Embed Size (px)
Citation preview

Frank M. Andrews, DVM, MS, DACVIMProfessor of LA Medicine
The University of Tennessee, CVM
Diseases of the Diseases of the StomachStomach
Diseases of the Diseases of the StomachStomach
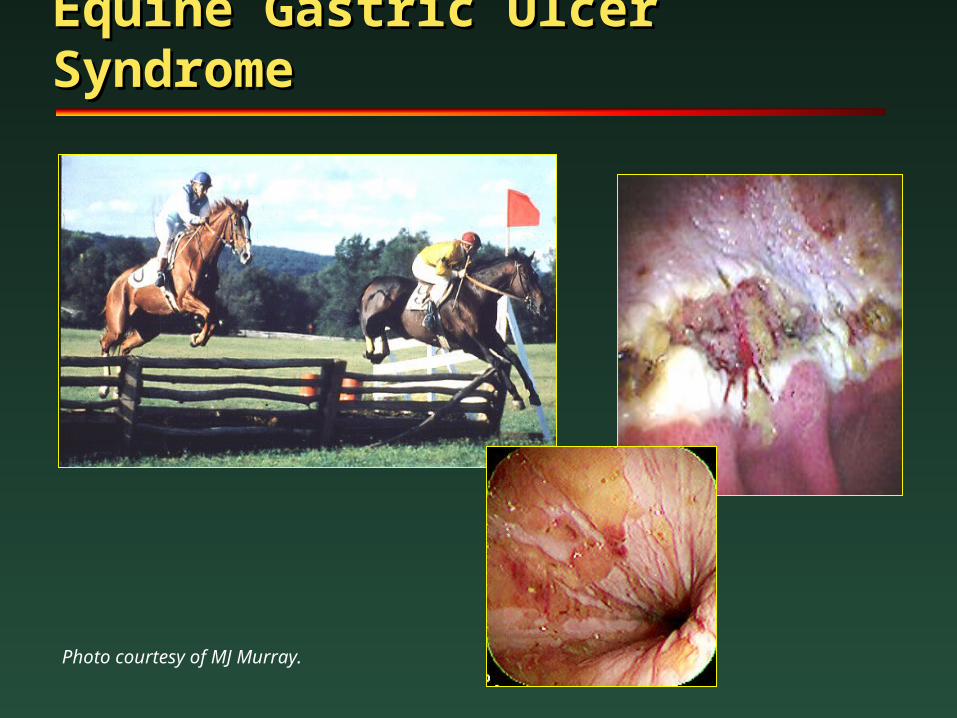
Equine Gastric Ulcer Equine Gastric Ulcer SyndromeSyndrome
Photo courtesy of MJ Murray.
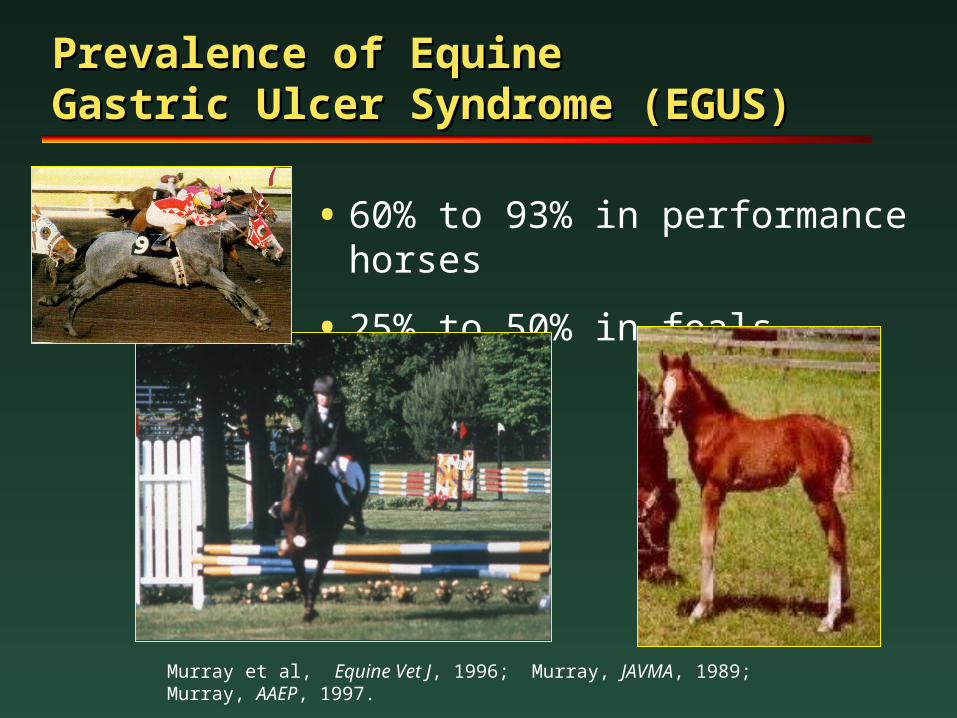
Prevalence of Equine Prevalence of Equine Gastric Ulcer Syndrome (EGUS)Gastric Ulcer Syndrome (EGUS)
• 60% to 93% in performance horses
• 25% to 50% in foals
Murray et al, Equine Vet J, 1996; Murray, JAVMA, 1989; Murray, AAEP, 1997.
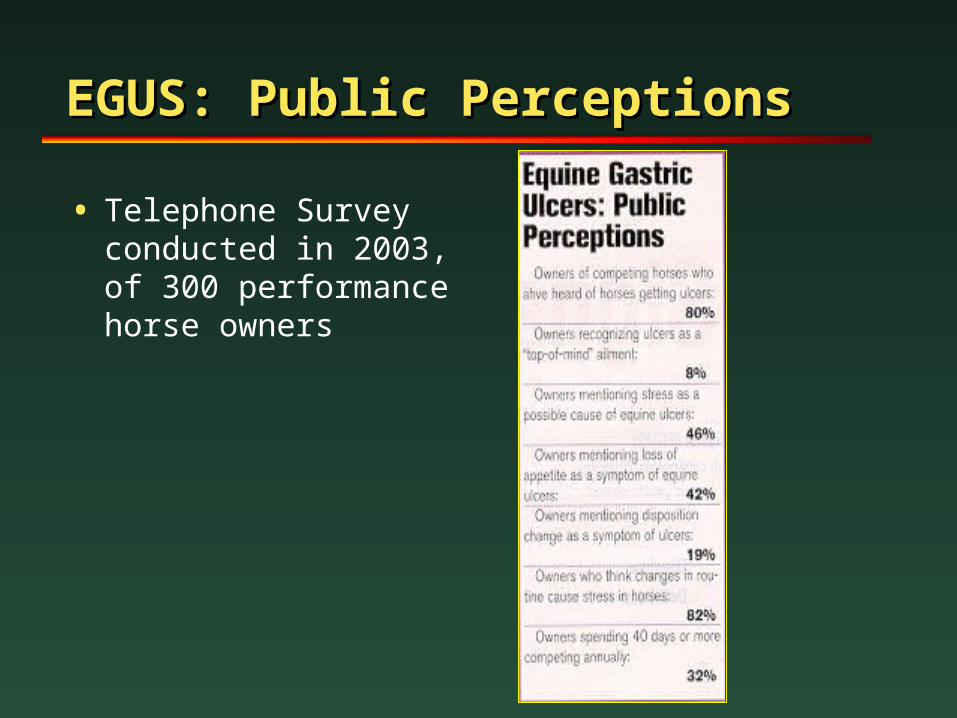
EGUS: Public PerceptionsEGUS: Public Perceptions
• Telephone Survey conducted in 2003, of 300 performance horse owners
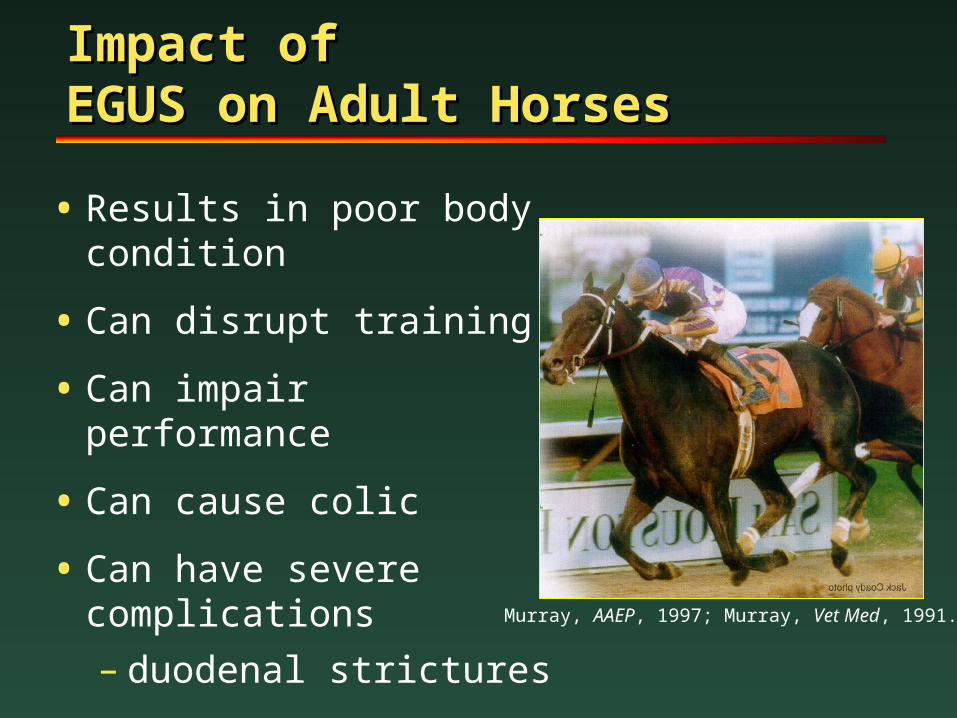
Impact of Impact of EGUS on Adult HorsesEGUS on Adult Horses
• Results in poor body condition
• Can disrupt training
• Can impair performance
• Can cause colic
• Can have severe complications
– duodenal strictures Murray, AAEP, 1997; Murray, Vet Med, 1991.
