Embed Size (px)
Citation preview

NATIONAL MULTIPLE SCLEROSIS SOCIETY, MID-AMERICA CHAPTER FORM 990 TAX YEAR 2011
PUBLIC DISCLOSURE COPY
1X8510 1.000
BKD, LLP1201 Walnut, Suite 1700Kansas City, MO 64106-2246
Mr. George HansNational MS Society, Mid-America Chapter7611 State Line RoadKansas City, MO 64114

. .1201 Walnut, Suite 1700 Kansas City, MO 64106-2246 816.221.6300
XL03313.000
PRIVATEMr. George HansNational MS Society, Mid-America Chapter7611 State Line RoadKansas City, MO 64114
Enclosed are the original and one copy of your income tax returns for the period ended September30, 2012 for:
NATIONAL MULTIPLE SCLEROSIS SOCIETY, MID-AMERICA CHAPTER as follows...
2011 990 - Return of Organization Exempt from Income Tax 2011 8879-EO - IRS e-file Signature Authorization
Each original should be dated, signed and filed in accordance with the filing instructions. Thecopy should be retained for your files.
Upon an audit of the return(s), requests may be made for supporting documentation. Therefore, werecommend that you retain all pertinent records.
An additional copy of the Form 990 has been included, to be made available for publicinspection upon request. Please note that all statements of donors' contributions are notsubject to public inspection and have been removed, as appropriate.
Form 990 must be made available for public inspection for a period of three years, beginningwith the date the return is filed. The available document must be an exact copy of the returnand schedules (including schedule B), as filed with the IRS, except that the names and theaddresses of the contributors may be excluded. Any organization that fails to comply with thisprovision is subject to a penalty of $20 for each day that inspection is not permitted, up to amaximum of $10,000. Any organization that willfully fails to comply shall be subject to anadditional penalty of $5,000. You are also required to provide copies of the return if youreceive such a request. Should you receive a request for inspection or for copies of your return,you may want to contact us for further details.
These returns were prepared from information provided by you or your representative. Thepreparation of tax returns does not include the independent verification of information used. Therefore, we recommend you review the returns before signing to ensure there are no omissions ormisstatements. If you note anything which may require a change to the returns, please contact usbefore filing them.
Before preparing your tax return, we provided you with access to a summary of transactionsidentified by the U.S. Treasury as reportable transactions. The law provides for a penalty ashigh as $200,000 per transaction for failure to adequately disclose any of them on your taxreturn if applicable. Unless you notified us otherwise, your tax return was prepared with the

Mr. George Hans
assumption you have not engaged in any reportable transaction. Otherwise, we have prepared yourtax return in accordance with the information you provided to us and have attached theappropriate disclosure statement to your tax return. We are not liable for any penaltiesresulting from your failure to provide us with accurate and timely information about suchtransactions or to timely file the required disclosure statements. If you have any questionsabout reportable transactions, please contact us before filing your return.
We sincerely appreciate this opportunity to serve you. Please contact us if you have questionsconcerning the returns or if we may be of further assistance.
Sincerely,
Jakeb D. Blake

. .1201 Walnut, Suite 1700 Kansas City, MO 64106-2246 816.221.6300
XL03313.000
Instructions for filing NATIONAL MULTIPLE SCLEROSIS SOCIETY, MID-AMERICA CHAPTER Form 8879-EO - IRS E-file Signature Authorization for the period ended September 30, 2012
*************************
Signature... The original IRS e-file Signature Authorization form should be signed (use full name) and dated by the taxpayer.
Filing... Return your signed Form 8879-EO to:
BKD, LLP 1201 Walnut, Suite 1700 Kansas City MO 64106-2246
Or fax your signed Form 8879-EO to:
BKD, LLP eFile Administration 816-221-6380
Payment of tax... No payment of tax is required.
Form 8879-EO serves as a replacement for your signature that would beaffixed to form 990 if you paper filed your return.Please DO NOT separately file form 990 with the Internal RevenueService. Doing so will delay the processing of your return.
We must receive your signed form before we can electronicallytransmit your return which is due on February 15, 2013. Wewould appreciate your returning this form as soon as possibleas this will expedite the processing of your return. The InternalRevenue Service will notify us when your return is accepted.Your return is not considered filed until the Internal RevenueService confirms their acceptance, which may occur after the duedate of your return.

IRS e-file Signature Authorizationfor an Exempt Organization OMB No. 1545-1878Form 8879-EO
For calendar year 2011, or fiscal year beginning , 2011, and ending , 20 Do not send to the IRS. Keep for your records.See instructions on back.
Department of the TreasuryInternal Revenue Service Name of exempt organization
Name and title of officer
Employer identification number
Type of Return and Return Information (Whole Dollars Only)Part ICheck the box for the return for which you are using this Form 8879-E0 and enter the applicable amount, if any, from the return. If youcheck the box on line 1a, 2a, 3a, 4a, or 5a, below, and the amount on that line for the return being filed with this form was blank, thenleave line 1b, 2b, 3b, 4b, or 5b, whichever is applicable, blank (do not enter -0-). But, if you entered -0- on the return, then enter -0-on the applicable line below. Do not complete more than 1 line in Part I.1a2a3a4a5a
Form 990 check hereForm 990-EZ check hereForm 1120-POL check hereForm 990-PF check hereForm 8868 check here
b Total revenue, if any (Form 990, Part VIII, column (A), line 12) 1b2b3b4b5b
b Total revenue, if any (Form 990-EZ, line 9) b Total tax (Form 1120-POL, line 22) b Tax based on investment income (Form 990-PF, Part VI, line 5) b Balance Due (Form 8868, Part I, line 3c or Part II, line 8c) Declaration and Signature Authorization of OfficerPart II
Under penalties of perjury, I declare that I am an officer of the above organization and that I have examined a copy of theorganization's 2011 electronic return and accompanying schedules and statements and to the best of my knowledge and belief, theyare true, correct, and complete. I further declare that the amount in Part I above is the amount shown on the copy of theorganization's electronic return. I consent to allow my intermediate service provider, transmitter, or electronic return originator (ERO)to send the organization's return to the IRS and to receive from the IRS (a) an acknowledgement of receipt or reason for rejection ofthe transmission, (b) the reason for any delay in processing the return or refund, and (c) the date of any refund. If applicable, Iauthorize the U.S. Treasury and its designated Financial Agent to initiate an electronic funds withdrawal (direct debit) entry to thefinancial institution account indicated in the tax preparation software for payment of the organization's federal taxes owed on thisreturn, and the financial institution to debit the entry to this account. To revoke a payment, I must contact the U.S. Treasury FinancialAgent at 1-888-353-4537 no later than 2 business days prior to the payment (settlement) date. I also authorize the financial institutionsinvolved in the processing of the electronic payment of taxes to receive confidential information necessary to answer inquiries andresolve issues related to the payment. I have selected a personal identification number (PIN) as my signature for the organization'selectronic return and, if applicable, the organization's consent to electronic funds withdrawal.
Officer's PIN: check one box onlyto enter my PIN as my signatureI authorize
ERO firm name Enter five numbers, butdo not enter all zeros
on the organization's tax year 2011 electronically filed return. If I have indicated within this return that a copy of the return isbeing filed with a state agency(ies) regulating charities as part of the IRS Fed/State program, I also authorize the aforementionedERO to enter my PIN on the return's disclosure consent screen.
As an officer of the organization, I will enter my PIN as my signature on the organization's tax year 2011 electronically filed return.If I have indicated within this return that a copy of the return is being filed with a state agency(ies) regulating charities as part ofthe IRS Fed/State program, I will enter my PIN on the return's disclosure consent screen.
Officer's signature Date
Certification and AuthenticationPart IIIERO's EFIN/PIN. Enter your six-digit electronic filing identificationnumber (EFIN) followed by your five-digit self-selected PIN.
do not enter all zeros
I certify that the above numeric entry is my PIN, which is my signature on the 2011 electronically filed return for the organizationindicated above. I confirm that I am submitting this return in accordance with the requirements of Pub. 4163, Modernized e-File (MeF)Information for Authorized IRS e-file Providers for Business Returns. ERO's signature Date
ERO Must Retain This Form - See InstructionsDo Not Submit This Form To the IRS Unless Requested To Do So
For Paperwork Reduction Act Notice, see back of form. Form 8879-EO (2011)
JSA
1E1676 1.000
10/01 09/30 12
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
KAY JULIAN, CHAPTER PRESIDENT
X 3,992,831.
8 8 2 3 2X BKD, LLP
02/15/2013
4 3 0 3 2 5 4 4 0 1 6
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 2
OMB No. 1545-0047
Return of Organization Exempt From Income TaxForm Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except black lung
benefit trust or private foundation)
Open to PublicDepartment of the TreasuryInternal Revenue Service The organization may have to use a copy of this return to satisfy state reporting requirements. Inspection
, 2011, and ending , 20A For the 2011 calendar year, or tax year beginningD Employer identification numberC Name of organization
B Check if applicable:
Addresschange Doing Business As
E Telephone numberNumber and street (or P.O. box if mail is not delivered to street address) Room/suiteName change
Initial return
Terminated City or town, state or country, and ZIP + 4Amendedreturn
G Gross receipts $Applicationpending
H(a) Is this a group return foraffiliates?
F Name and address of principal officer: Yes No
Are all affiliates included? Yes NoH(b)If "No," attach a list. (see instructions)Tax-exempt status:I 501(c) ( ) (insert no.) 4947(a)(1) or 527501(c)(3) Website:J H(c) Group exemption numberK Form of organization: Corporation Trust Association Other L Year of formation: M State of legal domicile:
SummaryPart I1 Briefly describe the organization's mission or most significant activities:
234567
Check this boxNumber of voting members of the governing body (Part VI, line 1a)Number of independent voting members of the governing body (Part VI, line 1b)Total number of individuals employed in calendar year 2011 (Part V, line 2a)Total number of volunteers (estimate if necessary)Total gross unrelated business revenue from Part VIII, column (C), line 12Net unrelated business taxable income from Form 990-T, line 34
if the organization discontinued its operations or disposed of more than 25% of its net assets. 3 4 5 6Act
iviti
es&
Gov
erna
nce
a 7a b 7bPrior Year Current Year COPY FOR
PUBLIC INSPECTION
89
10111213141516
171819
202122
Contributions and grants (Part VIII, line 1h)Program service revenue (Part VIII, line 2g)Investment income (Part VIII, column (A), lines 3, 4, and 7d)Other revenue (Part VIII, column (A), lines 5, 6d, 8c, 9c, 10c, and 11e)Total revenue - add lines 8 through 11 (must equal Part VIII, column (A), line 12)Grants and similar amounts paid (Part IX, column (A), lines 1-3)Benefits paid to or for members (Part IX, column (A), line 4)Salaries, other compensation, employee benefits (Part IX, column (A), lines 5-10)Professional fundraising fees (Part IX, column (A), line 11e)Total fundraising expenses (Part IX, column (D), line 25)Other expenses (Part IX, column (A), lines 11a-11d, 11f-24f)Total expenses. Add lines 13-17 (must equal Part IX, column (A), line 25)Revenue less expenses. Subtract line 18 from line 12
Total assets (Part X, line 16)Total liabilities (Part X, line 26)Net assets or fund balances. Subtract line 21 from line 20
Rev
enue
ab
Exp
ense
s
Beginning of Current Year End of Year N
etA
sset
sor
Fund
Bal
ance
s
Signature BlockPart II
SignHere
Under penalties of perjury, I declare that I have examined this return, including accompanying schedules and statements, and to the best of my knowledge and belief, it is true,correct, and complete. Declaration of preparer (other than officer) is based on all information of which preparer has any knowledge.
Signature of officer Date Type or print name and title
Date Check ifself-employed
PTINPrint/Type preparer's name Preparer's signature
PaidPreparerUse Only EIN
Phone no.Firm's name
Firm's address May the IRS discuss this return with the preparer shown above? (see instructions) Yes NoFor Paperwork Reduction Act Notice, see the separate instructions. Form 990 (2010)JSA1E1065 1.000
10/01 09/30 12NATIONAL MULTIPLE SCLEROSIS SOCIETY,
MID-AMERICA CHAPTER44-0613436
7611 STATE LINE ROAD STE 100 (913) 432-3926
KANSAS CITY, MO 64114 4,577,288.KAY JULIAN X
7611 STATE LINE RD, SUITE 100 KANSAS CITY, MO 64114X
WWW.MSMIDAMERICA.ORG 1048X 1955 KS
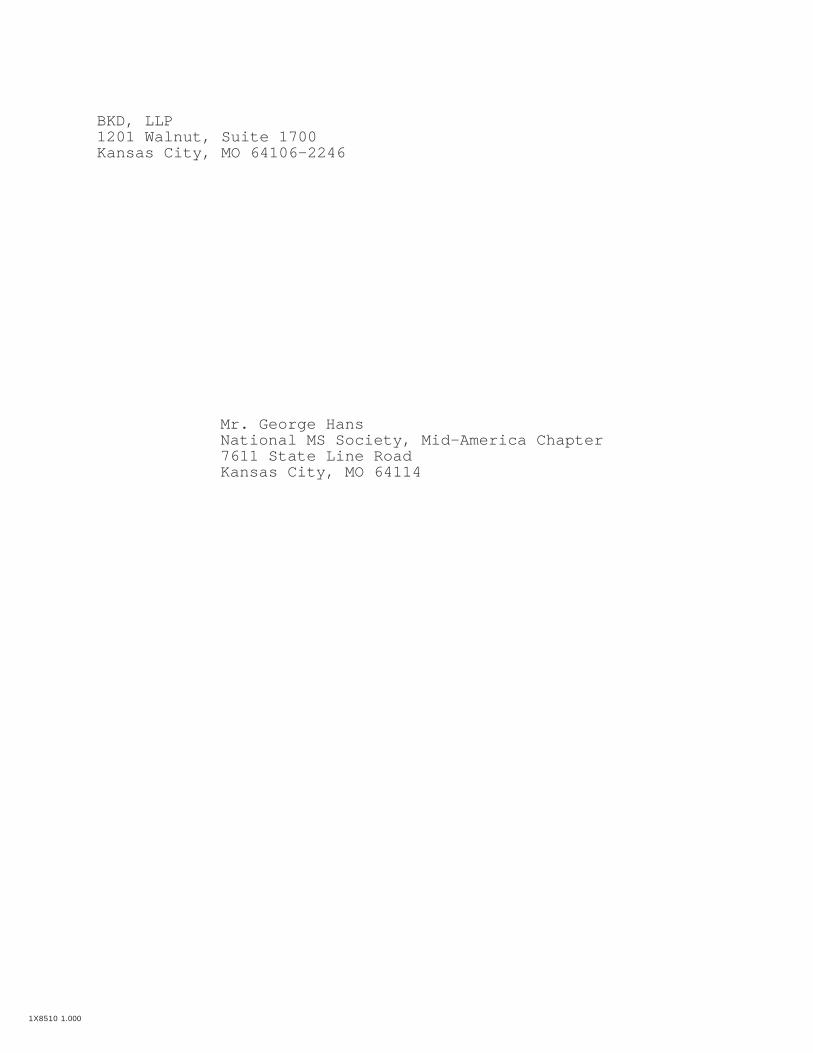
WE MOBILIZE PEOPLE AND RESOURCES TO DRIVE RESEARCH FOR A CURE AND TOADDRESS THE CHALLENGES OF EVERYONE AFFECTED BY MS.
12.11.37.
2,204.00
3,316,977. 4,171,690.3,035. 5,910.1,683. 461.
-521,497. -185,230.2,800,198. 3,992,831.
80,562. 117,609.0 0
1,198,715. 1,570,691.0 0
482,219.1,367,646. 2,189,460.2,646,923. 3,877,760.
153,275. 115,071.
2,196,679. 2,663,821.1,241,898. 1,485,863.
954,781. 1,177,958.
P01396137BKD, LLP 44-01602601201 WALNUT, SUITE 1700 KANSAS CITY, MO 64106-2246 816 221-6300
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 3

