Embed Size (px)
Citation preview

Si
Svagi
dN
MS.
r
Current Concepts
Four-Quadrant Approach to Capsulolabral Repair: AnArthroscopic Road Map to the Glenoid
Shane T. Seroyer, M.D., Shane J. Nho, M.D., M.S.,CDR Matthew T. Provencher, M.D., MC, USN, and Anthony A. Romeo, M.D.
Abstract: Advancing technology, improved instrumentation, and a desire to address intra-articularpathology with a minimally invasive approach have driven the expansion of arthroscopic shouldersurgery in the past 2 decades. Proponents cite greatly improved visualization, lack of the need toperform a capsulotomy, fewer subscapularis issues postoperatively, and improved access to the entireglenohumeral joint. Our understanding and recognition of glenohumeral joint pathology haveimproved, and our ability to appropriately treat it has also improved. Aside from the anteroinferiorand superior capsulolabral injury, orthopaedic surgeons have encountered and are able to addresscombined lesions, posterior labral tears, 270° to 360° labral tears, capsular laxity, humeral avulsionof the glenohumeral ligaments, associated glenoid or humeral bone loss, and partial-thickness rotatorcuff tears. To adequately address the extent of pathology encountered in a shoulder instability case,access to the inferior, posteroinferior, and posterior aspects is necessary. In this technical article wepresent a simplified approach using safe access points by dividing the glenohumeral joint into 4quadrants that allows for ease of instrumentation and implant placement. This will provide a blueprintfor the treatment of capsulolabral injuries. In addition to portal selection and location, we will discussseveral instruments we believe are advantageous in tissue manipulation and suture management.
stjhpogajAasaflpmle
houlder arthroscopy can be performed with thepatient in either the beach-chair or lateral decub-
tus position. The major advantage of the lateral po-
From the Section of Shoulder and Elbow Surgery, Division ofports Medicine, Department of Orthopedic Surgery, Rush Uni-ersity Medical Center (S.T.S., S.J.N., A.A.R.), Chicago, Illinois;nd Department of Orthopaedic Surgery, Division of Sports Sur-ery, Naval Medical Center San Diego (M.T.P.), San Diego, Cal-fornia, U.S.A.
The views expressed in this article are those of the authors ando not reflect the official policy or position of the Department of theavy, Department of Defense, or the United States Government.The authors report no conflict of interest.Address correspondence and reprint requests to Shane J. Nho,.D., M.S., Rush University Medical Center, 1725 W Harrison St,
te 1063, Chicago, IL 60612, U.S.A. E-mail: sjaynho@rushorthocom
© 2010 by the Arthroscopy Association of North America. Allights reserved.
0749-8063/10/2604-9506$36.00/0doi:10.1016/j.arthro.2009.09.019
Arthroscopy: The Journal of Arthroscopic and Related S
ition is that through balanced suspension, access tohe inferior and posterior aspects of the glenohumeraloint is optimized. Thus we prefer to perform gleno-umeral arthroscopy with the patient in the lateralosition. The patient is placed on a beanbag, with hisr her torso rolled 30° posteriorly to position thelenoid parallel with the floor. All bony prominencesre padded. An axillary roll is placed under the torsoust distal to the axilla to protect the brachial plexus.fter standard, sterile preparation and draping, the
rm is placed in a commercially available foamleeve, and dual balanced suspension is provided. Therm is placed in 45° of abduction and 15° of forwardexion. Ten pounds of distal suspension and tenounds of lateral suspension are routinely used. A skinarker is used to denote pertinent bony anatomic
andmarks and proposed portals, and preoperative an-sthetic is injected.
With the patient in the lateral decubitus position,
555urgery, Vol 26, No 4 (April), 2010: pp 555-562

woatptgputwc
P
nwas“
ttiaItitwocTttiebmutppttustj
df
A
wasiTotsattptrpumop
A
diaopbpTitlwloaacsdpptd
556 S. T. SEROYER ET AL.
hen the surgeon is working on the superior portionsf the glenoid (from 10- to 2-o’clock position), it isdvantageous to be positioned below the shoulder sohat the instruments do not need to be used in aronated position (“backhanded fashion”). Alterna-ively, work done inferiorly to this position on thelenoid is more easily performed when the surgeon isositioned above the shoulder. This will simplify these of curved suture-passing devices that require ro-ation for use. For the sake of simplicity in this article,hen describing position on the glenoid relative to the
lock face, we will be referring to a right shoulder.
PORTAL PLACEMENT
osterior Portal
Clinical examination and ancillary studies (mag-etic resonance imaging) should provide the surgeonith a preoperative plan that will guide him or her to
ccomplish the intraoperative goals. We begin arthro-copic shoulder surgery by establishing a posteriorviewing” portal and an anterior “working” portal.
