Embed Size (px)
Citation preview

Interesting Casesfrom
Liver Tumor Board
Jeffrey C. Weinreb, M.D.,FACRYale University School of Medicine

Common Liver Diseases
HemangiomaCystFNH
Focal Fat/SparingTHID
Non-Cirrhotic Cirrhotic
FibrosisRNDN
HCCCholangioca
Adenoma Metastasis
HemangiomaCystFNH
Focal Fat/SparingTHID
Non-Cirrhotic

Nonalcoholic Fatty Liver Disease(NAFLD)
• Pathology resembles alcohol-induced liver injury• Wide spectrum from simple steatosis, to
steatohepatitis (NASH, CASH), advanced fibrosis, cirrhosis, and end-stage liver disease
• Frequently associated with obesity, type 2 diabetes, and hyperlipidemia
• Usually asymptomatic, but may have fatigue, malaise and sensation of discomfort
• Most common cause of abnormal LFTs among adults in USA

Diffuse Fatty Liver• Pathology
– Triglyceride accumulation within hepatocytes
• CT– Attenuation of liver is at least 10HU
less that spleen or <40HU (on non-CE scans)
– Intrahepatic vessels may appear hyperattenuating c/w liver
• MR– SI loss on opposed-phase images
c/w in-phase images

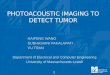
Focal Fat Deposition• May be round, geographic, or
perivascular• Characteristic locations
– adjacent to falciform lig or ligamentumvenosum, in the porta hepatis, and in the GB fossa.
• Absence of mass effect on vessels and other structures
• Poorly delineated margins• Contrast enhancement similar to or
less than normal liver
Radiology 2005;237:159-169
45 yo f with abdominal pain and daily alcohol consumption
Perivascular Fat Deposition
Opposed-phaseIn-phase
CT
MR

CT MR
– Fibrosis– Nodular regeneration– Disturbed blood flow
– Fibrosis– Nodular regeneration– Disturbed blood flow
Cirrhosis

Pseudocirrhosis• Clinical
– In some patients receiving chemotherapy, a morphologic pattern develops similar to that associated with cirrhosis.
– Most common with breast cancer, but occurs with other cancers and lymphoma
– May occur with hepatotoxic drugs without liver metastases – may be asymptomatic or may cause portal hypertension from
venous compression
• Pathology – Findings are suggestive of nodular regenerative hyperplasia
which is characterized by the formation of regenerative hepatic nodules with compression and atrophy of parenchyma but without hepatic fibrosis.
– There may or may not be foci of residual tumor. – It is thought to be a chemotherapeutic response due to
shrinkage of tumor with subsequent scarring and nodular regeneration of uninvolved areas
• Imaging– A lobular hepatic contour, segmental volume loss, and
enlargement of the caudate lobe.– Findings evolve over 1-3 months
AJR 1994; 163:1385-1388
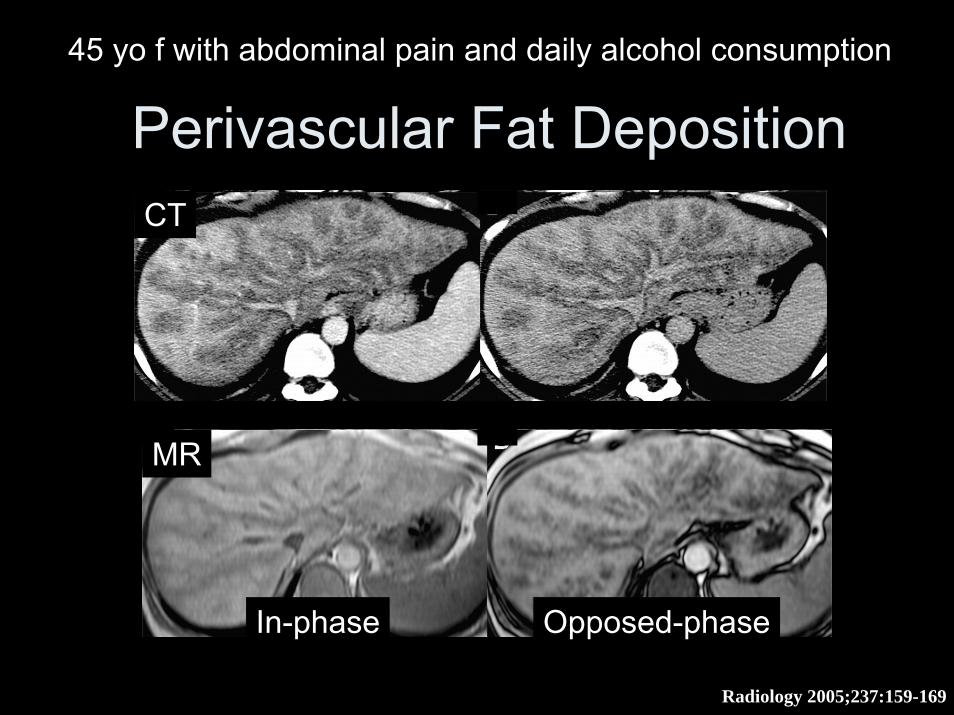
Cavernous Hemangioma
• Clinical– Common; 7-20% of adults; female
5:1• MRI
– Very bright on T2WIs–– Enhancing nodules that become Enhancing nodules that become
more numerous and confluent over more numerous and confluent over time intensity time intensity
–– Follows blood pool on Follows blood pool on allall phasesphases–– May not fill inMay not fill in

