Embed Size (px)
Citation preview

Foundation for American Healthcare Leadership
Summit
John E. Wennberg, MD, MPHJohn E. Wennberg, MD, MPH
Chicago, ILChicago, IL
June 17-18, 2004June 17-18, 2004

Developing New Financing and Care Delivery Developing New Financing and Care Delivery Models: How Should Your Sector Respond?Models: How Should Your Sector Respond?
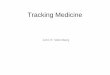
• Practice Variations can now be understood & Practice Variations can now be understood & interpreted normatively for all 3 categories of interpreted normatively for all 3 categories of care.care.

Ben
efit
to
Pat
ien
tsB
enef
it t
o P
atie
nts
% Use of Effective Care% Use of Effective Care
U.S. issome-wherein thiszone
Underuse of Effective CareUnderuse of Effective Care

Ben
efit
to
Pat
ien
tsB
enef
it t
o P
atie
nts
UNKNOWN
Units of Discretionary CareUnits of Discretionary Care
Misuse of Preference-Sensitive Care Misuse of Preference-Sensitive Care (e.g. discretionary surgery)(e.g. discretionary surgery)

U.S. issome-wherein thiszone
Frequency of CareFrequency of Care
Lif
e E
xpec
tan
cy
Lif
e E
xpec
tan
cy
Overuse of Supply-Sensitive ServicesOveruse of Supply-Sensitive Services

Developing New Financing and Care Delivery Developing New Financing and Care Delivery Models: How Should Your Sector Respond?Models: How Should Your Sector Respond?
• Variations can now be understood & interpreted Variations can now be understood & interpreted normatively for all 3 categories of care.normatively for all 3 categories of care.
• Remedies are available but have yet to be widely Remedies are available but have yet to be widely implemented.implemented.


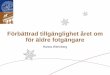
Knowledge of relevant treatment
options and outcomes
Concordance between patient values
and care receivedToronto trial
7.28
0.852.01
10.78
1.182.52
16.75
2.17
4.55
0
5
10
15
20
1 or 2 vesseldisease, w/o PLAD
disease
2 vessel + PLAD or3 vessel
left main disease
20-64 yrs65-74 yrs>=75 yrs
Impact of improved decision quality on surgery Impact of improved decision quality on surgery rates: CHDrates: CHD

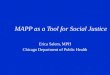
S P O R TS P O R TSpine Patient Outcomes Spine Patient Outcomes
Research Trial(s) Research Trial(s) model of new of potential partnershipsmodel of new of potential partnerships
Funded by: The National Institute of Arthritis and Musculoskeletal and Skin Diseases and the Office of Research on Women's Health, the National Institutes of Health,
and the National Institute of Occupational Safety and Health, the Centers for Disease Control and Prevention

San F ran cisco
Om ah a
St. L o u is
C h icag o
D etro it
C levelan d
A tlan ta
Ph i lad elp h ia N ew Yo rk (2)
H an o ver
S P O R T S ites
Copyright 1999, Trustees of Dartmouth College
**
****

Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
Functional and Clinical Outcomes
DeliverySystemDesign
DecisionSupport
ClinicalInformation
Systems
Self-Management
Support
Health System
Resources and Policies
Community
Health Care Organization
Chronic Care Model (Wagner)
Acknowledgements: Improving Chronic Illness Care, a national program of The Robert Wood Johnson Foundation

Developing New Financing and Care Delivery Developing New Financing and Care Delivery Models: How Should Your Sector Respond?Models: How Should Your Sector Respond?
• Variations can now be understood & interpreted Variations can now be understood & interpreted normatively for all 3 categories of care.normatively for all 3 categories of care.
• Remedies are available but have yet to be widely Remedies are available but have yet to be widely implemented.implemented.
• Reform requires population-based Reform requires population-based provider-provider-specificspecific performance monitoring for various performance monitoring for various sectors of care.sectors of care.

Supply-Sensitive Care can be measured for specific providersSupply-Sensitive Care can be measured for specific providers
Days in Hospitals During Last Six Months of LifeDays in Hospitals During Last Six Months of Life
8.08.0
12.012.0
16.016.0
20.020.0
24.024.0
28.028.0NYU Medical Center 27.1
Mount Sinai Hospital 22.8NY Presbyterian Hospital 21.6Cedars-Sinai Medical Center 21.3
Mass. General Hospital 16.5UCLA Medical Center 16.1Boston Medical Center 15.6
Brigham & Women's Hospital 13.9Beth Israel Deaconess 12.2UCSF Medical Center 11.5Stanford University Hospital 10.1

Supply-Sensitive Care can be measured for specific providersSupply-Sensitive Care can be measured for specific providers
Physician Visits During the Last Six Months of LifePhysician Visits During the Last Six Months of Life
10.010.0
20.020.0
30.030.0
40.040.0
50.050.0
60.060.0
70.070.0
80.080.0NYU Medical Center 76.2
UCLA Medical Center 43.9NY Presbyterian Hospital 40.3Mass. General Hospital 38.8
Cedars-Sinai Medical Center 66.2
Mount Sinai Hospital 53.9
Brigham & Women's Hospital 31.9Boston Medical Center 31.5Beth Israel Deaconess 29.2UCSF Medical Center 27.2Stanford University Hospital 22.6

