Embed Size (px)
Citation preview

Future HCV Treatment Paradigms
Mark Sulkowski, MDProfessor of Medicine
Medical Director, Viral Hepatitis CenterDivisions of Infectious Diseases and Gastroenterology/ Hepatology
Johns Hopkins Medical InstitutionsBaltimore Maryland USA

Investigational Agents for HCV
Interferons Antiviral agents
Therapeuticvaccines
Hosttarget
Replication, polyprotein processing and/or assembly
Entry
NS5Bpolymerase Inhibitors
NS3protease inhibitors
NS5Areplication complex inhibitors
2
miRNA-122 Cyclophilin
CYP inhibitors

Preclinical
Phase I
Phase II
Phase III
Filed
Boceprevir(MSD)
Telaprevir(Vertex/JJ)
TMC-435(Tibotec/JJ)
MK7009(MSD)
ITMN191/R7227 (Roche/Intermune)
BI201335(BI)
BMS650032(BMS)
GS9256(Gilead)MK5172
(MSD)
ABT450(ABT)
ACH2684(Achillion)
BMS 790052(BMS)
AZD-7295(AZN)
BMS 824393(BMS)PPI-1301
EDP-239(Enanta)
GSK
Vertex
Idenix719MSD
IFN λDebio 025/ NIM811
(Novartis)
Nitazoxamide(Romark)
Silibinine
Vitamine D
BMS
BI
ROCHE
Gilead
R7128(Roche)
GS- 7977Gilead)
BIJapan Tobacco
R0622 (Roche)Medivir (Tibotec)
GLS9393 (GSK)
BiocrystINX 189
(Inhibitrex)
BMS791325 (BMS)Filibuvir
(PFE)GS9190 (Gilead)
ANA598 (Anadys)BI201127
(BI)
Vx222 (Vertex)
ABT333ABT072 (ABT)
IDX 375 (Idenix)
IDX 184 (Idenix)
SCY-835
PPI-461
VBY-376
VX-985(Vertex)
VX-813(Vertex)
GS9451(Gilead)
RG7348(Roche)
TMC 647055 (Tibotec)
A837093(Abbott)
VX-916VX-759
CelgosivirBavituximab
Direct Acting Antivirals in Development
AVL-181(Avila)
AVL-192(Avila)
ACH-2928(Achillion)
GS-5885
Vertex
Abbott
Nucleoside NS5B
Polymerase Inhibitors
Nucleotide NS5B Polymerase Inhibitors
Non Nuc NS5BPolymerase inhibitors
NS3/4A Protease inhibitors
NS5A inhibitors
DAA combinations
Others
Cyclophilin. I
IDX 077 (Idenix)
IDX 079 (Idenix)
ABT267(ABT)
Adapted from Bourliere M, et al. Clin Res HepatolGastroenterol. 2011;35(suppl 2):S84-S95.
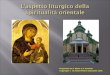
Regimens with one DAA + pegIFN alfa/RBV
Regimens with two DAAs (± pegIFN alfa and/or RBV) IFN-free Regimens
BI 201335 (PI) Daclatasvir (NS5A) Asunaprevir (PI) GS-7977 (NI) Simeprevir (TMC-435) (PI) Alisporivir (CYP) Vaniprevir (MK-7009, PI)
Daclatasvir + asunaprevir Sofosbuvir (GS-7977) + RBV Daclatasvir + asunaprevir Alisporivir ± RBV
Investigational HCV Regimens in Phase 3
New Interferons
Peginterferon-lambda-1a
NNI = non-nucleoside NS5B inhibitor, NI = nucleoside NS5B inhibitor, PI = protease inhibitor, RBV = ribavirin, NS5A = replication complex inhibitor Cyp= cyclophilin inhibitor

Multiple Combinations Will Emerge
• Different drugs can contribute variably to each goal. Not all components must be direct-acting antivirals (DAAs).
B
C
Prevention of emergent resistance (pre-existing or de novo)
+
+
AProfound suppression of broad range of viral variants, including pre-existing variants
5

INTERFERONS +/- DAA

EMERGE: PegIFN lambda-1a vs PegIFN alfa-2a in GT 2/3 HCV Treatment-Naive Pts
• Interim analysis of randomized, blinded, active-controlled phase IIb trial
Zeuzem S, et al. EASL 2012. Abstract 10.
Treatment-naive patients infected with
genotype 2/3 HCV
(N = 118)
PegIFN lambda-1a 120 µg/wk + RBV†
(n = 29)
PegIFN lambda-1a 180 µg/wk + RBV†
(n = 29)
PegIFN lambda-1a 240 µg/wk + RBV†
(n = 30)
Wk 24Genotyping at baseline
†RBV dosed at 800 mg/day for genotype 2/3 patients.
PegIFN alfa-2a 180 µg/wk + RBV†
(n = 30)

