Embed Size (px)
Citation preview

FUNDACION JIMENEZ DIAZ-IDC
Dra. Clotilde Vázquez Jefe de Departamento Endocrinología y Nutrición
Mercedes Ramírez Nutricionista
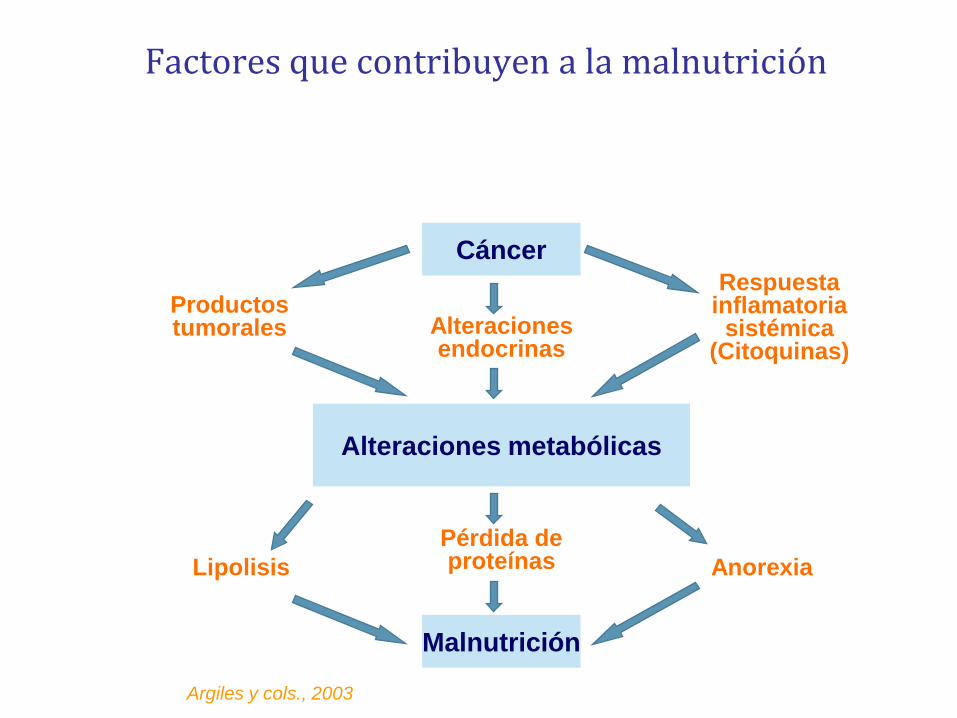
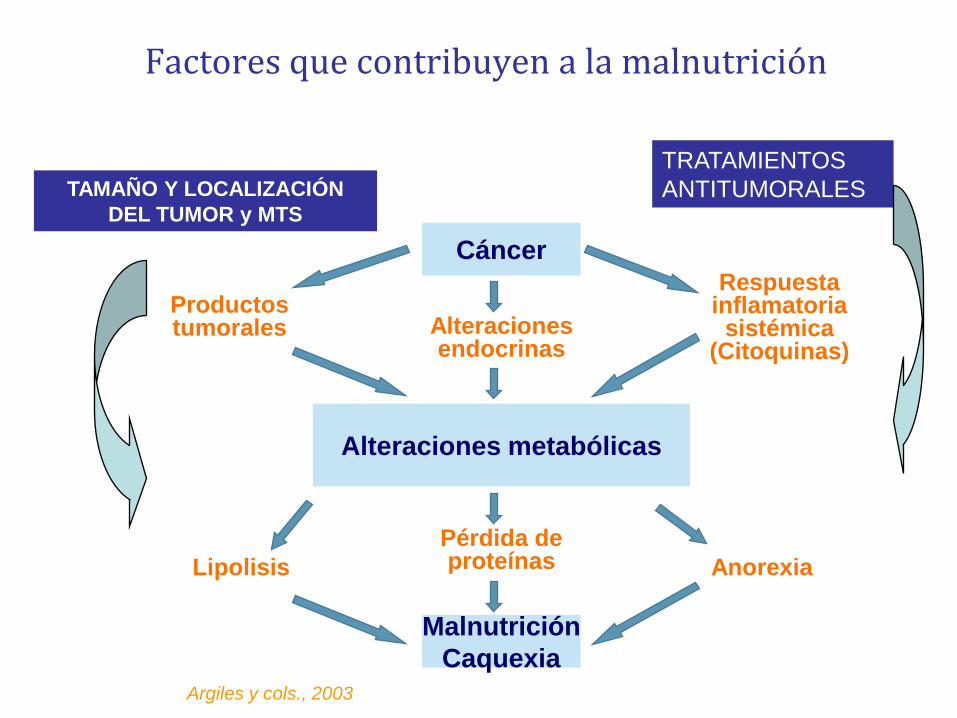
Argiles y cols., 2003
Factores que contribuyen a la malnutrición
Malnutrición
Alteraciones metabólicas
Cáncer
Productos tumorales Alteraciones
endocrinas
Respuesta inflamatoria
sistémica (Citoquinas)
Lipolisis
Pérdida de proteínas Anorexia
E0201257A 4
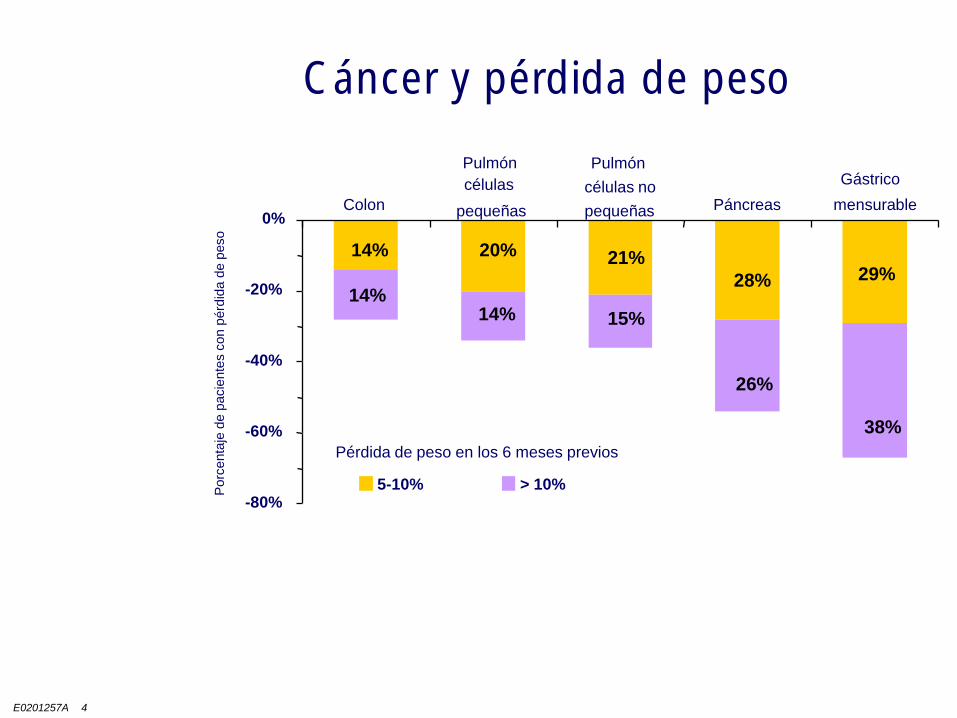
-80%
-60%
-40%
-20%
0%
5-10% > 10%
Pérdida de peso en los 6 meses previos
Colon
Pulmón
células
pequeñas
Pulmón
células no
pequeñas Páncreas
Gástrico
mensurable
14%
14%
20%
14%
21%
15%
28%
26%
29%
38%
DeWys et al. 1980. Am J Med. 69:491
Porc
enta
je d
e p
acie
nte
s c
on p
érd
ida d
e p
eso
Cáncer y pérdida de peso
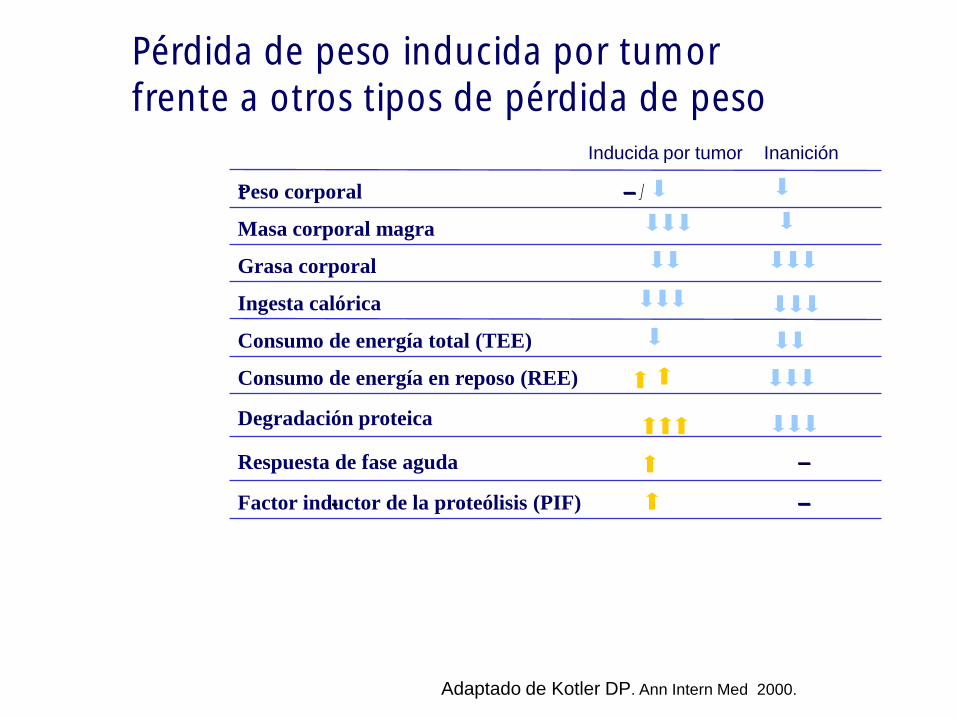
Pérdida de peso inducida por tumor frente a otros tipos de pérdida de peso
Adaptado de Kotler DP. Ann Intern Med 2000. 133:22
––Respuesta de fase aguda
Degradación proteica
––Factor inductor de la proteólisis (PIF)-
Consumo de energía en reposo (REE)
Consumo de energía total (TEE)
Ingesta calórica
Grasa corporal
Masa corporal magra
–– //tPeso corporal
InaniciónInducida por tumor
Argiles y cols., 2003
Factores que contribuyen a la malnutrición
Malnutrición
Caquexia
Alteraciones metabólicas
Cáncer
Productos tumorales Alteraciones
endocrinas
Respuesta inflamatoria
sistémica (Citoquinas)
Lipolisis
