Embed Size (px)
Citation preview
PATIENT HISTORY WORKSHEET
Please complete this entire 4 page form to allow us to update your prior information into our shared Electronic Medical Record
Gender: G Male G Female
Phone: Home: (_____)____________ Cell: (_____)____________ Work: (_____)____________
MEDICATIONSList any medications you take, prescription and nonprescription, and their dosage: G No medications
Medication
1. ____________________________________
2. ____________________________________
3. ____________________________________
4. ____________________________________
5. ____________________________________
6. ____________________________________
7. ____________________________________
8. ____________________________________
Dose
______________________________________
______________________________________
______________________________________
______________________________________
______________________________________
______________________________________
______________________________________
______________________________________
Preferred Pharmacy
Pharmacy: ___________________________________ Phone Number: ___________________________________
Address: _____________________________________ City: ____________________________________________
ALLERGIES & REACTIONS Please list any significant reactions you have to medications or foods: G None Medications: Latex: Aspirin: IV Contrast: Penicillin: Insect Stings: Sulfa (Bactrim): Food Reactions: Others:
For Office Use Only: Form to be SHREDDED after abstraction. Not for scanning into Med Rec
Rev.12/11 Page 1 of 4
Full Name: Address: City, State, Zip: Date of Birth:
Date of Service:
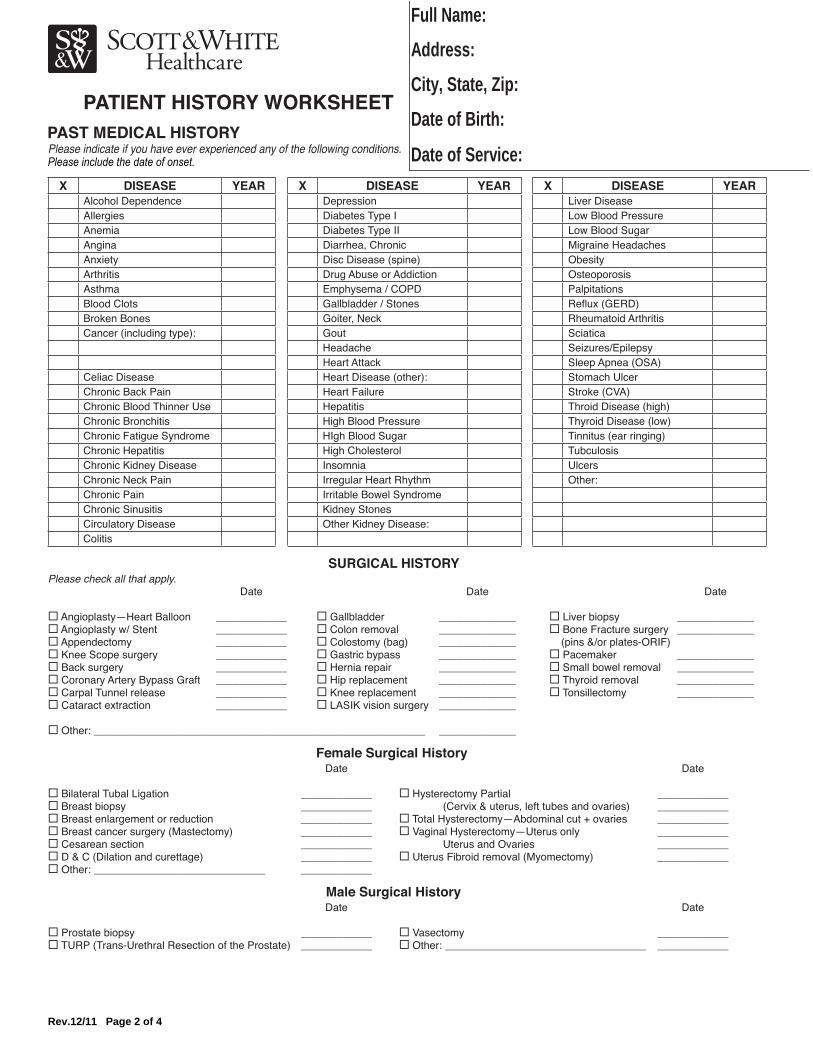
PATIENT HISTORY WORKSHEETPAST MEDICAL HISTORY
Rev.12/11 Page 2 of 4
X DISEASE YEAR X DISEASE YEAR X DISEASE YEARAlcohol Dependence Depression Liver DiseaseAllergies Diabetes Type I Low Blood PressureAnemia Diabetes Type II Low Blood SugarAngina Diarrhea, Chronic Migraine HeadachesAnxiety Disc Disease (spine) ObesityArthritis Drug Abuse or Addiction OsteoporosisAsthma Emphysema / COPD PalpitationsBlood Clots Gallbladder / Stones Reflux (GERD)Broken Bones Goiter, Neck Rheumatoid ArthritisCancer (including type): Gout Sciatica
Headache Seizures/EpilepsyHeart Attack Sleep Apnea (OSA)
