Embed Size (px)
Citation preview
FYS 4250Lecture 1
Welcome to FYS 4250
Today’s program
1. A short introduction to the course
2. Case 1
Introduction to FYS 4250• What is the main goal for FYS 4250?
– To give the students an overview of the basic concepts of biomedical instrumentation
Seemallorca.com
Introduction to FYS 4250• What should the student be capable of?
– Know the different medical technologies, describe the use, area of application and working principle, limitations, distinctive technological feature, strengths/weaknesses, sources of errors. Both alone and compared to other similar technologies
www.withfriendship.com
Introduction to FYS 4250• How shall we be able to reach our goals?
– 16 Patient cases, each introducing different aspects of medical technology
– 2 Repetitions of the main technologies– 1 Field trip to Oslo University Hospital– 2 Exams (Mid-term exam = 40% of your final grade, and the
final exam = 60% of your final grade)
Epicrapbattlesofthistory.wikia.com
Introduction to FYS 4250
• What about the practical issues?– We will use the “Medical Instrumentation, 4th
edition, John Webster”– We will use some offprints from other
sources– The time schedule will be published on the
homepage, any departure from this will be published in ”messages” at least 24h before the lecture
– Other practical issues will be delt with from the institute
Introduction to FYS 4250• Any other questions?
- Okay, let’s start. You’ll soon start to think as a biomedical engineer
Case 1
- 47 years old male, no chronic diseases, father died from cerebral haemorrage 63 years old. His mother is still alive, no diseases.
Case 1
• The patient comes to the emergency room complaining of severe shortness of breath and coughing, several episodes in the past lasting a day or two. He had an episode of rheumatic fever at age 14 years, denies any abuse of drugs or alcohol, no tobacco. On examination, heart rate is between 110 – 130 bpm, respiratory rate of 24 breaths per minute, with oxygen saturation of 92% oxygen. Coughing, producing frothy sputum with a pinkish tint. Bilateral inspiratory crackles can be heard in the lower lung fields.
- What is the most likely diagnosis?
Case 1
• Seems reasonable that the problems are related to the heart or the lungs. Typically an examination will start with the heart to exclude any possible life-threatening arrythmias
- What will you do now?
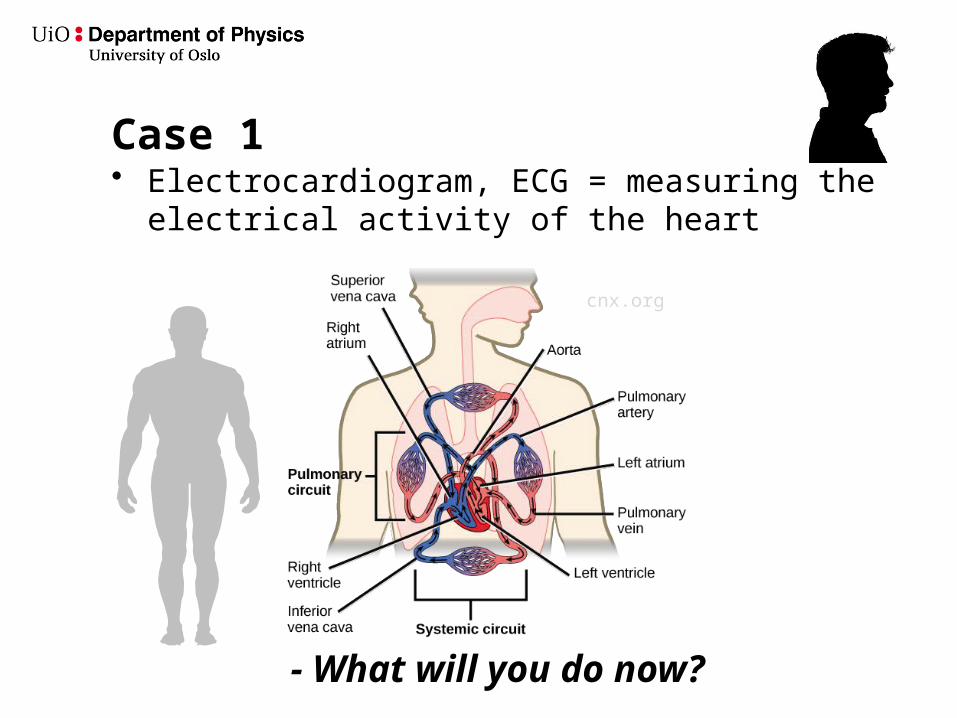
Case 1• Electrocardiogram, ECG = measuring the electrical
activity of the heart
- What will you do now?
cnx.org
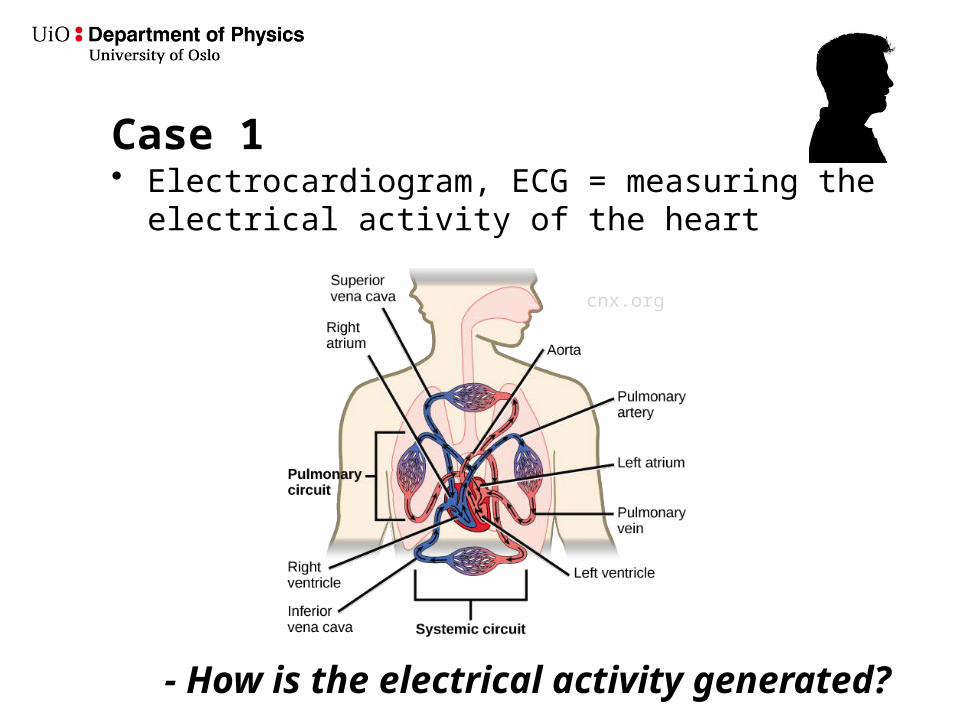
Case 1• Electrocardiogram, ECG = measuring the electrical
activity of the heart
- How is the electrical activity generated?