Form 990 (2011) Page 2Statement of Program Service AccomplishmentsPart IIICheck if Schedule O contains a response to any question in this Part III
1 Briefly describe the organization's mission:
2 Did the organization undertake any significant program services during the year which were not listed on theprior Form 990 or 990-EZ? Yes No If "Yes," describe these new services on Schedule O.
3 Did the organization cease conducting, or make significant changes in how it conducts, any programservices? Yes No If "Yes," describe these changes on Schedule O.
4 Describe the organization's program service accomplishments for each of its three largest program services, as measured byexpenses. Section 501(c)(3) and 501(c)(4) organizations and section 4947(a)(1) trusts are required to report the amount ofgrants and allocations to others, the total expenses, and revenue, if any, for each program service reported.
4a (Code: ) (Expenses $ including grants of $ ) (Revenue $ )
4b (Code: ) (Expenses $ including grants of $ ) (Revenue $ )
4c (Code: ) (Expenses $ including grants of $ ) (Revenue $ )
4d Other program services (Describe in Schedule O.)(Expenses $ including grants of $ ) (Revenue $ )4e Total program service expenses
JSA Form 990 (2011)1E1020 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
X
WE MOBILIZE PEOPLE AND RESOURCES TO DRIVE RESEARCH FOR A CURE AND TOADDRESS THE CHALLENGES OF EVERYONE AFFECTED BY MS.
X
X
854,883. 0 0
RESEARCH - REPRESENTS COSTS INCURRED TO SUPPORT SCIENTIFIC STUDIESOR INVESTIGATIONS PLUS ALL OTHER COSTS OR EXPENSES INCURRED WHILECONDUCTING A PROGRAM IN WHICH NEW KNOWLEDGE IS BEING SOUGHT TOFIND CAUSES OF THE DISEASE, TREATMENT, AND PREVENTION OF MULTIPLESCLEROSIS.
713,243. 117,609. 5,910.
CLIENT PROGRAMS - ARE THOSE PROGRAMS AND SERVICES PROVIDEDDIRECTLY TO INDIVIDUALS WHO ARE LIVING WITH MULTIPLE SCLEROSIS.THE PURPOSE OF THESE SERVICES IS TO PROVIDE PHYSICAL, EMOTIONAL,OR ASSISTIVE DEVICE SUPPORT. IT ALSO INCLUDES FURNISHING OFEQUIPMENT AND OTHER TANGIBLE ITEMS TO THOSE IN NEED PLUS ALL OTHERCOSTS OR EXPENSES INCURRED AS A RESULT OF LIVING WITH MULTIPLESCLEROSIS.
614,442. 0 0
OTHER NATIONAL PROGRAMS INCLUDES THE COSTS ASSOCIATED WITH FUNDINGCLIENT AND COMMUNITY SERVICE, PUBLIC EDUCATION, AND PROFESSIONALEDUCATION CONDUCTED BY THE NATIONAL ORGANIZATION FOR THE BENEFITOF INDIVIDUALS LIVING WITH MULTIPLE SCLEROSIS.
1,050,216. 0 0
3,232,784.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 4

Form 990 (2011) Page 3Checklist of Required SchedulesPart IV
Yes No
1
23
4
5
6
7
8
9
10
11
12
1314
15
16
17
18
19
20
Is the organization described in section 501(c)(3) or 4947(a)(1) (other than a private foundation)? If "Yes,"complete Schedule A 1
2
3
4
5
6
7
8
9
10
11a
11b
11c
11d11e
11f
12a
12b13
14a
14b
15
16
17
18
1920a20b
Is the organization required to complete Schedule B, Schedule of Contributors (see instructions)? Did the organization engage in direct or indirect political campaign activities on behalf of or in opposition tocandidates for public office? If "Yes," complete Schedule C, Part I Section 501(c)(3) organizations. Did the organization engage in lobbying activities, or have a section 501(h)election in effect during the tax year? If "Yes," complete Schedule C, Part II Is the organization a section 501(c)(4), 501(c)(5), or 501(c)(6) organization that receives membership dues,assessments, or similar amounts as defined in Revenue Procedure 98-19? If "Yes," complete Schedule C,Part III Did the organization maintain any donor advised funds or any similar funds or accounts for which donorshave the right to provide advice on the distribution or investment of amounts in such funds or accounts? If"Yes," complete Schedule D, Part I Did the organization receive or hold a conservation easement, including easements to preserve open space,the environment, historic land areas, or historic structures? If "Yes," complete Schedule D, Part II Did the organization maintain collections of works of art, historical treasures, or other similar assets? If "Yes,"complete Schedule D, Part III Did the organization report an amount in Part X, line 21; serve as a custodian for amounts not listed in PartX; or provide credit counseling, debt management, credit repair, or debt negotiation services? If "Yes,"complete Schedule D, Part IV Did the organization, directly or through a related organization, hold assets in temporarily restrictedendowments, permanent endowments, or quasi-endowments? If "Yes," complete Schedule D, Part V If the organization’s answer to any of the following questions is "Yes," then complete Schedule D, Parts VI,VII, VIII, IX, or X as applicable.
a
b
c
d
ef
a
Did the organization report an amount for land, buildings, and equipment in Part X, line 10? If "Yes," completeSchedule D, Part VI Did the organization report an amount for investments—other securities in Part X, line 12 that is 5% or moreof its total assets reported in Part X, line 16? If "Yes," complete Schedule D, Part VII Did the organization report an amount for investments-program related in Part X, line 13 that is 5% or moreof its total assets reported in Part X, line 16? If "Yes," complete Schedule D, Part VIII Did the organization report an amount for other assets in Part X, line 15 that is 5% or more of its total assetsreported in Part X, line 16? If "Yes," complete Schedule D, Part IX Did the organization report an amount for other liabilities in Part X, line 25? If "Yes," complete Schedule D, Part XDid the organization’s separate or consolidated financial statements for the tax year include a footnote that addressesthe organization's liability for uncertain tax positions under FIN 48 (ASC 740)? If "Yes," complete Schedule D, Part X Did the organization obtain separate, independent audited financial statements for the tax year? If "Yes,"complete Schedule D, Parts XI, XII, and XIII
b
ab
ab
Was the organization included in consolidated, independent audited financial statements for the tax year? If "Yes," and ifthe organization answered "No" to line 12a, then completing Schedule D, Parts XI, XII, and XIII is optional Is the organization a school described in section 170(b)(1)(A)(ii)? If "Yes," complete Schedule E Did the organization maintain an office, employees, or agents outside of the United States? Did the organization have aggregate revenues or expenses of more than $10,000 from grantmaking,fundraising, business, investment, and program service activities outside the United States, or aggregateforeign investments valued at $100,000 or more? If "Yes," complete Schedule F, Parts I and IV Did the organization report on Part IX, column (A), line 3, more than $5,000 of grants or assistance to anyorganization or entity located outside the United States? If "Yes," complete Schedule F, Parts II and IV Did the organization report on Part IX, column (A), line 3, more than $5,000 of aggregate grants or assistanceto individuals located outside the United States? If "Yes," complete Schedule F, Parts III and IV Did the organization report a total of more than $15,000 of expenses for professional fundraising serviceson Part IX, column (A), lines 6 and 11e? If "Yes," complete Schedule G, Part I (see instructions) Did the organization report more than $15,000 total of fundraising event gross income and contributions onPart VIII, lines 1c and 8a? If "Yes," complete Schedule G, Part II Did the organization report more than $15,000 of gross income from gaming activities on Part VIII, line 9a?If "Yes," complete Schedule G, Part III Did the organization operate one or more hospital facilities? If "Yes," complete Schedule HIf "Yes" to line 20a, did the organization attach a copy of its audited financial statements to this return?
Form 990 (2011)JSA
1E1021 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
XX
X
X
X
X
X
X
X
X
X
X
X
XX
X
X
X X X
X
X
X
X
X
X X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 5

Form 990 (2011) Page 4Checklist of Required Schedules (continued)Part IV
Yes No
21
22
23
24
25
26
27
28
2930
31
32
33
34
35
36
37
38
Did the organization report more than $5,000 of grants and other assistance to any government or organizationin the United States on Part IX, column (A), line 1? If "Yes," complete Schedule I, Parts I and II 21
22
23
24a24b
24c24d
25a
25b
26
27
28a
28b
28c29
30
31
32
33
3435a
35b
36
37
38
Did the organization report more than $5,000 of grants and other assistance to individuals in the United Stateson Part IX, column (A), line 2? If "Yes," complete Schedule I, Parts I and III Did the organization answer "Yes" to Part VII, Section A, line 3, 4, or 5 about compensation of theorganization's current and former officers, directors, trustees, key employees, and highest compensatedemployees? If "Yes," complete Schedule J
a
bc
da
b
ab
c
Did the organization have a tax-exempt bond issue with an outstanding principal amount of more than$100,000 as of the last day of the year, that was issued after December 31, 2002? If "Yes," answer lines 24bthrough 24d and complete Schedule K. If “No,” go to line 25 Did the organization invest any proceeds of tax-exempt bonds beyond a temporary period exception? Did the organization maintain an escrow account other than a refunding escrow at any time during the yearto defease any tax-exempt bonds? Did the organization act as an "on behalf of" issuer for bonds outstanding at any time during the year? Section 501(c)(3) and 501(c)(4) organizations. Did the organization engage in an excess benefit transactionwith a disqualified person during the year? If "Yes," complete Schedule L, Part I Is the organization aware that it engaged in an excess benefit transaction with a disqualified person in a prioryear, and that the transaction has not been reported on any of the organization's prior Forms 990 or 990-EZ?If "Yes," complete Schedule L, Part I Was a loan to or by a current or former officer, director, trustee, key employee, highly compensated employee, ordisqualified person outstanding as of the end of the organization's tax year? If "Yes," complete Schedule L, Part II Did the organization provide a grant or other assistance to an officer, director, trustee, key employee,substantial contributor or employee thereof, a grant selection committee member, or to a 35% controlledentity or family member of any of these persons? If "Yes," complete Schedule L, Part III Was the organization a party to a business transaction with one of the following parties (see Schedule L,Part IV instructions for applicable filing thresholds, conditions, and exceptions):A current or former officer, director, trustee, or key employee? If "Yes," complete Schedule L, Part IV A family member of a current or former officer, director, trustee, or key employee? If "Yes," completeSchedule L, Part IV An entity of which a current or former officer, director, trustee, or key employee (or a family member thereof)was an officer, director, trustee, or direct or indirect owner? If "Yes," complete Schedule L, Part IV Did the organization receive more than $25,000 in non-cash contributions? If "Yes," complete Schedule MDid the organization receive contributions of art, historical treasures, or other similar assets, or qualifiedconservation contributions? If "Yes," complete Schedule M Did the organization liquidate, terminate, or dissolve and cease operations? If "Yes," complete Schedule N,Part I Did the organization sell, exchange, dispose of, or transfer more than 25% of its net assets? If "Yes,"complete Schedule N, Part II Did the organization own 100% of an entity disregarded as separate from the organization under Regulationssections 301.7701-2 and 301.7701-3? If "Yes," complete Schedule R, Part I Was the organization related to any tax-exempt or taxable entity? If "Yes," complete Schedule R, Parts II, III,IV, and V, line 1
ab
Did the organization have a controlled entity within the meaning of section 512(b)(13)? Did the organization receive any payment from or engage in any transaction with a controlled entity within themeaning of section 512(b)(13)? If "Yes," complete Schedule R, Part V, line 2 Section 501(c)(3) organizations. Did the organization make any transfers to an exempt non-charitablerelated organization? If "Yes," complete Schedule R, Part V, line 2 Did the organization conduct more than 5% of its activities through an entity that is not a related organizationand that is treated as a partnership for federal income tax purposes? If "Yes," complete Schedule R,Part VI Did the organization complete Schedule O and provide explanations in Schedule O for Part VI, lines 11 and19? Note. All Form 990 filers are required to complete Schedule O.
Form 990 (2011)
JSA
1E1030 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
X
X
X
X
X
X
X
X
X
X
XX
X
X
X
X
X X
X
X
X
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 6

Form 990 (2011) Page 5Statements Regarding Other IRS Filings and Tax ComplianceCheck if Schedule O contains a response to any question in this Part V
Part V Yes No
1a1b
2a
7d
1
2
3
4
5
6
7
8
9
10
11
12
13
14
abc
a
b
aba
b
abca
b
a
bc
defgh
ab
ab
ab
ab
a
b
cab
Enter the number reported in Box 3 of Form 1096. Enter -0- if not applicable Enter the number of Forms W-2G included in line 1a. Enter -0- if not applicable Did the organization comply with backup withholding rules for reportable payments to vendors andreportable gaming (gambling) winnings to prize winners? 1c
2b
3a3b
4a
5a5b5c
6a
6b
7a7b
7c
7e7f7g7h
8
9a9b
12a
13a
14a14b
Enter the number of employees reported on Form W-3, Transmittal of Wage and TaxStatements, filed for the calendar year ending with or within the year covered by this return If at least one is reported on line 2a, did the organization file all required federal employment tax returns?Note. If the sum of lines 1a and 2a is greater than 250, you may be required to e-file (see instructions) Did the organization have unrelated business gross income of $1,000 or more during the year? If "Yes," has it filed a Form 990-T for this year? If "No," provide an explanation in Schedule O At any time during the calendar year, did the organization have an interest in, or a signature or other authorityover, a financial account in a foreign country (such as a bank account, securities account, or other financialaccount)? If “Yes,” enter the name of the foreign country:See instructions for filing requirements for Form TD F 90-22.1, Report of Foreign Bank and Financial Accounts.Was the organization a party to a prohibited tax shelter transaction at any time during the tax year? Did any taxable party notify the organization that it was or is a party to a prohibited tax shelter transaction?If "Yes" to line 5a or 5b, did the organization file Form 8886-T? Does the organization have annual gross receipts that are normally greater than $100,000, and did theorganization solicit any contributions that were not tax deductible? If "Yes," did the organization include with every solicitation an express statement that such contributions orgifts were not tax deductible? Organizations that may receive deductible contributions under section 170(c).Did the organization receive a payment in excess of $75 made partly as a contribution and partly for goodsand services provided to the payor? If "Yes," did the organization notify the donor of the value of the goods or services provided? Did the organization sell, exchange, or otherwise dispose of tangible personal property for which it wasrequired to file Form 8282? If "Yes," indicate the number of Forms 8282 filed during the year Did the organization receive any funds, directly or indirectly, to pay premiums on a personal benefit contract? Did the organization, during the year, pay premiums, directly or indirectly, on a personal benefit contract?If the organization received a contribution of qualified intellectual property, did the organization file Form 8899 as required? If the organization received a contribution of cars, boats, airplanes, or other vehicles, did the organization file a Form 1098-C?Sponsoring organizations maintaining donor advised funds and section 509(a)(3) supportingorganizations. Did the supporting organization, or a donor advised fund maintained by a sponsoringorganization, have excess business holdings at any time during the year? Sponsoring organizations maintaining donor advised funds.Did the organization make any taxable distributions under section 4966?Did the organization make a distribution to a donor, donor advisor, or related person?Section 501(c)(7) organizations. Enter:Initiation fees and capital contributions included on Part VIII, line 12Gross receipts, included on Form 990, Part VIII, line 12, for public use of club facilitiesSection 501(c)(12) organizations. Enter:Gross income from members or shareholders
10a10b
11a
11b
12b
13b13c
Gross income from other sources (Do not net amounts due or paid to other sourcesagainst amounts due or received from them.) Section 4947(a)(1) non-exempt charitable trusts. Is the organization filing Form 990 in lieu of Form 1041?If "Yes," enter the amount of tax-exempt interest received or accrued during the year Section 501(c)(29) qualified nonprofit health insurance issuers.Is the organization licensed to issue qualified health plans in more than one state? Note. See the instructions for additional information the organization must report on Schedule O.Enter the amount of reserves the organization is required to maintain by the states in whichthe organization is licensed to issue qualified health plans Enter the amount of reserves on hand Did the organization receive any payments for indoor tanning services during the tax year? If "Yes," has it filed a Form 720 to report these payments? If "No," provide an explanation in Schedule O
JSA Form 990 (2011)1E1040 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
10
X
37X
X
X
X X
X
XX
X
X X
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 7