The posterior portal is established blindly, by use ofhe posterolateral corner of the acromion as the ana-omic landmark.1 In a practice with a high volume ofnstability, this utilitarian portal needs to be located inposition to facilitate access to the posterior glenoid.
f one is using lateral decubitus patient positioning,he often described posterior portal placement of 2 cmnferior and 1 cm medial to the posterolateral corner ofhe glenoid may leave the surgeon too medial. Thisill make access to the posterior glenoid at the properblique angle for anchor insertion difficult, makingapsulolabral surgery technically more challenging.hus we establish this portal slightly more lateral than
ypically described; it is established nearly in line withhe lateral edge of the acromion, about 1.5 to 2 cmnferior to the most posterolateral tip. In patients withxcessive soft tissue, the “Romeo 3-finger shuck” cane used to assist in localizing the joint line and opti-izing portal placement.2 To do this, the surgeon,
sing the hand that corresponds to the operative ex-remity (e.g., for a left operative shoulder, the surgeonerforms the maneuver with his or her left hand),laces the middle finger over the coracoid process andhe index finger in the notch located directly posterioro the acromioclavicular joint and anterior to the scap-lar spine. The thumb can then be used to feel for theoft spot in the interval between the infraspinatus andhe teres minor. The hand is then used to “shuck” the
oint in an anterior-to-posterior direction, allowing oetermination of the joint line through tactile feedbackrom the thumb.
nterior Portal
The anterior portal3,4 is established next. This portalill serve as the initial working portal. This and all
dditional portals will be established by use of out-ide-in needle localization, to provide the optimalntra-articular position for approach to areas of injury.his portal will be slightly adjusted based on theperative plan. Initial diagnostic arthroscopic evalua-ion will confirm the anticipated surgical endeavor. Ifuperior labral pathology (SLAP lesion) is present, thenterior portal will be shifted to the superior aspect ofhe rotator interval to facilitate instrument manipula-ion over the biceps tendon for suture passage androvide access to the capsulolabral tissue posterior tohe biceps anchor (11 o’clock). Alternatively, if ante-ior or anteroinferior pathology is present, the anteriorortal is shifted slightly inferior, just above the rolledpper border of the subscapularis. This will allow aore direct approach to the 2- and 3-o’clock positions
f the glenoid and capsulolabral complex for anchorlacement and suture passage.
ccessory Portals
The decision regarding further portal placement isictated by the location of the pathology encounteredntraoperatively. The surgeon should be able to freelydjust the preoperative surgical plan based on intra-perative findings. The addition of quadrant-specificortals allows this adaptability. Portal placement muste contemplated and executed with a global surgicallan in mind and must satisfy several considerations.hey should be strategically placed to avoid crowding
nside the joint, facilitate access to all 4 quadrants ofhe glenoid surface, minimize trauma to the encapsu-ating soft-tissue structures, and allow for ease oforking outside the joint. They must also be estab-
ished with consideration of the following: the extentf visualization, the angle of approach to allow fornchor fixation into the glenoid, the proper workingngle to execute suture passage for labral fixation andapsular shifts, and cannula positioning to facilitateuture management and knot tying. Although generalescriptions can be made of the standard locations ofortals based on external landmarks, it must be em-hasized that these locations are only estimates. Pa-ient size, anatomy, and specific pathology constantlyictate minor variations in the cutaneous locations of
ur portals. In addition to securing the proper location
oaptft
mitmwmi
esnstic5scsdutatWalpcti
4aC1ttaoOii
F
ipfttTdlclntkasp3s
S
t7taacitmtnrvrtlo
P
iltot
557FOUR-QUADRANT CAPSULOLABRAL REPAIR
f entry into the joint, spinal needle localization alsoffords the surgeon the capability of evaluating theotential trajectory to areas of the glenoid and capsulehat need to be addressed. The surgeon must be mind-ul of the musculotendinous and neurovascular struc-ures at risk with portal placement.
It is advantageous to be familiar with the instru-ents of choice because many instruments have var-
ous inherent curvatures, which will inhibit their usehrough certain smaller-diameter cannulas. Further-ore, if a surgeon prefers to prepare the glenoid boneith a bur or a particular instrument, cannula place-ent should anticipate the necessary diameter for
nstrument passage.It is preferable to use cannulas in portals that are
stablished in intramuscular planes, minimizingoft-tissue damage. When intramuscular planes areot possible, the portal can be established and in-truments can be passed percutaneously, withouthe use of a cannula, to protect the soft tissues. Fornstance, the 5-o’clock trans-subscapularis portal5
an be used to place anchors from the 3-o’clock to:30 position on the glenoid, as well as for suturehuttling, but can be performed without the use of aannula, preventing iatrogenic damage of the sub-capularis tendon. The drill guide or suture-passingevices can be inserted into the portal, and thennder direct visualization, they can be used to punc-ure through the tendon and joint capsule at theppropriate position, with very minimal damage tohe tendon. We routinely make use of the Port of
ilmington portal6 for posterosuperior injuries andn anterosuperolateral portal for superior capsulo-abral work.7 The 7-o’clock portal8,9 is used forosteroinferior injuries as well as access to theapsule in the 5- to 6-o’clock area for suture shut-ling in anteroinferior injuries. The 5-o’clock portals used for anteroinferior work.
