Embed Size (px)
Citation preview
ECONOMIC BURDEN OF CANCER
MECHANISM IN JOS UNIVERSITY TEACHING HOSPITAL,
Ebere Omeje
GAJI, LUKA DUNG
PG/M.Sc/08/47711
ONOMIC BURDEN OF CANCER AND PAYMENT COPING
MECHANISM IN JOS UNIVERSITY TEACHING HOSPITAL,
PLATEAU STATE
DEPARTMENT OF NURSING SCIENCES
FACULTY OF HEALTH SCIENCES AND
TECHNOLOGY
Ebere Omeje Digitally Signed by: Content manager’s
DN : CN = Webmaster’s name
O= University of Nigeria, Nsukka
OU = Innovation Centre
1
AYMENT COPING
MECHANISM IN JOS UNIVERSITY TEACHING HOSPITAL,
DEPARTMENT OF NURSING SCIENCES
ACULTY OF HEALTH SCIENCES AND
: Content manager’s Name
Webmaster’s name
a, Nsukka

2
TITLE PAGE
ECONOMIC BURDEN OF CANCER AND PAYMENT COPING MECHANISM IN JOS
UNIVERSITY TEACHING HOSPITAL, PLATEAU STATE
M.Sc RESEARCH POST FIELD
PRESENTED
BY
GAJI, LUKA DUNG
PG/M.Sc/08/47711
DEPARTMENT OF NURSING SCIENCES
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY, UNIVERSITY OF NIGERIA,
ENUGU CAMPUS.

3
IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF MASTER OF
SCIENCE DEGREE IN COMMUNITY HEALTH NURSING
SUPERVISOR: DR. (MRS) I.L. OKORONKWO
DECEMBER, 2015
APPROVAL PAGE

4
CERTIFICATION

5
This is to certify that this dissertation is the original work carried out by Gaji, Luka Dung, in the Department
of Nursing Sciences, University of Nigeria, Enugu Campus, except as specified in acknowledgements and
references, and that the dissertation contained therein has not been submitted to this University or any
other institution for the award of a degree.
------------------------------------ --------------------------------
GAJI, Luka Dung
(Student) Date
------------------------------------ --------------------------------
Dr. (Mrs). I.L. Okoronkwo
(Supervisor) Date

6
DEDICATION
Dedicated to all people living with cancer who have made this study possible.

7
ACKNOWLEDGEMENTS
I am grateful to God Almighty who has shown me his faithfulness throughout the time of this research.
I sincerely appreciate my project supervisor, Dr. I.L. Okoronkwo for her untiring efforts, mentoring and
friendly co-operation throughout the period of this work. I remain grateful to you ma. I also acknowledge
Prof. I. Ehiemere, Dr. N.P. Ogbonnaya and Dr. E. Nwonu for their contributions and encouragement towards
the realization of this research work.
My gratitude also goes to Salamatu Ishaku, Monica Abua, Oyedele, Ijeoma Ilo and Makazi for their
contributions towards the achievement of this goal.
I thank my research assistants for their co-operation and time dedicated during the data collection.

8
Special appreciation goes to my wife and the entire family members, Rev. Dachung and Maisaje for their
immense prayers and support in all my academic activities. I love you all.
Lastly, I thank the people living with cancer and their relations for their understanding and co-operation
during the data collection process.
TABLE OF CONTENTS
PAGE
Title Page I
Approval Page ii
Certification iii
Dedication iv
Acknowledgement v

9
Table of Contents vi
List of Tables ix
List of Figures x
Abstract xi
CHAPTER ONE: INTRODUCTION
Background to the Study 1
Statement of the Problem 3
Purpose of the Study 4
Specific Objectives 4
Research Questions 5
Research Hypotheses 5
Significance of the Study 5
Scope of the Study 6
Operational Definition of Terms 6
CHAPTER TWO: LITERATURE REVIEW
Conceptual Review: 8

10
Conceptual Review on Cancer
Economic Burden of Cancer
Direct Cost
Indirect Cost
Payment Coping Mechanism 23
Theoretical Review: The Cost-of-Illness Framework. 26
Empirical Review 30
Summary of Reviewed Literature 39
CHAPTER THREE: RESEARCH METHOD
Research Design 41
Area of Study 41
Population of the Study 42
Sample 42
Inclusion Criteria 42
Sampling Procedure 43
Instrument for Data Collection 43
Validity of Instrument 43
Reliability of Instrument 44