Form 990 (2011) Page 6Governance, Management, and Disclosure For each "Yes" response to lines 2 through 7b below, and for a"No" response to line 8a, 8b, or 10b below, describe the circumstances, processes, or changes in ScheduleO. See instructions.
Part VI
Check if Schedule O contains a response to any question in this Part VISection A. Governing Body and Management
Yes No
1a
1b
1
2
3
4567
8
a
b
a
b
ab
Enter the number of voting members of the governing body at the end of the tax year. If there arematerial differences in voting rights among members of the governing body, or if the governing bodydelegated broad authority to an executive committee or similar committee, explain in Schedule O.Enter the number of voting members included in line 1a, above, who are independent
2
3456
7a
7b
8a8b
9
10a
10b11a
12a
12b
12c1314
15a15b
16a
16b
Did any officer, director, trustee, or key employee have a family relationship or a business relationship withany other officer, director, trustee, or key employee? Did the organization delegate control over management duties customarily performed by or under the directsupervision of officers, directors, or trustees, or key employees to a management company or other person? Did the organization make any significant changes to its governing documents since the prior Form 990 was filed?Did the organization become aware during the year of a significant diversion of the organization's assets?Did the organization have members or stockholders?
Did the organization have members, stockholders, or other persons who had the power to elect or appointone or more members of the governing body? Are any governance decisions of the organization reserved to (or subject to approval by) members,stockholders, or persons other than the governing body? Did the organization contemporaneously document the meetings held or written actions undertaken duringthe year by the following:The governing body?Each committee with authority to act on behalf of the governing body?
9 Is there any officer, director, trustee, or key employee listed in Part VII, Section A, who cannot be reached at
the organization's mailing address? If "Yes," provide the names and addresses in Schedule O Section B. Policies (This Section B requests information about policies not required by the Internal Revenue Code.)
Yes No
10
11
12
131415
16
ab
abab
c
ab
a
b
Did the organization have local chapters, branches, or affiliates? If "Yes," did the organization have written policies and procedures governing the activities of such chapters,affiliates, and branches to ensure their operations are consistent with the organization's exempt purposes? Has the organization provided a complete copy of this Form 990 to all members of its governing body before filing the form? Describe in Schedule O the process, if any, used by the organization to review this Form 990.Did the organization have a written conflict of interest policy? If "No," go to line 13 Were officers, directors, or trustees, and key employees required to disclose annually interests that could giverise to conflicts? Did the organization regularly and consistently monitor and enforce compliance with the policy? If "Yes,"describe in Schedule O how this was done Did the organization have a written whistleblower policy?Did the organization have a written document retention and destruction policy?Did the process for determining compensation of the following persons include a review and approval byindependent persons, comparability data, and contemporaneous substantiation of the deliberation and decision?The organization's CEO, Executive Director, or top management officialOther officers or key employees of the organizationIf "Yes" to line 15a or 15b, describe the process in Schedule O (see instructions.)
Did the organization invest in, contribute assets to, or participate in a joint venture or similar arrangementwith a taxable entity during the year? If "Yes," did the organization follow a written policy or procedure requiring the organization to evaluate itsparticipation in joint venture arrangements under applicable federal tax law, and take steps to safeguard theorganization's exempt status with respect to such arrangements?
Section C. Disclosure 1718
19
20
List the states with which a copy of this Form 990 is required to be filedSection 6104 requires an organization to make its Forms 1023 (or 1024 if applicable), 990, and 990-T (Section 501(c)(3)s only)available for public inspection. Indicate how you made these available. Check all that apply.
Own website Another's website Upon request
Describe in Schedule O whether (and if so, how), the organization made its governing documents, conflict of interest policy,and financial statements available to the public during the tax year.State the name, physical address, and telephone number of the person who possesses the books and records of theorganization:
JSA Form 990 (2011)1E1042 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
X
12
11
X
XX X X
X
X
XX
X
X
XX
X
X
XXX
XX
X
X X
KAY JULIAN 7611 STATE LINE ROAD, SUITE 100 KANSAS CITY, MO 64114 913-432-3926
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 8

Form 990 (2011) Page 7Compensation of Officers, Directors, Trustees, Key Employees, Highest Compensated Employees, andIndependent Contractors
Part VII
Check if Schedule O contains a response to any question in this Part VII Section A. Officers, Directors, Trustees, Key Employees, and Highest Compensated Employees1a Complete this table for all persons required to be listed. Report compensation for the calendar year ending with or within theorganization's tax year.
List all of the organization's current officers, directors, trustees (whether individuals or organizations), regardless of amountof compensation. Enter -0- in columns (D), (E), and (F) if no compensation was paid.
List all of the organization's current key employees, if any. See instructions for definition of "key employee."List the organization's five current highest compensated employees (other than an officer, director, trustee, or key employee)
who received reportable compensation (Box 5 of Form W-2 and/or Box 7 of Form 1099-MISC) of more than $100,000 from theorganization and any related organizations.
List all of the organization's former officers, key employees, and highest compensated employees who received more than$100,000 of reportable compensation from the organization and any related organizations.
List all of the organization's former directors or trustees that received, in the capacity as a former director or trustee of theorganization, more than $10,000 of reportable compensation from the organization and any related organizations.
List persons in the following order: individual trustees or directors; institutional trustees; officers; key employees; highestcompensated employees; and former such persons.
Check this box if neither the organization nor any related organization compensated any current officer, director, or trustee.
(A) (B) (C) (D) (E) (F)Name and Title Average
hours perweek
Position(do not check more than onebox, unless person is both anofficer and a director/trustee)
Reportablecompensation
fromthe
organization(W-2/1099-MISC)
Reportablecompensation from
relatedorganizations
(W-2/1099-MISC)
Estimatedamount of
othercompensation
from theorganizationand related
organizations
(describehours forrelated
organizationsin Schedule
O)
Individualtrusteeor
director
Institutionaltrustee
Officer
Keyem
ployee
Highestcom
pensatedem
ployee
Former
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(12)
(13)
(14)
Form 990 (2011)JSA
1E1041 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
BILL GAUTREAUXDIRECTOR/CHAIRPERSON 2.00 X X 0 0 0DAVID DICKEYDIRECTOR/VICE-CHAIRPERSON 2.00 X X 0 0 0ROBERT NAGELTREASURER, FINANCE COMM CHAIR 2.00 X X 0 0 0KIM SUCHASECRETARY, AUDIT COMM CHAIR 2.00 X X 0 0 0DAVID DORANDIRECTOR 2.00 X 0 0 0DON GEIERDIRECTOR 2.00 X 0 0 0TABBY OSBORNDIRECTOR 2.00 X 0 0 0JEFFREY PEIERDIRECTOR 2.00 X 0 0 0JOHN SNYDERDIRECTOR 2.00 X 0 0 0DAN WATKINSDIRECTOR 2.00 X 0 0 0ANNETTE WILESDIRECTOR 2.00 X 0 0 0KAY JULIANPRESIDENT 35.00 X X 131,692. 0 9,371.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 9

Form 990 (2011) Page 8Section A. Officers, Directors, Trustees, Key Employees, and Highest Compensated Employees (continued)Part VII
(A) (B) (C) (D) (E) (F)Estimatedamount of
othercompensation
from theorganizationand related
organizations
Name and title Averagehours per
week(describehours forrelated
organizationsin Schedule
O)
Position(do not check more than onebox, unless person is both anofficer and a director/trustee)
Reportablecompensation
fromthe
organization(W-2/1099-MISC)
Reportablecompensation from
relatedorganizations
(W-2/1099-MISC)
Individualtrusteeor
director
Institutionaltrustee
Officer
Keyem
ployee
Highestcom
pensatedem
ployee
Former
1b Sub-total c Total from continuation sheets to Part VII, Section A d Total (add lines 1b and 1c)2 Total number of individuals (including but not limited to those listed above) who received more than $100,000 of
reportable compensation from the organization Yes No
3 Did the organization list any former officer, director, or trustee, key employee, or highest compensatedemployee on line 1a? If "Yes," complete Schedule J for such individual 3
4 For any individual listed on line 1a, is the sum of reportable compensation and other compensation from theorganization and related organizations greater than $150,000? If “Yes,” complete Schedule J for suchindividual 4
5 Did any person listed on line 1a receive or accrue compensation from any unrelated organization or individualfor services rendered to the organization? If “Yes,” complete Schedule J for such person 5
Section B. Independent Contractors1 Complete this table for your five highest compensated independent contractors that received more than $100,000 of
compensation from the organization. Report compensation for the calendar year ending with or within the organization's taxyear.
(A)Name and business address
(B)Description of services
(C)Compensation
2 Total number of independent contractors (including but not limited to those listed above) who receivedmore than $100,000 in compensation from the organization
JSA Form 990 (2011)1E1055 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
131,692. 0 9,371.0 0 0
131,692. 0 9,371.
1
X
X
X
0
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 10

Form 990 (2011) Page 9Statement of Revenue
(C)Unrelatedbusinessrevenue
Part VIII(B)
Related orexemptfunctionrevenue
(D)Revenue
excluded from taxunder sections
512, 513, or 514
(A)Total revenue
1a1b1c1d1e
1f
1abcdef
g
2abcdef
6abc
b
c
8a
b
9a
b
10a
b
11abcde
Federated campaignsMembership duesFundraising eventsRelated organizationsGovernment grants (contributions)All other contributions, gifts, grants,
and similar amounts not included above
Noncash contributions included in lines 1a-1f:
$
Con
trib
utio
ns,G
ifts,
Gra
nts
and
Oth
erSi
mila
rAm
ount
s
h Total. Add lines 1a-1f Business Code
All other program service revenue g Total. Add lines 2a-2fPro
gram
Serv
ice
Rev
enue
3
45
Investment income (including dividends, interest, andother similar amounts)Income from investment of tax-exempt bond proceedsRoyalties
(i) Real (ii) Personal
Gross rentsLess: rental expensesRental income or (loss)
d Net rental income or (loss)
(i) Securities (ii) Other7a Gross amount from sales of
assets other than inventoryLess: cost or other basisand sales expensesGain or (loss)
d Net gain or (loss)
Gross income from fundraisingevents (not including $of contributions reported on line 1c).See Part IV, line 18Less: direct expenses
ab
ab
ab
c Net income or (loss) from fundraising events O
ther
Rev
enue
Gross income from gaming activities.See Part IV, line 19 Less: direct expenses
c Net income or (loss) from gaming activities Gross sales of inventory, lessreturns and allowances Less: cost of goods sold
c Net income or (loss) from sales of inventory Miscellaneous Revenue Business Code
All other revenueTotal. Add lines 11a-11d
12 Total revenue. See instructionsForm 990 (2011)
JSA1E1051 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
3,356,238.
815,452.
30,637.
4,171,690.
SERVICE PROGRAM FEES 900099 5,910. 5,910.
5,910.
461. 461.
0
0
0
0
3,356,238.
89,927.
584,457.
-494,530. -494,530.
0
0
MISCELLANEOUS INCOME 900099 309,300. 309,300.
309,300.
3,992,831. 5,910. -184,769.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 11

Form 990 (2011) Page 10Statement of Functional ExpensesPart IX
Section 501(c)(3) and 501(c)(4) organizations must complete all columns. All other organizations must complete column (A) but are notrequired to complete columns (B), (C), and (D).
Check if Schedule O contains a response to any question in this Part IX (A) (B) (C) (D)Do not include amounts reported on lines 6b,
7b, 8b, 9b, and 10b of Part VIII. Total expenses Program serviceexpenses
Management andgeneral expenses
Fundraisingexpenses
Grants and other assistance to governments andorganizations in the United States. See Part IV, line 2 1
1 Grants and other assistance to individuals inthe United States. See Part IV, line 22
2 3 Grants and other assistance to governments,
organizations, and individuals outside theUnited States. See Part IV, lines 15 and 16 Benefits paid to or for members4
5 Compensation of current officers, directors,trustees, and key employees
6 Compensation not included above, to disqualifiedpersons (as defined under section 4958(f)(1)) andpersons described in section 4958(c)(3)(B) Other salaries and wages7
8 Pension plan accruals and contributions (include section401(k) and 403(b) employer contributions)
9 Other employee benefitsPayroll taxesFees for services (non-employees):ManagementLegalAccountingLobbying
1011
12131415161718
192021222324
abcdefg
Professional fundraising services. See Part IV, line 1 7Investment management fees OtherAdvertising and promotionOffice expensesInformation technology
RoyaltiesOccupancyTravel
Payments of travel or entertainment expensesfor any federal, state, or local public officialsConferences, conventions, and meetingsInterestPayments to affiliatesDepreciation, depletion, and amortizationInsurance
Other expenses. Itemize expenses not coveredabove (List miscellaneous expenses in line 24e. Ifline 24e amount exceeds 10% of line 25, column(A) amount, list line 24e expenses on Schedule O.)
abcde All other expenses
25 Total functional expenses. Add lines 1 through 24e26 Joint costs. Complete this line only if the
organization reported in column (B) joint costsfrom a combined educational campaign andfundraising solicitation. Check here iffollowing SOP 98-2 (ASC 958-720)
JSA Form 990 (2011)1E1052 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
0
117,609. 117,609.
00
149,761. 104,833. 14,976. 29,952.
01,194,730. 819,898. 93,923. 280,909.
20,667. 14,800. 1,310. 4,557.99,240. 70,904. 6,943. 21,393.
106,293. 73,343. 8,503. 24,447.
000000
177,108. 152,389. 5,864. 18,855.0
139,069. 113,412. 6,069. 19,588.00
181,917. 124,982. 14,491. 42,444.83,525. 66,077. 2,564. 14,884.
037,425. 34,993. 524. 1,908.
01,469,325. 1,469,325.
18,995. 13,106. 1,520. 4,369.21,653. 14,941. 1,732. 4,980.
FURNITURE AND EQUIPMENT 34,419. 23,754. 2,752. 7,913.DUES AND MEMBERSHIPS 5,788. 4,038. 434. 1,316.PRIZES AND PROMOTIONAL ITEMS 3,970. 3,797. 14. 159._
16,266. 10,583. 1,138. 4,545.3,877,760. 3,232,784. 162,757. 482,219.
0
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 12