Conceptualizing the glenoid and labrum as a-quadrant grid is a fluid and simplistic way topproach any injury to the capsulolabral complex.omplex capsulolabral injuries involving more thanquadrant simply require the surgeon to use the
actical approach to each quadrant to easily managehe pathology. Mastery of specific portals to allowccess to each quadrant is an essential componentf the shoulder arthroscopist’s armamentarium.nce unrestricted access to the affected zone of
njury is achieved, repair becomes a simple exercise
n arthroscopic surgery. cive-O’clock Portal
The 5-o’clock portal is located approximately 2 cmnferior and slightly lateral to the standard anteriorortal. It provides access to the anterior and anteroin-erior glenoid and labrum. Needle localization allowshe portal to be placed in the most appropriate positiono provide linear access to the anteroinferior glenoid.he joint is entered at the junction of the middle andistal one third of the subscapularis tendon. This isocated proximal and medial to the anterior humeralircumflex vessels. The portal is lateral to the muscu-ocutaneous nerve and superolateral to the axillaryerve. The cephalic vein is a mean of 9.8 mm lateralo this portal.6 Because we do not use this portal fornot tying and because of its intratendinous location,cannula is not required. Drill guides for anchors and
uture-passing instruments are placed through thisortal in percutaneous fashion, which requires only a- to 4-mm percutaneous incision and stab through theubscapularis tendon.
even-O’clock Portal
One of the most useful portals for access to impor-ant areas of pathology in the glenohumeral joint is the-o’clock, or posterolateral, portal. The 7-o’clock por-al is established to access the posteroinferior glenoid,s well as for suture passing in the posterior quadrantnd anteroinferior capsule to perform an anteroinferiorapsular shift. This portal is typically located 3 cmnferior and 1 cm lateral to the posterolateral corner ofhe acromion. It enters the joint through the teresinor tendon at a relative safe distance of 39 mm from
he axillary nerve and 29 mm from the suprascapularerve.8,10 This is the only intratendinous portal that weoutinely cannulate. Its strategic location makes itery appealing for knot tying and suture management,endering cannula placement advantageous. Similar tohe 5-o’clock trans-subscapularis portal, the postero-ateral (7-o’clock) portal may also be used percutane-usly to place suture anchors.
ort of Wilmington
The Port of Wilmington portal11 is located approx-mately 1 cm lateral and 1 cm anterior to the postero-ateral corner of the acromion. It is ideal for access tohe posterosuperior region of the glenoid (10 to 11’clock). Because this portal is within the infraspina-us tendon and is used only for anchor placement, a