11
Ethical Considerations 44
Procedure for Data Collection 44
Method of Data Analysis 45
CHAPTER FOUR: PRESENTATION OF RESULTS 46
CHAPTER FIVE: DISCUSSION OF FINDINGS
Discussion of Findings 62
Direct medical cost of cancer incurred by patients and their households in JUTH.
Indirect medical cost of cancer incurred by patients and their households in JUTH.
Cost distribution among different socio-economic groups.
Payment coping mechanism utilized by different socio-economic groups.
Implications of Findings 66
Conclusions 67
Recommendations 67
Limitations of the Study 68
Suggestion for Further Study 68
Summary of the Study 68
REFERENCES 70

12
APPENDICES
Appendix I: Sample 73
Appendix II: Instrument for Data Collection 74
Appendix III: Reliability of the Study Instrument 80
Appendix IV: Ethical Clearance Approval from JUTH 81
Appendix V: Subject Informed Consent Form 82
LIST OF TABLES
Table 1: Demographic Characteristics of Respondents 46
Table 2: Direct medical cost of cancer incurred by patients and their
households in JUTH. 48
Table 3: Indirect medical cost of cancer incurred by patients and their
Households in JUTH. 50
Table 4: Indirect Medical Cost of Care 52

13
Table 5: Household Assets and social status 53
Table 6: Monthly income and expenditure among different socioeconomic groups 54
Table 7: Payment Coping Mechanism and Ease in paying for cancer management 55
Table 8: Difference in Cost Distribution among Socio-Economic Groups 57
Table 9: Difference between Payment mechanisms Utilized by cancer patients
and different socio-economic groups 59

14
LIST OF FIGURES
Figure I: Conceptual Model of the Study Adapted from the Cost-of-Illness Framework
(developed by researcher) 19

15
ABSTRACT
The economic burden of cancer and the stress of payment require that, health care providers provide quality
cost-effective care that will shorten the stay of patients in the hospital and reduce the frequency of visit to
health facilities. This study investigated the economic burden of cancer patients and payment coping
mechanism in Jos University Teaching Hospital, Plateau State. Four objectives and two hypotheses were
raised to guide the study. Cost-of-illness framework was used to assess the economic burden of cancer
patients and payment coping mechanism. A cross-sectional descriptive survey design was used for the study.
A sample of 179 cancer patients was drawn consecutively from an estimated population of 276 that used the
hospital in one year. Data were analyzed descriptively using frequencies, percentages, mean and standard
deviation. Chi-square was used to determine the association between socio-economic groups and payment
coping mechanisms utilized by cancer patients and between the cost distributions among different socio-
economic groups. Majority of respondents were ranked among the poorest, the mean monthly total income
of the patients is N65,978.74 + 104,036.97, mean monthly total expenses is N43,916.28 + 56,070.33, the
mean monthly patients’ expenditure is N43,916.28 + 56,070.33, the mean total annual loss was N217,515.19
+ 798,708.95, the mean patients’ annual loss as a percentage of their mean annual income is 11.38 + 19.13%
while as a percentage of their mean annual expenditure was 50.06 + 421.98. There was a significant
difference in the cost distribution of different socio-economic groups in terms of monthly patients’ total
income, monthly earnings of persons accompanying patients, patients’ monthly loss, accompanying persons’
monthly loss, total monthly loss, patients’ annual loss, accompanying persons’ annual loss and total annual
loss (P < 0.05). Payment coping mechanism utilized by most (78.8%) of the patients was their own money (i.e.
salary, earnings and/or savings). There was a significant difference between payment coping mechanism of
cancer patients (borrowed money/loan, sales of land) and different socio-economic groups (P < 0.05). There
is need for government to intervene by subsidizing the cost of cancer treatment. There is need for the
formation of a strong cancer Association in Plateau State so that cancer patients could pool their resources
together as a strong social support to help themselves.

16
CHAPTER ONE
INTRODUCTION
Background to the Study
Cancer is the second leading cause of death and disability in the world followed by heart disease
(Mathers & Lancer, 2006). It is a major public health issue and represents a significant burden of
disease. Based on the most complete and current data available, cancer accounts for one out of every
eight deaths annually (Mathers & Lancer, 2006). The incidence and death rates from cancer remain
significantly higher in the developing world including Nigeria (Boyle & Levin, 2008). It is
responsible for more deaths than all the deaths due to HIV/AIDS, TB and malaria combined (Okoye,
2010).
Cancer is a group of diseases characterized by uncontrolled growth and spread of abnormal cells
(Global cancer facts and figures, 2011). It affects different parts of the body and the name of the
cancer is given in relation to the part that is affected. It is a global disease that consumes resources.
The cost of cancer treatment globally is reported to be high. Records have it that developed countries
spend more on cancer treatment than developing countries; for example in the United States of
America, the economic burden from cancer is tagged at $895 billion nearly 20% more than heart
diseases toll ($753 billion) (John & Ross, 2009). The cancers which account for the largest costs on a
global scale, and the greatest burden in developed nations are; lung, colorectal and breast while in
low-income countries, the cancer with the greatest impact are cancer of the mouth and oropharynx,
cancer of the cervix, breast and prostate cancer (John & Rose, 2009).
According to John & Ross (2009) in Economist Intelligence Unit, WHO in 2002 reported that, in
developing countries especially Sub-Saharan Africa, cancer control including prevention and
detection is much less established with evidence showing that, only 5% of global resources for cancer