Pérdida de proteínas Anorexia
TAMAÑO Y LOCALIZACIÓN
DEL TUMOR y MTS
TRATAMIENTOS
ANTITUMORALES
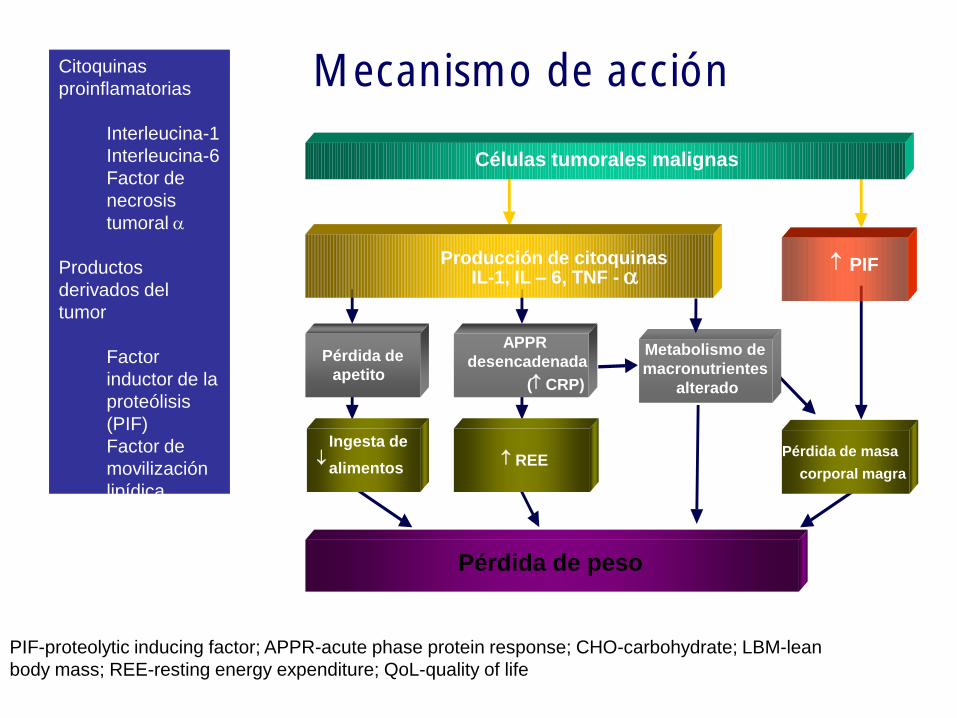
PIF-proteolytic inducing factor; APPR-acute phase protein response; CHO-carbohydrate; LBM-lean
body mass; REE-resting energy expenditure; QoL-quality of life
Pérdida de peso
Células tumorales malignas
Producción de citoquinasIL-1, IL – 6, TNF - a
PIF
APPR
desencadenada
( CRP)
Pérdida de
apetito
Pérdida de masa
corporal magra REE
Ingesta de
alimentos
Metabolismo de
macronutrientes
alterado
Mecanismo de acciónCitoquinas
proinflamatorias
Interleucina-1
Interleucina-6
Factor de
necrosis
tumoral a
Productos
derivados del
tumor
Factor
inductor de la
proteólisis
(PIF)
Factor de
movilización
lipídica
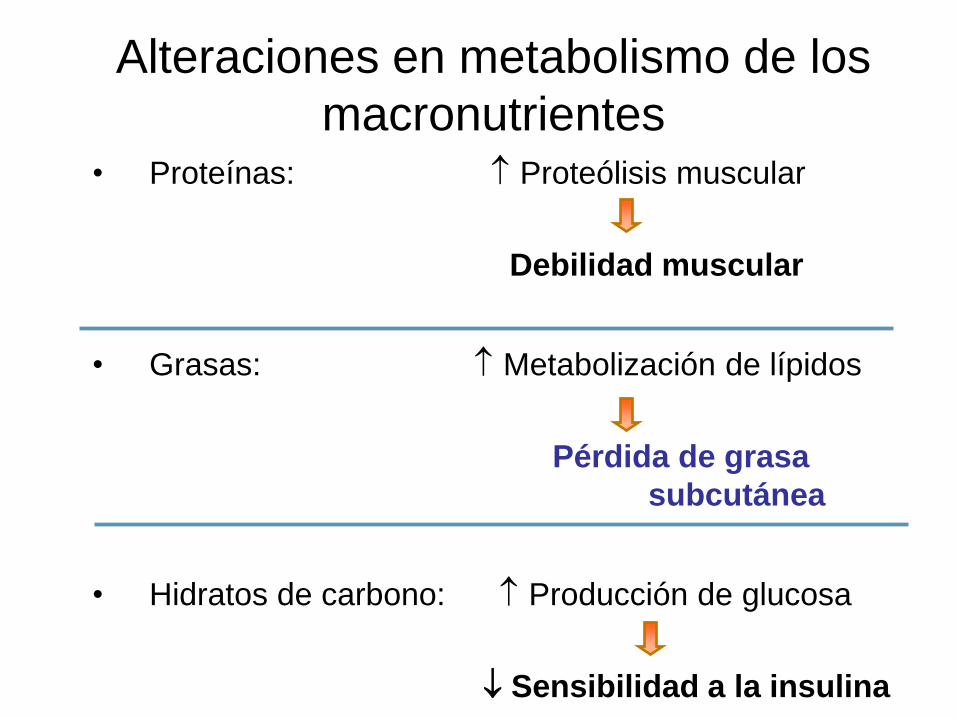
• Proteínas: Proteólisis muscular
Debilidad muscular
• Grasas: Metabolización de lípidos
Pérdida de grasa
subcutánea
• Hidratos de carbono: Producción de glucosa
Sensibilidad a la insulina
Alteraciones en metabolismo de los
macronutrientes
OBJETIVOS DEL TRATAMIENTO
NUTRICIONAL
• Preservar la masa magra
• Mejorar el estado inmunológico
• Mejorar la tolerancia del tratamiento antitumoral
• Disminuir el riesgo de complicacionesquirúrgicas
• Mejorar el estado funcional
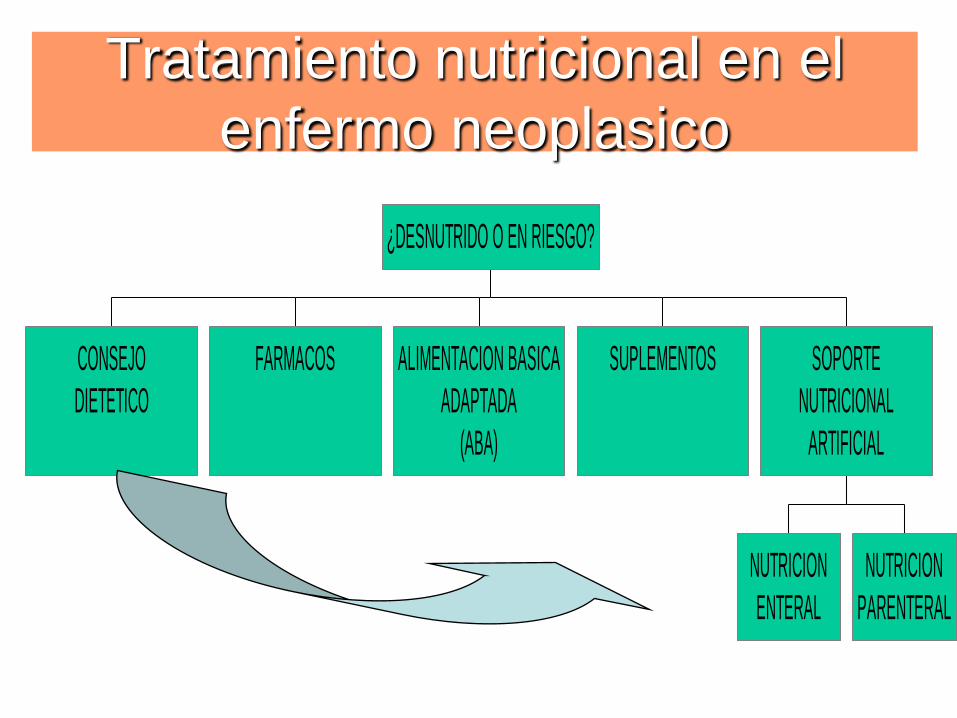
Tratamiento nutricional en el
enfermo neoplasico
CONSEJO
DIETETICO
FARMACOS ALIMENTACION BASICA
ADAPTADA
(ABA)
SUPLEMENTOS
NUTRICION
ENTERAL
NUTRICION
PARENTERAL
SOPORTE
NUTRICIONAL
ARTIFICIAL
¿DESNUTRIDO O EN RIESGO?
