Embed Size (px)
Citation preview

Review Series
MYELOPROLIFERATIVE NEOPLASMS
Genetic basis and molecular pathophysiology of classicalmyeloproliferative neoplasmsWilliam Vainchenker1-3 and Robert Kralovics4
1Unite Mixte de Recherche (UMR) 1170, INSERM, Villejuif, France; 2Gustave Roussy, Villejuif, France; 3Universite Paris-Saclay, UMR 1170, Villejuif,
France; and 4Research Center for Molecular Medicine of the Austrian Academy of Sciences, Vienna, Austria
The genetic landscapeofclassicalmyelopro-
liferative neoplasm (MPN) is in large part
elucidated. The MPN-restricted driver muta-
tions, including those in JAK2, calreticulin
(CALR), and myeloproliferative leukemia vi-
rus (MPL), abnormally activate the cytokine
receptor/JAK2 pathway and their down-
streameffectors,moreparticularlytheSTATs.
The most frequent mutation, JAK2V617F,
activates the 3 main myeloid cytokine recep-
tors (erythropoietin receptor, granulocyte
colony-stimulating factor receptor, and MPL)
whereas CALR or MPL mutants are re-
stricted to MPL activation. This explains why
JAK2V617F is associated with polycythemia
vera, essential thrombocythemia (ET), and
primarymyelofibrosis (PMF)whereasCALR
andMPLmutants are found in ET and PMF.
Other mutations in genes involved in epige-
netic regulation, splicing, and signaling co-
operatewith the3MPNdriversandplayakey
role in the PMF pathogenesis. Mutations in
epigenetic regulatorsTET2andDNMT3Aare
involved in disease initiation and may pre-
cede the acquisition of JAK2V617F. Other
mutations in epigenetic regulators such as
EZH2 and ASXL1 also play a role in disease
initiation and disease progression. Muta-
tions in the splicing machinery are predom-
inantlyfoundinPMFandareimplicatedinthe
development of anemia or pancytopenia.
Both heterogeneity of classical MPNs and
prognosis are determined by a specific
genomic landscape, that is, type of MPN
driver mutations, association with other
mutations, and their order of acquisition.
However, factors other than somatic mu-
tations play an important role in disease
initiation as well as disease progression
such as germ line predisposition, inflam-
mation, and aging. Delineation of these
environmental factors will be important to
better understand the precise pathogene-
sis of MPN. (Blood. 2017;129(6):667-679)
Introduction
The classical myeloproliferative neoplasms (MPNs), also called BCR-ABL2 MPNs, are the most frequent diseases among the myeloprolif-erative disorders. MPNs are characterized by excessive production ofterminally differentiated blood cells that are fully functional. ClassicalMPNs have been classified into 3 entities: polycythemia vera (PV),essential thrombocythemia (ET), and primary myelofibrosis (PMF),which have frequent disease-related complications, such as venous andarterial thrombosis, hemorrhages, and transformation to acute myeloidleukemia (AML).1 All MPN entities arise from a single somaticallymutated hematopoietic stem cell (HSC) that clonally expands and givesrise to virtually all myeloid cells, and B and natural killer (NK) cells.The clonal expansion of the MPN HSC is accompanied by single ormultilineage hyperplasia. PV is characterized not only by an excessof erythrocytes and predominant erythroid lineage involvement, butis also associated with a variable hyperplasia of the megakaryocytic/granulocytic lineages. ET is characterized by an increased platelet countwith a megakaryocytic hyperplasia, whereas PMF is a more heteroge-neous disorder both by its clinical and biological characteristics, definedby the presence of bone marrow fibrosis (excess of collagen fibers)and megakaryocytic hyperplasia. Myeloproliferation in PMF initiallypredominates in the bone marrow and later expands to extramedullarysites, such as the spleen.Although the clinical presentations of the3MPNentities are different in their typical forms, establishment of precisediagnosis at disease onset is often challenging. This is reflected by the2016 revision of the World Health Organization (WHO) diagnosticcriteria for MPN.2 In many cases, a continuum between these disease
subtypes can be observed, as documented by the progression of ET andPV to secondary myelofibrosis (MF). Furthermore, boundaries betweenthese 3 disorders cannot be well established, especially between ET andPMF. Thus, transitional entities may emerge describing disease statessuch as prefibrotic PMF (or early PMF) that displays an ET phenotype atdiagnosiswith typical bonemarrowhistology, butwith ahighprobabilityof progression to MF and worse prognosis than true ET.3
Somaticmutations are responsible for clonal expansionofHSCsnotonly in MPNs, but also in most types of myeloid malignancies. High-resolution genome analysis using microarray and next-generationsequencing (NGS) resulted in the discovery of several gene mutationsacross all myeloid malignancies. Only relatively few of these genemutations are found associated with a single or limited number ofdisease entities. Therefore, we classify these mutations into those thatare “restricted toMPN” and those that are “nonrestricted” and are foundalso in other myeloid malignancies (Table 1).
Mutations restricted to MPNs and their role inthe MPN pathogenesis
JAK2 gene mutations
Before 2005, the molecular pathogenesis of the BCR-ABL12 classicalMPNswas unknown. In 2005, amajor breakthroughwas the discovery
Submitted 15 October 2016; accepted 6 December 2016. Prepublished online
as Blood First Edition paper, 27 December 2016; DOI 10.1182/blood-2016-10-
695940.
© 2017 by The American Society of Hematology
BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6 667
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

Table 1. Somatic mutations in MPN
Gene functionand symbol Location Type of mutations Protein function Frequency Consequences Reference
Signaling MPN
driver
JAK2 9p24 JAK2V617F Tyrosine kinase associated with
cytokine receptors
95% PV, 50%-60% PMF and ET Increased RBC, platelet, and
granulocyte production
4-7
JAK2 exon 12 3% PV Increased RBC 17
MPL 1p34 MPL515L/K/A/R
MPLS505N
TPOR 2%-3% ET Increased platelet production 19, 22, 23
Other missense
mutations
3-5% PMF 25
CALR 19p13 Indel exon 9 Mutant: activator of MPL 20%-25% ET, 25%-30% PMF Increased platelet production 28, 29
Other signaling
LNK 12q24 Missense (loss of
function) deletion
Negative regulator of JAK2 1% ET, 2% PMF Synergy with JAK2V617F-
Disease progression
35
CBL 11q23;3 Missense (loss of
function)
Cytokine receptor internalization 4% PMF Disease progression
(progression to AML)
110
NRAS 1p13.2 Missense (activation) ERK/MAPK signaling Rare PMF Progression to leukemia (5%-
10% in secondary AML)
65
NF1 17q11 Missense deletion ERK/MAPK signaling Rare PMF Progression to leukemia (5%-
10% in secondary AML)
66
FLT3 13q12 FLT3-ITD Cytokine receptor (FLT3-L) MPN (,3%) Progression to leukemia (10%-
15% in secondary AML)
100
DNA methylation
TET2 4q24 Missense, nonsense
deletion
a-Ketoglutarate–dependent
dioxygenase
10%-20% MPN (ET, PV, and
PMF)
Initiation, 70
Oxidation of 5mC into 5hmC and
active 5mC demethylation
Mutations on 2 alleles
associated with progression
DNMT3A 2p23 Missense, hotspot DNA methylase, de novo
methylation
5%-10% MPN (ET, PV, and
PMF)
Initiation 74
IDH1 2q33.3 Missense, hotspot Neomorphic enzyme, generation
of 2-hydroxyglutarate blocking
a-ketoglutarate–dependent
enzymes
1%-3% PMF Initiation, Disease progression 111
IDH2 15q26.1 Missense, hotspot Neomorphic enzyme, generation
of 2-hydroxyglutarate blocking
a-ketoglutarate–dependent
enzymes
1%-3% PMF Initiation, Disease progression 111
Histone
modifications
EZH2 7q35-36 Missense, indel H3K27 methyltransferase, loss
of function
5%-10% PMF Initiation 82, 83
Disease progression
ASXL1 20q11 Nonsense/ indel Chromatin-binding protein
associated with PRC1 and 2
25% PMF Initiation 69
1%-3% ET/PV Rapid progression
Transcription
factors
TP53 17p13.1 Missense/ indel Transcription factor regulating
cell cycle, DNA repair and
apoptosis
,5% (20% of sAML) Progression to leukemia
(mutations on both alleles)
complex karyotype
98
CUX1 7q22 Deletion 7p Transcription factor regulating
TP53 and ATM
,3% Progression to leukemia 112
IKZF1 7p12.2 Deletion 7p, indel Master transcription factor in
lymphopoiesis
,3% Progression to leukemia 112
ETV6 12p13 Missense/ indel Transcription factor of the ETs
family
,3% Progression to leukemia 112
RUNX1 21q22.3 Nonsense/ missense/
indel
Master transcription factor in
hematopoiesis
,3% (10% of sAML) Progression to leukemia 112
RNA splicing
SRSF2 17q25.1 Missense, hotspot Serine/arginine-rich pre- RNA
splicing factor
,2% ET 10%-15% PMF
(association with IDH
mutations)
Initiation? Progression 94
SF3B1 2q33.1 Missense RNA-splicing factor 3b subunit
1, part of U2
,3% ET Phenotypic change (anemia) 113
U2AF1 21q22.3 Missense U2 small nuclear RNA-splicing
factor
10%-15% PMF Phenotypic change (anemia) 94
ATM, ataxia-telangiectasia mutated; RBC, red blood cell; sAML, secondary AML.