cnx.org
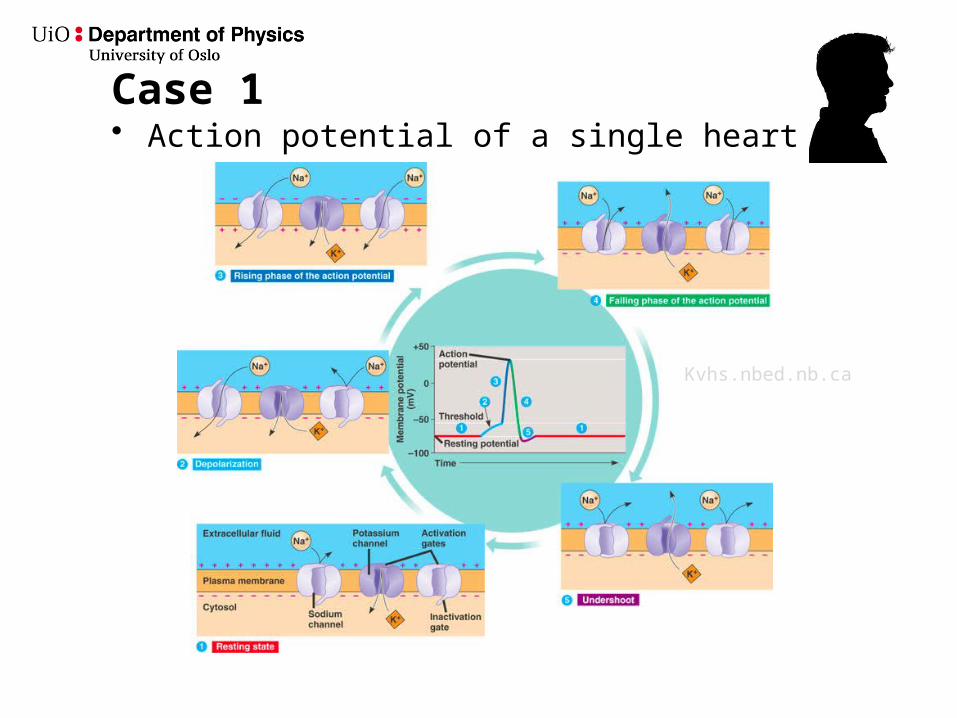
Case 1• Action potential of a single heart cell
Kvhs.nbed.nb.ca
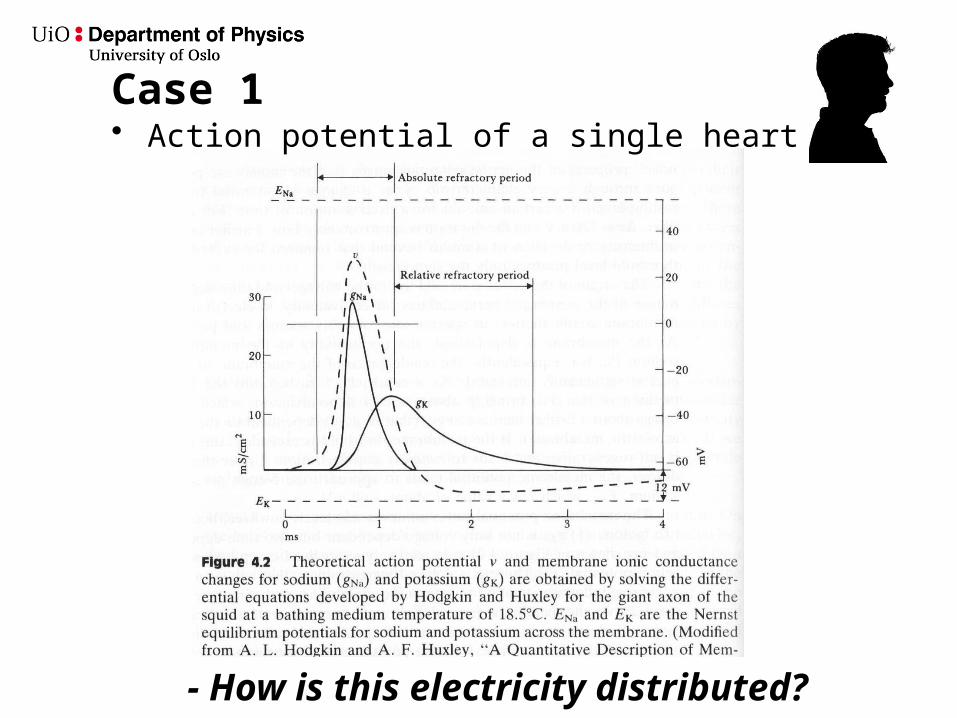
Case 1• Action potential of a single heart cell
- How is this electricity distributed?
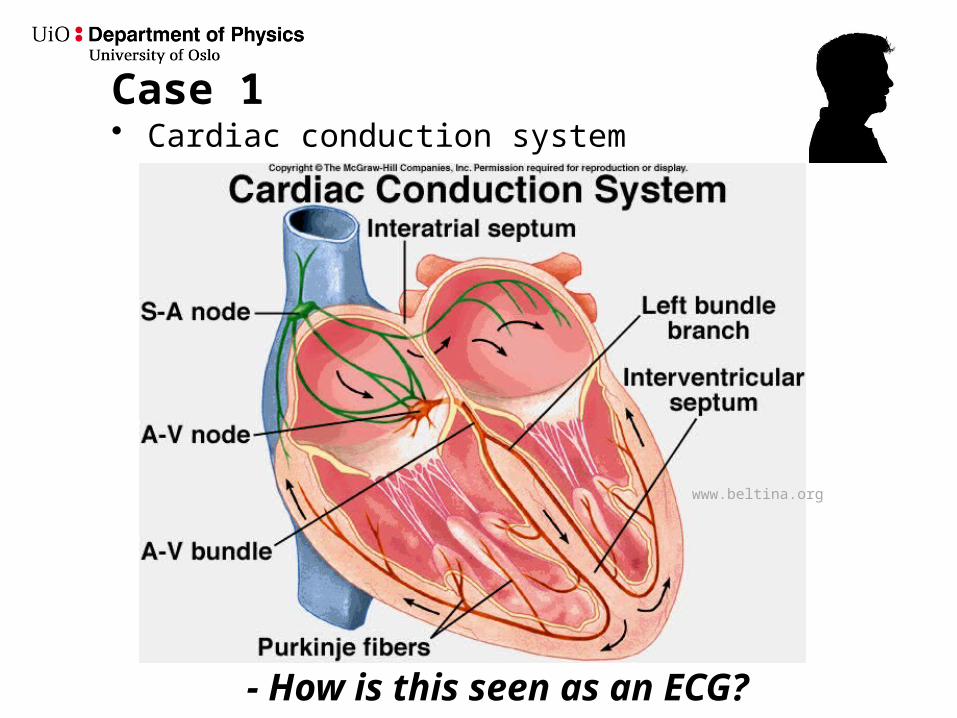
Case 1• Cardiac conduction system
- How is this seen as an ECG?
www.beltina.org
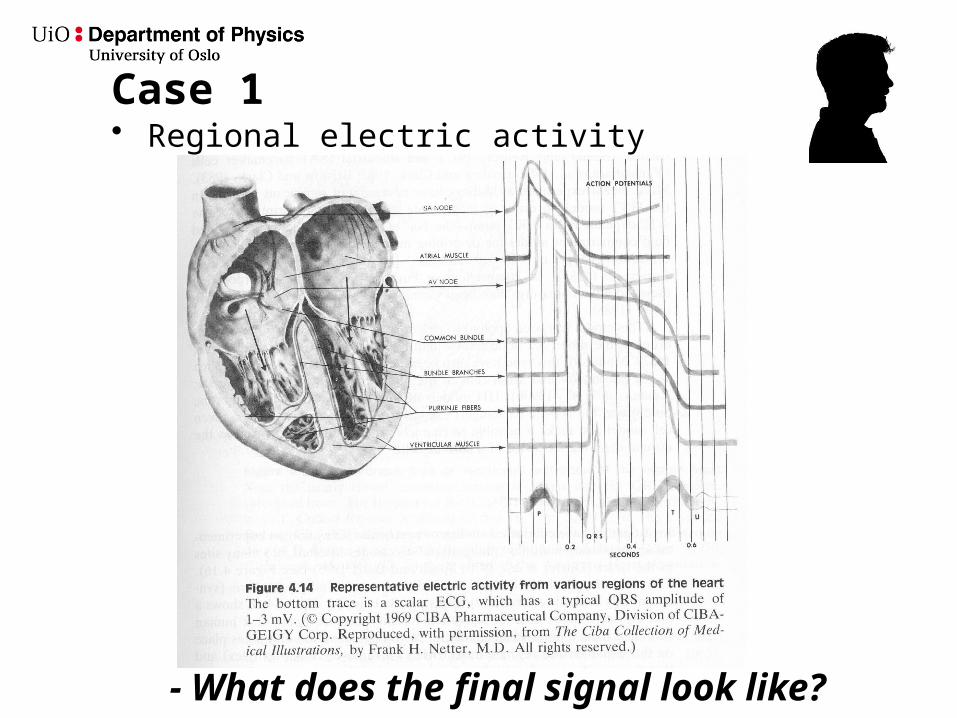
Case 1• Regional electric activity
- What does the final signal look like?