Celiac Disease Heart Disease (other): Stomach UlcerChronic Back Pain Heart Failure Stroke (CVA)Chronic Blood Thinner Use Hepatitis Throid Disease (high)Chronic Bronchitis High Blood Pressure Thyroid Disease (low)Chronic Fatigue Syndrome HIgh Blood Sugar Tinnitus (ear ringing)Chronic Hepatitis High Cholesterol TubculosisChronic Kidney Disease Insomnia UlcersChronic Neck Pain Irregular Heart Rhythm Other:Chronic Pain Irritable Bowel SyndromeChronic Sinusitis Kidney StonesCirculatory Disease Other Kidney Disease:Colitis
SURGICAL HISTORYPlease check all that apply. Date Date Date
G Angioplasty—Heart Balloon ____________ G Gallbladder _____________ G Liver biopsy _____________G Angioplasty w/ Stent ____________ G Colon removal _____________ G Bone Fracture surgery _____________G Appendectomy ____________ G Colostomy (bag) _____________ (pins &/or plates-ORIF) G Knee Scope surgery ____________ G Gastric bypass _____________ G Pacemaker _____________G Back surgery ____________ G Hernia repair _____________ G Small bowel removal _____________G Coronary Artery Bypass Graft ____________ G Hip replacement _____________ G Thyroid removal _____________G Carpal Tunnel release ____________ G Knee replacement _____________ G Tonsillectomy _____________G Cataract extraction ____________ G LASIK vision surgery _____________
G Other: ________________________________________________________ _____________
Female Surgical History Date Date
G Bilateral Tubal Ligation ____________ G Hysterectomy Partial ____________G Breast biopsy ____________ (Cervix & uterus, left tubes and ovaries) ____________G Breast enlargement or reduction ____________ G Total Hysterectomy—Abdominal cut + ovaries ____________G Breast cancer surgery (Mastectomy) ____________ G Vaginal Hysterectomy—Uterus only ____________G Cesarean section ____________ Uterus and Ovaries ____________G D & C (Dilation and curettage) ____________ G Uterus Fibroid removal (Myomectomy) ____________G Other: _____________________________ ____________
Male Surgical History Date Date
G Prostate biopsy ____________ G Vasectomy ____________G TURP (Trans-Urethral Resection of the Prostate) ____________ G Other: __________________________________ ____________
Full Name: Address: City, State, Zip: Date of Birth:
Date of Service: Please indicate if you have ever experienced any of the following conditions. Please include the date of onset.