annula is not used.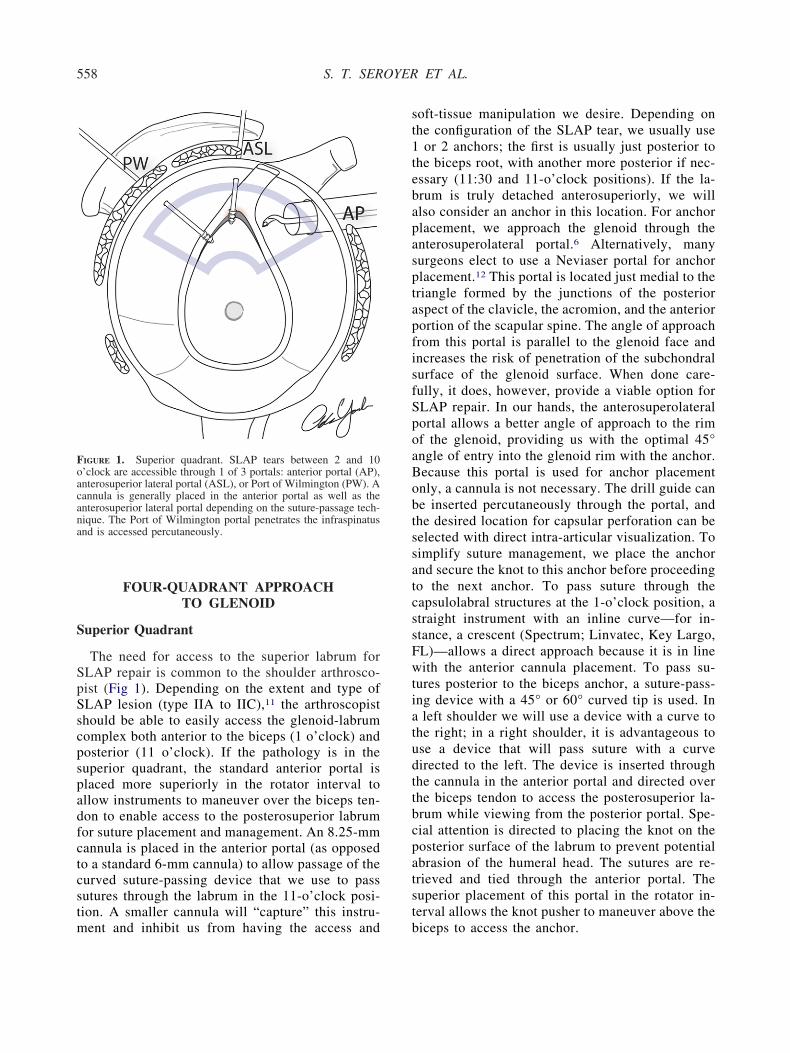
S
SpSscpspadfctcstm
st1tebapasptapfisfSpoaBobtssatcssFwtiatudttbcpatst
Foacana
558 S. T. SEROYER ET AL.
FOUR-QUADRANT APPROACHTO GLENOID
uperior Quadrant
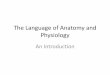
The need for access to the superior labrum forLAP repair is common to the shoulder arthrosco-ist (Fig 1). Depending on the extent and type ofLAP lesion (type IIA to IIC),11 the arthroscopisthould be able to easily access the glenoid-labrumomplex both anterior to the biceps (1 o’clock) andosterior (11 o’clock). If the pathology is in theuperior quadrant, the standard anterior portal islaced more superiorly in the rotator interval tollow instruments to maneuver over the biceps ten-on to enable access to the posterosuperior labrumor suture placement and management. An 8.25-mmannula is placed in the anterior portal (as opposedo a standard 6-mm cannula) to allow passage of theurved suture-passing device that we use to passutures through the labrum in the 11-o’clock posi-ion. A smaller cannula will “capture” this instru-
IGURE 1. Superior quadrant. SLAP tears between 2 and 10’clock are accessible through 1 of 3 portals: anterior portal (AP),nterosuperior lateral portal (ASL), or Port of Wilmington (PW). Aannula is generally placed in the anterior portal as well as thenterosuperior lateral portal depending on the suture-passage tech-ique. The Port of Wilmington portal penetrates the infraspinatusnd is accessed percutaneously.
ent and inhibit us from having the access and b
oft-tissue manipulation we desire. Depending onhe configuration of the SLAP tear, we usually use
or 2 anchors; the first is usually just posterior tohe biceps root, with another more posterior if nec-ssary (11:30 and 11-o’clock positions). If the la-rum is truly detached anterosuperiorly, we willlso consider an anchor in this location. For anchorlacement, we approach the glenoid through thenterosuperolateral portal.6 Alternatively, manyurgeons elect to use a Neviaser portal for anchorlacement.12 This portal is located just medial to theriangle formed by the junctions of the posteriorspect of the clavicle, the acromion, and the anteriorortion of the scapular spine. The angle of approachrom this portal is parallel to the glenoid face andncreases the risk of penetration of the subchondralurface of the glenoid surface. When done care-ully, it does, however, provide a viable option forLAP repair. In our hands, the anterosuperolateralortal allows a better angle of approach to the rimf the glenoid, providing us with the optimal 45°ngle of entry into the glenoid rim with the anchor.ecause this portal is used for anchor placementnly, a cannula is not necessary. The drill guide cane inserted percutaneously through the portal, andhe desired location for capsular perforation can beelected with direct intra-articular visualization. Toimplify suture management, we place the anchornd secure the knot to this anchor before proceedingo the next anchor. To pass suture through theapsulolabral structures at the 1-o’clock position, atraight instrument with an inline curve—for in-tance, a crescent (Spectrum; Linvatec, Key Largo,L)—allows a direct approach because it is in lineith the anterior cannula placement. To pass su-