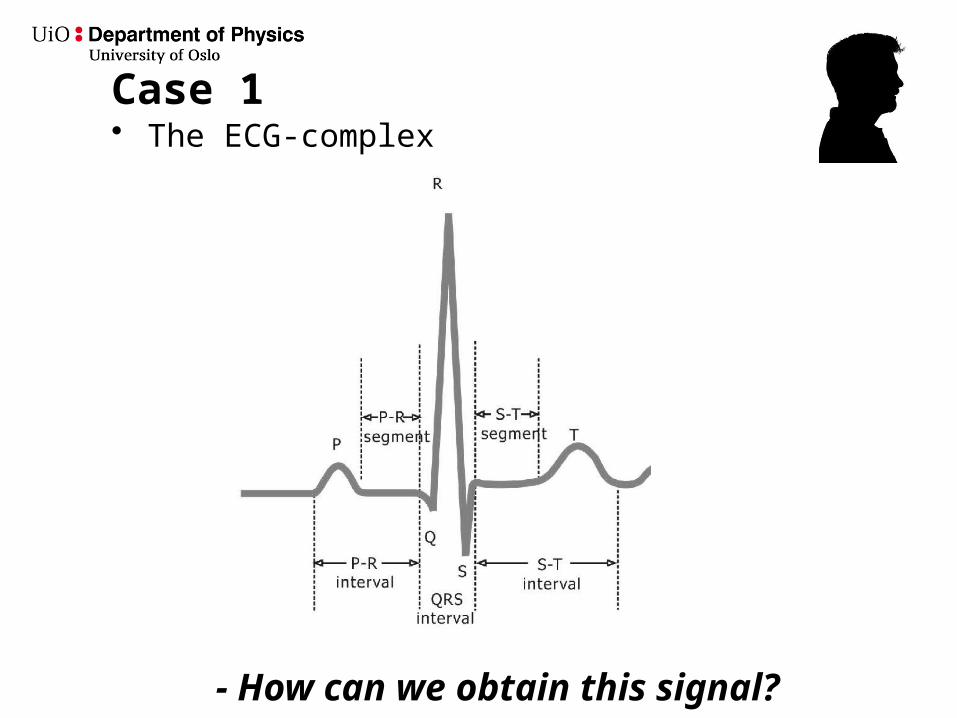
Case 1• The ECG-complex
- How can we obtain this signal?
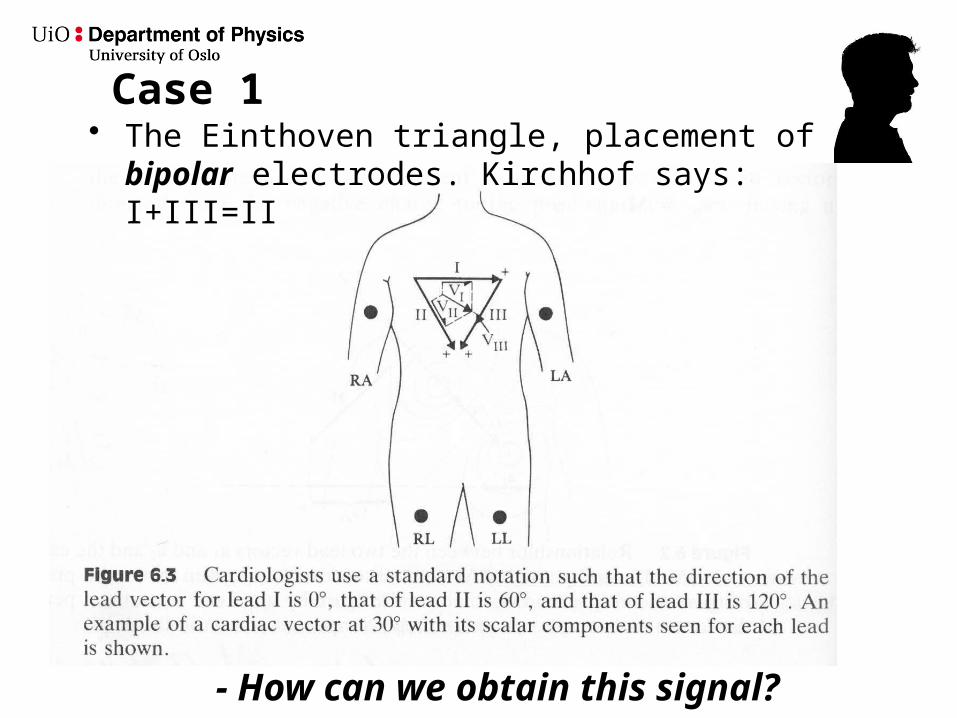
Case 1
- How can we obtain this signal?
• The Einthoven triangle, placement of bipolar electrodes. Kirchhof says: I+III=II
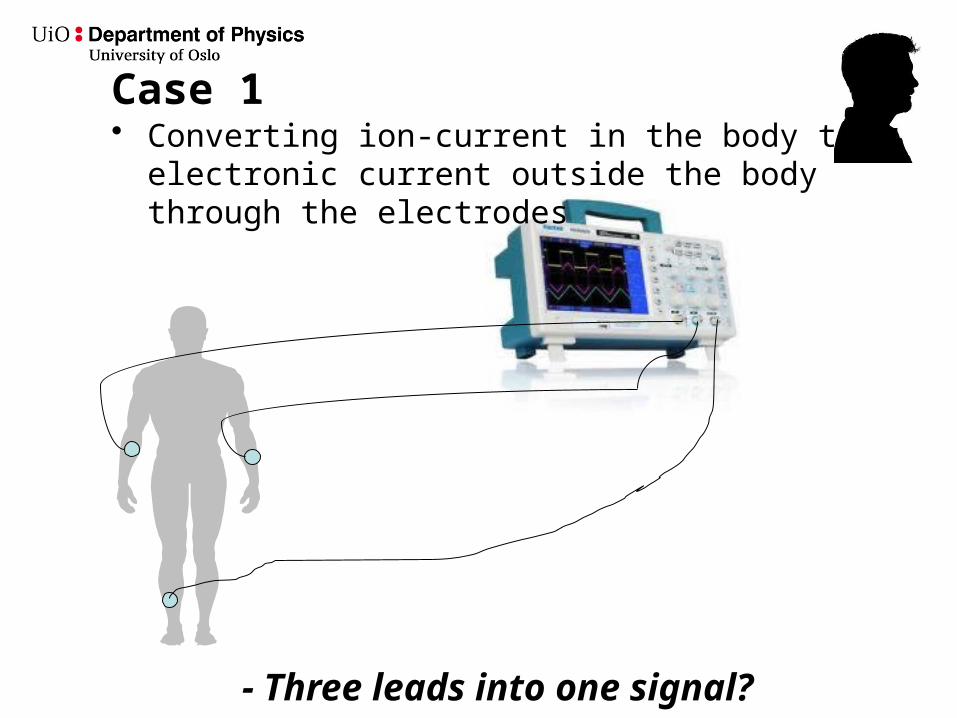
Case 1• Converting ion-current in the body to electronic
current outside the body through the electrodes
- Three leads into one signal?