17
are spent in the developing world. Owing to the fact that cancers are not detected in the early stages,
when many are more easily treatable, treatment is less effective. In developing countries, 80% of
patients with cancer progress to incurable stages (Kanavas, 2006). The specific economic challenges
relating to cancer control in the developing world are exacerbated by other related phenomena; which
include inadequate health systems infrastructure, scarcity of specialized skills (and specialists), high
diagnostic and treatment costs, and the resulting inability to provide lengthy, complex personalised
treatment regimens and follow-up care as necessary (Axios, 2009). Some of these challenges are
caused at least in part by inadequate funding thereby leaving patients, relations and care givers to bear
the cost of diagnosis and treatment. Globally, Africa has the least amount of funds voted for cancer
management. For instance, Africa with a population of 1,007,766 cancer patients spends $849m while
America with a population of 889, 640 cancer cases spends $153,941m (Beaulieu, Bloom, Bloom,
2009).
In Nigeria, cost of cancer diagnosis and treatment is borne out of pocket. Out of pocket spending,
(OOPS) is the major payment mechanism for health care in Nigeria and this can lead to catastrophic
spending especially for the poorest households (Onwuasigwe, 2010). Adebamowo (2007) observed
that, clinical services for cancer are grossly inadequate and poorly distributed. Only few centres have
functioning radiotherapy equipment. Radiological examinations are generally available; however,
access is limited by cost. He further stated that, although chemotherapy is available, high cost
prevents most patients from taking advantage of modern regimens. Adewale (2011) commenting in
Nigeria health journal opined that, the problem for a poor Nigerian could actually begin with these
tests as they are not only done in few centres but can also be quite expensive. Cost is the major reason
for non adherence to cancer screening and treatment for the people of low socioeconomic status

18
(Adewale, Lawan & Adesunkani, 2008).When the economic status of the patient is inadequate to
meet with the cost of screening and treatment, they look for other payment coping mechanism.
Payment coping mechanisms was short term strategy used to cope with the cost of medical care
(Adams & Ke, 2008). Payment coping mechanism consists of non-income financing of healthcare;
savings, borrowing and selling of assets (WHO, 2008). Although the Nigerian government provides
exemption for treatment of malaria in under 5s and pregnant women, there is no exemption for cancer
patients; a growing epidemic with largely increasing healthcare cost, especially with its late
diagnosis. Cancer like many other known communicable diseases, have not entered the government
policy agenda and as such, is not yet integrated into the primary health care system as resolved by the
World Health Assembly in 2002. All these reflect the economic burden and inability of most patients
to cope with the costs of screening tests and treatment of cancer.
Statement of Problem
There is dearth of evidence on the cost of cancer treatment and the distribution of costs among
various socioeconomic groups affected by cancer (World Bank, 2006). In Nigeria, the health
insurance coverage is still very low (5%) and cancer treatment is not in the benefit package and there
are no form of exemptions. For someone with cancer, the common means of payment for treatment
are direct out of pocket payments. Out of pocket payments have been shown to have impoverishing
effects on households (World Bank, 2006). This is further compounded by the fact that 60-70% of
Nigerians live below poverty line of 1 dollar per day (Merie-Nelly, 2013). Little is known about the
economic burden of cancer considering different socio-economic groups in Nigeria and their payment
coping mechanism.