668 VAINCHENKER and KRALOVICS BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

of a G to T somatic mutation at nucleotide 1849, in exon 14 of JAK2,resulting in the substitution of valine to phenylalanine at codon617 (JAK2V617F) in the pseudokinase domain.4-7 This mutation canbe found in around 70% of MPNs: 95% of PV and 50% to 60% of ETand PMF. The JAK2V617F mutation often undergoes a transitionfrom heterozygosity to homozygosity due to occurrence of mitoticrecombination resulting in copy-neutral loss of heterozygosity along avariable size region on the short armof chromosome9 (9pLOH).5,8 TheJAK2V617Fmutation arises in amultipotent hematopoietic progenitor,is present in all myeloid lineages, and can be also detected in lymphoidcells, mainly B and NK cells and more rarely and later in disease inT cells. It is absent in nonhematopoietic cells although it has been foundin endothelial cells of the spleen andof splanchnic veins of patientswithMF and/or splanchnic thrombosis as the Budd-Chiari syndrome.9 Thevariant allele frequency (VAF) ingranulocytes is highlyvariable,with acontinuum between the threshold of detection (around 1%) to 100%.TheVAF is usually low inET (around25%), is higher inPV (frequentlyover 50%), and is close to 100% inpost-PVorpost-ETMF. InPMF, theVAF is variable, but frequently high.10 The JAK2V617F is mainlyrestricted to classical MPNs with the exception of refractory anemiawith ring sideroblasts and thrombocytosis (RARS-T).11 It can rarely befound in some other malignant hemopathies.12 However, JAK2V617Fhas been detected at very low level (lower than 1%) in the normalpopulation, including in a neonate.13-15 It is 1 of the most frequentmutations found in the clonal hematopoiesis associated with aging(clonal hematopoiesis of indeterminate potential).16
JAK2 exon 12 mutations have been also found in MPNs and arepresent in the majority of JAK2V617F2 PV.17 They are not usuallyassociated with ET and PMF, but JAK2 exon 12mutation can progressto secondary MF.18 Several mutations have been described, most ofthem being in-frame small insertions and deletions. Exon 12 JAK2mutations are all located in the linker between the Src homology 2
(SH2) and the pseudokinase domains, a region between amino acids536 and 547, around Lys 539. The most frequent mutations being theN542-E543del (23%), E543-D544del (11%), and F537-K539delinsLand K539L (10%), respectively. The VAF in granulocytes can be lowand their detection may require specific techniques.
Thrombopoietin receptor gene (MPL) mutations
Two main types of myeloproliferative leukemia virus (MPL; thethrombopoietin [TPO] receptor [TPOR]) mutations located in exon10 have been associated with MPNs. The most frequent are mutationson the tryptophanW515 located at the boundary of the transmembraneand the cytosolic domains of MPL, the most prominent mutationsbeingMPLW515L andK.19 However, several other substitutions havebeen described such as W515R, W515A, and W515G.20 Mutationsare usually heterozygous, but can be homozygous during diseaseprogression.21 Mutations on MPLW515 are restricted to ET (around3%) and PMF (around 5%) and can be also found in RARS-T.22-24 Theother mutation, MPLS505N, is even rarer and is located in the trans-membrane domain, stabilizing receptors in active dimeric orienta-tions. Originally, this mutation was described in hereditary formof thrombocytosis as a germ line mutation.25 Later on, acquiredMPLS505N somaticmutations were described in ET in,1%of thecases.22,23 This underscores the similarities in mechanisms ofthrombocytosis between hereditary thrombocytosis and ET. Morerecently, a number of “noncanonical”mutations ofMPLwere found intriple-negative ET (ET negative for JAK2V617F, calreticulin [CALR]mutations, andMPLW515L/K /MPLS505N).Thesemutations are rareand lead to amino acid changes either in the extracellular (S204 orE230) or in the intracellular (Y591) domains.26,27 These noncanonicalmutations are more often acquired and lead to a trueMPN. In addition,germ line noncanonical mutations of MPL can also be detected,
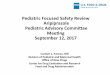
Figure 1. Role of cytokine receptors in the
oncogenic properties of JAK2V617F and CALR
mutants. (A) JAK2V617F activates signaling
through the 3 main homodimeric receptors EPOR,
MPL, and G-CSFR, which are involved in erythro-
cytosis, thrombocytosis, and neutrophilia, respec-
tively. (B) The CALR mutants mainly activate MPL
and at a low level the G-CSFR but not the EPOR,
explaining the thrombocytosis associated with
these mutants. Professional illustration by Som-
ersault18:24.
BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6 SOMATIC MUTATIONS AND MPNs 669
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

strongly suggesting that these triple-negative ET cases are in facthereditary thrombocytosis.
Mutations in the calreticulin gene: CALR
At the end of 2013, frameshift mutations in the CALR gene werediscovered in the majority of JAK22 and MPL2 ET and PMF (50%-60%ET and 75% PMF).28,29 There are.50mutations now described,but all are located in exon 9 inducing a11 (2112) frameshift. At thetime of writing, only the mutations leading to this 11 frameshift areknown to be pathogenic. The other nonpathogenic mutations areusually germ line variants of CALR. Specific shifting of the readingframe leads to a new C terminus devoid of the KDELmotif, importantfor the protein retention in the endoplasmic reticulum (ER). Themutated CALR protein contains a common new amino acid sequencethat bears positive charges. In contrast to wild-type (WT) CALR, thenegative charges required for calcium binding are lost at differentextents, depending on the mutant. The 2 most frequent mutationscorrespond to a 52-bp deletion (p.L367fs*46), also called type 1 and a5-bp insertion (p.K385fs*47), also called type 2. They represent nearlythe 2 extremes of modifications observed in exon 9: the del52 havinglost most of the WT exon 9 sequence and calcium-binding sites, andins5 being closer to the WT sequence having kept around 50% ofnegative charges. According to these structural changes, the othermutations have been classified as type 1–like and type 2–like usingalgorithms based on the preservation of an a helix close to WT intype 2–like mutation.30 There are great differences in the frequencybetween type 1 and type 2mutations in ET and PMF: in ET, type 1 andtype 2 mutations are closely distributed (55% vs 35%), whereas inPMF, type 1 are largely predominant (75% vs 15%).31 The presence ofCALRmutants in exceptional cases of PV has been reported, but theirrole in the pathogenesis of the PV remains unclear.32
CALRmutations are usually heterozygous although a few cases ofhomozygous mutations have been observed, more particularly fortype 2 mutations.28,29 Interestingly, homozygous CALRmutations areassociated with a defect in myeloperoxidase accumulation in primarygranules of granulocytes, and thus, can be suspected in an ET when a“myeloperoxidase deficiency” is detected by using a flow cytometer–based hematology analyzer.33
In contrast to JAK2V617F, theVAF formutantCALR in ET is high,on average around 40%.10 In rare cases of ET, the VAF can be lower,but almost never below 15%. This implies that CALR mutants mightgive a stronger clonal advantage when compared with JAK2V617F.Themolecular diagnosis is rendered easier by this highVAF and can beperformed by numerous techniques and routinely by sizing fluores-cently labeledpolymerase chain reaction products of exon9ofCALR.28
A few CALR polymorphisms have been detected not only as single-nucleotide polymorphisms, but also in phase deletions of exon 9.34
There is presently no evidence that these variants have any role inpathogenesis.
LNK mutations
In 2010, somatic mutations in exon 2 of LNK (SH2B3), an adaptorprotein which regulates JAK2 activation, were detected in 2 patients(PMF and ET).35 These mutations had a functional impact onproliferation and were considered as the driver of the disease. Recentstudies have questioned the role of LNK as a true driver of thedisease.36 LNK mutations have been found in many different typesof hemopathies, more particularly in erythrocytosis.37 Some ofthese mutations can be germ line, including the initially describedLNKE208Q; some others are secondary somatic mutations associatedwith JAK2V617F orCALRmutations, more particularly during diseaseprogression.38Thus, rather than primary drivers,LNKmutations appear
Figure 2. The CALR mutants bind and activate
MPL. (A) WT CALR binds to MPL in the ER
by interaction of its lectin domain with MPL
N-glycosylation, controls the quality of the proteins,
and then comes away from the receptor, which
traffics to the cell surface mainly by the conven-
tional route to the cell surface. A completely
glycosylated MPL (mature form) is expressed at
the cell surface where it binds TPO to be activated.
CALR mutants bind to MPL in the ER by the same
interaction as the WT but the interaction is re-
inforced by the new C terminus. (B) The mutant
CALR remains bound to MPL and probably traffics
to the membrane both conventionally and un-
conventionally (autophagosomes and pre-Golgi)
to the membrane. This leads to the presence of
an immature MPL form on which the mutant CALR
is bound. Activation of MPL is dependent on the
new C terminus and also takes place on the
membrane (Stefan Constantinescu, W.V., unpub-
lished results). In cell lines, this leads to activation
of mainly the STAT pathway whereas the extra-
cellular signal-regulated kinase (ERK) is slightly
activated and the PI3K pathway even less. In cell
lines, MPL that binds mutant CALR can only be
slightly activated by TPO. Professional illustration
by Somersault18:24.
