Embed Size (px)
Citation preview

REVIEW ARTICLE
Fumaric acid esters for psoriasis: a systematic review
D. Smith1
Received: 15 November 2015 / Accepted: 16 May 2016 / Published online: 7 June 2016
� Royal Academy of Medicine in Ireland 2016
Abstract
Background Psoriasis is a chronic skin disease associated
with increased morbidity and mortality. Effective and safe
long term treatment options are required tomanage the illness
successfully. A number of systemic agents are available,
however, each of them has potentially significant side effects.
Fumaric acid esters (FAE) are used first line in Germany for
the management of moderate to severe psoriasis, however,
their use in Ireland is on an unlicensed basis (Clinical and
Experimental Dermatology 37:786–801, 2012).
Objectives The purpose of this literature review is to
evaluate the efficacy and safety of FAEs in the manage-
ment of moderate to severe psoriasis in adult patients. The
reviewer intends to systematically review all available lit-
erature on the efficacy and/or safety of fumaric acid esters
in the management of moderate to severe psoriasis in adult
patients.
Methods A systematic review of the literature was per-
formed by one reviewer. The PubMed, TRIP, Embase,
and Cochrane Collaboration databases were systemati-
cally interrogated to include randomised controlled tri-
als, cohort studies and case studies evaluating the
efficacy and/or safety of FAEs in the management of
moderate to severe psoriasis in adult patients. Inclusion
criteria were studies which included adults over 18 years
of age, with a diagnosis of moderate to severe chronic
plaque psoriasis, who were treated with FAEs and no
other systemic anti-psoriatic agents concurrently.
Exclusion criteria were studies involving children, mild
psoriasis, studies which did not include patients with
chronic plaque psoriasis, the use of FAE for the man-
agement of illnesses other than psoriasis, and patients
treated with more than one systemic anti-psoriatic agent
concurrently.
Results In total 19 articles were selected for review
including 2 randomised placebo controlled trials, 1 non-
randomised comparative study, 7 retrospective cohort
studies, 2 prospective cohort studies and 7 case studies.
The findings suggest that FAEs are a safe and effective
treatment option for the management of moderate to
severe psoriasis in adult patients. Gastrointestinal side
effects may occur on treatment initiation and may be
minimised by slow dose titration. Lymphocytopenia and
eosinophilia are common, however, they are rarely of
significance and there is no high level of evidence avail-
able to suggest a resultant increased risk of infection or
malignancy. Rarely alterations of renal and hepatic
function may occur, however, these are largely reversible
on treatment withdrawal.
Conclusion In conclusion, the use of FAE in the man-
agement of moderate to severe psoriasis is a promising
treatment option, especially for those patients intolerant
of, or unresponsive to other agents. If blood parameters
are closely monitored during treatment as per the Euro-
pean Medicine Agencies guidelines (European Medicines
Agency, ‘Updated recommendations to minimise the risk
of the rare brain infection PML with Tecfidera’, http://
www.ema.europa.eu/docs/en_GB/document_library/Press_
release/2015/10/WC500196017.pdf, 2015) they may be
safely used in practice. The licensing of FAEs in Ireland for
the treatment of moderate to severe psoriasis would be
desirable, increasing available treatment options.
Keywords Fumaric acid esters � Fumaderm � Psoriasis
& D. Smith
1 Department of Dermatology, University Hospital Limerick,
Limerick, Ireland
123
Ir J Med Sci (2017) 186:161–177
DOI 10.1007/s11845-016-1470-2

Introduction
Psoriasis is a chronic skin condition with systemic mani-
festations, which presents in 2–3 % of the population
[20, 24]. The disease typically has an early onset, usually
between the ages of 20 and 30. It also has a chronic
relapsing nature [6, 18]. Recent epidemiological studies
have highlighted the association between moderate to
severe psoriasis and the metabolic syndrome and cardio-
vascular disease [26]. Psoriasis patients also have a higher
incidence of depressive illness and a decreased life
expectancy [6, 26]. Given the high morbidity and increased
mortality associated with moderate to severe psoriasis
effective, affordable and safe long term treatment options
are essential.
European guidelines (2009) have focused on the man-
agement of chronic plaque psoriasis which accounts for
more than 80 % of cases. This variant is defined by sharply
demarcated, erythematous and scaly plaques, typically on
extensor surfaces [18]. Tools for assessing severity include
the Psoriasis Area and Severity Index (PASI), with mod-
erate to severe disease being defined as a PASI of[10
[18]. In addition other measures such as the Physicians
Global Assessment of disease severity (PGA), body surface
area (BSA), or quality of life indices such as the Impact of
Psoriasis on health related quality of life (HRQoL) may be
used [18]. For moderate to severe disease phototherapy,
systemic agents and biologics may be used [18]. However,
many treatment modalities carry the risk of significant side
effects.
While phototherapy is a safe treatment option, there is a
risk of actinic damage, premature skin aging and potential
carcinogenic effects [18]. In addition, many patients over
time have disease which becomes refractory to ultraviolet
light.
Systemic antipsoriatic agents include methotrexate,
cyclosporin and fumaric acid esters. Methotrexate is an
effective treatment modality. Although it is potentially
hepatotoxic, the vast majority of patients do not suffer
hepatic damage from methotrexate as it is used in pso-
riasis. Methotrexate is also teratogenic, this necessitates
that patients use effective contraception during therapy
and for 6 months post-methotrexate. While cyclosporin
therapy is valuable acutely, long term use is not advo-
cated given the risk of cutaneous malignancies, lym-
phoma, raised blood pressure and nephrotoxicity [6].
Topical and oral retinoids may also be used; however,
these are contraindicated during pregnancy and concep-
tion and may cause hypertriglyceridemia [6]. As with
methotrexate, alcohol abuse with retinoids is also prob-
lematic as it is associated with an increased risk of
hepatic toxicity.
The biological therapies licensed for psoriasis consist of
monoclonal antibodies such as infliximab, adalimumab and
ustekinumab. Biologicals or monoclonal antibodies are
highly effective; however, they may pose an increased risk
of immunosuppression, and are an expensive treatment
modality [6, 18]. There is a theoretical risk of increased
haematological malignancies; however, there is no research
evidence that biological agents used for psoriasis cause an
increased risk of lymphoma and/or haematological malig-
nancies [6].
Systemic therapy with fumaric acid esters (FAEs) has
been licensed in Germany since 1994 for the treatment of
moderate to severe psoriasis [18]. Licensed preparations
fumaderm initial and fumaderm are available. Both contain
a mixture of dimethylfumarate (DMF), and three salts of
ethyl hydrogen fumarate. DMF is considered to be the
active ingredient. FAEs are thought to have immunomod-
ulatory, anti-inflammatory, antiproliferative and apoptotic
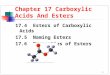
actions on activated T cells [9]. A standard dose protocol
(Fig. 1) is recommended whereby the dose is gradually
increased to improve tolerance. Individual dose adjustment
is then made according to therapeutic response; the highest
daily recommended dose is 1.2 g (equals 720 mg DMF, 6
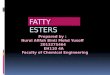
tablets) [18]. During therapy full blood count, liver
enzymes, urine sediment and serum creatinine must be
recorded (Fig. 2).
In the UK and Ireland the use of FAEs is on an irregular
and unlicensed basis [9]. It is unclear why fumaric acid
esters are not yet licensed for the treatment of moderate to
severe psoriasis in Ireland, while they have been success-
fully used to manage psoriasis in Germany for over
30 years. The use of such agents could offer the promise of
a safe, and effective long term treatment modality which is
more cost efficient than biological agents [11]. They also
have a 60 % 4-year drug survival, comparable with bio-
logical agents [11].
Fig. 1 FAE dosage scheme. With permission, Pathirana et al. [18]
162 Ir J Med Sci
123