• PegIFN lambda-1a 180 μg dosage chosen for phase III trials
EMERGE: Efficacy and Safety Outcomes
Zeuzem S, et al. EASL 2012. Abstract 10.
SVR2
4 (%
)
0
40
60
80
100
65.5
20
75.9
60.053.3
N = 29 29 30 30Lambda120 µg
Lambda180 µg
Lambda240 µg
Alfa180 µg
Adverse Event, %Lambda180 µg(n = 29)
Alfa180 µg(n = 30)
Hemoglobin low<10g/dL or ∆ > 3.4 g/dL 6.9 44.8
RBV dose reduction(Hemoglobin associated) 0 23.3
Neutrophils low< 750/mm3 0 27.6
Platelets low< 100,000/mm3 0 24.1
PegIFN dose reduction(hematologic abnormality) 0 23.3
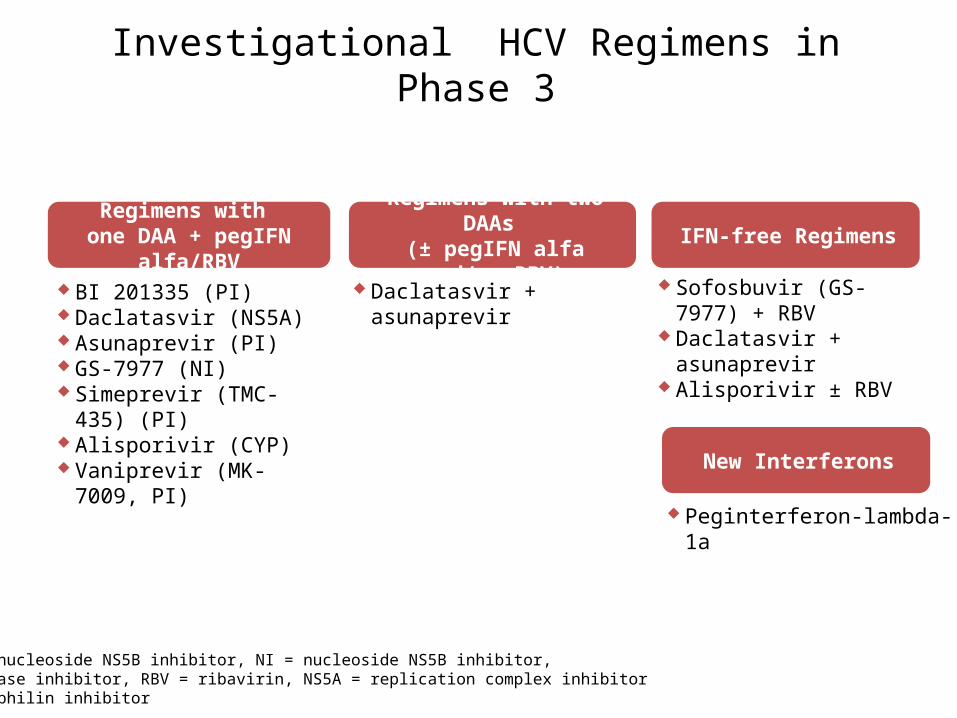
ATOMIC: Sofosbuvir (GS-7977 (NI) + PegIFN/RBV
Kowdley KV, et al. EASL 2012. Abstract 1
GS-7977 + PR
n=125
n=155
GS-7977 + PR
GS-7977 + PR
n=52
weeks0 24
GS-7977 ± RBV
RVR
98
97
94
SVR4
92
92
94
SVR12
NA
NA
90
EOT
99
99
98
Treatment naïve, mainly Gen1 (few G4/6), non-cirrhotic
No S282T mutation seen in 4 relapse pts
12
Viral Response Rates (%)