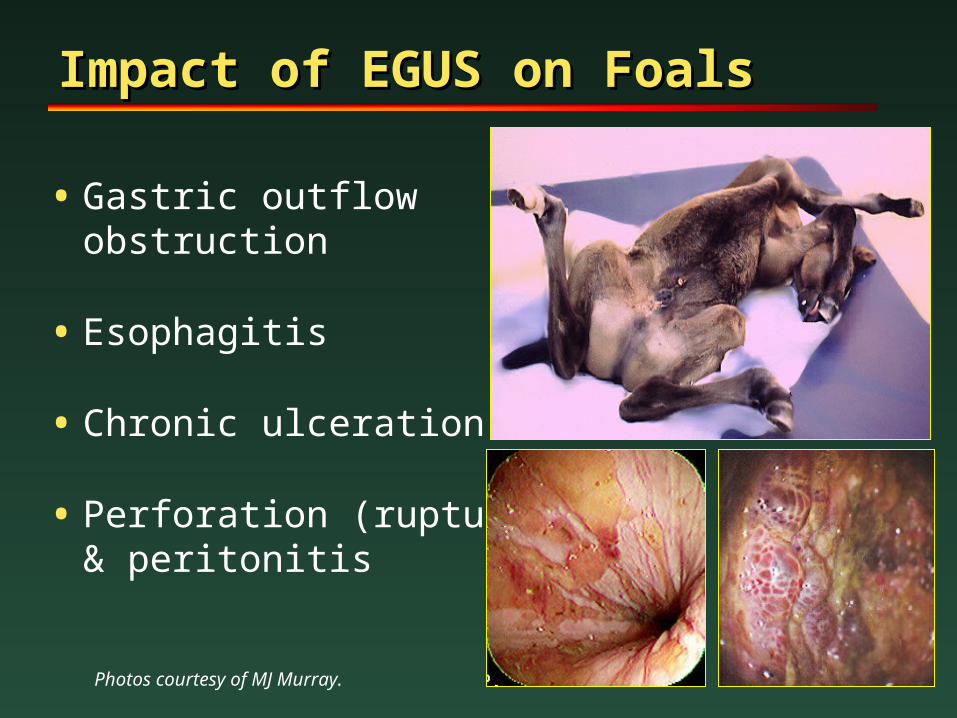
Impact of EGUS on FoalsImpact of EGUS on Foals
• Gastric outflow obstruction
• Esophagitis
• Chronic ulceration
• Perforation (rupture) & peritonitis
Photos courtesy of MJ Murray.
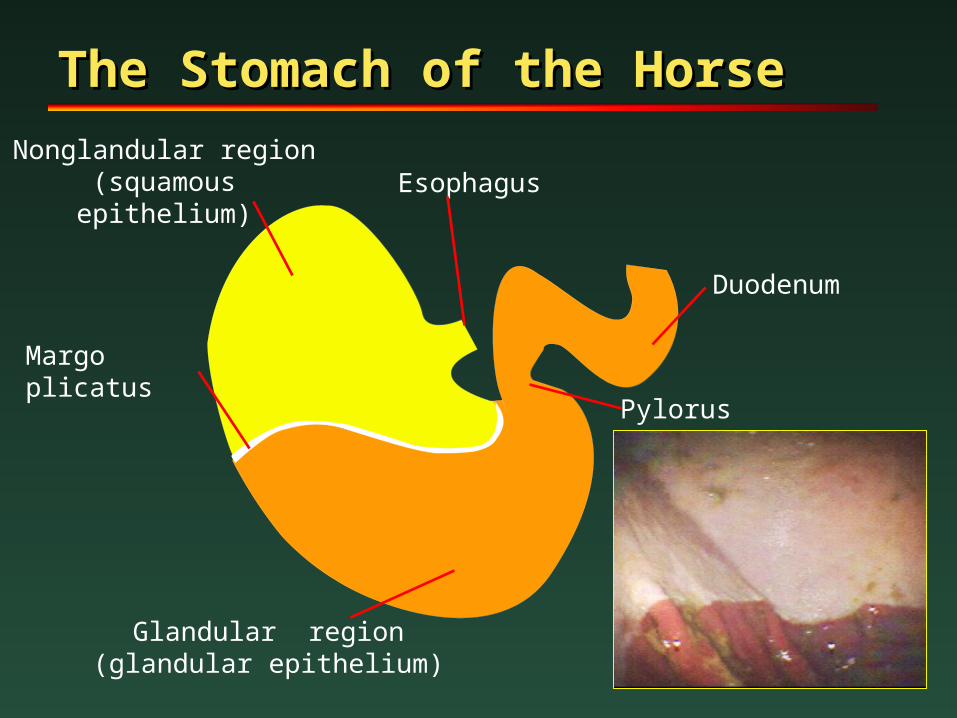
The Stomach of the HorseThe Stomach of the Horse
Margo plicatus
Glandular region(glandular epithelium)
Pylorus
Esophagus
Duodenum
Nonglandular region(squamous epithelium)
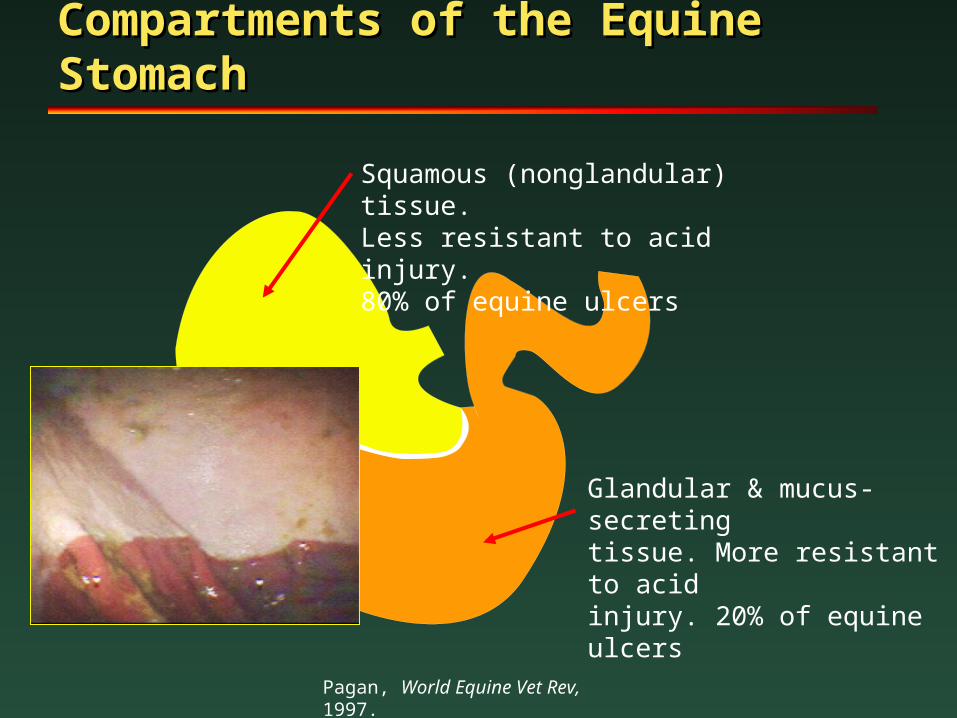
Compartments of the Equine Compartments of the Equine StomachStomach
Squamous (nonglandular) tissue.Less resistant to acid injury.80% of equine ulcers
Glandular & mucus-secretingtissue. More resistant to acidinjury. 20% of equine ulcers
Pagan, World Equine Vet Rev, 1997.
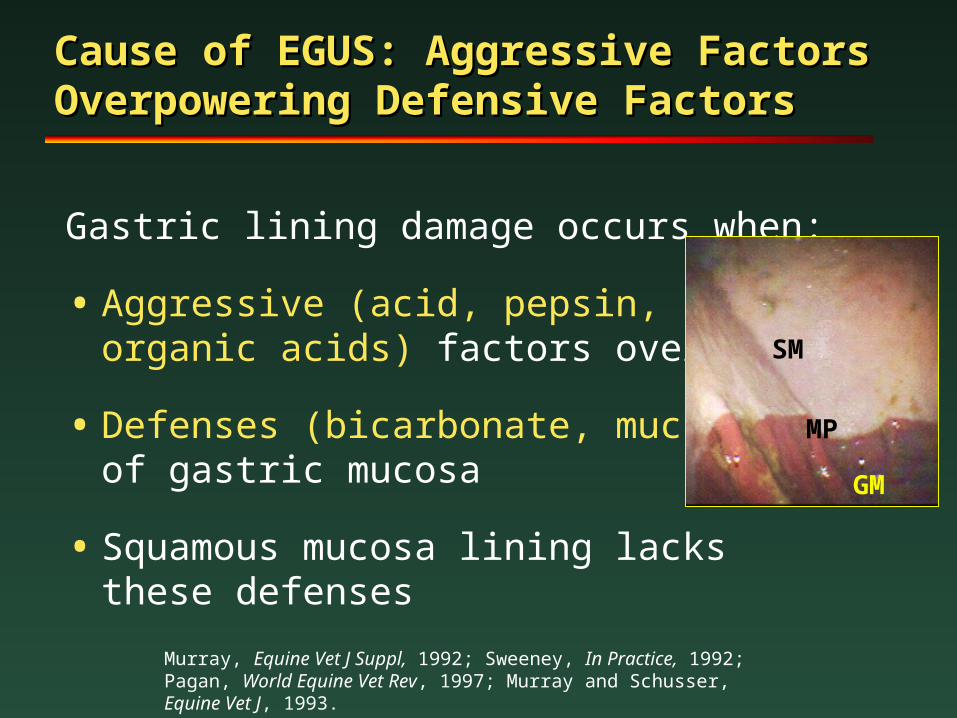
Cause of EGUS: Aggressive Factors Cause of EGUS: Aggressive Factors Overpowering Defensive FactorsOverpowering Defensive Factors
Gastric lining damage occurs when:
• Aggressive (acid, pepsin, bile,organic acids) factors overpower
• Defenses (bicarbonate, mucus)of gastric mucosa
• Squamous mucosa lining lacks these defenses
Murray, Equine Vet J Suppl, 1992; Sweeney, In Practice, 1992; Pagan, World Equine Vet Rev, 1997; Murray and Schusser, Equine Vet J, 1993.