19
In Jos University Teaching Hospital (JUTH), about 9 patients have had to sign against medical advice
within 7 months as a result of their inability to cope with the cost of their investigations/treatment.
Some of the patients are only able to take the 1st phase of chemotherapy while subsequent phases are
forgone. JUTH is a major centre in Plateau State, with facilities for screening and treatment. One
would expect a reduction in the number of people attending the oncology clinic but this is not the
case.
Given the incidence of cancer and the national government decision to address cancer, a study of how
households are affected by cancer will aid in the formulation of policies that may help to prevent
households from being pushed into poverty. Therefore, this study was undertaken to determine the
economic burden and payment coping mechanism of households affected by cancer.
Purpose of the Study
The purpose of this study was to determine the economic burden of cancer and payment coping
mechanism among cancer patients receiving treatment in Jos University Teaching Hospital (JUTH),
Plateau State.
Specific objectives
The objectives of this study were to:
1. Determine the direct medical cost of cancer incurred by patients and their households in
JUTH.
2. Assess the indirect medical cost of cancer incurred by patients and their households in JUTH.
3. Estimate the cost distribution among different socio-economic groups.
4. Identify the payment coping mechanism utilized by different socio-economic groups.

20
Research Questions
1. What are the direct medical costs incurred by cancer patients and their households in JUTH?
2. What are the indirect medical cost of cancer incurred by patients and their households in
JUTH?
3. What is the cost distribution among different socio-economic groups?
4. What is the payment coping mechanism utilized by different socio-economic groups?
Research Hypotheses
1. There will be no significant difference in the cost distribution of cancer treatment among
different socio-economic groups.
2. There will be no significant difference in the payment coping mechanisms between different
socio-economic groups.
Significance of the Study
It will assist cancer societies in making a case towards the inclusion of cancer management in the
National Health Insurance Scheme considering the economic burden of its management.
The findings of this study will help to reveal the direct and indirect costs of treatment borne by cancer
patients. The findings will serve as a tool to advocate for the inclusion of cancer care into the
National Policy Agenda and to source for support from both governmental and non-governmental
bodies towards the management of cancer. It will provide a better understanding of the economic
impact of the disease and challenge to health care providers towards rendering qualitative cost-
effective care that will shorten the stay of patients in the hospital: and reduce the frequency of visits
to the health care facility thereby reducing cost of health care of cancer patients.

21
The findings will assist policy makers and other stake holders in decision making, particularly
towards resource allocation and research funding.
Scope of the Study
The study was delimited to all those who had been diagnosed of cancer and have been receiving
treatment from JUTH within the past one year. Both males and females within the ages of 18 years
and above were studied. Out-patients and in-patients were studied. Medical-Surgical units, specialist
clinics, and family medicine were used. Insignificant cost of cancer was not included in this study.
Operational Definition of Terms
Economic Burden: refers to both medical and non-medical costs incurred by cancer patients in the
management of their ailment. It is classified into direct and indirect costs.
Direct cost (financial cost): This has to do with cost related to investigations, diagnoses, treatment,
admissions, follow up costs and travel cost.
Indirect cost: They are those things that will be forgone for the sake of this illness e.g. time spent
travelling, waiting time in hospital, time spent out-of-work, time accompanying relative, time lost
through premature death or premature retirement.
Payment Coping Mechanism: refers to the use of ones’ income (salary and savings), someone else
paying, money borrowed/loans, community based support, sale of household assets, gifts, appeal for
support/ begging, temporary stoppage of children’s education, cutting down on minimum
consumption expenses to pay for treatment and tests.
Cancer patient: refers to someone who has been diagnosed by a physician as having cancer of any
type.

22
Cancer family/significant others: this includes, parents, brothers, sisters, surrogate or friend who
accompanies patient for treatment and have lived consistently with this experience for at least one
year.
Different socio-economic population group; this refers to the categorization of study patients into
various levels or classes. This will be determined using asset ownership like Radio, Television,
bicycle, air conditioner, electric fan, Motorcycle, Fridge, kerosene stove, generator, gas cooker and
car on a socio-economic status index, type of food and living accommodation. Socio-economic
population is also categorized into poorest, poorer and least poor.

23
CHAPTER TWO
LITERATURE REVIEW
This chapter presents review of literatures relevant to this work on economic burden and payment
coping mechanism of cancer patients. The literature was reviewed under, Conceptual, Theoretical and
Empirical reviews.
Concept of Cancer
Cancer is a group of diseases characterized by uncontrolled growth and spread of abnormal cells
(Lemone, Burke, Bauldoff, 2011). Burke, Mohn-Brown and Eby (2011) said, cancer develops when
normal cells mutate into abnormal, deviant cells that grow uncontrollably and continue to reproduce
within the body. They further explained that, cancer can affect any body tissue and has many different
manifestations which make care of the client complex. It is a disruptive and life-threatening
experience that affects the patients and their significant others.
Cancer can affect every race, and all ages; it has no respect for one’s status. Cancer is the second
leading cause of death and it is a major health problem in Nigeria and the world at large (Global
Cancer facts and figures, 2011). The presentation of the disease at times could be subtle until it
manifests as full blown Cancer. However, there are warning signs which are abbreviated as
CAUTION (Osborn, Wraa, Watson, Holleran, 2014).
C = Change in bladder or bowel habit
A = A sore or boil that fail to heal
U = Unusual bleeding or discharge
T = Thickening or lump/swelling/mole