ASPIRE: Simeprevir (PI) + PegIFN/RBV in Treatment Experienced Patients
Zeuzem S, et al. EASL 2012. Abstract 2
Simeprevir
+ P/R
weeks0 48
Treatment experienced, G1, includes cirrhotics
PegIFN + RBV
12
n=66
Simeprevir +
PegIFN/RBVPegIFN + RBV
Simeprevir + PegIFN + RBV
24
n=68
n=66
PegIFN + RBV
n=65
100
80
60
40
20
0
85*
SVR2
4 (%
)
75*
19
51*
9
37
Relapsers PartialResponders
Null Responders
* Represents pooled simeprevir duration at 150mg dose
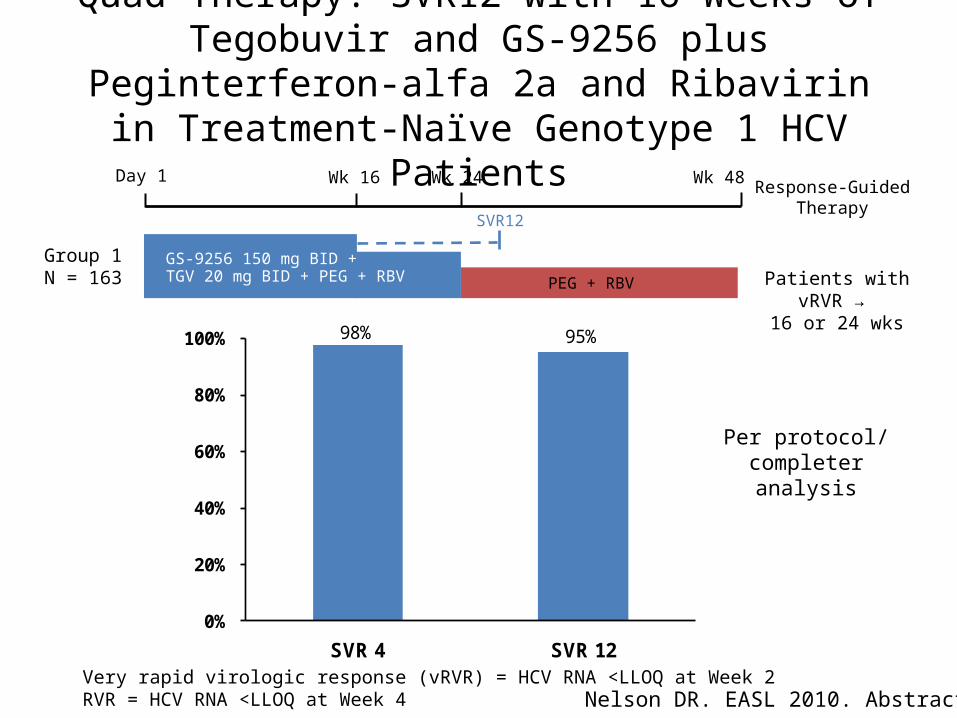
Quad Therapy: SVR12 with 16 Weeks of Tegobuvir and GS-9256 plus Peginterferon-alfa 2a and Ribavirin in
Treatment-Naïve Genotype 1 HCV Patients
Patients with vRVR → 16 or 24 wks
Group 1N = 163
Very rapid virologic response (vRVR) = HCV RNA <LLOQ at Week 2RVR = HCV RNA <LLOQ at Week 4
PEG + RBV
GS-9256 150 mg BID +TGV 20 mg BID + PEG + RBV
Day 1 Wk 48Wk 16 Wk 24 Response-Guided Therapy
SVR12
98% 95%
0%
20%
40%
60%
80%
100%
SVR 4 SVR 12
Nelson DR. EASL 2010. Abstract 12
Per protocol/ completer analysis
CYCLOPHILIN INHIBITOR + RBV

VITAL-1: Alisporivir-Based Therapy for Trt-Naive GT2/3 Pts
Pawlotsky JM, et al. EASL 2012. Abstract 1405.
Treatment-naive patients
with chronic GT 2/3 HCV infection
(N = 340)
Alisporivir 1000 mg QD
(n = 83)
Alisporivir 600 mg QD + RBV
(n = 84)
Alisporivir 800 mg QD + RBV
(n = 94)
Wk 24Stratified by HCV RNA and HCV genotype
Alisporivir 600 mg QD + PegIFN
(n = 39)
PegIFN alfa-2a/RBV (n = 40)
All pts received alisporivir loading dose of 600 mg BID during first wk. PegIFN alfa-2a dosed 180 µg/wk. RBV dosed 800 mg/day.
Wk 4: RVR assessed Wk 6
24-wkF/U
Alisporivir 600 mg QD + PegIFN/RBV
Alisporivir 1000 mg QD
Alisporivir 600 mg QD + PegIFN/RBV
Alisporivir 600 mg QD + RBV
Alisporivir 600 mg QD + PegIFN/RBV
Alisporivir 800 mg QD + RBV 800 mg/day
Alisporivir 600 mg QD + PegIFN/RBV
Alisporivir 600 mg QD + PegIFN
RVR:
No RVR:
RVR:
No RVR:
RVR:
No RVR:
RVR:
No RVR:

VITAL-1: SVR12 by Per-Protocol Analysis
• High SVR rates with alisporivir-based therapy, including IFN-free regimens– However, development of alisporivir currently on hold due to 3 cases of pancreatitis
(with 1 death) in > 1800 patients treated to date
Pawlotsky JM, et al. EASL 2012. Abstract 1405..
Overall SVR12 SVR12 in Pts Receiving IFN-free Therapy
SVR1
2 (%
)
0
40
60
80
100
20
ALV1000
81 83 81 77
58
ALV600RBV
ALV800RBV
ALV600Peg
P/R0
40
60
80
100
20
ALV1000
8293 91
ALV600RBV
ALV800RBV
82 84 93 39 40n = 17 29 32n =

PI +/- NON-NUCLEOSIDE POLYMERASE INHIBITOR +/- NS5A INHIBITOR +/- RBV

Co-Pilot (M12-746) Study: ABT-450/r + ABT-333 Treatment
ABT-450/r 250/100 mg QD + ABT-333 400 mg BID + RBV
Arm 1Treatment-naïve (N=19)
ABT-450/r 150/100 mg QD + ABT-333 400 mg BID + RBV
Arm 2Treatment-naïve (N=14)
ABT-450/r 150/100 mg QD + ABT-333 400 mg BID + RBV
Arm 3Prior P/R non-responders (N=17)
12 Weeks (On Treatment) Follow UpPeriod
Poordad F, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1399.

Co-Pilot Study: Demographics and Baseline Characteristics
Arm 1N=19
Arm 2N=14
Arm 3N=17
Male, n (%) 10 (52.6) 14 (100) 11 (64.7)White, n (%) 15 (78.9) 12 (85.7) 13 (76.5)Hispanic/Latino, n (%) 3 (15.8) 0 4 (23.5)Mean Age ± SD (years) 53.6 ± 9.78 50.9 ± 10.45 52.3 ± 9.03Mean BMI ± SD (kg/m2) 27.3 ± 3.84 24.6 ± 3.08 27.6 ± 4.65
IL28 genotype , n (%) CC CT TT
10 (52.6)7 (36.8)2 (10.5)
5 (35.7)7 (50.0)2 (14.3)
012 (70.6)5 (26.3)
HCV genotype, n (%) 1a 1b
17 (89.5)2 (10.5)
11 (78.6)3 (21.4)
16 (94.1)1 (5.9)
HCV RNA Mean ± SD (log10 IU/mL) >800,000 IU/mL, n (%)
6.25 ± 0.8014 (73.7)
6.44 ± 1.1511 (78.6)
6.93 ± 0.4717 (100)
Non-responder status Partial responder Null responder
- - 11 (64.7)6 (35.3)
Poordad F, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1399.

Co-Pilot Study: Virologic Results
Poordad F, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1399.

ABT-267 + PegIFN/RBV in treatment-naïve subjects Results
cEVR, complete early virological response; LLOD, lower limit of detection (15 IU/mL); LLOQ, lower limit of quantitation (25 IU/mL); P/R, PegIFN/RBV;SE, standard error; QD, once daily
• Safety:− ABT-267 had an adverse event profile similar to placebo− No serious adverse events
EASL, Barcelona, Spain, 18–22 April 2012; Abstract 1210
Placebo ABT-267 5 mg QD
ABT-267 50 mg QD
ABT-267 200 mg QD
0
10
20
30
40
50
60
70
80
90
100
33
87.5 8675
33
12.5
<LLOQ, <LLOD
Pati
en
ts a
ch
ievin
g W
eek 1
2 c
EV
R
(%)
66%
100%
86%
75%
Week 12 cEVR rates