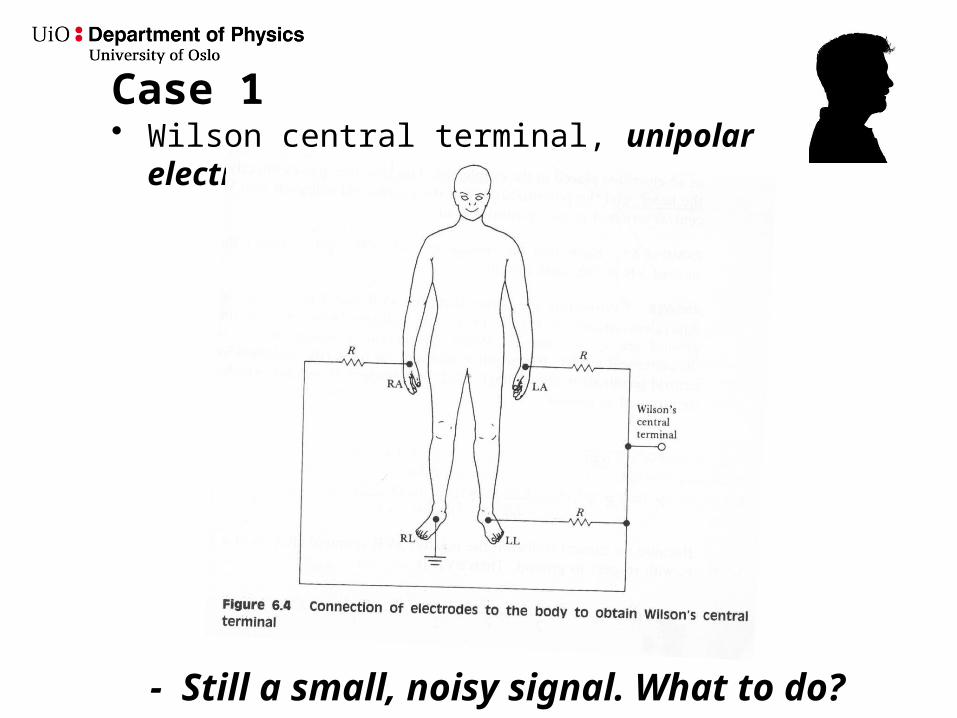
Case 1• Wilson central terminal, unipolar electrodes
- Still a small, noisy signal. What to do?
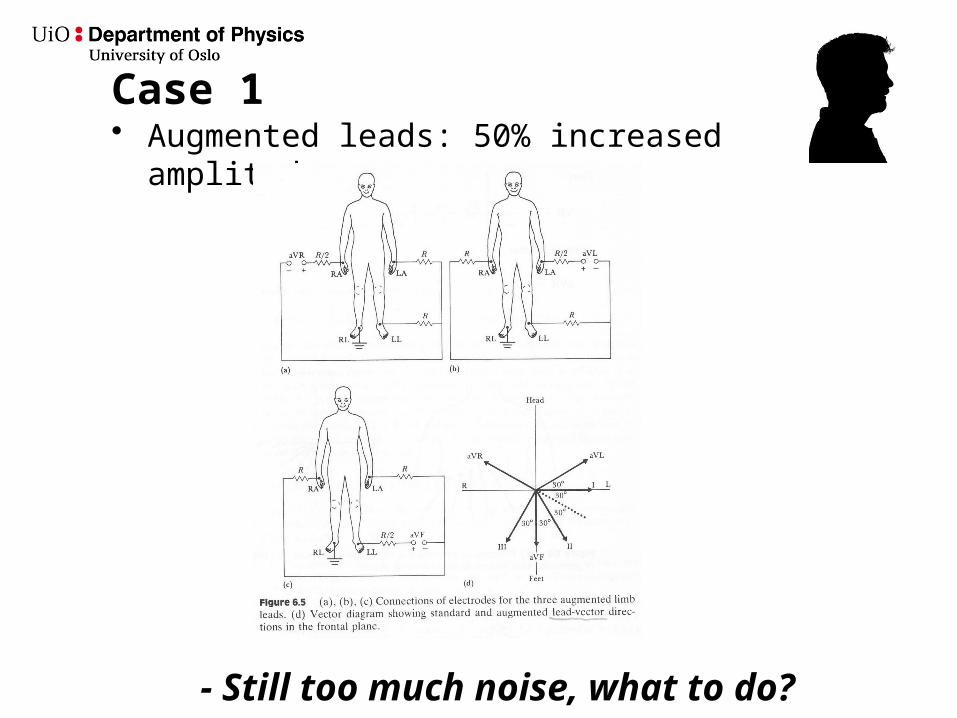
Case 1• Augmented leads: 50% increased amplitude
- Still too much noise, what to do?
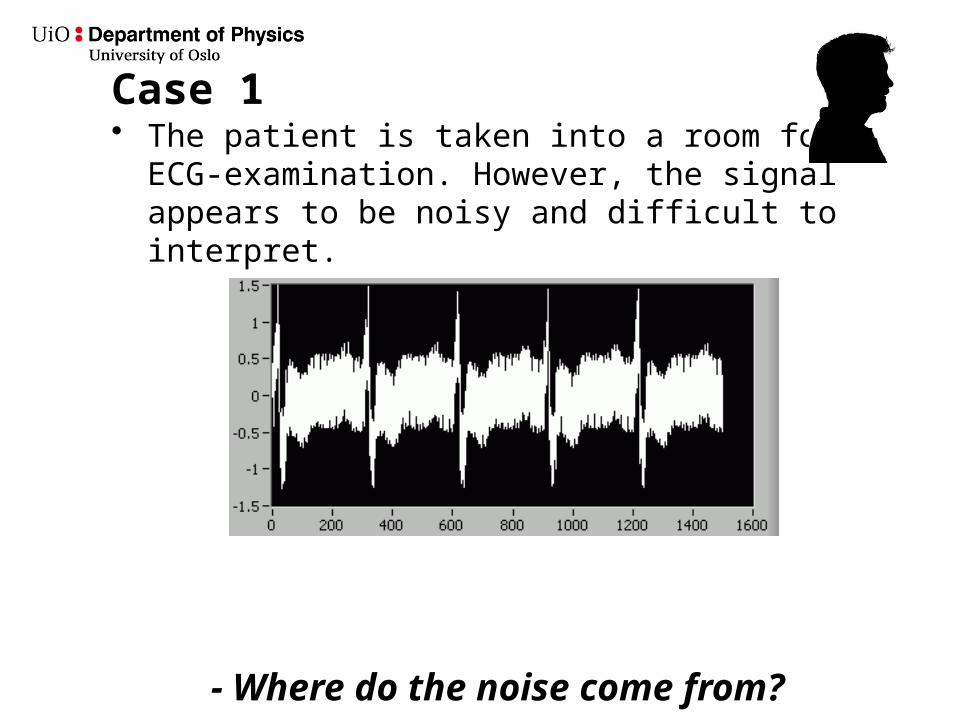
Case 1• The patient is taken into a room for ECG-
examination. However, the signal appears to be noisy and difficult to interpret.
