Embed Size (px)
Citation preview

Fundamentals of Genetic Cancer Risk Assessment
Bita Nehoray, MS, CGCThe Faculty credentials are located in the Biography Slide and CCGCoP Education Portal under Faculty Pages
Camtasia Studio and Zoom were used to compose each module
The modules are approximately 1 hour each, for a more accurate count please refer to the course Syllabus
The Original Release Date for Distance Learning Modules is 2021. Ongoing evidence-based updates to all distance lecture modules are provided through supplemental materials and discussion facilitated during the weekly Web
Conference Review sessions held each Friday during the distance learning segment of the intensive course. Modules may also periodically be re-recorded to address significant technological and evidence-based advances in topics related
to cancer genetics and genomics.
The CME Termination Date for these Modules is: October 2025.
This Cancer Genetics Education Program (CGEP) is supported in part funding from the NIH 5R25CA171998 periodic updates have been made to several Modules

Bita Nehoray, MS, CGC, is a licensed board-certified genetic counselor specializing in cancer genetics. She received her Master’s degree in Human Genetics and Genetic Counseling from Stanford University. Ms. Nehoray joined the City of Hope Division of Clinical Cancer Genomics in 2012, where she provides cancer genetics services for patients and families suspected to have a hereditary predisposition to cancer, with a focus in Li-Fraumeni syndrome. She is fluent in Spanish and Farsi and is committed to advancing the provision of cancer genetics services to medically underserved and culturally diverse populations. Current research projects include understanding cancer risk, penetrance, prevalence, and clinical outcomes for individuals with TP53pathogenic variants as part of the LiFT UP study, evaluating the spectrum of germline variants in Israeli breast cancer patients, and assessing community-based provider experiences with polygenic risk scores in genetic cancer risk assessment. She also serves on the genetic counseling advisory committee for the Li-Fraumeni Syndrome Association. She is an active member of the National Society of Genetic Counselors, Southern California Genetic Counselors, and the American Society of Human Genetics.
BIOGRAPHY:

• Consultant for Invitae Corporation
Disclosures:

Fundamentals of Genetic Cancer Risk Assessment
Bita Nehoray, MS, CGC Senior Genetic Counselor
Division of Clinical Cancer Genomics, City of Hope

Learning objectives
After completing this module the participant should be better able to:
• Describe fundamentals of the genetic cancer risk assessment (GCRA) process
• Take a comprehensive cancer family history• Explain the importance of and strategies for confirming key cancers• Identify sporadic, familial, and hereditary cancer patterns

Objective
Describe fundamentals of the genetic cancer risk assessment (GCRA) process

Genetic Cancer Risk Assessment (GCRA)
A specialized clinical practice employing genetic and genomic tools to identify individuals and families with inherited cancer risk.
• Requires knowledge of:• Genetics • Oncology• Individual and family counseling skills

Why does it matter?
GCRA allows us to:• Identify individuals with inherited cancer risk• Recommend high-risk screening and preventive care• Reduce cancer burden

Established standards of practice for GCRA
Healthcare professional organizations (ASCO, NSGC, ONS) have set forth guidelines outlining standards of practice for:• Cancer risk counseling• Risk assessment• Genetic testing

Established standards of practice for GCRA• Introduction/engagement• Document patient and family cancer history• Assess psychosocial and interpersonal dynamics• Discuss basic principles of cancer genetics• Assess/interpret personal and family medical history to establish a differential
diagnosis• Assess mutation probabilities/empiric risks• Develop genetic testing strategies• Facilitate informed consent when test pursued• Physical examination• Disclose/interpret results• Develop personalized risk management plan• Case administration and management
Weitzel, et al. CA Cancer J Clin. Sept-Oct 2011;61(5):327-59.

Models of practice for GCRA
• Practice models are evolving to accommodate the growing demand and the limited time/resources for GCRA
• Academic/Comprehensive model• Community models
• Medical practice model• Genetic referral model• Triage model• Group counseling model• Telemedicine model• Remote open-access model
• Direct Access Testing/CareStoll, et al. Am J Med Genetic C Semin Med Genet. 2018 Mar;178(1):24-37.
Weitzel, et al. CA Cancer J Clin. Sept-Oct 2011;61(5):327-59.
Raspa, et al. Interact J Med Res. 2021 Feb 25;10(1):e23523.