While there have been some systematic reviews and
meta analyses on the safety of treatments for moderate to
severe psoriasis [15, 22], the author is unaware of any
literature reviews looking exclusively at the efficacy and/or
safety of FAEs in the management of moderate to severe
psoriasis in adult patients. The aim of this literature review
is to evaluate the efficacy and safety of FAE therapy in the
management of moderate to severe psoriasis in adult
patients.
Methods
One reviewer independently performed a literature review
of studies investigating the efficacy and/or safety of
fumaric acid ester use in the treatment of moderate to
severe psoriasis in adult patients published between Jan-
uary 1972 and December 2014. Case studies pertaining to
adult patients with moderate to severe chronic plaque
psoriasis which included evidence on safety and potential
adverse events were also selected for inclusion.
The PubMed, TRIP, Embase and Cochrane Collabora-
tion databases were systematically searched using the fol-
lowing combination of Medical Subject Headings (MeSH):
‘Psoriasis or Psoriatic AND fumaric acids or Fumarate
esters or fumarates or dimethylfumarate or fumaderm or
FAE AND toxicity or toxic or toxin or toxins or effect or
effects or outcome or outcomes or follow up or follow-up’.
The literature search was limited to articles written in
English. All references obtained from the databases were
screened. After all articles were identified, the reference
lists of each article were screened for additional relevant
articles.
Relevant studies were initially detected by reviewing the
title and abstract, and for the remaining studies by
reviewing the complete article. The literature review
included randomised controlled trials, case control studies,
cohort studies and case reports.
Inclusion criteria (Fig. 3) were adults over 18 years of
age, with a diagnosis of moderate to severe chronic plaque
psoriasis (and other variants if included), who were treated
with fumaric acid esters and no other systemic anti-psori-
atic agents concurrently. Exclusion criteria (Fig. 3) were
studies involving children, mild psoriasis, studies which
did not include patients with chronic plaque psoriasis, the
use of FAE for the management of illnesses other than
psoriasis, and patients treated with more than one systemic
antipsoriatic agent concurrently. A statement from German
experts reported that FAEs should not be used in combi-
nation with other systemic agents due to a lack of clinical
evidence [14]; for this reason studies in which patients
were treated with more than one systemic antipsoriatic
agent concurrently were excluded from this literature
review. Figure 4 summarises the study selection process.
Results
A total of 248 articles were retrieved during the database
search, 44 of which were duplicates. Of the 204 articles,
156 were excluded by title (Fig. 5). 107 of these papers
did not answer the research question, 28 articles were
unavailable in English, 3 papers evaluated the use of
FAE therapy in patients with psoriasis and multiple
sclerosis, and 9 papers looked exclusively at the use of
FAEs in the management of multiple sclerosis. A further
6 papers were excluded by title as they evaluated the use
of FAE therapy in granulomatous skin disease, granu-
loma annulare, autoimmune myocarditis, necrobiosis
lipoidica, or sarcoidosis. A further 3 papers were
excluded by title as they evaluated the use of FAE
therapy in children.
24 articles were excluded after reading the abstract (see
Fig. 5), and 6 articles were excluded on reading the full
text. 2 of these articles evaluated the use of FAEs in
patients with mild psoriasis, and 4 studies included patients
treated with FAEs and another systemic antipsoriatic agent
concurrently.
On hand searching the reference lists of selected articles,
1 further study was selected for inclusion in the review.
Fig. 2 FAE laboratory controls. With permission, Pathirana et al. [18]
Ir J Med Sci 163
123

In light of the specific aims of the study and strict
inclusion criteria, only 19 articles were finally included for
full review. The final studies included were 2 randomised
placebo controlled trials, 1 non-randomised comparative
study, 7 retrospective cohort studies, 2 prospective cohort
studies and 7 case studies. On completion of the study
selection process, data concerning all outcomes of interest
were extracted from all eligible studies and entered into
table format for evaluation (see Tables 1 and 2).
Discussion
In answer to the review question on the efficacy and safety
of fumaric acid esters in the management of moderate to
severe psoriasis in adult patients, this review found 19
studies that met the inclusion criteria. These included 2
randomised placebo controlled trials, 1 non-randomised
comparative study, 7 retrospective cohort studies, 2
prospective cohort studies and 7 case studies. The search
was limited to papers in the English language, which may
have introduced language bias. The references of each
article were searched; however, key people within the field
of psoriasis were not contacted to see if they had any
unpublished literature which could be included in the
review.
All studies examined the efficacy and/or safety of
fumaric acid use in the treatment of adults with moderate to
severe psoriasis. While all studies included participants
with chronic plaque psoriasis, some studies also included
patients with nail psoriasis, palmopustular and guttate
psoriasis. The majority of studies included patients treated
Fig. 3 Inclusion and exclusion
criteria
164 Ir J Med Sci
123

with FAE according to a standard dose protocol as previ-
ously described. The bulk of the studies were completed in
tertiary referral centres (Table 2).
Efficacy
Treatment with FAEs is suggested for adults with moderate
to severe psoriasis [18]. While they are employed as a first
line therapy in Germany, their use in Ireland remains
unlicensed [9]. Two randomised controlled trials [1, 16]
met the inclusion criteria for this literature review and both
demonstrated a statistically significant treatment response
for FAE therapy. Furthermore, all other included studies
demonstrated an improvement in the majority of psoriasis
patients managed with FAE therapy, however, there was
significant heterogeneity between the outcome measures of
treatment efficacy in the included studies.
The majority of patients were managed according to a
standard dose protocol as previously outlined [18]. Treat-
ment response varied from 82 % [4, 7] to 55 % [8]. Disease
flare on treatment initiation leading to discontinuation was
rarely reported [8, 9, 23]; however, this may have been due
to discontinuation of other systemic antipsoriatic agents
[23].
In addition, a previous lack of response to other sys-
temic agents did not prevent a good treatment response to
FAEs [8]; therefore, they may be a valuable treatment
option for patients who fail to respond to other agents.Fig. 4 Selection process for relevant citations
Fig. 5 Overview of study
selection process
Ir J Med Sci 165
123

