Embed Size (px)
Citation preview

Medical and Pediatric Oncology 6:15-22 (1979)
Fungal Peritonitis and Malignancy: Report of Two Patients and Review of the Literature Gene Kopelson, MD, Margarita SiIva-Hutner, P ~ D , and James Brown, MD
Departments of Medicine (Divisions of Clinical Oncology and Infectious Diseases), and Dermatology, and the Mycology Laboratory, Columbia-Presbyterian Medical Center, New York
Two patients developed isolated Candida albicans peritonitis in association with intraabdominal malignancy. Although additional factors predisposing to the development of fungal peritonitis were present, we postulate that tu- mor-related local factors permitted fungi t o cross the gut wall and to enter the peritoneum, where the host immune status determined whether the infec- tion spread. These two cases are the sixth and seventh reported cancer patients who developed fungal peritonitis, but the first two who had the fungal infec- tion localized to the peritoneum; and this is the first report known to us specifically associating intraabdominal malignancy and fungal peritonitis. Pa- tients who develop fungal peritonitis may have a primary or metastatic intra- adbdominal malignancy, and fungi should be considered as a cause of peritoni- tis in cancer patients.
Key words: peritonitis, candidiasis
INTRODUCTION
The increased risk of systemic fungal infection in cancer patients is well known [ 1-51. However fungal peritonitis, itself uncommon [ 6 ] , rarely has been described in cancer pa- tients [7-1 l ] . We report two patients with intraabdominal neoplasm who developed fungal peritonitis, review the literature on this subject, and discuss possible pathophysiological mechanisms and clinical implications.
During part of the preparation of this manuscript, Dr. Kopelson was a Senior Medical Student, College of Physicians and Surgeons, Columbia University. His present address is Department of Radiation Med- icine, Massachusetts General Hospital, Boston, MA 021 14 Address reprint requests to Dr. Margarita Silva-Hutner, Mycology Laboratory, Columbia-Presbyterian Medical Center, 630 West 168 Street, New York, NY 10032.
0098-1532/79/0601-0015$01.70 0 1979 Alan R. Liss, Inc.

16 Kopelson, Silvs-Hutner, and Brown
Case 1 (AS 237-3602] A 58-year 011 white male presented with epigastric pain, jaundice, and weight loss.
During initial evaluation at another hospital, he was found to have hepatomegaly, a left Mar mass on chest roentgenogram, and a sputum cytology positive for malignant cells. Treatment a t this time included hyperalimentation via an indwelling plastic catheter, in- sertion of a foley catheter, and intravenous cephalothin. He was transferred to the Colum- bia-Presbyterian Medical Center following a massive upper gastrointestinal hemorrhage, and upon admission was cachexic with a temperature of 101.4"F. Cephalotlun was dis- continued, and intravenous ampicillin was substituted. On the fourth hostpital day, he developed ascites and a tender right-upper-quadrant mass. Abdominal ultrasound dis- closed dilatation of the gallbladder. Additional laboratory studies included: white blood count 5800/mm3 (93% polys and 7% lymphocytes), bilirubin 20 mg%, gamma glutamyl transpeptidase 770 units, BUN 64, creatinine 6.3 mg%. Chest roentgenogram showed the previously-mentioned left hilar mass with no evidence of pulmonary parenchymal abnor- mality. Celiac axis angiography showed no intestinal lesions and gastroscopy showed only gastritis. On the fifth day he underwent an exploratory laparatomy that disclosed 2.5 liters of serosanguinous ascitic fluid, a dilated and thickened gallbladder, and a hard mass in the pancreas. The liver was normal in appearance except for a coating of fibrinous exudate. A cholecystostomy was performed and biopsies were obtained of the liver and omentum. Subsequently. the patient deteriorated rapidly, and he died on the second post- operative day. Postmortem permission was refused.
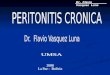
Routine culture of the ascitic fluid was postive for Candida albicans; multiple blood, urine, and other cultures were negative for any organisms. The liver capsule had clusters of thin hyphae, pseudo-hyphae and blastopores typical of Candida albicans (Fig. 1); the liver parenchyma did not contain fungi. The omentum showed focal necrosis and a few small areas invaded by thin Candida hyphae and yeast cells. In addition, the omentum had numerous foci consisting of wider, clustered, radiating, branching, septate hyphae compatible with Aspergillus (Fig. 2 ) . There was minimal histologic evidence of inflamma- tory cell response. The liver biopsy showed parenchymal bile stasis and periportal clustkrs of highly anaplastic cells of uncertain primary origin.
Case 2 (JP 192-00-81 1 A 75-year old white male was admitted to the Columbia-Presbyterian Medical Cen-
ter with a one day history of abdominal pain, nausea, and vomiting. Barium enema demonstrated a constricting lesion of the sigmoid colon with radiographic characteristics of a neoplasm. Over the next two days while undergoing preparation for surgery, the patient developed clinical evidence of peritonitis. White blood count at this time was 6200/mm3(78% polys, 18% lymphocytes). He was placed on clindamycin and gentamicin. At laparotomy several hours later, two liters of bile-stained ascitic fluid, diffuse fibrinous peritonitis, and a free perforation of a duodenal ulcer were found. The duodenal ulcer was plicated, and a left hemicolectomy was performed. The peritoneal cultures grew Candida albicans. Histologically the patient's neoplasm was a moderately well-differen- tiated adenocarcinoma, transmural in extent, with 3/3 positive mesocolic lymph nodes (Dukes C). Postoperatively the patient continued t o drain bilious fluid from the abdomen which on direct examination showed yeast with mycelia, and on repeated culture showed Candida albicans. He defervesced and cleared all evidence of peritonitis while receiving antibiotic therapy consisting only of clindamycin and gentamicin without fungicidal