Form 990 (2011) Page 11Balance SheetPart X
(A)Beginning of year
(B)End of year
Cash - non-interest-bearingSavings and temporary cash investmentsPledges and grants receivable, netAccounts receivable, net
12345
1234
5
6789
10c1112131415161718192021
222324
2526
Receivables from current and former officers, directors, trustees, keyemployees, and highest compensated employees. Complete Part II ofSchedule L Receivables from other disqualified persons (as defined under section4958(f)(1)), persons described in section 4958(c)(3)(B), and contributingemployers and sponsoring organizations of section 501(c)(9) voluntaryemployees' beneficiary organizations (see instructions)
6
Notes and loans receivable, netInventories for sale or usePrepaid expenses and deferred charges
789
10a
10b
10
111213141516171819202122
232425
26
a Land, buildings, and equipment: cost orother basis. Complete Part VI of Schedule DLess: accumulated depreciationbInvestments - publicly traded securitiesInvestments - other securities. See Part IV, line 11Investments - program-related. See Part IV, line 11Intangible assetsOther assets. See Part IV, line 11Total assets. Add lines 1 through 15 (must equal line 34)
Ass
ets
Accounts payable and accrued expensesGrants payableDeferred revenueTax-exempt bond liabilities
Escrow or custodial account liability. Complete Part IV of Schedule DPayables to current and former officers, directors, trustees, keyemployees, highest compensated employees, and disqualified persons.Complete Part II of Schedule LLi
abili
ties
Secured mortgages and notes payable to unrelated third partiesUnsecured notes and loans payable to unrelated third parties
Other liabilities (including federal income tax, payables to related thirdparties, and other liabilities not included on lines 17-24). Complete Part Xof Schedule D Total liabilities. Add lines 17 through 25
and completeOrganizations that follow SFAS 117, check herelines 27 through 29, and lines 33 and 34.
272829
3031323334
Unrestricted net assetsTemporarily restricted net assetsPermanently restricted net assets
Capital stock or trust principal, or current fundsPaid-in or capital surplus, or land, building, or equipment fundRetained earnings, endowment, accumulated income, or other fundsTotal net assets or fund balancesTotal liabilities and net assets/fund balances
272829
3031323334
andOrganizations that do not follow SFAS 117, check here
complete lines 30 through 34.
Net
Ass
ets
orFu
ndB
alan
ces
Form 990 (2011)
JSA1E1053 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
2,788. 181,989.1,631,896. 1,713,909.
416,524. 592,463.1,092. 0
0 0
0 00 00 0
36,406. 29,357.
229,571.85,355. 106,868. 144,216.
0 00 00 00 0
1,105. 1,887.2,196,679. 2,663,821.
296,995. 342,585.0 0
3,539. 5,231.0 00 0
0 00 28,269.0 0
941,364. 1,109,778.1,241,898. 1,485,863.
X
950,293. 1,158,510.4,488. 19,448.
0 0
954,781. 1,177,958.2,196,679. 2,663,821.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 13

Form 990 (2011) Page 12Reconciliation of Net AssetsPart XICheck if Schedule O contains a response to any question in this Part XI
12345
123456
Total revenue (must equal Part VIII, column (A), line 12) Total expenses (must equal Part IX, column (A), line 25) Revenue less expenses. Subtract line 2 from line 1 Net assets or fund balances at beginning of year (must equal Part X, line 33, column (A)) Other changes in net assets or fund balances (explain in Schedule O) Net assets or fund balances at end of year. Combine lines 3, 4, and 5 (must equal Part X, line 33,column (B)) 6
Financial Statements and ReportingPart XIICheck if Schedule O contains a response to any question in this Part XII
Yes No1
2
3
Accounting method used to prepare the Form 990: Cash Accrual OtherIf the organization changed its method of accounting from a prior year or checked "Other," explain inSchedule O.
2a2b
2c
3a
3b
abc
d
a
b
Were the organization's financial statements compiled or reviewed by an independent accountant?Were the organization's financial statements audited by an independent accountant?If "Yes" to line 2a or 2b, does the organization have a committee that assumes responsibility for oversightof the audit, review, or compilation of its financial statements and selection of an independent accountant?If the organization changed either its oversight process or selection process during the tax year, explain inSchedule O.If "Yes" to line 2a or 2b, check a box below to indicate whether the financial statements for the year wereissued on a separate basis, consolidated basis, or both:
Both consolidated and separate basisSeparate basis Consolidated basisAs a result of a federal award, was the organization required to undergo an audit or audits as set forth inthe Single Audit Act and OMB Circular A-133?If "Yes," did the organization undergo the required audit or audits? If the organization did not undergo therequired audit or audits, explain why in Schedule O and describe any steps taken to undergo such audits
Form 990 (2011)
JSA1E1054 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
X
3,992,831.3,877,760.
115,071.954,781.108,106.
1,177,958.
X
XX
X
X
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 14

OMB No. 1545-0047SCHEDULE A Public Charity Status and Public Support(Form 990 or 990-EZ)Complete if the organization is a section 501(c)(3) organization or a section
4947(a)(1) nonexempt charitable trust.
Department of the Treasury Open to PublicInspection Attach to Form 990 or Form 990-EZ. See separate instructions.Internal Revenue Service
Name of the organization Employer identification number
Reason for Public Charity Status (All organizations must complete this part.) See instructions.Part IThe organization is not a private foundation because it is: (For lines 1 through 11, check only one box.)
1234
5
67
89
1011
A church, convention of churches, or association of churches described in section 170(b)(1)(A)(i).A school described in section 170(b)(1)(A)(ii). (Attach Schedule E.)A hospital or a cooperative hospital service organization described in section 170(b)(1)(A)(iii).A medical research organization operated in conjunction with a hospital described in section 170(b)(1)(A)(iii). Enter thehospital's name, city, and state:An organization operated for the benefit of a college or university owned or operated by a governmental unit described insection 170(b)(1)(A)(iv). (Complete Part II.)A federal, state, or local government or governmental unit described in section 170(b)(1)(A)(v).An organization that normally receives a substantial part of its support from a governmental unit or from the general publicdescribed in section 170(b)(1)(A)(vi). (Complete Part II.)A community trust described in section 170(b)(1)(A)(vi). (Complete Part II.)An organization that normally receives: (1) more than 331/3 % of its support from contributions, membership fees, and grossreceipts from activities related to its exempt functions - subject to certain exceptions, and (2) no more than 331/3% of itssupport from gross investment income and unrelated business taxable income (less section 511 tax) from businessesacquired by the organization after June 30, 1975. See section 509(a)(2). (Complete Part III.)An organization organized and operated exclusively to test for public safety. See section 509(a)(4).An organization organized and operated exclusively for the benefit of, to perform the functions of, or to carry out thepurposes of one or more publicly supported organizations described in section 509(a)(1) or section 509(a)(2). See section509(a)(3). Check the box that describes the type of supporting organization and complete lines 11e through 11h.a Type I b Type II c Type III - Functionally integrated d Type III - Other
e
f
g
h
By checking this box, I certify that the organization is not controlled directly or indirectly by one or more disqualifiedpersons other than foundation managers and other than one or more publicly supported organizations described in section509(a)(1) or section 509(a)(2).If the organization received a written determination from the IRS that it is a Type I, Type II, or Type III supportingorganization, check this box Since August 17, 2006, has the organization accepted any gift or contribution from any of thefollowing persons?
Yes No(i)
(ii)(iii)
A person who directly or indirectly controls, either alone or together with persons described in (ii)and (iii) below, the governing body of the supported organization? 11g(i)
11g(ii)
11g(iii)
A family member of a person described in (i) above?A 35% controlled entity of a person described in (i) or (ii) above?
Provide the following information about the supported organization(s).
(i) Name of supportedorganization
(ii) EIN (iii) Type of organization(described on lines 1-9above or IRC section(see instructions))
(iv) Is theorganization incol. (i) l isted inyour governing
document?
(v) Did you notifythe organization
in col. (i) ofyour support?
(vi) Is theorganization in
col. (i) organizedin the U.S.?
(vii) Amount ofsupport
Yes No Yes No Yes No
(A)
(B)
(C)
(D)
(E)
TotalFor Paperwork Reduction Act Notice, see the Instructions forForm 990 or 990-EZ.
Schedule A (Form 990 or 990-EZ) 2011
JSA1E1210 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 15

Schedule A (Form 990 or 990-EZ) 2011 Page 2Support Schedule for Organizations Described in Sections 170(b)(1)(A)(iv) and 170(b)(1)(A)(vi)(Complete only if you checked the box on line 5, 7, or 8 of Part I or if the organization failed to qualify underPart III. If the organization fails to qualify under the tests listed below, please complete Part III.)
Part II
Section A. Public Support(a) 2007 (b) 2008 (c) 2009 (d) 2010 (e) 2011 (f) TotalCalendar year (or fiscal year beginning in)
1 Gifts, grants, contributions, andmembership fees received. (Do notinclude any "unusual grants.")
2 Tax revenues levied for theorganization's benefit and either paidto or expended on its behalf
3 The value of services or facilitiesfurnished by a governmental unit to theorganization without charge
4 Total. Add lines 1 through 3 5 The portion of total contributions by
each person (other than agovernmental unit or publiclysupported organization) included online 1 that exceeds 2% of the amountshown on line 11, column (f)
6 Public support. Subtract line 5 from line 4.Section B. Total Support
(a) 2007 (b) 2008 (c) 2009 (d) 2010 (e) 2011 (f) TotalCalendar year (or fiscal year beginning in)
7 Amounts from line 4 8 Gross income from interest, dividends,
payments received on securities loans,rents, royalties and income from similarsources
9 Net income from unrelated businessactivities, whether or not the businessis regularly carried on
10 Other income. Do not include gain orloss from the sale of capital assets(Explain in Part IV.)
11 Total support. Add lines 7 through 10Gross receipts from related activities, etc. (see instructions)
12
1415
12 13 First five years. If the Form 990 is for the organization's first, second, third, fourth, or fifth tax year as a section 501(c)(3)
organization, check this box and stop here Section C. Computation of Public Support Percentage
%%
14 Public support percentage for 2011 (line 6, column (f) divided by line 11, column (f))Public support percentage from 2010 Schedule A, Part II, line 14
15 16a 331/3 % support test - 2011. If the organization did not check the box on line 13, and line 14 is 331/3 % or more, check
this box and stop here. The organization qualifies as a publicly supported organization b 331/3 % support test - 2010. If the organization did not check a box on line 13 or 16a, and line 15 is 331/3 % or more,
check this box and stop here. The organization qualifies as a publicly supported organization 17a 10%-facts-and-circumstances test - 2011. If the organization did not check a box on line 13, 16a, or 16b, and line 14 is
10% or more, and if the organization meets the "facts-and-circumstances" test, check this box and stop here. Explain inPart IV how the organization meets the "facts-and-circumstances” test. The organization qualifies as a publicly supportedorganization
b 10%-facts-and-circumstances test - 2010. If the organization did not check a box on line 13, 16a, 16b, or 17a, and line15 is 10% or more, and if the organization meets the "facts-and-circumstances" test, check this box and stop here.Explain in Part IV how the organzation meets the "facts-and-circumstances" test. The organization qualifies as a publiclysupported organization
18 Private foundation. If the organization did not check a box on line 13, 16a, 16b, 17a, or 17b, check this box and seeinstructions
Schedule A (Form 990 or 990-EZ) 2011
JSA
1E1220 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
3,258,342. 2,970,312. 2,756,778. 3,316,977. 4,171,690. 16,474,099.
3,258,342. 2,970,312. 2,756,778. 3,316,977. 4,171,690. 16,474,099.
91,741.
16,382,358.
3,258,342. 2,970,312. 2,756,778. 3,316,977. 4,171,690. 16,474,099.
17,848. 4,653. 3,659. 1,683. 461. 28,304.
526. 96. 49,238. 309,300. 359,160.ATCH 116,861,563.
552,291.
97.1699.37
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 16

Schedule A (Form 990 or 990-EZ) 2011 Page 3Support Schedule for Organizations Described in Section 509(a)(2)(Complete only if you checked the box on line 9 of Part I or if the organization failed to qualify under Part II.If the organization fails to qualify under the tests listed below, please complete Part II.)
Part III
Section A. Public Support(a) 2007 (b) 2008 (c) 2009 (d) 2010 (e) 2011 (f) TotalCalendar year (or fiscal year beginning in)
1 Gifts, grants, contributions, and membership fees
received. (Do not include any "unusual grants.")
2 Gross receipts from admissions, merchandise
sold or services performed, or facilities
furnished in any activity that is related to the
organization's tax-exempt purpose 3 Gross receipts from activities that are not an
unrelated trade or business under section 513 4 Tax revenues levied for the
organization's benefit and either paidto or expended on its behalf
5 The value of services or facilitiesfurnished by a governmental unit to theorganization without charge
6 Total. Add lines 1 through 5 7a Amounts included on lines 1, 2, and 3
received from disqualified persons b Amounts included on lines 2 and 3
received from other than disqualifiedpersons that exceed the greater of $5,000or 1% of the amount on line 13 for the year
c Add lines 7a and 7b 8 Public support (Subtract line 7c from
line 6.) Section B. Total Support
(a) 2007 (b) 2008 (c) 2009 (d) 2010 (e) 2011 (f) TotalCalendar year (or fiscal year beginning in)9 Amounts from line 6
10a Gross income from interest, dividends,payments received on securities loans,rents, royalties and income from similarsources
b Unrelated business taxable income (lesssection 511 taxes) from businessesacquired after June 30, 1975
c Add lines 10a and 10b 11 Net income from unrelated business
activities not included in line 10b,whether or not the business is regularlycarried on
12 Other income. Do not include gain orloss from the sale of capital assets(Explain in Part IV.)
13 Total support. (Add lines 9, 10c, 11,and 12.)
14 First five years. If the Form 990 is for the organization's first, second, third, fourth, or fifth tax year as a section 501(c)(3)organization, check this box and stop here
Section C. Computation of Public Support Percentage1516
Public support percentage for 2011 (line 8, column (f) divided by line 13, column (f))Public support percentage from 2010 Schedule A, Part III, line 15
1516
1718
%%
%%
Section D. Computation of Investment Income Percentage171819
20
Investment income percentage for 2011 (line 10c, column (f) divided by line 13, column (f))Investment income percentage from 2010 Schedule A, Part III, line 17
a
b
331/3 % support tests - 2011. If the organization did not check the box on line 14, and line 15 is more than 331/3 %, and line17 is not more than 331/3 %, check this box and stop here. The organization qualifies as a publicly supported organization331/3 % support tests - 2010. If the organization did not check a box on line 14 or line 19a, and line 16 is more than 331/3 %, andline 18 is not more than 331/3 %, check this box and stop here. The organization qualifies as a publicly supported organization Private foundation. If the organization did not check a box on line 14, 19a, or 19b, check this box and see instructions
JSA Schedule A (Form 990 or 990-EZ) 20111E1221 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 17
Schedule A (Form 990 or 990-EZ) 2011 Page 4Supplemental Information. Complete this part to provide the explanations required by Part II, line 10;Part II, line 17a or 17b; and Part III, line 12. Also complete this part for any additional information. (Seeinstructions).
Part IV
Schedule A (Form 990 or 990-EZ) 2011JSA
1E1225 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
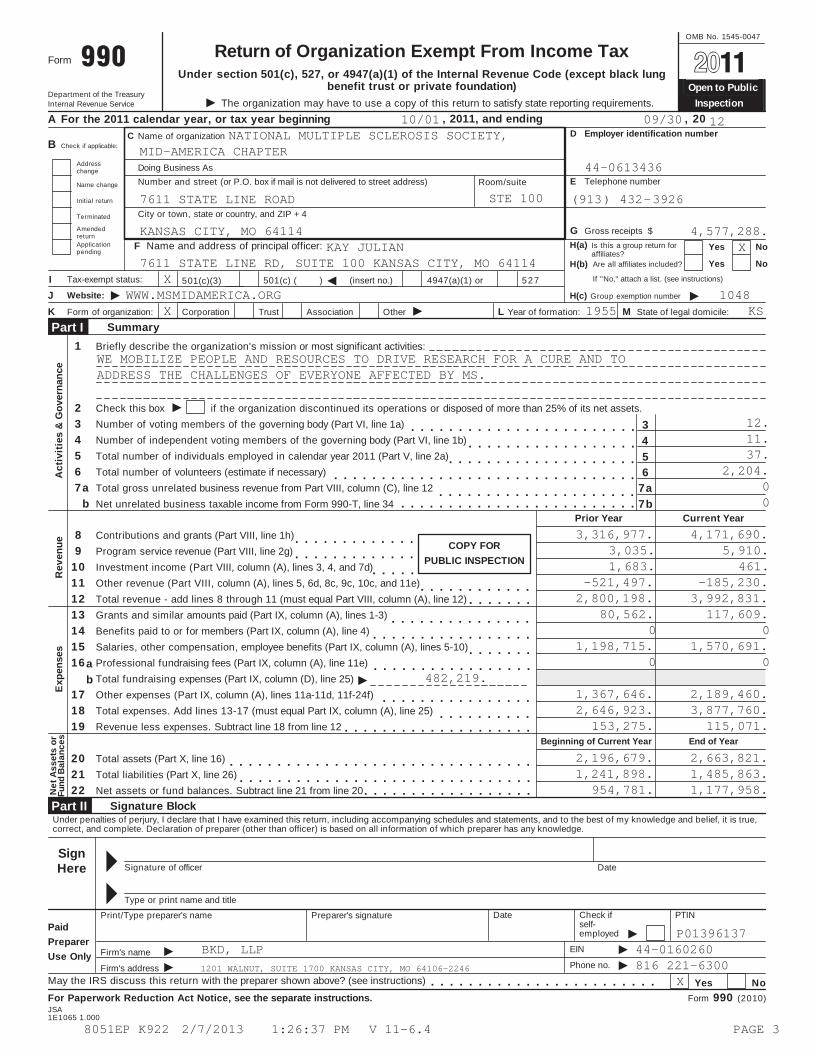
ATTACHMENT 1SCHEDULE A, PART II - OTHER INCOME
DESCRIPTION 2007 2008 2009 2010 2011 TOTAL
MISCELLANEOUS INCOME 526. 96. 49,238. 309,300. 359,160.
TOTALS 526. 96. 49,238. 309,300. 359,160.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 18

