
States also protected physicians against competition from nurses and allied health professionals. Uwe Reinhardt, a Princeton University scholar who is often critical of right-of-center health care policy,77 wrote a deeply critical
76. Rebecca Skloot, The Immortal Life of Henrietta Lacks (New York: Crown, 2010). Skloot tells a fas-cinating story and gives a depressing glimpse of the Jim Crow–era interactions between the African-American community and the US medical system.77. Reinhardt, “Talmudic-Like Studies of Republican Health Reform Ideas,” Health Care Blog, August 18, 2013, http://thehealthcareblog.com/blog/2013/08/18/talmudic-like-studies-of-republican -health-reform-ideas/.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
35
piece in 2013 on restrictive medical licensure.78 He wrote this after the California Medical Association successfully blocked efforts to expand the allowable scope of practice for nurse practitioners. Reinhardt lays out an impressive case ques-tioning the structure of medical licensing. He cites, approvingly, the following passage from economist Milton Friedman’s Capitalism and Freedom:
Licensure therefore frequently establishes essentially the medi-eval guild kind of regulation in which the state assigns power to members of the profession. . . .
The most obvious social cost is that any one of these mea-sures, whether it be registration, certification or licensure, almost inevitably becomes a tool in the hands of a special producer group to obtain a monopoly position at the expense of the rest of the public. There is no way to avoid this result. . . .
The members [of the profession] look solely at technical standards of performance, and argue that we must have only first-rate physicians even if this means that some people get no medical service—though of course they never put it that way. Nonetheless, the view that people should get only the “opti-mum” medical service always leads to a restrictive policy.79
Reinhardt also quotes Friedman as follows:
I myself am persuaded that licensure has reduced both the quantity and quality of medical practice; that it has reduced the opportunities available to people who would like to be physi-cians, forcing them to pursue occupations they regard as less attractive; that it has forced the public to pay more for less sat-isfactory medical service, and that it has retarded technologi-cal development both in medicine itself and in the organization of medical practice. I conclude that licensure should be elimi-nated as a requirement for the practice of medicine.80
78. Reinhardt, “The Dubious Case for Professional Licensing,” New York Times, October 11, 2013, http://economix.blogs.nytimes.com/2013/10/11/the-dubious-case-for-professional-licensing/.79. Friedman, Capitalism and Freedom, 40th anniversary ed. (Chicago: University of Chicago Press, 1962), 141–53.80. Ibid., 158.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
36
Increased knowledge of the human genome stands poised to change the very nature of health care—if it is allowed to do so. The study of human health has since antiquity been based on averages of large groups of people. Now that we are beginning to understand how the molecular structure of DNA impacts body and mind, we are also becoming capable of tailoring preventive care and treatment of illness to individual human beings.
To do so, however, we will have to overcome a great deal of institutional inertia. The FDA is perhaps the most visible obstacle along this path. Its regula-tory methodologies rely on slow, large-sample studies using classical statistical models. The FDA’s central operating principle is the precautionary principle—the notion of pre-market clearance, meaning that a drug or medical device must be proven safe and effective before it can be allowed on the market. And yet the FDA’s traditional methodologies are inconsistent with personalized, molecu-lar, precision medicine. Medicine designed (as at present) for an “average” per-son will likely be less than optimal for any actual person. Personalized medicine offers the possibility of more efficient treatment of individuals’ illnesses.
The FDA—and health care in general—has been mired since the early 1960s in the aftermath of the thalidomide disaster. In the late 1950s, approxi-mately 10,000 children were born with horrifying deformities after their moth-ers took the antinauseal drug thalidomide during critical periods of pregnancy. The disaster never occurred in the United States because the FDA was slow in granting approval to the drug.81 This episode reinforced the notion that slow is good and that well-established insiders should exert nearly complete control over the flow of innovation.82
The problem with this mode of operation is that excessive conservatism has likely prevented millions from receiving treatments that could have saved their lives or eased their pain. The FDA has traded an overt risk for a hidden one.83 Often such negatives—opportunities forgone—are difficult to envision. Recently, this idea of unseen deaths from excessive risk-aversion received a vivid and widely seen representation in the film Dallas Buyers Club, based on
81. James H. Kim and Anthony R. Scialli, “Thalidomide: The Tragedy of Birth Defects and the Effective Treatment of Disease,” Toxicological Sciences 122, no. 1 (2011): 1–6, http://toxsci.oxford journals.org/content/122/1/1.full.82. Note that thalidomide returned to the market in the 1990s after a long review process that included input from the victims of the 1950s disaster. Brigid Schulte, “Panel Urges FDA to End Long Ban on Thalidomide: The Drug Was Once Used for Morning Sickness; It Would Now Be Used on Leprosy under Tight Rules,” Philadelphia Inquirer, September 6, 1997, http://articles.philly.com /1997-09-06/news/25552672_1_thalidomide-erythema-nodosum-leprosum-leprosy.83. Arthur Daemmrich and Georg Krücken, “Risk versus Risk: Decision-Making Dilemmas of Drug Regulation in the United States and Germany,” Science as Culture 9, no. 4 (2000): 505–34.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
37
the actual story of Ron Woodroof, a Texas electrician and rodeo enthusiast who contracted HIV/AIDS in the 1980s.84 Woodroof was told he had 30 days to live and was denied access to AZT and other newly available treatments for AIDS. These drugs, he was informed, had not been adequately tested for safety and effectiveness. Facing a death sentence, Woodroof was not interested in the precautionary principle. Both in the film and in real life, he procured the drugs in Mexico, smuggled them into the United States, and began a large-scale
84. Jean-Marc Vallée, Dallas Buyers Club (2013).
Outlaw permissionless innovation: Ron Woodroof was diagnosed with AIDS in 1986 and told he would die within 30 days. Doctors denied him experimental treatments because the FDA needed more years of testing to deem them safe and effective. Woodroof smuggled drugs from Mexico, distributed them to AIDS sufferers in Dallas, and lived seven more years. Credit: Dallas Morning News.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
38
operation to distribute them to other AIDS sufferers. In the end, he survived for seven years. As Woodroof’s character says in the movie portrayal,
Oh, I’m the drug dealer? No, you’re the fucking drug dealer. I mean, goddamn, people are dyin’. And y’all are up there afraid that we’re gonna find an alternative without you.85
The FDA was forced to partially relent in the case of HIV/AIDS. The AIDS community was highly politicized, and the human misery of sufferers denied treatment was too visible and too obvious. Furthermore, HIV is a per-fect example of how the FDA’s methodology fails. HIV evolves at an astonish-ing pace. For all practical purposes the viruses in a sufferer’s body at the end of a test would be entirely different from those in the same sufferer’s body at the start of the test—raising questions about how meaningful the results could ever be. Furthermore, HIV’s interaction with a person and its susceptibility to treatment depend greatly on the sufferer’s particular DNA structure.86 Thus, large-sample tests are unlikely to accurately describe the virus’s impact on spe-cific individuals.87
85. Ibid. Ron Woodroof is played by Matthew McConaughey.86. Peter W. Huber, The Cure in the Code: How 20th Century Law Is Undermining 21st Century Medicine (Philadelphia: Basic Books, 2013), 93.87. Ibid., 132.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
39
IV. LIMITS OF SUPPLY
Our whole role in life is to give you something you didn’t know you wanted. And then once you get it, you can’t imagine your life without it.
—Apple CEO Tim Cook, repeating a maxim attributed to Steve Jobs
This paper argues that a shift from Fortress to Frontier would benefit the health and finances of Americans. Here I argue that the task begins by easing limits on the supply of health care services, thereby clearing
the way for innovators to take health care in directions we cannot yet imagine.The government’s release of the ARPANET did not create the IT inno-
vations that followed. But this action created an environment that would attract and nurture innovators who could create them. And a vital part of that environment was the relatively hands-off approach taken by the federal and state governments. Innovators did not have to slow-walk their ideas through expensive, time-consuming regulatory processes.
When imagining a similar process in health care, it’s helpful to recall just how far IT has come in a short period of time. It is also important to understand how reasonable it would have been to stymie the supply of IT, given the risks it posed (and poses).