670 VAINCHENKER and KRALOVICS BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

more as predisposition mutations when germ line or secondarymutations, increasing the pathogenicity of JAK2V617F and CALRwhen acquired.36
MPN-restricted mutations activate JAK2kinase–dependent cytokine receptorpathways
JAK2 is a member of the JAK family characterized by 2 kinasedomains: 1 catalytically active at the C terminus and 1 catalyticallyinactive (or veryweak) pseudokinase that prevents self-activationof thekinase domain.39 At the N terminus, JAKs possess a four-point-oneezrin radixinmoesin (FERM)-like domain and a SH2-like domain. The
noncovalent attachment of JAKs to cytokine receptors depends onthe FERM domain. The JAK family kinases can be considered asthe catalytic part of the hematopoietic cytokine receptor family as theyare constitutively bound to the receptors intracellularly. In addition,the association of JAKs with receptors is important for their pro-per trafficking to the cell surface. Homodimeric receptors such aserythropoietin (EPO) receptor (EPOR),MPL, and granulocyte colony-stimulating factor receptor (G-CSFR) use JAK2, whereas heteromericreceptors use JAK1 and JAK2/tyrosine kinase 2 (TYK2) or JAK3.Cytokine binding induces changes in the conformation of receptors,whichactivate the JAKsbound to the receptorby trans-phosphorylation.The activated JAKs will phosphorylate the receptors, which aresubsequently used as a docking site for other signaling molecules,more particularly the STATs. In the canonical pathway, STATs arephosphorylated by the JAKs, which induce their homodimerization
Table 2. Mouse models
Mouse models Phenotype Reference
JAK2V617F
Retrovirus
C57Bl/6 PV progressing to MF 114-116
BALB/c Severe lethal PV to MF 115, 116
Transgenic
Vav huJAK2V617F ET/PV progressing to MF 117
H2K muJak2V617F ET/PV progressing to MF 118
Inducible JAK2min promoter huJAK2V617F
Vav Cre ET 57
Mx Cre PV with thrombocytosis 57
Pf4Cre (MK specific) No phenotype 119
Mild ET and a PV after transplantation 120
Tie2Cre (HSC and endothelial cell) ET with neutrophilia progressing to osteopetrosis
with bleeding diathesis
119
Knock-in
Constitutive muJak2V617F PV with thrombocytosis progressing to MF 121
Germ line induction of muJAK2V617F PV progressing to MF 55
E2Acre
Germ line induction of huJAK2V617F (cDNA)
Stella Cre
Heterozygous Mild ET 122
Homozygous PV 122
muJAK2V617F
Mx Cre
Heterozygous ET/PV progressing to MF 123
Homozygous Severe PV progressing to MF 123
EpoR Cre (erythroid specific)
Heterozygous Mild erythrocytosis 124
Homozygous Erythrocytosis 124
muJAK2V617F heterozygous
Vav Cre ET progressing to PV progressing to MF 56
Scl Cre PV progressing to MF 125
huJAK2V617F (cDNA) heterozygous Mild ET progressing in PV (10% cases) 58
Mx Cre
CALR
Retrovirus
CALRdel52 Mild ET, ET progressing to MF 50,51
CALRins5 Mild ET 51
Transgenic
H-2Kb promoter ET 126
Knock-in
Constitutive muCALRdel 61 ET 60
Inducible humanized CALRdel52 Caroline Marty, Isabelle Plo, Harini Nivarthi, R.K.,
W.V., unpublished resultsVav Cre ET (short-term follow-up)
SCL CreER ET (short-term follow-up
cDNA, complementary DNA.
BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6 SOMATIC MUTATIONS AND MPNs 671
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

or heterodimerization and subsequent trafficking to the nucleuswhere they regulate transcription of their target genes (Figure 1).The pseudokinase domainof JAK2has2 roles: 1 is to inhibit the kinasedomain and the other is to promote cytokine-dependent activation.V617F activates JAK2 by a mechanism, which is not completelyunderstood, but both structural and functional data have establishedthat the first conformational change induced by V617F involvesthe helix C of the pseudokinase domain.40,41 Mutations in exon 12are located upstream of the pseudokinase domain, and the mecha-nism of activation appears different than that for JAK2V617F.42
JAK2V617F or JAK2 exon 12 mutations, when expressed ininterleukin-3 (IL-3)-dependent cell lines, induce cytokine hypersen-sitivity or cytokine independence. The presence of homodimericreceptors such as EPOR greatly facilitates this biological effect.43
The presence of a cytokine receptor is absolutely required to inducesignaling by JAK2V617F at low expression levels. JAK2V617Finduces constitutive activation of STATs, and of the phosphatidy-linositol 3-kinase (PI3K) and MAPK pathways. This cytokinehypersensitivity or independence induced by JAK2V617F in celllines mimics the EPO hypersensitivity or independence previouslydescribed in PV erythroid progenitors.4,44 In addition to this acti-vation of the canonical pathway of cytokine receptors, 2 reports havedescribed that JAK2V617F acts on chromatin by phosphorylatingH3Y41, decreasing the binding of heterochromatin protein 1a andPRMT5, impairing its ability tomethylate histone substrates.45,46 It isunknown whether these effects on chromatin are really important inthe pathogenesis of MPNs.
Activation of MPL by TPO induces the activation of JAK2 andTYK2, which are constitutively bound to the receptor, but onlythe activation of JAK2 is indispensable for signaling and inductionof proliferation by MPL. MPLW515 is located in the amphipathic
domain ofMPL, which prevents spontaneous activation ofMPL.47 Allsubstitutions of W515, except W515C and W515P, will lead to theactivation of MPL in the absence of TPO and will activate JAK2. TheS505Nmutation induces a stable active dimer. However, both types ofmutations activate constitutive signaling through induction of pro-ductive dimerization of the transmembrane helix of MPL.20,25
CALR in contrast is not a signaling molecule, but an ER chaperoneinvolved in the quality control of N-glycosylated proteins and incalcium storage. The initial publication onCALRmutations has shownthat CALRdel52 was able to activate STAT5 and this was impeded byJAK2 inhibition.28 Recent studies have established that CALRmutantscan activate MPL and subsequently JAK248-52 (Figure 2). MutantCALR requires both its mutant C terminus and MPL for oncogenictransformation.49,50,53 WT CALR and mutant CALR bind to theN-glycosylated residue of the extracellular domain of MPL in the ER,and the lectin-binding activity of CALRmutants as well as the new tailare required forMPL activation49 (Figure 2). This binding is reinforcedby the newC terminus and its positive charges, which lead to activationof the receptor.50,53 It is unknown at which cellular compartment MPLis activated, but there is evidence that CALR mutants behave asan abnormal chaperone and traffics with MPL to the cell surface.47 Inthis case, MPL activation can occur anywhere from the ER to thecell surface. Moreover, CALR mutants are secreted and may inducecytokine secretion by monocytes.54 CALR mutants also appear toslightly activate the G-CSFR, but not the other cytokine receptors.49
Whether this activation of G-CSFR plays a role in the pathogenesis ofmutant CALR1 MPN is unknown (Figure 1).
Overall, the main MPN-associated mutations, JAK2V617F, JAK2exon 12 mutants, MPLW515L/K, and CALR mutants, activate thecytokine/receptor/JAK2 pathways and their downstream signaling,JAK2V617F, through the 3 homodimeric receptors (EPOR, MPL,
Figure 3. MKs play a central role in MPN
pathogenesis. The MPL/JAK2 pathway is acti-
vated by the 3 MPN-restricted mutations (JAK2V617F,
CALR mutants, and MPL mutants) placing MK
hyperplasia and eventually dysplasia as a central
determinant in MPN. MKs are mainly involved in
platelet production, and also play an important role
in the hematopoietic niche by regulating HSCs,
remodeling the marrow by secretion of TGF-b1 and
other cytokines (platelet-derived growth factor
[PDGF], vascular endothelial growth factor [VEGF])
which ultimately lead to MF, and also inducing a
neo-osteogenesis by inducing an osteoblastic dif-
ferentiation through TGF-b1 and inhibiting osteoclast
differentiation through osteoprotegerin. Furthermore,
MKs secrete numerous inflammatory cytokines
such as IL1a. The mechanisms of local activation
of TGF-b1 are poorly known. OPG, osteoprotegerin;
RANK, receptor activator of NF-kB; RANKL, RANK
ligand; TGF, transforming growth factor; TSP,
thrombospondin. Professional illustration by Somer-
sault18:24.
672 VAINCHENKER and KRALOVICS BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

G-CSFR) and CALR mutants through mainly MPL (Figure 1). Thismay explain also why these different mutations are usually mutuallyexclusive. However, rarely, 2 of these mutations can be detected inthe same patient, but usually they are present in different clones orsubclones.
MPN-restricted mutations drive myeloproliferative disorders
and give rise to different diseases in murine models
All 3 MPN mutation types have been expressed in mice to investigatewhether they are drivers of MPNs and to model the disease (Table 2).JAK2V617F has been expressed in mouse hematopoiesis by severalapproaches: retroviral transduction of HSC followed by bone marrowtransplantation, transgenicmice, and constitutive or inducible knock-in(KI) mice. Whatever the model, expression of JAK2V617F inducesa myeloproliferative phenotype with certain differences. The mostfrequent phenotype has been a PV-like disorder progressing toMF.55,56
A correlation between the level of expression and the phenotypehas been found: low expression being associated with an ET-likephenotype and a higher expression (30%of theWTormore)with aPV-like phenotype.57 Further phenotypic variability may be related tothe use of human vs murine JAK2V617F. The heterozygous KI of thehuman JAK2V61F displays a very mild ET phenotype and the ho-mozygous KI induces an erythrocytosis.58 Thus, in mouse models,JAK2V617F is the driver of the myeloproliferative disorder and thelevel of expression ingreat part determines thephenotypeof theMPN, asituation close to the human setting. Recently, JAK2 exon 12 transgenicmice have been obtained that developed isolated erythrocytosis.59
The erythroid phenotype was even more marked than in JAK2V617Ftransgenic mice. This was attributed to important changes in iron
metabolism including decreased expression in hepcidin and increasedexpression in transferrin receptor-1 and erythroferrone that favor ironavailability for erythroblasts.
ForMPLW515K/L/A, only retroviral models have been described.Although these models are far from ideal because they lead to theexpression ofMPLW515 mutant in all types of hematopoietic cells,an ET-like disorder rapidly progressing toMF is usually observed, aphenotype close to the mice expressing a high level of TPO.19
For CALR mutants, retroviral models have been used to inducea myeloproliferative disorder reminiscent of an ET-like pheno-type, which in the case of CALRdel52 may progress to MF. In thismouse model, the presence of MPL is indispensable for diseasedevelopment.50,51 A recent transgenic model for CALRdel52 also ledto an ET-like phenotype that was ameliorated by ruxolitinib, similarresults being obtained in del61 or del52 KI mice60 (Caroline Marty,Isabelle Plo, Harini Nivarthi, W.V., R.K., unpublished results).