OMB No. 1545-0047Schedule B Schedule of Contributors
(Form 990, 990-EZ,or 990-PF) Department of the TreasuryInternal Revenue Service
Attach to Form 990, Form 990-EZ, or Form 990-PF.
Name of the organization Employer identification number
Organization type (check one):
Filers of:
Form 990 or 990-EZ
Section:
501(c)( ) (enter number) organization
4947(a)(1) nonexempt charitable trust not treated as a private foundation
527 political organization
501(c)(3) exempt private foundation
4947(a)(1) nonexempt charitable trust treated as a private foundation
501(c)(3) taxable private foundation
Form 990-PF
Check if your organization is covered by the General Rule or a Special Rule.Note. Only a section 501(c)(7), (8), or (10) organization can check boxes for both the General Rule and a Special Rule. Seeinstructions.
General Rule
For an organization filing Form 990, 990-EZ, or 990-PF that received, during the year, $5,000 or more (in money orproperty) from any one contributor. Complete Parts I and II.
Special Rules
For a section 501(c)(3) organization filing Form 990 or 990-EZ that met the 33 1/3 % support test of the regulationsunder sections 509(a)(1) and 170(b)(1)(A)(vi) and received from any one contributor, during the year, a contribution ofthe greater of (1) $5,000 or (2) 2% of the amount on (i) Form 990, Part VIII, line 1h, or (ii) Form 990-EZ, line 1.Complete Parts I and II.
For a section 501(c)(7), (8), or (10) organization filing Form 990 or 990-EZ that received from any one contributor,during the year, total contributions of more than $1,000 for use exclusively for religious, charitable, scientific, literary,or educational purposes, or the prevention of cruelty to children or animals. Complete Parts I, II, and III.
For a section 501(c)(7), (8), or (10) organization filing Form 990 or 990-EZ that received from any one contributor,during the year, contributions for use exclusively for religious, charitable, etc., purposes, but these contributions didnot total to more than $1,000. If this box is checked, enter here the total contributions that were received during theyear for an exclusively religious, charitable, etc., purpose. Do not complete any of the parts unless the General Ruleapplies to this organization because it received nonexclusively religious, charitable, etc., contributions of $5,000 ormore during the year $
Caution. An organization that is not covered by the General Rule and/or the Special Rules does not file Schedule B (Form 990,990-EZ, or 990-PF), but it must answer "No" on Part IV, line 2, of its Form 990; or check the box on line H of its Form 990-EZ or onPart I, line 2, of its Form 990-PF, to certify that it does not meet the filing requirements of Schedule B (Form 990, 990-EZ, or 990-PF).
For Paperwork Reduction Act Notice, see the Instructions for Form 990, 990-EZ, or 990-PF. Schedule B (Form 990, 990-EZ, or 990-PF) (2011)
JSA
1E1251 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
X 3
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 19

Schedule B (Form 990, 990-EZ, or 990-PF) (2011) Page 2Name of organization Employer identification number
Contributors (see instructions). Use duplicate copies of Part I if additional space is needed.Part I
(a)No.
(b)Name, address, and ZIP + 4
(c)Total contributions
(d)Type of contribution
PersonPayrollNoncash$
(Complete Part II if there isa noncash contribution.)
(a)No.
(b)Name, address, and ZIP + 4
(c)Total contributions
(d)Type of contribution
PersonPayrollNoncash$
(Complete Part II if there isa noncash contribution.)
(a)No.
(b)Name, address, and ZIP + 4
(c)Total contributions
(d)Type of contribution
PersonPayrollNoncash$
(Complete Part II if there isa noncash contribution.)
(a)No.
(b)Name, address, and ZIP + 4
(c)Total contributions
(d)Type of contribution
PersonPayrollNoncash$
(Complete Part II if there isa noncash contribution.)
(a)No.
(b)Name, address, and ZIP + 4
(c)Total contributions
(d)Type of contribution
PersonPayrollNoncash$
(Complete Part II if there isa noncash contribution.)
(a)No.
(b)Name, address, and ZIP + 4
(c)Total contributions
(d)Type of contribution
PersonPayrollNoncash$
(Complete Part II if there isa noncash contribution.)
Schedule B (Form 990, 990-EZ, or 990-PF) (2011)JSA
1E1253 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
1 X
99,621.
2 X
130,000.
3 X
200,000.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 20

Schedule B (Form 990, 990-EZ, or 990-PF) (2011) Page 3Name of organization Employer identification number
Noncash Property (see instructions). Use duplicate copies of Part II if additional space is needed.Part II
(a) No.fromPart I
(c)FMV (or estimate)(see instructions)
(b)Description of noncash property given
(d)Date received
$
(a) No.fromPart I
(c)FMV (or estimate)(see instructions)
(b)Description of noncash property given
(d)Date received
$
(a) No.fromPart I
(c)FMV (or estimate)(see instructions)
(b)Description of noncash property given
(d)Date received
$
(a) No.fromPart I
(c)FMV (or estimate)(see instructions)
(b)Description of noncash property given
(d)Date received
$
(a) No.fromPart I
(c)FMV (or estimate)(see instructions)
(b)Description of noncash property given
(d)Date received
$
(a) No.fromPart I
(c)FMV (or estimate)(see instructions)
(b)Description of noncash property given
(d)Date received
$
Schedule B (Form 990, 990-EZ, or 990-PF) (2011)JSA
1E1254 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 21

Schedule B (Form 990, 990-EZ, or 990-PF) (2011) Page 4Name of organization Employer identification number
Exclusively religious, charitable, etc., individual contributions to section 501(c)(7), (8), or (10) organizationsthat total more than $1,000 for the year. Complete columns (a) through (e) and the following line entry.
Part III
For organizations completing Part III, enter the total of exclusively religious, charitable, etc.,contributions of $1,000 or less for the year. (Enter this information once. See instructions.) $Use duplicate copies of Part III if additional space is needed.
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
Schedule B (Form 990, 990-EZ, or 990-PF) (2011)JSA
1E1255 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 22

SCHEDULE C OMB No. 1545-0047Political Campaign and Lobbying Activities(Form 990 or 990-EZ)
For Organizations Exempt From Income Tax Under section 501(c) and section 527 Attach to Form 990 or Form 990-EZ.Complete if the organization is described below. Open to PublicDepartment of the Treasury See separate instructions.Internal Revenue Service InspectionIf the organization answered "Yes" to Form 990, Part IV, line 3, or Form 990-EZ, Part V, line 46 (Political Campaign Activities), then Section 501(c)(3) organizations: Complete Parts I-A and B. Do not complete Part I-C.
Section 501(c) (other than section 501(c)(3)) organizations: Complete Parts I-A and C below. Do not complete Part I-B.Section 527 organizations: Complete Part I-A only.
If the organization answered "Yes" to Form 990, Part IV, line 4, or Form 990-EZ, Part VI, line 47 (Lobbying Activities), then Section 501(c)(3) organizations that have filed Form 5768 (election under section 501(h)): Complete Part II-A. Do not complete Part II-B.Section 501(c)(3) organizations that have NOT filed Form 5768 (election under section 501(h)): Complete Part II-B. Do not complete Part II-A.
If the organization answered "Yes" to Form 990, Part IV, line 5 (Proxy Tax) or Form 990-EZ, Part V, line 35c (Proxy Tax), then Section 501(c)(4), (5), or (6) organizations: Complete Part III.Name of organization Employer identification number
Complete if the organization is exempt under section 501(c) or is a section 527 organization.Part I-A
123
4
Provide a description of the organization's direct and indirect political campaign activities in Part IV.Political expendituresVolunteer hours
$
Complete if the organization is exempt under section 501(c)(3).Part I-B$Enter the amount of any excise tax incurred by the organization under section 4955
Enter the amount of any excise tax incurred by organization managers under section 4955If the organization incurred a section 4955 tax, did it file Form 4720 for this year?
1234
$
YesYes
NoNo
ab
Was a correction made?If "Yes," describe in Part IV.
Complete if the organization is exempt under section 501(c), except section 501(c)(3).Part I-C
1
2
3
4
Enter the amount directly expended by the filing organization for section 527 exempt functionactivities $ Enter the amount of the filing organization's funds contributed to other organizations for section527 exempt function activities $ Total exempt function expenditures. Add lines 1 and 2. Enter here and on Form 1120-POL,line 17b $ Did the filing organization file Form 1120-POL for this year? Yes No
5 Enter the names, addresses and employer identification number (EIN) of all section 527 political organizations to which the filingorganization made payments. For each organization listed, enter the amount paid from the filing organization's funds. Also enterthe amount of political contributions received that were promptly and directly delivered to a separate political organization, suchas a separate segregated fund or a political action committee (PAC). If additional space is needed, provide information in Part IV.
(a) Name (b) Address (c) EIN (d) Amount paid fromfiling organization's
funds. If none, enter -0-.
(e) Amount of politicalcontributions received and
promptly and directlydelivered to a separatepolitical organization. If
none, enter -0-.
(1)
(2)
(3)
(4)
(5)
(6)
Schedule C (Form 990 or 990-EZ) 2011For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ.
JSA1E1264 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 23

Page 2Schedule C (Form 990 or 990-EZ) 2011
Complete if the organization is exempt under section 501(c)(3) and filed Form 5768 (election undersection 501(h)).
Part II-A A Check if the filing organization belongs to an affiliated group (and list in Part IV each affiliated group member'sname, address, EIN, expenses, and share of excess lobbying expenditures).
B Check if the filing organization checked box A and "limited control" provisions apply.Limits on Lobbying Expenditures
(The term "expenditures" means amounts paid or incurred.)(a) Filing
organization's totals(b) Affiliatedgroup totals
1 abcdef
Total lobbying expenditures to influence public opinion (grass roots lobbying)Total lobbying expenditures to influence a legislative body (direct lobbying)Total lobbying expenditures (add lines 1a and 1b)Other exempt purpose expendituresTotal exempt purpose expenditures (add lines 1c and 1d)Lobbying nontaxable amount. Enter the amount from the following table in bothcolumns.
If the amount on line 1e, column (a) or (b) is:Not over $500,000Over $500,000 but not over $1,000,000Over $1,000,000 but not over $1,500,000Over $1,500,000 but not over $17,000,000Over $17,000,000
The lobbying nontaxable amount is:20% of the amount on line 1e.$100,000 plus 15% of the excess over $500,000.$175,000 plus 10% of the excess over $1,000,000.$225,000 plus 5% of the excess over $1,500,000.$1,000,000.
ghij
Grassroots nontaxable amount (enter 25% of line 1f)Subtract line 1g from line 1a. If zero or less, enter -0-Subtract line 1f from line 1c. If zero or less, enter -0-If there is an amount other than zero on either line 1h or line 1i, did the organization file Form 4720reporting section 4911 tax for this year?
Yes No
4-Year Averaging Period Under Section 501(h)(Some organizations that made a section 501(h) election do not have to complete all of the five
columns below. See the instructions for lines 2a through 2f on page 4.)
Lobbying Expenditures During 4-Year Averaging Period
Calendar year (or fiscal yearbeginning in)
(a) 2008 (b) 2009 (c) 2010 (d) 2011 (e) Total
2 a Lobbying nontaxable amount
b Lobbying ceiling amount(150% of line 2a, column (e))
c Total lobbying expenditures
d Grassroots nontaxable amount
e Grassroots ceiling amount(150% of line 2d, column (e))
f Grassroots lobbying expenditures
Schedule C (Form 990 or 990-EZ) 2011
JSA1E1265 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 24

Page 3Schedule C (Form 990 or 990-EZ) 2011
Complete if the organization is exempt under section 501(c)(3) and has NOT filed Form 5768(election under section 501(h)).
Part II-B
(a) (b)For each "Yes" response to lines 1a through 1i below, provide in Part IV a detailed descriptionof the lobbying activity. Yes No Amount
During the year, did the filing organization attempt to influence foreign, national, state or locallegislation, including any attempt to influence public opinion on a legislative matter orreferendum, through the use of:
1
abcdefghij
Volunteers?Paid staff or management (include compensation in expenses reported on lines 1c through 1i)?Media advertisements?Mailings to members, legislators, or the public?Publications, or published or broadcast statements?Grants to other organizations for lobbying purposes?Direct contact with legislators, their staffs, government officials, or a legislative body?Rallies, demonstrations, seminars, conventions, speeches, lectures, or any similar means?Other activities?Total. Add lines 1c through 1i
2 a Did the activities in line 1 cause the organization to be not described in section 501(c)(3)?
If "Yes," enter the amount of any tax incurred under section 4912If "Yes," enter the amount of any tax incurred by organization managers under section 4912If the filing organization incurred a section 4912 tax, did it file Form 4720 for this year?
b c d
Complete if the organization is exempt under section 501(c)(4), section 501(c)(5), or section501(c)(6).
Part III-A
Yes No123
Were substantially all (90% or more) dues received nondeductible by members?Did the organization make only in-house lobbying expenditures of $2,000 or less?Did the organization agree to carry over lobbying and political expenditures from the prior year?
1 2 3
Complete if the organization is exempt under section 501(c)(4), section 501(c)(5), or section501(c)(6) and if either (a) BOTH Part III-A, lines 1 and 2, are answered "No" OR (b) Part III-A, line 3, isanswered "Yes."
Part III-B
1 Dues, assessments and similar amounts from members 1 2 Section 162(e) nondeductible lobbying and political expenditures (do not include amounts of
political expenses for which the section 527(f) tax was paid).abc
Current yearCarryover from last yearTotal
2a2b2c3
45
3 Aggregate amount reported in section 6033(e)(1)(A) notices of nondeductible section 162(e) dues 4 If notices were sent and the amount on line 2c exceeds the amount on line 3, what portion of the
excess does the organization agree to carryover to the reasonable estimate of nondeductible lobbyingand political expenditure next year?
5 Taxable amount of lobbying and political expenditures (see instructions) Supplemental InformationPart IV
Complete this part to provide the descriptions required for Part I-A, line 1; Part I-B, line 4; Part I-C, line 5; Part II-A; and Part II-B, line1. Also, complete this part for any additional information.
Schedule C (Form 990 or 990-EZ) 2011JSA1E1266 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
XX
XX 584.
XX
X 15,018.XX
15,602.X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 25