Evans et al. J Clin Oncol. 1987;5:113E0201257A 23
Tratamiento Nutricional
.
• Nutrición parenteral total
• Nutrición enteral SNG o PEG
• Soporte nutricional enteral oral
• Consejo Nutricional
• Agentes Farmacológicos
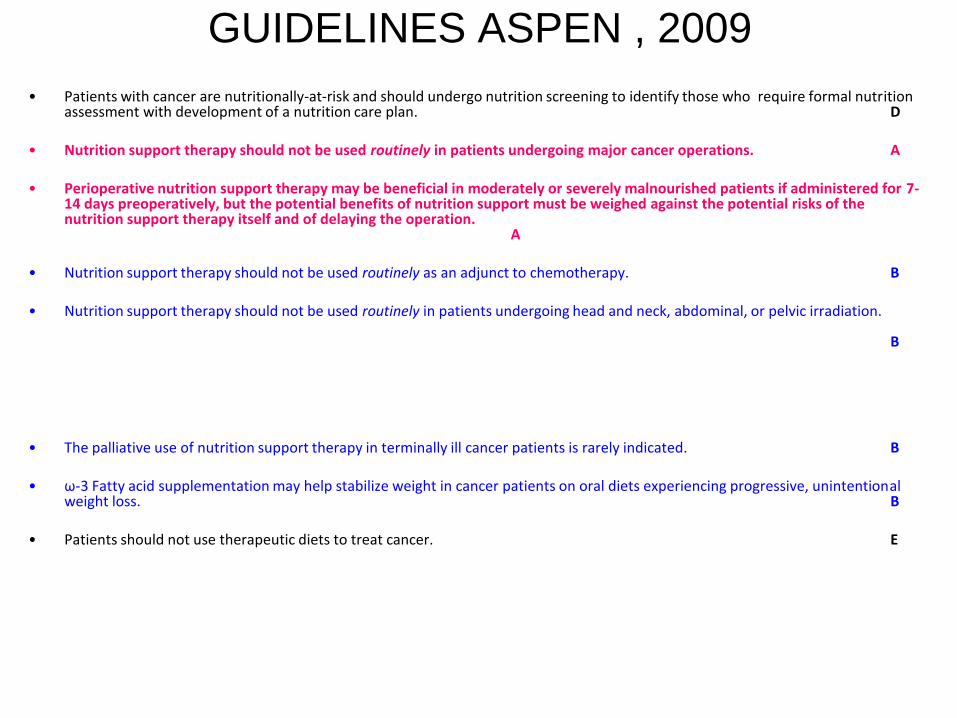
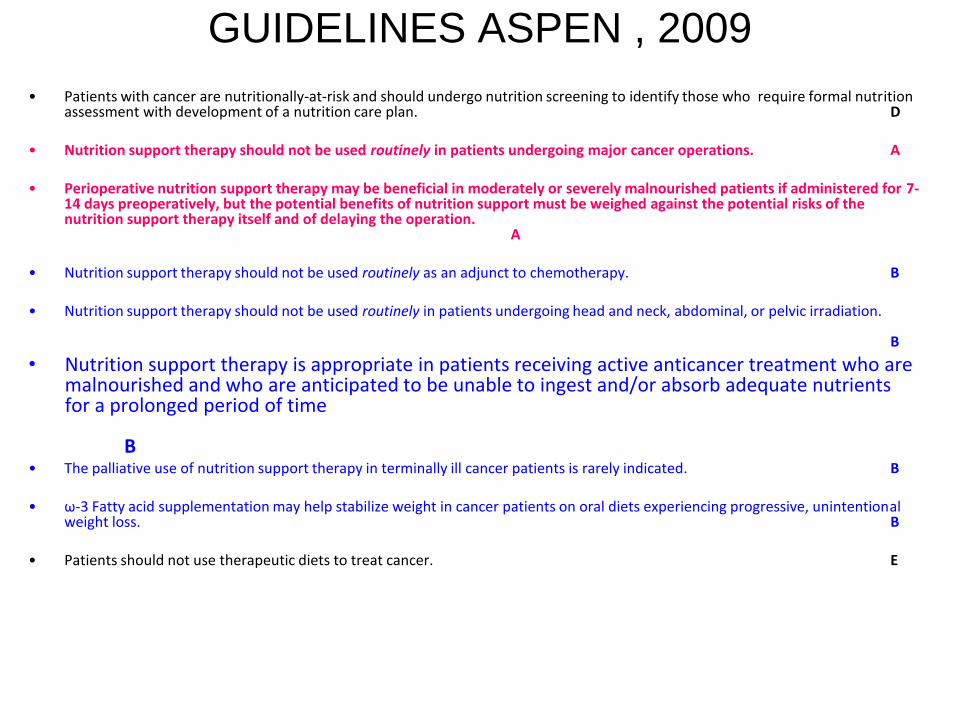
GUIDELINES ASPEN , 2009
• Patients with cancer are nutritionally-at-risk and should undergo nutrition screening to identify those who require formal nutrition assessment with development of a nutrition care plan. D
• Nutrition support therapy should not be used routinely in patients undergoing major cancer operations. A
• Perioperative nutrition support therapy may be beneficial in moderately or severely malnourished patients if administered for 7-14 days preoperatively, but the potential benefits of nutrition support must be weighed against the potential risks of the nutrition support therapy itself and of delaying the operation.
A
• Nutrition support therapy should not be used routinely as an adjunct to chemotherapy. B
• Nutrition support therapy should not be used routinely in patients undergoing head and neck, abdominal, or pelvic irradiation.
B
• The palliative use of nutrition support therapy in terminally ill cancer patients is rarely indicated. B
• ω-3 Fatty acid supplementation may help stabilize weight in cancer patients on oral diets experiencing progressive, unintentional weight loss. B
• Patients should not use therapeutic diets to treat cancer. E
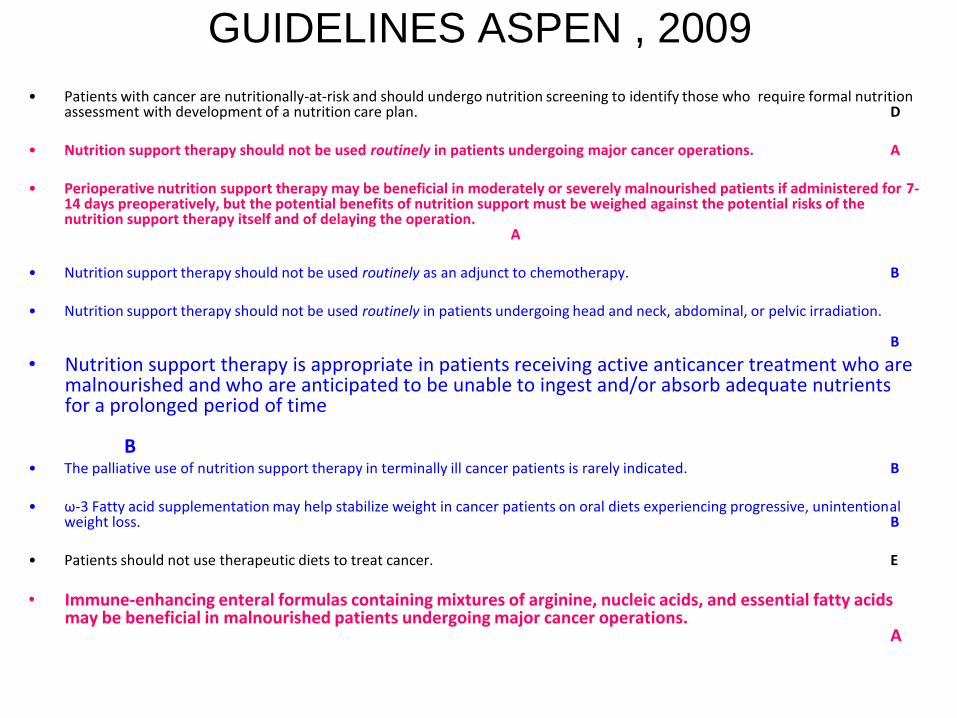
GUIDELINES ASPEN , 2009
• Patients with cancer are nutritionally-at-risk and should undergo nutrition screening to identify those who require formal nutrition assessment with development of a nutrition care plan. D
• Nutrition support therapy should not be used routinely in patients undergoing major cancer operations. A
• Perioperative nutrition support therapy may be beneficial in moderately or severely malnourished patients if administered for 7-14 days preoperatively, but the potential benefits of nutrition support must be weighed against the potential risks of the nutrition support therapy itself and of delaying the operation.
A
• Nutrition support therapy should not be used routinely as an adjunct to chemotherapy. B
• Nutrition support therapy should not be used routinely in patients undergoing head and neck, abdominal, or pelvic irradiation.
B
• Nutrition support therapy is appropriate in patients receiving active anticancer treatment who are malnourished and who are anticipated to be unable to ingest and/or absorb adequate nutrients for a prolonged period of time
B• The palliative use of nutrition support therapy in terminally ill cancer patients is rarely indicated. B
• ω-3 Fatty acid supplementation may help stabilize weight in cancer patients on oral diets experiencing progressive, unintentional weight loss. B
• Patients should not use therapeutic diets to treat cancer. E
GUIDELINES ASPEN , 2009
• Patients with cancer are nutritionally-at-risk and should undergo nutrition screening to identify those who require formal nutrition assessment with development of a nutrition care plan. D
• Nutrition support therapy should not be used routinely in patients undergoing major cancer operations. A
• Perioperative nutrition support therapy may be beneficial in moderately or severely malnourished patients if administered for 7-14 days preoperatively, but the potential benefits of nutrition support must be weighed against the potential risks of the nutrition support therapy itself and of delaying the operation.