Fungal Peritonitis and Malignancy 17
Fig. 1. Hyphae, pseudohyphae and blastospores of Candida albicans on liver capsule of patient 1 , stained with periodic acid-Schiff (PAS), X 337.
Fig. 2. Branching septate hyphae in clusters compatible with Aspergillus on omentum of patient 1 , stained with PAS, X 337.

18 Kopelson, Silva-Hutner, and Brown
agents. Candida serology showed negative precipitin reaction but postive agglutinin titers of 1 :320. The patient recovered fully and left the hospital without evidence of neoplasm or infection.
DISCUSSION
Disruption of anatomic barriers by disease or iatrogenic procedures predisposes pa- tients to systemic mycoses; cancer patients have the added predisposing factor of defec- tive host immunity due to the tumor itself or to anti-neoplastic therapy [ l , 12, 131. Fun- gal peritonitis, on the other hand, has always been associated with direct peritoneal con- tamination (intestinal perforation, abdominal surgery, or peritoneal dialysis [6, 14-1 61 ), although many of the reported patients also had received steroids.
Fungal peritonitis rarely has been reported in cancer patients. In one series of 494 febrile adults with leukemia in whom infection was sought, although 68 fungal infections were found, in none was fungal peritonitis documented [17] . Hutter and Collins found two abdominal cavity cultures positive for Candida in 202 cancer hospital patients with fungal infections, but specific case histories were not mentioned [9].
mens were sent to the Mycology Laboratory of the Columbia-Presbyterian Medical Center for fungal cultures. Of these 74, 13 (1 8%) were positive for fungi. And of these 13,2 (1 5%) were associated with intraabdominal neoplasm.
A review of the literature reveals to our best knowledge only five previously reported patients with both cancer and fungal peritonitis; they are summarized along with our two patients in Table I.
spread C albicans infection”; apparently this fungal infection was not localized to the peritoneum, and predisposing factors other than the tumor were not mentioned [8]. The patient mentioned by Louria et al had tumor resection, multiagent chemotherapy (cyclo- phosphamide and actinomycin-D), indwelling catheters and methicillin prior to fungal peritonitis; in addition multiple blood cultures grew the organism, and that patient also did not have isolated fungal peritonitis [ lo] . The patient described by Symmers had widespread intraabdominal cancer plus intraperitoneal radioactive gold as another pre- disposing factor [ 111. In the patients described by Bernhardt et al [7] and Bayer et al [6] , predisposing factors included gastrointestinal surgery and instrumentation; the pa- tient of Bayer et a1 also had steroids [6] . That cultures were positive from multiple sites in one patient [7] and visceral involvement found at autopsy in the other [6] makes it clear that the fungal infection was not limited to the peritoneum in them.
In our patient 2, the development of a perforated duodenal ulcer most likely ex- plains the pathogenesis of the infection; however the presence of mycelial forms indicates that the infection may very well have been present for much longer than this [ 131 at a time when the only major factor was the intraabdominal tumor (and an as-yet-unper- forated ulcer). However in patient 1, iatrogenic factors and gastrointestinal bleeding were all predisposing factors. But in both patients, multiple blood and other cultures remained negative. Indeed the unique picture presented by our two patients was that of localized fungal peritonitis in association with intraabdominal cancer in which known predisposing factors were minimal; the one factor common to both patients which pos- sibly could explain such isolated fungal peritonitis was the extant intraabdominal cancer
During the period from July 1, 1975, to March 31, 1977,74 peritoneal fluid speci-
The patient described by Bodey developed pelvic peritonitis secondary to “wide-

