Embed Size (px)
Citation preview

ARTICLE IN PRESS
JID: ANL [mNS; February 19, 2020;21:9 ]
Auris Nasus Larynx xxx (xxxx) xxx
Contents lists available at ScienceDirect
Auris Nasus Larynx
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / a n l
Case Report
Frontal sinusitis associated with orbital decompression for
Graves’ orbitopathy
Shun Tatehara
a , Go Inokuchi a , ∗, Hiroko Takeda
a , Shunsuke Kuroki a , Hisami Fujio
a , Atsushi Azumi b , Ken-ichi Nibu
a
a Department of Otolaryngology - Head and Neck Surgery, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-cho, Chuo-ku, Kobe, Hyogo, 650-0017, Japan b Kobe Kaisei Hospital, Department of Ophthalmology, Kobe, Japan
A R T I C L E I N F O
Article history: Received 17 June 2019 Accepted 30 January 2020 Available online xxx
Keywords: Graves’ orbitopathy Orbital decompression Frontal sinusitis Endoscopic sinus surgery Endoscopic modified Lothrop procedure
A B S T R A C T
Orbital decompression (OD) for Graves’ orbitopathy usually includes removal of orbital medial wall. While OD occasionally cause or worsen chronic sinusitis because of the obstructed sinus drainage by prolapsed orbital fat, to date few reports have been published on the management or prevention of sinusitis associated with OD. Here, we present two patients (three sides) with newly developed and one patient (one side) with worsening obstructive frontal sinusitis following OD. These three patients had OD including the removal of the superior attachment of uncinated process to lamina papyracea. Endoscopic modified Lothrop procedure (EMLP) was useful to relieve symptoms and keep an enough access to frontal sinuses for all cases. We also performed EMLP for another two patients (four sides) with pre-existing sinusitis before OD. Worsening of sinusitis could be avoided by EMLP before OD. EMLP was useful approach for both treatment and prevention of sinusitis related to OD. The superior attachment site of uncinated process and the pattern of frontal sinus drainage might predict the occurrence of obstructive frontal sinusitis following OD.
© 2020 Oto-Rhino-Laryngological Society of Japan Inc. Published by Elsevier B.V. All rights reserved.
1
a
i
me
l
t
t
c
p
m
m
G
o
b
t
f
h0
. Introduction
Graves’ disease is an autoimmune disorder caused byn excess of thyroid stimulating immunoglobulins. Approx-mately 40% to 75% of patients develop various orbital
anifestations including exophthalmos, proptosis, periorbital dema and chemosis, eyelid retraction, ocular dysmotilityeading to squint and diplopia, and optic neuropathy [1] . Sys-emic corticosteroids and external beam radiation are usefulreatment strategies that minimize proptosis and optic nerve
∗ Corresponding author. E-mail address: [email protected] (G. Inokuchi).
s
a
s
ttps://doi.org/10.1016/j.anl.2020.01.011 385-8146/© 2020 Oto-Rhino-Laryngological Society of Japan Inc. Published by
Please cite this article as: S. Tatehara, G. Inokuchi and H. Takeda et al., FrontAuris Nasus Larynx, https:// doi.org/ 10.1016/ j.anl.2020.01.011
ompression during the acute inflammatory phase. However,atients in the chronic fibrosis phase who are unresponsive toedical therapy need surgical intervention. Orbital decompression (OD) for Graves’ orbitopathy, the
ost frequent and invalidating extrathyroidal expression ofraves’ disease, is generally safe and effective. Overall post-perative sinusitis reportedly occurs in 3.5%–6.1% of patients,ut 40% of those with preoperative sinusitis develop obstruc-ive sinusitis after OD [2 , 3] . Sinusitis after OD is often re-ractory to medical therapy and difficult to manage becauseinus drainage is blocked by prolapsed orbital fat.