- Where do the noise come from?
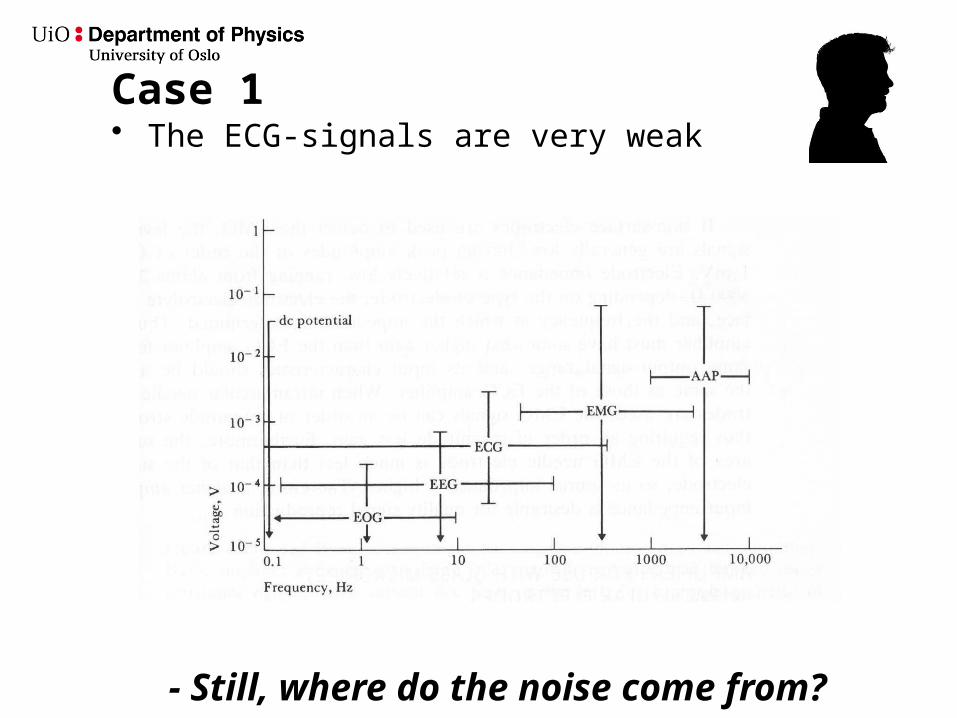
Case 1• The ECG-signals are very weak
- Still, where do the noise come from?
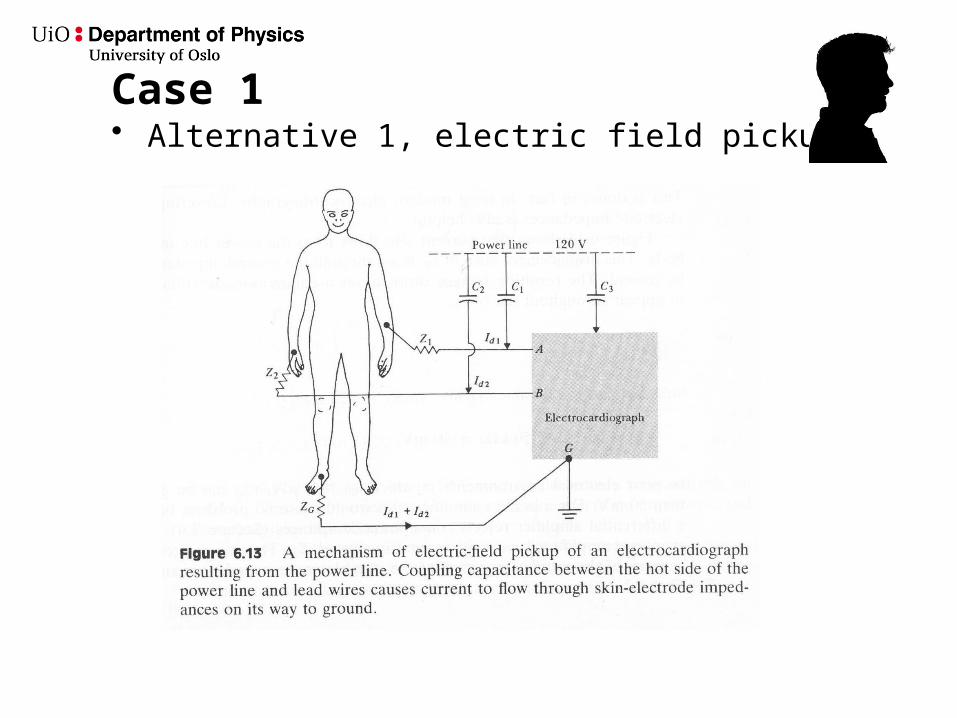
Case 1• Alternative 1, electric field pickup
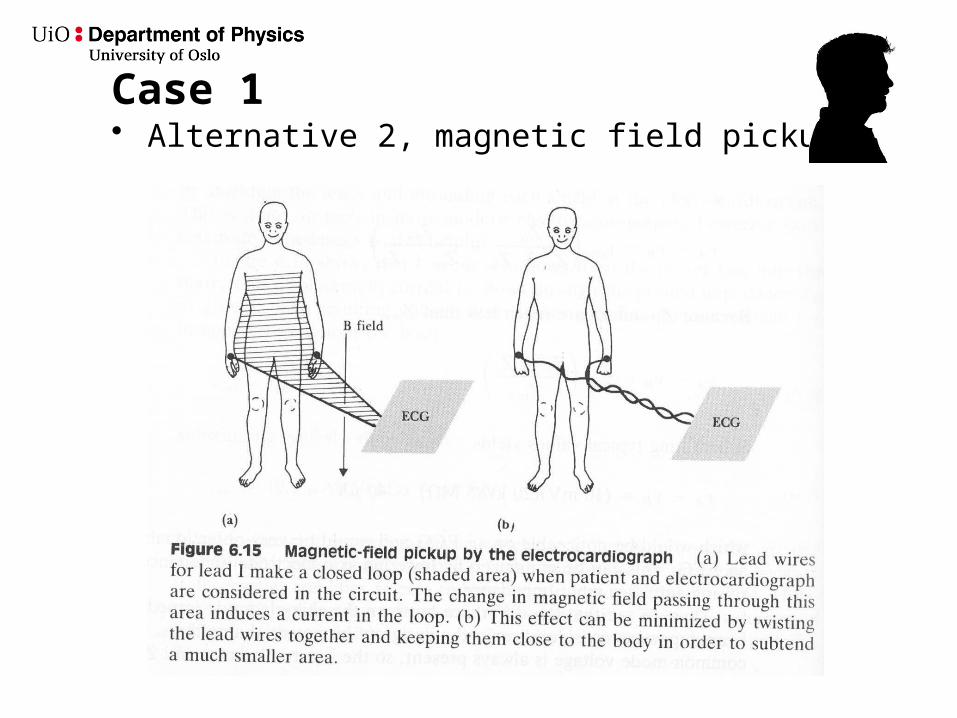
Case 1• Alternative 2, magnetic field pickup
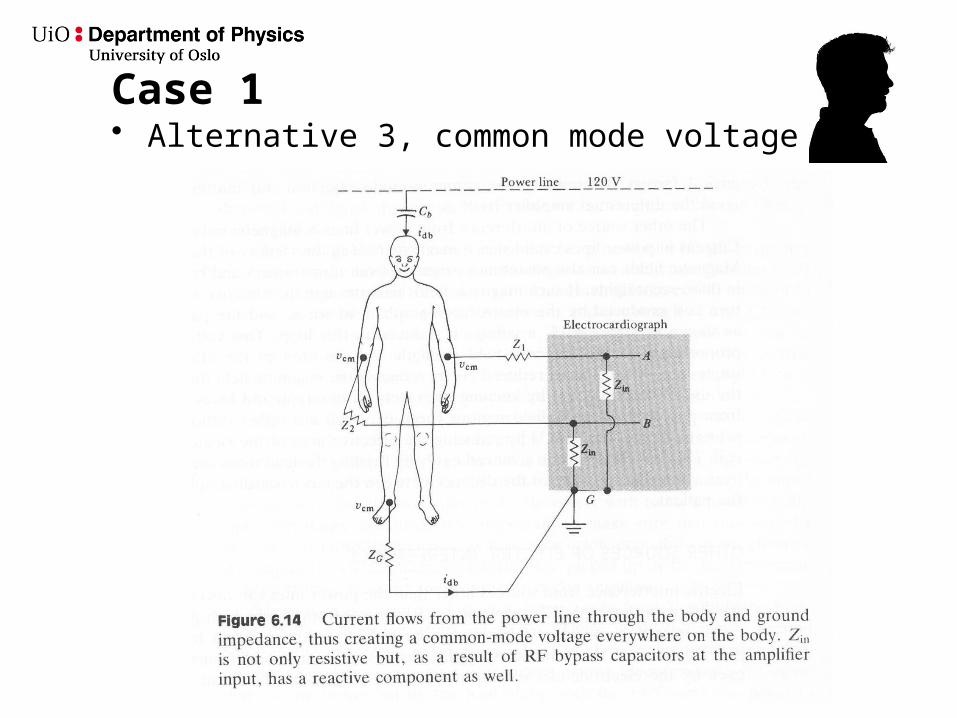
Case 1• Alternative 3, common mode voltage
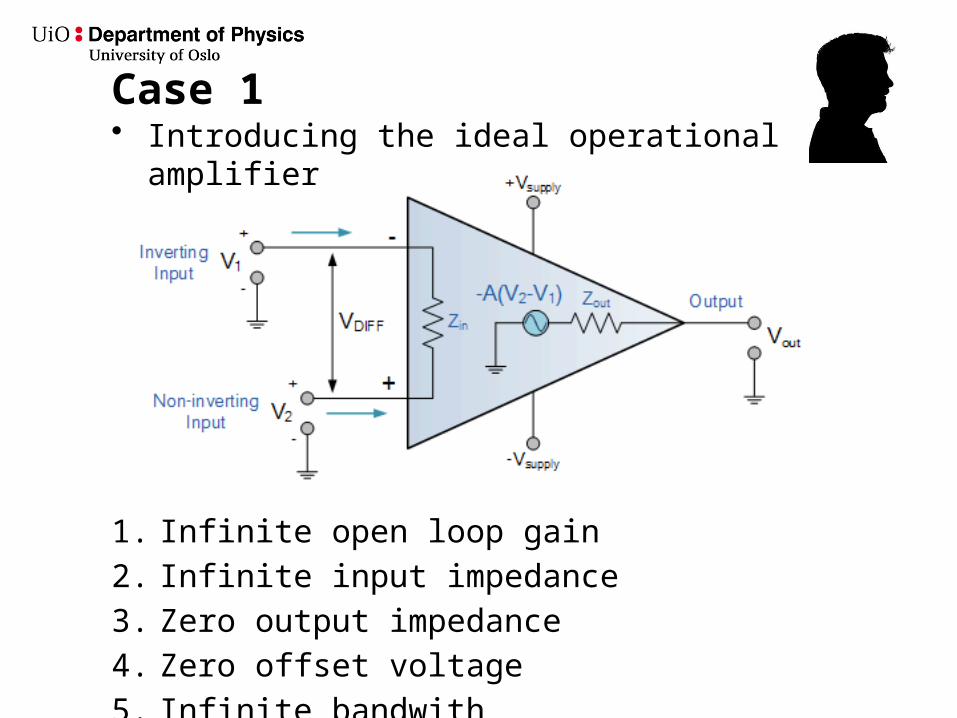
Case 1• Introducing the ideal operational amplifier