A
• Nutrition support therapy should not be used routinely as an adjunct to chemotherapy. B
• Nutrition support therapy should not be used routinely in patients undergoing head and neck, abdominal, or pelvic irradiation.
B
• Nutrition support therapy is appropriate in patients receiving active anticancer treatment who are malnourished and who are anticipated to be unable to ingest and/or absorb adequate nutrients for a prolonged period of time
B• The palliative use of nutrition support therapy in terminally ill cancer patients is rarely indicated. B
• ω-3 Fatty acid supplementation may help stabilize weight in cancer patients on oral diets experiencing progressive, unintentional weight loss. B
• Patients should not use therapeutic diets to treat cancer. E
• Immune-enhancing enteral formulas containing mixtures of arginine, nucleic acids, and essential fatty acids may be beneficial in malnourished patients undergoing major cancer operations.
A
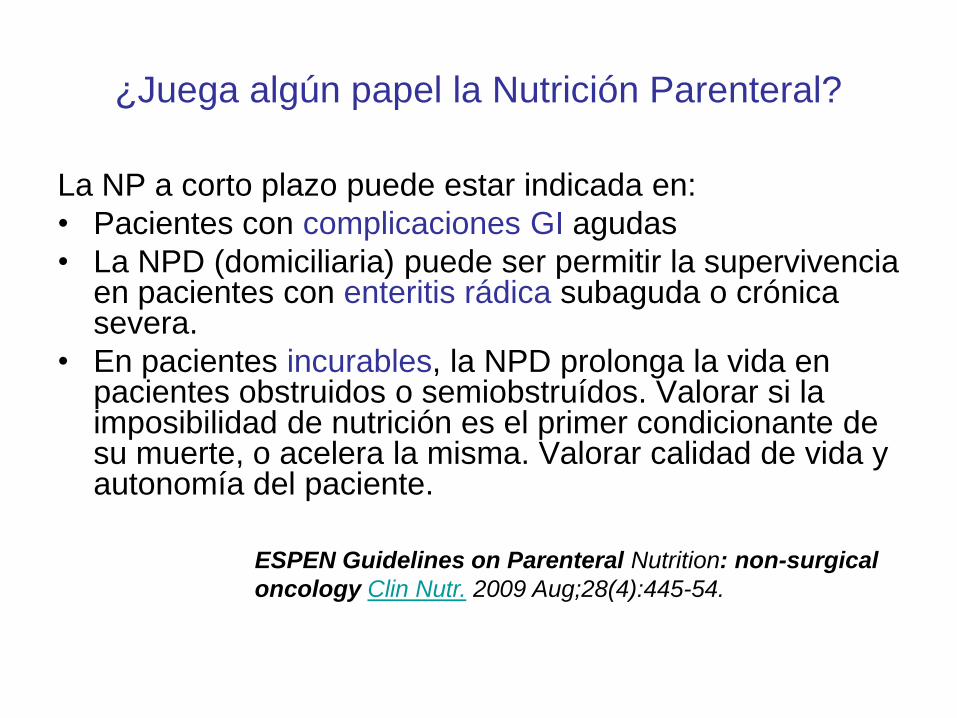
¿Juega algún papel la Nutrición Parenteral?
La NP a corto plazo puede estar indicada en:
• Pacientes con complicaciones GI agudas
• La NPD (domiciliaria) puede ser permitir la supervivencia en pacientes con enteritis rádica subaguda o crónica severa.
• En pacientes incurables, la NPD prolonga la vida en pacientes obstruidos o semiobstruídos. Valorar si la imposibilidad de nutrición es el primer condicionante de su muerte, o acelera la misma. Valorar calidad de vida y autonomía del paciente.
ESPEN Guidelines on Parenteral Nutrition: non-surgical
oncology Clin Nutr. 2009 Aug;28(4):445-54.
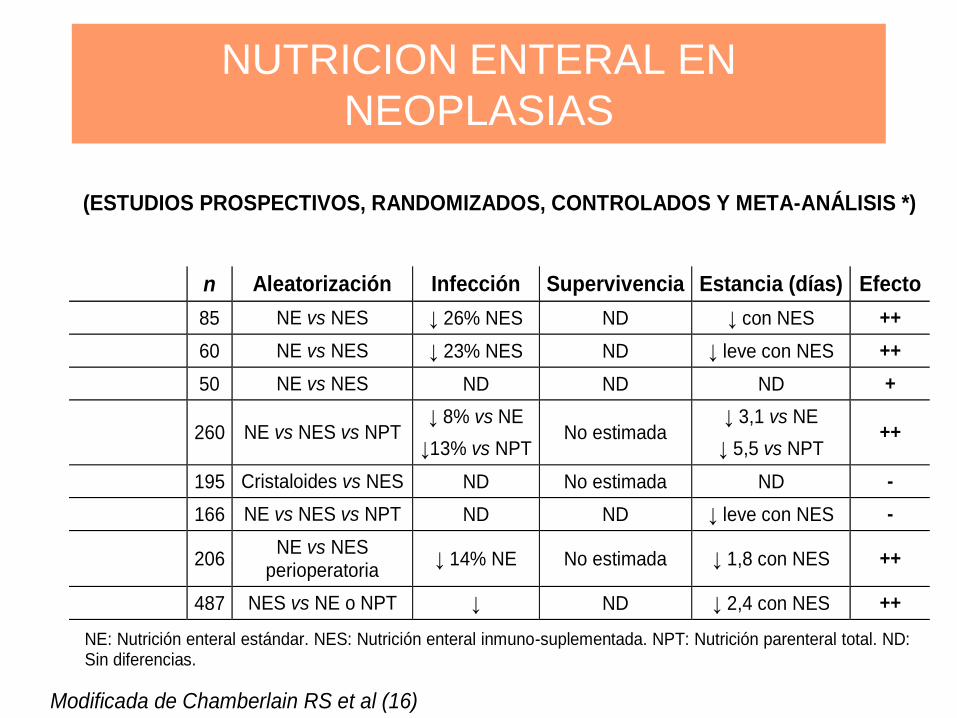
NUTRICION ENTERAL EN
NEOPLASIAS
(ESTUDIOS PROSPECTIVOS, RANDOMIZADOS, CONTROLADOS Y META-ANÁLISIS *)
n Aleatorización Infección Supervivencia Estancia (días) Efecto
85 NE vs NES ↓ 26% NES ND ↓ con NES ++
60 NE vs NES ↓ 23% NES ND ↓ leve con NES ++
50 NE vs NES ND ND ND +
260 NE vs NES vs NPT ↓ 8% vs NE
↓13% vs NPT No estimada
↓ 3,1 vs NE
↓ 5,5 vs NPT ++
195 Cristaloides vs NES ND No estimada ND -
166 NE vs NES vs NPT ND ND ↓ leve con NES -
206 NE vs NES
perioperatoria ↓ 14% NE No estimada ↓ 1,8 con NES ++
487 NES vs NE o NPT ↓ ND ↓ 2,4 con NES ++
NE: Nutrición enteral estándar. NES: Nutrición enteral inmuno-suplementada. NPT: Nutrición parenteral total. ND: Sin diferencias.
Modificada de Chamberlain RS et al (16)
Medical Nutrition Therapy (MNT) en
Oncología Radioterapica
(American Dietetic Association, ADA)
Intensive nutrition intervention following the ADA MNT protocol results in improved dietary intake compared with
standard practice and seems to beneficially impact nutrition-related outcomes previously observed in oncology outpatients
receiving radiotherapy. The ADA MNT protocol for radiation oncology is a useful guide to the level of nutrition support
required.
PRACTICA CLÍNICA EN ONCOLOGÍA
RADIOTERÁPICA TUMORES DE CABEZA Y
CUELLO. HOSPITAL RAMON Y CAJAL
• Nutricionista: Visita desde la 1ª semana y con periodicidad semanal.
• Valoración P-VSG.
• Clave en el algoritmo de decisiones: pérdida de peso y progresión de la disfagia
ANTE INGESTA INADECUADA O
PÉRDIDA DE PESO Y/O ALTERACIONES
BIOQUÍMICAS
• Suplementos nutricionales.
• Seguimiento semanal nutricionista.
ANTE DISFAGIA SEVERA O
DISFAGIA A LIQUIDOS
• SNG o GASTROSTOMÍA RADIOLOGICA.
• Revisión semanal ATS nutrición/médico
nutrición.
• Se retira SNG cuando es capaz de ingerir
> 50% de los requerimientos.