Long Distance, Short Time
To grasp the enormous changes that have taken place in information technol-ogy over the past 25 years, consider the following hypothetical scenario:
While camping high in the Rockies, Efram signed and depos-ited his paycheck in his bank account. Then he purchased The Complete Works of Shakespeare and read Macbeth. A bit later, on YouTube, he watched the Beatles sing “Yellow Submarine.” Using Google Translate, he converted the lyrics into Hindi and then Skyped his friend Arjun, who is working at McMurdo Station, Antarctica. Efram sang his translation to Arjun, who grimaced, but then commented on the beauty of the towering mountain behind Efram. After hanging up, Arjun emailed a restaurant in Denver (a city he has never visited), and an hour later a drone delivered Indian food to Efram’s campsite—all paid for with bitcoins. While eating his tikka masala, Efram toured McMurdo Station via Street View and asked Siri for the

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
40
current temperature there. “Brrrr. It’s 10 degrees below zero Fahrenheit, Efram,” she answered. Then he accessed Netflix and watched Seven Samurai before dozing off to a selection of Malian jazz, courtesy of iTunes Radio.
The entire cost of this sequence of events was $34.77—$0.99 for the Kindle edition of Shakespeare, $2.00 for the film, $26.78 for the food, and $5.00 for the drone delivery service. And the whole set of interactions required only Efram’s iPad and Arjun’s cell phone—the two devices together costing less than $1,000.
Tell this story to someone in 2014 and he or she might be mildly surprised by the drone and bitcoins, but will likely find the rest of the story cute—even mundane.88 Nothing remarkable. If you had told the story to someone in 1989, however, he or she would have assumed you were a lunatic or an overwrought science fiction buff.
Now try the same thought exercise in health care. Since 1989, there have been some miraculous innovations, but the 1989 patient and the 1989 doctor would still find their 2014 surroundings fairly familiar. A 2014 patient trans-ported back to 1989 might sorely lack some newer drugs and procedures and equipment, but would have little trouble navigating the hospitals, doctors’ waiting rooms, insurance filings, pharmacies, and so forth.
How IT Could Have Been Slowed
Why are we so much more risk-averse and deferential to insiders in health care than in other fields, such as IT? One argument stresses that health care involves life versus death, health versus sickness, and comfort versus pain. But is health care so different in this respect? Engineers, pilots, auto mechanics, taxi drivers, electricians, food handlers, firefighters, and legions of others can also cause (or fail to prevent) pain, sickness, and death. Conversely, one could argue that microcomputers and cell phones have contributed as much to the task of sav-ing lives as MRIs and heart transplants. After all, the massive data flows, smart systems, Internet applications, and telecommunications are critical parts of the modern health care system.
88. Drone food deliveries are not yet commonplace, but the delay is a function of regulation, not technology. See Eli Dourado, “The Most Important Issue of the 2012 Election? TacoCopters,” Eli Dourado, September 7, 2012, http://elidourado.com/blog/tacocopters/.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
41
Knowing what we know today, it would not be hard to persuade a cau-tious observer in 1989 to radically slow the pace of IT innovation. IT arguably poses personal risks as grave as those that health care poses. Cell phones have been essential components of improvised explosive devices in war zones. The 9/11 atrocities would have been difficult or impossible to carry out without cell phones. Thieves have used the Internet to steal. Stalkers have used the Internet to terrify their prey. Child predators find their victims on the web. People have been murdered by strangers they met in chatrooms. IT has allowed individu-als and governments to violate others’ privacy in countless ways. Drug dealers and terrorist networks organize their efforts via cell phone and Internet. The Internet has greatly reduced the cost of destroying another’s reputation, and news accounts tell of suicides following cyberbullying.
Our laws demand terribly high standards of safety and efficacy for drugs. We require no such standards for computers, cell phones, and software, but given the nefarious uses to which they are sometimes put, decades ago one could easily have argued for doing so. Had we done so, we would now be living in a much poorer, less interesting world—and perhaps one with even greater risks to life and limb than we have now. No online predators or improvised explosive devices, but also no OnStar to save you after an automobile crash or smartphone to alert police to your life-threatening situation and geographic location.
We can ascribe the rapid rate of technological change in electronics to, using my colleague Adam Thierer’s expression, “permissionless innovation.”89 This refers to a relatively unbridled ability to start and end companies and to offer new products and services. Permissionless innovation is the opposite of the precautionary principle—the notion that policy should focus most heavily on preventing bad things from happening.
Innovation in the Near Term
Moving IT from the Fortress to the Frontier was largely an act of choice. Various parts of the federal government decided to step away from IT and let innovators flourish. Why this happened ought to puzzle political scientists for a long while. Our restraint of health care within the Fortress may also puzzle the same analysts.
Moving health care from the Fortress to the Frontier may be more a
89. Thierer, Permissionless Innovation, 4–5. The phrase was listed among four innovation buzzwords by Dominic Basulto in “Four Innovation Buzzwords You Need to Know,” Washington Post, October 16, 2014, http://wapo.st/1reP6R8.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
42
matter of necessity than of choice. We are entering a period of rapid techno-logical advances that will radically alter health care. Many of these advances require only modest capital and labor inputs that governments cannot easily control or prohibit. If US law obstructs these technologies here, it will be fea-sible for Americans to obtain them by Internet, by mail, or by travel.
We are likely to see, or are already beginning to see, the following:
• Genomic knowledge will offer the possibility of personalized medicine—drugs custom-made for a single person, based on his or her molecular structure.90 Cancer was once viewed as a single disease. Now we know it is many diseases. Soon, we may view Joe’s colon cancer and Ed’s colon cancer as distinct entities.
• 3-D printing will evolve from offering inexpensive prosthetics to print-ing new organs, made of the recipients’ own cells—reducing or eliminat-ing the need for donors or immunosuppressants.91
90. Huber, Cure in the Code, 132.91. Stephanie Innes, “Instead of Waiting for Donor Organs, Patients Could Have New Ones Grown in the Lab,” Arizona Daily Star, October 27, 2013, http://bit.ly/1vVSh7T (featured on the University of Arizona’s website); “Utilizing Organovo Novotissues in Research: Living, Three-Dimensional Human Tissue Models for Research and Therapeutic Applications,” Organovo website, accessed October 3, 2014, http://www.organovo.com/tissues-services.
Fortress and Frontier compete: Celera Genomics (a private company) and the National Human Genome Research Institute (a public agency) competed to map the human genome, finishing the task shortly after 2000. Here, President Bill Clinton recognizes the achievement, flanked by Celera’s J. Craig Venter (left) and NHGRI’s Francis Collins (right). Credit: Ron Sachs/CNP/Sygma/Corbis.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
43
• Artificial intelligence will mine mountains of data, gathered in real time from vast arrays of patients, and will detect patterns leading to treatments that could never arise from human intuition or 20th cen-tury statistical methods. Already IBM’s Watson technology explores the Internet and the world to learn far beyond what its programmers ever envisioned.92 Manhattan Institute scholar Peter Huber argues that Google search algorithms could have identified AIDS or asbestos injuries far earlier by identifying clusters of Kaposi’s sarcoma or mesothelioma,93 though such methods have yet to be verified as reliable and consistent with data privacy.
• Social media will allow medical professionals and ordinary people to enjoy unprecedented synergies from shared information.94 (Of course, this data-sharing carries the possibility of privacy breaches and misuse of data.)
• Wearable telemetry will allow health care providers to monitor indi-viduals’ biometrics in microscopic detail on a continuous basis. Instead of the single atypical blood pressure reading during a checkup, they will have access to moment-by-moment measurements as the patient goes through daily life.95 (Again, on the downside, breach of privacy is a concern.)
• Telemedicine will offer patients instantaneous primary and specialty care from remote providers. For a rare and difficult surgery, why depend
92. This, of course, is the stuff of science fiction. Some will think of HAL, the sentient computer in 2001: A Space Odyssey—a modern rendering of the Frankenstein story. In fact, one problem is that Watson found its (his?) way onto the web’s Urban Dictionary and began using obscenities.93. Huber, Cure in the Code, 18.94. Oliver Sacks describes the web-based community of achromatopsia sufferers, whose debilitat-ing genetic condition results in total color blindness. Earlier in history, people with the condition and their physicians rarely, if ever, encountered a single other sufferer (except, perhaps, a sibling with the same inheritance). Now medical science is learning about the illness via crowdsourcing. Oliver Sacks, Island of the Colorblind (London: Vintage, 1998). RareShare (http://rareshare.org/) is a central social networking site for victims of various extremely rare conditions. These innovations are not totally unprecedented: in Innovator’s Prescription, Christensen, Grossman, and Hwang note that ancient Greek physicians practiced a sort of crowdsourcing. They would take a patient with an unidenti-fied illness and lay him down in the middle of the agora, asking passersby if they had ever seen the patient’s symptoms before.95. Nicholas Gonzalez, “Big Data Analytics for Device-Driven Data Will Drive Even Bigger Change,” Wired: Innovation Insights, August 22, 2013, http://insights.wired.com/profiles/blogs/big-data -analytics-for-device-driven-data#axzz38ILF43pj. For a survey of mobile medical devices, see Nathan Cortez, “The Mobile Health Revolution?,” UC Davis Law Review 47 (2014): 1173–230, avail-able through SSRN at http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2284448.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
44
on local surgeons when robotics and the web provide access to the world’s leading expert?96
• Nanobots will be able to analyze and treat patients from within their own bodies. Disastrous genetic aberrations will become treatable illnesses.97
The question, then, is how one might move the health care environment in America toward the Frontier—giving innovators the freedom and incentive to take advantage of these and other developing technologies. The next section offers some suggestions.