SM
GM
MP
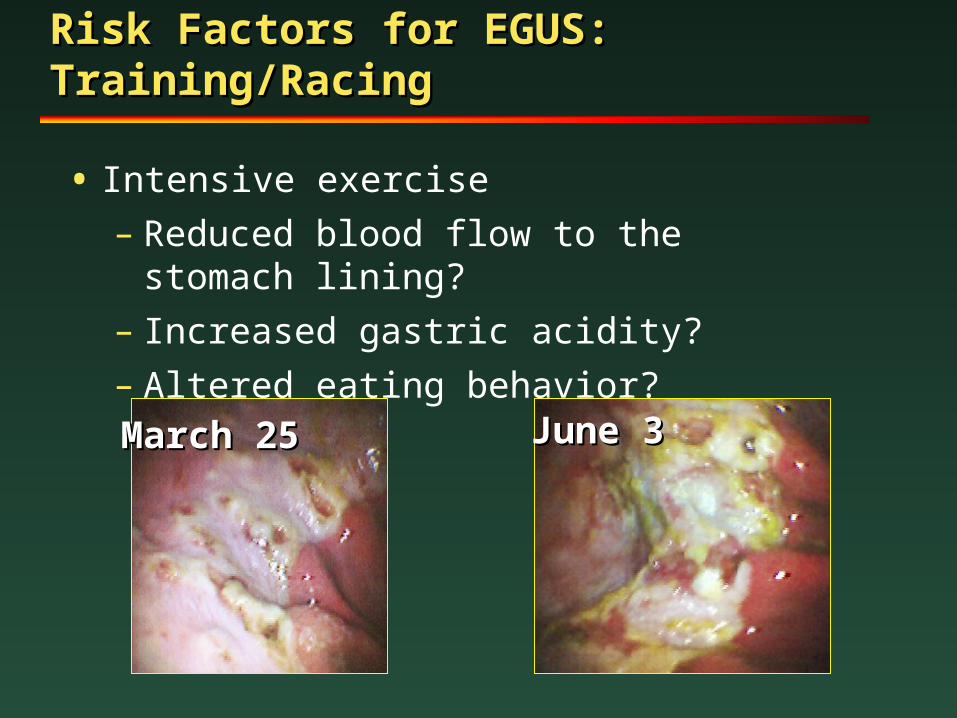
Risk Factors for EGUS: Risk Factors for EGUS: Training/RacingTraining/Racing
• Intensive exercise
– Reduced blood flow to the stomach lining?
– Increased gastric acidity?
– Altered eating behavior?
March 25March 25 June 3June 3
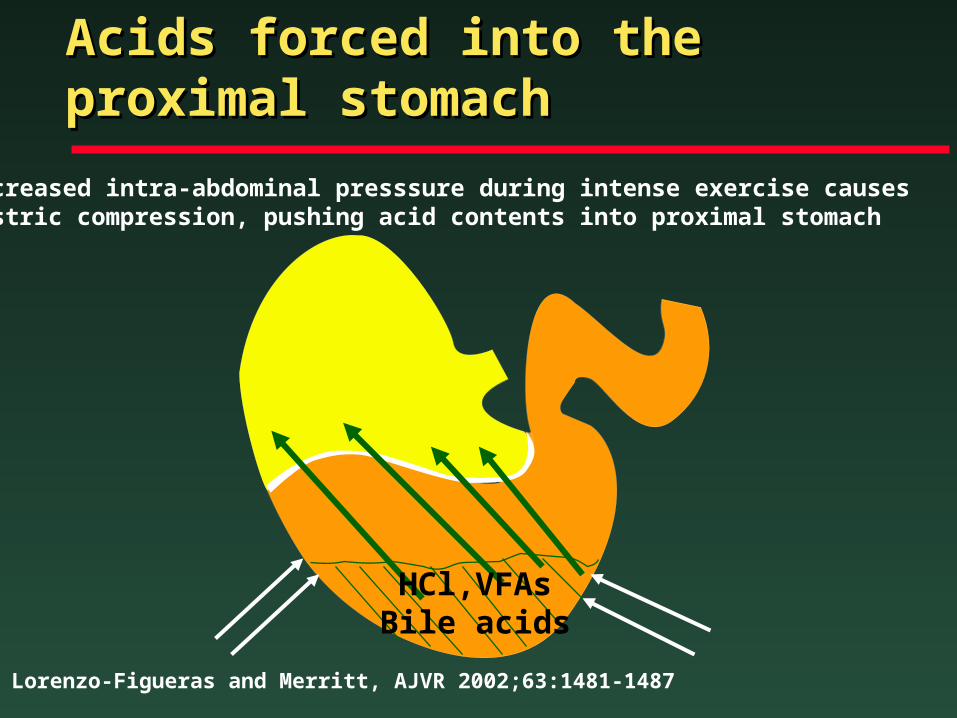
Acids forced into the Acids forced into the proximal stomachproximal stomach
Increased intra-abdominal presssure during intense exercise causes gastric compression, pushing acid contents into proximal stomach
Lorenzo-Figueras and Merritt, AJVR 2002;63:1481-1487
HCl,VFAsBile acids
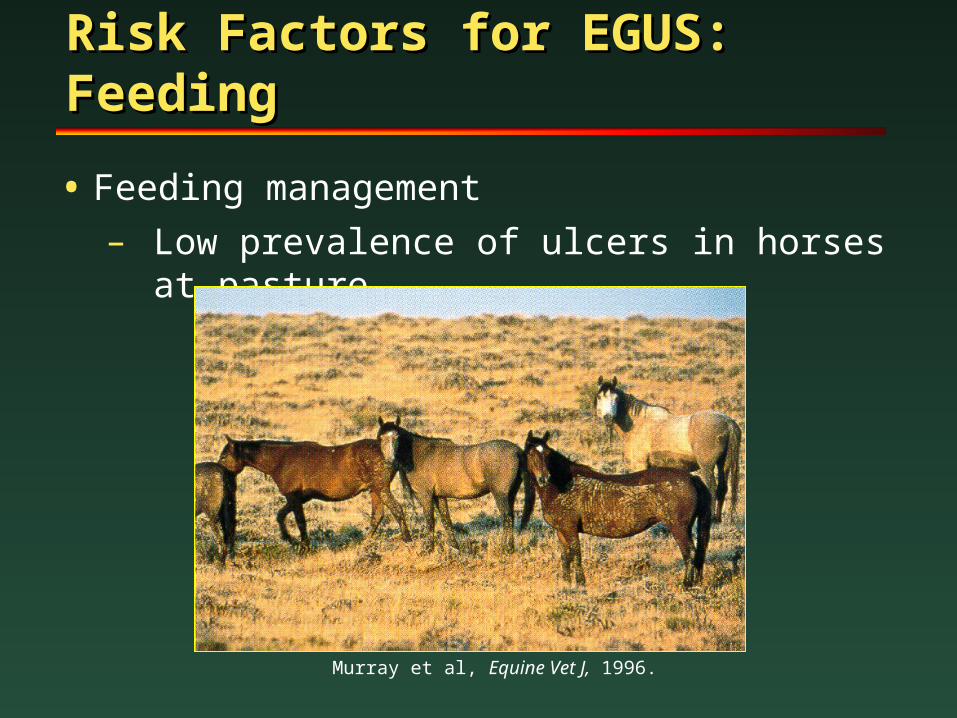
Risk Factors for EGUS: Risk Factors for EGUS: FeedingFeeding
• Feeding management
– Low prevalence of ulcers in horses at pasture
Murray et al, Equine Vet J, 1996.
Risk Factors for EGUS: Risk Factors for EGUS: FeedingFeeding
– Decreased acid when roughage available
– Increased serum gastrin when fed concentrates (grains & sweet feeds)
– Intermittent feed deprivation =gastric ulcers
– Stall confinement = gastric ulcers
– Feeding alfalfa hay may help!
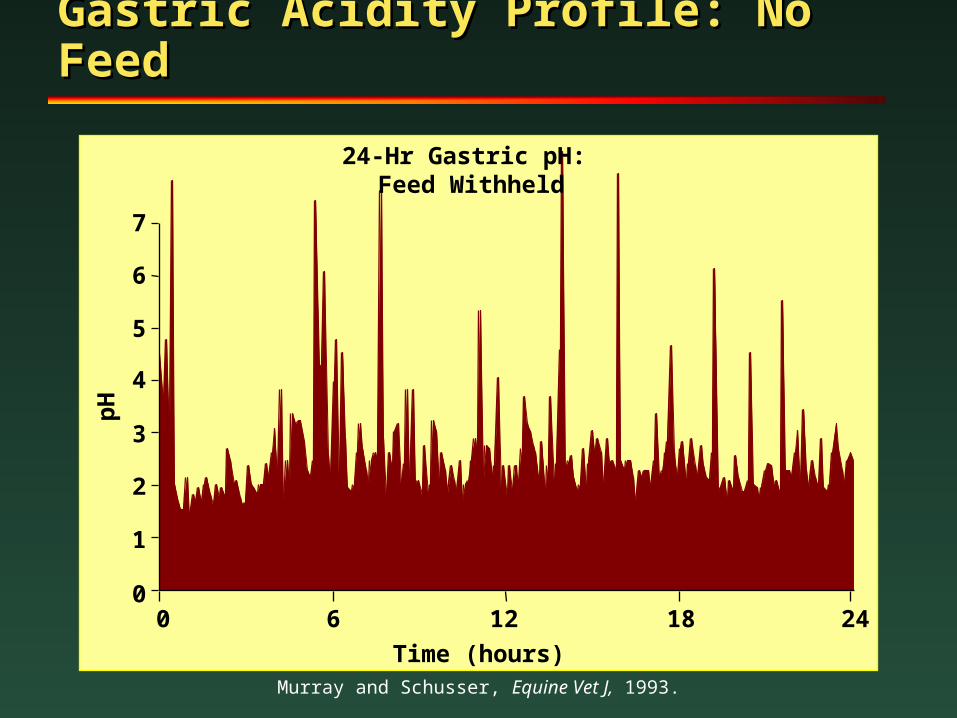
Gastric Acidity Profile: No FeedGastric Acidity Profile: No Feed
Murray and Schusser, Equine Vet J, 1993.
0
1
2
3
4
5
6
7
pH
24-Hr Gastric pH: Feed Withheld
0 6 12 18 24
Time (hours)
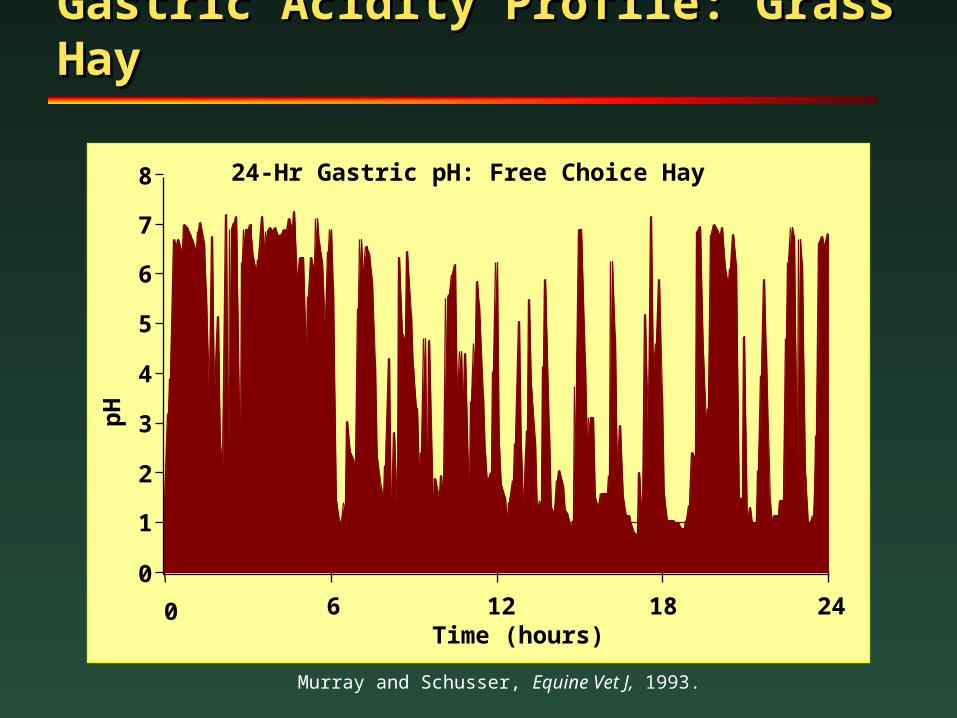
Gastric Acidity Profile: Grass Gastric Acidity Profile: Grass HayHay
Murray and Schusser, Equine Vet J, 1993.