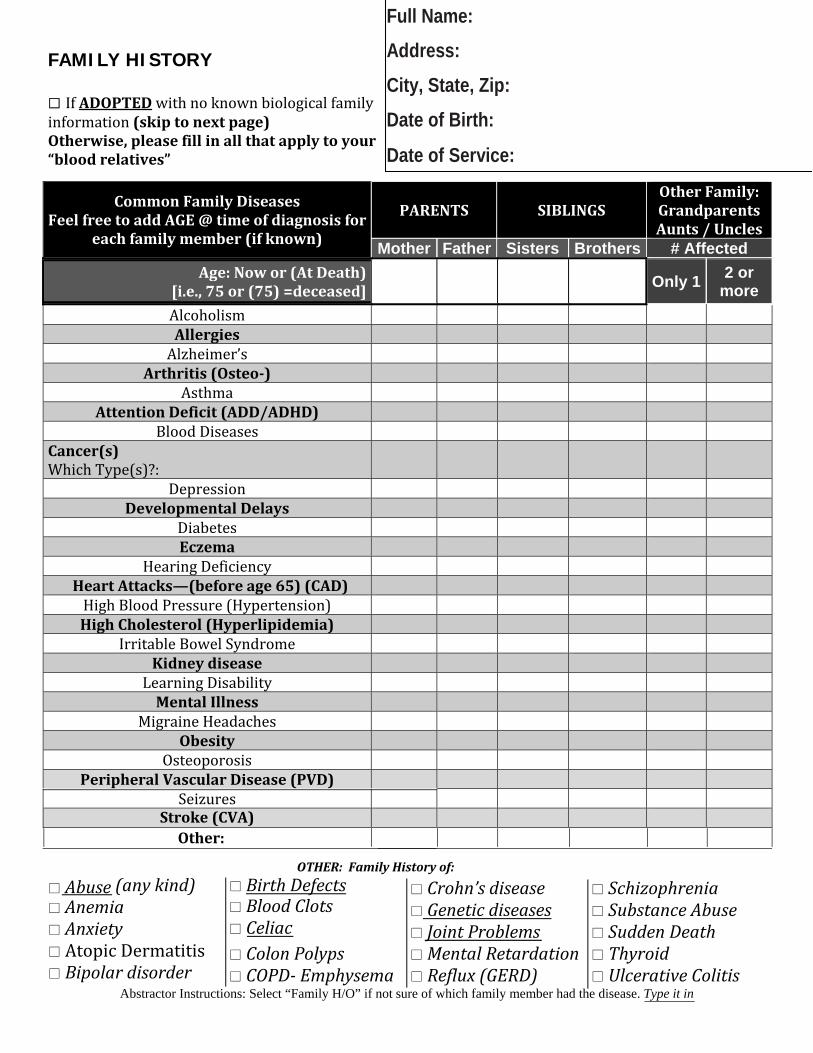
FAMILY HISTORY
If ADOPTED with no known biological family information (skip to next page) Otherwise, please fill in all that apply to your “blood relatives”
Common Family Diseases Feel free to add AGE @ time of diagnosis for
each family member (if known)
PARENTS SIBLINGS Other Family: Grandparents Aunts / Uncles
Mother Father Sisters Brothers # Affected Age: Now or (At Death)
[i.e., 75 or (75) =deceased] Only 1 2 or
more Alcoholism Allergies Alzheimer’s
Arthritis (Osteo) Asthma
Attention Deficit (ADD/ADHD) Blood Diseases
Cancer(s) Which Type(s)?:
Depression Developmental Delays
Diabetes Eczema
Hearing Deficiency Heart Attacks—(before age 65) (CAD) High Blood Pressure (Hypertension) High Cholesterol (Hyperlipidemia)
Irritable Bowel Syndrome Kidney disease Learning Disability Mental Illness
Migraine Headaches Obesity
Osteoporosis Peripheral Vascular Disease (PVD)
Seizures
OTHER: Family History of: Abuse (any kind) Anemia Anxiety Atopic Dermatitis Bipolar disorder
Birth Defects Blood Clots Celiac Colon Polyps COPD Emphysema
Crohn’s disease Genetic diseases Joint Problems Mental Retardation Reflux (GERD)
Schizophrenia Substance Abuse Sudden Death Thyroid Ulcerative Colitis
Abstractor Instructions: Select “Family H/O” if not sure of which family member had the disease. Type it in
Full Name: Address: City, State, Zip: Date of Birth:
Date of Service:
Stroke (CVA)
Other:
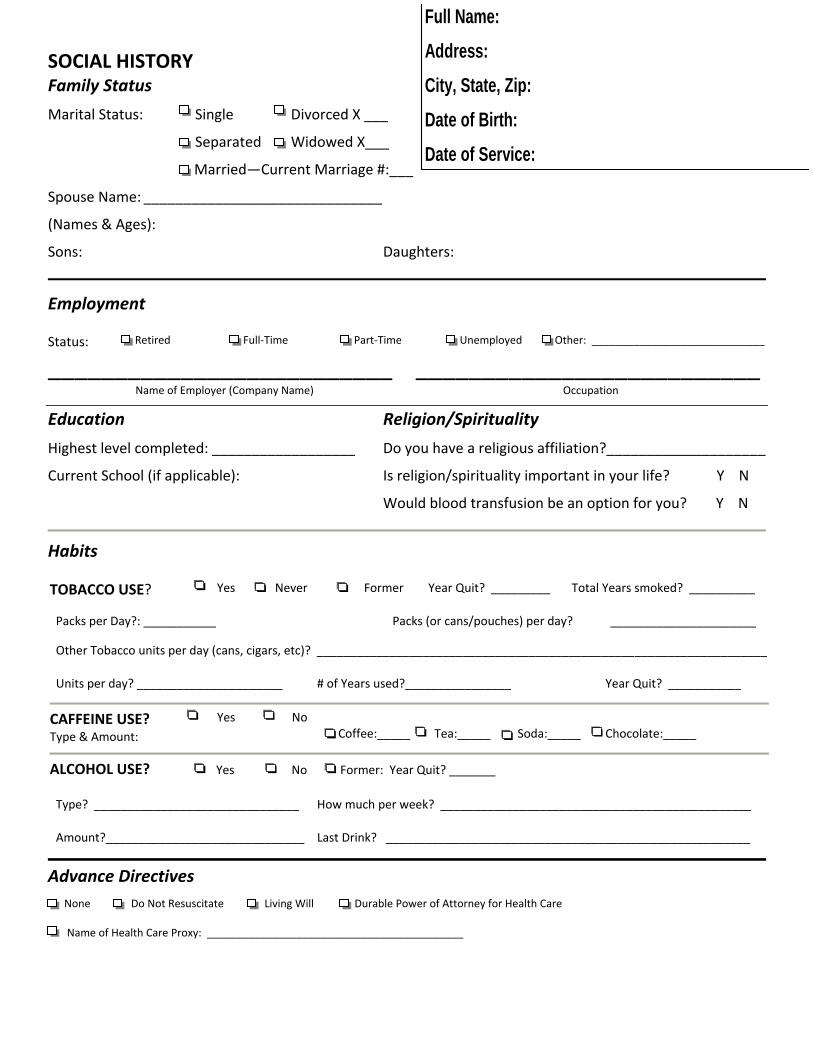
SOCIAL HISTORY Family Status
Marital Status: Single Divorced X ___
Separated Widowed X___