0.00.0
10.010.0
20.020.0
30.030.0
40.040.0
50.050.0
60.060.0
70.070.0
80.080.0
Preference-sensitive care for specific providersPreference-sensitive care for specific providers
Invasive Cardiac Procedures (1998-2001)Invasive Cardiac Procedures (1998-2001)
Non-BlackMales
BlackMales
Non-BlackFemales
BlackFemales

Resource Inputs can be measured for specific providersResource Inputs can be measured for specific providers
Physician Labor Inputs in Managing Cohorts of Physician Labor Inputs in Managing Cohorts of Chronically Ill Patients During Last Six Months of LifeChronically Ill Patients During Last Six Months of Life
FTE Physicians per 1,000FTE Physicians per 1,000
Hosp AHosp A
Hosp BHosp B
Hosp CHosp C
Hosp DHosp D
PrimaryPrimary CareCare
MedicalMedicalSpec.Spec.
1919 7676
3131 132132
2626 2020
3030 2727

Resource Inputs can be measured for specific providersResource Inputs can be measured for specific providers
Physician Labor Inputs in Managing Cohorts of Physician Labor Inputs in Managing Cohorts of Chronically Ill Patients During Last Six Months of LifeChronically Ill Patients During Last Six Months of Life
FTE Physicians per 1,000FTE Physicians per 1,000
Hosp AHosp A
Hosp BHosp B
Hosp CHosp C
Hosp DHosp D
PrimaryPrimary CareCare
MedicalMedicalSpec.Spec.
Med Spec./lMed Spec./lPrimary MDPrimary MD
1919 7676 4.14.1
3131 132132 4.34.3
2626 2020 0.80.8
3030 2727 0.90.9
//

Estimating Actuarial Costs of Managing Estimating Actuarial Costs of Managing Patient Cohorts with Chronic IllnessPatient Cohorts with Chronic Illness

Actuarial Costs estimated for specific providersActuarial Costs estimated for specific providers
Medicare Spending During the Last Six Months of Medicare Spending During the Last Six Months of Life For Hospitals and PhysiciansLife For Hospitals and Physicians
10,00010,000
15,00015,000
20,00020,000
25,00025,000
30,00030,000
35,00035,000
40,00040,000

Association Between Medicare Payments 18-24 Association Between Medicare Payments 18-24 Months and 0-6 Months Before DeathMonths and 0-6 Months Before Death
R2 = 0.795,0005,000
10,00010,000
15,00015,000
20,00020,000
25,00025,000
30,00030,000
35,00035,000
40,00040,000
1,5001,500 3,5003,500 5,5005,500 7,5007,500
Total Payments 18-24 Mos. Before DeathTotal Payments 18-24 Mos. Before Death
To
tal P
aym
ent
in L
ast
6 M
on
ths
To
tal P
aym
ent
in L
ast
6 M
on
ths

Developing New Financing and Care Delivery Developing New Financing and Care Delivery Models: How Should Your Sector Respond?Models: How Should Your Sector Respond?
• Variations can now be understood & interpreted Variations can now be understood & interpreted normatively for all 3 categories of care.normatively for all 3 categories of care.
• Remedies are available but have yet to be widely Remedies are available but have yet to be widely implemented.implemented.
• Reform requires population-based Reform requires population-based provider-provider-specificspecific performance monitoring. performance monitoring.
• Reform requires partnerships between providers Reform requires partnerships between providers and payers to redesign care process and allow and payers to redesign care process and allow high quality providers to prosperhigh quality providers to prosper

What “High Quality” Providers need to do:What “High Quality” Providers need to do:
• Eliminate Underservice of Effective CareEliminate Underservice of Effective Care• Reduce Medical Mistakes Reduce Medical Mistakes • Learn What Works (Outcomes Research)Learn What Works (Outcomes Research)• Assure Informed Patient Choice (Shared Decision Assure Informed Patient Choice (Shared Decision
Making)Making)• Promote Conservative Practice Patterns (When Promote Conservative Practice Patterns (When
More Isn’t Better) More Isn’t Better) • Achieve Efficient Allocation of ResourcesAchieve Efficient Allocation of Resources

What payers need to do:What payers need to do:
• Demand Excellence in all 3 categoriesDemand Excellence in all 3 categories• Partner with Centers of Excellence who agree to reduce Partner with Centers of Excellence who agree to reduce
unwarranted variation in all 3 categoriesunwarranted variation in all 3 categories• Work with Centers of Excellence to design new payment Work with Centers of Excellence to design new payment
methods to promote and reward quality and efficiencymethods to promote and reward quality and efficiency• Support outcomes research as part of everyday practiceSupport outcomes research as part of everyday practice• Create incentives for the wide redesign of U.S. health care Create incentives for the wide redesign of U.S. health care

Dartmouthatlas.orgDartmouthatlas.org
Thank You!!!!!Thank You!!!!!