Time (hours)
0
1
2
3
4
5
6
7
8
pH
24-Hr Gastric pH: Free Choice Hay
0 6 12 18 24
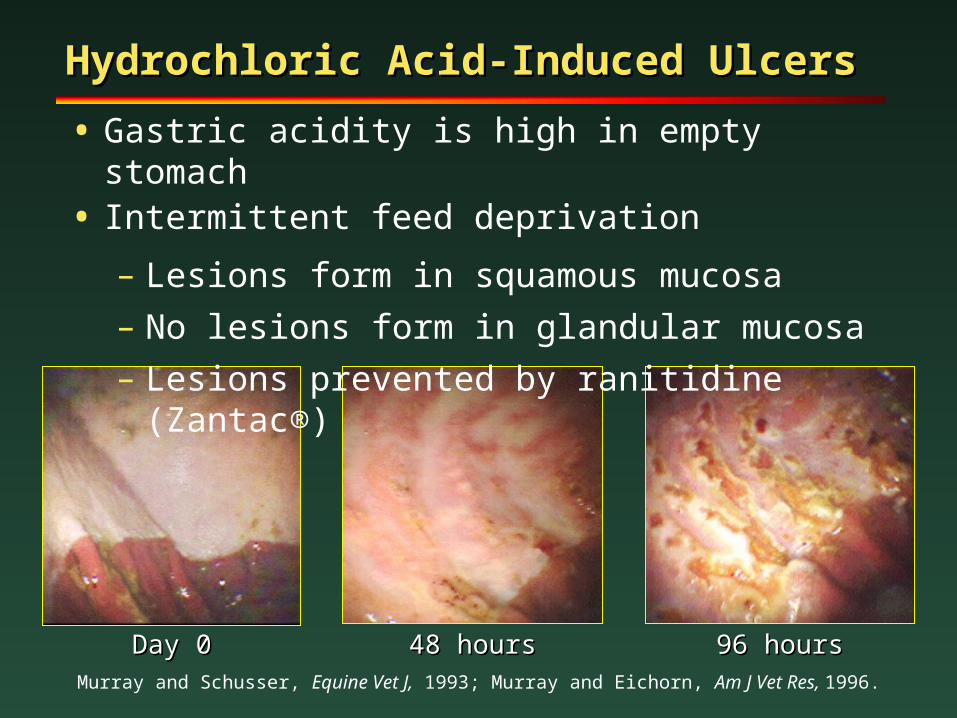
Day 0Day 0 48 hours48 hours 96 hours96 hours
Hydrochloric Acid-Induced UlcersHydrochloric Acid-Induced Ulcers
• Gastric acidity is high in empty stomach• Intermittent feed deprivation
– Lesions form in squamous mucosa
– No lesions form in glandular mucosa
– Lesions prevented by ranitidine (Zantac®)
Murray and Schusser, Equine Vet J, 1993; Murray and Eichorn, Am J Vet Res, 1996.
Risk Factors for EGUS: Risk Factors for EGUS: Stress Stress
1. Physical stress– Illness– Painful musculoskeletal disorder
2. Behavioral stress– Stall confinement – Transport– Unfamiliar environment,
social regrouping
Risk Factors for EGUS:Risk Factors for EGUS:Non-Steroidal Anti-Inflammatory Drugs Non-Steroidal Anti-Inflammatory Drugs
• Phenylbutazone & Flunixin Meglumineand other NSAIDs
• Associated with ulcers throughout the intestinal tract (Cecum & Colon)
• Inhibit prostaglandins, interrupting mucosal blood flowand mucus
• Local toxicity
Murray, Vet Med, 1991.
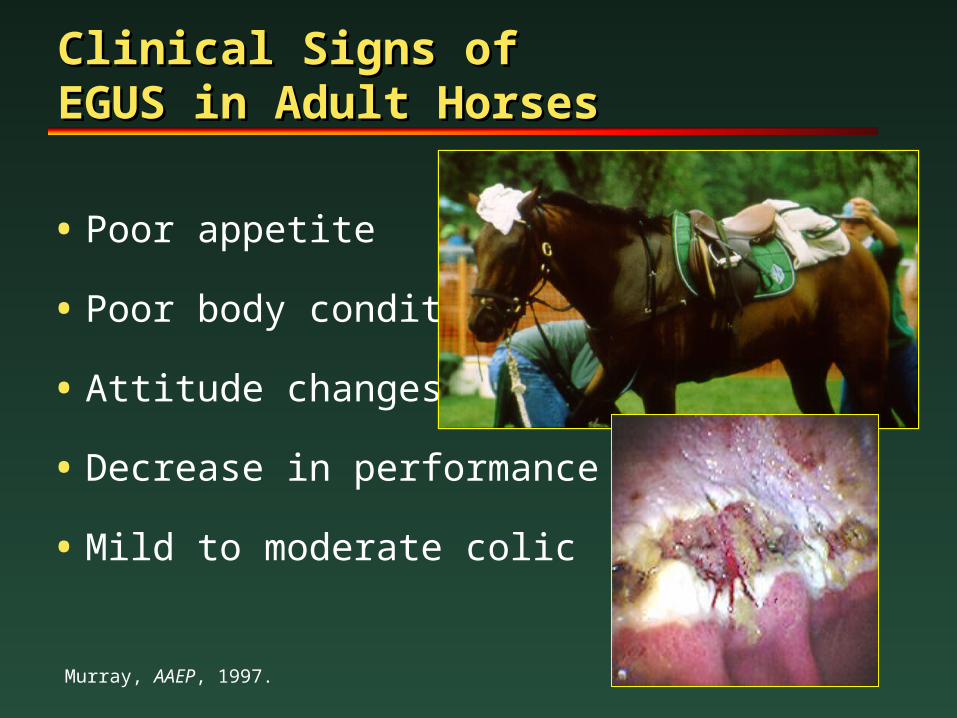
Clinical Signs ofClinical Signs ofEGUS in Adult Horses EGUS in Adult Horses
• Poor appetite
• Poor body condition
• Attitude changes
• Decrease in performance
• Mild to moderate colic
Murray, AAEP, 1997.
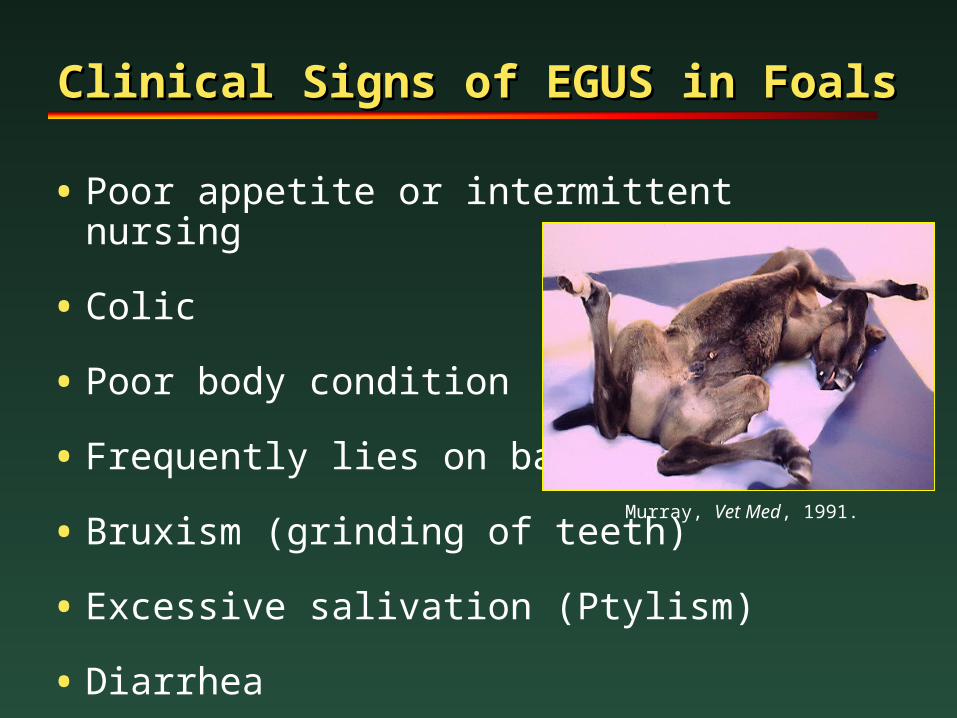
Clinical Signs of EGUS in Foals Clinical Signs of EGUS in Foals
• Poor appetite or intermittent nursing
• Colic
• Poor body condition
• Frequently lies on back
• Bruxism (grinding of teeth)
• Excessive salivation (Ptylism)
• Diarrhea
Murray, Vet Med, 1991.