Table
1Summaryofincluded
articles
Title
andauthor(s)
Studydesign
No.ofpatients
Intervention
Outcomemeasuresreported
Results
HeelanandMarkham
(2012).‘Fumaric
acid
esters
asa
suitable
firstline
treatm
entforsevere
psoriasis:an
Irish
experience’[9]
Retrospective
cohortstudy.
Single
regional
referral
centre
45(28men,17women).Age
range21–71years.42had
chronic
plaque,
2had
palmoplantarand1had
nail
psoriasis
Standarddose
protocol.The
mediantreatm
entdurationof
thecohortincludingthe
ongoingtreatm
entwas
11.2
months
Notreported
32Patients
(71%)showed
asignificant
improvem
entin
theirpsoriasis
Noim
provem
entwas
seen
in7patients
(16%).1(2
%)showed
worseningof
thedisease,and5(11%)wereunableto
tolerate
treatm
ent
Adverse
events
occurred
in66%—
diarrhoea
(44.4
%),abdominal
cram
ps
(40%),flushing(40%)andheadaches
(6.7
%).Adverse
eventsledto
treatm
ent
discontinuationin
33%
Lymphopenia
developed
in24%
(treatmentwas
discontinued
in1of
thesepatients).Eosinophilia
occurred
in
18%
(warrantedtreatm
entwithdrawal
in1patient).Trace
transientproteinuria
occurred
in3patients,proteinuria(1?)
occurred
in1patient
Nopatientrequired
treatm
entstoppage
dueto
deterioratingrenal
function.1
patienthad
atransientincrease
in
creatinine,
whichnarmalised
spontaneously
Reich,K
etal.(2009).
‘Efficacy
andsafety
of
fumaric
acid
esters
in
thelongterm
treatm
entof
psoriasis—
a
retrospectivestudy
(FUTURE)[20]
Retrospective
multicentre
cohortstudy
(163centres
included)
984patients58.2
%(572)were
male,
41.8
%(411)female.
Themeanagewas
50.5
years.87.3
%ofthe
included
patients
had
chronic
stable
psoriasis,38.3
%scalp
psoriasis,22.6
%nail
psoriasis
StandardFAEdose
protocol.
71%
were
treatedcontinually
withFAE
forat
least2years.Mean
treatm
entdurationforthis
patientcollectivewas
50months.Therapywith
FAEover
more
than
3years
(withinterruptionsnolonger
than
6months)
was
administeredto
46%
ofthe
patients.Meantreatm
ent
durationforthiscollective
was
66months
Leucocytes,lymphocytes,
eosinophils,granulocytes,
serum
creatinine,
glutamyltransf-erase,alanine
aminotransfera-se
and
aspartate
aminotransfera-se.
Severityofskin
symptoms
was
assessed
byPhysician’s
Global
Assessm
ent(PGA)
andPsoriasis
Areaand
severityindex
(PASI).Data
werereported
from
baseline
andafter3,6,12,24,and36
ormore
monthsoftherapy
After
3monthsoftherapy30.8
%of
patientswere‘‘markedly
improved’’or
‘‘clear’’andan
additional
50%
of
patients‘‘slightlyim
proved’’
After
6monthsoftherapy67%
of
patientswere‘‘markedly
improved’’or
‘‘clear’’;after1yearthisdegreeof
improvem
entwas
documentedin
76%
ofpatients
41%
ofpatientshad
lymphcytopenia
(after
24months)
and12%
leucopenia
(after
24months)
Anelevationofliver
enzymes
(GGT,
ALATorASAT)occurred
in13%
of
patients(after
3months)
Anelevationofthecreatininelevel
occurred
in6%
(after
24months)
166 Ir J Med Sci
123

Table
1continued
Title
andauthor(s)
Studydesign
No.ofpatients
Intervention
Outcomemeasuresreported
Results
Brewer
andRogers
(2007).‘Fumaric
acid
esters
inthe
managem
entofsevere
psoriasis’[3]
Retrospective
cohortstudy
31patients(21men,10
women).Agerange
27–78years
old.93.5
%had
chronic
plaquepsoriasis
and
6.5
%had
palmoplantar
pustularpsoriasis
Standarddose
protocol
Fullbloodcount(FBC),urea,
electrolytes,creatinine,
liver
functiontests(LFTs),
urinalysis—
measuredat
baseline,
then
once
weekly
for1month,fortnightlyfor
2months,then
once
every
2months.Response
was
described
as‘excellent’ifthe
skin
was
clear/minim
al
psoriasis,‘good’ifa
significantim
provem
entwas
noted,and‘failed’ifthere
was
noresponse/intolerance
2Patientswithdrew
from
thestudyat
the
beginning(1
dueto
noncompliance,1
dueto
breastcancer)
Oftheremaining29patients,17(58.6
%)
showed
goodto
excellentim
provem
ent
4Patients
did
notrespondto
treatm
ent
27patients
(87.1
%)experiencedside
effects—
flushing(67.8
%),abdominal
cram
ps(48.4
%),diarrhoea
(61.3
%),
andnausea(16.1
%)
Side-effectsledto
withdrawal
of
treatm
entin
8patients(27.6
%)afteran
averageof3months.Gastrointestinal
(GI)(3),lymphopenia
(2),flushing(1),
fatigue(1),generalised
rash
(1)
Lymphopenia
occurred
in19patients
(61.3
%)—
This
resulted
in
discontinuationoftreatm
entin
2
patients
Leucopenia
developed
in5patients
(16.1
%),eosinophilia
in10(32.3
%)
Atransientrise
inliver
enzymes
occurred
in4(12.9
%)
Nochangein
serum
creatinineoccurred
inanypatient
Fikaet
al.
(2006).‘Fumaric
acid
esters
inpsoriasis’[7]
Retrospective
cohortstudy
11(5
men,6women).Age
range19–59years.73%
had
chronic
plaquepsoriasis
and
27%
guttatepsoriasis
Patients
weretreatedwithan
FAEregim
eaccordingto
published
guidelines
Clinical
exam
inationonly
9Patients(82%)showed
improvem
entin
theirpsoriasis.3patients
(27%)
discontinued
treatm
ent—
dueto
side
effectsin
2(22.2
%),lack
ofefficacy
(1)andlack
ofcompliance
(1).Side-
effectswereseen
inallpatients—
GI
(82%),flushingin
18%.
Lymphocytopenia
developed
during
treatm
entin
6patients(54%).
Transienteosinophilia
was
noticedin
3
patients(27%).Nosignificant
abnorm
alitieswerenotedin
renal
or
liver
function
Ir J Med Sci 167
123