We treated two patients (three sides) with newly developednd one patient (one side) with worsening obstructive frontalinusitis following OD by endoscopic sinus surgery (ESS)
Elsevier B.V. All rights reserved.
al sinusitis associated with orbital decompression for Graves’ orbitopathy,

2 S. Tatehara, G. Inokuchi and H. Takeda et al. / Auris Nasus Larynx xxx (xxxx) xxx
ARTICLE IN PRESS
JID: ANL [mNS; February 19, 2020;21:9 ]
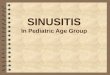
Fig. 1. Attachment of uncinated process to orbital medial wall was removed and prolapsed orbital fat blocked the drainage from frontal sinus (Case 5). MRI before OD revealed no sinusitis and uncinate process (UP) attached to lamina papyracea (A). Left ethmoid and frontal sinusitis (B, C) by prolapsed orbital fat (arrowheads) was shown. The superior attachment of UP to lamina papyracea was removed after OD. Contra-lateral (E) and anterior (F) approach direction to frontal sinus by endoscopic modified Lothrop procedure (EMLP) was indicated by arrow.
s
f
t
t
s
p
f
t
e
a
p
3
w
l
c
a
i
l
n
o
s
m
U
(
m
s
including endoscopic modified Lothrop procedure (EMLP).We also performed ESS for another two patients (four sides)with pre-existing sinusitis before OD. As few reports havebeen published on sinusitis related to OD, this report aims tointroduce the management and prevention of frontal sinusitisassociated with OD.
2. Case reports
Case 1: A 35-year-old female with frontal pain and swolleneyelids was referred to our hospital. She had a OD for Graves’orbitopathy five months ago. Computed tomography (CT)revealed bilateral frontal and right sphenoid sinusitis withblocked sinus drainage caused by prolapsed orbital fat. Whilefrontal pain was relieved by intravenous antibiotics, we rec-ommended surgery to prevent recurrent sinusitis. Since themiddle meatuses were completely blocked by orbital fat, weselected the outside-in modified endoscopic Lothrop approach(EMLP) for the frontal sinus, drilling frontal process of themaxilla without confirming the frontal recess in middle mea-tus [4] . We also adopted the trans-septal approach for thesphenoid sinuses. The septum of both frontal and sphenoidsinuses were removed. The patient has remained free fromsinusitis after ESS for 17 months.
Case 2: Another 35-year old male with worsening foul-smelling nasal drip due to refractory sinusitis after OD wasreferred to our hospital. CT revealed sinusitis in the rightfrontal and maxillary sinuses. Pre-operative MRI before ODshowed sinusitis in right frontal and maxillary sinuses and this
Please cite this article as: S. Tatehara, G. Inokuchi and H. Takeda et al., FrontAuris Nasus Larynx, https:// doi.org/ 10.1016/ j.anl.2020.01.011
inusitis got worse after OD. We used the same approach asor Case 1 for the frontal sinus and extended inferior antros-omy for the maxillary sinus, creating wide nasoantral windowhrough inferior meatus [5] . This patient has been free frominusitis after ESS for 15 months.
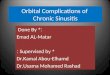
Case 3: A 45-year-old female was referred to our de-artment for the treatment of sinusitis. She was scheduledor OD since medication and radiotherapy failed to suppresshe progression of orbitopathy. A standard endoscopic trans-thmoidal approach was used, which involved making largepertures in the maxillary, sphenoid, and frontal sinuses. Theostoperative period was uneventful and OD was performed months after ESS. Migrated orbital fat in middle meatusas shown in Fig 3 . No obstructive sinusitis has occurred at
east 14 months after ESS. Case 4: A 46-year-old female with refractory sinusitis
aused by nasal polyps was referred to us for medical ther-py. Trans-ethmoidal ESS, similar to that for Case 3 and alsonvolving large apertures in the sinuses was performed, fol-owed by OD 3 months later. Since then, no obstructive si-usitis or complications such as diplopia, nasal obstruction, orlfactory loss have been noted during the 17 months after theurgery.
Case 5: A 61-year old male with history of left OD 12onths ago was referred because of left frontal sinusitis.ncinated process (UP) was attached to medial orbital wall
Fig 1 A) and removed by OD ( Fig 1 D). UP was lateralizededially by orbital fat and blocked drainage from left fontal
inus ( Fig 1 B and C). Same EMLP could relieve left frontal
al sinusitis associated with orbital decompression for Graves’ orbitopathy,

S. Tatehara, G. Inokuchi and H. Takeda et al. / Auris Nasus Larynx xxx (xxxx) xxx 3
ARTICLE IN PRESS
JID: ANL [mNS; February 19, 2020;21:9 ]
Table 1 Clinical characteristics of sinusitis related to orbital decompression.