24
I = Indigestion
O = Obvious change in mole or wart
N = Nagging cough or hoarseness of voice
When one of these CAUTION signs manifests, the individual is expected to seek for medical
attention. However, when the means to seek for medical attention at the right time is not possible due
to financial constraints on the side of the patient, the illness progresses to a cancerous state.
Cancer is a disease that has stages of development namely:
Initiation: A state of irreversible attention in the cell genetic structure resulting from the action of
chemical, physical or biologic agents (carcinogens).
Promotion state: The presence of promoting agents leads to irreversible proliferation of the altered
initiated cells and subsequently with increase in the initiated cell population, the likelihood of a
second cell mutation is increased.
Stage of progression: This is characterized by increased growth rate of the tumour as well as by
increased invasiveness and metastasis. Or,
T – tumour size (primary site)
N – node involvement (regional)
M – metastasis, absence or presence (at distant side) (LeMone, Burke, 2008).

25
Common Types of Cancer
Some of the common cancers are:
Breast Cancer: Breast cancer is a malignant (cancerous) growth that begins in the tissues of the
breast (Fasoranti, 2011). It is the most common cancer in women affecting one in every eight women
during their lives but can also appear in men. It often presents as breast lump or bloody nipple
discharge (Adebamowo, 2007; Omolara, 2011). Breast cancer as a public health problem is growing
throughout the world, but especially in developing regions, where the incidence has increased as
much as 5% per year (Groot, Baltussen, Carin, Groot, Anderson and Gebrielet, 2006). In 2008, there
were an estimated 1.4 million new cases worldwide (Global cancer facts in figure, 2011) and each
year, breast cancer is newly diagnosed in more than 1 million women worldwide and more than
400,000 women die from it (Groot et al, 2006).
In Nigeria, the number of women at risk of breast cancer increased steadily from approximately 24.5
million in 1990 to approximately 40 million in 2010 and is projected to rise to over 50 million by
2020 (Akarolo, 2010). The rising incidence of breast cancer is being driven by increasing life
expectancy, improved control of infectious diseases, and changing lifestyle, diet, physical activity and
obstetric practices (Adebamawo, 2002, Akarolo, 2010).
Cervical Cancer: The cervix is the lower part of the womb or uterus and is commonly referred to as
the neck of the woman (Okoye, 2010). Carcinoma of the cervix (Ca cervix) is a malignant neoplasm
of the cervix uteri or cervical area. Cervical cancer is the seventh most common cancer in the world
and second commonest cancer of women (Omolara, 2008; Nwankwo, 2011) and an estimated 400-
500 new cases occur per year, 80% of these in low income countries (Omolara, 2008 &
Onwuasigiwe, 2010). In 2005, 260,000 women died from it globally, nearly 95% of them in

26
developing countries (Nnodu, 2010). The incidence rate of cervical cancer in Nigeria is 25/100,000
(Olatunbunsun, 2007, Nnodu 2010, Onwuasigiwe 2010 & Amosu 2011) while the reported
prevalence rates for HPV in the general population and HPV in women with cervical cancer are
26.3% and 24.8% respectively (Nndu, 2010, Amosu, 2011).
Cervical cancer is a vicious killer of women today, which ought not to be because cancer of the
cervix is easily seen and treated, provided diagnosis is made early (Olatunbunsun, 2007). The initial
presentation may be vaginal bleeding, while symptoms may appear after the cancer is in its advanced
stages, the early stages may appear asymptomatic (Amosu, 2011). Symptoms of advanced cervical
cancer may include: abnormal vaginal bleeding that includes bleeding occurring between regular
menstrual periods, bleeding after sexual intercourse, douching or pelvic examination and menstrual
period that lasts longer and are heavier (Onwuasigiwe, 2010). Loss of appetite, weight loss, fatigue,
pelvic pain, back pain, leg pain, single swollen leg, leaking of urine or faeces from the vagina, and
bone fractures (Amosu, 2011).
Prostate Cancer: The prostate gland a part of the male reproductive system is an organ that is
located at the front of the rectum and base of the urinary bladder. Prostate cancer is a malignant
tumour that consists of cells from the prostate glands (Onwuasigiwe, 2010). Prostate cancer is the
second leading cause of cancer death in African American men. An estimated 35,110 cases of
prostate cancer and 5.300 death are expected to occur among African American men in 2011,
accounting for 40% of all cancers diagnosed in African American men. It is estimated that 1 in 5
African American men will be diagnosed with prostate cancer in their lifetime (Cancer figure, 2011).
About three quarters of cases worldwide occur in men aged 65 years or more, it is rarely found in
men aged 40 years (Onwuasigiwe, 2010). Early prostate cancer usually has no symptoms. With
more advanced disease, individuals may experience weak or interrupted urine flow; inability to