Table
1continued
Title
andauthor(s)
Studydesign
No.ofpatients
Intervention
Outcomemeasuresreported
Results
Sladden
etal.(2006).
‘Fumaric
acid
esters
forseverepsoriasis:
theLeicestershire
experience’[23]
Retrospective
cohortstudy.
Single
centre
30patients(21men
and9
women).Agerange
31–62years.Allpatients
had
moderateorseverechronic
plaquepsoriasis
StandarddosingProtocol
Notreported
8Patients(27%)discontinued
FAE
therapy(range2–6weeks),alldueto
GI
side-effects.2patientsstopped
dueto
disease
flare(H
owever
both
had
recently
withdrawnmethotrexateoracitretin)
Treatmentwas
withdrawnin
1dueto
glomerulonephritis(noproven
causal
linkwithFAE)
Oftheremaining19patients,4showed
someim
provem
entin
theirpsoriasis,
and15were‘clear
orvirtually
clear’
13(of19)developed
lymphocytopenia,2
patientsrequired
dose
reductionas
a
result.2patents
developed
microscopic
haematuriabut,afternephrologyand
urologyreview,continued
FAE
treatm
ent
Harries
etal.(2005)
‘Fumaric
acid
esters
forseverepsoriasis:a
retrospectivereview
of58cases’
[8]
Retrospective
single
centre
cohortstudy
58patients25women
and33
men.Themeanageofthe
patients
was
47.2
years
(range14–77years).94%
had
chronic
plaquepsoriasis,
3%
guttatepsoriasis,3%
palmoplantarpustular
psoriasis
Eachpatientfollowed
an
individually
tailoredFAE
dose
regim
enbased
ona
standardprotocol
Notreported
32Patients
(55%)showed
improvem
ent
intheirpsoriasis.Noim
provem
entwas
seen
in28%
ofpatients.16%
showed
disease
worsening.Themeantimeto
initialim
provem
entwas
5.6
weeks
(range2–20weeks)
32(55%)discontinued
FAEtreatm
ent
dueto
subjectiveadverse
events
(15),
lack
ofefficacy
(12)andlaboratory
abnorm
alities(4)
Theremaining26patients
(45%)
continued
FAEtreatm
ent
Side-effectswerereported
intwo-thirds
ofpatients—
abdominal
pain(61%),
diarrhoea
(55%),flushing(45%),
nausea(21%)andmalaise
(15%)
Lymphocytopenia
developed
during
treatm
entin
57%.This
prompteddose
reductionin
2patients,andeventual
treatm
entwithdrawal
in1ofthese
patients
Atransienteosinophiliaoccurred
in31%;
thisrevertedto
norm
alin
allcases
4patientsshowed
elevated
liver
enzymes
promptingtreatm
entdiscontinuationin
3cases
168 Ir J Med Sci
123

Table
1continued
Title
andauthor(s)
Studydesign
No.ofpatients
Intervention
Outcomemeasuresreported
Results
Carboniet
al.(2004).
‘Fumaricacid
estersin
thetreatm
entof
psoriasis:an
Italian
experience’[4]
Prospective
cohortstudy
40patients(25males
and15
females).Agerange
18–72years.Moderateto
severeplaquepsoriasis
Dim
ethylfum-arate
was
given
atadaily
dose
of30–360mg
foraminim
um
of6months,
accordingto
astandarddose
protocol.Doseswere
gradually
reducedas
soonas
remissionoccurred
PASIscore.Clinical
and
photographic
documentation.
Bloodandurineat
0,15,30,
90and180daysandthen
every3months.
Haemachrome,
renal
and
hepatic
functiontests
33Patients
(82.5
%)achieved
complete
clinical
remissionwithFAEtreatm
ent:
8after3monthsand25after6months
Adverse
events,such
asintolerable
abdominal
cram
psandincoercible
diarrhoea,occurred
in4patientswho,
forthisreasoninterruptedtherapy
Hoefnagel
etal.(2003).
‘Longtern
safety
aspects
ofsystem
ic
therapywithfumaric
acid
esters
insevere
psoriasis’[10]
Retrospective
cohortstudy
66patients,41men
and25
women.94%
had
psoriasis
vulgaris,5%
had
guttate
psoriasis
and1patienthad
arthropathic
psoriasis
All66patientsweretreated
withindividually
differing
dosesofFAE.Attheonsetof
therapywithFAEthedose
was
gradually
builtupto
a
maxim
um
of6highstrength
tablets
in27(41%)of66
patients.Themean
maintenance
dosagewas
between3–4highstrength
tablets
per
day
Laboratory
param
eterswere
monitoredmonthly
duringthe
first6monthsoftreatm
ent
andthereafter
at3-m
onthly
intervals.Theseincluded
total
leucocyte
count,relative
percentages
oflymphocytes
andeosinophils,serum
creatinine,
andliver
enzymes
(ALT,GGT)
Adverse
events
werereported
in73%
andledto
treatm
entwithdrawal
in9
patients.Thesewereusually
mild—
flushing(55%),diarrhoea
(42%),
nausea(14%),tiredness(14%)and
stomachcomplaints
(12%)
In22(35%)arelativelymphocytopenia
existedat
thestartoftherapy.Ofthe41
patientswithoutarelative
lymphocytopenia
atthestartoftherapy,
31(76%)developed
thisaftertherapy
onset.Therapywas
permanently
discontinued
in4,temporarily
discontinued
in1,andthedose
reduced
in5.In
8patientsnoactionwas
taken,
andlymphocyte
countsincreased
spontaneouslyto[10%
Thecourseofthemedianleucocyte
count
duringaperiodof12years
oftreatm
ent
did
notshow
anymarked
alterations
Eosinophilia
occurred
in14%—
transient
inall,requiringnoaction
Elevated
LFTsoccurred
in25%.In
14an
isolatedelevationofGGTwas
observed.This
resolved
spontaneously
ornarmalised
afterdose
reductionin
all
but3patients.In
2patients
elevated
LFTswerethereasonto
withdraw
therapypermanentlyandin
1patientto
withdraw
temporarily
Elevated
serum
creatinineoccurred
in1
patient.ReintroductionofFAEsdid
not
altercreatininelevelsin
thispatient
Ir J Med Sci 169
123

Table
1continued
Title
andauthor(s)
Studydesign
No.ofpatients
Intervention
Outcomemeasuresreported
Results
Mrowietz
etal.(1998).
‘Treatmentofsevere
psoriasis
withfumaric
acid
esters:scientific
backgroundand
guidelines
for
therapeuticuse’[14]
Prospective
multicentre
study(12
dermatological
centres
in
Germany)
101patients,68male,
31
female.
Agerange
21–69years.Patients
with
severepsoriasisofdifferent
clinical
types
(e.g.,psoriasis
vulgaris.Guttatepsoriasis,
exanthem
atic
psoriasis)were
included
inthestudy
Standarddose
protocol.
Treatmentdurationwas
16weeks
PASIscore
was
assessed.
Pruritus,jointpainandnail
involvem
entwereassessed
usingascore
from
0to
4.
Patients
wereasked
for
adverse
events
atvisits.At
baselineandtreatm
entend
complete
skin
&physical
exam
wereperform
edto
detectanychanges
relatedto
therapy.Lab
values
measured
ateach
visitincluded:serum
creatinine.
Bloodureaand
nitrogen
(BUN),serum
glutamic
oxaloacetic—
transaminase,
serum
glutamic—
pyruvic
transaminase,GGT,uricacid,
LDH,alkalinephosphatase,
cholineesterase,bilirubin.
Serum
cholesteroland
triglycerides,electrolytes,
urinechem
istry,FBC
and
differential
count.Blood
pressure
andbodyweight
werealso
measured
70Patients
completedthestudy
31Discontinued
thestudydueto
adverse
events(G
Iin
5,flush
1,increasing
pruritus1,lack
ofefficacy
2,jobreasons
2,non-compliance
20)
Evaluationofoverallefficacy
showed
a
decreasein
PASIof80%
after
4monthsofFAEtherapy
Adecreaseoflymphocytesmore
than
50%
below
baselineoccurred
in10
patients
Duringweeks4and8meaneosinophil
countswereabovethenorm
alrange,but
allreturned
tonorm
alat
theendof
therapy
Nopatientshowed
changes
inrenal
function
Adverse
events
werereported
in69%
mainly
consistingofGIcomplaints
(56%)andflushing(51%)
170 Ir J Med Sci
123