Key components of GCRA
While models vary based on practice setting and resources, comprehensive GCRA will entail one or more consultative sessions:
Pre-test consultation Results disclosure

Key components of the pre-test consultation
• Engage patient & assess concerns/motivations• Document patient and family cancer history• Explain principles of heredity and cancer genetics• Facilitate informed consent; initiate testing

Key components of results disclosure
• Interpret/communicate genetic test results• Provide personalized risk management recommendations and
resources• Facilitate adaptation and coping with impact of result• Assist patient with plan for communication of
results/recommendations with at-risk family members

Getting started
• Establish rapport and contract with the patient• Assess patient concerns and motivations for GCRA• Clarify misconceptions• Determine perception of cancer risk and basis for perceived risk
http://juanaraujo.com.br/category/blog/

Factors influencing risk perception
• Personal/family experience with and communications about cancer• Personality traits, coping style, risk tolerance level• Perceptions, beliefs, attitudes about health and illness• Age, education, occupation• Cultural, social, religious norms
https://www.avetta.com/blog/will-i-need-do-risk-assessment-every-job

Objective
Take a comprehensive cancer family history

Why is a detailed family history so important?
• GCRA is dependent on the gathering of accurate, detailed, and relevant information and the family history is a fundamental component of this process
• Provides basis for:• Making a diagnosis• Determining risk• Making recommendations for medical management• Assessing the needs for patient education and psychosocial support
Schuette, J.L., et al. (2009). The Ultimate Genetic Tool: The Family History.

Family history should be obtained for ALLpatients• Who?
• Consultand/Client= individual(s) seeking genetic evaluation• Proband= affected family member who brings family to medical attention
• What?• Identify the reason for GCRA
• Where?• Obtain the family history in a comfortable and confidential environment
• When?• Usually obtained in the client’s presence• If using family history questionnaires in advance of the appointment, confirm
the reported history in client’s presence

Taking a comprehensive family history
• At least 3-generations for each lineage• Specify exact biological relationship• Age, or age/cause of death• All cancers and age at diagnosis • Determine if primary, recurrence, or metastatic disease• Location of primary cancers, stage, laterality, treatment• Pertinent chemoprevention/surgeries*• Predisposing conditions/precursor lesions• Pertinent physical findings*e.g. tamoxifen, OCPs, hysterectomy, oophorectomy, mastectomy, colectomy, gastrectomy, thyroidectomy

Taking a comprehensive family history (cont.)
• Current health status/significant illnesses• Reproductive history/issues (e.g., infertility, OCP/HRT use)• Congenital anomalies• Environmental exposures (e.g., radiation, chemicals, second-hand
smoke, tobacco use, alcohol consumption, excessive sun exposure)• Ethnicity/Ancestry (including if Ashkenazi or other Jewish ancestry)

More than just a family history…
• Careful exploration of the family history may also bring insight into the family’s…• Prior discussions of genetic counseling/testing
• Experience with and perception of cancer risk, screening, diagnosis, treatment, outcomes
• Social relationships and communications between/among relatives
• Potential for ethical dilemmas (e.g., biological relationships, sharing of information)
• Coping style/skills, potential for psychological distress
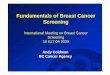
The pedigree
• Quick and accurate visual record assisting in providing genetic counseling and disease risk assessment.• Standardized human pedigreenomenclature has been
adopted internationally.
NCCN, 2021Bennett, et al. J. Genet Counseling 17: 424-433, 2008

Demonstrating relationshipsrelationship line
descent line sibship line
individual’s line
Consultand and/or Proband

Three generation pedigree

Use the pedigree to help determine
• Probability of hereditary cancer predisposition• Cancer risk for patient, family members• Cancer cases needing confirmation/documentation• Genetic testing-if appropriate, test(s) to offer, who to test• Need for screening, prevention, support services• Eligibility for research study participation