1. Infinite open loop gain
2. Infinite input impedance
3. Zero output impedance
4. Zero offset voltage
5. Infinite bandwith
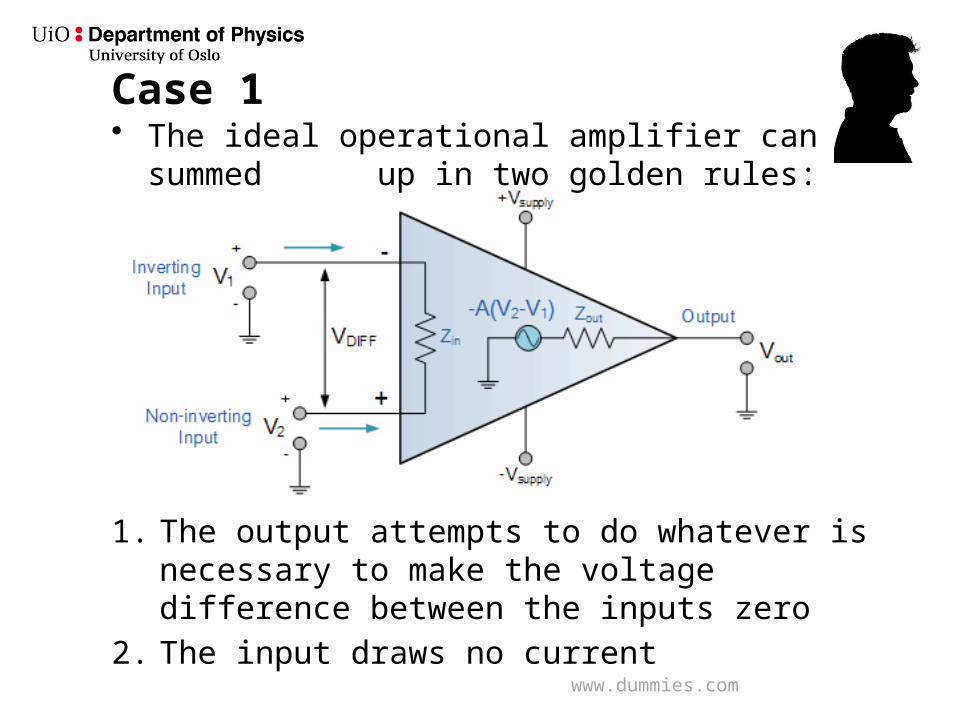
Case 1• The ideal operational amplifier can be summed up
in two golden rules:
1. The output attempts to do whatever is necessary to make the voltage difference between the inputs zero
2. The input draws no current
www.dummies.com
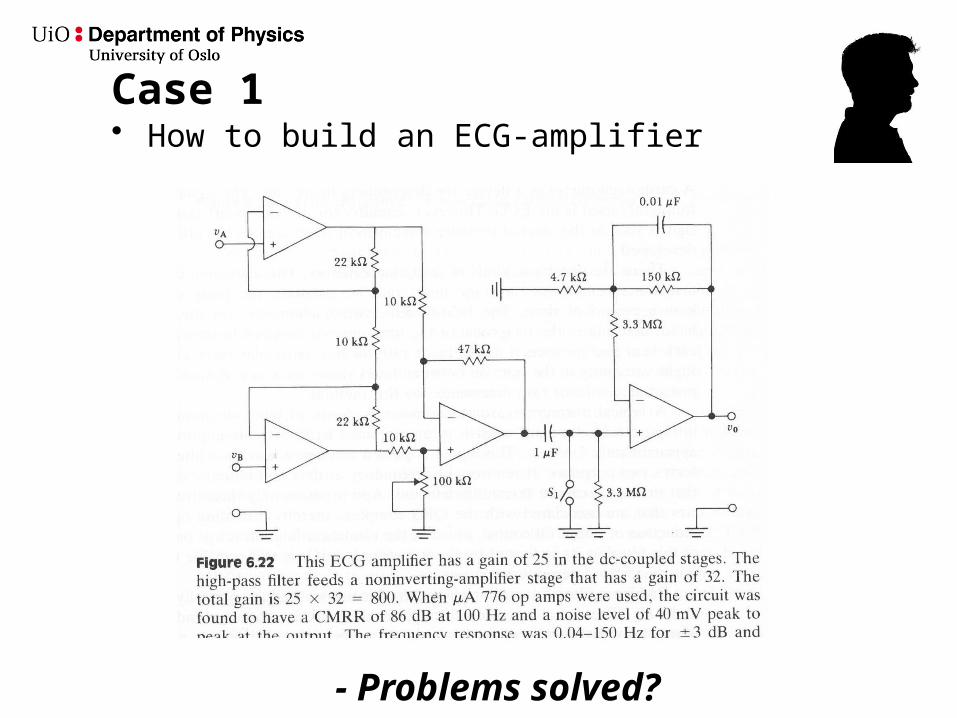
Case 1• How to build an ECG-amplifier
- Problems solved?