Married—Current Marriage #:___
Spouse Name: ______________________________
(Names & Ages):
Sons: Daughters:
Employment
Status: Retired Full‐Time Part‐Time Unemployed Other: _____________________________
__________________________ __________________________Name of Employer (Company Name) Occupation
Education Religion/Spirituality
Highest level completed: __________________ Do you have a religious affiliation?____________________ Current School (if applicable): Is religion/spirituality important in your life? Y N
Would blood transfusion be an option for you? Y N
Habits
TOBACCO USE? Yes Never Former Year Quit? _________ Total Years smoked? __________
Packs per Day?: ___________ Packs (or cans/pouches) per day? ______________________
Other Tobacco units per day (cans, cigars, etc)? ____________________________________________________________________ Units per day? ______________________
# of Years used?________________
Year Quit? ___________
CAFFEINE USE? Type & Amount:
Yes No Coffee:_____ Tea:_____ Soda:_____
Chocolate:_____
ALCOHOL USE? Yes No Former: Year Quit? _______ Type? _______________________________ How much per week? _______________________________________________ Amount?______________________________
Last Drink? _______________________________________________________
Advance Directives
Rev. 4/11 Page 4 of 4
None Do Not Resuscitate Living Will Durable Power of Attorney for Health Care
Name of Health Care Proxy: ___________________________________________
Full Name:Address: City, State, Zip: Date of Birth: Date of Service:





