Objective
Explain the importance of and strategies for confirming key cancers

Reliability of reports
• Reports of breast cancer in first degree relatives are highly reliable (>90%)
• Tendency to over-report with multiple relatives• Reports of “female” gynecologic cancers may be inaccurate• Metastatic disease and recurrences are often reported as new
primary cancers
Parent ME et al 1997 J Cancer EducEeorola H et al, 2000 Eur J Cancer

“Women’s Cancer”
• Used to describe• Uterus• Ovaries• Cervix
• Paramount to differentiate to • Decide if testing is appropriate• Decide which genes to test• Provide appropriate empiric risks and management recommendations
http://my.clevelandclinic.org/services/ob-gyn-womens-health/departments-centers/gynecologic-oncology

Tools for verification
• Confirm verbal reports with documented records• Pathology reports• Medical records• Death certificates
• Consider• Natural history of disease• Symptoms• Treatment

Objective
Identify sporadic, familial, and hereditary cancer patterns

SPORADIC FAMILIAL HEREDITARY
FeaturesFew affected family members
Caused by an accumulation of mutations throughout lifeNot hereditary
FeaturesClusters of cancer in a family
Genetic predisposition is not evident in the family history
FeaturesCancer in more than 2 generationsCaused by mutations in genes
Bilateral breast cancer
Multiple related cancers

When to suspect hereditary cancer
• Earlier age at diagnosis than expected• Multiple generations with cancer• Multiple cancers in one generation• Rare types of cancer• Bilaterality• Constellation of tumors characteristic of a specific syndrome

When to suspect hereditary cancer
• No family history of cancer, however:• Limited family structure• Little information about the family• Relatives are young• Early age at diagnosis (single case indicator)• “Skipped” generations (incomplete penetrance)• Risk-reducing chemoprevention/surgeries• Possibility of de novo mutations• Populations with founder mutations

Family structure may limit risk assessment
Limited family structure:Fewer than 2 first- or second-degree female relatives older than age 45
in one lineage (maternal or paternal)
Weitzel et al. 2007. Limited Family Structure and BRCA Gene Mutation Status in Single Cases of Breast Cancer. JAMA. Vol. 297(23).

Diagnosed ≤ 50y with an
unknown or limited family
history
The probability of mutation detection associated with these criteria will vary based on family structure. Individuals with unknown or limited family history/structure, such as fewer than 2 first- or second-degree female relatives having lived beyond age 45 in either lineage, may have underestimated probability of familial mutation detection. The likelihood of mutation detection may be very low in families with a large number of unaffected female relatives. Clinical judgment should be used to determine the appropriateness of genetic testing. The maternal and paternal sides should be considered independently. – NCCN, 2016