How can you tell that a Horse How can you tell that a Horse has EGUS? (Diagnosis)has EGUS? (Diagnosis)
• Clinical signs are suggestive of, but not specific for, EGUS
• Lab: Mild anemia
• Response to treatment can be useful
• Gastric endoscopy is only definitive diagnostic tool
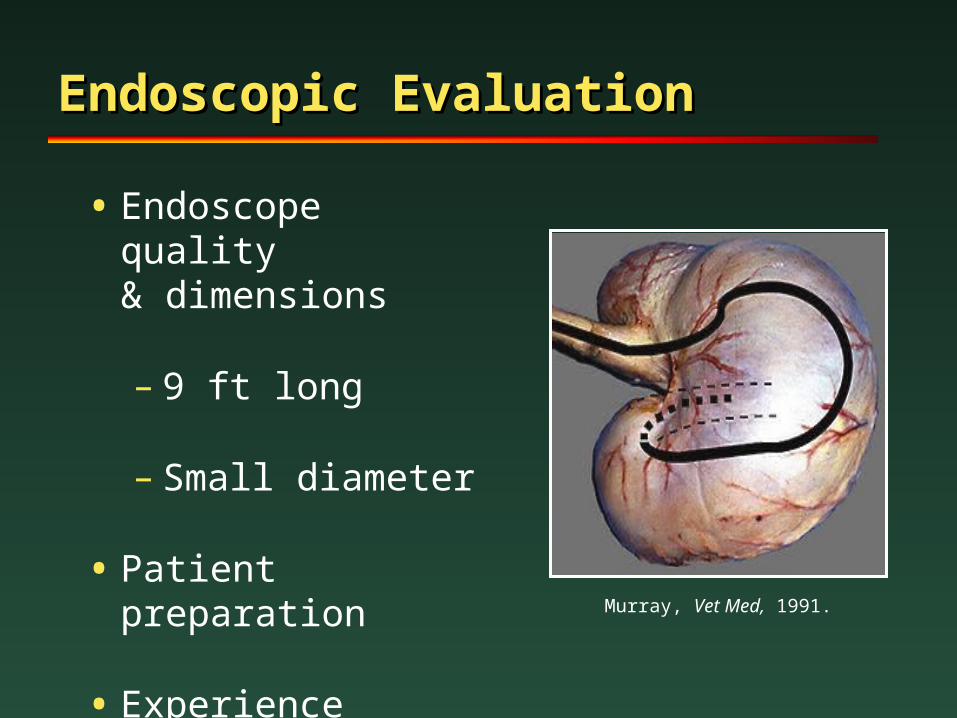
Endoscopic EvaluationEndoscopic Evaluation
• Endoscope quality& dimensions
– 9 ft long
– Small diameter
• Patient preparation
• Experience Murray, Vet Med, 1991.
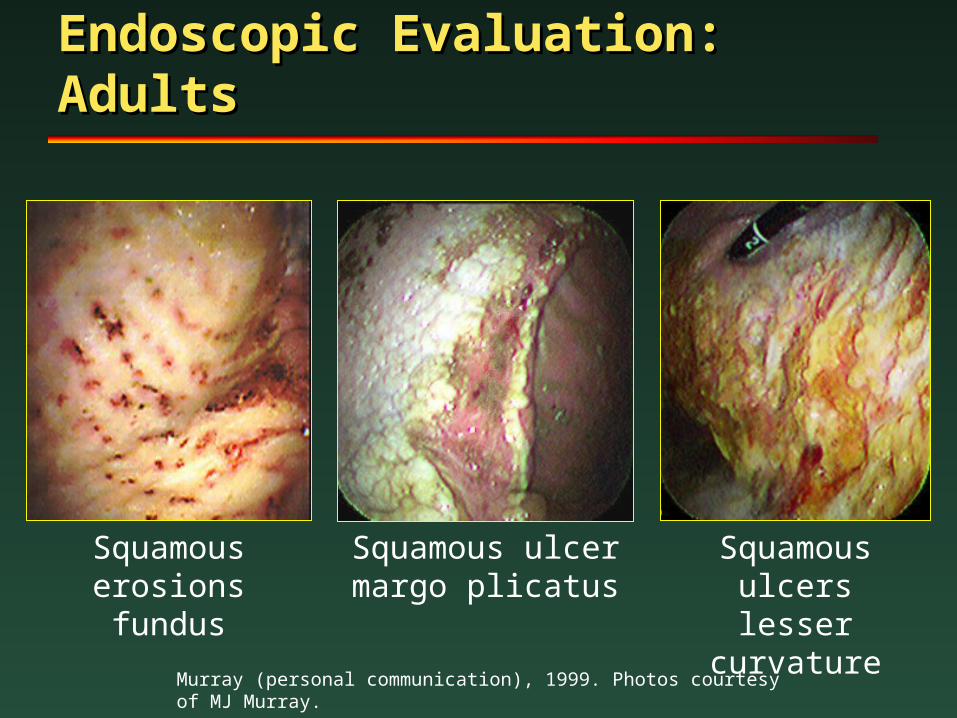
Squamous erosionsfundus
Squamous ulcerslesser curvature
Squamous ulcermargo plicatus
Endoscopic Evaluation: Endoscopic Evaluation: AdultsAdults
Murray (personal communication), 1999. Photos courtesy of MJ Murray.
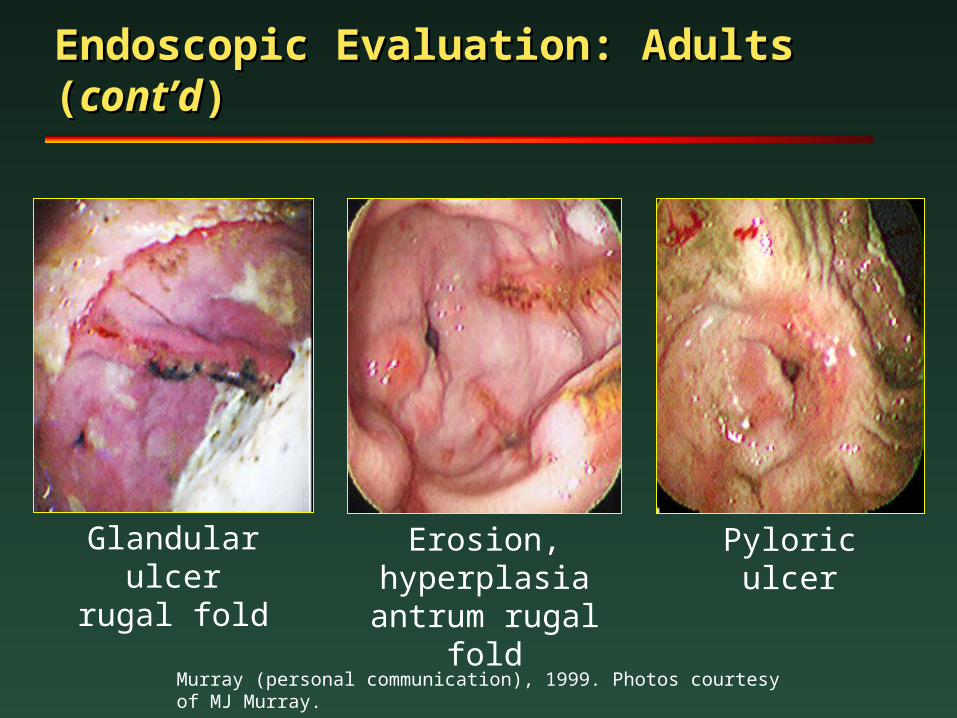
Glandular ulcerrugal fold
Erosion, hyperplasia
antrum rugal fold
Pyloric ulcer
Endoscopic Evaluation: Adults Endoscopic Evaluation: Adults ((cont’dcont’d))
Murray (personal communication), 1999. Photos courtesy of MJ Murray.
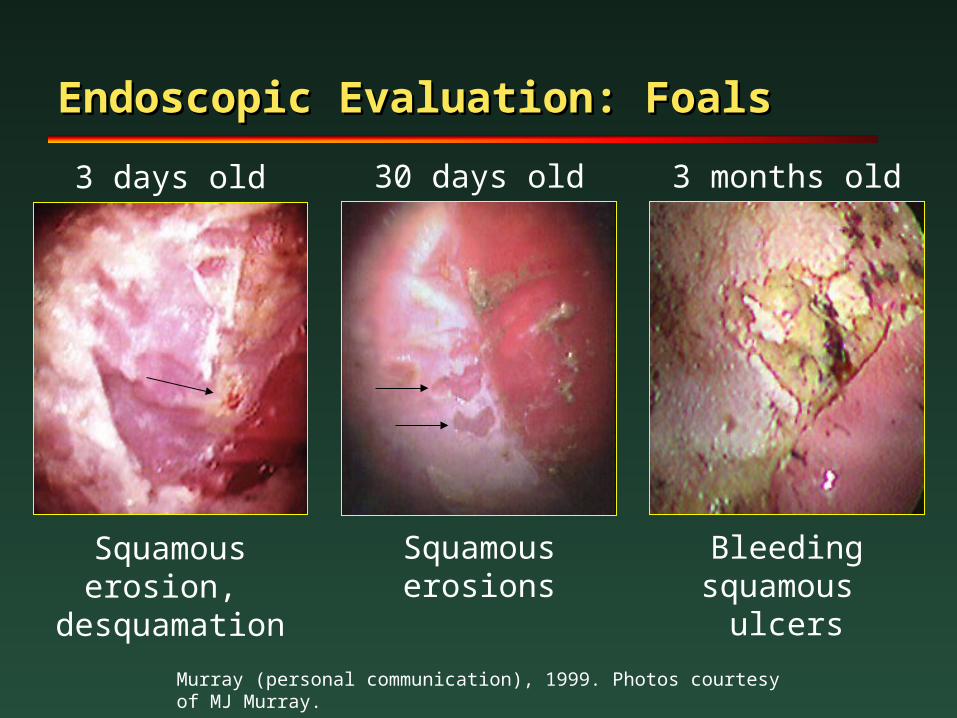
Squamous erosion,
desquamation
3 days old
Squamous erosions
30 days old
Bleeding squamous
ulcers
3 months old
Endoscopic Evaluation: FoalsEndoscopic Evaluation: Foals
Murray (personal communication), 1999. Photos courtesy of MJ Murray.
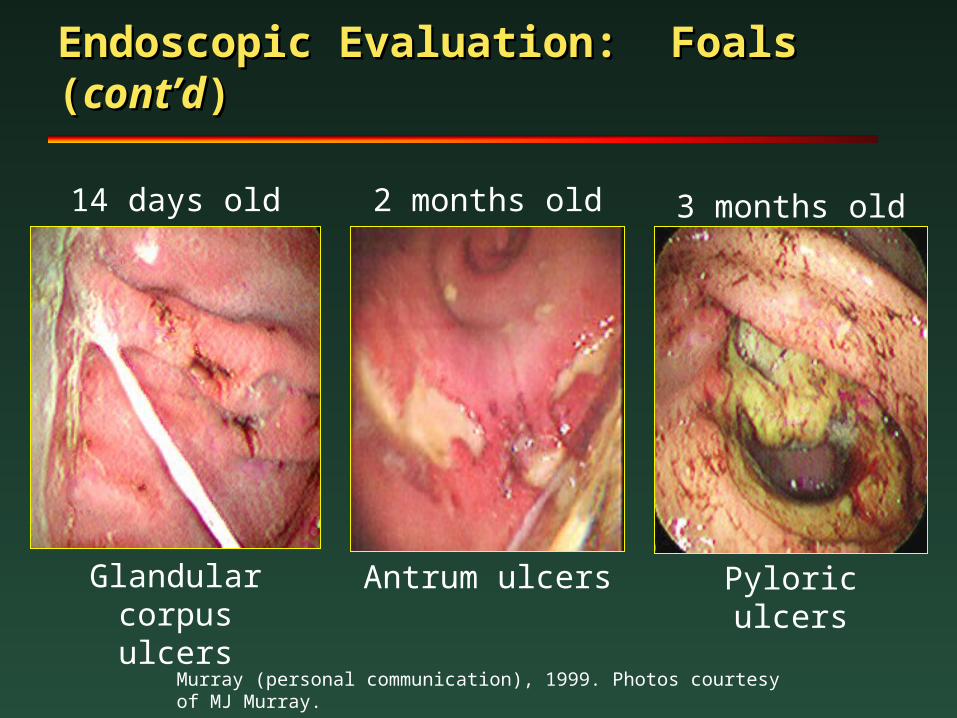
Glandular corpusulcers
14 days old 2 months old
Antrum ulcers
3 months old
Pyloric ulcers
Endoscopic Evaluation: Foals Endoscopic Evaluation: Foals ((cont’dcont’d))
Murray (personal communication), 1999. Photos courtesy of MJ Murray.