96. Wired’s telemedicine articles can be found at http://www.wired.com/tag/telemedicine/.97. Julie Steenhuysen, “Nanotech Robots Deliver Gene Therapy through Blood,” Reuters, March 21, 2010, http://www.reuters.com/article/2010/03/21/us-cancer-rnai-idUSTRE62K1BK20100321.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
45
V. ISLAND-HOPPING AND LEAPFROGGING
What’s the biggest thing we could do to “bend the cost curve,” as well as finally tackle the ridiculous inefficiency and consequent low quality of health-care delivery? Look for every limit on supply of health care
services, especially entry by new companies, and get rid of it.
—John Cochrane, University of Chicago
For the most part America’s current health care debate has not been Fortress versus Frontier, but rather one Fortress versus another Fortress. The Affordable Care Act imposes a high degree of central-
ized control over the sector—both over health insurance and over health care itself. Many Repeal and Replace backers support strong controls on care and insurance at the state level. A shift to the Frontier is not prominent in the dis-cussions. At this juncture, wholesale repeal of the ACA seems unlikely during the next few years.
To shift health care toward the Frontier may require a disaggregated approach. Identify legions of obstructions to supply and innovation, and elimi-nate them. For a metaphor, think of America’s World War II Pacific Theater operations: pursue thousands of islands simultaneously and autonomously. This chapter will suggest some potential “islands” where one might begin.
The virtues of this island-by-island strategy include the following: (1) Pursuing smaller, more targeted goals raises the probability of some rapid vic-tories. (2) Those near-term victories could lead to some highly visible near-term examples of lives saved, suffering eased, and costs cut. (3) Different coali-tions could form around each island, eliminating the need for one grand bar-gain. (4) Different groups could simultaneously deal with federal, state, and private limits on the supply of health care. (4) The piecemeal, decentralized nature of this strategy obviates the need for total control of Washington, DC.
Expanding on the World War II analogy, a military historian suggested to me that such a strategy could entail both island-hopping (taking adjacent islands one by one) and leapfrogging (going around tougher islands to focus on opportune targets). Island-hopping reformers might move state-by-state against a particular barrier (e.g., certificate-of-need laws) or policy-by-policy within a single state. Leapfrogging would entail discontinuous leaps from state to state and policy to policy.
One of the more intriguing possibilities is that smaller fixes offer the possibility of temporary and unconventional alliances. A conservative or lib-ertarian in Texas could rail against regulatory impediments to telemedicine;

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
46
in doing so, he or she would likely find some allies among the high-tech entre-preneurs and Lyft-loving98 millennials in Austin and among Latinos in South Texas. The same conservative or libertarian could complain about the FDA’s ban of 23andMe; in doing so, he or she would again likely find allies among Silicon Valley entrepreneurs, among left-leaning users of Uber taxi services, and among privacy advocates.
The Washington Post recently ran an article on the FDA’s cease-and-desist order against 23andMe’s services. The article noted that the family of the company’s cofounder, Anne Wojcicki, is deeply involved in progressive poli-tics. But it also noted the shock and furor with which Silicon Valley received the news, and the technology community’s antipathy toward precautionary regulation.99
Author Steven Johnson has written about the unusual alliances that form over technology issues. He cites the example of the battle over the Stop Online Piracy Act (SOPA), which would have subjected Internet users to considerable
98. Patrick Tolbert, “Austin Impounds Lyft Drivers’ Cars,” KXAN.com, June 2, 2014, http://kxan.com /2014/06/02/austin-impounds-lyft-drivers-cars/.99. Ariana Eunjung Cha, “23andMe Co-founder Anne Wojcicki’s Washington Charm Offensive,” Washington Post, June 27, 2014, http://www.washingtonpost.com/national/health-science/23andme -co-founder-anne-wojcickis-washington-charm-offensive/2014/06/27/b465b086-f240-11e3-9ebc -2ee6f81ed217_story.html.
Fortress snatches Frontier: 23andMe offers home genetics tests (left) providing consumers with information on roughly 250 aspects of their DNA. The FDA ordered 23andMe to stop providing customers with explanatory materials about their personal results. Since then, 23andMe has been reduced from a potentially powerful health maintenance tool to a DNA-based genealogy service. Pictured on the right is CEO Anne Wojcicki. Credit: 23andMe (left) and Jean Philippe Piter (right).

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
47
liability over use of copyrighted materials. As described by Johnson, SOPA was initially pushed by a bipartisan coalition in Congress. It was effectively defeated by an online uprising against the bill. When the episode was over, Johnson stressed, the result could not be cast as a victory for Left or Right, for Democrats or Republicans.100
The pages below name a dozen specific areas where obstacles block the supply of health care. As the previous section stated, eliminating obstacles to supply can be essential to enticing and nurturing innovators.
The list of potential fixes described below is not comprehensive; it is merely illustrative of the possibilities for meaningful reform. It comprises 35 potential solutions categorized into 12 general areas. In truth, the number of potential solutions is far higher. “Abolish certificate-of-need requirements” is one entry, but dozens of states have certificate-of-need laws. “Abolish cer-tificate-of-need requirements in Virginia” and “abolish certificate-of-need requirements in Ohio” could be viewed as two different proposals. “Expand the scope of practice for nurse practitioners in California” and “expand the scope of practice for optometrists in California” could be considered two sepa-rate policy actions. Thus, one could devise hundreds of self-contained policy initiatives. And separating them in this way creates hundreds of opportunities for strange-bedfellow coalitions—coalitions that could never coalesce into a unified, national, omnibus bill to repeal and replace the ACA.
This section suggests some ideas for reform along the lines of economist John Cochrane’s challenge to “look for every limit on supply of health care ser-vices . . . and get rid of it.”101 Just as a pair of scissors requires both blades, inno-vation requires flexibility on both the supply and the demand sides of the mar-ket. Innovators must be free to supply new goods and services—and consumers must be free to purchase the innovations. Public policy can short-circuit the process by discouraging either the supply side or the demand side. And it can do so either by overtly prohibiting participation or by making participation prohibitively costly or risky.
The rest of this section details a few of these supply-side and demand-side barriers. Each discussion includes possible solutions that others have proposed. Among the many potential limits on supply not addressed here are inefficiencies in patent and copyright law, obstacles to specialty hospitals, and import and reimport of drugs.
100. Steven Johnson, Future Perfect: The Case for Progress in a Networked Age (New York: Riverhead Books, 2012), 211–16.101. John H. Cochrane, “After the ACA: Freeing the Market for Health Care” (working paper, June 2014), http://faculty.chicagobooth.edu/john.cochrane/research/papers/after_aca.pdf.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
48
The FDA’s Approval Process for New Drugs and Devices Is Slow, and Its Evaluation Methodologies ObsoleteThe FDA’s approval process for new drugs and medical devices is slow, bur-densome, expensive, and unpredictable.102 The process inhibits the develop-ment and dissemination of new drugs. Milton and Rose Friedman identified a key incentive problem in the FDA’s regulatory system: the consequences of releasing a harmful drug are visible, whereas the consequences of failing to release a valuable drug are invisible. Hence, they argued, the FDA has an innate bias against approvals.103
As noted previously, the thalidomide experience remains a driving force behind the FDA’s go-slow approach.104 Manhattan Institute scholar Paul Howard writes, “Aside from the efficacy requirement, the FDA arguably learned the wrong lessons from the thalidomide tragedy: namely, that its pri-mary job was to keep bad things from happening, rather than accelerate mar-ket access for truly innovative medicines.”105 Tufts University scholars Joseph DiMasi and Christopher-Paul Milne and George Mason University scholar Alex Tabarrok estimate that a more efficient approval process could save $900 million in development costs annually, plus add an estimated $4 trillion to the economy in social value from lives saved.106 As noted earlier, this phenomenon came to the public’s attention in the early days of the HIV/AIDS crisis and was dramatized in the film Dallas Buyers Club.