ures posterior to the biceps anchor, a suture-pass-ng device with a 45° or 60° curved tip is used. Inleft shoulder we will use a device with a curve to
he right; in a right shoulder, it is advantageous tose a device that will pass suture with a curveirected to the left. The device is inserted throughhe cannula in the anterior portal and directed overhe biceps tendon to access the posterosuperior la-rum while viewing from the posterior portal. Spe-ial attention is directed to placing the knot on theosterior surface of the labrum to prevent potentialbrasion of the humeral head. The sutures are re-rieved and tied through the anterior portal. Theuperior placement of this portal in the rotator in-erval allows the knot pusher to maneuver above the
iceps to access the anchor.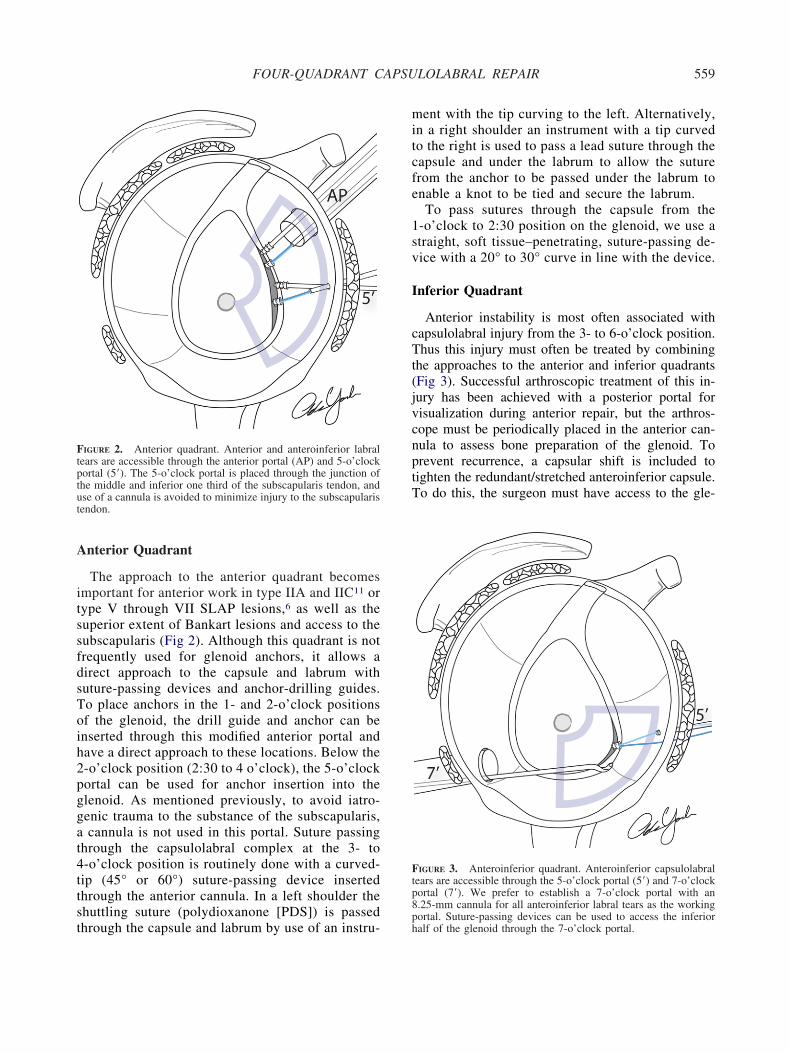
A
itssfdsToih2pggat4ttst
mitcfe
1sv
I
cTt(jvcnptT
Ftptut
Ftp8
559FOUR-QUADRANT CAPSULOLABRAL REPAIR
nterior Quadrant
The approach to the anterior quadrant becomesmportant for anterior work in type IIA and IIC11 orype V through VII SLAP lesions,6 as well as theuperior extent of Bankart lesions and access to theubscapularis (Fig 2). Although this quadrant is notrequently used for glenoid anchors, it allows airect approach to the capsule and labrum withuture-passing devices and anchor-drilling guides.o place anchors in the 1- and 2-o’clock positionsf the glenoid, the drill guide and anchor can benserted through this modified anterior portal andave a direct approach to these locations. Below the-o’clock position (2:30 to 4 o’clock), the 5-o’clockortal can be used for anchor insertion into thelenoid. As mentioned previously, to avoid iatro-enic trauma to the substance of the subscapularis,cannula is not used in this portal. Suture passing
hrough the capsulolabral complex at the 3- to-o’clock position is routinely done with a curved-ip (45° or 60°) suture-passing device insertedhrough the anterior cannula. In a left shoulder thehuttling suture (polydioxanone [PDS]) is passed
IGURE 2. Anterior quadrant. Anterior and anteroinferior labralears are accessible through the anterior portal (AP) and 5-o’clockortal (5=). The 5-o’clock portal is placed through the junction ofhe middle and inferior one third of the subscapularis tendon, andse of a cannula is avoided to minimize injury to the subscapularisendon.
hrough the capsule and labrum by use of an instru-ph
ent with the tip curving to the left. Alternatively,n a right shoulder an instrument with a tip curvedo the right is used to pass a lead suture through theapsule and under the labrum to allow the suturerom the anchor to be passed under the labrum tonable a knot to be tied and secure the labrum.To pass sutures through the capsule from the
-o’clock to 2:30 position on the glenoid, we use atraight, soft tissue–penetrating, suture-passing de-ice with a 20° to 30° curve in line with the device.