Treatment of EGUS Treatment of EGUS
• Eliminate clinical signs
• Promote healing
• Prevent complications
• Prevent recurrences
MacAllister, Vet Med, 1995.1
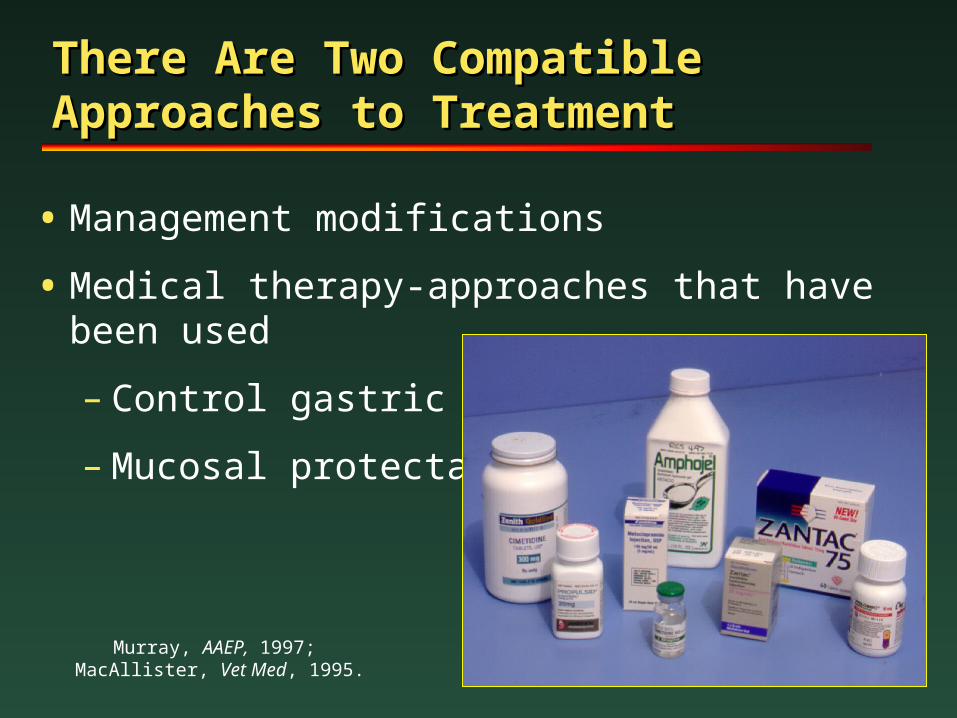
There Are Two Compatible There Are Two Compatible Approaches to TreatmentApproaches to Treatment
• Management modifications
• Medical therapy-approaches that have been used
– Control gastric acid
– Mucosal protectants
Murray, AAEP, 1997; MacAllister, Vet Med, 1995.
Traditional Management Traditional Management ModificationsModifications
• Reduce level of training
• Diet modifications
– Limit periods of fasting
– Increase roughage
• pasture turnout (green grass)
• free choice hay
• Alfalfa hay-dietary antacid
– Reduce grain/concentratesSeahorn, LSU Equine Vet Res Program Newsletter, 1998; Pagan, World Equine Vet Rev, 1997.
Traditional Management Traditional Management ModificationsModifications
Dietary ManagementDietary Management
• Fresh Rice Bran and Rice Bran Oil
– Contains surface active phospholipids and cytoprotective factors that maintain health of the stomach lining
– Rancidity can be a problem
• Produces ketoaldehydes which are ulcerogenic
– Steam pasteurization can help decrease potential for rancidity
– Storage in refrigerator
Management ModificationsManagement Modifications
Limit stressful events
• Long-term stall confinement
• Trailering
• Overcrowding
Organic Acids (VFAs or SCFAs) Organic Acids (VFAs or SCFAs) High Concentrate DietsHigh Concentrate Diets
• Acetic, Butyric, Propionic, and Valeric Acids
• Byproducts of carbohydrate fermentation inthe stomach
• Synergistic with HCl
• May lead to non-glandular ulcers
• Increased VFA’s with increased grain
Medical Management of Medical Management of EGUSEGUS
• Neutralizing agents
– Antacids
• Antisecretory agents
– Histamine H2 receptor antagonists
– Prostaglandin analog
– Acid pump inhibitors
• Others (antibiotics, neutriceuticals)
MacAllister, Vet Med, 1995.
**GastroGard, Merial LTD, Atlanta, GA. Only Drug Approved for horses
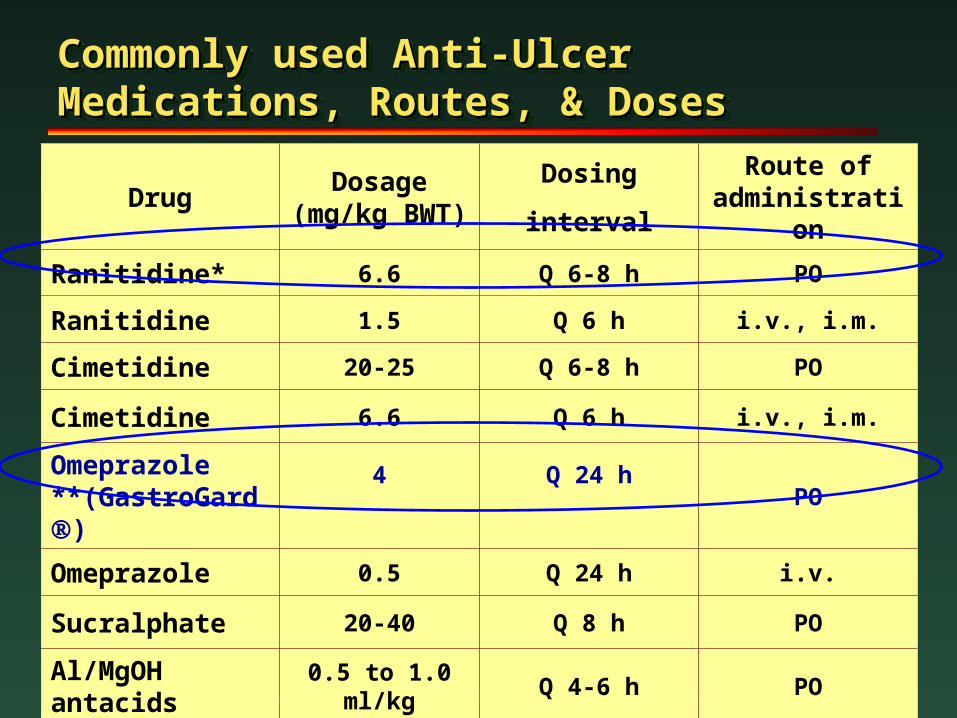
Commonly used Anti-UlcerCommonly used Anti-UlcerMedications, Routes, & DosesMedications, Routes, & DosesCommonly used Anti-UlcerCommonly used Anti-UlcerMedications, Routes, & DosesMedications, Routes, & Doses
DrugDosage
(mg/kg BWT)
Dosing
interval
Route of administration
Ranitidine* 6.6 Q 6-8 h PO
Ranitidine 1.5 Q 6 h i.v., i.m.
Cimetidine 20-25 Q 6-8 h PO
Cimetidine 6.6 Q 6 h i.v., i.m.
Omeprazole **(GastroGard)
4 Q 24 hPO
Omeprazole 0.5 Q 24 h i.v.