A more recent example of the cost of withholding approval involves FDA delays in allowing the use of a vaccine to protect against the deadly meningi-tis B bacteria. Bexsero, a vaccine produced by Novartis, is available in Europe, Canada, and Australia, but not in the United States. In the case of meningitis B
102. For a good discussion of the problems with FDA medical regulations, see Huber, Cure in the Code. For an outline of the potentially lethal effects of the FDA’s sluggish procedures, see Nick Gillespie, “Kill the FDA (before It Kills Again),” Daily Beast, March 9, 2014, http://www.thedaily beast.com/articles/2014/03/09/kill-the-fda-before-it-kills-again.html. See also Competitive Enterprise Institute, “FDA Too Slow to Approve New Medical Drugs and Devices,” news release, April 30, 2002, http://cei.org/news-releases/fda-too-slow-approve-new-medical-drugs-and-devices.103. Milton and Rose Friedman, Free to Choose: A Personal Statement, 1st Harvest ed. (New York: Harcourt Brace, 1990 [1979]), 203–10.104. Margaret Hamburg, “50 Years after Thalidomide: Why Regulation Matters,” FDA Voice (US Food and Drug Administration), February 7, 2012, http://blogs.fda.gov/fdavoice/index.php/2012 /02/50-years-after-thalidomide-why-regulation-matters/.105. Howard, “50 Years after Thalidomide: What Lessons Should We Learn?,” Medical Progress Today (Manhattan Institute), February 8, 2012, http://www.medicalprogresstoday.com/2012/02 /50-years-after-thalidomide-what-lessons-should-we-learn.php.106. DiMasi, Milne, and Tabarrok, “An FDA Report Card: Wide Variance in Performance Found among Agency’s Drug Review Divisions” (Project FDA Report No. 7, Manhattan Institute, April 2014), http://www.manhattan-institute.org/html/fda_07.htm#.U8-hJWONigB.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
49
outbreaks (some on college campuses), authorities have had to plead with the FDA for special permission to import and administer the drug. One student, Emily Stillman, died while the approval process played out. Her mother is con-ducting a campaign for an expedited approval process.107
The FDA evaluates drugs on the basis of “gold stan-dard” statistical tests, developed in the middle of the 20th century. These tests demand large samples of test sub-jects, generally require many years of observation, and are extremely expensive to conduct. Peter Huber argues that the FDA’s gold standard methods are not appropriate in an era when molecular structure is observable and when inexpensive computing power allows more appropriate statistical analyses that would have been prohibitively expensive or impossible in the past.108
Huber argues that modern science is being shoe-horned into antiquated statistical methodologies, slowing the pace of drug development. In particular, he argues, the traditional tests cannot accommodate molecular medi-cine—drugs fitted to a single individual’s DNA. Congress could implement some or all of the following reforms:
• Allow adaptive licensing. Currently, drug approval is mostly thumbs-up or thumbs-down. Some have proposed that approval proceed in stages. Patients with serious, time-critical illnesses would gain early access to a drug not yet approved for the general pop-ulation. In turn, data from these early users would inform the approval process at later stages.109
107. For a description of the Stillman case and other examples where slow approval has resulted in loss of life and limb, see Henry I. Miller, “A Grieving Mother Acts, While the FDA Dithers,” Forbes, May 21, 2014, http://www.forbes.com/sites/henrymiller/2014/05/21/3230/.108. See Huber, Cure in the Code. Huber also surveys gold-standard-related issues in “The Digital Future of Molecular Medicine: Rethinking FDA Regulation” (Project FDA Report No. 6, Manhattan Institute, May 2013), http://www.manhattan-institute.org/html/fda_06.htm#.VC8P5oBdVfQ.109. See H.-G. Eichler et al., “Adaptive Licensing: Taking the Next Step in the Evolution of Drug Approval,” Clinical Pharmacology & Therapeutics 91, no. 3 (2012): 426–37, http://www.nature.com/clpt/journal/v91/n3/full /clpt2011345a.html.
“The traditional tests cannot accommodate molecular medicine—drugs fitted to a single individual’s DNA.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
50
• Institute right-to-try laws. Several states have approved or are consid-ering “right to try” legislation that would grant terminally ill patients a right to access as-yet-unapproved drugs.110
• Permit the “Free to Choose Medicine” option. This plan would retain the FDA’s present approval process (perhaps with improvements over time), but would grant doctors and patients the option of using unap-proved drugs under certain conditions.111
• Make full use of modern data techniques and sources. Artificial intel-ligence systems make widespread use of Bayesian statistical methods, which Google, Amazon, and others use to predict behavior. The FDA should make better use of such techniques and also integrate data from Google and other search engines into the data-mining process. (As noted earlier, the efficacy of this technology needs study, and privacy concerns need to be addressed.)
The FDA’s Scope Is Overbroad
The FDA is stifling innovation by exerting authority over too many goods and services, which it does by expanding the definition of a drug or medical device. There is an ongoing discussion over the extent of the FDA’s authority to reg-ulate cell phones and other wireless devices, since, for example, cell phones often have health-related apps.112 (For now, the FDA has relented somewhat in its drive for more control over such devices.) A striking example of the FDA’s reach (as discussed earlier) is the recent experience of 23andMe, which sells a $99 home genetics test that informs consumers of their status with respect to more than 240 genetic factors—a powerful tool for individuals who wish to
110. See Goldwater Institute, “Media Advisory: Missouri Becomes Third State in Nation to Give Dying Patients’ ‘Right to Try’ Life-Saving Experimental Medicines; Michigan Lawmakers to Take Up Reform This Week,” news release, July 15, 2014, http://goldwaterinstitute.org/article/media-advisory -missouri-becomes-third-state-nation-give-dying-patients-right-try-life-saving; Christina Corieri, “Everyone Deserves the Right to Try: Empowering the Terminally Ill to Take Control of Their Treatment” (Policy Report No. 266, Goldwater Institute, Phoenix, AZ, February 11, 2014), http://goldwaterinstitute.org/article/everyone-deserves-right-try-empowering-terminally-ill-take -control-their-treatment.111. Bartley J. Madden and Gregory Conko, “Free to Choose Medicine,” Engage 14, no. 3 (October 2013), available at http://www.fed-soc.org/publications/detail/free-to-choose-medicine.112. “Wireless Medical Devices,” US Food and Drug Administration website, last updated June 12, 2014, http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ConnectedHealth /WirelessMedicalDevices/default.htm.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
51
manage their own health carefully.113 The FDA argued that the service consti-tuted the practice of medicine and banned the company from distributing some of the information provided by its service.114
Meanwhile, the founders of Google recently voiced hesitation about adding health care to their business plan because of the pervasiveness of health care regulations.115 The FDA may soon require generic drug manufac-turers to implement expensive label warnings about new safety concerns; the regulation would also expose the manufacturers to lawsuits.116 And finally, the FDA is—possibly illegally—regulating one’s own adult stem cells as if they were drugs.117
In the Internet era, it is essential to ask whether the FDA’s current approval process is fundamentally anachronistic. In the 20th century, one could argue that FDA approval was justified by the fact that information about the risks and rewards of drugs and devices was difficult for patients and even doctors to come by. Today, however, the web offers vast quantities of informa-tion, as well as powerful tools for evaluating the quality of that information. One might ask whether the FDA has become redundant or, thanks to institu-tional limits and malincentives, inferior to more informal sources of informa-tion on drug and device safety.118
Alex Tabarrok notes that Western Europe has a far more focused and rapid drug approval process. Tabarrok writes, “One key reason for Europe’s efficient approval process is that European governments don’t review medi-cal devices directly. Instead they certify independent ‘notified bodies’ that
113. 23andMe website, accessed October 3, 2014, https://www.23andme.com/. See also Peter Huber, “Is the Food and Drug Administration Killing Personalized Medicine?,” Reason, December 2, 2013, http://www.geneticliteracyproject.org/2013/12/02/is-the-food-and-drug-administration-killing -personalized-medicine/.114. Alberto Gutierrez, Food and Drug Administration, to Anne Wojcicki, CEO of 23andMe, November 22, 2013, Warning Letter, available at http://www.fda.gov/iceci/enforcementactions /warningletters/2013/ucm376296.htm.115. Michael F. Cannon, “Google Co-founders Sergey Brin & Larry Page: Health Care Regulation Is Blocking Innovation,” Cato at Liberty (Cato Institute), July 10, 2014, http://www.cato.org/blog /google-co-founders-sergey-brin-larry-page-health-care-regulation-blocking-innovation.116. Scott Gottlieb, Alex Brill, and Robert W. Pollock, “Proposed FDA Generic Drug Regulation: Higher Prices, No Public Health Benefit” (Health Policy Outlook, American Enterprise Institute, Washington, DC, March 2014), http://www.aei.org/article/proposed-fda-generic-drug-regulation -higher-prices-no-public-health-benefit/.117. Scott Gottlieb and Colleen Klasmeier, “The FDA Wants to Regulate Your Cells,” Wall Street Journal, August 7, 2012, http://online.wsj.com/news/articles/SB10000872396390444405804577558992030043820.118. For a discussion of problems with FDA medical regulations, see Huber, Cure in the Code.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
52
specialize and compete to review new products.”119 The notified bodies expedite approvals via reciprocity agree-ments. In the United States, Underwriters Laboratories plays a similar role in assuring the safety of electrical devices and other systems.