A Randomized, Open Label, Multi-center Study to Evaluate the Antiviral Activity, Safety, and Pharmacokinetics, of ABT-450
With Ritonavir (ABT-450/r) in Combination With ABT-267 and/or ABT-333 With and Without Ribavirin (RBV) in
Treatment-Naïve and Null Responder Subjects With Genotype 1 Chronic Hepatitis C Virus Infection
• N = 560 • 14 active treatment arms testing combinations of DAAs and
RBV– No interferon
• This study is ongoing, but not recruiting participants
ClinicalTrials.gov Identifier: NCT01464827
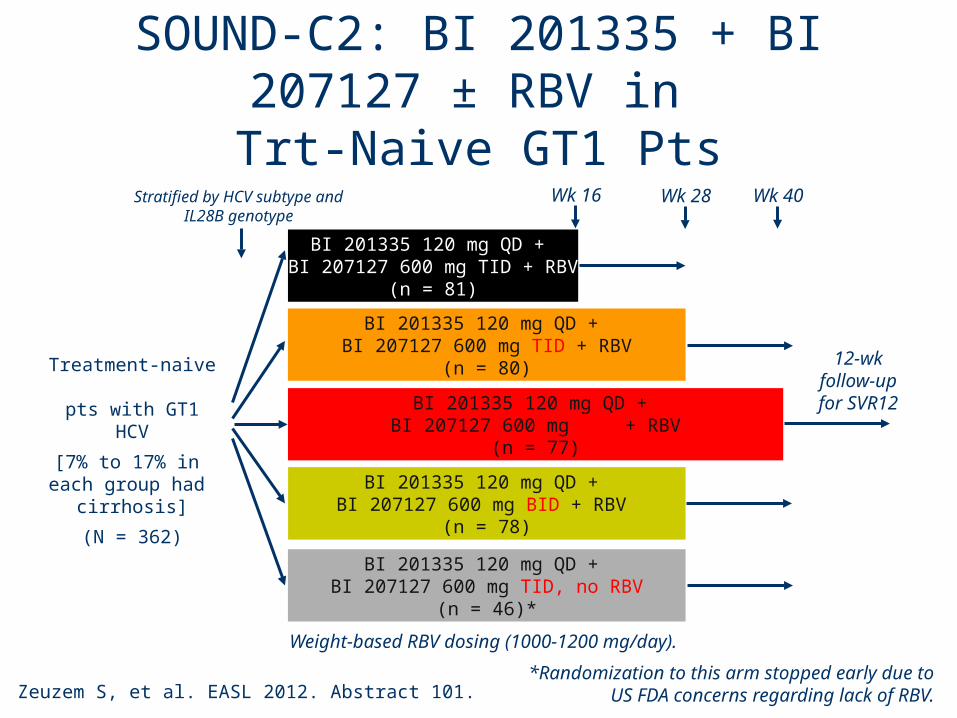
SOUND-C2: BI 201335 + BI 207127 ± RBV in
Trt-Naive GT1 Pts
Zeuzem S, et al. EASL 2012. Abstract 101.
Treatment-naive pts with GT1 HCV
[7% to 17% in each group had
cirrhosis]
(N = 362)
BI 201335 120 mg QD + BI 207127 600 mg TID + RBV
(n = 81)
BI 201335 120 mg QD + BI 207127 600 mg TID + RBV
(n = 80)
BI 201335 120 mg QD + BI 207127 600 mg TID + RBV
(n = 77)
Wk 16
BI 201335 120 mg QD + BI 207127 600 mg BID + RBV
(n = 78)
BI 201335 120 mg QD + BI 207127 600 mg TID, no RBV
(n = 46)*
Stratified by HCV subtype and IL28B genotype
*Randomization to this arm stopped early due to US FDA concerns regarding lack of RBV.
12-wk follow-up
for SVR12
Wk 28 Wk 40
Weight-based RBV dosing (1000-1200 mg/day).

SOUND-C2: Higher SVR12 in Pts With GT 1b HCV, IL28B CC, BID Dosing
Zeuzem S, et al. EASL 2012. Abstract 101.
SVR1
2 (%
)
SVR1
2 (%
)
0
40
60
80
100
20n/N =
32
7584 82
1anon-CC
1aCC
1bnon-CC
1bCC
BID28wkRBV
TID28wk
TID40wkRBV
TID28wkRBV
TID16wkRBV
32
71
38
71
42
62
32
82
53
0
1a non-CC All 1b and 1a-CC
SVR according to IL28B and HCV subtype:BID28wk + RBV (ITT)
SVR according to IL28B and HCV subtype(ITT)
0
40
60
80
100
20
7/22 6/8 31/37 9/11
HCV Subtype and IL28B Genotype

4-Drug Therapy With GS-5885, GS-9451, Tegobuvir, and RBV in Tx-Naive GT1 HCV
• Interim analysis of randomized phase II study
Sulkowski M, et al. EASL 2012. Abstract 1421.
Tx-naive patients with chronic GT1
HCV infection(N = 140)
GS-5885 30 mg QD +GS-9451 200 mg QD + Tegobuvir 30 mg BID +
Ribavirin (n = 46)
Randomized 1:2; stratified by HCV RNA
(≤ vs > 800,000 IU/mL) and HCV 1 subtype (1a vs 1b)
*Patients with HCV RNA ≥ 25 IU/mL at Wk 2 offered rescue therapy including pegIFN or study discontinuation.†Patients rerandomized if HCV RNA < 25 IU/mL at Wks 2-10.
GS-5885 90 mg QD +GS-9451 200 mg QD + Tegobuvir 30 mg BID +
Ribavirin (n = 94)
Wk 2* Wk 12 Wk 24
GS-5885 90 mg QD +GS-9451 200 mg QD + Tegobuvir 30 mg BID +
Ribavirin
Follow-up
Rerandomized†
Follow-upfor SVR24