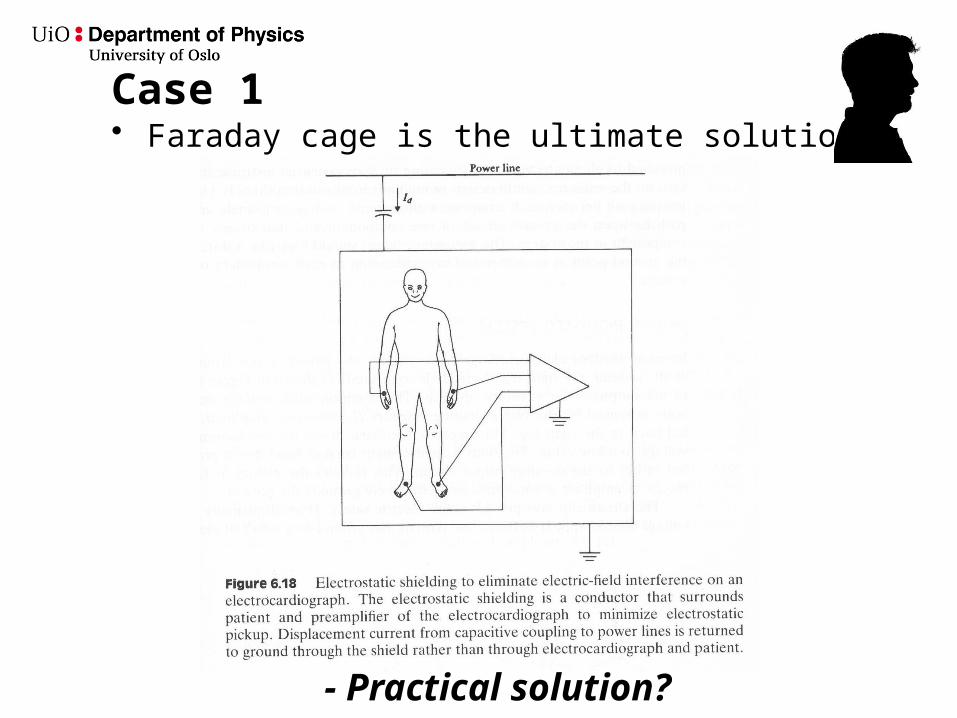
Case 1• Faraday cage is the ultimate solution
- Practical solution?
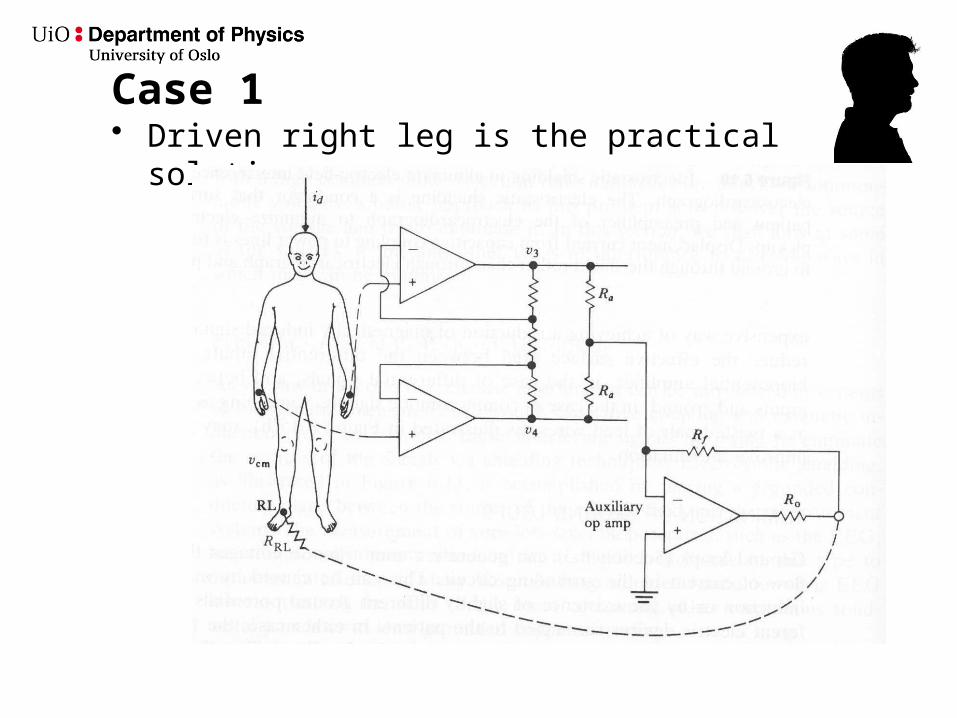
Case 1• Driven right leg is the practical solution
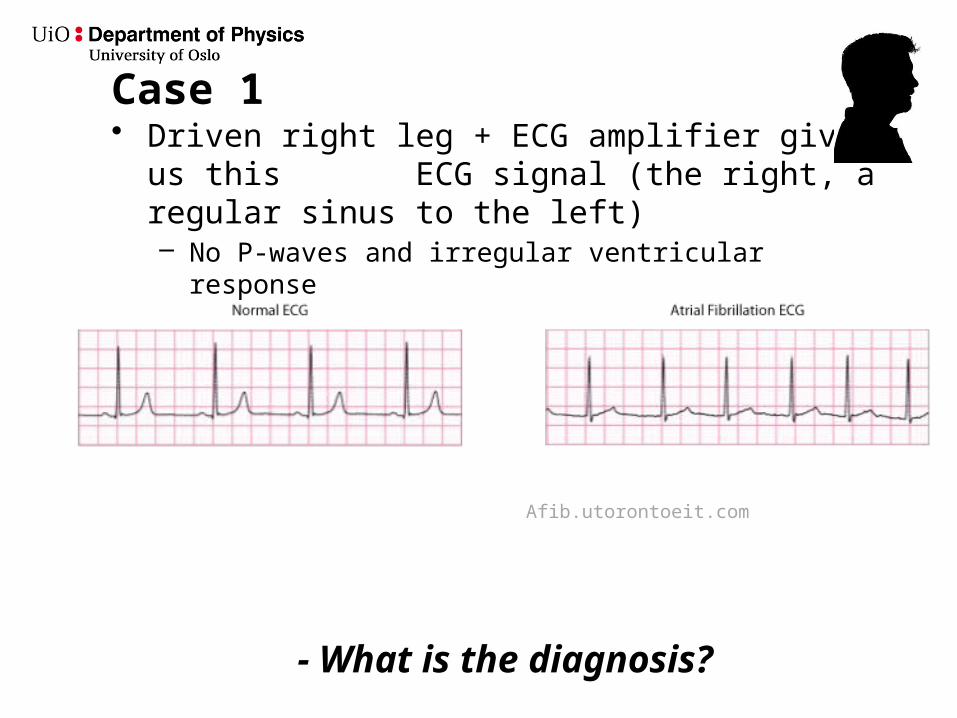
Case 1• Driven right leg + ECG amplifier gives us this
ECG signal (the right, a regular sinus to the left)– No P-waves and irregular ventricular response
Afib.utorontoeit.com
- What is the diagnosis?