It’s also worth noting that not all the federal gov-ernment’s potential innovation-stifling restrictions come from the FDA. The Health Insurance Portability and Accountability Act is also a force to reckon with.120 This act governs health care privacy issues, and the flows of personal health data into the cloud and into databases presents pos-sibilities of privacy breaches. Going forward, a recurring challenge will be balancing the desire for privacy against the potential for improving health through technology.
Four potential reforms follow:
• Guarantee Americans a “right to know.” Acknowledge that individuals have a right to pos-sess their own genetic information and to receive information about how to interpret the results.121
• Legislate constraints on the FDA’s authority over various classes of devices. Senators Deb Fischer (R-NE) and Angus King (I-ME) have suggested such reforms.122
• Shift to a narrower, more decentralized approval process. The European approval process described by Tabarrok is a possible model.
119. Tabarrok, review of Innovation Breakdown: How the FDA and Wall Street Cripple Medical Advances, by Joseph V. Gulfo, Wall Street Journal, August 11, 2014, http://online.wsj.com/articles/book-review-innovation -breakdown-by-joseph-v-gulfo-1407799461.120. Mark Sullivan, “Health Apps Could Be Heading into a HIPAA Showdown,” VentureBeat, June 13, 2014, http://venturebeat.com/2014/06 /13/health-apps-could-be-heading-into-a-hipaa-showdown/.121. Cha, “23andMe Co-founder Anne Wojcicki’s Washington Charm Offensive.” See also descriptions of the potential benefits of products like 23andMe in Huber, Cure in the Code, chapter 18, “The Right to Sniff.”122. Deb Fischer and Angus King, “FDA’s Slow Process Hurts Innovation,” USA Today, February 15, 2014, http://www.usatoday.com/story/opinion /2014/02/15/fischer-king-health-information-technology/5464693/.
“Acknowledge that individuals have a right to possess their own genetic information and to receive information about how to interpret the results.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
53
• Restrict the FDA to a safety-only role. Currently, the FDA is charged with assuring the safety and efficacy of drugs and devices. Andy Grove, former CEO of Intel, has suggested that the FDA’s role be limited to safety only and that questions of efficacy be left to the market.123
Certificate-of-Need Laws Discourage Innovation and Competition
Many states require that hospital developers obtain government permission before building a new facility, or expanding an existing one, or even adding a specific piece of medical equipment, such as a CT scan machine. This has the effect of protecting established providers from competition. It is also a poten-tial source of corruption.
Many certificate-of-need (CON) laws were responses to the National Health Planning and Resources Development Act of 1974.124 The reasoning behind CON was that additional supply of medical resources would lead to additional demand—a dubious hypothesis. CON laws, the proponents argued, would help restrain health care spending. A 2004 report from the Federal Trade Commission and the Department of Justice explains, “The Agencies believe that, on balance, CON programs are not successful in containing health care costs, and that they pose serious anticompetitive risks that usu-ally outweigh their purported economic benefits. Market incumbents can too easily use CON procedures to forestall competitors from entering an incum-bent’s market.”125
Health care policy scholars Christopher Conover and Frank Sloan find no evidence that the repeal of CON laws has resulted in increased spending.126 Therefore, state governments should make the following reform:
• Abolish certificate-of-need requirements.
123. Alex Tabarrok, “Andy Grove on Reforming the FDA,” Marginal Revolution, October 1, 2011, http://marginalrevolution.com/marginalrevolution/2011/10/andy-grove-on-reforming-the-fda.html.124. Pub. L. No. 93-641, 88 Stat. 2225 (1975).125. Federal Trade Commission and Department of Justice, “Improving Health Care: A Dose of Competition,” July 2004, http://www.ftc.gov/reports/improving-health-care-dose-competition -report-federal-trade-commission-department-justice.126. Conover and Sloan, “Does Removing Certificate-of-Need Regulations Lead to a Surge in Health Care Spending?,” Journal of Health Politics, Policy and Law 23, no. 3 (June 1998): 455–81. See also Jon Sanders, “Certified: The Need to Repeal CON; Counter to Their Intent, Certificate of Need Laws Raise Health Care Costs” (Spotlight No. 445, John Locke Foundation, Raleigh, NC, October 25, 2013), http://www.johnlocke.org/research/show/spotlights/296.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
54
Protectionist Licensing Practices Constrain the Supply of Physicians
A maze of medical licensing restrictions constricts the supply of physicians throughout the United States. States differ in their willingness to license inter-national medical graduates. Some states put barriers in the way of doctors moving from other states. These restrictions make it difficult to optimize man-power levels, a problem that is likely worse at the specialty level. In some states, they create physician shortages.
These restrictions have negative impacts on innovation. First, a certain amount of innovation comes from serendipity—a doctor from one state sharing observations with his new colleagues in a different state. Furthermore, current licensing arrangements impede the development of telemedicine.
University of Virginia scholars Brenton Peterson, Sonal Pandya, and David Leblang describe how physician licensing boards use their pow-ers to erect protectionist barriers against migrants and would-be migrants: “Licensure regulations ostensibly serve the public interest by certifying com-petence, but they can simultaneously be formidable barriers to entry by skilled migrants.” They show that in states where physicians have greater control over licensing, barriers to entry are greater and fewer migrants enter. They estimate that “over a third of all US states could reduce their physician shortages by at least 10 percent within 5 years just by equalizing migrant and native licensure requirements.”127 An earlier version of their paper catalogs restrictions on the licensing of currently out-of-state doctors.128
State governments should institute the following reforms:
• Expand licensing reciprocity agreements with other states.
• Establish an interstate licensing compact.129
127. Peterson, Pandya, and Leblang, “Doctors with Borders: Occupational Licensing as an Implicit Barrier to High Skill Migration,” Public Choice 160, no. 1-2 (July 2014): 45–63, http://link.springer .com/article/10.1007%2Fs11127-014-0152-8#page-2.128. Peterson, Pandya, and Leblang, “Doctors with Borders: Occupational Licensing as an Implicit Barrier to High Sckill Migration” (working paper, University of Virginia Department of Politics, March 2013), http://www.batten.virginia.edu/sites/default/files/fwpapers/Leblang_Pandya _Peterson_Doctors.pdf.129. See Robert Pear, “Medical Boards Draft Plan to Ease Path to Out-of-State and Online Treatment,” New York Times, June 29, 2014, http://mobile.nytimes.com/2014/06/30/us/medical -boards-draft-plan-to-ease-path-to-out-of-state-and-online-treatment.html?partner=rssnyt&emc =rss&_r=1&referrer=.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
55
Scope-of-Practice Limits Constrain the Value of Nonphysician ProvidersThe US health care system could gain greater efficiency by pushing back the limits within which certain providers can practice. Some states, for instance, allow nurse prac-titioners to have independent practices.130 The Chicago Tribune’s Steve Chapman suggests nurse practitioners as a way of easing physician shortages.131 Ophthalmologists have fought fiercely against allowing optometrists to cross over into their turf.132 Primary care physicians have fought against allowing pharmacists to write certain prescrip-tions.133 Psychologists have also sought the ability to pre-scribe medications.134
The following reforms would expand the scope of practice for certain medical providers:
• Allow nurse practitioners, optometrists, and others to practice independently of physicians. Eighteen states currently allow nurse practitioners this option. In 2013, the California legislature declined to do so.135
130. For an estimation of cost savings from increasing nurse practitioners’ scope of practice, see Morris M. Kleiner et al., “Relaxing Occupational Licensing Requirements: Analyzing Wages and Prices for a Medical Service” (NBER Working Paper No. 19906, National Bureau of Economic Research, February 2014), http://m.nber.org//papers/w19906.131. Steve Chapman, “Nursing Our Way Out of a Doctor Shortage,” Reason, April 19, 2010, http://reason.org/news/printer/nursing-doctor-shortage.132. Jena Passut, “Kentucky Governor Signs Law to Expand Optometric Scope of Practice,” EyeWorld, March 2011, http://www.eyeworld.org /article-kentucky-governor-signs-law-to-expand-optometric-scope-of -practice.133. “FDA Proposal to Allow Pharmacists to Prescribe Some Drugs Sparks Swift Rebuke from AAFP,” American Academy of Family Physicians, May 2, 2012, http://www.aafp.org/news/government-medicine/20120502 pharmprescribing.html.134. See, for example, Kim L. Lavoie and Richard P. Fleet, “Should Psychologists Be Granted Prescription Privileges? A Review of the Prescription Privilege Debate for Psychiatrists,” Canadian Journal of Psychiatry 47, no. 5 (June 2002): 443–49. 135. Melanie Mason, “State Bill to Boost Use of Nurse Practitioners Goes Nowhere,” Los Angeles Times, September 1, 2013, http://articles.latimes .com/2013/sep/01/local/la-me-healthcare-20130902.