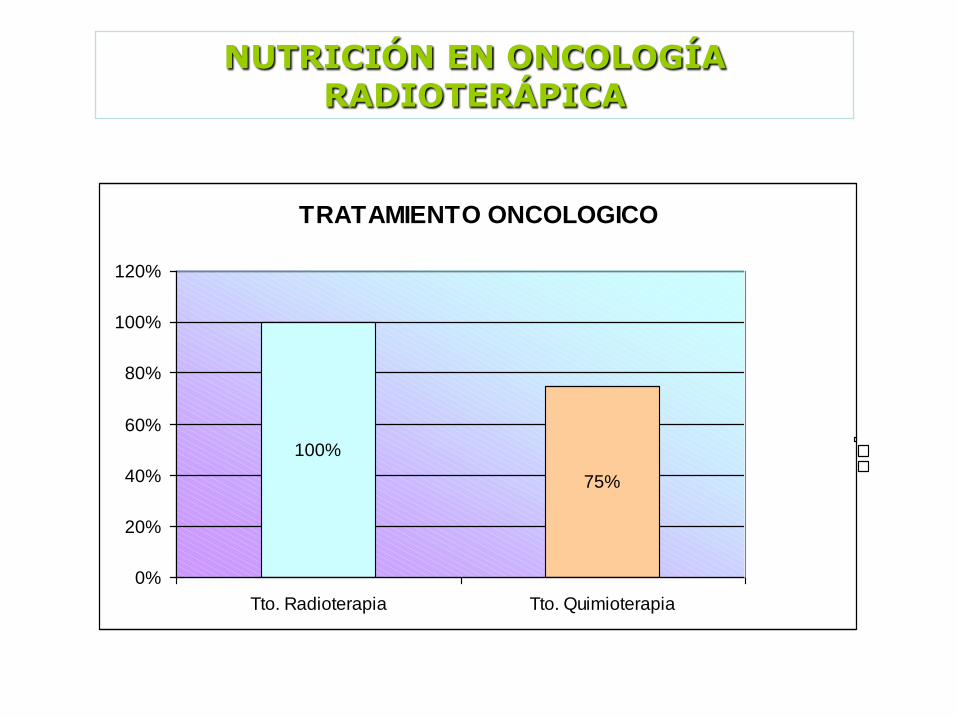
NUTRICIÓN EN ONCOLOGÍA RADIOTERÁPICA
TRATAMIENTO ONCOLOGICO
100%
75%
0%
20%
40%
60%
80%
100%
120%
Tto. Radioterapia Tto. Quimioterapia
49 pacientes cáncer de cabeza y cuello
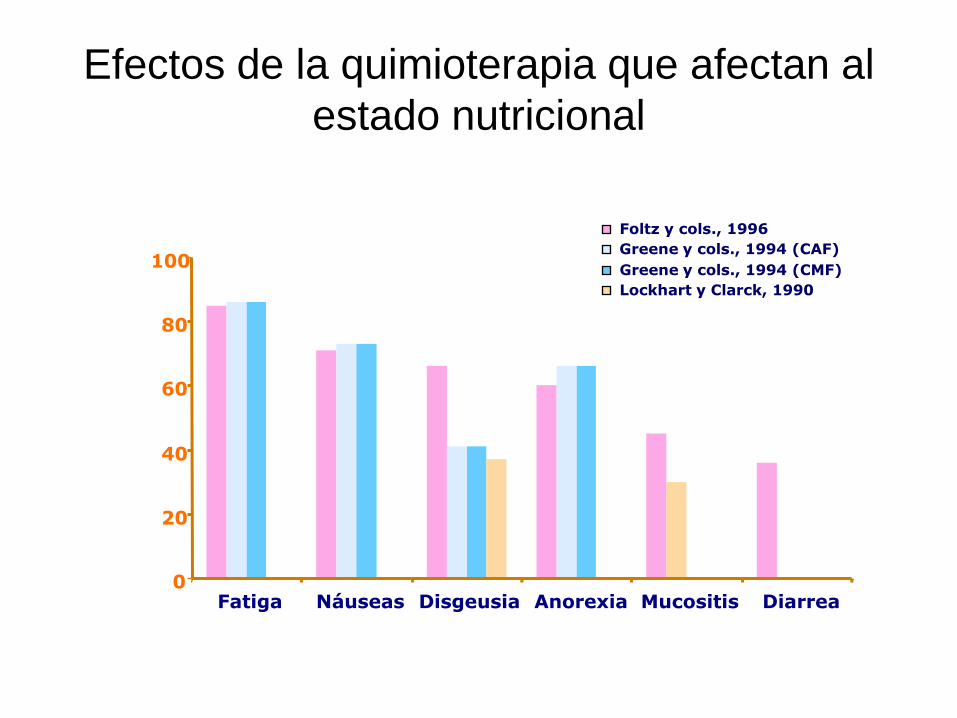
Efectos de la quimioterapia que afectan al
estado nutricional
0
20
40
60
80
100
Fatiga Náuseas Disgeusia Anorexia Mucositis Diarrea
Foltz y cols., 1996
Greene y cols., 1994 (CAF)
Greene y cols., 1994 (CMF)
Lockhart y Clarck, 1990
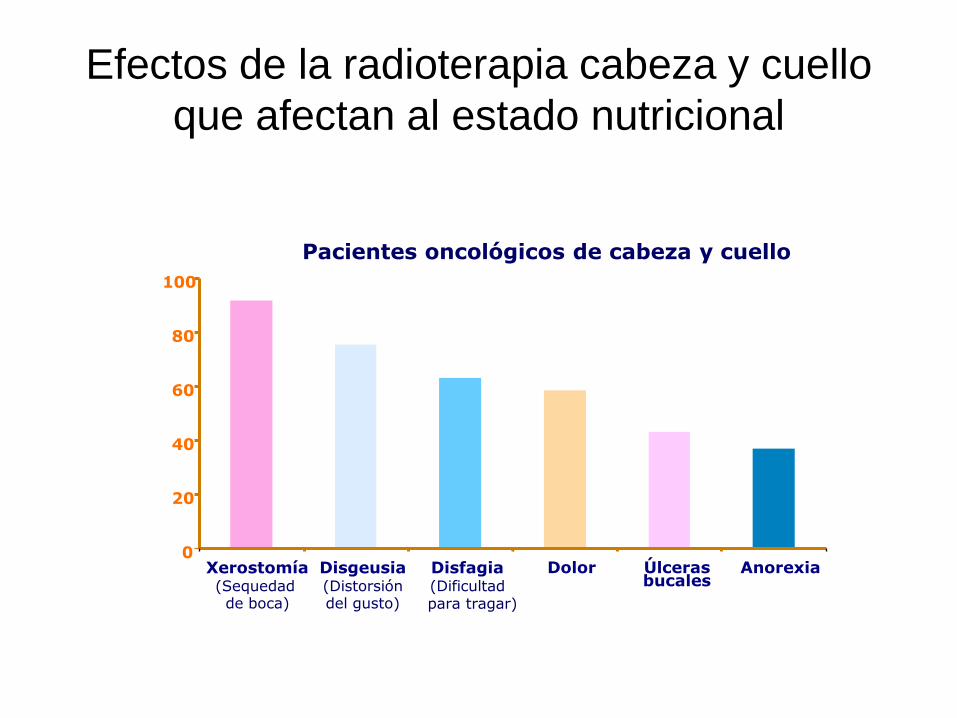
Efectos de la radioterapia cabeza y cuello
que afectan al estado nutricional
0
20
40
60
80
100
Xerostomía(Sequedad de boca)
Disgeusia(Distorsióndel gusto)
Disfagia(Dificultadpara tragar)
Dolor Úlcerasbucales
Anorexia
Pacientes oncológicos de cabeza y cuello
CONSEJO DIETETICO ANTE DISFAGIA
Y/O MUCOSITIS
• Alimentos a temperatura ambiente
• Comidas pequeñas y frecuentes
• Beber agua entre horas
• Alimentos cocidos, suaves,de consistencia según tolerancia
• Evitar alimentos irritantes: ácidos,picantes,...
• Valorar ABA, suplementos o N enteral
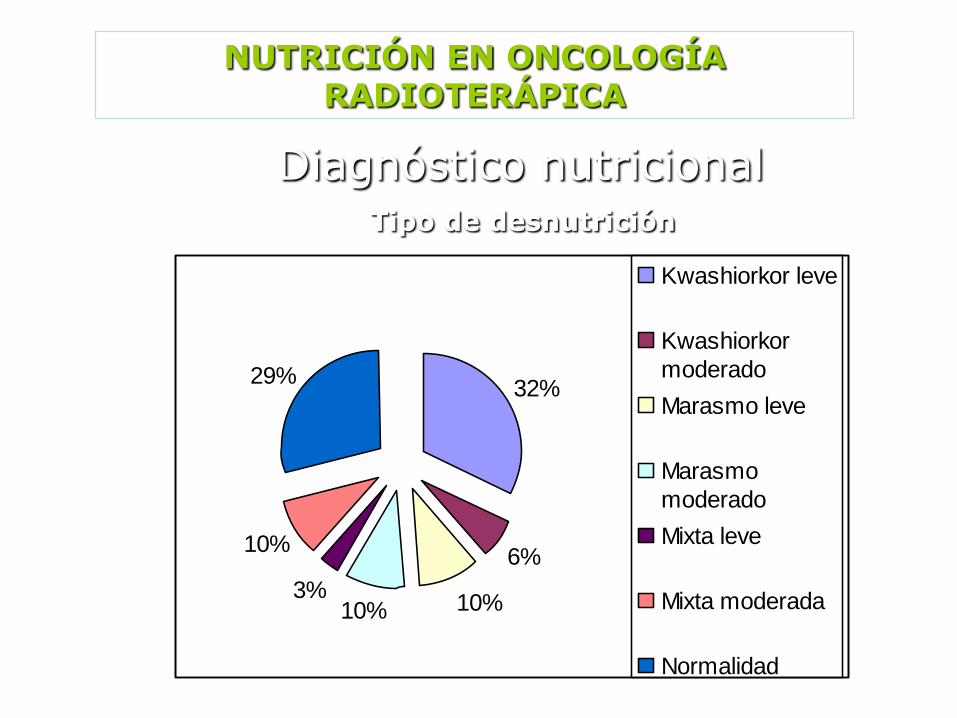
NUTRICIÓN EN ONCOLOGÍA RADIOTERÁPICA
Diagnóstico nutricionalTipo de desnutrición
32%
6%
10%10%3%
10%
29%
Kwashiorkor leve
Kwashiorkor
moderado
Marasmo leve
Marasmo
moderado
Mixta leve
Mixta moderada
Normalidad
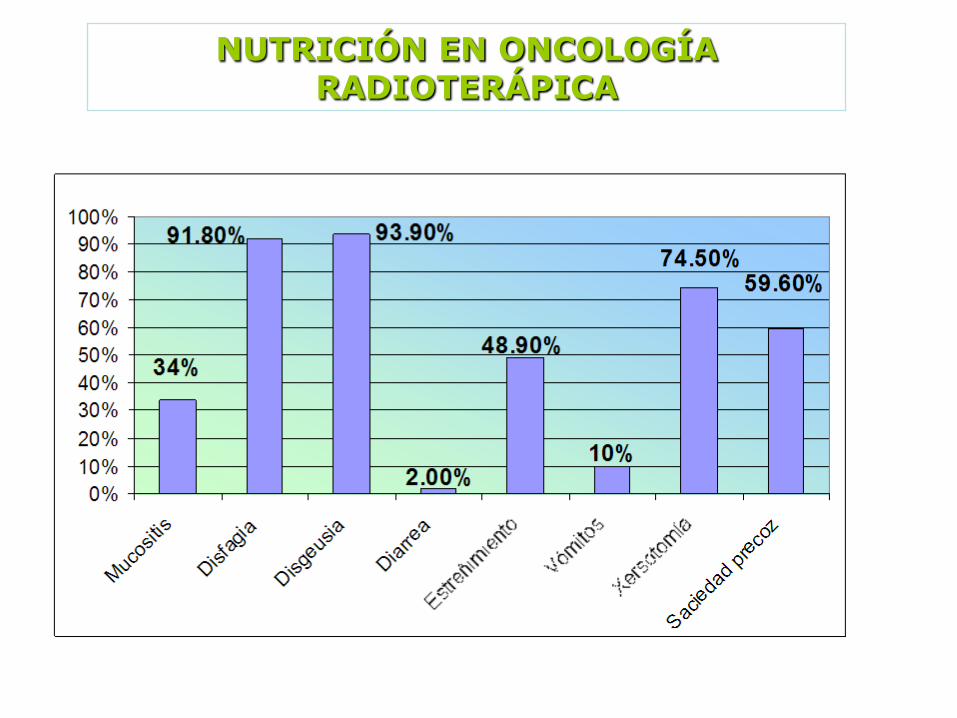
NUTRICIÓN EN ONCOLOGÍA RADIOTERÁPICA
Síntomas según frecuencia
Evans et al. J Clin Oncol. 1987;5:113E0201257A 23
Tratamiento Nutricional
.