Peliosis Hepatis• Pathology
– Rare benign disorder causing sinusoidal dilatation & presence of multiple blood filled lacunar spaces
– Usually a path (not imaging) diagnosis• Clinical
– Associated with chronic wasting diseases,steroid medications, sprue, diabetes, vasculitis, hematological disorders
– Bacillary peliosis hepatis caused by Bartonella species in HIV-positive patients
– Complications: Liver failure/cholestasis/portal hypertension/liver rupture leading to shock

Peliosis Hepatis– CT Findings– NECT
• Multiple hepatic areas of low attenuation • CT findings differ with size of lesions, presence or absence of
thrombus within cavity & presence of hemorrhage – CECT
• Larger cavities communicating with sinusoids have same attenuation as blood vessels
• Thrombosed cavities will have same appearance as nonenhancing nodules
• Arterial phase: Early globular vessel-like enhancement – Multiple small accumulations of contrast, hyperdense in
center or periphery of lesion • Portal phase: Centrifugal or centripetal enhancement without
mass effect on hepatic vessels • Delayed phase: Late diffuse homogenous hyperattenuation
characteristic of phlebectatic type

Peliosis Hepatis• MR Findings
– T1WI • Hypointense• ↑ Signal due to presence of subacute blood
suggestive of hemorrhagic necrosis – T2WI
• Hyperintense• Multiple foci of ↑ signal due to presence of
subacute blood – Post-C
• Lesions usually show contrast-enhancement • Cystic cavity with enhancing rim representing
hematoma • Strong contrast-enhancement with "branching"
appearance caused by vascular component

Focal Nodular Hyperplasia (FNH)• Clinical
– Common; 2-5% of adults; female 4:1– Mostly young women with incidental mass– No malignant potential
• MRI– Looks almost like normal liver on non-c scans– 13% multiple– May be lobulated or have pseudocapsule (no true capsule)– Never bleed, no Ca++– Rarely contain lipid– Scar hypo on T1 and hyper on T2– Homogenously intensely enhances on HAP– Homogenously washes out rapidly– Delayed enhancement of scar– Only approx 20% have “classic” features– Persistant hyperintensity on delayed scans with Gd-BOPTA

Fibrolamellar Carcinoma (FLC)• Pathology
– Diffuse fibrous stroma comprising fibrolamellar bands of collagen and fibrocytes arranged in a lamellar pattern and in delicate bands between nests of tumor cells
• Clinical – Uncommon– Primarily young adult (mean age 28)– Not associated with hepatitis B virus, cirrhosis or
metabolic abnormalities– Usually normal serum markers – Better prognosis than classic HCC; 5 year survival is
60%• Imaging Findings
– Heterogeneously-enhancing, large, lobulated mass with hypointense central scar and radial septa on T2WI
• Size: Vary from 5-20 cm (mean 13 cm) – Compared with FNH, FLC is bigger and more
heterogeneous, frequently with calcified (68%) central/eccentric scar & features of malignancy (vessel/biliary obstruction, nodal & lung metastases)

Hepatic MassesFNH FLC
Prevalence common rareBlood Products never rareCa++ rare commonFat unusual neverCentral Scar common commonLate Enhanced Scar common someHomogen Art Phase common neverHomogen PV Phase common never

Ciliated Hepatic Foregut Cyst• Pathology
– Derives from embryologic foregut– Solitary, unilocular cyst made up of ciliated
pseudostratified columnar epithelaium, a subepithelial layer of connective tissue layer, a smooth muscle layer, and an outer fibrous capsule
• Clinical– Rare. – Typically appears in 50 yo patients with male
predominance – Can show malignant transformation (extremely
rare)– Since it is the only cililated cyst that occurs in the
liver, FNA is diagnostic• Imaging
– Usually located in subcapsular location on the anterior aspect of the liver at the insertion of the falciform ligament (medial seg left lobe)
– May calcifyPathology Oncology Research 2002;8(4):278-279BMC Cancer 2006, 6:244Radiology 1990;175:475-477