Table
1continued
Title
andauthor(s)
Studydesign
No.ofpatients
Intervention
Outcomemeasuresreported
Results
Altmeyer
etal.(1994).
‘Antipsoriatic
effect
offumaric
acid
derivatives:resultsof
amulticenterdouble-
blindstudyin
100
patients’[1]
Randomised
double
blind
study
comparingthe
use
offumaric
acid
derivatives
withplacebo
100patients.Agerange
18–70years.
Psoriasis[
10%
ofbody
surfacearea,including
chronic
plaque,
exanthem
atic
guttate,
pustular,and
psoriatic
erythrodermaforat
least2years
Either
placeboordrugin
tablet
form
accordingto
auniform
randomisationschedule.The
drugwas
available
in‘initial’
and‘forte’
tablets.Thedose
was
escalatedaccordingto
a
standardprotocol.Patients
given
placebowere
administeredthesame
amountoftabletsas
thedrug
group
Laboratory
studiesmeasuredon
day
0,andafter
2,4,6,8,12,16weeks
including:haemoglobin,
erythrocyte,leucocyte,and
differential
counts;platelet
count;levelsofbilirubin,
creatinine,
urea,
uricacid,
glucose,alkaline-
phosphatase,
transaminases,
gam
ma-GT,cholesterol,
triglycerides,calcium,
sodium,potassium
and
urinalysis.Creatinine
clearance
was
determined
at
Oweeksandafter16weeks.
PASIscore
was
completed.
Pruritus,arthralgia,andnail
deform
itieswereassessed
on
thebasis
ofaclinical
score
from
0to
4.Ateach
visitboth
thephysician
andthepatient
wereasked
toassess
the
outcomeoftherapyandany
sideeffects
Asignificanttreatm
entdifference
usingthe
PASIscore(p\
0.0001)was
foundin
favourofthedruggroup.Inthedruggroup
71.3
%ofpatientsshowed
remission,
18%
showed
noresponse
and10.2
%
showed
deterioration.82%
oftheplacebo
groupremained
unchanged
ordeteriorated
Adverse
reactionsoccurred
in75.5
%of
thedruggroupand16%
oftheplacebo
group.Therewerenochanges
in
haemobin
orerythrocyte
countduring
the16weeks.Leucocytesshowed
a
milddecreasein
week8in
both
groups,
withnofurther
changes
afterthis
Eosinophilsshowed
asignificantincrease
inthedruggroupfrom
2%
(weekO)to
3.4
%(w
eek2)(p\
0.05)
Platelets,bilirubin,urea,
creatinine,
glucose,alkalinephosphatase,
transaminases,gam
maG
T,cholesterol,
triglycerides,andurinalysisdid
not
changesignificantlyin
either
group
Therewerenosignificantdifferencesin
creatinineclearance
ineither
group
KolbachandNieboer
(1992).‘Fumaric
acid
therapyin
psoriasis:
Resultsandside
effectsof2years
of
treatm
ent’[13]
Non-randomised
comparative
study(choice
oftherapywas
determined
by
patients
insurance)
196patients[18years
with
nummularandplaquetype
psoriasis
withat
least10%
involvem
entofbodysurface
TheDMFAEgroup(n
=129)
received
60mgcapsulesof
dim
ethylfuma-ricacid
esters,
increasedweekly
by60mgto
amaxim
um
of240mg/day.
TheFACgroup(n
=67)was
treatedwithfumaderm
‘mite’
initially,increasingto
fumaderm
‘forte’,whichwas
increasedweekly
toa
maxim
um
of4‘forte’
tablets
per
day
Therapeuticevaluationwas
doneat3–6.6–12,12–18,and
18–24months.Resultswere
scoredaccordingto
a
simplified
severityscore.
Improvem
entof[75%
was
sufficient,less
extensive
improvem
ent,deterioration
andexacerbationwerecalled
insufficient.Sideeffectswere
noted.Lab
testsincluded:
urinalysis,whitebloodcell
countwithdifferential,
haemoglobin,serum
creatinine,
bloodurea
nitrogen
(BUN),transaminase
andalkalinephosphatase
levels
After
24months55%
oftheFACgroup
continued
treatm
entas
opposedto
16%
oftheDMFAEgroup
50%
OftheFACgroupattained
sufficient
results.Thiswas
statisticallysignificant.
18%
oftheFACgroupstopped
dueto
sideeffects,26%
intheDMFAEgroup
Inthefirst6monthsGIcomplaints
were
most
frequentin
both
groups
Milddeviationsofliver
andrenal
function
wereseen
in3patientsin
theDMFAE
groupand1patientin
theFACgroup.
They
disappearedafterdiscontinuation.
Leucocytopenia
occurred
in4%
(not
specified
inwhichgroup)
After24months86%oftheDMFAEgroup
and81%
oftheFACgrouphad
lympho-
penia,discontinuationledtonorm
alisation
inmostcasesafterupto6months
Ir J Med Sci 171
123

Table
1continued
Title
andauthor(s)
Studydesign
No.ofpatients
Intervention
Outcomemeasuresreported
Results
Nugteren-H
uyinget
al.
(1990).‘Fumaric
acid
therapyforpsoriasis:
Arandomised,double
blind,placebo
controlled
trial’[16]
Randomised
double
blind,
placebo
controlled
trial
39psoriasispatients
(12
women
and27men).Age
range20–73years.Severe
psoriasis[
10%
body
surfacearea
Patients
wererandomly
assigned
to3groups.Group1
(n=
12)weretreatedwith
oralentericcoated
tablets
containingamixture
of
dim
ethylfuma-rate,and
magnesium,calcium
andzinc
monoethylfu-m
arate.Group2
Patients
weretreatedwith
oralentericcoated
tablets
containingoctylhydrogen
fumarate,andmagnesium
and
zincmonoethylfu-m
arate.
Group3Patientsweretreated
withaplacebo.Alltablets
had
thesameappearance,size
andcolour
Extentandactivityofskin
disease
was
assessed
by
estimatingthepercentageof
bodysurfaceaffected
with
psoriasisandbyscoringthe
degreeofinfiltrationand
scalingoftheplaques
(from
0
noinfiltrationorscaling,to
8
verysevereinfiltratingor
scaling).Thefollowinglab
investigationswere
perform
ed:ESR,leucocyte
differential
count,
haemoglobin,haematocrit,
urea,
creatinine,
AST,ALT,
lactate-dehydrogenase,
alkaline-phosphatase,
gam
ma
glutamyltransfe-rase,total
bilirubin,glucose
andprotein.
Urinalysisforlevelsof
glucose
andprotein
and24h
creatinineclearance
rate
Nodifferencesfoundbetweengroupsat
baseline.
Of39patients,34completed
thestudy
Group1—
themeanpercentageofbody
surfaceaffected
withpsoriasiswas
reducedfrom
21%
(atbaseline)
to
6.7
%after16weeks.Thiswas
statisticallysignificantfrom
groups2
and3(p
B0.01)
After
16weeksthescore
forscalingin
group1was
significantlylower
than
in
groups2and3(p
B0.0.1)
Ingroup1,6patients
showed
complete
clearance,and3showed
improvem
ent.
Ingroup2nosuch
resultsoccurred
and
ingroup3only
1patientshowed
improvem
ent.In
group1themainside
effectswereflushing(12),diarrhoea
(13),fatigue(7),andnausea(6).One
patientbecam
eilldueto
renal
insufficiency
Atransientrise
inliver
functiontests
occurred
in8patientsin
group1,and4
patientsin
group2
Transienteosinophilia
occurred
in5
patientsin
group1
Lymphopenia
occurred
in4patients
in
group1
172 Ir J Med Sci
123