• Nutrición parenteral total
• Nutrición enteral SNG o PEG
• Soporte nutricional enteral oral
• Consejo Nutricional
• Agentes Farmacológicos
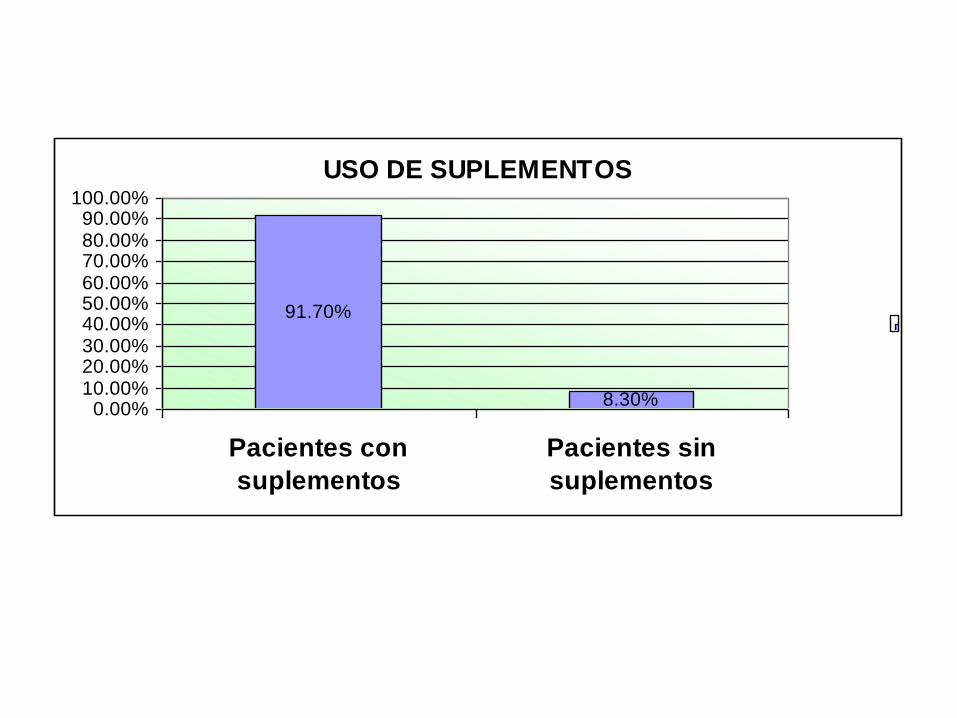
USO DE SUPLEMENTOS
91.70%
8.30%0.00%
10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
100.00%
Pacientes con
suplementos
Pacientes sin
suplementos
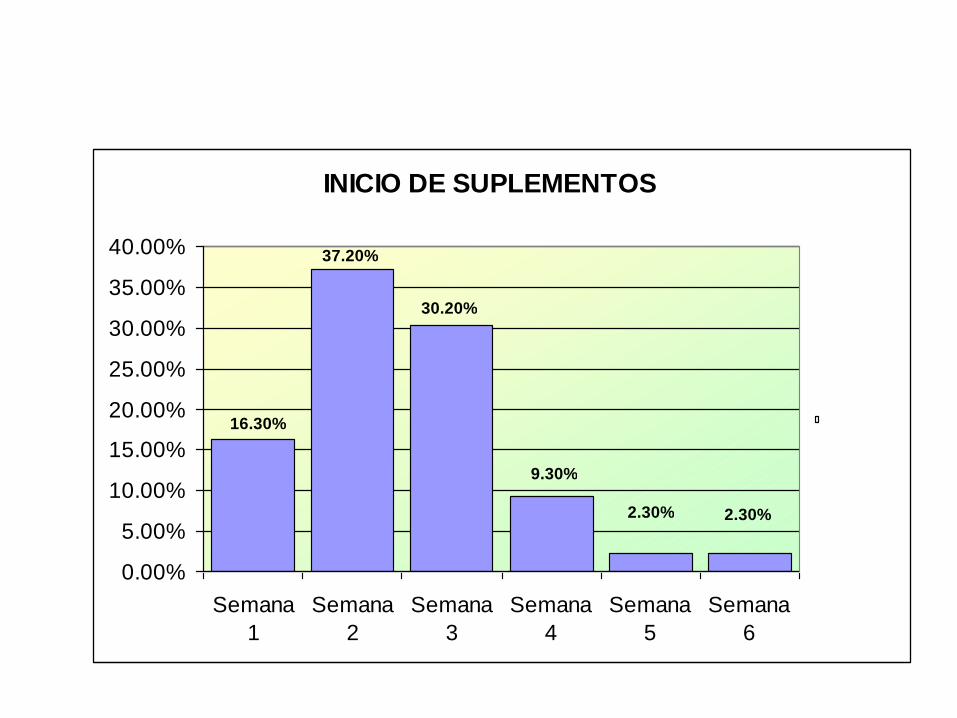
INICIO DE SUPLEMENTOS
16.30%
37.20%
30.20%
9.30%
2.30%2.30%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Semana
1
Semana
2
Semana
3
Semana
4
Semana
5
Semana
6
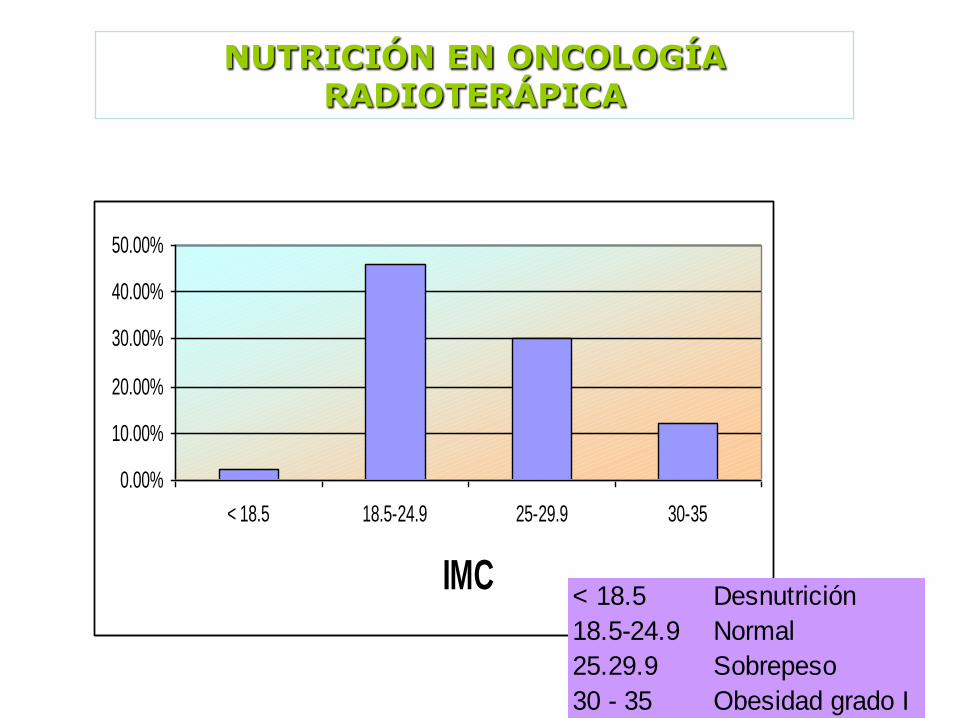
NUTRICIÓN EN ONCOLOGÍA RADIOTERÁPICA
Estado nutricional inicial
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
< 18.5 18.5-24.9 25-29.9 30-35
IMC< 18.5 Desnutrición
18.5-24.9 Normal
25.29.9 Sobrepeso
30 - 35 Obesidad grado I
0.00%
20.00%
40.00%
60.00%
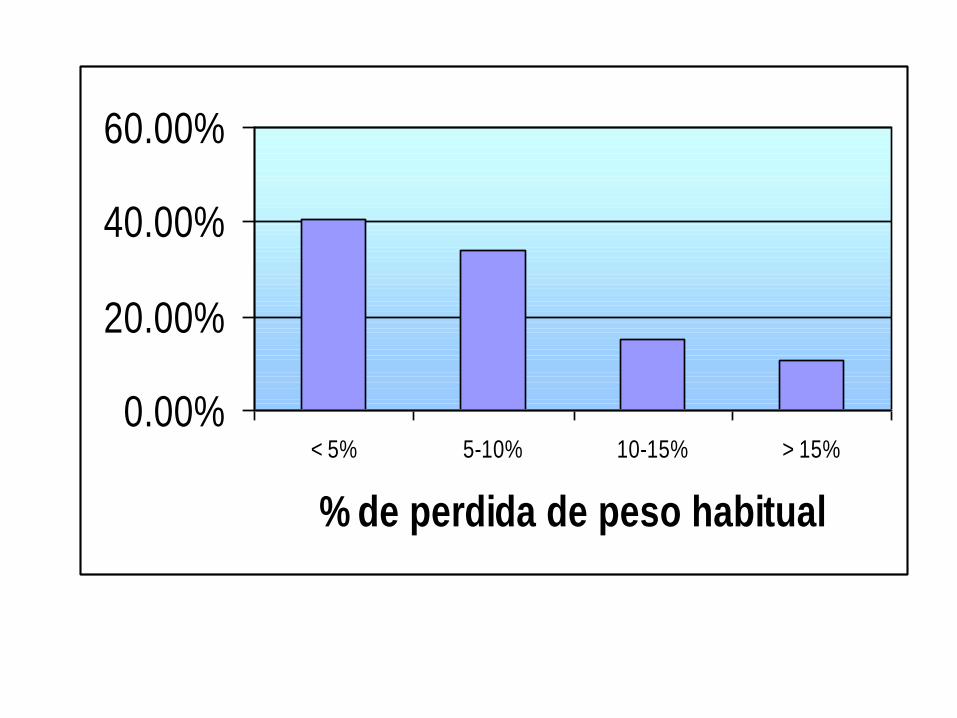
< 5% 5-10% 10-15% > 15%
% de perdida de peso habitual
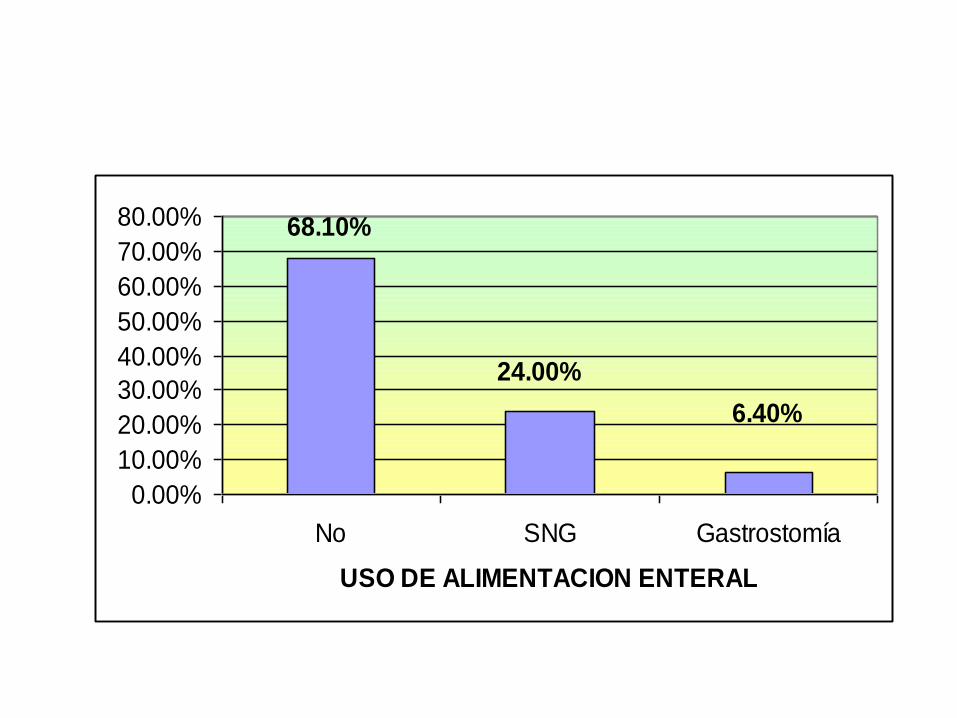
6.40%
24.00%
68.10%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
No SNG Gastrostomía
USO DE ALIMENTACION ENTERAL
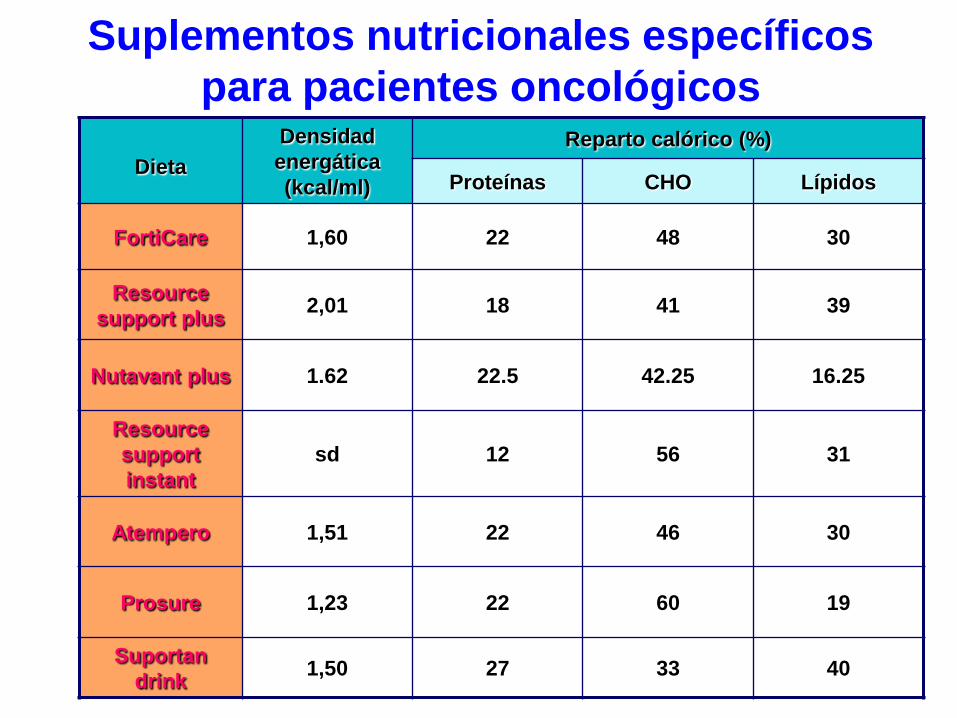
Suplementos nutricionales específicos
para pacientes oncológicos
Dieta
Densidad
energática
(kcal/ml)
Reparto calórico (%)
Proteínas CHO Lípidos
FortiCare 1,60 22 48 30
Resource
support plus2,01 18 41 39
Nutavant plus 1.62 22.5 42.25 16.25
Resource
support
instant
sd 12 56 31
Atempero 1,51 22 46 30
Prosure 1,23 22 60 19
Suportan
drink1,50 27 33 40
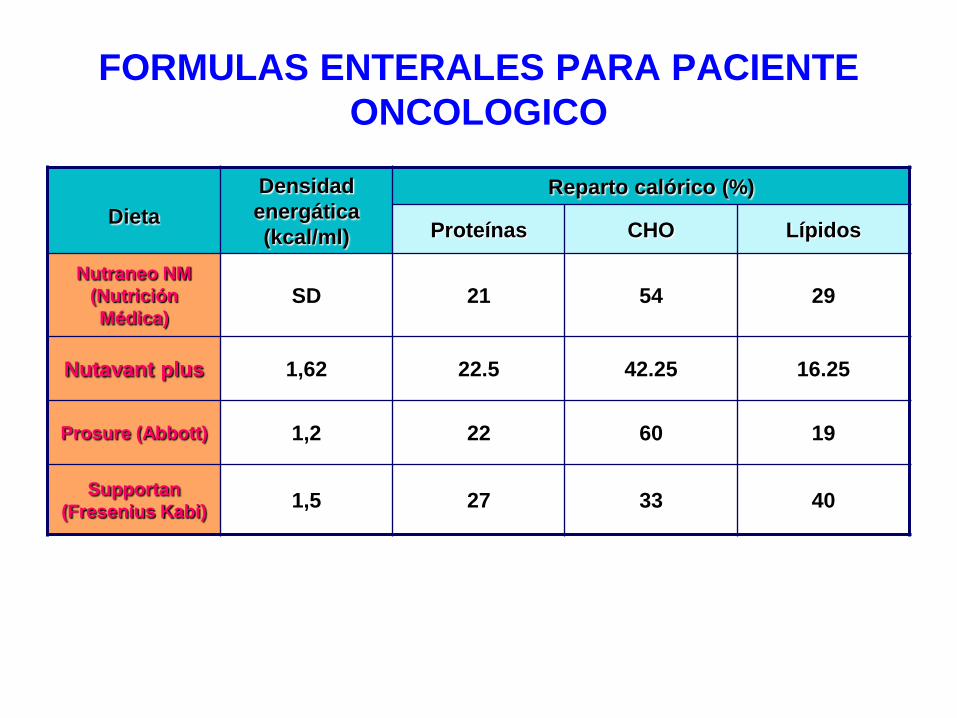
FORMULAS ENTERALES PARA PACIENTE
ONCOLOGICO
Dieta
Densidad
energática
(kcal/ml)
Reparto calórico (%)
Proteínas CHO Lípidos
Nutraneo NM
(Nutrición
Médica)SD 21 54 29
Nutavant plus 1,62 22.5 42.25 16.25
Prosure (Abbott) 1,2 22 60 19
Supportan
(Fresenius Kabi)1,5 27 33 40
E0201257A 27
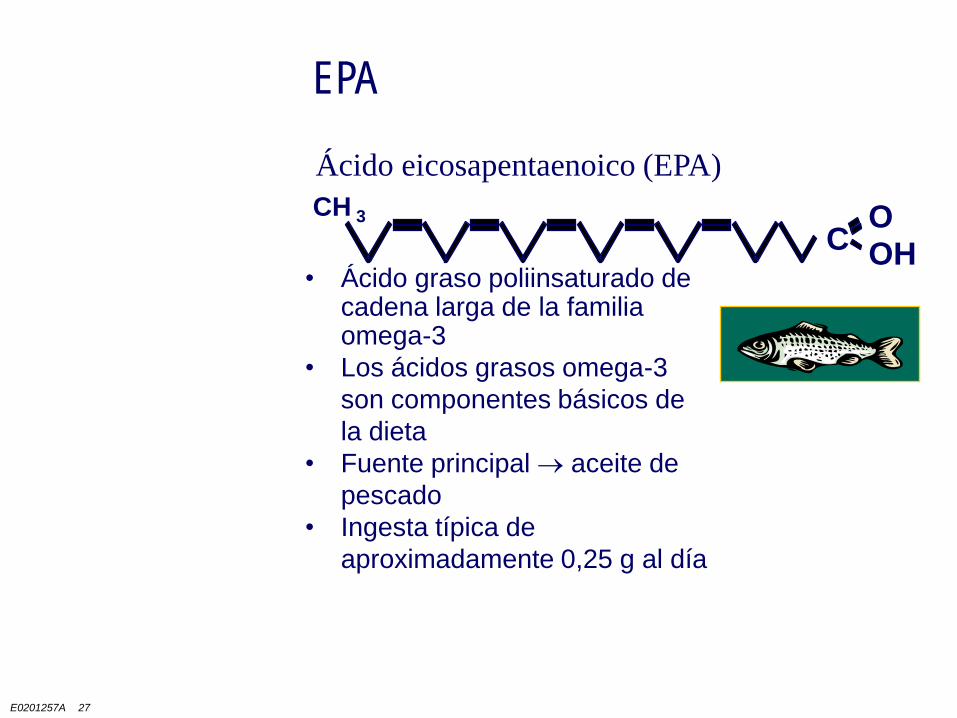
EPA
Ácido eicosapentaenoico (EPA)
C OHOCH 3
• Ácido graso poliinsaturado de cadena larga de la familia omega-3
• Los ácidos grasos omega-3
son componentes básicos de
la dieta
• Fuente principal aceite de
pescado
• Ingesta típica de
aproximadamente 0,25 g al día