Fungal Peritonitis and Malignancy 19
(patient 1 with secondary liver involvement [possibly from a pancreatic primary], and patient 2 with a primary colon cancer).
It is known that besides causing local effects, gastrointestinal tumors may affect remote parts of the gastrointestinal system [18]. It is also known that Candida albicans, a normal inhabitant of the gut [13], can migrate across the gut wall into the blood- stream [ 191 . Perhaps as-yet-unknown local or systemic factors related to the tumors, alone or in conjunction with these other known predisposing factors, permitted fungi similarly to cross the gut wall and to gain access to the peritoneum; perhaps such migra- tion was related or facilitated by the fact that the tumor of patient 2 was transmural.
Another mechanism, thought to possibly account for the occurrence of apparent spontaneous bacterial peritonitis in a patient with intraabdominal cancer, was impaired hepatic reticuloendothelial filtration of organisms due to liver metastases [20] . That this explanation may not be entirely adquate to account for the fungal peritonitis in our two patients is evidenced in that although patient 1 did have liver metastases, patient 2 had no known liver involvement.
The immune system of the host may have determined whether the fungal peritonitis evolved into sepsis: patient 1 had only microscopic metastases and patient 2 had only local nodal involvement (with subsequent isolated fungal peritonitis), whereas the other patients in Table I had more massive tumor burdens and/or were receiving immunosuppressive anti- tumor therapy (with subsequent fungal peritonitis and other visceral involvement). That other factors besides host immunity may be involved in the ability of the peritoneum to restrict fungi to the peritoneum was suggested in one series of noncancer patients with fungal peritonitis [6], in which the impermeability of functional stomata between the peritoneum and vascular channels to such organisms was thought to be a major factor.
established by culture. In addition, fungal serology demonstrated negative precipitins and high agglutinin titers in our patient 2. Such data can be consistent with visceral in- volvement even after antifungal therapy is terminated [14].
sine [6,14, 161 or abdominal drainage [6]. Although one group of patients who were untreated with amphotericin-B reportedly had a poor prognosis, this may be because that group had severe underlying diseases in which death would have been predictable anyway [ 161. However our patient 2 survived his fungal peritonitis without the aid of fungicidal agents, probably since correction of the underlying perforation controlled the infection. In patient 1, death occurred before cultures and definite pathology re- ports came, and thus no antifungal therapy was initiated.
The diagnosis of fungal peritonitis in our patients and those from the literature was
The therapy of fungal peritonitis has consisted of amphotericin-B or 5-fluorocyto-
CONC LUS I ON
Cancer patients are at the same risk for developing fungal peritonitis as other patients who have the known risk factors enumerated above. But the additional pre- sence of intraabdominal malignancy itself (locally or via a remote effect) may be an ad- ded risk factor for fungal peritonitis (possibly by in some way permitting fungi to gain access to the peritoneum and to remain localized there, and/or by tumor-caused hepatic reticuloendothelial dysfunction). Thus patients who develop fungal peritonitis may have an underlying intraabdominal cancer; and in cancer patients who develop peritonitis, fungi should be considered in the list of etiologies.