SVR-4 rates among patients with HCV RNA < 25 IU/mL at week 2

Effect of IL28B genotype, subtype and NS5A dose on week 2 response and breakthrough

Viral breakthrough was associated with resistance to PI, NS5A and NNI

Daclatasvir (NS5A) + Asunaprevir (PI)
Suzuki F, et al. EASL 2012. Abstract 14
100
80
60
40
20
0
91
SVR2
4 (%
)
9/10
n=21Weeks
0 24
Gen1b, non-cirrhotic
Daclatasvir + Asunaprevir
Daclatasvir + Asunaprevir
n=22
64Nullresponder
IFNintolerant
Nullresponder
IFN ineligible and intolerant
Among pts with breakthrough (7%) or relapse (9%), low plasma concentrations of DAC and ASU

NUCLEOS(T)IDE ANALOGUE POLYMERASE INHIBITOR +/- PI +/- NS5A INHIBITOR +/- RBV

INFORM-SVR: Mericitabine + danoprevir/ritonavir ± RBVin treatment-naïve GT-1: Study design
• Randomised Phase 2b study of response-guided mericitabine + ritonavir-boosted danoprevir ± RBV in treatment-naive GT-1 HCV patients– n=169: 67% HCV GT-1a; 69% IL28B non-CC
Week 24Week 12
Mericitabine 1000 mg BD + danoprevir/ritonavir
100/100 mg BD + RBV 1000/1200 mg QD
Mericitabine + danoprevir/ritonavir + RBV
Mericitabine + danoprevir/ritonavir + RBV
A
B
apatients with eRVR were re-randomised at Week 12 to maintain or stop treatmentbDue to unacceptable relapse rates, re-randomisation was halted and patients in Arm B on active treatment were offered PegIFN/RBV BID, twice daily; eRVR, early rapid virological response; GT, genotype; PegIFN, pegylated interferon; RBV, ribavirin
No treatment
No eRVR
Mericitabine 1000 mg BD + danoprevir/ritonavir
100/100 mg BD + placebo
Mericitabine + danoprevir/ritonavir + placebob
Mericitabine + danoprevir/ritonavir + placebob
No treatmenta
No eRVR
Week 4
EASL, Barcelona, Spain, 18–22 April 2012; Abstract 1412
eRVRa
eRVRa

INFORM-SVR: Mericitabine + danoprevir/ritonavir ± RBVin treatment-naïve GT-1 (Abstract 1412): Results
Mericitabine + danoprevir/ritonavir
+ RBV
Mericitabine + danoprevir/ritonavir
+ placebo
HCV RNA ≤15 IU/mL at Week 4 (%) 91 93
Mericitabine 1000 mg + danoprevir/ritonavir + RBV scheduled for 24 weeks
(n=63)
SVR8: Overall, % (n) 41 (26/63)
GT-1a 26 (11/42)
GT-1b 71 (15/21)
AEs, adverse events; SVR8: sustained virological response at Week 8 EASL, Barcelona, Spain, 18–22 April 2012; Abstract 1412
• Four serious AEs and two discontinuations due to AEs in overall population