27
urinate or difficulty starting or stopping the urine flow; the need to urinate frequently, especially at
night; blood in the urine; or pain or burning with urination. Continual pain in the lower back, pelvis,
or upper thighs may be an indication of spread of the disease to bones. Many of these symptoms,
however, are similar to those caused by benign conditions (Global cancer facts & figure, 2011).
Causes/risk factors of cancer
Heredity/genetic factors: The genetic changes that characterize cancer occur as a consequence of
defective hereditary malaria. A single inherited mutant gene may be enough to cause a very high
cancer risk. Although cancers sometimes cluster in families, it does not follow the rigid inheritance
pattern characteristic of a mutation to a single gene. Genetic polymorphism of metabolic enzymes
seems to influence the risk of bladder cancer. A substantial variation in Insulin Growth Factor (IGF),
a peptide growth factor, has been identified as cause of prostate cancer
Family history: Cervical cancer may seem to run in families and 2-3 times higher risk if a mother or
sister has the disease (Omolara, 2008). A higher incidence of prostate cancer also has been reported
among male relatives of breast cancer patients.
Sex: Certain cancers are common in both sexes while some occur in only one sex alone. Some of the
male cancers are: penile cancer, prostate cancer, testicular cancer, breast cancer. Some of the female
cancers are: breast cancer, cervical cancer, fallopian tube cancer, ovarian cancer, uterine cancer.
Cancer found in both sex are: lung cancer, bowel cancer, liver cancer, kidney cancer, colorectal
cancer. Kaposi Sarcoma was about 10 times more common in men than women of older age group
(Global cancer facts & figure, 2011).
Age: Increasing age is a determinant of cervical cancer which is found to be more in women between
the 4th and 5th decade (Omolara, 2008). Older women have more chances of having breast Cancer

28
(Fasoranti, 2011). The incidence of breast cancer starts to increase at about the age of 20 years and
rises rapidly to about the age of 50 years, when the rate of increase reduces somewhat, and by 75
years of age the incidence starts to decline (Akarolo, 2010).
Race/Ethnicity: Cervical cancer is believed to be found more in some ethnic groups like Africa,
Latinos and rare in Jews (Omolara, 2008).
Life Style Determinants
Smoking/tobacco use: At a global level, tobacco causes more premature deaths from cancer and even
greater numbers from other causes. It is responsible for 30% of all cancer deaths (Cancer figure,
2011). Smoking is associated with increased risk of at least 16 types of cancer: nasopharynx, nasal
cavity and paranasal sinuses, lip, oral cavity, pharynx, larynx, lung, oesophagus, pancreas, uterine
cervix, kidney, bladder, stomach, colorectal, and acute myeloid leukaemia (Cancer figure, 2010).
Current smokers have a higher risk of being HPV positive and this risk increases with number of
cigarettes smoked per day and the duration of smoking (Omolara, 2008).
Contraceptives/ Hormones: The use of hormonal contraceptives; injectables and pills has been
associated with a slight risk of cervical cancer (Omolara, 2008).
Sexual debut/unsafe sex: Early commencement of sexual activity especially in adolescence is
associated with greater risk of cervical cancer because of vulnerability to HPV infection. Sexual
debut before 18-20 years is a strong determinant of cervical cancer (Omolara, 2008).
Parity: There is increased risk of breast cancer among women with low parity or nulliparous women.
There is also an association between risk of breast cancer and late age at first birth. There has been a
consistent association of high parity with cervical cancer (Omolara, 2008).
29
Overweight/obesity: Obesity increases the risk of many cancers, including cancers of the breast (in
postmenopausal women), colon, endometrium, kidney, and adenocarcinoma of the esophagus
(Cancer figure, 2011). Increasing evidence also suggests that being overweight increases the risk of
developing other illnesses following a cancer diagnosis (Cancer figure, 2011).
Diet/Nutrition: Diets high in fats or a high consumption of meat, salting and pickling as well as
additives increase the risk of cancer. Many epidemiologic studies have shown that populations that
eat diets high in vegetables and fruits and low in animal fat, meat, and/or caloric’s have reduced risk
of the most common cancers (Cancer figure, 2011). Some studies indicate that excessive amount of
animal products in the diet increases the risk of colorectal cancer. It has been suggested that
deficiencies of some micronutrients may increase risk of cervical cancer, probably through their
influence on immune system (Omolara, 2008).
Physical activity: Studies have shown that regular physical activity is associated with lower risk of
several types of cancer, including cancers of the breast, colon, prostate, and endometrium (Cancer
figure, 2011).
Occupation: Various occupational categories associated with increased risk of bladder cancer
include workers with dyestuffs, aromatic amine manufacturing, rubber workers, leather workers, and
painters. Other factors known to increase risk of lung cancer are occupational exposures to asbestos,
some metals (e.g nickel, arsenic and cadmium).
Hygiene: Environmental and personal hygiene have been associated with cervical cancer in low-
income countries example the re-using of sanitary towels in Mali (Omolara 2008).
Social-cultural environment: This influences lifestyle and sexual behaviour globally and in Nigeria
although some variations occur due to the prevailing customs in the different regions (Omolara,