“The US health care system could gain greater efficiency by pushing back the limits within which certain providers can practice.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
56
• Allow pharmacists to write certain prescriptions independently of physicians. In 2013, a new California law declared pharmacists to be health care providers. According to the University of Southern California’s School of Pharmacy, “The bill authorizes pharmacists to pro-vide basic care services in collaboration with physicians, medical homes and other systems of care where patients receive treatments.”136
The Vagaries of Tort Law Invite Lawsuits and Judgments and Deter InnovationPhysicians and other providers can be sued for performing procedures explic-itly approved by the FDA and other agencies. In other words, a doctor can fol-low the letter of the law and standard medical practice, and a jury can second-guess these prior approvals.
A 2010 Harvard study estimated that the costs of the medical liability system—insurance premiums, judgments and settlements, and defensive medi-cine—add roughly 2.4 percent ($55 billion in 2010) to US health expenditures.137 A PricewaterhouseCoopers article puts the estimate at 10 percent, on the high end for such studies.138 While these percentages are not earthshaking, they do show that the distortions related to the medical liability system constitute an expensive problem. Furthermore, none of these estimates include the extent to which a nebulous legal environment discourages innovation.
In 2013, the Congressional Budget Office conducted a study on options for limiting malpractice costs in 2013 and mentioned several legislative strate-gies for doing so.139 Possibilities include the following:
136. “Pharmacists Are Declared Providers in California,” University of Southern California School of Pharmacy, October 3, 2013, https://pharmacyschool.usc.edu/feature/pharmacists-are-declared -providers-in-california/.137. Michelle M. Mello et al., “National Costs of the Medical Liability System,” Health Affairs 29, no. 9 (September 2010): 1569–77, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3048809/.138. Lawrence J. McQuillan and Hovannes Abramyan, “The Facts about Medical Malpractice Liability Costs,” Health Policy Prescriptions (Pacific Research Institute) 7, no. 10 (October 2009), http://www.pacificresearch.org/docLib/20091007_HPPv7n10_1009.pdf. McQuillan and Abramyan review a number of studies and note that while malpractice-induced expenditures may be a small percentage of overall health expenditures, there may be a very large effect in certain subsectors of health care.139. “Options for Reducing the Deficit: 2014 to 2023,” Congressional Budget Office, November 13, 2013, http://www.cbo.gov/budget-options/2013/44892.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
57
• Cap awards for noneconomic damages. Limit the amount of the award a party can receive for noneconomic damages, such as pain and suffering, to some dollar figure—for instance, $250,000.140
• Shorten the statute of limitations.141 Shorten the statute to one year (for adults) and three years (for children).
• Establish a fair-share rule.142 Stipulate that a defendant is only respon-sible for a percentage of the final award reflecting the particular defen-dant’s share of responsibility for the injury.
• Establish vaccine safe harbors. The vagaries of the US tort system have damaged America’s capacity to produce or procure vaccines. Notably, benefit-cost analyses have shown childhood vaccines to provide the greatest bang for the buck of any medical intervention.
• Institute “loser pays” rules. In some countries, an unsuccessful plaintiff in a tort case may have to pay the defendant’s legal costs.143
ACA Taxes on Name-Brand Drugs and Medical Devices Deter InnovationTwo of the ACA’s taxes penalize medical innovation in the arenas of drugs and devices. This is especially destructive at a time when genomic medicine, 3-D printing, wireless telemetry, and a host of other blockbuster innovations are just taking shape.
First is a tax on name-brand pharmaceuticals, which discourages manu-facturers from developing new drugs. The Preserving Access to Orphan Drugs Act of 2013 was offered as a way of lifting this burden on certain research.144 Second is a 2.3 percent gross receipts tax on medical devices, discouraging product development and diffusion.
Economist Douglas Holtz-Eakin makes the case against the device tax.145 As a gross receipts tax, the device tax falls especially hard on start-ups, which
140. Ibid.141. Ibid.142. Ibid.143. Marie Gryphon, “Reconsidering ‘Loser Pays,’” Manhattan Institute, accessed August 31, 2014, http://www.manhattan-institute.org/html/reconsidering_loser_pays.html.144. H.R. 2315, 113th Cong. (2013–2014).145. Holtz-Eakin, “Kill the Medical Device Tax,” The Hill, January 7, 2014, http://thehill.com/blogs /congress-blog/economy-budget/194534-kill-the-medical-device-tax.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
58
often take financial losses in their early years. Hence, it requires innovators to absorb sometimes large losses in the years before they begin to earn profits. Health care scholars Michael Ramlet, Robert Book, and Han Zhong explore the ramifications of the tax.146 AdvaMed, the trade organization for makers of medical devices, also provides resources on the issue.147
The federal government should do the following:
• Repeal the drug tax.
• Repeal the medical device tax.
Federal Tax Law Discourages the Creation and Diffusion of In-novative Insurance Policies and Innovative Modes of CareHealth care policy scholar John Goodman describes two aspects of federal tax law that discourage innovative insurance policies and health care provi-sion. First, employers can deduct the cost of employee health insurance as a business expense, while an individual cannot similarly deduct the cost of self-insurance through, for example, a health savings account. Second, those who receive health insurance through employers can pay their premiums with pre-tax dollars, while those purchasing insurance on the individual market must use post-tax dollars. This disparity artificially lowers the cost of group plans and artificially raises the cost of individual plans. It may well be the single most anticompetitive factor in the health insurance market.148
These tax provisions have been described as inequitable, since their ben-efits are greatest for those in the highest tax brackets. But they have profound effects on health insurance and health care markets. One effect is to relieve most individuals of any need to do comparison shopping with respect to insur-ance policies. This, in turn, limits the value they would gain by evaluating a broad swath of health care providers. Thanks to this immobilizing effect, inno-vative insurers and innovative providers have far less motivation or capacity to pitch their innovations to consumers (i.e., patients) and, in turn, less motiva-tion to innovate in the first place.
146. Ramlet, Book, and Zhong, “The Economic Impact of the Medical Device Excise Tax” (report, American Action Forum, June 4, 2012), http://americanactionforum.org/research/the-economic -impact-of-the-medical-device-excise-tax.147. “Medical Device Tax,” AdvaMed website, accessed August 31, 2014, http://advamed.org /issues/19/medical-device-tax.148. Goodman, Priceless, 188.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
59
Mercatus scholar Jeremy Horpedahl and his coau-thor, Harrison Searles, note that the employer tax exemp-tion constitutes the single largest tax expenditure in the federal tax code, with a cost to the federal government of $300 million in fiscal year 2012. They also note that this provision encourages excessive expenditure on insurance while making the insurance market less competitive.149
In addition, these tax inequities have encouraged the propagation of health insurance policies that are actu-ally more medical service prepayment plans than they are true insurance. Insurance is normally intended to pro-tect against large and unexpected financial losses—not to pay for small and routine expenditures. John Goodman and others have noted the importance of consumers hav-ing skin in the game.150 We know from the RAND Health Insurance Experiment that consumers do spend less on health care when they experience some marginal cost.151
With these goals in mind, the federal government should make the following changes to the tax code:
• Establish parity between the tax treatment of third-party premiums and contributions to health savings accounts.
• Eliminate the tax exclusion for health insurance and replace it with a level tax credit.152
149. Horpedahl and Searles, “The Tax Exemption of Employer-Provided Health Insurance” (Mercatus on Policy, Mercatus Center at George Mason University, July 2013), http://mercatus.org/publication/tax-exemption -employer-provided-health-insurance.150. Goodman was among the earliest advocates of health savings accounts and touted their benefits in “Health Savings Accounts Will Revolutionize American Health Care” (Brief Analysis No. 464, National Center for Policy Analysis, Dallas, TX, January 15, 2004), http://www.ncpa.org/pub/ba464.151. Joseph P. Newhouse, “Consumer-Directed Health Plans and the RAND Health Insurance Experiment,” Health Affairs 23, no. 6 (2004): 107–13, http://content.healthaffairs.org/content/23/6/107.full.html.152. Goodman outlines a proposal to replace the tax exclusion with a level tax credit to bolster the individual market and portability. John C. Goodman, “Replace Obamacare, Stat,” National Review, March 24, 2014, http://www.nationalreview.com/article/372980/replace-obamacare-stat -john-c-goodman/page/0/1.