N
0
TABL
E 1.
Rep
orte
d C
ance
r Pa
tient
s W
ith F
un
d Pe
rito
nitis
Pred
ispo
sing
Fac
tors
a Fu
ngal
Cul
ture
s:
Pati-
en
t no
. U
nder
- A
nti-
Pe
ri-
Fung
al
Ant
i-
(ref
er-
Age
, ly
ing
GI
Inst
ru-
tum
or
Org
anis
m
to-
sero
l-
fung
al d
rug
ence
) se
x tu
mor
in
jury
‘ m
ente
d th
erap
y is
olat
ed
neum
Blo
od
Oth
er
ogy
ther
apy
Out
com
e
1 (t
his
58,M
re
port
)
2 (t
his
75,M
re
port
)
3 IS
] 42
,F
4 [l
o]
13,M
Live
r Y
es
Met
ast-
as
es;
unkn
own
prim
ary
Col
on
? C
arci
n-
oma
Acu
te
Mye
loge
n-
ous Leu-
kem
ia
Abd
o-
Yes
m
inal
rh
abde
m
yosa
r-
com
a w
ith
omen
tal &
pe
rito
neal
se
edin
g
Yes
No b Yes
No
Cal
bica
ns
Pos
Neg
N
eg
Not
N
one
done
No
Cal
bica
ns
Pos
Neg
b C
albi
cans
Po
s
Yes
T
glab
rata
Po
s Po
s
Neg
N
eg.P
re-
Non
e ci
pitin
s;
Pos
1:32
0 A
gglu
tinin
s b
b b
Am
pho-
te
rici
n B
b
Die
d po
st-
oper
ativ
ely
Rec
over
ed;
aliv
e an
d well b
Blo
od c
u tu
res
be-
cam
e ne
g-
ativ
e; la
ter
died
of
caus
es
unre
late
d to
fung
al
infe
ctio
n

5 [7
] 43
,F
Cer
vix
Yes
Y
es
b C
albi
cans
C
arci
nom
a
6 [6
] b,
F C
ervi
x Y
es
Yes
b C
albi
cans
C
arci
nom
a w
ith c
ar-
cino
mat
ous
smal
l bow
el
obst
ruct
ion
Pos
Pos b
Pos
b 7
[ll]
b,
F O
varia
n b
Yes
Y
es
Pgou
gero
tii
Pos
Car
cino
ma
with
intr
a-
peri
tone
al
met
asta
ses
Pos
Non
e D
ied;
auto
psy
show
ed w
ide
spre
ad v
isce
ral
fung
al in
volv
e-
men
t
b N
one
Die
d w
ith
diss
emin
ated
C
andi
dias
is
at a
utop
sy
b A
mph
o-
Die
d of
tum
or
teri
cin
B 9
mon
ths
late
r;
no e
vide
nce
of
fung
al p
erito
nitis
aOth
er t
han
mal
igna
ncy.
bN
ot s
tate
d in
rep
ort.
‘Gas
troin
test
inal
pa
thol
ogy
or su
rger
y.
? =
See
text
dis
cuss
ion.
Po
s = P
ositi
ve; N
eg =
Neg
ativ
e; G
I =
Gas
troi
ntes
tinal
; M
= M
ale;
F =
Fem
ale;
All
ages
are
in y
ears
.
00 c 2 s 2. 3.
a
U