30
2008). There is a lower frequency of penile cancer in men who are circumcised especially in
countries where it is a cultural practice.
Illiteracy: Worldwide, illiteracy is closely associated with higher prevalence of HPV infection and
cervical cancer. It may also be due to ignorance about cervical cancer (Omolara, 2008).
Religion: Cervical cancer is rare in nuns and Muslims in North Africa and Middle East compared to
Sub-Saharan Africa (Omolara, 2008).
Socioeconomic status: Nigerian women of low SES have higher risk of cervical cancer (Omolara,
2008).
Infections: Infectious agents may account for about 15% of cancers in the world (Omolara, 2008).
Diagnosis and Treatment
The effective decisions about cancer treatment are based on the results of accurate diagnostic findings
performed by a multidisciplinary team. A person with cancer typically undergoes a battery of test to
determine the location, extend and tumour type of the malignancy. Diagnostic modalities need to be
individualized to the patient and may include a thorough history and physical examination,
appropriate imaging test invasive procedures such as biopsies, laboratory studies and pathology
examination of tissue of blood (Osborn et al, 2014).
Treatment of cancer aims to cure the disease or considerably prolong life while improving the
patient’s quality of life (WHO, 2008). Treatment options are dependent on cancer stage and choices
available. Some of the treatment options are surgery, radiotherapy and chemotherapy, hormonal
therapies stem cell and bone marrow transplants singly or as a combination (Osborn, Wraa, Watson &
Holleran, 2014). There is also rehabilitation which aims to improve life from impairments due to

31
cancer. When cancers are detected early, treatment given, higher cure rates are more likely than when
it is at an advanced stage. Palliative care is a treatment which aims to relieve pains and cancer
symptoms rather than cure. It is best for advanced cancers where there are no chances of cure.
Improved access to oral morphine is mandatory for the treatment of moderate to severe cancer pain,
suffered by over 80% of cancer patients in terminal phased if palliative care is to be used. Individuals
who are undergoing cancer screening test are not considered patients. Only when an abnormal screen
test is discovered, is the individual considered a patient (Osborn, et al, 2014).
Prevention and Control of Cancer
Cancer prevention can take the form of primary prevention approach which is cost effective and can
be used to reduce exposure to the major risk factors at both individual and community level. They
include increasing physical fitness, control of obesity, tobacco and alcohol as well as promotion of
health diet rich in vegetables and fruit (Omolara, 2008). Primary prevention can be by health
promotion strategies involving communication for behavioural change. Use of vaccines where
available to prevent disease and tobacco control can also be a part of this approach. Cancer control
can also take the form of a secondary prevention approach which involves screening, early detection
and diagnosis at stages where the disease is still curable as well as reproductive health intervention.
Regular screening ensures that precancerous changes are detected early enough so that they can be
treated. Pap smear is a preferred screening method for cervical cancer and has contributed to 50 –
70% reduction in its incidence in developed counties (Omolara, 2008). Tertiary prevention is the
management of a disease with the goal of preventing progression, recurrence or complications
(Osborn et al, 2014). Regardless of the approach used, emphasis on cancer prevention should be
placed on the risk factors and the prevalence of a cancer type in a country based on their situation
analysis.