“Insurance is normally intended to protect against large and unexpected financial losses—not to pay for small and routine expenditures.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
60
American Medical Education De-emphasizes Critical Thinking and Interdisciplinary Collaboratio nWhile praising American medical education, Clayton Christensen, Jerome Grossman, and Jason Hwang note that the pedagogy used in medical schools is roughly a century old and that this has negative effects on the delivery of health care and on the cost of doing so. They argue that medical schools must respond in two ways: by improving the performance of current modes of delivery, and by allowing and absorbing disruptive innovation. In this case, disruptive inno-vation includes competition from foreign medical graduates, alternative train-ing (such as osteopathic schools), nurse practitioners, and in-house corporate medical schools.153
Christensen, Grossman, and Hwang note that current training, homog-enized since the time of the Flexner Report, is in many ways archaic. Medical education remains focused on individual knowledge rather than on the inter-disciplinary teams and networks that characterize much of modern medicine. The classroom and clinical portions of medical school are sequential, with the tour through subdisciplines close to random. The result is a highly frag-mented field.154
Christensen, Grossman, and Hwang go on to describe Toyota’s manufac-turing methods and their applicability to medical education. Among the critical differences between current medical education and Toyota’s method is that the former is “variable learning” and the latter “variable time.” In a variable learn-ing environment, students pass through a sequence of courses in lockstep. The degree of mastery in a given component varies widely across students. In a vari-able time environment, students must attain a given mastery over a component before moving to the next one, meaning different students require different amounts of time to pass through specific components.155
Potential reforms to American medical education include the following:
• Shift curricula from variable learning to variable time.
• Interweave classroom and clinical components.
• Remove obstacles (e.g., licensing) to alternative forms of medical edu-cation—such as osteopathy and for-profit, offshore medical schools—and to the acceptance of their trainees.
153. Christensen, Grossman, and Hwang, Innovator’s Prescription, chapter 10.154. Ibid.155. Ibid.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
61
Medicare’s Price Controls Skew Treatment Patterns
In the 21st century, Medicare arguably poses the single greatest fiscal threat to the US government. Health economist Victor Fuchs has said, “If we solve our health care spending, practically all our fiscal problems go away.” And if not, “then almost anything else we do will not solve our fiscal problems.”156
Medicare reimburses providers on the basis of inputs, not outputs or value. Thus the formula overpays for some services and underpays for others. In some cases, Medicare will only pay for extraordinarily expensive procedures when far less expensive substitutes are available.
Darshak Sanghavi, fellow and managing director of the Engelberg Center for Health Care Reform at the Brookings Institution, provides an excellent explanation of the problems with Medicare’s reimbursement system. What follows here draws heavily on Sanghavi’s piece.157 The core of Medicare’s reim-bursement system is the Resource-Based Relative Value Scale, a 1985 meth-odology that establishes the relative reimbursement rates for thousands of services—based on the providers’ efforts, rather than the effectiveness of pro-cedures or their usefulness to patients. The scale’s rates are adjusted over time for geographic location and for inflation.
The Medicare reimbursement rates exert a powerful influence on almost all other health insurance plans, public and private. Private plans, in other words, use an adjusted set of Medicare prices. Sanghavi further notes that the primary source of data for setting the relative values is the American Medical Association, whose recommendations Medicare rarely overrides. The result, he notes, is a steady increase of specialists’ rates vis-à-vis those of primary care doctors.
Medicare’s reimbursement rules contain countless limits on the supply of health care services. Here is a tiny sample: (1) Radiological scans are routinely read in places like India and Australia—and especially during nighttime hours in the United States. It is less expensive and more efficient to pay a doctor in Australia to read scans by day (Australian time) than it is to have a doctor in America read the scan in the middle of the night (American time). Even if the doctor in Australia is an American citizen, trained and board-certified in America and indemnified in America, Medicare will not reimburse for that
156. Victor Fuchs, interview by Gina Kolata, “Knotty Challenges in Health Care Costs,” New York Times, March 5, 2012, http://www.nytimes.com/2012/03/06/health/policy/an-interview-with -victor-fuchs-on-health-care-costs.html?_r=1&.157. Darshak Sanghavi, “The Fix Is In: The Hidden Public-Private Cartel That Sets Health Care Prices,” Slate, September 2, 2009, http://www.slate.com/articles/news_and_politics/prescriptions /2009/09/the_fix_is_in.single.html.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
62
service.158 (2) In general, Medicare will not reimburse phy-sicians for telephone or email consultations.159 This sets physicians apart from almost all other professionals and requires patient visits when calls or emails would do. (3) Medicare will not reimburse for medical tourism (medical services performed in other countries). This is true even if the physician performing the services is US-trained and US board-certified and if the physician’s hospital is certi-fied by the Joint Commission—the organization that certi-fies the quality of American hospitals and other health care organizations.
Some potential solutions to this problem follow:
• Allow Medicare and other programs to reimburse for imported medical services, such as radiologi-cal scans.
• Allow Medicare to reimburse for emails and tele-phone consultations.
• Allow Medicare to reimburse for medical tourism.
• Shift reimbursement rate-setting to a more decen-tralized, market-driven methodology. Sanghavi recommends internalizing rate-setting within the federal government rather than outsourcing much of the task to the American Medical Association. It is not clear, however, that this would change matters a great deal; the rates would still be driven through a central bottleneck. The alternative would be to decentralize the process. How one might accomplish that is a lengthy topic for another paper.
158. “Medicare Regulation FAQ—Teleradiology,” American College of Radiology website, accessed August 31, 2014, http://www.acr.org/FAQs /Medicare-Regulation-FAQs-Teleradiology.159. John C. Goodman, “How Doctors Are Trapped, Part II,” Health Policy Blog (National Center for Policy Analysis), January 23, 2012, http://health blog.ncpa.org/how-doctors-are-trapped-part-ii/.
“In general, Medicare will not reimburse physicians for telephone or email consultations.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
63
Insurance Market Mandates Skew the Mix of Health Care ExpendituresOne way for government to limit the supply of one health care service is to mandate that you (or your third-party payer) buy other things, thereby leaving less disposable income for the service in question.
Health care now occupies more than 18 percent of US GDP. The ACA mandates a list of essential health benefits, plus a lengthy list of preventive services, that all insurance policies must cover at zero marginal cost. In addi-tion, states have long maintained varying lists of mandatory health insurance benefits.
Starting in 2014, the ACA requires small-group and individual insurance plans to cover a set of essential health benefits.160 This set of mandated ben-efits homogenizes the design of the affected policies, reducing the incentive for insurers to innovate over policy design. This also likely prompts a high demand for some services, which in turn claim an excessively large share of the avail-able medical resources. The ACA also mandates that every insurance policy include a long list of preventive services. The notion of crowding out within health care has been eloquently stated by John Goodman and his colleagues, Gerald Musgrave and Devon Herrick:
Medical research has pushed the boundaries of what doctors can do for us in every direction. The Cooper Clinic in Dallas now offers an extensive checkup (with a full body scan) for about $1,500 or more. Its clients include Ross Perot, Larry King, and other high-profile individuals. Yet if everyone in America took advantage of this opportunity, we would increase our nation’s health bill by a third. More than 900 diagnostic tests can be done on blood alone, and one doesn’t need much imagination to justify, say, $5,000 worth of tests each year. But if everyone did so, we would double the nation’s health care bill. Americans purchase nonprescription drugs almost twelve billion times a year and almost all of these are acts of self-medication. Yet if everyone sought a physician’s advice before making such pur-chases, we would need twenty-five times the number of pri-mary care physicians we currently have. Some 1,100 tests can
160. Robert F. Graboyes, “Essential Health Benefits: The Secretary’s Joystick,” Health Policy Forum (Altarum Institute), May 3, 2011, http://altarum.org/health-policy-blog/essential-health-benefits -the-secretary%E2%80%99s-joystick#sthash.aQrvMzYS.dpuf.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
64
be done on our genes to determine if we have a predisposition toward one disease or another. At, say, $1,000 a test, it would cost more than $1 million for a patient to run the full gamut. But if every American did so, the total cost would run to about thirty times the nation’s total output of goods and services.