nferior Quadrant
Anterior instability is most often associated withapsulolabral injury from the 3- to 6-o’clock position.hus this injury must often be treated by combining
he approaches to the anterior and inferior quadrantsFig 3). Successful arthroscopic treatment of this in-ury has been achieved with a posterior portal forisualization during anterior repair, but the arthros-ope must be periodically placed in the anterior can-ula to assess bone preparation of the glenoid. Torevent recurrence, a capsular shift is included toighten the redundant/stretched anteroinferior capsule.o do this, the surgeon must have access to the gle-
IGURE 3. Anteroinferior quadrant. Anteroinferior capsulolabralears are accessible through the 5-o’clock portal (5=) and 7-o’clockortal (7=). We prefer to establish a 7-o’clock portal with an.25-mm cannula for all anteroinferior labral tears as the working
ortal. Suture-passing devices can be used to access the inferioralf of the glenoid through the 7-o’clock portal.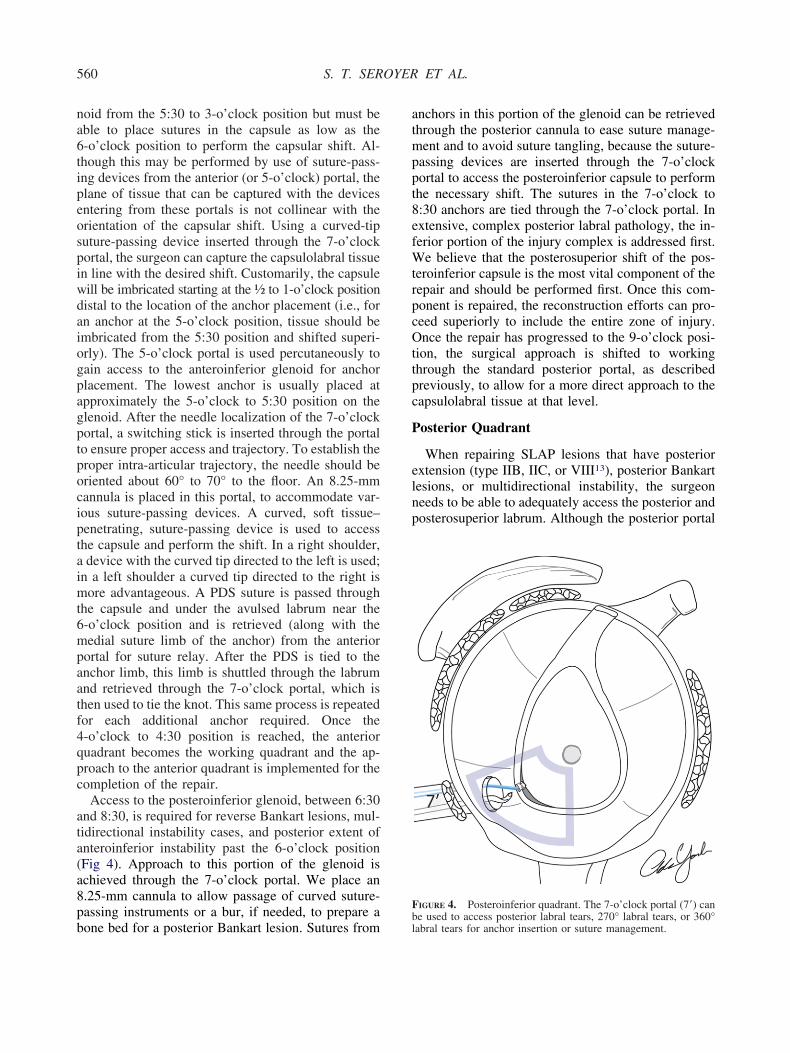
na6tipeospiwdaiogpagptpociptaimt6mpaatf4qpc
ata(a8pb
atmppt8efWtrpcOttpc
P
elnp
F
560 S. T. SEROYER ET AL.
oid from the 5:30 to 3-o’clock position but must beble to place sutures in the capsule as low as the-o’clock position to perform the capsular shift. Al-hough this may be performed by use of suture-pass-ng devices from the anterior (or 5-o’clock) portal, thelane of tissue that can be captured with the devicesntering from these portals is not collinear with therientation of the capsular shift. Using a curved-tiputure-passing device inserted through the 7-o’clockortal, the surgeon can capture the capsulolabral tissuen line with the desired shift. Customarily, the capsuleill be imbricated starting at the ½ to 1-o’clock positionistal to the location of the anchor placement (i.e., forn anchor at the 5-o’clock position, tissue should bembricated from the 5:30 position and shifted superi-rly). The 5-o’clock portal is used percutaneously toain access to the anteroinferior glenoid for anchorlacement. The lowest anchor is usually placed atpproximately the 5-o’clock to 5:30 position on thelenoid. After the needle localization of the 7-o’clockortal, a switching stick is inserted through the portalo ensure proper access and trajectory. To establish theroper intra-articular trajectory, the needle should beriented about 60° to 70° to the floor. An 8.25-mmannula is placed in this portal, to accommodate var-ous suture-passing devices. A curved, soft tissue–enetrating, suture-passing device is used to accesshe capsule and perform the shift. In a right shoulder,device with the curved tip directed to the left is used;
n a left shoulder a curved tip directed to the right isore advantageous. A PDS suture is passed through
he capsule and under the avulsed labrum near the-o’clock position and is retrieved (along with theedial suture limb of the anchor) from the anterior
ortal for suture relay. After the PDS is tied to thenchor limb, this limb is shuttled through the labrumnd retrieved through the 7-o’clock portal, which ishen used to tie the knot. This same process is repeatedor each additional anchor required. Once the-o’clock to 4:30 position is reached, the anterioruadrant becomes the working quadrant and the ap-roach to the anterior quadrant is implemented for theompletion of the repair.