Table
2Summaryofincluded
Casestudies
Title
andAuthor(s)
Patient(s)
Intervention
Casesummary
Erm
iset
al.(2013).‘PMLin
apatienttreated
withfumaric
acid’[5]
One74yearold
man
OralFAEtherapyfor3years
indosesofupto
120mgofdim
ethyl—
fumarateand95mgof
monoethyl—
fumarate,
each
taken
twicedaily
PMLwas
diagnosedduringtherapywithFAE,treatm
ent
was
discontinued.Differential
bloodcountrevealed
grade3lymphocytopenia.(Retrospectiveanalysis
revealedthat
thelymphocytopenia
had
reached
an
unrecognised
grade3statuswithin
1yearafterthe
initiationoftreatm
entwithFAE)
Reidet
al.(2013).‘D
eToniFanconiSyndrome
secondaryto
fumaric
acid
esters’[21]
Onefemaleage
37years
FAE240mgthreetimes
daily.18monthsoftherapy,
heldfor15monthswhilepregnant,reintroducedfor
7monthsbefore
thedevelopmentofDeToni
Fanconisyndrome
DeToniFanconisyndromedeveloped
duringFAE
therapy,thisresolved
within
4weeksoftreatm
ent
cessation.Thepatienthad
norm
allabparam
etersbefore
commencingtherapy
van
Oosten
etal.(2013).‘PMLin
apatient
treatedwithdim
ethylfumaratefrom
a
compoundingpharmacy’[25]
One43yearold
lady
420mgofPsorinovo(D
imethylfumaric
acid)
per
day
for6years
AdiagnosisofPMLwas
madewhilereceivingFAE
therapy,thiswas
subsequentlystopped.Haematologic
studiesrevealedapreviouslyunrecognised
lymphopenia,
withacountof200lymphocytesper
cubic
millimetre
(norm
alrange,
600–2900)
Barth
etal.(2011).‘M
alignantmelanoma
duringtreatm
entwithfumaric
acid
esters-
coincidence
ortreatm
entrelated?’
[2]
Patient1:45yearold
malePatient2:
74yearold
male
Both
patientsweretreatedwithFAE(unspecified
dose),Patient1for4yearsandPatient2for8years
Patient1Nosignificantrisk
factors
formelanoma.
A
nodularmelanoma(Breslow
depth
2.4
mm,Clark
level
IV)was
foundin
theleftpectoralregion.Follow-up
excisionandtwosentinel
lymphnodes
werefree
of
tumour.Patient2Developed
apigmentedskin
lesion
Breslow
depth
0.35mm,Clark
level
II(U
nderlyingrisk
factors
included
ahistory
ofchronic
actinic
dam
age,
squam
ouscellcarcinoma(SCC),methotrexate,
acitretin
andciclosporinuse.In
additiontherewas
ahistory
of
PUVA
andsunlampuse)
Ogilvie
etal.(2011).‘Proteinuriawithfumaric
acid
estertreatm
entforpsoriasis’[17]
Patient1:A
55year
old
malePatient2:
N/A
Patient3:A
58-yearold
lady
Patient1and3—
StandardFAEdose
protocolas
per
manufacturer
Patient1Had
developed
areducedglomerularfiltration
rateonciclosporin9yearspreviously,andhad
apossible
IgA
nephropathy.Within
2weeksofFAEtherapyhe
developed
proteinuriawithatraceofbloodonurinalysis.
FAEwas
stopped
butinvestigationsdid
notuncover
any
abnorm
alfindings.Within
2weeksofstoppingtheFAE,
proteinuriahad
resolved,andFAEwas
restarted
4monthslater.Within
3weeksofrestartingproteinuria
was
detected(‘???’).Once
more,discontinuationof
treatm
entwas
followed
byresolutionofproteinuria.
Patient3Within
1month
afterreachingthestandard
maxim
um
dose
ofFAE,thepatientdeveloped
proteinuria(‘???’)whichresolved
within
3monthsof
treatm
entcessation
Ir J Med Sci 173
123

A meaningful disease improvement may be seen after
6–8 weeks of therapy when FAEs are administered
according to a standard dose protocol [18], however, some
studies [20] demonstrate that a significant clinical effect
can be expected between weeks 12 and 24. Reich et al.
(2009) reported that rates of improvement and disease
clearance continued to increase up to 1 year after com-
mencing treatment. This information is important to ensure
that a final judgment of therapy success is not made pre-
maturely. Treatment failure should therefore not be
determined before 6 months of continuous treatment [20].
Safety and tolerability
Gastrointestinal symptoms and flushing
According to European guidelines, gastrointestinal adverse
effects may occur in up to 60 % of psoriasis patients
treated with FAEs, particularly in the first few weeks after
initiation of therapy [18]. Flush symptoms such as feeling
warm, reddening of the face, and headache lasting for
minutes to hours are also common upon treatment initia-
tion [18]. These symptoms were an extremely common
occurrence upon treatment initiation in the studies included
in this literature review [1, 3, 7–10, 13, 14, 16, 23].
Treatment withdrawal due to such adverse events ranged
from 33 % [9] to 18 % [13]. The literature review has
shown that these side effects are extremely common and
may be better tolerated, if therapy is commenced at a low
dose and gradually increased over a period of weeks [18].
Once remission has been achieved, the dose may be
reduced to a lower maintenance dose to maintain clinical
response while minimising the risk of side effects.
Alterations of full blood count
Leucocytopenia, lymphocytopenia and eosinophilia can be
observed during therapy with FAEs. If leucocytes drop
below 3000/lL and lymphocytes below 500/lL, the dose
must be reduced or the treatment stopped [18].
An increase in eosinophils is temporary and usually
observed between weeks 4 and 10 of treatment [18]. There
were no associated adverse events reported in any of the
studies described. Eosinophilia was frequently self-limiting
and rarely necessitated treatment withdrawal
[1, 3, 7, 8, 10, 14, 16]. However, Heelan and Markham
(2012) reported one patient who required treatment dis-
continuation due to eosinophilia.
The most frequently occurring change in blood count
was a relative lymphocytopenia [3, 7–10, 13, 14, 20, 23].
This infrequently required dose reduction for some patients
[8, 10, 23] or rarely treatment withdrawal [3, 8–10]. It has
been suggested that lymphocytopenia could be influencedTable
2continued
Title
andAuthor(s)
Patient(s)
Intervention
Casesummary
JenningsandMurphy(2009).‘Squam
ouscell
carcinomaas
acomplicationoffumaric
acid
esterim
munosuppression’[12]
A49yearold
male
FAEtherapyfor7weeks,withslow
dose
titrationas
per
manufacturer’sinstructions
Improvem
entin
psoriasis
at6weeks,butdeveloped
3
SCCs.Totallymphocyte
countduringthisperiodwas
reducedandlymphocytesubsetsrevealedlowCD4,CD8
andCD19counts.Thepatienthad
ahistory
ofsun
exposure,an
outdoorlifestyle,actinic
dam
age,
PUVA
use,methotrexate,
ciclosporin,andahistory
ofSCC
on
ciclosporin.FAEwas
discontinued
andsix-m
onth
follow-uphas
notrevealedanynew
SCCs
RaschkaandKoch
(1999).‘Longterm
treatm
ent
ofpsoriasis
usingfumaric
acid
preparations
canbeassociated
withsevereproxim
altubular
dam
age’
[19]
A38yearold
female
420mgfumaric
acid
b.i.d
for5years
Thepatientcomplained
offatigueandweaknessfor
4monthsas
wellas
polydipsiaof3±
4lper
day.A
proxim
altubulardam
agewithglycosuria,
hypophosphatem
ia,proteinuriaandhypuricemia
after
long-term
therapywithfumaric
acid
was
diagnosed.
FAEwas
stopped
immediately;symptomspersisted
for
6monthsaftercessationoftherapy
174 Ir J Med Sci
123