In conclusion, the 3MPN oncogenes are true drivers of the diseasephenotype with JAK2 exon 12 giving only an erythrocytosis pheno-type, JAK2V617Fgiving rise toET,PV, andMF,whereasCALRmutantandMPLW515L/K/A are associated with ET and MF, resembling thephenotype observed in patients. The current data sustain the hypothesisthat the phenotype ofMPNs ismostly related to the types of receptorsthat are activated. However, in all models, MPL activation plays acentral role by its role on HSCs and onmegakaryocytes (MKs).19,51,61
MK hyperplasia plays a central role in the pathogenesis of MPNs notonly by increasing platelet production, but also by serving as a nichefor HSCs, by remodeling bone marrow leading to MF and also byinducing neo-osteogenesis (Figure 3). However, in none of themodelsdid mice develop a PMF, whereas they did develop secondary MF(post-ET or post-PV); no leukemic transformation is observed during
Figure 4. Genes involved in epigenetic regula-
tion and leukemic transformation. The mecha-
nisms by which the genes involved in the epigenetic
regulation described in Table 1 lead to modifica-
tions in gene regulation are detailed. Some genes
involved in leukemic transformation (N-Ras path-
way and transcription factors such as p53, RUNX1)
are also described. MEK, MAPK/ERK-kinase; RAF,
rapidly accelerated fibrosarcoma; SOS, Son of
Sevenless; TF, transcription factor. Professional
illustration by Somersault18:24.
BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6 SOMATIC MUTATIONS AND MPNs 673
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

disease progression. The different STATs may play an important rolein disease phenotype: STAT5 being required for the PV development,STAT3 inhibiting the thrombocytosis, and STAT1 increasing thethrombocytosis.62,63
“Nonrestricted” acquired mutations and theirrole in the MPN pathogenesis
The 3 main driver mutations do not explain the entire heterogeneity ofthe classical BCR-ABL2 MPNs. The development of NGS, as well asother whole-genome analysis techniques, allowed the identification ofseveral acquiredmutations inMPNs (Table 1). However, none of thesemutations is restricted to MPNs and they are even more frequent inmyelodysplastic syndromes (MDSs) and AML. This underscores thecontinuum between the different myeloid malignancies, and mostof these mutations are involved in phenotypic changes and diseaseprogression in MPNs.
Mutations identified in myeloid malignancies target DNA methyl-ation regulators (TET2, DNMT3A, IDH1/2), histone modifiers(Polycomb repressor complex 1 and 2members, IDH1/2), transcriptionfactors (TP53, CUX1, IKZF1, FOXP1, ETV6, RUNX1), proteinsinvolved in signaling (NF1, NRAS, KRAS, LNK, CBL, FLT3), andsplicing factors (SF3B1, SRSF2, U2AF1, ZRSR2) (Figure 4).64-66 Asthe majority of the mutations are loss of function and act as dominant-negative or via haploinsufficiency or complete homozygous loss, itseems thatmost of themutated genes aremyeloid tumor suppressors. InMPNs, targeted gene panel sequencing studies identified patients withmultiple gene mutations. Although recurrent single-gene mutationswere identified, individual gene mutations had too low frequency toallow convincing evidence of association with disease progression.However, the number of detected mutations (as an indirect measure ofgenetic complexity or progression of clonal evolution) allowed theidentification of high-risk patients.67
However, in ET and PV, in themajority of cases, only 1mutation ina MPN driver gene is found. In contrast, in the majority of PMF, moresomatic mutations are found (3 mutations or more). Some differencesare observed in the coexpression of mutations along the type ofMPNs.An example obtained by whole-exome sequencing is illustratedin Table 3. However, in several studies using targeted gene panelsequencing studies,mutations in spliceosomegenes appear very rare inPV, in comparisonwithET. Thismaybe due to the continuumbetweenET and RARS-T or prefibrosis/PMF. Similarly, in PMF, there areno major differences with respect to the association of JAK2V617F,and CALR or MPL mutants with the different mutations in epige-netic regulators. On the other hand, spliceosome genes mutations are
extremely rare inCALRPMF in comparisonwith JAK2V617F. Thus,PMF appears not to be a pure MPN, but a mixed myeloproliferative/myelodysplastic syndrome. The presence of mutations in genes otherthan the 3 MPN-restricted driver genes increases the myelodysplasticfeatures of the disease and the severity of the disease, explaining thecontinuity between MPN, MPN/MDS, and MDS (Figure 5).
It is beyond the scope of this review to cover all the recurrent genemutations in detail. Therefore, wewill focus onTET2 andDNMT3A, astheymay represent themost important modifiers of theMPN-restrictedoncogenicmutations, onEZH2whose role has been recently studied indetail, and on addition of sex combs like 1 (ASXL1) and SRSF2, whichare all associated with a poor prognosis in MF.
TET2 and DNMT3A mutations and their role in disease initiation
The TET and DNMT3A protein families play a central role in theregulation ofDNAmethylation at cytosine guanine dinucleotide (CpG)sequences (Figure 4): the DNMT3 protein family is involved in themethylation of cytosines (5mC), whereas the TET protein family inactive demethylation through oxidation of 5mC into 5hmC.68 TET2mutations have been the first mutations, along with ASXL1, to beidentified in JAK2V617F1MPNs.69,70 All TET2mutations are loss-of-function point mutations or deletions, usually on 1 allele, but morerarely on both somatic alleles. TET2 mutations have been identifiedinitially as mutations preceding JAK2V617F and are responsible forclonal dominance.70 Their frequency ranges from10% to 20%and theyare found in all MPN subtypes. For comparison, TET2 mutationsare present in 50% to 60% of chronic myelomonocytic leukemia(CMML).71 TET2 mutations can be also secondary mutations afterJAK2V617F or CALR mutations and induce an expansion of double-mutated stem cells and progenitors.72 It has been suggested that whenTET2mutates first, the subsequent occurrence of JAK2V617F inducesan ET phenotype, in contrast to the situation in which JAK2V617Fmutates first and the phenotype is more likely PV. Secondary TET2mutations can also be associated with progression, more particularlywhen the mutation is homozygous.73
DNMT3A mutations are less frequent than TET2 mutations inMPNs (5%-10%) and in the majority of the cases precede JAK2V617For MPL mutations.74 As in other malignant hemopathies, the R882His the most prevalent DNMT3A mutation. Both TET2 and DNMT3Amutations increase the self-renewal capacities of HSCs in both humansand mice.75,76 The precise mechanism is not completely understood,but TET2 and DNMT3A control the expression of genes involved inHSCproperties aswell as differentiation. It has been recently suggestedthatTET2-deficientHSCs aremore prone to differentiation than normalHSCs, with the derepression of transcription factors such as Klf1.68
TET2 and DNMT3A are the 2 most frequently mutated genesassociated with clonal hematopoiesis during aging.77-79 On the other
Table 3. Co-occurrence of mutations
PV JAK2V617F ET JAK2V617F ET CALRmut ET MPLm PMF JAK2V617F PMF CALRmut PMF MPLm
% (No. of patients)
TET2 8.33 (4) 5.26 (3) 0 (0) 0 (0) 28.95 (11) 2.63 (1) 2.63 (1)
DNMT3A 6.25 (3) 7.02 (4) 0 (0) 3.51 (2) 7.89 (3) 0 (0) 0 (0)
ASXL1 0 (0) 3.51 (2) 0 (0) 1.75 (1) 15.79 (6) 7.89 (3) 0 (0)
IDH1/IDH2 2.08 (1) 1.75 (1) 0 (0) 0 (0) 2.63 (1) 0 (0) 0 (0)
EZH2 2.08 (1) 0 (0) 1.75 (1) 0 (0) 2.63 (1) 2.63 (1) 0 (0)
SF3B1 4.17 (2) 0 (0) 0 (0) 0 (0) 2.63 (1) 0 (0) 0 (0)
U2AF1 0 (0) 0 (0) 0 (0) 0 (0) 7.89 (3) 0 (0) 0 (0)
Results are extracted from Nangalia et al29 because it is one of the rare studies in which all types of MPNs are available. Overall, 143 patients: PV, 43; ET, 57; and PMF,
38. Percentages are expressed for each MPN, irrespective of the MPN drive mutation. Thus, percentages are calculated on a very low number of patients due to the
heterogeneity of the disorder, explaining differences with other studies, more particularly for the mutations in splicing genes.
674 VAINCHENKER and KRALOVICS BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

hand, there is no clear evidence that these mutations induce geneinstability. However, by inducing a clonal hematopoiesis and thusincreasing replication ofmutated stem cells, theymay indirectly inducesecondarymutations. Theymay also favor leukemogenesis by progres-sively modifying the equilibrium between self-renewal and differen-tiation. DNMT3A mutation may predispose to leukemic progressionin MPNs. In mouse models, Tet2 loss increased the competitivereconstitution capacities of Jak2V617F-expressing HSCs and alsoworsened the MPN phenotype with an increase in extramedullaryhematopoiesis without leukemic transformation.80,81
Overall, these 2 types of mutations increase the self-renewal ofJAK2V617F HSCs and play an important role in disease initiation.However, they can also induce disease progression when they occur assecondary mutations, but their role inMF and leukemic transformationremains elusive.