Schedule C (Form 990 or 990-EZ) 2011 Page 4Supplemental Information (continued)Part IV
Schedule C (Form 990 or 990-EZ) 2011JSA
1E1500 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 26

OMB No. 1545-0047SCHEDULE D Supplemental Financial Statements(Form 990) Complete if the organization answered "Yes," to Form 990,Part IV, line 6, 7, 8, 9, 10, 11a, 11b, 11c, 11d, 11e, 11f, 12a, or 12b.
Open to PublicDepartment of the Treasury Attach to Form 990. See separate instructions.Internal Revenue Service Inspection
Name of the organization Employer identification number
Organizations Maintaining Donor Advised Funds or Other Similar Funds or Accounts. Complete if theorganization answered "Yes" to Form 990, Part IV, line 6.
Part I
(a) Donor advised funds (b) Funds and other accounts
12345
6
Total number at end of yearAggregate contributions to (during year)Aggregate grants from (during year)Aggregate value at end of year
Did the organization inform all donors and donor advisors in writing that the assets held in donor advisedfunds are the organization’s property, subject to the organization's exclusive legal control? Yes NoDid the organization inform all grantees, donors, and donor advisors in writing that grant funds can be usedonly for charitable purposes and not for the benefit of the donor or donor advisor, or for any other purposeconferring impermissible private benefit? Yes No
Conservation Easements. Complete if the organization answered "Yes" to Form 990, Part IV, line 7.Part II1 Purpose(s) of conservation easements held by the organization (check all that apply).
Preservation of land for public use (e.g., recreation or education)Protection of natural habitatPreservation of open space
Preservation of an historically important land areaPreservation of a certified historic structure
2
3
45
6
7
8
9
Complete lines 2a through 2d if the organization held a qualified conservation contribution in the form of a conservationeasement on the last day of the tax year.
Held at the End of the Tax Year
2a2b2c
2d
abcd
Total number of conservation easementsTotal acreage restricted by conservation easementsNumber of conservation easements on a certified historic structure included in (a)Number of conservation easements included in (c) acquired after 8/17/06, and not on ahistoric structure listed in the National RegisterNumber of conservation easements modified, transferred, released, extinguished, or terminated by the organization during thetax yearNumber of states where property subject to conservation easement is locatedDoes the organization have a written policy regarding the periodic monitoring, inspection, handling ofviolations, and enforcement of the conservation easements it holds?Staff and volunteer hours devoted to monitoring, inspecting, and enforcing conservation easements during the year
Amount of expenses incurred in monitoring, inspecting, and enforcing conservation easements during the year
Does each conservation easement reported on line 2(d) above satisfy the requirements of section 170(h)(4)(B)(i) and section 170(h)(4)(B)(ii)?
Yes No$
Yes No In Part XIV, describe how the organization reports conservation easements in its revenue and expense statement, andbalance sheet, and include, if applicable, the text of the footnote to the organization’s financial statements that describes theorganization’s accounting for conservation easements.
Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets.Complete if the organization answered "Yes" to Form 990, Part IV, line 8.
Part III
1a If the organization elected, as permitted under SFAS 116 (ASC 958), not to report in its revenue statement and balance sheetworks of art, historical treasures, or other similar assets held for public exhibition, education, or research in furtherance ofpublic service, provide, in Part XIV, the text of the footnote to its financial statements that describes these items.
b If the organization elected, as permitted under SFAS 116 (ASC 958), to report in its revenue statement and balance sheetworks of art, historical treasures, or other similar assets held for public exhibition, education, or research in furtherance ofpublic service, provide the following amounts relating to these items: (i)(ii)
Revenues included in Form 990, Part VIII, line 1Assets included in Form 990, Part X
$$
2 If the organization received or held works of art, historical treasures, or other similar assets for financial gain, provide thefollowing amounts required to be reported under SFAS 116 (ASC 958) relating to these items: a Revenues included in Form 990, Part VIII, line 1Assets included in Form 990, Part X
$$b
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Schedule D (Form 990) 2011JSA
1E1268 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 27

Schedule D (Form 990) 2011 Page 2Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets (continued)Part III
Using the organization's acquisition, accession, and other records, check any of the following that are a significant use of its
Provide a description of the organization's collections and explain how they further the organization's exempt purpose in PartXIV.
3
4
5
collection items (check all that apply):Public exhibitionScholarly researchPreservation for future generations
Loan or exchange programsOther
abc
de
During the year, did the organization solicit or receive donations of art, historical treasures, or other similarassets to be sold to raise funds rather than to be maintained as part of the organization's collection? Yes No
Escrow and Custodial Arrangements. Complete if the organization answered "Yes" to Form 990, Part IV,line 9, or reported an amount on Form 990, Part X, line 21.
Part IV
1a
b
cdef
2ab
Is the organization an agent, trustee, custodian or other intermediary for contributions or other assets notincluded on Form 990, Part X?If "Yes," explain the arrangement in Part XIV and complete the following table:
Beginning balanceAdditions during the yearDistributions during the yearEnding balanceDid the organization include an amount on Form 990, Part X, line 21?If "Yes," explain the arrangement in Part XIV.
Yes No
Amount 1c1d1e1f
Yes No Endowment Funds. Complete if the organization answered "Yes" to Form 990, Part IV, line 10.Part V
(a) Current year (b) Prior year (c) Two years back (d) Three years back (e) Four years back
1abc
de
fg
abc
3a
b
Beginning of year balanceContributionsNet investment earnings, gains,and lossesGrants or scholarshipsOther expenditures for facilitiesand programsAdministrative expensesEnd of year balance
2
4
Provide the estimated percentage of the current year end balance (line 1g, column (a)) held as:Board designated or quasi-endowment %Permanent endowment %Temporarily restricted endowment %The percentages in lines 2a, 2b, and 2c should equal 100%.Are there endowment funds not in the possession of the organization that are held and administered for theorganization by:(i) unrelated organizations(ii) related organizationsIf "Yes" to 3a(ii), are the related organizations listed as required on Schedule R?Describe in Part XIV the intended uses of the organization's endowment funds.
Yes No 3a(i)
3a(ii)3b
Land, Buildings, and Equipment. See Form 990, Part X, line 10.Part VI
Description of property (a) Cost or other basis(investment)
(b) Cost or other basis(other)
(c) Accumulateddepreciation
(d) Book value 1a
bcde
LandBuildingsLeasehold improvementsEquipmentOther Total. Add lines 1a through 1e. (Column (d) must equal Form 990, Part X, column (B), line 10(c).)
Schedule D (Form 990) 2011
JSA1E1269 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
55,000. 55,000.
700. 700.
173,871. 85,355. 88,516.144,216.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 28

Schedule D (Form 990) 2011 Page 3Investments - Other Securities. See Form 990, Part X, line 12.Part VII
(a) Description of security or category(including name of security)
(b) Book value (c) Method of valuation:Cost or end-of-year market value
(1) Financial derivatives(2) Closely-held equity interests(3) Other
(A)(B)(C)(D)(E)(F)(G)(H)(I) Total. (Column (b) must equal Form 990, Part X, col. (B) line 12.)
Investments - Program Related. See Form 990, Part X, line 13.Part VIII(a) Description of investment type (b) Book value (c) Method of valuation:
Cost or end-of-year market value
(1)(2)(3)(4)(5)(6)(7)(8)(9)
(10) Total. (Column (b) must equal Form 990, Part X, col. (B) line 13.)
Other Assets. See Form 990, Part X, line 15.Part IX(a) Description (b) Book value
(1)(2)(3)(4)(5)(6)(7)(8)(9)
(10) Total. (Column (b) must equal Form 990, Part X, col. (B) line 15.) Other Liabilities. See Form 990, Part X, line 25.Part X
1. (a) Description of liability (b) Book value(1)(2)(3)(4)(5)(6)(7)(8)(9)
(10)(11)
Federal income taxes
Total. (Column (b) must equal Form 990, Part X, col. (B) line 25.)
2. FIN 48 (ASC 740) Footnote. In Part XIV, provide the text of the footnote to the organization's financial statements that reports theorganization's liability for uncertain tax positions under FIN 48 (ASC 740).JSA Schedule D (Form 990) 20111E1270 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
DUE TO NATIONAL MS SOCIETY 1,109,220.DUE TO OTHER MS CHAPTERS 558.
1,109,778.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 29

Schedule D (Form 990) 2011 Page 4Reconciliation of Change in Net Assets from Form 990 to Audited Financial StatementsPart XI
123456789
10
Total revenue (Form 990, Part VIII, column (A), line 12)Total expenses (Form 990, Part IX, column (A), line 25)Excess or (deficit) for the year. Subtract line 2 from line 1Net unrealized gains (losses) on investmentsDonated services and use of facilitiesInvestment expensesPrior period adjustmentsOther (Describe in Part XIV.)Total adjustments (net). Add lines 4 through 8Excess or (deficit) for the year per audited financial statements. Combine lines 3 and 9
123456789
10
Reconciliation of Revenue per Audited Financial Statements With Revenue per ReturnPart XII
12
34
5
Total revenue, gains, and other support per audited financial statementsAmounts included on line 1 but not on Form 990, Part VIII, line 12:Net unrealized gains on investmentsDonated services and use of facilitiesRecoveries of prior year grantsOther (Describe in Part XIV.)Add lines 2a through 2dSubtract line 2e from line 1Amounts included on Form 990, Part VIII, line 12, but not on line 1 :Investment expenses not included on Form 990, Part VIII, line 7bOther (Describe in Part XIV.)Add lines 4a and 4bTotal revenue. Add lines 3 and 4c. (This must equal Form 990, Part I, line 12.)
1
2e3
4c5
abcde
abc
2a2b2c2d
4a4b
Reconciliation of Expenses per Audited Financial Statements With Expenses per ReturnPart XIII
12
34
5
12
34
5
Total expenses and losses per audited financial statementsAmounts included on line 1 but not on Form 990, Part IX, line 25:Donated services and use of facilitiesPrior year adjustmentsOther lossesOther (Describe in Part XIV.)Add lines 2a through 2dSubtract line 2e from line 1Amounts included on Form 990, Part IX, line 25, but not on line 1:Investment expenses not included on Form 990, Part VIII, line 7bOther (Describe in Part XIV.)Add lines 4a and 4bTotal expenses. Add lines 3 and 4c. (This must equal Form 990, Part I, line 18.)
1
2e3
4c5
abcde
abc
2a2b2c2d
4a4b
Supplemental InformationPart XIV
Complete this part to provide the descriptions required for Part II, lines 3, 5, and 9; Part III, lines 1a and 4; Part IV, lines 1b and 2b;Part V, line 4; Part X, line 2; Part XI, line 8; Part XII, lines 2d and 4b; and Part XIII, lines 2d and 4b. Also complete this part to provideany additional information.
Schedule D (Form 990) 2011
JSA
1E1271 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
3,992,831.3,877,760.
115,071.
115,071.
4,358,822.
130,418.
235,573.365,991.
3,992,831.
3,992,831.
4,243,751.
130,418.
235,573.365,991.
3,877,760.
3,877,760.
SEE PAGE 5
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 30

Schedule D (Form 990) 2011 Page 5Supplemental Information (continued)Part XIV
Schedule D (Form 990) 2011
JSA
1E1226 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
RECONCILIATION OF REVENUES
SCHEDULE D, PART XII, LINE 2D
SPECIAL EVENT EXPENSES $ 235,573
RECONCILIATION OF EXPENSES
SCHEDULE D, PART XIII, LINE 2D
SPECIAL EVENT EXPENSES $ 235,573
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 31

OMB No. 1545-0047Supplemental Information Regarding
Fundraising or Gaming ActivitiesSCHEDULE G(Form 990 or 990-EZ)
Complete if the organization answered "Yes" to Form 990, Part IV, lines 17, 18, or 19, or if theorganization entered more than $15,000 on Form 990-EZ, line 6a. Open to Public
Department of the Treasury Attach to Form 990 or Form 990-EZ. See separate instructions.Internal Revenue Service InspectionName of the organization Employer identification number
Fundraising Activities. Complete if the organization answered "Yes" to Form 990, Part IV, line 17.Form 990-EZ filers are not required to complete this part.Part I
1 Indicate whether the organization raised funds through any of the following activities. Check all that apply.abcd
Mail solicitationsInternet and email solicitationsPhone solicitationsIn-person solicitations
efg
Solicitation of non-government grantsSolicitation of government grantsSpecial fundraising events
a2 Did the organization have a written or oral agreement with any individual (including officers, directors, trusteesor key employees listed in Form 990, Part VII) or entity in connection with professional fundraising services? Yes No
b If "Yes," list the ten highest paid individuals or entities (fundraisers) pursuant to agreements under which the fundraiser is to becompensated at least $5,000 by the organization.
(v) Amount paid to(or retained by)
fundraiser listed incol. (i)
(iii) Did fundraiser havecustody or control of
contributions?
(vi) Amount paid to(or retained by)
organization
(i) Name and address of individualor entity (fundraiser)
(iv) Gross receiptsfrom activity(ii) Activity
Yes No1
2
3
4
5
6
7
8
9
10
Total 3 List all states in which the organization is registered or licensed to solicit contributions or has been notified it is exempt from
registration or licensing.
Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ. Schedule G (Form 990 or 990-EZ) 2011JSA
1E1281 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 32

Schedule G (Form 990 or 990-EZ) 2011 Page 2Fundraising Events. Complete if the organization answered "Yes" to Form 990, Part IV, line 18, or reported morethan $15,000 of fundraising event contributions and gross income on Form 990-EZ, lines 1 and 6b. List events withgross receipts greater than $5,000.
Part II
(a) Event #1 (b) Event #2 (c) Other Events (d) Total events(add col. (a) through
col. (c))(event type) (event type) (total number)
12
3
Gross receiptsLess: CharitablecontributionsGross income (line 1 minusline 2)
Rev
enue
4
5
6
7
8
9
1011
Cash prizes
Noncash prizes
Rent/facility costs
Food and beverages
Entertainment
Other direct expenses
Direct expense summary. Add lines 4 through 9 in column (d)Net income summary. Combine line 3, column (d), and line 10
( )
Dire
ctE
xpen
ses
Gaming. Complete if the organization answered "Yes" to Form 990, Part IV, line 19, or reported morethan $15,000 on Form 990-EZ, line 6a.
Part III
(d) Total gaming (addcol. (a) through col. (c))
(b) Pull tabs/instantbingo/progressive bingo (c) Other gaming(a) Bingo
1
2
3
Gross revenue
Cash prizes
Noncash prizes
Rev
enue
4
5
6
7
8
Rent/facility costs
Other direct expenses
Volunteer labor
Direct expense summary. Add lines 2 through 5 in column (d)
Net gaming income summary. Combine line 1, column d, and line 7
Dire
ctE
xpen
ses
YesNo
YesNo
YesNo
% % % ( )
9
10
Enter the state(s) in which the organization operates gaming activities:Is the organization licensed to operate gaming activities in each of these states?If "No," explain:
Were any of the organization's gaming licenses revoked, suspended or terminated during the tax year?If "Yes," explain:
ab
Yes No ab
Yes No Schedule G (Form 990 or 990-EZ) 2011
JSA1E1282 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
WALK MS BIKE MS 3.
1,003,668. 2,037,969. 404,528. 3,446,165.
980,896. 1,974,620. 400,722. 3,356,238.
22,772. 63,349. 3,806. 89,927.
187,402. 338,361. 58,694. 584,457.
584,457.-494,530.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 33