Notice that in hypothetically spending all of this money, we have not yet cured a single disease or treated an actual ill-ness. In these examples, we are simply collecting information. If in the process of the search we actually found something that warranted treatment, we could spend even more.161
A 2003 study by Duke University scholars asked what would happen if every American received the minimum level of preventive services recom-mended by the US Preventive Services Task Force. The result was that these services would consume roughly 7.5 hours per day for every primary care phy-sician in America. Note that this would leave doctors with practically no time to treat sick people.162
Like the ACA’s essential health benefits, state benefit mandates homog-enize the design of health insurance policies, leaving less room for innovation and optimization. Until 2012, the Council for Affordable Health Insurance issued a survey of state benefit mandates each year. In 2012, the council found that there were 2,271 state mandates in total—an average of 45 mandates per state, ranging from 13 in Utah to 69 in Rhode Island.163 These mandates might increase total health care expenditures, or they might skew expenditures from nonmandated services to mandated ones—and perhaps to services with lower marginal value to patients.
Potential solutions to this problem include the following:
• Eliminate the ACA’s essential health benefits.
• Eliminate the ACA’s list of mandatory preventive services.
• Eliminate state benefit mandates.
161. Goodman, Musgrave, and Herrick, Lives at Risk: Single-Payer National Health Insurance around the World (Lanham, MD: Rowman & Littlefield, 2004), 2.162. Kimberly S. H. Yarnall et al., “Primary Care: Is There Enough Time for Prevention?,” American Journal of Public Health 93, no. 4 (April 2003): 635–41, http://ajph.aphapublications.org/doi /abs/10.2105/AJPH.93.4.635.163. “CAHI Identifies 2,271 State Health Insurance Mandates,” Council for Affordable Health Insurance, April 9, 2013, http://www.cahi.org/cahi_contents/newsroom/article.asp?id=1115.

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
65
Unbreachable Walls Separate Americans across Many Insurance Markets, Minimizing the Usefulness of Competition between PlansThe American health insurance system is highly frag-mented, which is not itself a problem. There are, after all, thousands of companies selling auto insurance, homeown-ers insurance, life insurance, and so on. But the problem with health insurance fragmentation is that US laws lock Americans into their own market fragments.
Government insurance programs include Medicare for the elderly, Medicaid for lower-income people, the Children’s Health Insurance Program for lower-income children, the Indian Health Service for American Indians, Veterans Affairs for veterans, TRICARE for active and retired members of the military (and their families), Federal Employees Health Benefits for federal employees, a variety of programs for employees of individual states, and high-risk pools for individuals with preexisting con-ditions. In the private sector, there are large-group, small-group, and individual fully insured plans, and there are self-insured plans as well. The small-group and individual markets are generally separate in each state. And there are additional lines of fragmentation within these categories.
While there is some minimal overlap between cat-egories, it is often impossible or impractical for people to move between these fragments. Hence, health insurance is one of the few consumer products where there is virtually no point in leaning over your fence and asking a neighbor for advice.
Reforms that could potentially reduce this fragmen-tation include the following:
• Allow health insurers to sell health insurance across state lines. Currently, an insurer in one state cannot sell health insurance to purchasers in other states.164
164. This idea likely requires further research. While cross-border insur-ance sales are a tenet of right-of-center policy proposals, others cred-ibly argue that in practice, such arrangements would have either trivial
“Health insurance is one of the few consumer products where there is virtually no point in leaning over your fence and asking a neighbor for advice.”

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
66
• Allow groups such as trade associations to form their own risk pools. Legislation should allow association health plans and small business health plans.
• Allow Medicaid recipients to cash out and buy private coverage.165
or negative effects. For example, health care consultant and analyst Robert Laszewski argues that interstate purchases would increase market instability, that the idea would not dovetail with current market conditions, and that it is an expensive and convoluted way to deal with the problem of exces-sive benefit mandates. He notes that Georgia created an interstate purchase option in 2011, but no out-of-state carriers took up the offer. Laszewski challenges, “I suggest the supporters of this idea first ask the leaders of the insurance industry if they would even do this under the best of circum-stances.” Robert Laszewski, “Silly Republican Insurance Reform Ideas,” Health Care Blog, March 17, 2014, http://thehealthcareblog.com/blog/2014/03/17/silly-republican-reform-ideas/.165. See Avik Roy, How Medicaid Fails the Poor, Encounter Broadside No. 36 (New York: Encounter Books, 2013); Robert F. Graboyes, “Medicaid and Health,” in The Economics of Medicaid: Assessing the Costs and Consequences, ed. Jason Fichtner (Arlington, VA: Mercatus Center at George Mason University, 2014).

MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
67
CONCLUSION
This paper has argued that the post–World War II health care debate has largely focused on the most equitable way to distribute the health care resources currently available. “Do we determine the allocation
of funds and resources at the state level or the federal level?” “To what extent should consumers control the selection of health-related goods and services?” “If we train a certain number of physicians in 2014, how many of them should go into oncology and how many into primary care?” “How should we divvy up the resources among old people, poor people, middle-class people, children, inner-city communities, rural communities, and so forth?”
While the policy debate stagnates, medical science has progressed and advances in information technology have opened the door to novel ways of delivering health care services. I argue here that refocusing the debate onto how best to encourage innovation, both in medical technology and in the orga-nization of the entire health care industry, is the best route out of our debilitat-ing policy deadlock.
The relevant question is, “How soon will the health care industry experi-ence the dramatic transformations already seen in the modern IT industry?” In a Frontier world, many of the innovations described above could become com-monplace within the next five or ten years. In fact, some are already on their way to becoming so. In a Fortress world, however, they may take a generation or more. Or innovators, frustrated by a Fortress America, might develop their innovations in Frontier India, Singapore, Thailand, or Costa Rica.166 America could cease to be the world’s premier innovator.
The specific reform suggestions described in this paper are only a few of the ways health care legislation, regulation, and education could be molded into innovation-friendly policy. In each case, successful reform will hinge on allowing American consumers to buy what they want, and allowing producers to sell it to them. It will require unleashing the same creative forces that have brought us revolutionary advances in the fields of computing, telecommunica-tions, and transportation.
In truth, most Americans don’t care how the institutions from which they seek health care are organized, or whether Republicans or Democrats have writ-ten the rules of the game—they simply want better health care at lower cost.
That is the ultimate measure of success.
166. All these countries currently boast state-of-the-art hospitals catering to Americans and other for-eign patients.


MERCATUS CENTER AT GEORGE MASON UNIVERSIT Y
69
ABOUT THE AUTHOR
Robert F. Graboyes is a senior research fellow for the Mercatus Center at George Mason University. He specializes in the economics of health care and teaches in master’s and doctoral programs at Virginia Commonwealth University and the University of Virginia. He has also taught at George Mason University, the George Washington University, and the University of Richmond. Previously, he was a sub-Saharan Africa economist at Chase Manhattan Bank and, in that capacity, traveled extensively in Africa and Europe. He has also served as a regional economist at the Federal Reserve Bank of Richmond and twice visited the Republic of Kazakhstan as a health care scholar. Graboyes earned his PhD in economics from Columbia University.
ACKNOWLEDGMENTS
Many thanks go to Lydia Mashburn, Emily Washington, and Ted Bolema for shepherding this paper from its origins to the finished product. Angela Kuck’s guidance throughout the year has been essential to finding the right words to apply to my ideas. Anna Mills and Dana Williams have provided great support for my research in many ways. Thanks to Michael Mandel and two anonymous reviewers for helpful comments on earlier drafts. Corrie Schwab’s superb edits and Garrett Brown’s tireless guidance were essential to bringing this project to a close. Finally, so many people at Mercatus have contributed to this paper in one way or another that I can’t even begin to name them individually. Thanks to all of them, and to others who have helped along the way. And my greatest thanks go to my wife, Alanna, for her endless support; she read far more drafts of this paper than any human should ever read of anything.

ABOUT THE MERCATUS CENTER AT GEORGE MASON UNIVERSITY
The Mercatus Center at George Mason University is the world’s premier university source for market-oriented ideas—bridging the gap between aca-demic ideas and real-world problems.
A university-based research center, Mercatus advances knowledge about how markets work to improve people’s lives by training graduate students, con-ducting research, and applying economics to offer solutions to society’s most pressing problems.
Our mission is to generate knowledge and understanding of the institu-tions that affect the freedom to prosper and to find sustainable solutions that overcome the barriers preventing individuals from living free, prosperous, and peaceful lives.
Founded in 1980, the Mercatus Center is located on George Mason University’s Arlington campus.





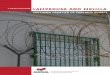





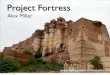
















![Introduction - Augsburg Fortress · Introduction - Augsburg Fortress ... ,d] ] ]](https://img.pdfslide.net/doc/110x75/5d6044f688c993a17a8bdfc8/introduction-augsburg-introduction-augsburg-fortress-d-.jpg)