Loss of EZH2 function promotes MF development and
poor prognosis
EZH2 is 1 of the 2 histonemethyltransferases of the PRC2complex andis involved in the repressive H3K27 trimethylation (H3K27m3)(Figure 4). Loss-of-functionmutations and cytogenetic lesions inEZH2and other PRC2members (SUZ12, JARID2,EED) have been describedinMPNs and across all myeloid malignancies.82,83EZH2 is mutated in5% to 10%of PMF,more particularly associatedwith JAK2V617F and
gives a poor prognosis.84 Three recent studies have shown that Ezh2loss in a murine MPN model expressing JAK2V617F dramaticallymodifies the MPN phenotype. JAK2V617F/Ezh22/2 double mutantmice had significantly reduced survival due to rapid acceleration tolethal MF.85-87 Furthermore, strong cooperation between Ezh2 lossand JAK2V617F on disease initiation by increasing the fitness ofJAK2V617F stem cells was reported. At the cellular level, Ezh2 lossincreased megakaryopoiesis at the expense of erythropoiesis. Thephenotype of the JAK2V617F/Ezh22/2 double mutant mice wasrelated to changes in the expression of PRC2 target genes and moreparticularly of the Lin28b/let7/Hmga2 axis. The overexpression ofHmga2, a gene that was previously found deregulated in human PMF,appears to play an important role in this phenotype.86,87
ASXL1 and SRSF2 mutations are associatedwith a poor prognosis
ASXL1 encodes for an epigenetic regulator, which binds to chromatin.Interestingly, it has been shown that ASXL1 recruits the PRC2 com-plex to specific loci through a direct interaction between ASXL1 andEZH288 (Figure 4). However, the role of ASXL1 is wider than EZH2because it can be also involved in the PRC1 complex by its associa-tion with the deubiquitinating enzyme (DUB) BRCA-1–associated
Figure 5. Presence of myeloproliferative and
myelodysplastic features in MPN. (A-C) The 3
MPN-restricted drivers lead to a myeloproliferative
phenotype. All of the additional mutations in genes
involved in epigenetics and splicing modify the
differentiation and give a myelodysplastic pheno-
type even if some of them such as TET2, DNMT3A,
and EZH2 clearly play an important role in initiation.
Moreover, there are additional mutations involved in
splicing that induce myelodysplastic features leading
to MF, cytopenia, and eventually progression to
leukemia. Professional illustration by Somersault18:
24.
BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6 SOMATIC MUTATIONS AND MPNs 675
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

protein (BAP1), a critical tumor suppressor in solid tumor.89 In addition,ASXL1 also binds to nuclear hormone receptors such as RARa andestrogen receptors. The ASXL family plays an important role indevelopment as shown in Drosophila by regulating Hox genes. Inhumans, de novo or germ line ASXL1 mutations are responsible fora developmental syndrome called the Bohring-Opitz syndrome.90
Somatic mutations in ASXL1 were first described by Birnbaum’sgroup, first in MDS and CMML and then in MPN.69,91 They are thesecond mutations by their frequency in epigenetic regulators afterTET2 in MPNs. However, they are essentially associated with PMFwith a frequency around 25%. The ASXL1 mutations are associatedwith an aggravation in the prognosis, whatever the InternationalPrognostic Scoring System (iPSS) classification. Mutations are lossof function and are associated with a higher frequency of AMLtransformation. These genetic alterations are either focal deletion ornonsense mutation or insertion/deletion leading to frameshift, themost common variant being the c.1934dupG;p.Gly646TrpfsX12variant. In mice, Asxl1 deletion leads to profound cytopenia with adysplasia associated with a profound defect in HSC self-renewalproperties that are corrected by Tet2 deletion.92
SRSF2 mutations are also associated with MPNs having a poorprognosis.93 Mutations in genes encoding spliceosome proteins weredetected in different hematopoietic malignancies in 2011, but moreparticularly in MDS.94 Spliceosome gene mutations in MPNs areessentially restricted to ET and MF. The most frequent mutationsinclude SRSF2,SF3B1, andU2AF1 and are associatedwith anemia andthrombocytopenia.95 SRSF2 encodes for a protein, which is a memberof the serine/arginine-rich splicing factor family that binds toexonic splicing enhancer (ESE) sequences in the pre–messengerRNA (mRNA). There is increasing evidence that SRSF2 mutations,essentially on the proline 95 are not loss of functions, but recognizepreferentially the CCNG ESE motifs whereas the WT sequencerecognizes both the CCNG and GGNG ESE motifs. This alters thesplicing of numerous pre-mRNA and leads to numerous functionallyrelevant misspliced events. In consequence, mice with a heterozygousSrsf2P95H mutant develop a cytopenia by myelodysplasia whereas ahomozygousSrsf2knockoutwhen induced inadults leads tocytopeniadue to a decrease in hematopoietic progenitors associated withincreased apoptosis mimicking a bone marrow aplasia.96 Particularly,it has been shown that the Srsf2 P95H mutation in mice can lead to amissplicing and nonsense-mediated decay of Ezh2.97 Knowing thatSRSF2 mutations are enriched in leukemic transformation of MPNs(19% of the cases), this further establishes that EZH2 and the PRC2complex are important factors in the development of MF andprogression toward leukemia.
The p53 pathway and the development ofsecondary AML
Various mutations and cytogenetic lesions targeting the TP53 tumor-suppressor function are found in around 40% to 50% of secondaryleukemia of MPNs. This usually includes missense mutations ordeletions in theTP53gene or amplificationof chromosome1q targetingMDM4, a TP53 transcriptional inhibitor.98 Heterozygous TP53-mutated clones can be found early in MPN, but evolution to leukemiais associated with its clonal dominance and transition from heterozy-gosity to homozygosity for themutation.98Thismodeof transformationmimics therapy-related leukemia and is quite different from sporadicleukemia.99Presently, the onlymousemodelwhich leads to leukemia isthe overexpression of JAK2V617F in a Tp53 knockout model.65 The
role of therapy in the induction or on the selection of TP53-mutatedclones is presently unknown. TP53 as well as DNMT3Amutations areapparently more frequent in post-PV or -ET AML than on post-MFleukemia.100 Other secondary leukemia are mainly associated withmutations in ASXL1, SRSF2, IDH1/2, CBL, and LNK. Late eventsinclude RUNX1 mutations (30% of the cases), FLT3–internal tandemduplication (15%of the cases),N-RAS,NF1, and deletion in IKZF1 andCUX1100,101 (Figure 4). The complex mutational profile of patients inthe leukemic stage indicates that all patients at this stage are geneticallyunique with complex clonal hierarchies. Treatment is challenging andrelapse almost always occurs.
Important factors for initiation
Aging
There is increasing evidence that JAK2V617F is relatively frequent inthe aging healthy population and is presently estimated to be,0.5%.13
This indicates that JAK2V617F alone is sufficient to engender clonalhematopoiesis and suggests it has a disease-initiating role in MPN.
However, JAK2V617F being a frequent mutation, it has a lowpenetrance to give a MPN, suggesting that other factors must beassociated to JAK2V617F to give rise to a disease. Aging is generallyassociated with a deregulation of HSCs, which lose their function andbecomemyeloid-biased and less quiescent as a consequenceof intrinsicand environmental changes. Overall, this suggests that JAK2V617FHSCs have higher competitive properties in this context, explainingwhy MPNs are age-related diseases.
Inflammation
All MPNs, particularly PMF, are associated with an important in-flammatory response as demonstrated by the presence of highplasma levels of inflammatory cytokines as well as constitutionalsymptoms alleviated by anti-inflammatory therapies such corticoidand ruxolitinib.102 These inflammatory cytokines are synthetized bythe mutated and nonmutated hematopoietic cells as well as by non-hematopoietic cells such as mesenchymal stromal cells.103 Moreparticularly, it has beendemonstrated that the JAK2V617Fprogenitorssecrete IL1b, which induces the apopotic death of nestin1 cellsproviding a favorable environment for JAK2V617F HSCs.104 More-over, it has been shown that tumor necrosis factor a (TNFa) gives acompetitive advantage to JAK2V617FHSCs.105 IL33mayhave similarproperties.106 The inflammatory cytokines might also be involved inextramedullar hematopoiesis by favoring colonization of JAK2V617FHSCs and progenitors in the spleen.
Predisposition
Several susceptibility alleles that correspond to common polymor-phisms in genes such as JAK2, particularly the JAK2 46/1 haplotype,TERT,MECOM, SH2B3,CHEK2, PINT, andGFI1B, may weakly (bytwofold to sixfold) increase the development of the disease.13,107 Themechanism is presently unknown but these predisposition variantsinvolve genes that play a role either inDNAdamage response (CHEK2,TERT, JAK2 46/1 haplotype) or in the JAK2/STATpathway.Recently,predisposition factorswere discovered in the trueMPN familieswith anautosomal pattern of inheritance but with an incomplete penetrance,suggesting that they are strong predisposing factors. Although RBBP6mutations were found in MF families, a copy-number variation of
676 VAINCHENKER and KRALOVICS BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

6 genes with 2 genes involved (ATG2B and GSKIP) was identified inMPN families with a particularly aggressive phenotype.108,109
Conclusions
The mutational landscape in classical MPN is much more complexthan initially thought. However, abnormal activation of JAK2 is thecommon feature of disease, causing mutations in the 3 genesdriving the MPNs. The genetic cause remains unknown in around15% of chronic thrombocytosis classified as ET and in ,10% ofPMF. The rare triple-negative PMF appearsmore likely to beMDSswith secondary fibrosis. In the majority of ET and PV, onlymutations in JAK2, CALR, andMPL can be found, suggesting thatthe deregulation in the cytokine receptor/JAK2 pathway is suffi-cient to induce a clonal myeloproliferative disorder reinforcing theconcept that JAK2 is themain therapeutic target. Themechanism ofJAK2 activationmay define 2main types ofMPNs: (1) those drivenby JAK2V61F, leading to ET, PV, and PMF and associated withproliferation and activation of the 3 main myeloid lineages(erythroid, granulocytic, and MK/platelet lineages) and (2) thosedriven by CALR and MPL mutants which are associated with ETand PMF and target essentially the MK/platelet lineage.
PMF represents a different disorder, which may be geneticallycloser to MDS, and its development may require the occurrence ofseveral drivers preceding the JAK2V617F mutations and the presenceof inflammation in the bone marrow microenvironment. The clinicalheterogeneity seems to be mainly related to the combination ofmutations and perhaps their order of acquisition. The precise role ofeach mutation and their impact onMPN phenotype will require further
studies. Futureworkon thepathogenesis ofMPNswill bemore focusedon the interaction between extrinsic factors and acquired geneticabnormalities in disease initiation and progression.