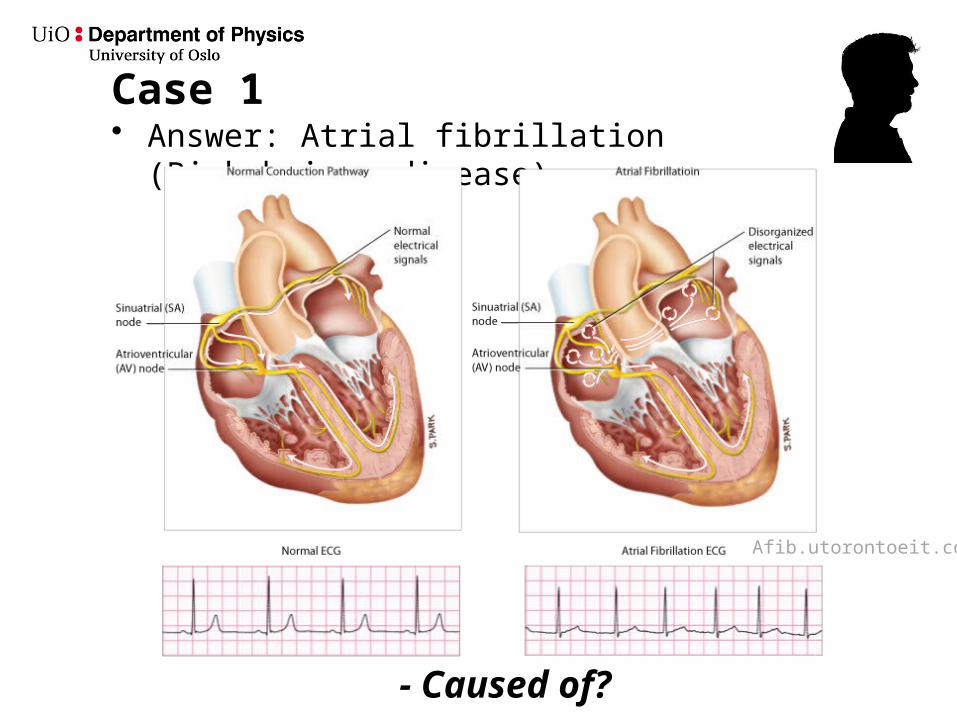
Case 1• Answer: Atrial fibrillation (Birkebeiner disease)
- Caused of?
Afib.utorontoeit.com
Case 1
• Answer: Because of the loss of atrial contraction, the atrial fibrillation has caused a pulmonary edema.
-This is most probably caused by rheumatic heart disease
- Atrial fibrillation have an increasing incidence with age, affecting 10% of patients older than 75 years of age
- Atrial depolarisation, often at rates exceeding 300-400 bpm
- The most common arrhythmia for which patients seek doctor
Toy, Patlan, Cruse, Faustinella, Case Files Internal medicine, McGrawhill
- Is it dangerous?
Case 1
• Answer: Yes– It may trigger a rapid ventricular rate leading to myocardial
ischemia or heart failure– Atrial fibrillation is a common cause of stroke, due to
thrombus formation in the noncontractile atria
The two most common causes are hypertension and coronary atherosclerosis
If patient is hemodynamically unstable, urgent cardioversion is indicated. Not all patients can be cardioverted, and the longer the fibrillation, the more likely the patient is to stay there because of electrical remodeling of the heart.
Toy, Patlan, Cruse, Faustinella, Case Files Internal medicine, McGrawhill
- What is rheumatic heart disease?
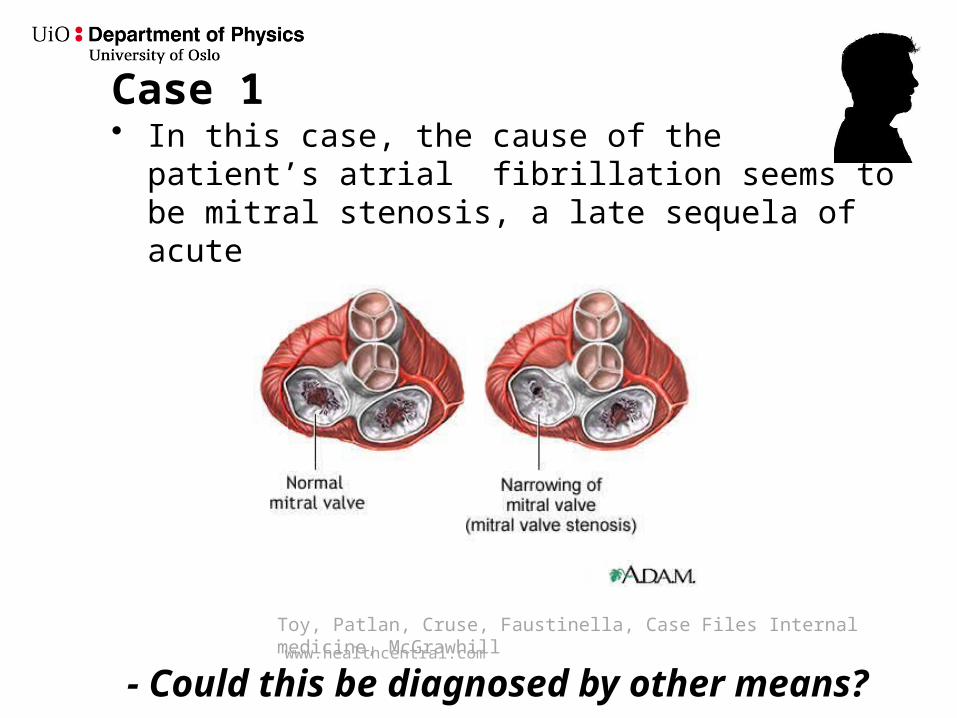
Case 1• In this case, the cause of the patient’s atrial
fibrillation seems to be mitral stenosis, a late sequela of acute rheumatic fever
Toy, Patlan, Cruse, Faustinella, Case Files Internal medicine, McGrawhill
- Could this be diagnosed by other means?www.healthcentral.com
Case 1
• Yes, by a stethoscope. A loud S1 and an opening snap following S2 with a low-pitched diastolic rumble.
• Yes by ultrasound• Yes by MRI• Yes by CT
More about this later in the course
Toy, Patlan, Cruse, Faustinella, Case Files Internal medicine, McGrawhill
- And the prognosis?
Case 1
• Very good if converted properly by surgery or medications
Toy, Patlan, Cruse, Faustinella, Case Files Internal medicine, McGrawhill