Case Age Sex Sinusitis before OD Sinusitis after OD Attachment of Uncinate Process
Procedure Interval Follow up
1 35 F R – FS.SS Orbit ESS after OD 5M 17M
L – FS Orbit 2 35 M R Et, MS FS, MS Orbit ESS after OD 6M 15M
L – – Orbit 3 46 F R FS, Et, MS – Skull base ESS before OD 3M 14M
L FS, Et, MS – Skull base 4 46 F R FS, Et, MS – Orbit ESS before OD 3M 17M
L Et, MS – Orbit 5 61 M R – -, No OD Orbit ESS after OD 12M 1M
L – Et, FS Orbit
M, male; F, Female; R, right; L, left; Et, Ethmoid sinus; MS, Maxillary sinus; FS, Frontal sinus; SS, Sphenoid sinus; ESS, Endoscopic sinus surgery; OD, Orbital decompression.
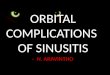
Fig. 2. The mechanism of obstructing the drainage from frontal sinus depending on the superior attachment of the uncinate process (UP). Uncinate process ( ∗) attached to lamina papyracea (A). Removal of superior attachment of UP by OD leads to obstruction of outflow tracts from frontal sinus (arrowheads). UP attached to cribriform plate (B). Orbital fat migrates into middle meatus, but wider outflow tracts would less likely to be obstructed.
p
s
3
a
W
p
e
o
s
b
o
b
T
i
p
p
t
c
m
U
c
a
m
1
o
r
d
1
o
s
i
ain and eye swelling. Characteristic of all patients werehown in Table 1 .
. Discussion
Orbital decompression surgery for Graves’s orbitopathy is technique that varies among institutions and departments.
hile transconjunctival and transcarnuncular approaches areopular among ophthalmologists [6 , 7] , recently the transnasalndoscopic approach has come into use among otolaryngol-gists [8 , 9] . Our co-author adopted the balanced decompres-ion, which includes the removal of medial and lateral orbitalony wall. Regardless of the surgical methods, the medialrbital wall (lamina papyracea) is usually removed and or-ital fat would migrate into ethmoid sinus to some extent.hough Orbital fat decompression might be preferable only
n terms of sinusitis [10] , the optimal choice of surgical ap-roach for Graves’ orbitopathy is beyond the scope of this
Please cite this article as: S. Tatehara, G. Inokuchi and H. Takeda et al., FrontAuris Nasus Larynx, https:// doi.org/ 10.1016/ j.anl.2020.01.011
aper. The issue is the difficulty of predicting to what extenthe middle meatus would be blocked by the migrated orbitalontents.
Frontal sinus outflow tracts were classified into two types,edial or lateral to the UP [11] . The superior attachment ofP was reported to be lamina papyracea (type 1/2, 63%),
ribriform plate (type 3/4, 15%), skull base (type 5, 14%),nd middle turbinate (type 6, 8%) [12] . Frontal sinusitis wasost common in attachment type of lamina papyracea, type
/2. Outlet tracts from frontal sinus in type 1/2 would beriginally narrow and easily blocked by orbital fat when ODemoved superior attachment of UP ( Fig. 2 A). Frontal sinusrainage is less likely to be obstructed in Type 3/4 than type/2 ( Fig. 2 B). The UP superior attachment was type 1/2 inur series of newly (3 sides) and worsening (1 side) frontalinusitis after OD.
The draft guideline for Graves’s orbitopathy was releasedn 2018 by Japan thyroid association. As this guideline rec-
al sinusitis associated with orbital decompression for Graves’ orbitopathy,

4 S. Tatehara, G. Inokuchi and H. Takeda et al. / Auris Nasus Larynx xxx (xxxx) xxx
ARTICLE IN PRESS
JID: ANL [mNS; February 19, 2020;21:9 ]
Fig. 3. Pre and post-ESS CT and endoscopic view (Case 3). Pre-OD CT revealed sinusitis in bilateral ethmoid and right maxillary sinuses (A). No soft tissue density was observed 3 months after ESS (B). Orbital fat ( ∗) migrated to middle meatus after OD, but outflow tracts from frontal sinuses were widely kept open by EMLP before OD (C).
D
p
R
[
[
[
ommends MRI evaluation of severity for Graves’s orbitopathy,the rate of detecting comorbid sinusitis might increase there-after. There are no practical guidelines about the managementof sinusitis associated with Graves’s orbitopathy. The inci-dence of sinusitis after OD was reported from 3.5% to 6.3%[2 , 3 , 8] . Those patients were often required ESS after OD.