22 Kopelson, Silva-Hutner, and Brown
ACKNOWLEDGMENTS
The authors would like to thank Doctors Saul Sanders and Leon Harisiadis for their helpful suggestions, and Dr. Raffael Lattes for reviewing some of the pathologic material.
REFERENCES
1. Dilworth JA, Mandell GL: Infections in cancer patients. Semin Oncol 2:349-359, 1975. 2. Pizzuto J, Lopez R: Opportunistic candidiasis in a group of patients with hematologic diseases,
In “Proceedings of the Third International Conference on the Mycoses.” Pan American Health Organization (Scientific Publication No. 304), Washington DC, 1975, pp 198-209.
3. Remington JS, Anderson SE Jr: Penumocystis and fungal infections in patients with malignancies. Intl J Rad Oncol Biol Phys 1:313-315,1976.
4. Rosen PP: Opportunistic fungal infections in patients with neoplastic diseases. In “Pathology Annual: 1976.” Sommers SC (ed). New York: AppletonCenturyCrofts, 1976, pp 255-315.
5 . Singer C, Kaplan MH, Armstrong D: Bacteremia and fungemia complicating neoplastic disease. Am J Med 62~732-742, 1977.
6. Bayer AS, Blumenkrantz MJ, Montgomerie JZ, Galpin JE, Coburn JW, Guzo LB: Candida peri- tonitis. Report of 22 cases and review of the English literature. Am J Med 61:832-840, 1976.
7. Bernhardt HE, Orlando JC, Benfield JR, Hirose FM, Foos RY: Diseminated candidiasis in surgical patients. Surg Gynecol Obstet 134:819-825, 1972.
8. Bodey GP: Fungal infections complicating acute leukemia. J Chronic Disease 19:667-687,1966. 9. Hutter RVP, Collins HS: The occurrence of opportunistic fungus infections in a cancer hospital.
Lab Invest 11:1035-1045.1962.
Arch Intern Med 119:247-252, 1967.
Infections.” Chick EW, Balows A, Furcolow ML (eds). Springfield, Ill: Charles C Thomas, 1975,
10. Louria DB, Blevins A, Burdick R, Lieberman P: Fungemia caused by “nonpathogenic” yeasts.
11. Symmers WStC: Histopathology of opportunistic fungal infections. In “Opportunistic Fungal
pp 269-284. 12. Louria DB: Defenses against candida infections. Intl J Rad Oncol Biol Phys 1:309-311, 1976. 13. Rippon JW: “Medical Mycology.” Philadelphia: WB Saunders, 1974, pp 175-204. 14. Mandell IN, Ahern MJ, Kliger AS, Andriole VT: Candida peritonitis complicating peritoneal
dialysis: successful treatment with low dose amphotericin-B therapy. Clin Nephrol6:429-496, 1976.
15. Montemartini C, Specchia G, Dander B: Peritonitis caused by Candidad albicans. Digestion 3:
16. Reeves KO, Ripepi AC, Carter RE Jr, Williams TW Jr: Candida peritonitis in a quadriplegic:
17. Bodey CP, Rodriguez V, Chang H-Y, Narboni C: Fever and infection in leukemic patients. Cancer
18. Troncale FJ: Distant manifestations of colonic carcinoma. Ann NY Acad Sci 230:332-337, 1974. 19. Krause W, Matheis H, Wulf K: Fungemia and funguria after oral administration of Candida albicans.
20. Isner J, MacDonald JS, Schein PS: Spontaneous streptococcus pneumonia peritonitis in a patient
368-371,1970.
treatment with amphotericinl. South Med J 65:325-328, 1972.
41:1610-1622,1978.
Lancet 1598-599, 1969.
with metastatic gastric cancer. Cancer 39:2306-2309, 1977.










![Abdominal CT Findings of Cholecystogastric Fistula · the fistula [9]. Cholangitis; peritonitis; cholecystitis intestinal obstruction gastrointestinal hemorrhage and malignancy are](https://img.pdfslide.net/doc/110x75/5f7a5d1adfd91a379605cde5/abdominal-ct-findings-of-cholecystogastric-fistula-the-fistula-9-cholangitis.jpg)