G S - 7 9 7 7 + R B V
GS-7977 + RBV
G S - 7 9 7 7 + P E G + R B V
GS-7977 + PEG + RBVG S - 7 9 7 7 + R B V
GS-7977 + RBVG S - 7 9 7 7 + P E G + R B V
GS-7977 + PEG + RBVG S - 7 9 7 7 + P E G + R B V
GS-7977 + PEG + RBV
n= 9
n= 10
n= 10
G S - 7 9 7 7
GS-7977
G T 2 / 3 T r e a t m e n t- N a ïv e ( G S - 7 9 7 7 + R B V + P E G )
GT 2/3 Treatment-Naïve (GS-7977 + RBV +PEG) G S - 7 9 7 7 + R B V ( G T 1 N u l l R e s p o n d e r s )
GS-7977 + RBV (GT 1 Null Responders) G S - 7 9 7 7 + R B V ( G T 1 T r e a t m e n t- N a iv e )
GS-7977 + RBV (GT 1 Treatment-Naive) G S - 7 9 7 7 + R B V ( G T 2 / 3 T r e a t m e n t- E x p e r ie n c e d )
GS-7977 + RBV (GT 2/3 Treatment-Experienced)
n= 11
n= 10
n= 10
n= 10
n= 25
n= 25
Wk 4 Wk 8 Wk1 2Wk 0
GT 2/3 Tx-naive
Gane E, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1113.
Electron Study: Treatment of GS-7977
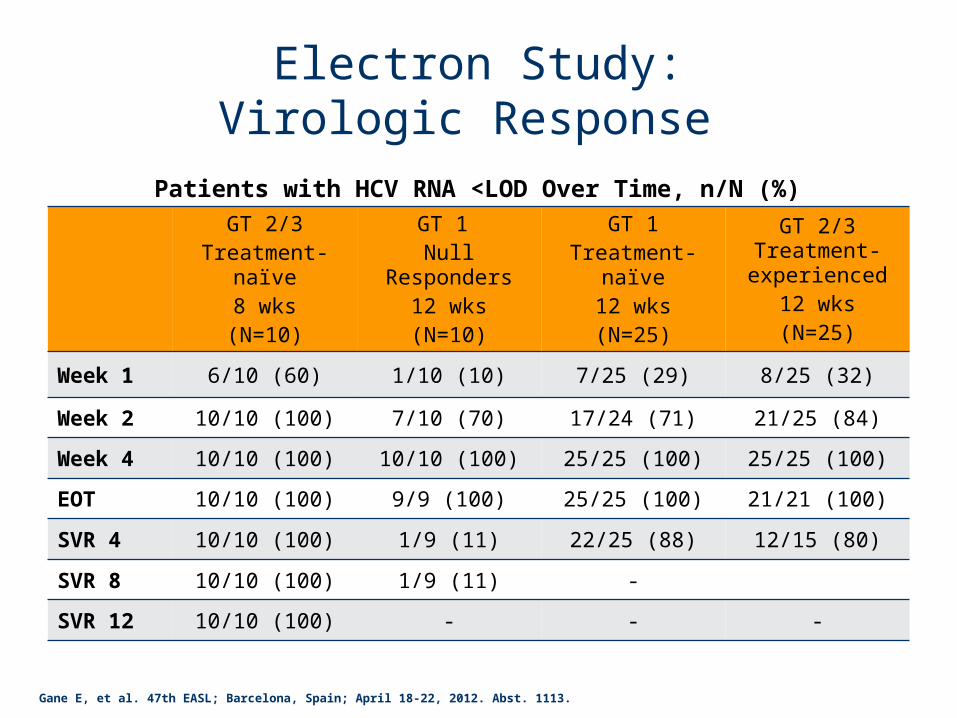
Electron Study:Virologic Response
GT 2/3Treatment-naïve
8 wks(N=10)
GT 1 Null Responders
12 wks(N=10)
GT 1Treatment-naïve
12 wks(N=25)
GT 2/3 Treatment- experienced
12 wks(N=25)
Week 1 6/10 (60) 1/10 (10) 7/25 (29) 8/25 (32)
Week 2 10/10 (100) 7/10 (70) 17/24 (71) 21/25 (84)
Week 4 10/10 (100) 10/10 (100) 25/25 (100) 25/25 (100)
EOT 10/10 (100) 9/9 (100) 25/25 (100) 21/21 (100)
SVR 4 10/10 (100) 1/9 (11) 22/25 (88) 12/15 (80)
SVR 8 10/10 (100) 1/9 (11) -
SVR 12 10/10 (100) - - -
Patients with HCV RNA <LOD Over Time, n/N (%)
Gane E, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1113.

Study AI444-040: Treatment with GS-7977 + BMS-790052
RBV: 1000-1200 mg daily according to body weight for GT1 patients ; 800 mg daily for GT2/3 patients
N = 15
N = 16
N = 14Chronic HCV GT1a/1b or GT2/3
infection, treatment-naive
SVR12Week 24 SVR4 SVR48Week 1 Week 4 Week 12
Group C: (GT1a/1b) DCV 60 mg QD + GS-7977 400 mg QD
Group D: (GT2/3) DCV 60 mg QD + GS-7977 400 mg QD Follow-up
Group E: (GT1a/1b) DCV 60 mg QD + GS-7977 400 mg QD + RBV Follow-up
N = 14
Group F: (GT2/3) DCV 60 mg QD +GS-7977 400 mg QD + RBV Follow-up
N = 15
N = 14
Group A: (GT1a/1b) GS-7977 400 mg QD x 7d, then add DCV 60 mg QD Follow-up
Group B: (GT2/3) GS-7977 400 mg QD x 7d, then add DCV 60 mg QD Follow-up
Follow-up
Sulkowski M, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1422.