Acknowledgments
The authors are indebted to Isabelle Plo, Caroline Marty, and StefanConstantinescu for their help to improve the manuscript.
This work was supported by grants from Ligue Nationale Contrele Cancer (“Equipe labellisee 2016”), from INSERM, and fromLaboratoryofExcellenceGlobuleRouge-Excellence.W.V.was fundedby the program “Investissements d’avenir”. R.K. received funding fromthe Austrian Science Fund (SFB F4702 and P29018-B30).
Authorship
Contribution: W.V. and R.K. wrote the manuscript.Conflict-of-interest disclosure: The authors declare no competing
financial interests.ORCID profiles: R.K., 0000-0002-6997-8359.Correspondence: William Vainchenker, INSERM UMR 1170,
Institut Gustave Roussy, 39, Rue Camille Desmoulins, Villejuif,94805 France; e-mail: [email protected]; and Robert Kralovics, Re-search Center for Molecular Medicine of the Austrian Academy ofSciences, Lazarettgasse 14, AKHBT 25.3, A-1090 Vienna, Austria;e-mail: [email protected].
References
1. Spivak JL. The chronic myeloproliferativedisorders: clonality and clinical heterogeneity.Semin Hematol. 2004;41(2 suppl 3):1-5.
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016revision to the World Health Organizationclassification of myeloid neoplasms and acuteleukemia. Blood. 2016;127(20):2391-2405.
3. Barbui T, Thiele J, Passamonti F, et al.Survival and disease progression in essentialthrombocythemia are significantly influenced byaccurate morphologic diagnosis: an internationalstudy. J Clin Oncol. 2011;29(23):3179-3184.
4. James C, Ugo V, Le Couedic JP, et al. A uniqueclonal JAK2 mutation leading to constitutivesignalling causes polycythaemia vera. Nature.2005;434(7037):1144-1148.
5. Kralovics R, Passamonti F, Buser AS, et al.A gain-of-function mutation of JAK2 inmyeloproliferative disorders. N Engl J Med.2005;352(17):1779-1790.
6. Levine RL, Wadleigh M, Cools J, et al. Activatingmutation in the tyrosine kinase JAK2 inpolycythemia vera, essential thrombocythemia,and myeloid metaplasia with myelofibrosis.Cancer Cell. 2005;7(4):387-397.
7. Baxter EJ, Scott LM, Campbell PJ, et al;Cancer Genome Project. Acquired mutation ofthe tyrosine kinase JAK2 in humanmyeloproliferative disorders. Lancet. 2005;365(9464):1054-1061.
8. Kralovics R, Guan Y, Prchal JT. Acquireduniparental disomy of chromosome 9p is afrequent stem cell defect in polycythemia vera.Exp Hematol. 2002;30(3):229-236.
9. Sozer S, Fiel MI, Schiano T, Xu M, MascarenhasJ, Hoffman R. The presence of JAK2V617F
mutation in the liver endothelial cells of patientswith Budd-Chiari syndrome. Blood. 2009;113(21):5246-5249.
10. Rumi E, Pietra D, Ferretti V, et al; AssociazioneItaliana per la Ricerca sul Cancro GruppoItaliano Malattie Mieloproliferative Investigators.JAK2 or CALR mutation status defines subtypesof essential thrombocythemia with substantiallydifferent clinical course and outcomes. Blood.2014;123(10):1544-1551.
11. Szpurka H, Tiu R, Murugesan G, et al.Refractory anemia with ringed sideroblastsassociated with marked thrombocytosis(RARS-T), another myeloproliferative conditioncharacterized by JAK2 V617F mutation. Blood.2006;108(7):2173-2181.
12. Levine RL, Loriaux M, Huntly BJ, et al. TheJAK2V617F activating mutation occurs inchronic myelomonocytic leukemia and acutemyeloid leukemia, but not in acute lymphoblasticleukemia or chronic lymphocytic leukemia.Blood. 2005;106(10):3377-3379.
13. Hinds DA, Barnholt KE, Mesa RA, et al. Germline variants predispose to both JAK2 V617Fclonal hematopoiesis and myeloproliferativeneoplasms. Blood. 2016;128(8):1121-1128.
14. Hirsch P, Mamez AC, Belhocine R, et al. Clonalhistory of a cord blood donor cell leukemia withprenatal somatic JAK2 V617F mutation.Leukemia. 2016;30(8):1756-1759.
15. McKerrell T, Park N, Moreno T, et al;Understanding Society Scientific Group.Leukemia-associated somatic mutations drivedistinct patterns of age-related clonalhemopoiesis. Cell Reports. 2015;10(8):1239-1245.
16. Steensma DP, Bejar R, Jaiswal S, et al. Clonalhematopoiesis of indeterminate potential and itsdistinction from myelodysplastic syndromes.Blood. 2015;126(1):9-16.
17. Scott LM, Tong W, Levine RL, et al. JAK2 exon12 mutations in polycythemia vera and idiopathicerythrocytosis. N Engl J Med. 2007;356(5):459-468.
18. Passamonti F, Elena C, Schnittger S, et al.Molecular and clinical features of themyeloproliferative neoplasm associated withJAK2 exon 12 mutations. Blood. 2011;117(10):2813-2816.
19. Pikman Y, Lee BH, Mercher T, et al. MPLW515Lis a novel somatic activating mutation inmyelofibrosis with myeloid metaplasia. PLoSMed. 2006;3(7):e270.
20. Defour JP, Chachoua I, Pecquet C,Constantinescu SN. Oncogenic activation ofMPL/thrombopoietin receptor by 17 mutationsat W515: implications for myeloproliferativeneoplasms. Leukemia. 2016;30(5):1214-1216.
21. Rumi E, Pietra D, Guglielmelli P, et al;Associazione Italiana per la Ricerca sul CancroGruppo Italiano Malattie Mieloproliferative.Acquired copy-neutral loss of heterozygosity ofchromosome 1p as a molecular event associatedwith marrow fibrosis in MPL-mutatedmyeloproliferative neoplasms. Blood. 2013;121(21):4388-4395.
22. Beer PA, Campbell PJ, Scott LM, et al. MPLmutations in myeloproliferative disorders:analysis of the PT-1 cohort. Blood. 2008;112(1):141-149.
23. Chaligne R, James C, Tonetti C, et al. Evidencefor MPL W515L/K mutations in hematopoietic
BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6 SOMATIC MUTATIONS AND MPNs 677
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

stem cells in primitive myelofibrosis. Blood.2007;110(10):3735-3743.
24. Malcovati L, Della Porta MG, Pietra D, et al.Molecular and clinical features of refractoryanemia with ringed sideroblasts associated withmarked thrombocytosis. Blood. 2009;114(17):3538-3545.
25. Ding J, Komatsu H, Wakita A, et al. Familialessential thrombocythemia associated with adominant-positive activating mutation of thec-MPL gene, which encodes for the receptor forthrombopoietin. Blood. 2004;103(11):4198-4200.
26. Cabagnols X, Favale F, Pasquier F, et al.Presence of atypical thrombopoietin receptor(MPL) mutations in triple-negative essentialthrombocythemia patients. Blood. 2016;127(3):333-342.
27. Milosevic Feenstra JD, Nivarthi H, Gisslinger H,et al. Whole-exome sequencing identifies novelMPL and JAK2 mutations in triple-negativemyeloproliferative neoplasms. Blood. 2016;127(3):325-332.
28. Klampfl T, Gisslinger H, Harutyunyan AS,et al. Somatic mutations of calreticulin inmyeloproliferative neoplasms. N Engl J Med.2013;369(25):2379-2390.
29. Nangalia J, Massie CE, Baxter EJ, et al. SomaticCALR mutations in myeloproliferative neoplasmswith nonmutated JAK2. N Engl J Med. 2013;369(25):2391-2405.
30. Pietra D, Rumi E, Ferretti VV, et al. Differentialclinical effects of different mutation subtypes inCALR-mutant myeloproliferative neoplasms.Leukemia. 2016;30(2):431-438.
31. Cabagnols X, Defour JP, Ugo V, et al.Differential association of calreticulin type 1 andtype 2 mutations with myelofibrosis and essentialthrombocytemia: relevance for diseaseevolution. Leukemia. 2015;29(1):249-252.
32. Broseus J, Park JH, Carillo S, Hermouet S,Girodon F. Presence of calreticulin mutations inJAK2-negative polycythemia vera. Blood. 2014;124(26):3964-3966.
33. Theocharides AP, Lundberg P, Lakkaraju AK,et al. Homozygous calreticulin mutations inpatients with myelofibrosis lead to acquiredmyeloperoxidase deficiency. Blood. 2016;127(25):3253-3259.
34. Szuber N, Lamontagne B, Busque L.Novel germline mutations in the calreticulingene: implications for the diagnosis ofmyeloproliferative neoplasms [published onlineahead of print 27 July 2016]. J Clin Pathol.
35. Oh ST, Simonds EF, Jones C, et al. Novelmutations in the inhibitory adaptor protein LNKdrive JAK-STAT signaling in patients withmyeloproliferative neoplasms. Blood. 2010;116(6):988-992.
36. Rumi E, Harutyunyan AS, Pietra D, et al.LNK mutations in familial myeloproliferativeneoplasms. Blood. 2016;128(1):144-145.
37. Lasho TL, Pardanani A, Tefferi A. LNK mutationsin JAK2 mutation-negative erythrocytosis. N EnglJ Med. 2010;363(12):1189-1190.
38. Pardanani A, Lasho T, Finke C, Oh ST, GotlibJ, Tefferi A. LNK mutation studies in blast-phase myeloproliferative neoplasms, and inchronic-phase disease with TET2, IDH, JAK2or MPL mutations. Leukemia. 2010;24(10):1713-1718.