Schedule G (Form 990 or 990-EZ) 2011 Page 31112
Does the organization operate gaming activities with nonmembers?Is the organization a grantor, beneficiary or trustee of a trust or a member of a partnership or other entityformed to administer charitable gaming?
Yes No Yes No
13
14
Indicate the percentage of gaming activity operated in:The organization's facilityAn outside facility
ab
13a13b
%%
Enter the name and address of the person who prepares the organization's gaming/special events books andrecords:
Name
Address 15 a
b
c
Does the organization have a contract with a third party from whom the organization receives gamingrevenue? Yes No If "Yes," enter the amount of gaming revenue received by the organization $ and theamount of gaming revenue retained by the third party $ .If "Yes," enter name and address of the third party:Name
Address 16 Gaming manager information:Name Gaming manager compensation $Description of services provided
Director/officer Employee Independent contractor
17 Mandatory distributions:a
b
Is the organization required under state law to make charitable distributions from the gaming proceeds toretain the state gaming license? Yes No Enter the amount of distributions required under state law to be distributed to other exempt organizationsor spent in the organization's own exempt activities during the tax year $
Supplemental Information. Complete this part to provide the explanation required by Part I, line 2b,columns (iii) and (v), and Part III, lines 9, 9b, 10b, 15b, 15c, 16, and 17b, as applicable. Also complete thispart to provide any additional information (see instructions).
Part IV
Schedule G (Form 990 or 990-EZ) 2011
JSA
1E1503 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 34
OM
BN
o.15
45-0
047
SCHE
DU
LEI
(For
m99
0)G
rant
san
dO
ther
Assi
stan
ceto
Org
aniz
atio
ns,
Gov
ernm
ents
,and
Indi
vidu
als
inth
eU
nite
dSt
ates
Com
plet
eif
the
orga
niza
tion
answ
ered
"Yes
"to
Form
990,
Part
IV,l
ine
21or
22.
Att
ach
toFo
rm99
0.O
pen
toPu
blic
Dep
artm
ento
fthe
Trea
sury
Inte
rnal
Rev
enue
Ser
vice
In
spec
tion
Nam
eof
the
orga
niza
tion
Empl
oyer
iden
tific
atio
nnu
mbe
r
Gen
eral
Info
rmat
ion
onG
rant
san
dAs
sist
ance
Par
tI1 2
Doe
sth
eor
gani
zatio
nm
aint
ain
reco
rds
tosu
bsta
ntia
teth
eam
ount
ofth
egr
ants
oras
sist
ance
,the
gran
tees
'elig
ibilit
yfo
rthe
gran
tsor
assi
stan
ce,a
ndth
ese
lect
ion
crite
riaus
edto
awar
dth
egr
ants
oras
sist
ance
?D
escr
ibe
inP
artI
Vth
eor
gani
zatio
n's
proc
edur
esfo
rm
onito
ring
the
use
ofgr
antf
unds
inth
eU
nite
dS
tate
s.
Yes
No
Gra
nts
and
Oth
erA
ssis
tanc
eto
Gov
ernm
ents
and
Org
aniz
atio
nsin
the
Uni
ted
Stat
es.C
ompl
ete
ifth
eor
gani
zatio
nan
swer
ed"Y
es"
toFo
rm99
0,P
artI
V,l
ine
21,f
oran
yre
cipi
entt
hatr
ecei
ved
mor
eth
an$5
,000
.Che
ckth
isbo
xif
noon
ere
cipi
entr
ecei
ved
mor
eth
an$5
,000
.P
artI
Ican
bedu
plic
ated
ifad
ditio
nals
pace
isne
eded
Par
tII
(a
)Nam
ean
dad
dres
sof
orga
niza
tion
orgo
vern
men
t(f)
Met
hod
ofva
luat
ion
(boo
k,FM
V,ap
prai
sal,
othe
r)
(c)I
RC
sect
ion
ifap
plic
able
(d)A
mou
ntof
cash
gran
t(e
)Am
ount
ofno
n-ca
shas
sist
ance
(g)D
escr
iptio
nof
non-
cash
assi
stan
ce(h
)Pur
pose
ofgr
ant
oras
sist
ance
(b)E
IN1 (1
)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(12)
2 3
Ent
erto
taln
umbe
rof
sect
ion
501(
c)(3
)an
dgo
vern
men
torg
aniz
atio
nslis
ted
inth
elin
e1
tabl
eE
nter
tota
lnum
ber
ofot
her
orga
niza
tions
liste
din
the
line
1ta
ble
For
Pape
rwor
kR
educ
tion
ActN
otic
e,se
eth
eIn
stru
ctio
nsfo
rFor
m99
0.S
ched
ule
I(Fo
rm99
0)(2
011)
JSA
1E12
881.
000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,
MID-AMERICA CHAPTER
44-0613436
X
8051EP K922
2/7/2013
1:26:37 PM
V 11-6.4
PAGE 35
Sch
edul
eI(
Form
990)
(201
1)Pa
ge2
Gra
nts
and
Oth
erA
ssis
tanc
eto
Indi
vidu
als
inth
eU
nite
dSt
ates
.Com
plet
eif
the
orga
niza
tion
answ
ered
"Yes
"on
Form
990,
Part
IV,l
ine
22.
Par
tIII
can
bedu
plic
ated
ifad
ditio
nals
pace
isne
eded
.P
artI
II
(f)D
escr
iptio
nof
non-
cash
assi
stan
ce(a
)Typ
eof
gran
tora
ssis
tanc
e(e
) Met
hod
ofva
luat
ion
(boo
k,F
MV
,app
rais
al,o
ther
)(b
)Num
bero
fre
cipi
ents
(d)A
mou
ntof
non-
cash
assi
stan
ce(c
)Am
ount
ofca
shgr
ant
1 2 3 4 5 6 7S
uppl
emen
talI
nfor
mat
ion.
Com
plet
eth
ispa
rtto
prov
ide
the
info
rmat
ion
requ
ired
inPa
rtI,
line
2,an
dan
yot
hera
dditio
nali
nfor
mat
ion.
Par
tIV
Sch
edul
eI(
Form
990)
(201
1)
JSA
1E15
042.
000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,
44-0613436
FINANCIAL ASSISTANCE TO PEOPLE WITH MS
209.
117,609.
PROCESS FOR MONITORING THE USE OF GRANTS IN THE U.S.
SCHEDULE I, PART I, LINE 2
MS-RELATED ORGANIZATION GRANTEES ARE REQUIRED TO SUBMIT FINANCIAL AND
PROGRAM PROGRESS REPORTS THAT ARE REVIEWED AND APPROVED BEFORE ADDITIONAL
FUNDING IS PROVIDED.
8051EP K922
2/7/2013
1:26:37 PM
V 11-6.4
PAGE 36

OMB No. 1545-0047SCHEDULE M Noncash Contributions(Form 990) Complete if the organizations answered "Yes" on Form990, Part IV, lines 29 or 30.
Department of the TreasuryInternal Revenue Service
Open To PublicInspectionAttach to Form 990.
Name of the organization Employer identification number
Types of PropertyPart I(c)
Noncash contributionamounts reported on
Form 990, Part VIII, line 1g
(a)Check if
applicable
(b)Number of contributions or
items contributed
(d)Method of determining
noncash contribution amounts
12345
6789
1011
1213
14
1516171819202122232425262728
Art - Works of artArt - Historical treasuresArt - Fractional interestsBooks and publicationsClothing and householdgoodsCars and other vehiclesBoats and planesIntellectual propertySecurities - Publicly tradedSecurities - Closely held stockSecurities - Partnership, LLC,or trust interestsSecurities - MiscellaneousQualified conservationcontribution - HistoricstructuresQualified conservationcontribution - OtherReal estate - ResidentialReal estate - CommercialReal estate - OtherCollectiblesFood inventoryDrugs and medical suppliesTaxidermyHistorical artifactsScientific specimensArcheological artifacts
OtherOtherOtherOther
((((
))))
29 Number of Forms 8283 received by the organization during the tax year for contributions forwhich the organization completed Form 8283, Part IV, Donee Acknowledgement 29
Yes No30
31
32
33
a
b
a
b
During the year, did the organization receive by contribution any property reported in Part I, lines 1-28 thatit must hold for at least three years from the date of the initial contribution, and which is not required to beused for exempt purposes for the entire holding period? 30a If "Yes," describe the arrangement in Part II.Does the organization have a gift acceptance policy that requires the review of any non-standardcontributions? 31 Does the organization hire or use third parties or related organizations to solicit, process, or sell noncashcontributions? 32a If "Yes," describe in Part II.If the organization did not report an amount in column (c) for a type of property for which column (a) is checked,describe in Part II.
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Schedule M (Form 990) (2011)
JSA
1E1298 1.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
X 20. 30,072. FMV
FLOWERS/DECOR X 1. 565. FMV
X
X
X
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 37

Schedule M (Form 990) (2011) Page 2Supplemental Information. Complete this part to provide the information required by Part I, lines 30b, 32b,and 33. Also complete this part for any additional information.
Part II
Schedule M (Form 990) (2011)JSA
1E1508 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
NUMBER OF CONTRIBUTIONS
SCHEDULE M, PART I, COLUMN B
THE NUMBER IN COLUMN B REPRESENTS THE NUMBER OF CONTRIBUTIONS DURING THE
YEAR.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 38

Supplemental Information to Form 990 or 990-EZ OMB No. 1545-0047SCHEDULE O(Form 990 or 990-EZ)
Complete to provide information for responses to specific questions onForm 990 or 990-EZ or to provide any additional information.
Attach to Form 990 or 990-EZ.
Open to PublicInspection
Department of the TreasuryInternal Revenue Service Name of the organization Employer identification number
For Privacy Act and Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ. Schedule O (Form 990 or 990-EZ) (2011)JSA
1E1227 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
SIGNIFICANT NEW PROGRAM SERVICES
FORM 990, PART III, LINE 2
THE CHAPTER WAS FORMED ON OCTOBER 1, 2011, AS THE RESULT OF A MERGER
BETWEEN TWO EXISTING NATIONAL MULTIPLE SCLEROSIS CHAPTERS: NEBRASKA
CHAPTER AND MID AMERICA CHAPTER. BOTH OF THESE ENTITIES SHARED THE COMMON
MISSION OF PROVIDING SERVICES TO PEOPLE WITH MULTIPLE SCLEROSIS, SUPPORT
MULTIPLE SCLEROSIS RESEARCH THROUGH ITS NATIONAL ORGANIZATION AND EDUCATE
THE PUBLIC ABOUT THE IMPACT OF MULTIPLE SCLEROSIS.
PROGRAM SERVICE ACCOMPLISHMENTS
FORM 990, PART III, LINE 4D
COMMUNITY PROGRAMS - INCLUDES NETWORKING AND COLLABORATING WITH OTHER
COMMUNITY ORGANIZATIONS THAT CAN AND DO HAVE AN IMPACT ON THOSE AFFECTED
BY MULTIPLE SCLEROSIS, INCLUDING PROGRAMS DESIGNED TO DETECT DISEASE OR
HEALTH PROBLEMS, PLANNING AND IMPROVING COMMUNITY HEALTH PRACTICES,
SUPPORTING CLINICS OR OTHER PUBLIC HEALTH FACILITIES, CONDUCTING
REHABILITATIVE AND SIMILAR-TYPE PROGRAMS, PLUS ALL OTHER EXPENSES
INCURRED IN PERFORMING FUNCTIONS WHICH, DIRECTLY OR INDIRECTLY, BENEFIT
THE MULTIPLE SCLEROSIS COMMUNITY. TOTAL EXPENSES: $605,813.
PUBLIC EDUCATION - REPRESENTS PROGRAMS CONDUCTED FOR THE PURPOSE OF
INFORMING AND EDUCATING THE GENERAL PUBLIC ABOUT MULTIPLE SCLEROSIS AND
ITS EFFECTS, THE DISTRIBUTION OF LITERATURE AND OTHER MATERIALS DESIGNED
TO INCREASE THE PUBLIC'S AWARENESS AND KNOWLEDGE ABOUT THIS DISEASE,
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 39

Schedule O (Form 990 or 990-EZ) 2011 Page 2Name of the organization Employer identification number
Schedule O (Form 990 or 990-EZ) 2011JSA
1E1228 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
INCLUDING COMPLEXITY AND VARIETY OF SYMPTOMS OR PHYSICAL CONDITIONS, PLUS
ALL OTHER COSTS OR EXPENSES WHICH DIRECTLY RELATE TO THE PERFORMANCE OF
HEALTH EDUCATIONAL SERVICE. TOTAL EXPENSES: $334,970.
PROFESSIONAL EDUCATION AND TRAINING REPRESENTS ACTIVITIES OR PROGRAMS
DESIGNED TO IMPROVE THE KNOWLEDGE, SKILLS AND CRITICAL JUDGMENT OF
PHYSICIANS AND OTHER HEALTHCARE PROFESSIONALS ENGAGED (DIRECTLY OR
INDIRECTLY) IN PROVIDING CLIENT SERVICES BY KEEPING THEM ABREAST OF NEW
DIAGNOSTIC TECHNIQUES, THERAPIES, ETC. TOTAL EXPENSES: $109,433.
SIGNIFICANT CHANGES TO ORGANIZATIONAL DOCUMENTS
FORM 990, PART VI, SECTION A, LINE 4
ON OCTOBER 1, 2011, THE FORMER NEBRASKA CHAPTER REALIGNED AND MERGED WITH
THE MID-AMERICA CHAPTER. ORGANIZATIONAL DOCUMENTS AND BY-LAWS WERE
REVISED ACCORDINGLY TO REFLECT THE REALIGNMENT.
FORM 990 REVIEW PROCESS
FORM 990, PART VI, SECTION B, LINE 11B
AN INDEPENDENT ACCOUNTING FIRM PREPARES AND REVIEWS THE 990. THE 990 IS
THEN REVIEWED BY THE CHAPTER'S OFFICERS WITH ANY CORRECTIONS OR
CLARIFICATIONS BEING ADDRESSED PRIOR TO THE AUDIT COMMITTEE REVIEW. THE
CHAPTER'S AUDIT COMMITTEE REVIEWS AND APPROVES THE FORM 990 PRIOR TO
DISTRIBUTION TO THE ENTIRE BOARD. A COPY OF THE 990 FORM AND ACCOMPANYING
SCHEDULES IS PROVIDED TO THE ENTIRE BOARD WITH A PERIOD FOR PROVIDING
COMMENTS, EDITS OR CORRECTIONS PRIOR TO SUBMISSION TO THE IRS.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 40