The surgical approach for obstructive sinusitis after ODis challenging. It is impossible to use the customary trans-ethmoidal ESS and special attention needs to be paid to therisk of damaging the orbital contents. The outside-in modi-fied endoscopic Lothrop procedure [3] to the frontal sinus isrequired to keep wide enough drainage. The trans-septal ap-proach to the sphenoid sinus and extended inferior antrostomyvia the inferior meatus to maxillary sinus [5] are needed onlywhen symptomatic sinusitis existed in sphenoid and maxillarysinuses. However, sinus packing for hemorrhaging should beavoided since sinus infection could easily spread into orbit.Use of a surgical navigation system is therefore mandatoryto verify anatomical landmarks and avoid damaging orbitalcontents. Considering all these technical challenges and re-strictions, checkups for sinusitis and vigorous treatment be-fore OD should be considered. Limitation of this study wasthe method of retrospective case series. The true incidence ofsinusitis associated with OD and our speculation about themechanism of frontal sinusitis should be investigated in fur-ther study.
4. Conclusion
OD might develop or worsen the sinusitis by obstructingthe frontal sinus drainage. ESS including EMLP was usefulboth for the management and prevention of frontal sinusi-tis associated with OD. The superior attachment of uncinateprocess to lamina papyracea and removal might predict thehigh-risk group of frontal sinusitis after OD. Checkups forsinus CT and vigorous treatment against sinusitis before ODcould be recommended.
Disclosure statement
None of the authors has received financial support or hasa conflict of interest regarding this study.
Please cite this article as: S. Tatehara, G. Inokuchi and H. Takeda et al., FrontAuris Nasus Larynx, https:// doi.org/ 10.1016/ j.anl.2020.01.011
eclaration of Competing Interest
All authors have no conflict of interest related with thisaper.
eferences
[1] Wiersinga WM , Smit T , van der Gaag R , Mourits M , Koornneef L .Clinical presentation of Graves’ ophthalmopathy. Ophthalmic Res1989;21:73–82 .
[2] Antisdel JL , Gumber D , Holmes J , Sindwani R . Management ofsinonasal complications after endoscopic orbital decompression forGraves’ orbitopathy. Laryngoscope 2013;123:2094–8 .
[3] Carrasco JR , Castillo I , Bilyk JR , Pribitkin EA , Savino PJ . Incidenceof infraorbital hypesthesia and sinusitis after orbital decompression forthyroid-related orbitopathy: a comparison of surgical techniques. Oph-thalmic Plast Reconstr Surg 2005;21:188–91 .
[4] Chin D , Snidvongs K , Kalish L , Sacks R , Harvey RJ . The outside-inapproach to the modified endoscopic Lothrop procedure. Laryngoscope2012;122:1661–9 .
[5] Michel J , Radulesco T , Penicaud M , Dessi P . Extended inferior antros-tomy for maxillary sinus surgery. Clin Otolaryngol 2018;43:786–8 .
[6] Sellari-Franceschini S , Dallan I , Bajraktari A , Fiacchini G , Nardi M ,Rocchi R , et al. Surgical complications in orbital decompression forGraves’ orbitopathy. Acta Otorhinolaryngol Ital 2016;36:265–74 .
[7] Rootman DB . Orbital decompression for thyroid eye disease. Surv Oph-thalmol 2018;63:86–104 .
[8] Gulati S , Ueland HO , Haugen OH , Danielsen A , Rødahl E . Long-termfollow-up of patients with thyroid eye disease treated with endoscopicorbital decompression. Acta Ophthalmol 2015;93:178–83 .
[9] Tyler MA , Zhang CC , Saini AT , Yao WC . Cutting-edge endonasal surgi-cal approaches to thyroid ophthalmopathy. Laryngoscope Investig Oto-laryngol 2018;26(3(2)):100–4 .
10] Cheng AM , Wei YH , Tighe S , Sheha H , Liao SL . Long-term outcomesof orbital fat decompression in Graves’ orbitopathy. Br J Ophthalmol2018;102:69–73 .
11] Landsberg R , Friedman M . A computer-assisted anatomical study of thenasofrontal region. Laryngoscope 2001;111:2125–30 .
12] Turgut S , Ercan I , Sayin I , Basak M . The relationship between frontalsinusitis and localization of the frontal sinus outflow tract: a comput-er-assisted anatomical and clinical study. Arch Otolaryngol Head NeckSurg 2005;131:518–22 .
al sinusitis associated with orbital decompression for Graves’ orbitopathy,