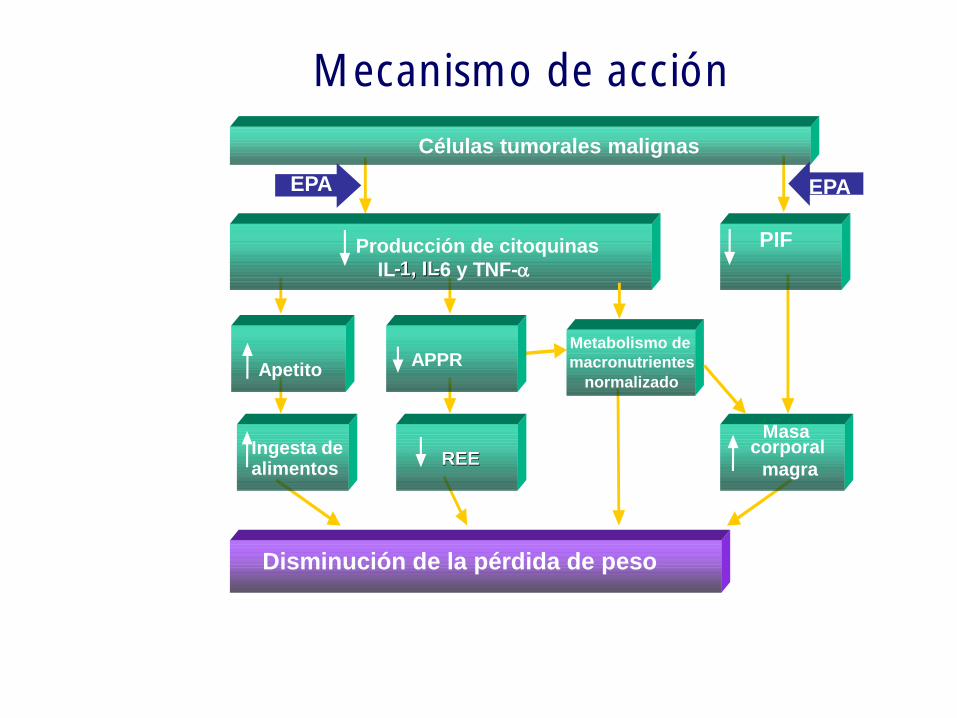
Disminución de la pérdida de peso
Células tumorales malignas
Producción de citoquinas
IL--1, IL1, IL--6 y TNF-a
PIF
APPR Apetito
Metabolismo de
macronutrientes
normalizado
Masacorporal
magraREEREE
Ingesta de
EPAEPA
alimentos
Mecanismo de acción
Arginina
• Immunoenhanced enteral nutrition formulas in head and neck cancer surgery: a systematic review.
• Casas Rodera P1, de Luis DA, Gómez Candela C, Culebras JM.
• Significant malnutrition exists in a high percentage of patients with head and neck cancer. Malnutrition is associated with defects in immune function that may impair the host response to malignancy. Malnutrition and immunosupression make patients highly susceptible to postoperative infections and complications.
• OBJECTIVES:
• Some studies of patients receiving immuno-nutrition in the perioperative period in head and neck cancer have shown beneficial effects on clinical outcome and inmune status. The authors carried out a systematic review of randomised control trials to determine whether perioperative immunonutrition has a role in the treatment of head and neck cancer.
• METHODS:
• 14 trials of polymeric nutritional supplementation with immunonutrition were identified. Two studies compared two types of immunonutrition.
• RESULTS:
• A reduction in the length of postoperative hospital stay was seen in some trials, but the reason for this reduction is not clear. Some studides showed statistical differences with less complications in arginine-enhanced group and also showed a significant decrease of fistula complications in patients treated with a high arginine dose enhanced formula, if compared with a medium dose of arginine. CONCLUSSION: Those planning future studies face challenges. A suitable powered clinical trial is required before firm recommendations can be made on the use of immunonutrition in head and neck cancer patients postoperatively
Nutr Hosp. 2012 May-Jun;27(3):681-90.
ANTIOXIDANTES Y RADIOTERAPIA