Schedule O (Form 990 or 990-EZ) 2011 Page 2Name of the organization Employer identification number
Schedule O (Form 990 or 990-EZ) 2011JSA
1E1228 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
CONFLICT OF INTEREST POLICY
FORM 990, PART VI, SECTION B, LINE 12C
ON AN ANNUAL BASIS, THE AUDIT COMITTEE REVIEWS THE CODE OF CONDUCT FORMS
FILED BY DIRECTORS, OFFICERS AND EMPLOYEES FOR POTENTIAL CONFLICTS. WHERE
POTENTIAL CONFLICTS EXIST, THE DIRECTOR, OFFICER OR EMPLOYEE IS NOT
ALLOWED TO PARTICIPATE IN ANY VOTE AND TRANSACTIONS ARE SUBJECT TO
COMPETITIVE BIDDING. AT THE CURRENT TIME, NO POTENTIAL CONFLICTS OF
INTEREST HAVE BEEN IDENTIFIED.
COMPENSATION REVIEW
FORM 990, PART VI, SECTION B, LINES 15A & B
THE COMPENSATION COMMITTEE WHICH IS COMPRISED OF AT LEAST THREE BUT NO
MORE THAN FIVE INDEPENDENT DIRECTORS DETERMINES THE COMPENSATION OF THE
PRESIDENT AND OTHER KEY EMPLOYEES. THE NATIONAL ORGANIZATION PROVIDES
EACH CHAPTER WITH COMPARABLE SALARY DATA FOR PRESIDENTS AT NATIONAL
MULTIPLE SCLEROSIS SOCIETY CHAPTERS AND OTHER VOLUNTARY HEALTH AGENCIES
OF SIMILAR BUDGET SIZE(S) AND GEOGRAPHICAL LOCATION(S). IN ADDITION, THE
PRESIDENT'S PERFORMANCE IS EVALUATED ANNUALLY IN A JOINT REVIEW PROCESS
BY THE NATIONAL ORGANIZATION'S CEO OR HER DESIGNEE AND THE LOCAL
COMMITTEE OF INDEPENDENT DIRECTORS. THE PRESIDENT CONDUCTS PERFORMANCE
EVALUATIONS FOR THE OTHER KEY EMPLOYEES AND DETERMINES THEIR
COMPENSATION, WHICH IS SUBMITTED TO THE COMPENSATION COMMITTEE FOR
REVIEW.
AVAILABILITY OF DOCUMENTS
FORM 990, PART VI, SECTION C, LINE 19
THE CHAPTER'S GOVERNING DOCUMENTS AND CODE OF CONDUCT FORMS ARE AVAILABLE
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 41

Schedule O (Form 990 or 990-EZ) 2011 Page 2Name of the organization Employer identification number
Schedule O (Form 990 or 990-EZ) 2011JSA
1E1228 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,MID-AMERICA CHAPTER 44-0613436
UPON REQUEST. THE CHAPTER'S FORM 990, AND FINANCIAL STATEMENTS ARE
AVAILABLE ON THE CHAPTER'S WEBSITE AND WILL ALSO BE PROVIDED IN A HARD
COPY FORMAT UPON REQUEST. THE BOOKS AND RECORDS OF THE ORGANIZATION ARE
LOCATED AT THE NATIONAL MULTIPLE SCLEROSIS SOCIETY, MID-AMERICA CHAPTER,
7611 STATE LINE ROAD SUITE 100, KANSAS CITY, MO 64114. 913-432-3926
OTHER CHANGES IN NET ASSETS
FORM 990, PART XI, LINE 5
NEBRASKA CHAPTER MERGER $108,106
CHANGE IN OVERSIGHT PROCESS
FORM 990, PART XII, LINE 2C
THE MID-AMERICA CHAPTER SELECTED NEW AUDITORS FOR FISCAL YEAR 2012.
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 42

OM
BN
o.15
45-0
047
SCHE
DU
LER
(For
m99
0)Re
late
dO
rgan
izat
ions
and
Unr
elat
edPa
rtne
rshi
ps
Com
plet
eif
the
orga
niza
tion
answ
ered
"Yes
"to
Form
990,
Part
IV,l
ine
33,3
4,35
,36,
or37
.D
epar
tmen
toft
heTr
easu
ryIn
tern
alR
even
ueS
ervi
ce
Ope
nto
Publ
icIn
spec
tion
Att
ach
toFo
rm99
0.S
eese
para
tein
stru
ctio
ns.
Nam
eof
the
orga
niza
tion
Empl
oyer
iden
tific
atio
nnu
mbe
r
Iden
tific
atio
nof
Dis
rega
rded
Entit
ies
(Com
plet
eif
the
orga
niza
tion
answ
ered
"Yes
"to
Form
990,
Part
IV,l
ine
33.)
Par
tI(a
)N
ame,
addr
ess,
and
EIN
ofdi
sreg
arde
den
tity
(b)
Prim
ary
activ
ity(c
)Le
gald
omic
ile(s
tate
orfo
reig
nco
untry
)
(d)
Tota
linc
ome
(e)
End-
of-y
eara
sset
s(f)
Dire
ctco
ntro
lling
entit
y
(1)
(2)
(3)
(4)
(5)
(6)
Iden
tific
atio
nof
Rel
ated
Tax-
Exem
ptO
rgan
izat
ions
(Com
plet
eif
the
orga
niza
tion
answ
ered
"Yes
"to
Form
990,
Part
IV,l
ine
34be
caus
eit
had
one
orm
ore
rela
ted
tax-
exem
ptor
gani
zatio
nsdu
ring
the
tax
year
.)P
artI
I
(a)
Nam
e,ad
dres
s,an
dE
INof
rela
ted
orga
niza
tion
(b)
Prim
ary
activ
ity(c
)Le
gald
omic
ile(s
tate
orfo
reig
nco
untry
)
(d)
Exe
mpt
Cod
ese
ctio
n
(e)
Pub
licch
arity
stat
us(if
sect
ion
501(
c)(3
))
(f)D
irect
cont
rollin
gen
tity
(g)
Sec
tion
512(
b)(1
3)co
ntro
lled
entit
y?
Yes
No
(1)
(2)
(3)
(4)
(5)
(6)
(7)
For
Pape
rwor
kR
educ
tion
ActN
otic
e,se
eth
eIn
stru
ctio
nsfo
rFor
m99
0.S
ched
ule
R(F
orm
990)
2011
JSA
1E13
071.
000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,
44-0613436
NATIONAL MULTIPLE SCLEROSIS SOCIETY,
MID-AMERICA CHAPTER
44-0613436
NATIONAL MULTIPLE SCLEROSIS SOCIETY
13-5661935
733 THIRD AVENUE
NEW YORK, NY 10017
NATL. ORG
NY
501(C)(3)
07
N/A
X
8051EP K922
2/7/2013
1:26:37 PM
V 11-6.4
PAGE 43

Sch
edul
eR
(For
m99
0)20
11Pa
ge2
Iden
tific
atio
nof
Rel
ated
Org
aniz
atio
nsTa
xabl
eas
aPa
rtne
rshi
p(C
ompl
ete
ifth
eor
gani
zatio
nan
swer
ed"Y
es"t
oFo
rm99
0,Pa
rtIV
,lin
e34
beca
use
itha
don
eor
mor
ere
late
dor
gani
zatio
nstre
ated
asa
partn
ersh
ipdu
ring
the
tax
year
.)Pa
rtIII
(a)
Nam
e,ad
dres
s,an
dE
INof
rela
ted
orga
niza
tion
(b)
Prim
ary
activ
ity(c
)Le
gal
dom
icile
(sta
teor
fore
ign
coun
try)
(d)
Dire
ctco
ntro
lling
entit
y
(e)
Pre
dom
inan
tin
com
e(re
late
d,un
rela
ted,
excl
uded
from
tax
unde
rse
ctio
ns51
2-51
4)
(f)S
hare
ofto
tal
inco
me
(g)
Sha
reof
end-
of-y
ear
asse
ts
(h)
Dis
prop
ortio
nate
allo
catio
ns?
(i)C
ode
V-U
BI
amou
ntin
box
20of
Sche
dule
K-1
(For
m10
65)
(j)G
ener
alor
man
agin
gpa
rtner
?
(k)
Per
cent
age
owne
rshi
p
Yes
No
Yes
No
(1)
(2)
(3)
(4)
(5)
(6)
(7)
Iden
tific
atio
nof
Rel
ated
Org
aniz
atio
nsTa
xabl
eas
aC
orpo
ratio
nor
Trus
t(C
ompl
ete
ifth
eor
gani
zatio
nan
swer
ed"Y
es"t
oFo
rm99
0,Pa
rtIV
,lin
e34
beca
use
itha
don
eor
mor
ere
late
dor
gani
zatio
nstre
ated
asa
corp
orat
ion
ortru
stdu
ring
the
tax
year
.)Pa
rtIV
(a)
Nam
e,ad
dres
s,an
dE
INof
rela
ted
orga
niza
tion
(b)
Prim
ary
activ
ity(c
)Le
gald
omic
ile(s
tate
orfo
reig
nco
untry
)
(d)
Dire
ctco
ntro
lling
entit
y
(e)
Type
ofen
tity
(Cco
rp,S
corp
,or
trust
)
(f)S
hare
ofto
tal
inco
me
(g)
Sha
reof
end-
of-y
eara
sset
s
(h)
Per
cent
age
owne
rshi
p
(1)
(2)
(3)
(4)
(5)
(6)
(7)
Sch
edul
eR
(For
m99
0)20
11JS
A
1E13
081.
000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,
44-0613436
8051EP K922
2/7/2013
1:26:37 PM
V 11-6.4
PAGE 44

Sch
edul
eR
(For
m99
0)20
11Pa
ge3
Tran
sact
ions
With
Rel
ated
Org
aniz
atio
ns(C
ompl
ete
ifth
eor
gani
zatio
nan
swer
ed"Y
es"t
oFo
rm99
0,Pa
rtIV
,lin
e34
,35,
35a,
or36
.)Pa
rtV
Yes
No
Not
e.C
ompl
ete
line
1if
any
entit
yis
liste
din
Par
tsII,
III,o
rIV
ofth
issc
hedu
le.
1D
urin
gth
eta
xye
ar,d
idth
eor
gani
zatio
nen
gage
inan
yof
the
follo
win
gtr
ansa
ctio
nsw
ithon
eor
mor
ere
late
dor
gani
zatio
nslis
ted
inP
arts
II–IV
?R
ecei
ptof
(i)in
tere
st(ii
)ann
uitie
s(ii
i)ro
yalti
esor
(iv)r
entf
rom
aco
ntro
lled
entit
yG
ift,g
rant
,or
capi
talc
ontr
ibut
ion
tore
late
dor
gani
zatio
n(s)
Gift
,gra
nt,o
rca
pita
lcon
trib
utio
nfr
omre
late
dor
gani
zatio
n(s)
Loan
sor
loan
guar
ante
esto
orfo
rrel
ated
orga
niza
tion(
s)Lo
ans
orlo
angu
aran
tees
byre
late
dor
gani
zatio
n(s)
Sal
eof
asse
tsto
rela
ted
orga
niza
tion(
s)P
urch
ase
ofas
sets
from
rela
ted
orga
niza
tion(
s)E
xcha
nge
ofas
sets
with
rela
ted
orga
niza
tion(
s)Le
ase
offa
cilit
ies,
equi
pmen
t,or
othe
rass
ets
tore
late
dor
gani
zatio
n(s)
Leas
eof
faci
litie
s,eq
uipm
ent,
orot
her
asse
tsfro
mre
late
dor
gani
zatio
n(s)
Per
form
ance
ofse
rvic
esor
mem
bers
hip
orfu
ndra
isin
gso
licita
tions
forr
elat
edor
gani
zatio
n(s)
Per
form
ance
ofse
rvic
esor
mem
bers
hip
orfu
ndra
isin
gso
licita
tions
byre
late
dor
gani
zatio
n(s)
Sha
ring
offa
cilit
ies,
equi
pmen
t,m
ailin
glis
ts,o
rot
her
asse
tsw
ithre
late
dor
gani
zatio
n(s)
Sha
ring
ofpa
idem
ploy
ees
with
rela
ted
orga
niza
tion(
s)
Rei
mbu
rsem
entp
aid
tore
late
dor
gani
zatio
n(s)
fore
xpen
ses
Rei
mbu
rsem
entp
aid
byre
late
dor
gani
zatio
n(s)
fore
xpen
ses
Oth
ertr
ansf
erof
cash
orpr
oper
tyto
rela
ted
orga
niza
tion(
s)O
ther
tran
sfer
ofca
shor
prop
erty
from
rela
ted
orga
niza
tion(
s)
a b c d e f g h i j k l m n o p q r
1a 1b 1c 1d 1e 1f 1g 1h 1i 1j 1k 1l 1m 1n 1o 1p 1q 1r
2
Ifth
ean
swer
toan
yof
the
abov
eis
"Yes
,"se
eth
ein
stru
ctio
nsfo
rin
form
atio
non
who
mus
tcom
plet
eth
islin
e,in
clud
ing
cove
red
rela
tions
hips
and
trans
actio
nth
resh
olds
.(a
)N
ame
ofot
hero
rgan
izat
ion
(b)
Tran
sact
ion
type
(a–r
)
(c)
Am
ount
invo
lved
(d)
Met
hod
ofde
term
inin
gam
ount
invo
lved
(1)
(2)
(3)
(4)
(5)
(6)
Sch
edul
eR
(For
m99
0)20
11JS
A
1E13
091.
000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,
44-0613436
X X X X X X X X X X X X X X X X X X
8051EP K922
2/7/2013
1:26:37 PM
V 11-6.4
PAGE 45
Sch
edul
eR
(For
m99
0)20
11Pa
ge4
Unr
elat
edO
rgan
izat
ions
Taxa
ble
asa
Part
ners
hip
(Com
plet
eif
the
orga
niza
tion
answ
ered
"Yes
"on
Form
990,
Part
IV,l
ine
37.)
Par
tVI
Pro
vide
the
follo
win
gin
form
atio
nfo
rea
chen
tity
taxe
das
apa
rtne
rshi
pth
roug
hw
hich
the
orga
niza
tion
cond
ucte
dm
ore
than
five
perc
ent
ofits
activ
ities
(mea
sure
dby
tota
lass
ets
orgr
oss
reve
nue)
that
was
nota
rela
ted
orga
niza
tion.
See
inst
ruct
ions
rega
rdin
gex
clus
ion
forc
erta
inin
vest
men
tpar
tner
ship
s.(b
)P
rimar
yac
tivity
(a)
Nam
e,ad
dres
s,an
dE
INof
entit
y
(h)
Dis
prop
ortio
nate
allo
catio
ns?
(e)
Are
allp
artn
ers
sect
ion
501(
c)(3
)or
gani
zatio
ns?
(c)
Lega
ldom
icile
(sta
teor
fore
ign
coun
try)
(f)S
hare
ofto
tali
ncom
e
(g)
Sha
reof
end-
of-y
ear
asse
ts
(i)C
ode
V-U
BI
amou
ntin
box
20of
Sch
edul
eK
-1(F
orm
1065
)
(j)G
ener
alor
man
agin
gpa
rtner
?
(k)
Per
cent
age
owne
rshi
p
(d)
Pre
dom
inan
tin
com
e(r
elat
ed,
unre
late
d,ex
clud
edfr
omta
xun
der
sect
ion
512-
514)
Yes
No
Yes
No
Yes
No
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(12)
(13)
(14)
(15)
(16)
Sch
edul
eR
(For
m99
0)20
11
JSA
1E13
101.
000
NATIONAL MULTIPLE SCLEROSIS SOCIETY,
44-0613436
8051EP K922
2/7/2013
1:26:37 PM
V 11-6.4
PAGE 46

Schedule R (Form 990) 2011 Page 5Supplemental InformationComplete this part to provide additional information for responses to questions on Schedule R (seeinstructions).
Part VII
Schedule R (Form 990) 2011
1E1510 2.000
NATIONAL MULTIPLE SCLEROSIS SOCIETY, 44-0613436
8051EP K922 2/7/2013 1:26:37 PM V 11-6.4 PAGE 47