by previous use of other systemic agents in a number of
patients, or it may be an intrinsic characteristic of psoriasis,
however, studies on this are lacking [10]. Harries et al.
(2005) suggested that there may be a link between a
reduced lymphocyte count and a beneficial response to
treatment, noting that the reduced lymphocyte count may
be part of the therapeutic process. Dose reduction or ces-
sation of therapy should be considered in the face of a
significant lymphocytopenia [10].
There are some case studies of malignancy [2, 12] as
well as infections such as PML [5, 25] occurring in patients
treated with FAEs. However, in the latter cases, the
patients had unrecognised lymphocytopenia, the levels of
which merited treatment withdrawal. In October 2015 the
European Medicines Agency [27] reviewed cases of PML
which occurred with Fumaderm and Psorinovo, both used
to treat psoriasis. The EMA recommended that a complete
blood count be performed at the start of treatment and
suggested that in the presence of values outside the normal
range, treatment should not be started. During treatment,
blood cell counts should be monitored every 4 weeks; if
the lymphocyte count drops below 0.7 9 109/L, the dose
should be halved. If, during a follow-up check after
4 weeks, the lymphocyte count remains below this value,
treatment must be discontinued. If therapy is continued in
presence of a lymphocyte count below 0.7 9 109/L, the
risk of PML cannot be excluded. If the lymphocyte count
drops below 0.5 9 109/L, treatment should be
discontinued.
Overall, there is no high level of evidence to suggest an
increased risk of malignancy or infections when treated
with FAEs. However, prescribers must be alert to the
possibility of such occurrences given the potential
immunosuppression. Differential white cell counts must be
closely monitored during FAE therapy, and treatment
withdrawn if leucocytes or lymphocytes drop below the
aforementioned levels.
Nephrotoxicity
European guidelines suggest that occasionally proteinuria
may occur during therapy, but disappears after dose
reduction or cessation of treatment [18]. Nephrotoxicity is
generally regarded as a rare event; however, there are case
reports of proteinuria [9, 17], reversible renal insufficiency
[16], microscopic haematuria [23] and proximal tubular
damage [19, 21] associated with FAE therapy. Both
Hoefnagel et al. (2003) and Heelan and Markham (2012)
found one patient to have a transient increase in serum
creatinine while on FAE therapy. In the latter case, this
normalised spontaneously, while in the former case it
resolved on treatment discontinuation and did not recur on
later reintroduction of treatment. Ismail et al. (2014) noted
that one patient in their retrospective study required dis-
continuation of therapy due to a reversible creatinine rise.
Similarly, Reich et al. (2009) noted an elevated creatinine
in 6 % of their cohort at 24 months.
The cases of such renal injury were all reversible upon
treatment cessation; however, their occurrence reinforces
the need for strict monitoring of renal function while
patients are receiving FAEs. Urinalysis is also important in
screening for proximal renal tubular dysfunction [21].
European guidelines [18] recommend renal function tests
prior to treatment, monthly for the first 6 months of treat-
ment, with further testing according to clinical signs or risk
factors. It has been suggested that renal impairment may be
associated with an initial overdose of FAEs, therefore, slow
dose titration as per protocol may also help to reduce the
occurrence of renal impairment [1, 10].
Hepatotoxicity
In rare cases, an isolated increase in ALT or bilirubin may
be seen while undergoing FAE therapy [18]. Hoefnagel
et al. (2003) found this to occur in 25 % of 63 patients;
however, they doubted an association with FAE therapy.
Similarly, Harries et al. (2005) reported three patients who
had to discontinue therapy due to abnormalities of liver
function. The liver enzyme abnormalities resolved spon-
taneously or on dose reduction in nearly all cases. There
were no case reports of any patient suffering hepatic
impairment as a result of FAE therapy. Despite limited
evidence to link raised liver enzymes to fumaric acid ester
therapy, vigilant screening of hepatic function should also
occur during therapy.
Limitations
Finally, it needs to be acknowledged that this literature
review has important limitations. Methodological short
comings of some of the included studies may have com-
promised the overall results. Most of the selected studies
were limited by small sample size. There was also a large
heterogeneity between studies concerning the type of
psoriasis treated, as well as follow up and outcome mea-
sures utilised. The majority of the studies were also short
term. The review also included a number of case studies
which represent a weak level of evidence.
In addition to the aforementioned weaknesses, a large
number of studies (28) had to be excluded from the review
as they were not available in English. This undoubtedly
introduced a language bias. Publication bias may also have
been a factor as only published articles available from the
aforementioned databases were included. Involving greater
than one reviewer may have enhanced the validity of the
Ir J Med Sci 175
123