When should genetic testing be offered?
• When there is a reasonable likelihood of identifying a cancer predisposing mutation
• When there is a genetic test available that can be adequately interpreted
• When the results will influence the patient and/or their family’s healthcare • Patient wants information (empowerment)
https://www.samahope.org/dont-dna-test-just-buy-scale/ASCO, 2003; NCCN, 2021
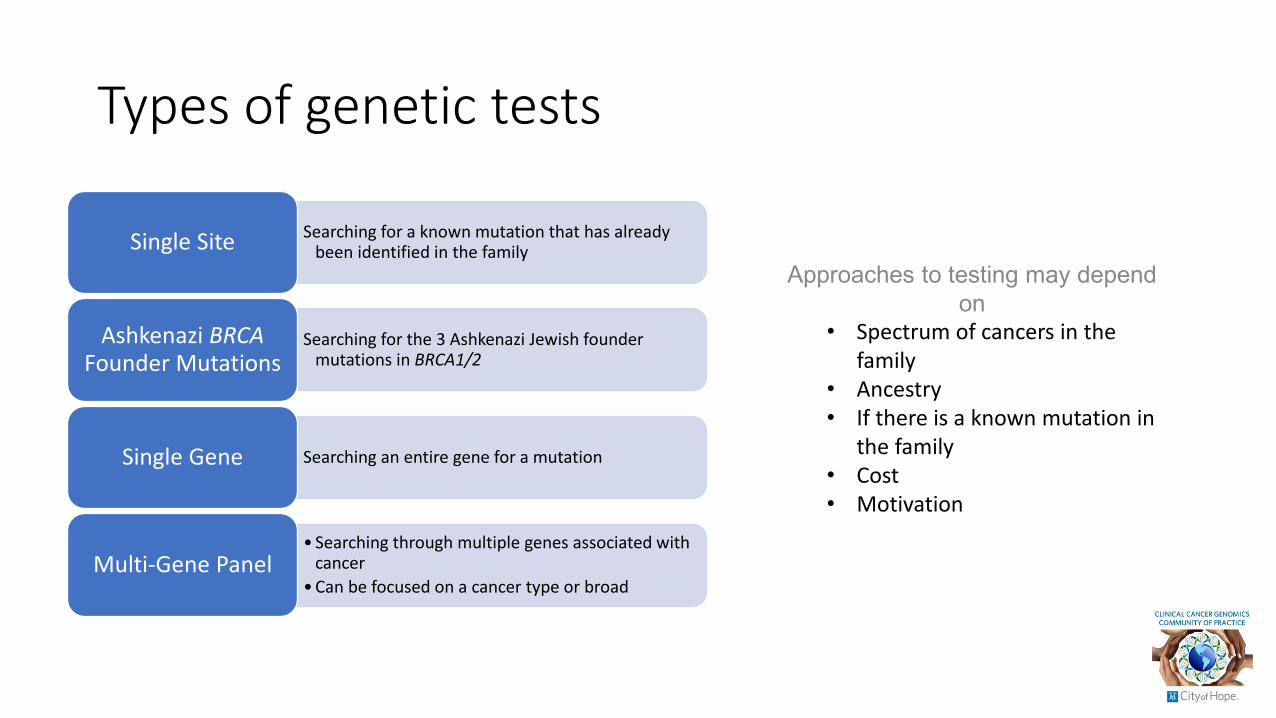
Types of genetic tests
Searching for a known mutation that has already been identified in the familySingle Site
Searching for the 3 Ashkenazi Jewish founder mutations in BRCA1/2
Ashkenazi BRCAFounder Mutations
Searching an entire gene for a mutationSingle Gene
• Searching through multiple genes associated with cancer
• Can be focused on a cancer type or broadMulti-Gene Panel
Approaches to testing may depend on
• Spectrum of cancers in the family
• Ancestry• If there is a known mutation in
the family• Cost• Motivation

Deciding which test to order
• Review the pedigree for cancers that may have a genetic etiology• Assess for syndromic patterns of cancer• Review established consensus testing guidelines (NCCN, IGCLC, etc.)• Establish a differential diagnosis

When to consider additional/updated testing
BRCA sequencing
commercially available
BRCA rearrangement
analysis commercially
available
Multi-gene panel testing (sans BRCA)
Supreme court ruling
invalidating BRCA gene
patents
Multi-gene panel testing increasingly becomes common
practice 2013201220061996

When to consider additional/updated testing
Some reasons to consider update testing, particularly if prior testing was
uninformative with respect to explaining personal and/or family history:
• Young age at diagnosis
• Criteria met for genes/syndromes not captured on prior testing
• Update to testing technologies since last test (e.g. rearrangement analysis needed)
• Family history is very suggestive of an inherited cancer syndrome
• Considerable time has passed since past testing was completed
• Highly motivated/information seeking patient

Providing informed consent
• Description of the test• Implications of the results• Alternatives• Costs/insurance coverage• Ethical, legal, social issues (“ELSI”) including any discrimination
concerns and family impact
Ultimately, testing is the individual’s choice.

Pre-test consultation
• Anticipatory guidance• Help patient/family understand and consider the medical and psychosocial
implications of testing• Role play “what if” scenarios
• Determine motivations and expectations• Are they realistic?
• Create a plan for results disclosure• Timeframe• Method (e.g. in person, phone)• Who will be present

Pre-test consultation (cont.)
• Possible test result outcomes• Positive• Inconclusive (variant of uncertain significance)• Negative (including uninformative vs informative negatives)
• Prepare for emotional reactions• Patient• Family• Provider

Results disclosure
• Interpret results clearly at patient’s level of understanding• Provide individualized risk management recommendations for patient• Elicit patient feedback and questions• Any additional testing indicated• Implications for family members
• Management• Testing• How to communicate results to family members
• Referrals • Follow-up/re-contact plan