39. Vainchenker W, Constantinescu SN. JAK/STATsignaling in hematological malignancies.Oncogene. 2013;32(21):2601-2613.
40. Bandaranayake RM, Ungureanu D, Shan Y,Shaw DE, Silvennoinen O, Hubbard SR. Crystalstructures of the JAK2 pseudokinase domainand the pathogenic mutant V617F. Nat StructMol Biol. 2012;19(8):754-759.
41. Shan Y, Gnanasambandan K, Ungureanu D,et al. Molecular basis for pseudokinase-dependent autoinhibition of JAK2 tyrosinekinase. Nat Struct Mol Biol. 2014;21(7):579-584.
42. Leroy E, Dusa A, Colau D, et al. UncouplingJAK2 V617F activation from cytokine-inducedsignalling by modulation of JH2 aC helix.Biochem J. 2016;473(11):1579-1591.
43. Lu X, Levine R, Tong W, et al. Expression of ahomodimeric type I cytokine receptor is requiredfor JAK2V617F-mediated transformation. ProcNatl Acad Sci USA. 2005;102(52):18962-18967.
44. Ugo V, Marzac C, Teyssandier I, et al.Multiple signaling pathways are involved inerythropoietin-independent differentiation oferythroid progenitors in polycythemia vera. ExpHematol. 2004;32(2):179-187.
45. Dawson MA, Bannister AJ, Gottgens B, et al.JAK2 phosphorylates histone H3Y41 andexcludes HP1alpha from chromatin. Nature.2009;461(7265):819-822.
46. Liu F, Zhao X, Perna F, et al. JAK2V617F-mediated phosphorylation of PRMT5downregulates its methyltransferase activity andpromotes myeloproliferation. Cancer Cell. 2011;19(2):283-294.
47. Staerk J, Lacout C, Sato T, Smith SO,Vainchenker W, Constantinescu SN. Anamphipathic motif at the transmembrane-cytoplasmic junction prevents autonomousactivation of the thrombopoietin receptor. Blood.2006;107(5):1864-1871.
48. Balligand T, Achouri Y, Pecquet C, et al.Pathologic activation of thrombopoietin receptorand JAK2-STAT5 pathway by frameshift mutantsof mouse calreticulin. Leukemia. 2016;30(8):1775-1778.
49. Chachoua I, Pecquet C, El-Khoury M, et al.Thrombopoietin receptor activation bymyeloproliferative neoplasm associatedcalreticulin mutants. Blood. 2016;127(10):1325-1335.
50. Elf S, Abdelfattah NS, Chen E, et al. Mutantcalreticulin requires both its mutant C-terminusand the thrombopoietin receptor for oncogenictransformation. Cancer Discov. 2016;6(4):368-381.
51. Marty C, Pecquet C, Nivarthi H, et al. Calreticulinmutants in mice induce an MPL-dependentthrombocytosis with frequent progression tomyelofibrosis. Blood. 2016;127(10):1317-1324.
52. Nivarthi H, Chen D, Cleary C, et al.Thrombopoietin receptor is required for theoncogenic function of CALR mutants. Leukemia.2016;30(8):1759-1763.
53. Araki M, Yang Y, Masubuchi N, et al. Activationof the thrombopoietin receptor by mutantcalreticulin in CALR-mutant myeloproliferativeneoplasms. Blood. 2016;127(10):1307-1316.
54. Garbati MR, Welgan CA, Landefeld SH, et al.Mutant calreticulin-expressing cells inducemonocyte hyperreactivity through a paracrinemechanism. Am J Hematol. 2016;91(2):211-219.
55. Mullally A, Lane SW, Ball B, et al. PhysiologicalJak2V617F expression causes a lethalmyeloproliferative neoplasm with differentialeffects on hematopoietic stem and progenitorcells. Cancer Cell. 2010;17(6):584-596.
56. Hasan S, Lacout C, Marty C, et al. JAK2V617Fexpression in mice amplifies early hematopoieticcells and gives them a competitive advantagethat is hampered by IFNa. Blood. 2013;122(8):1464-1477.
57. Tiedt R, Hao-Shen H, Sobas MA, et al. Ratioof mutant JAK2-V617F to wild-type Jak2determines the MPD phenotypes in transgenicmice. Blood. 2008;111(8):3931-3940.
58. Li J, Spensberger D, Ahn JS, et al. JAK2 V617Fimpairs hematopoietic stem cell function in aconditional knock-in mouse model of JAK2V617F-positive essential thrombocythemia.Blood. 2010;116(9):1528-1538.
59. Grisouard J, Li S, Kubovcakova L, et al.JAK2 exon 12 mutant mice display isolatederythrocytosis and changes in iron metabolismfavoring increased erythropoiesis. Blood. 2016;128(6):839-851.
60. Balligand T, Achouri Y, Chachoua I, PecquetC, Defour JP, Constantinescu SN. Crispr/Cas9engineered 61bp deletion in the Calr gene ofmice leads to development of thrombocytosis[abstract]. Blood. 2016;128(22):4274.
61. Sangkhae V, Etheridge SL, Kaushansky K,Hitchcock IS. The thrombopoietin receptor, MPL,is critical for development of a JAK2V617F-induced myeloproliferative neoplasm. Blood.2014;124(26):3956-3963.
62. Walz C, Ahmed W, Lazarides K, et al. Essentialrole for Stat5a/b in myeloproliferative neoplasmsinduced by BCR-ABL1 and JAK2(V617F) inmice. Blood. 2012;119(15):3550-3560.
63. Grisouard J, Shimizu T, Duek A, et al. Deletionof Stat3 in hematopoietic cells enhancesthrombocytosis and shortens survival in a JAK2-V617F mouse model of MPN. Blood. 2015;125(13):2131-2140.
64. Pasquier F, Cabagnols X, Secardin L, Plo I,Vainchenker W. Myeloproliferative neoplasms:JAK2 signaling pathway as a central target fortherapy. Clin Lymphoma Myeloma Leuk. 2014;14(suppl):S23-S35.
65. Rampal R, Ahn J, Abdel-Wahab O, et al.Genomic and functional analysis of leukemictransformation of myeloproliferative neoplasms.Proc Natl Acad Sci USA. 2014;111(50):E5401-E5410.
66. Stegelmann F, Bullinger L, Griesshammer M,et al. High-resolution single-nucleotidepolymorphism array-profiling inmyeloproliferative neoplasms identifies novelgenomic aberrations. Haematologica. 2010;95(4):666-669.
67. Vannucchi AM, Lasho TL, Guglielmelli P,et al. Mutations and prognosis in primarymyelofibrosis. Leukemia. 2013;27(9):1861-1869.
68. Zhang X, Su J, Jeong M, et al. DNMT3A andTET2 compete and cooperate to represslineage-specific transcription factors inhematopoietic stem cells. Nat Genet. 2016;48(9):1014-1023.
69. Carbuccia N, Murati A, Trouplin V, et al.Mutations of ASXL1 gene in myeloproliferativeneoplasms. Leukemia. 2009;23(11):2183-2186.
70. Delhommeau F, Dupont S, Della Valle V, et al.Mutation in TET2 in myeloid cancers. N Engl JMed. 2009;360(22):2289-2301.
71. Kosmider O, Gelsi-Boyer V, Ciudad M, et al;Groupe Francophone des Myelodysplasies.TET2 gene mutation is a frequent andadverse event in chronic myelomonocyticleukemia. Haematologica. 2009;94(12):1676-1681.
72. Ortmann CA, Kent DG, Nangalia J, et al. Effectof mutation order on myeloproliferativeneoplasms. N Engl J Med. 2015;372(7):601-612.
73. Lundberg P, Karow A, Nienhold R, et al. Clonalevolution and clinical correlates of somaticmutations in myeloproliferative neoplasms.Blood. 2014;123(14):2220-2228.
74. Stegelmann F, Bullinger L, Schlenk RF, et al.DNMT3A mutations in myeloproliferativeneoplasms. Leukemia. 2011;25(7):1217-1219.
75. Challen GA, Sun D, Jeong M, et al. Dnmt3ais essential for hematopoietic stem celldifferentiation. Nat Genet. 2011;44(1):23-31.
678 VAINCHENKER and KRALOVICS BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

76. Quivoron C, Couronne L, Della Valle V, et al.TET2 inactivation results in pleiotropichematopoietic abnormalities in mouse andis a recurrent event during humanlymphomagenesis. Cancer Cell. 2011;20(1):25-38.
77. Genovese G, Kahler AK, Handsaker RE, et al.Clonal hematopoiesis and blood-cancer riskinferred from blood DNA sequence. N Engl JMed. 2014;371(26):2477-2487.
78. Jaiswal S, Fontanillas P, Flannick J, et al. Age-related clonal hematopoiesis associated withadverse outcomes. N Engl J Med. 2014;371(26):2488-2498.
79. Xie M, Lu C, Wang J, et al. Age-relatedmutations associated with clonal hematopoieticexpansion and malignancies. Nat Med. 2014;20(12):1472-1478.
80. Chen E, Schneider RK, Breyfogle LJ, et al.Distinct effects of concomitant Jak2V617Fexpression and Tet2 loss in mice promotedisease progression in myeloproliferativeneoplasms. Blood. 2015;125(2):327-335.
81. Kameda T, Shide K, Yamaji T, et al. Loss ofTET2 has dual roles in murine myeloproliferativeneoplasms: disease sustainer and diseaseaccelerator. Blood. 2015;125(2):304-315.
82. Ernst T, Chase AJ, Score J, et al. Inactivatingmutations of the histone methyltransferase geneEZH2 in myeloid disorders. Nat Genet. 2010;42(8):722-726.
83. Puda A, Milosevic JD, Berg T, et al. Frequentdeletions of JARID2 in leukemic transformationof chronic myeloid malignancies. Am J Hematol.2012;87(3):245-250.
84. Guglielmelli P, Biamonte F, Score J, et al. EZH2mutational status predicts poor survival inmyelofibrosis. Blood. 2011;118(19):5227-5234.