review. In addition, the review may have been more
comprehensive, if grey literature was included and key
researchers in the area were contacted for additional
research papers.
Conclusions
In light of the chronic nature of psoriasis, safe and effective
long term treatment options are of major importance. The
aim of this literature review was to evaluate the efficacy
and safety of fumaric acid esters in the management of
moderate to severe psoriasis in adult patients. 19 articles
were selected for review. Overall, the use of fumaric acid
esters for the treatment of moderate to severe psoriasis has
been shown to be an effective and safe long term treatment
agent.
Gastrointestinal side effects and flushing are common at
treatment initiation and may limit treatment. The occur-
rence of serious adverse events such as hepatic or renal
injury appears to be very rare, and although there are some
case reports of renal injury, these were all reversible upon
cessation of treatment. Haematological disturbances such
as moderate lymphocytopenia are common; however, there
is no high level of evidence available to suggest any
increased risk of malignancy.
The characteristic spectrum of adverse events which
may occur enables easy monitoring of patients during the
course of treatment [14]. FBC, liver enzymes, serum cre-
atinine and urinalysis must be vigilantly recorded [18]. If
the drug is monitored as per the manufacturer’s protocols,
it is likely to be a safe agent. For patients who experience
adverse reactions or intolerance of other systemic antip-
soriatic agents, FAEs may be a viable treatment alternative.
While this literature review only included studies in
which fumaric acid ester therapy was used in isolation to
manage moderate to severe psoriasis, studies such as that
completed by Ismail et al. (2014) suggest that FAEs may
be used safely in combination with other systemic and
biological agents. When used in combination with other
therapies, they may in fact facilitate dose reduction of more
toxic agents [26]. The use of fumaric acid esters in com-
bination with other treatment modalities would be a valu-
able topic for future research.
Fumaric acid ester therapy has been utilised for over
30 years for the management of psoriasis [26]. Fumaderm
is licensed in Germany for treating adults with moderate to
severe plaque psoriasis in whom topical therapy is not
effective. The licensing of FAEs in Ireland for the treat-
ment of moderate to severe psoriasis would be desirable,
increasing available treatment options. This systematic
review suggests that they are an effective long term treat-
ment option. They may be safely used in practice when
administered in accordance with the European Medicine
Agency guidelines [27].
Acknowledgments With special thanks to Dr Bart Ramsay, Con-
sultant Dermatologist, University Hospital Limerick.
References
1. Altmeyer PJ, Matthes U, Pawlak F et al (1994) Antipsoriatic
effect of fumaric acid derivatives: results of a multicenter double-
blind study in 100 patients. J Am Acad Dermatol 30:977–981
2. Barth D, Simon JC, Wetzig T (2011) ‘Malignant melanoma
during treatment with fumaric acid esters—coincidence or treat-
ment related? JDDG. J der Deutschen Dermatologischen
Gesellschaft 3:223–224
3. Brewer L, Rogers S (2007) Fumaric acid esters in the manage-
ment of severe psoriasis. Clin Exp Dermatol 32:246–249
4. Carboni I, De Felice C, De Simoni I et al (2004) Fumaric acid
esters in the treatment of psoriasis: an Italian experience. J Der-
matol Treat 15:23–26
5. Ermis U, Weis J, Schulz JB (2013) PML in a patient treated with
fumaric acid. N Engl J Med 368(17):1657–1658
6. Fairhurst DA, Ashcroft DM, Griffiths EM (2005) ‘Optimal
Management of Severe Plaque Form of Psoriasis. Am J Clin
Dermatol 6(5):283–294
7. Fika Z, Williams REA, Williamson DJ (2006) Fumaric acid
esters in psoriasis. Br J Dermatol 154(3):567–568
8. Harries MJ, Chalmers RJG, Griffiths CEM (2005) Fumaric acid
esters for severe psoriasis: a retrospective review of 58 cases. Br J
Dermatol 153:549–551
9. Heelan K, Markham T (2012) Fumaric acid esters as a suit-
able first line treatment for severe psoriasis: an Irish experience.
Clin Exp Dermatol 37:786–801
10. Hoefnagel JJ, Thio HB, Willemze R et al (2003) Long term safety
aspects of systemic therapy with fumaric acid esters in severe
psoriasis. Br J Dermatol 149:363–369
11. Ismail N, Collins P, Rogers S et al (2014) Drug survival of
fumaric acid esters for psoriasis: a retrospective study. Br J
Dermatol 171:397–402
12. Jennings L, Murphy GM (2009) Squamous cell carcinoma as a
complication of fumaric acid ester immunosuppression. Eur Acad
Dermatol Venereol 23:1445–1469
13. Kolbach DN, Niebor C (1992) ‘Fumaric acid therapy in psoriasis:
Results and side effects of 2 years of treatment’. J Am Acad
Dermatol 27(5 part 1): 769–771
14. Mrowietz U, Christophers E, Altmeyer P (1998) Treatment of
severe psoriasis with fumaric acid esters: scientific background
and guidelines for therapeutic use. Br J Dermatol 141:424–429
15. Naldi L, Griffiths CEM (2005) Traditional therapies in the
management of moderate to severe chronic plaque psoriasis: an
assessment of the benefits and risks. Br J Dermatol 152:597–615
16. Nugteren-HuyingWM, van der Schroeff JG,Hermans J et al (1990)
Fumaric acid therapy for psoriasis: a randomised, double blind,
placebo controlled study. J Am Acad Dermatol 22(2):311–312
17. Ogilvie S, Lewis Jones S, Dawe R et al (2011) Proteinuria with
fumaric acid ester treatment for psoriasis. Clin Exp Dermatol
36:632–634
18. Pathirana D, Ormerod AD, Saiag P et al (2009) ‘European S3-
Guidelines on the systemic treatment of psoriasis vulgaris. Eur
Acad Dermatol Venereol 23(2):5–70
19. Raschka C, Koch HJ (1999) Long term treatment of psoriasis
using fumaric acid preparations can be associated with severe
proximal tubular damage. Hum Exp Toxicol 18:738–739
176 Ir J Med Sci
123

20. Reich K, Thaci D, Mrowietz U et al (2009) Efficacy and safety of
fumaric acid esters in the long term treatment of psoriasis- a
retrospective study (FUTURE). JDDG. J der Deutschen Derma-
tologischen Gesellschaft 7:603–610
21. Reid C, Holian J, Kane D et al (2013) De Toni Fanconi Syndrome
secondary to fumaric acid esters. Br J Dermatol 169(1):24
22. Schmitt J, Zhang Z, Wozel G et al (2008) Efficacy and tolera-
bility of biologic and nonbiologic systemic treatments for mod-
erate to severe psoriasis: meta-analysis of randomised controlled
trials. Br J Dermatol 159:513–526
23. Sladden MJ, Osborne JE, Hutchinson PE (2006) Fumaric acid
esters for severe psoriasis: the Leicestershire experience. Br J
Dermatol 155:841–865
24. Thaci D, Weisenseel P, Philipp S et al (2013) ‘Efficacy and safety
of fumaric acid esters in patients with psoriasis on medication for
comorbid conditions – a retrospective evaluation (FACTS). J Ger
Soc Dermatol 1610–0379:439–445
25. Van Oosten BW, Killestein J, Barkhof F et al (2013) PML in a
patient treated with dimethylfumarate from a compounding
pharmacy. N Engl J Med 368(17):1658–1659
26. Wu Y, Mills D, Bala M (2008) Psoriasis: cardiovascular risk
factors and other disease comorbidities. J Drugs Dermatol
7:373–377
27. European Medicines Agency (2015). ‘Updated recommendations
tominimise the risk of the rare brain infection PMLwithTecfidera’.
Available at: http://www.ema.europa.eu/docs/en_GB/document_
library/Press_release/2015/10/WC500196017.pdf. Accessed Mar
1, 2016
Ir J Med Sci 177
123