Study AI444-040: Key Results
mITT analysis, bars not reaching 100% after Week 4 reflect missing values.PT, post treatment
Sulkowski M, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1422.
Week 2 Week 4 Week 12 Week 24(EOT) PT Week 4
N=
% < LOD
% < LLOQ67 79 67 100 100 100 100 93 100 87 86 93 100 100 100SVR4

Study AI444-040: SVR-4 according to genotype 1A/B and IL28B
• Overall SVR4 – 95.5% across GT 1,2 & 3• GT1: 100% of patients (44/44) achieved SVR4 • No difference in SVR4 by HCV GT1 subtype or IL28B genotype• Ribavirin did not increase the magnitude of HCV RNA decline or influence SVR
Sulkowski M, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1422.
IL28B Genotype(rs12979860)

Study AI444-040: GT2/3 Naïve
Sulkowski M, et al. 47th EASL; Barcelona, Spain; April 18-22, 2012. Abst. 1422.
N=44
GT2/3SVR4=40/44
GT2Total n=26
SVR4=24/26
GT3Total n=18
SVR4=16/18
GT2/3 – No RBVSVR4=28/30
2 viral failures
GT2/3 + RBVSVR4=12/14
2 LTFU
1 breakthrough (3a)1 relapse (3a)
2 LTFU (2a, last RNA UND)
2012 - 201X: Multiple DAA Combinations in Developmen
• Clinical trials to determine “best” combinations and minimum duration needed to achieve cure – Multiple regimens may lead to reduced cost per
cure• Role of Interferon alfa (lambda?) will evolve
but not become extinct

TYPICAL DAY IN THE CLINIC, JUNE 201X

Patient 1• 47 year old woman presents after being declined for
life insurance – Infection likely due to blood shortly after birth – PMH: None– Social history: Married with 3 children; Recent change to
new job with more responsibility– HCV genotype 1B; IL28B CC; Biopsy shows no fibrosis
• Treatment: – Oral therapy --- combination of 2 DAAs with no IFN and no
RBV for 12 weeks ($$)– PegIFN/RBV ($)

Patient 2• 66 year old man infected at age 20 via IDU
– PMH: type 2 DM, hypertension, obesity, mild renal insufficiency; anemia; heroin use off/on (methadone); depression (incompletely controlled)
– HCV genotype 1A; IL28B TT; Biopsy shows cirrhosis • Treatment:
– Multiple DAAs with nucleos(t)ide analogue ($$$) – No IFN due to contraindications

Patient 3• 59 year old man otherwise healthy
– HCV genotype 1A; IL28B TT; Biopsy shows Ishak 3/6 fibrosis
• Prior therapy – 1997: IFN alfa/RBV – stop at wk 24 with HCV RNA 5,500
copies/mL– 2011: PegIFN/RBV/Telaprevir – stop at wk 5
• Week 0: 11,389,000 IU/mL (7.06 log10)• Week 2: 17,710 IU/mL (4.25 log10)• Week 4: 153, 060 IU/mL (5.18 log10)
• Treat: Multiple DAAs +/- IFN +/- RBV ($$$$)

Patient 4• 59 year old man with decompensated liver
disease – MELD = 25 – Ascites – HCC less than 2 CM on MRI
• Treatment:– :Multiple DAAs – pre or post-transplant ($$$$)– 5 year survival for HCV expected to be similar to
similar to HBV

Patient 5• 22 year old man tested positive for HCV EIA using
finger stick test while attending needle exchange – Actively injecting heroin (~30 USD/day) uses new
needles when he can– Staying with “friends”– HIV seronegative
• Lost to follow-up • Treatment:
– Contingent Incentive Care x oral DAAs for 12 weeks ($$)– Cost-effective with individual and public health benefit?

Future Treatment Paradigms
• Personalized medicine– Cost– Virus – 1A or 1B or other genotype; Resistance to
DAAs– Patient – cirrhosis, ESLD, HCC, willing and able to
take IFN alfa; substance abuse? • Effectiveness may be limited by failure to
translate to the infected populations

















![Elizabeth Sherman, PharmD, AAHIVPhivaidsinstitute.med.miami.edu/documents/...HIV-HCV...• SVR rates similar to HCV monoinfected [1,2] • In HCV/HIV coinfection, treat HCV as though](https://img.pdfslide.net/doc/110x75/5fbc30e57653e03e261e9924/elizabeth-sherman-pharmd-aa-a-svr-rates-similar-to-hcv-monoinfected-12.jpg)