Access to the posteroinferior glenoid, between 6:30nd 8:30, is required for reverse Bankart lesions, mul-idirectional instability cases, and posterior extent ofnteroinferior instability past the 6-o’clock positionFig 4). Approach to this portion of the glenoid ischieved through the 7-o’clock portal. We place an.25-mm cannula to allow passage of curved suture-assing instruments or a bur, if needed, to prepare a
one bed for a posterior Bankart lesion. Sutures frombl
nchors in this portion of the glenoid can be retrievedhrough the posterior cannula to ease suture manage-ent and to avoid suture tangling, because the suture-
assing devices are inserted through the 7-o’clockortal to access the posteroinferior capsule to performhe necessary shift. The sutures in the 7-o’clock to:30 anchors are tied through the 7-o’clock portal. Inxtensive, complex posterior labral pathology, the in-erior portion of the injury complex is addressed first.
e believe that the posterosuperior shift of the pos-eroinferior capsule is the most vital component of theepair and should be performed first. Once this com-onent is repaired, the reconstruction efforts can pro-eed superiorly to include the entire zone of injury.nce the repair has progressed to the 9-o’clock posi-
ion, the surgical approach is shifted to workinghrough the standard posterior portal, as describedreviously, to allow for a more direct approach to theapsulolabral tissue at that level.
osterior Quadrant
When repairing SLAP lesions that have posteriorxtension (type IIB, IIC, or VIII13), posterior Bankartesions, or multidirectional instability, the surgeoneeds to be able to adequately access the posterior andosterosuperior labrum. Although the posterior portal
IGURE 4. Posteroinferior quadrant. The 7-o’clock portal (7=) can
e used to access posterior labral tears, 270° labral tears, or 360°abral tears for anchor insertion or suture management.
iwpTpati(fp
p7smeptpfatargtcssdeaptdusstdaar
mvtp
psaasd(pttclvtodba
G
S
A
I
P
561FOUR-QUADRANT CAPSULOLABRAL REPAIR
s our standard viewing portal, for posterior injuries,e will switch the arthroscope to the anterior portal torovide better visualization of the posterior labrum.o access the posterosuperior glenoid for anchorlacement in the 9:30 to 10:30 position, the suturenchor drill guide is placed percutaneously throughhe Port of Wilmington portal. A curved suture-pass-ng device is placed through the posterior portalcurved to the right for right shoulders and to the leftor left shoulders). The knots will be tied through theosterior cannula.As the extent of the injury progresses down the
osterior glenoid and labrum, the posterior and-o’clock portals are used for anchor placement anduture passage and management. The arthroscope re-ains in the anterior cannula for visualization. The
xtent of the patient’s capsulolabral injury and theatient’s clinical presentation and symptoms will dic-ate our approach to the capsule. If the patient hasosteroinferior instability complaints and a posteroin-erior capsular injury, the posterior surgery is initiatedt the 7-o’clock position on the glenoid so that theissues in the posteroinferior axillary recess can beccessed to perform a capsular shift in a posterosupe-ior direction. The 9- and 10-o’clock positions on thelenoid are easily accessed for anchor placement withhe drill guide introduced into the joint through theannula in the standard posterior portal. To avoidubchondral penetration of the anchors on the glenoidurface, the surgeon’s hand must be almost perpen-icular to the floor, once the guide is placed on thedge of the glenoid. In the 9- and 10-o’clock positions,superior capsular shift is not necessary. The capsularlication/fixation is performed in a horizontal direc-ion. To accomplish this, a straight suture-passingevice with an inline curve to it (the same instrumentsed at the 2-o’clock position anteriorly) can be in-erted through the posterior cannula to place the PDSuture through the capsule and labrum at the level ofhe anchor. Standard suture relay is then performed toeliver the suture from the anchor through the capsulend labrum. The sutures in the 9- and 10-o’clocknchors will be tied through the cannula in the poste-ior portal.