Education/counseling strategies
• Communication• Tailor your discussion to the patient/family’s level of understanding
• Simplified concepts• Analogies• Cultural sensitivity
• Tools• Diagrams• Printed materials• Reliable websites• Decision aids
1 in 20
5%

Back to care delivery models…

Traditional care delivery models
• Traditional care delivery models are time intensive and are exacerbated by the limited genetics workforce but high demand for genetics care.
• Barriers• Geography• Wait time• Limited number of clinical geneticists/genetic counselors

Challenges to delivering GCRA and possible solutions
Raspa, et al. Interact J Med Res. 2021 Feb 25;10(1):e23523.
Limited # of genetic specialists
• Alternative delivery models (telegenetics, group counseling, use of extenders)
• GCAs• Health technologies and
patient education tools
Wait time and length of appointments
• Alternative delivery models (telegenetics, embedding genetics provider in non-genetic clinical settings)
• Health technologies and patient education tools
Delivery of services by non-genetics providers
• Alternative delivery models (provider-to-provider consultations, partnership model)
• Training and education resources
• Health technologies and patient education tools

Alternative care delivery models
• Telegenetics (Provider-to-Patient)• Video or telephone-based delivery for some or all encounters• Delivered as a group or individually• Benefits: See more patients, reduce wait time, improve costs, reduced travel time
and increase convenience for patients• Challenges: Technical problems or limited access (e.g. web-based platforms),
preference for in-person care by some patients/providers resulting in reduction in the quality of the interaction
• Group counseling• Benefit: Increased efficiency by decreasing time spent with patients• Challenge: Most patients preferred individual counseling to group counseling
Stoll, et al. Am J Med Genetic C Semin Med Genet. 2018 Mar;178(1):24-37.
Weitzel, et al. CA Cancer J Clin. Sept-Oct 2011;61(5):327-59.
Raspa, et al. Interact J Med Res. 2021 Feb 25;10(1):e23523.

Alternative care delivery models
• Telegenetics (Provider-to-Provider)• Primary care providers have access to specialty providers• Patterned after the extension for Community Healthcare Outcomes model
• Partnership models between genetics & non-genetics providers• Multidisciplinary team based/collaborative approach• Benefits: Ability of the genetic counselor to build a long-term relationship
because of the frequency of visits, reducing burden of frequent visits to see each provider separately, reduced financial burden to patients
Stoll, et al. Am J Med Genetic C Semin Med Genet. 2018 Mar;178(1):24-37.
Weitzel, et al. CA Cancer J Clin. Sept-Oct 2011;61(5):327-59.
Raspa, et al. Interact J Med Res. 2021 Feb 25;10(1):e23523.

Direct-access testing
• Testing marketed directly to consumers• Also known as: Direct-to-consumer; Direct access; Patient initiated testing; At-home
genetic/DNA testing• Genetic testing may be completed with/without a patient-provider
interaction• Some companies offer the option to opt-in or out of genetic counseling
provided by the company• Know the offerings/limitations for each company and their test offerings
• Reporting process (VUS, reclassifications)• Coverage (e.g. full gene vs hotspots/SNPs)• Is confirmation testing/repeated testing through another lab warranted?

Clinic efficiencies/resources
• Documentation• Use of templates for clinic notes and patient facing materials/letters
• Clinic-based questionnaires to collect medical/family history• Paper• Electronic
• Educational materials/counseling aids• Health technologies and patient educational tools
• Chatbots• Consenting videos
• Genetic counseling assistants

Summary
• GCRA requires recognition of patient characteristics, family history, knowledge about genetic test options and testing strategies
• Explain concepts at the level of comprehension of the patient • A detailed family history is an integral part of GCRA and necessary in order to
perform accurate and tailored risk assessment• Anticipate and discuss potential ethical, legal, social and risk management issues
before testing• Provide risk-appropriate surveillance and management guidelines for all cases• Question as needed (reliability of reports, motivations, risk perception,
comprehension)• Consider a care delivery model that works best for your patient population; there
is no one size fits all!

Thank You!