Sucralphate 20-40 Q 8 h PO
Al/MgOH antacids
0.5 to 1.0 ml/kg Q 4-6 h PO
GASTROGARDGASTROGARD®® (Omeprazole) (Omeprazole)
• New oral-paste formulation of omeprazole developed specifically for horses
• Well-studied, effective, and safe therapy for EGUS
• Approved for use in horses, March 1999
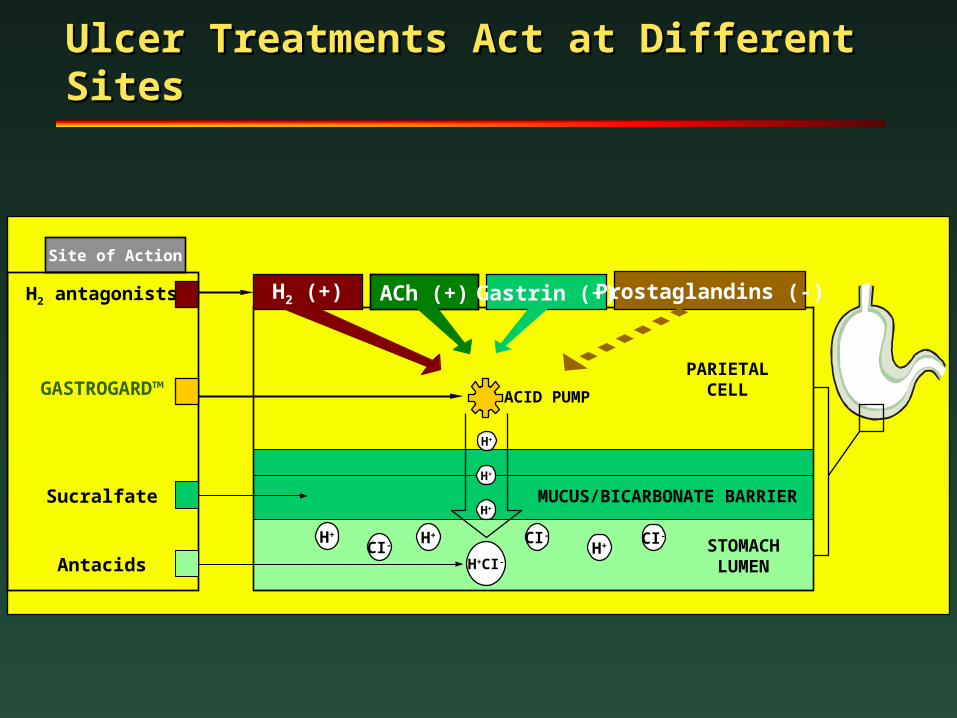
Ulcer Treatments Act at Different Ulcer Treatments Act at Different SitesSites
Site of Action
H2 antagonists
GASTROGARD™
Sucralfate
Antacids H+CI-
H2 (+) ACh (+) Gastrin (+) Prostaglandins (-)
H+ H+
CI- CI-
H+CI-
STOMACHLUMEN
MUCUS/BICARBONATE BARRIER
PARIETALCELL
H+
H+
H+
ACID PUMP
0
25
50
75
100
Improved Healed
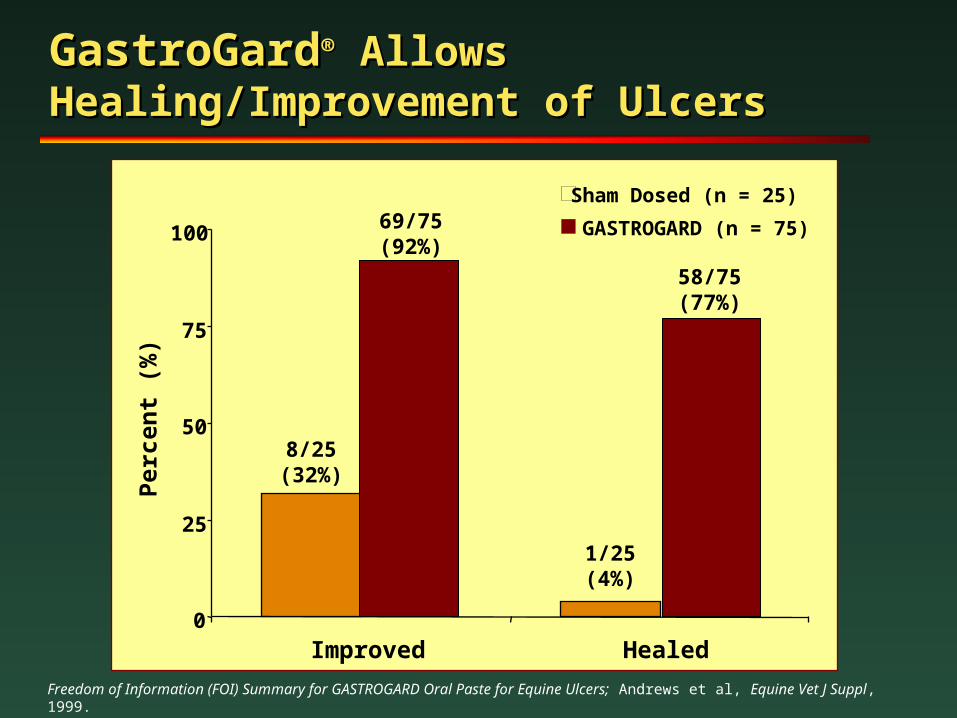
GastroGardGastroGard®® Allows Allows Healing/Improvement of UlcersHealing/Improvement of Ulcers
Per
cen
t (%
)
Sham Dosed (n = 25)
GASTROGARD (n = 75)
8/25(32%)
69/75(92%)
1/25(4%)
58/75(77%)
Freedom of Information (FOI) Summary for GASTROGARD Oral Paste for Equine Ulcers; Andrews et al, Equine Vet J Suppl, 1999.
GastroGardGastroGard®® AdvantagesAdvantages
Andrews et al, Comp Cont Educ Pract Bet, 1996.
• Profound gastric acid suppression
• Prolonged duration of action
• Once-daily dosing
• Well studied in horses
• No reported treatment-related
health problems in equine trials
• Prevents ulcer recurrence
• Can maintain training program
• Approved for use in horses (GASTROGARD®)
GastroGardGastroGard®®: Disadvantages: Disadvantages
• No IV formulation available in US
Andrews et al, Comp Cont Educ Pract Bet, 1996.
UlcerGardUlcerGard
• Prevention of ulcers
• Non-perscription strength of Gastrogard
• Sold through veterinarians
Histamine HHistamine H22 Receptor Receptor AntagonistsAntagonists
• Zantac® (ranitidine), Tagamet® (cimetidine)
• Competitive inhibition of the interaction of histamine with parietal cell
• Dose-dependent inhibition of gastric acid secretion
MacAllister, Vet Med, 1995.
Histamine HHistamine H22 Receptor Antagonists: Receptor Antagonists: Advantages & DisadvantagesAdvantages & Disadvantages
• Availability
• Low cost (generic)
• Zantac® has been shown to significantly inhibit gastric acid secretion in horses
• Must be administered 3X daily
Murray, AAEP, 1997.
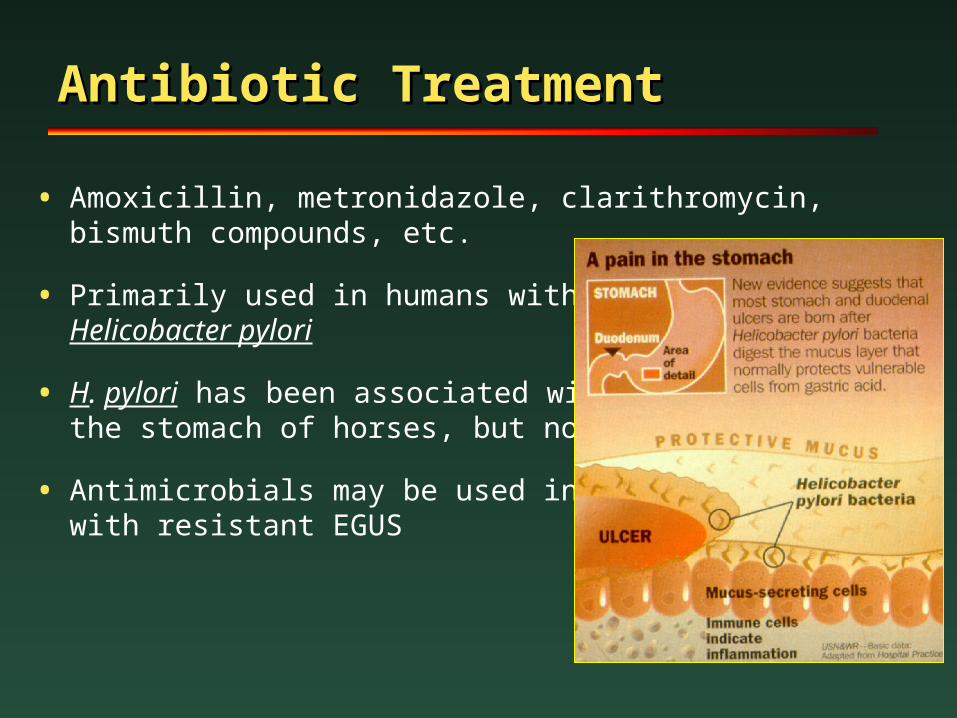
Antibiotic TreatmentAntibiotic Treatment
• Amoxicillin, metronidazole, clarithromycin,bismuth compounds, etc.
• Primarily used in humans with Helicobacter pylori
• H. pylori has been associated withthe stomach of horses, but not EGUS
• Antimicrobials may be used in horses with resistant EGUS
Recent Studies on Helicobacter Recent Studies on Helicobacter spp.spp.
• Helicobacter specific DNA isolated from horse stomachs
• 2 horses with squamous erosions
• 1 horse with glandular erosions
• ACVIM Forum-Dallas (May 2002)
Scott DR, Marcus EA, Shirazi-Beechey SSP, et al. Evidence of Helicobacter infection in the horse. Proc Am Soc Microbiology 2001.
Feed Supplements Feed Supplements (Neutriceuticals)(Neutriceuticals)
NeighLox® (Kentucky Performance Products)
• Antacid and Coating Agents:
– Aluminum Phosphate, Calcium Carbonate
– Dihydroxy-AluminiumSodium Carbonate
• Labeled for preventionof heartburn
• No studies in horsesto prove or disprove
• Probably does not cause any harm
Feed Supplements Feed Supplements (Neutriceuticals)(Neutriceuticals)
G.U.T (Uckele Health & Nutrition)
• Gastric ulcer transnutrient for horses with ulcers
• Ingredients
– Gelatin
– Lactobacillus acidophilus, L. lactis
• Feed 15 grams (1 scoop) twice daily in horses with ulcers
• No studies proving efficacy
Feed Supplements Feed Supplements (Neutriceuticals)(Neutriceuticals)
TractGard (Foxden Equine)
• Equine GI rehydrator, antacid, digestaid, and electrolyte salt
• Ingredients (1 to 2 scoops daily)
– Calcium carbonate, Sodium sequiscarbonate, KCl, MgSO4, distiller’s grain, yeast, and linseed meal
• No studies on efficacy
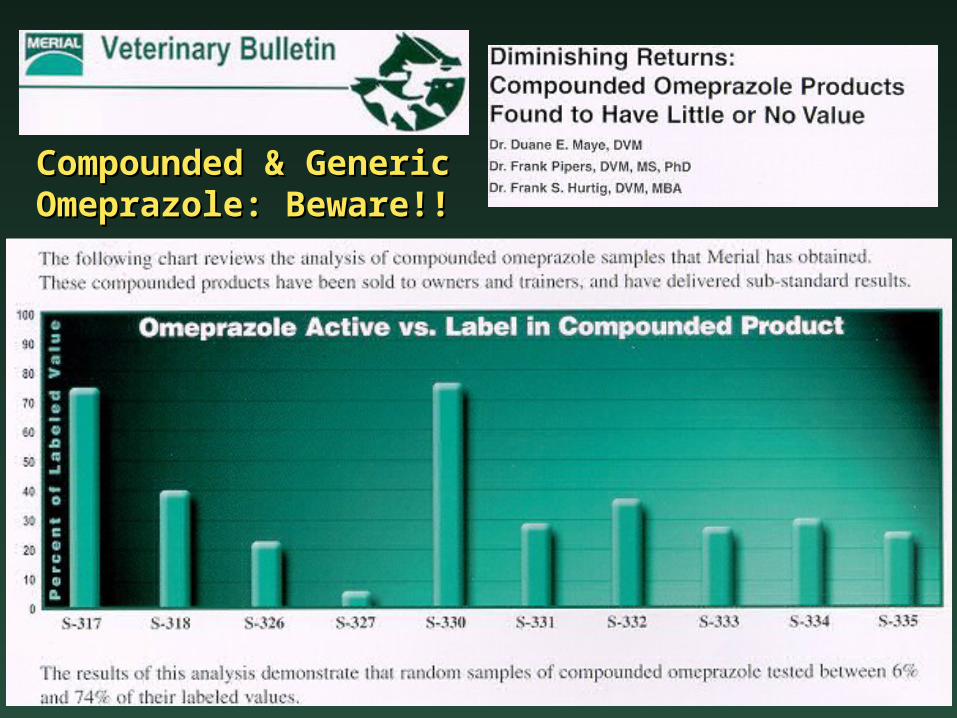
Compounded & GenericCompounded & GenericOmeprazole: Beware!!Omeprazole: Beware!!