Antioxidants do protect against radiation-induced oncogenic transformation in experimental systems; however, we do not have comparable human studies that show the same association. Antioxidants do reduce the painful side effects of radiation therapy, thus supporting the beneficial effects of antioxidants in protecting normal cells in radiation therapy and in being used in conjunction with treatment for certain cancers.
When considering antioxidant supplementation during treatment, it is doubtful whether high doses of radiation given in certain treatments would be rendered less effective if patients took a daily supplement of antioxidants—for example, at RDA levels—yet, we do not know and more research is needed.
Experimental studies showing that antioxidants, including phytochemicals, induce apoptosis in cancer cells but not in normal cells are in vitro phenomena. At this point, one can only speculate on an in vivo correlation. More studies are needed when considering adjuvant therapy with radiation.
At present, with limited available data, most radiation oncologists counsel their patients to refrain from taking antioxidant supplements during radiation therapy. Others, however, consider the data and suggest that a cautious and judicious use of antioxidants that helps the patient maintain a good quality of life may be helpful in cancer treatment.
American Dietetic Association, 2011
RESULTADOS EN ONCOLOGÍA
RADIOTERÁPICA TUMORES DE CABEZA Y
CUELLO. HOSPITAL RAMON Y CAJAL
• No pérdida de peso global
• Pérdida leve de masa magra
• Mejoría de la calidad de vida
• Tolerancia variable (individual) de los
suplementos : sabor, consistencia…
E0201257A 46
Conclusión
• Mayor implicación de los oncólogos en la Nutrición
• Evaluación del estado nutricional del paciente
• Aplicación precoz de las medidas nutricionales para evitar
la pérdida de peso en vez de intentar restituir una
desnutrición importante
• Incorporación de nuevos fármacos y estrategias
• Intentar mejorar la calidad de vida del paciente y la
tolerancia a los tratamientos oncológicos actuando sobre
la nutrición
• Abordaje del problema multidisciplinario con la estrecha
colaboración de los especialistas en Nutrición