85. Yang Y, Akada H, Nath D, Hutchison RE, MohiG. Loss of Ezh2 cooperates with Jak2V617F inthe development of myelofibrosis in a mousemodel of myeloproliferative neoplasm. Blood.2016;127(26):3410-3423.
86. Shimizu T, Kubovcakova L, Nienhold R, et al.Loss of Ezh2 synergizes with JAK2-V617F ininitiating myeloproliferative neoplasms andpromoting myelofibrosis. J Exp Med. 2016;213(8):1479-1496.
87. Sashida G, Wang C, Tomioka T, et al. The lossof Ezh2 drives the pathogenesis of myelofibrosisand sensitizes tumor-initiating cells tobromodomain inhibition. J Exp Med. 2016;213(8):1459-1477.
88. Abdel-Wahab O, Adli M, LaFave LM, et al.ASXL1 mutations promote myeloidtransformation through loss of PRC2-mediatedgene repression. Cancer Cell. 2012;22(2):180-193.
89. Dey A, Seshasayee D, Noubade R, et al. Lossof the tumor suppressor BAP1 causes myeloidtransformation. Science. 2012;337(6101):1541-1546.
90. Hoischen A, van Bon BW, Rodrıguez-SantiagoB, et al. De novo nonsense mutations in ASXL1cause Bohring-Opitz syndrome. Nat Genet.2011;43(8):729-731.
91. Gelsi-Boyer V, Trouplin V, Adelaıde J, et al.Mutations of polycomb-associated gene ASXL1in myelodysplastic syndromes and chronicmyelomonocytic leukaemia. Br J Haematol.2009;145(6):788-800.
92. Abdel-Wahab O, Gao J, Adli M, et al. Deletionof Asxl1 results in myelodysplasia and severedevelopmental defects in vivo. J Exp Med. 2013;210(12):2641-2659.
93. Zhang SJ, Rampal R, Manshouri T, et al.Genetic analysis of patients with leukemictransformation of myeloproliferative neoplasmsshows recurrent SRSF2 mutations that areassociated with adverse outcome. Blood. 2012;119(19):4480-4485.
94. Yoshida K, Sanada M, Shiraishi Y, et al.Frequent pathway mutations of splicingmachinery in myelodysplasia. Nature. 2011;478(7367):64-69.
95. Wassie E, Finke C, Gangat N, et al. Acompendium of cytogenetic abnormalities inmyelofibrosis: molecular and phenotypiccorrelates in 826 patients. Br J Haematol. 2015;169(1):71-76.
96. Komeno Y, Huang YJ, Qiu J, et al. SRSF2is essential for hematopoiesis, and itsmyelodysplastic syndrome-related mutationsdysregulate alternative pre-mRNA splicing.Mol Cell Biol. 2015;35(17):3071-3082.
97. Kim E, Ilagan JO, Liang Y, et al. SRSF2mutations contribute to myelodysplasia bymutant-specific effects on exon recognition.Cancer Cell. 2015;27(5):617-630.
98. Harutyunyan A, Klampfl T, Cazzola M, KralovicsR. p53 lesions in leukemic transformation.N Engl J Med. 2011;364(5):488-490.
99. Wong TN, Ramsingh G, Young AL, et al. Roleof TP53 mutations in the origin and evolutionof therapy-related acute myeloid leukaemia.Nature. 2015;518(7540):552-555.
100. Courtier F, Carbuccia N, Garnier S, et al.Genomic analysis of myeloproliferativeneoplasms in chronic and acute phases[published online ahead of print 14 October2016]. Haematologica.
101. Milosevic JD, Puda A, Malcovati L, et al. Clinicalsignificance of genetic aberrations in secondaryacute myeloid leukemia. Am J Hematol. 2012;87(11):1010-1016.
102. Tefferi A. Pathogenesis of myelofibrosis withmyeloid metaplasia. J Clin Oncol. 2005;23(33):8520-8530.
103. Plo I. p53 at the crossroads of MPN treatment.Blood. 2014;124(5):668-669.
104. Arranz L, Sanchez-Aguilera A, Martın-Perez D,et al. Neuropathy of haematopoietic stem cellniche is essential for myeloproliferativeneoplasms. Nature. 2014;512(7512):78-81.
105. Fleischman AG, Aichberger KJ, Luty SB, et al.TNFa facilitates clonal expansion of JAK2V617Fpositive cells in myeloproliferative neoplasms.Blood. 2011;118(24):6392-6398.
106. Mager LF, Riether C, Schurch CM, et al. IL-33signaling contributes to the pathogenesis ofmyeloproliferative neoplasms. J Clin Invest.2015;125(7):2579-2591.
107. Tapper W, Jones AV, Kralovics R, et al. Geneticvariation at MECOM, TERT, JAK2 and HBS1L-MYB predisposes to myeloproliferativeneoplasms. Nat Commun. 2015;6:6691.
108. Harutyunyan AS, Giambruno R, Krendl C, et al.Germline RBBP6 mutations in familialmyeloproliferative neoplasms. Blood. 2016;127(3):362-365.
109. Saliba J, Saint-Martin C, Di Stefano A, et al.Germline duplication of ATG2B and GSKIPpredisposes to familial myeloid malignancies.Nat Genet. 2015;47(10):1131-1140.
110. Grand FH, Hidalgo-Curtis CE, Ernst T, et al.Frequent CBL mutations associated with11q acquired uniparental disomy inmyeloproliferative neoplasms. Blood. 2009;113(24):6182-6192.
111. Tefferi A, Lasho TL, Abdel-Wahab O, et al.IDH1 and IDH2 mutation studies in 1473 patientswith chronic-, fibrotic- or blast-phase essentialthrombocythemia, polycythemia vera ormyelofibrosis. Leukemia. 2010;24(7):1302-1309.
112. Klampfl T, Harutyunyan A, Berg T, et al.Genome integrity of myeloproliferativeneoplasms in chronic phase and during diseaseprogression. Blood. 2011;118(1):167-176.
113. Lasho TL, Finke CM, Hanson CA, et al. SF3B1mutations in primary myelofibrosis: clinical,histopathology and genetic correlates among155 patients. Leukemia. 2012;26(5):1135-1137.
114. Lacout C, Pisani DF, Tulliez M, Gachelin FM,Vainchenker W, Villeval JL. JAK2V617Fexpression in murine hematopoietic cells leadsto MPD mimicking human PV with secondarymyelofibrosis. Blood. 2006;108(5):1652-1660.
115. Wernig G, Mercher T, Okabe R, Levine RL, LeeBH, Gilliland DG. Expression of Jak2V617Fcauses a polycythemia vera-like disease withassociated myelofibrosis in a murine bonemarrow transplant model. Blood. 2006;107(11):4274-4281.
116. Zaleskas VM, Krause DS, Lazarides K, et al.Molecular pathogenesis and therapy ofpolycythemia induced in mice by JAK2 V617F.PLoS One. 2006;1:e18.
117. Xing S, Wanting TH, Zhao W, et al.Transgenic expression of JAK2V617F causesmyeloproliferative disorders in mice. Blood.2008;111(10):5109-5117.
118. Shide K, Shimoda HK, Kumano T, et al.Development of ET, primary myelofibrosis andPV in mice expressing JAK2 V617F. Leukemia.2008;22(1):87-95.
119. Etheridge SL, Roh ME, Cosgrove ME, et al.JAK2V617F-positive endothelial cells contributeto clotting abnormalities in myeloproliferativeneoplasms. Proc Natl Acad Sci USA. 2014;111(6):2295-2300.
120. Zhan H, Ma Y, Lin CH, Kaushansky K. JAK2(V617F)-mutant megakaryocytes contribute tohematopoietic stem/progenitor cell expansion ina model of murine myeloproliferation. Leukemia.2016;30(12):2332-2341.
121. Marty C, Lacout C, Martin A, et al.Myeloproliferative neoplasm induced byconstitutive expression of JAK2V617F in knock-in mice. Blood. 2010;116(5):783-787.
122. Li J, Kent DG, Godfrey AL, et al. JAK2V617Fhomozygosity drives a phenotypic switch inmyeloproliferative neoplasms, but is insufficientto sustain disease. Blood. 2014;123(20):3139-3151.
123. Akada H, Yan D, Zou H, Fiering S, HutchisonRE, Mohi MG. Conditional expression ofheterozygous or homozygous Jak2V617Ffrom its endogenous promoter induces apolycythemia vera-like disease. Blood. 2010;115(17):3589-3597.
124. Akada H, Akada S, Hutchison RE, Mohi G.Erythroid lineage-restricted expression ofJak2V617F is sufficient to induce amyeloproliferative disease in mice.Haematologica. 2012;97(9):1389-1393.
125. Lamrani L, Lacout C, Ollivier V, et al. Hemostaticdisorders in a JAK2V617F-driven mouse modelof myeloproliferative neoplasm. Blood. 2014;124(7):1136-1145.
126. Shide K, Kameda T, Yamaji T, et al. Calreticulinmutant mice develop essential thrombocythemiathat is ameliorated by the JAK inhibitor ruxolitinib[published online ahead of print 29 November2016]. Leukemia.
BLOOD, 9 FEBRUARY 2017 x VOLUME 129, NUMBER 6 SOMATIC MUTATIONS AND MPNs 679
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom

online December 27, 2016 originally publisheddoi:10.1182/blood-2016-10-695940
2017 129: 667-679
William Vainchenker and Robert Kralovics myeloproliferative neoplasmsGenetic basis and molecular pathophysiology of classical
http://www.bloodjournal.org/content/129/6/667.full.htmlUpdated information and services can be found at:
(127 articles)Review Series (683 articles)Review Articles
(1625 articles)Myeloid Neoplasia (4376 articles)Free Research Articles
(4497 articles)Clinical Trials and Observations Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society
For personal use only.on March 16, 2017. by guest www.bloodjournal.orgFrom