Conclusions- GeneralConclusions- General
• EGUS is a major cause of illness
• 60-93% of performance horses have EGUS
• Impacts health, performance, economics
• Occurs when aggressive factors overpower gastric defenses
Conclusions- GeneralConclusions- General
• Diagnosis requires endoscopy
• Presumptive diagnosis made based on clinical signs following complete diagnostic evaluation
• Treatment: management and medical interventions
Conclusions- TreatmentConclusions- Treatment
• Zantac®-healing 3X daily treatment
• Dietary supplements-not tested
• GastroGard® (omeprazole)
– Only FDA approved treatment
– Provides potent, long-lasting gastric acid suppression in horses(once daily administration)
– 92% to 99% improvement in ulcer scores in trials and a wide safety margin
• UlcerGard Prevention of Ulcers
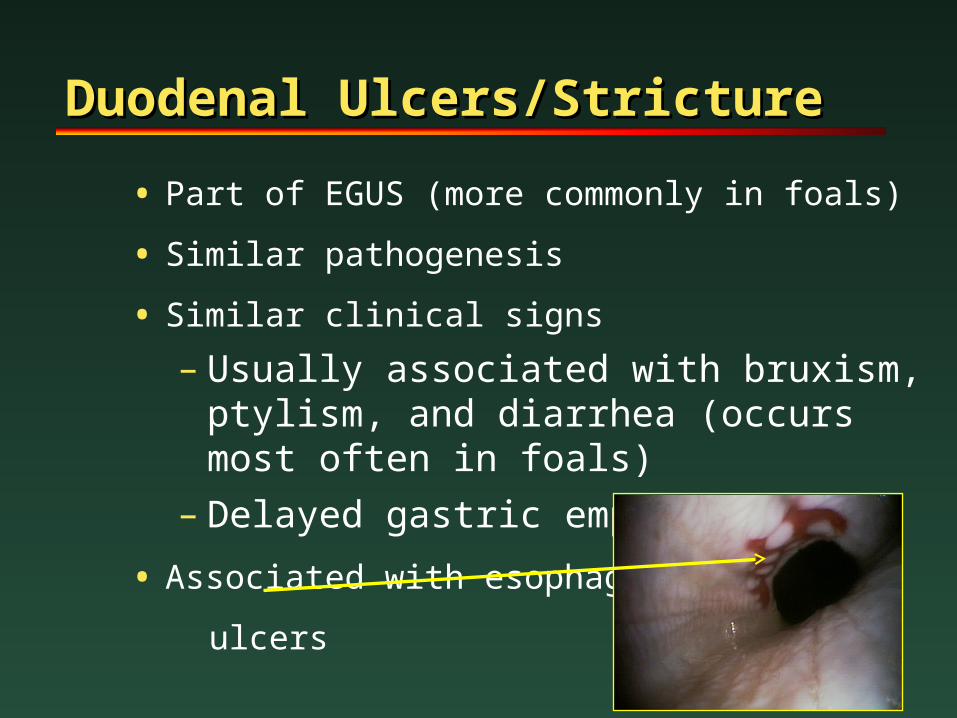
Duodenal Ulcers/StrictureDuodenal Ulcers/Stricture
• Part of EGUS (more commonly in foals)
• Similar pathogenesis
• Similar clinical signs
– Usually associated with bruxism, ptylism, and diarrhea (occurs most often in foals)
– Delayed gastric emptying
• Associated with esophageal
ulcers
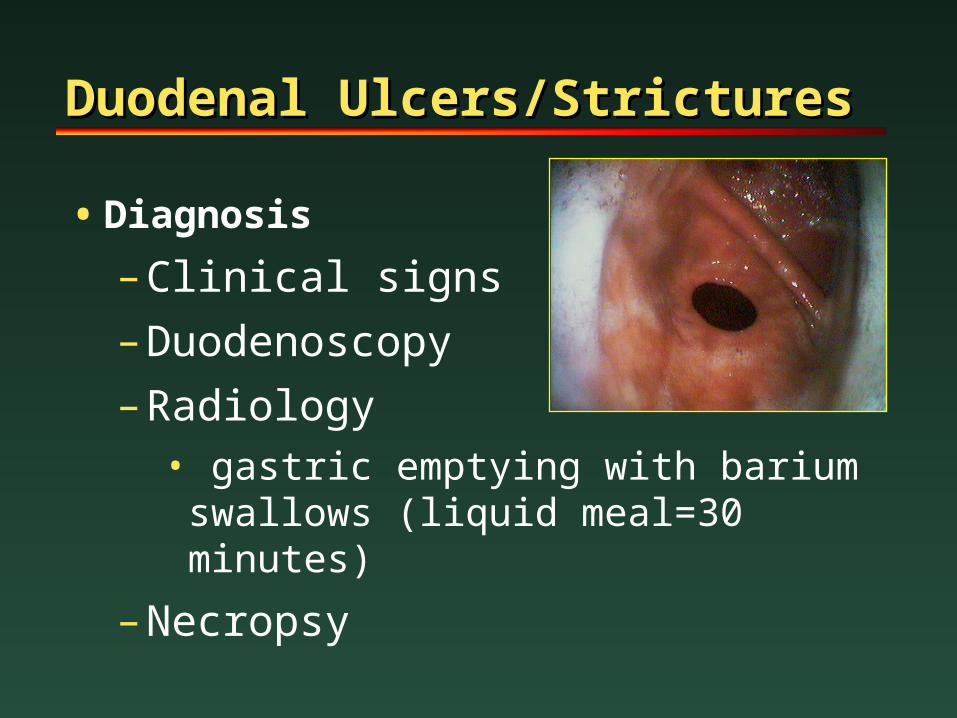
Duodenal Ulcers/StricturesDuodenal Ulcers/Strictures
• Diagnosis
– Clinical signs
– Duodenoscopy
– Radiology• gastric emptying with barium swallows
(liquid meal=30 minutes)
– Necropsy
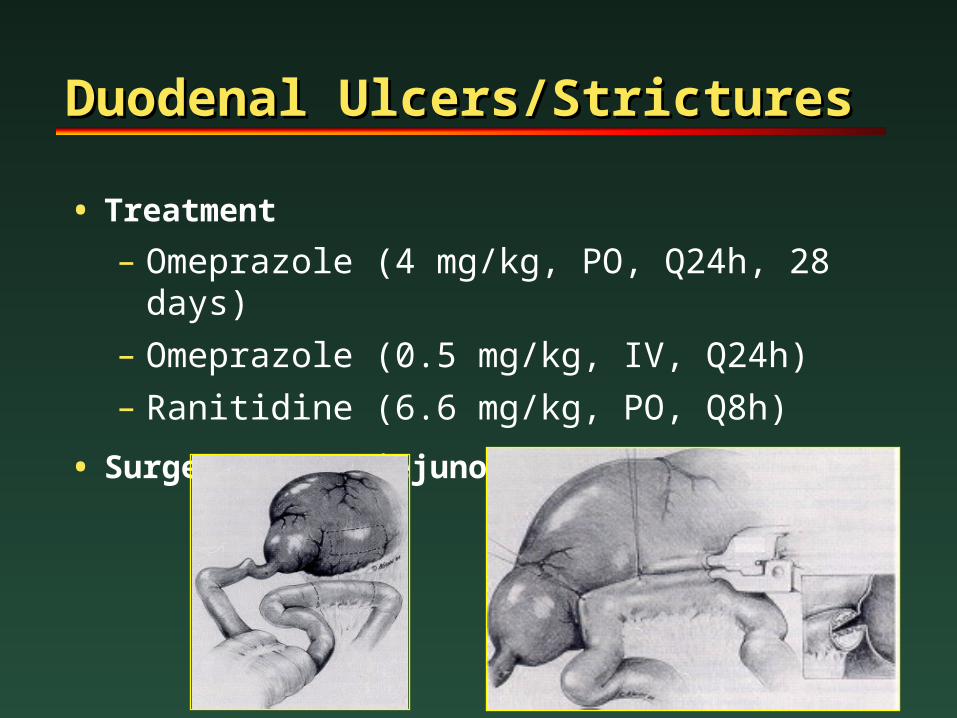
Duodenal Ulcers/StricturesDuodenal Ulcers/Strictures
• Treatment
– Omeprazole (4 mg/kg, PO, Q24h, 28 days)
– Omeprazole (0.5 mg/kg, IV, Q24h)
– Ranitidine (6.6 mg/kg, PO, Q8h)
• Surgery-Gastrojejunostomy (foals only?)
Gastric NeoplasiaGastric Neoplasia
• Uncommon in older horses
• Squamous cell carcinoma, most common
– Others: lymphosarcoma, adenosarcoma
• Arises from squamous mucosa and metastasizes to the abdominal cavity and viscera and/or extends up the esophagus
• Clinical signs:
– Chronic weight loss
– Anemia
– Naso-gastric reflux
– Colic
Gastric NeoplasiaGastric Neoplasia
• Diagnosis
– Clinical Signs
– Endoscopy (definitive)
– Abdominal ultrasound
– Necropsy
• Treatment: None
• Prognosis: Grave
Gastric ImpactionGastric Impaction
• Infrequent cause of Colic in horses
• Dry feed material and decreased water intake
• May occur during winter when dry hay is fed and water intake is lower
• Diagnosed at surgery in horses with colic
• Endoscopic examination
• Treatment with dioctyl sodium succinate (DSS)
– 5% solution via NG tube in 4 to 6 L fluid
• Lavage at surgery, resolve in 24 – 48 hours















![WELCOME [] · Dr. Doug Walker MBA, PhD – Associate Professor – Department of Marketing Kansas State University Dr. William Whitehouse DVM, DACVIM (SAIM) - Assistant Professor,](https://img.pdfslide.net/doc/110x75/5f0c67a97e708231d4353c72/welcome-dr-doug-walker-mba-phd-a-associate-professor-a-department-of-marketing.jpg)