CONCLUSIONS
Glenohumeral capsulolabral pathology is a com-on entity faced by the general orthopaedist. Ad-
ances in arthroscopic techniques and instrumenta-ion have allowed capsulolabral reconstruction to be
erformed entirely through an arthroscopic ap- eroach. The arthroscopist must develop a tacticalurgical approach that will allow access and visu-lization to the entire glenoid and labrum. Adopting4-quadrant approach the glenoid and labrum can
implify this process and allow an effective, repro-ucible approach to the entire surface of the glenoidTable 1). The approaches to the superior, anterior,osterior, and inferior quadrants can be combined toreat complex cases that involve pathology thatraverses multiple quadrants. The surgeon’s surgi-al approach should include consideration of theocation of portal placement, suture management,isualization, and ability to approach necessary por-ions of the glenoid for anchor fixation. Percutane-us portal utilization can help prevent iatrogenicamage to soft-tissue structures that may be causedy cannulas. The detailed approach described in thisrticle will allow the arthroscopist access to the
TABLE 1. Pearls and Tips for Arthroscopic Managementof Glenohumeral Pathology
eneral tipsWith the patient in the lateral decubitus position, the surgeon
should be positioned to avoid backhanding instruments, thatis, standing below the shoulder for superior glenoid-labrumwork (proximal to 10 and 2 o’clock) and above the shoulderfor inferior work
Know cannula diameters required for passage of instrumentsof choice
Perform outside-in needle localization to establish portals, ensuringproper access and angle of approach to glenoid and labrum
Avoid use of cannula if possible in intratendinous locationsPlace knots on posterior surface of labrum to prevent potential
abrasion of humeral headuperior quadrantShift anterior portal to superior portion of rotator interval to
allow access to capsule/labrum posterior to bicepsPlace anchors percutaneously through anterosuperolateral portal
nterior quadrantShift anterior portal to inferior portion of rotator intervalEstablish 5-o’clock portal (no cannula) to access 3- to
4-o’clock position of glenoid/labrumnferior quadrant
Drill 4-o’clock to 5:30 anchors from 5-o’clock portalEstablish 7-o’clock portal to access capsule in line with
intended anterosuperior capsular shiftUse suture-passing device with tip curved to left for right
shoulder and curved to right for left shoulderosterior quadrantEstablish 7-o’clock portal for posteroinferior glenoid accessOrient needle about 60°-70° to floor to establish proper
intra-articular trajectory through 7-o’clock portalPosition hand relatively perpendicular to floor (lateral
decubitus) to allow proper orientation of anchor in glenoid
ntire glenohumeral joint and transform repair of
cc
f
1
1
1
1
562 S. T. SEROYER ET AL.
omplex intra-articular pathology into simple exer-ises in arthroscopic surgical technique.
Acknowledgment: The authors thank Adam Yanke, M.D.,or his illustrations.
REFERENCES
1. Andrews JR, Carson WG Jr, Ortega K. Arthroscopy of theshoulder: Technique and normal anatomy. Am J Sports Med1984;12:1-7.
2. Mazzocca AD, Noerdlinger M, Cole B, Romeo A. Arthros-copy of the shoulder: Indications and general principles oftechniques. In: McGinty J, ed. Operative arthroscopy. Phila-delphia: Lippincott Williams & Wilkins, 2003;412-427.
3. Matthews LS, Zarins B, Michael RH, Helfet DL. Anteriorportal selection for shoulder arthroscopy. Arthroscopy 1985;1:33-39.
4. Wolf EM. Anterior portals in shoulder arthroscopy. Arthros-copy 1989;5:201-208.
5. Davidson PA, Tibone JE. Anterior-inferior (5 o’clock) portalfor shoulder arthroscopy. Arthroscopy 1995;11:519-525.
6. Lo IK, Lind CC, Burkhart SS. Glenohumeral arthroscopyportals established using an outside-in technique: Neurovas-cular anatomy at risk. Arthroscopy 2004;20:596-602.
7. Laurencin CT, Deutsch A, O’Brien SJ, Altchek DW. Thesuperolateral portal for arthroscopy of the shoulder. Arthros-copy 1994;10:255-258.
8. Davidson PA, Rivenburgh DW. The 7-o’clock posteroinferiorportal for shoulder arthroscopy. Am J Sports Med 2002;30:693-696.
9. Chhabra A, Diduch DR, Anderson M. Arthroscopic repair of aposterior humeral avulsion of the inferior glenohumeral liga-ment (HAGL) lesion. Arthroscopy 2004;20:73-76 (suppl 2).
0. Meyer M, Graveleau N, Hardy P, Landreau P. Anatomic risksof shoulder arthroscopy portals: Anatomic cadaveric study of12 portals. Arthroscopy 2007;23:529-536.
1. Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAPlesions: Three subtypes and their relationships to superior insta-bility and rotator cuff tears. Arthroscopy 1998;14:553-565.
2. Neviaser TJ. Arthroscopy of the shoulder. Orthop Clin NorthAm 1987;18:361-372.
3. Seroyer S, Tejwani SG, Bradley JP. Arthroscopic capsulola-bral reconstruction of the type VIII superior labrum anteriorposterior lesion: Mean 2-year follow-up on 13 shoulders. Am J
Sports Med 2007;35:1477-1483.