32
Tobacco use is a known cause of a lot of cancers. Its use can be acquired from peers and then it
becomes a habit due to the addictive properties of tobacco. Action against stopping the use of tobacco
should take into cognizance these issues and it requires individual, community and government
participation and a lot of behavioural changes. Dietary modification has been seen as a way in
preventing cancer. Fruits and vegetables are said to have protective effect against cancer. For
instance, vitamin C is believed to protect against stomach ulcer, beta carotene against lung cancer.
Alcohol use as a cancer risk factor is not only on the type of alcohol consumed but also the quantity.
Any intervention to control excessive alcohol use should involve the individual together with a lot of
health promotion and education.
Increasing physical activities like walking can help reduce obesity which can result in cancer. To
prevent some occupational cancers, health promotion measures need to be taken as well as
improvement in organizational safety guards. Knowledge on sexual and reproductive factors should
be enhanced to reduce the risk of certain cancers. Oral contraceptives, use of estrogens for
menopausal and post-menopausal symptoms, early sexual intercourse and multiple partners’ issues
should be part of educational programme on lifestyle behaviours. In all it can be seen that health
promotion is the key to cancer control and prevention and as such education, environmental support
and public health policies are of great importance (Osborn et al, 2014).
Economic Burden of Cancer
When a patient is diagnosed with cancer, the burden of treatment does not lie on the patient alone.
Other family members are affected physically and economically as well. When a patient is diagnosed
with cancer, the financial resources of the family may be affected by the loss of ability to work and

33
the needs of well family members may be neglected because of the focus on the ill members (Walsh
& Crumbie, 2007).
The economic burden of health care expenditure on individuals challenged with chronic illness
especially where prepayment system is absent is a growing concern (Ke, Evans & Carrin, 2007).
This includes direct cost of medical care and indirect cost from productivity losses due to patient's
disability and time spent by family members accompanying patients to seek care. Cancer remains one
of the leading causes of morbidity and mortality world wide (Kanavas, 2006). It is the second most
common cause of death in United States, accounting for nearly 1 for every 4 deaths (American
cancer society, 2014). In Africa, cancer is an emerging public health problem.
Cancer accounted for close to one trillion dollars in economic losses from premature death and
disability in 2009(John & Ross, 2009). The economic burden from cancer was $895 billion which
was nearly 20% more than heart disease’s toll ($753 billion). They further reported that, the loss of
working man-hours and life caused by cancer represents the single largest drain on nation’s
economies (USA), compared to all other causes of death, including HIV/AIDS, heart disease and
infections etc. This shows that, cancer consumes a lot of funds in the developed world where a
reasonable percentage of their budget goes to health (John & Ross, 2009).
Estimate shows that there were 12.7 million new cancer cases in 2008 worldwide, of which 5.6
million occurred in economically developed countries and 7.1 million in economically developing
countries (Global Cancer facts & figures, 2011). It was further estimated that 7.6 million cancer
deaths occurred (about 21,000 cancer deaths a day); 2.8 million in economically developed countries
and 4.8 million in economically developing countries. (Global Cancer facts & figures, 2011, Ferlay et
al, 2010).

34
If adequate measures are not taken to curtail the global burden of cancer in the developing world, the
rise will reach 66% by 2015 and even higher by 2020. The low level of awareness about cancer and
the high cost of therapy observed in Nigeria as well as the lifestyle and behavioural risks
superimposed on cultural beliefs amplify the chances of developing cancer in high risk patients
(Mehta, 2012). He suggested a multidisciplinary approach with multi-faceted treatment protocols
which has helped in India, as the way forward. He lamented that 70% - 80% report to health facilities
at the late stage of the disease when nothing can no-longer be done and this happens only when they
must have wasted time at taking alternative treatments to no avail (Mehta, 2012).
Cancer patients in developing countries like Nigeria pay a large share of the health care costs out of
pocket (OOPs) due to lack of financial risk protection mechanisms (Onwujekwu, Uzochukwu,
Obikeze, Okonkwo, Ochonwa, Onoka et al, 2010; Onah & Govenderz, 2014). Cancer exerts a heavy
economic burden on individuals, national health system and society at large and the burden borne
depends on the differences in purchasing power and social insurance policies of the countries they
live in. It affects quality of life, not only of the patients and their immediate families but also the
society. High medical cost as seen in the treatment of cancer poses a barrier to seeking health care
(Onwujekwu et al, 2010; Onah & Govenderz, 2014) and can be a major cause of indebtedness and
impoverishment of households since there is paucity of financial risk protection mechanism in
Nigeria.
The National Health Insurance Scheme (NHIS) presently covers only people that are employed by the
federal government less than 5% of the population (Onwujekwe et al, 2010), others and even the
enrollees of the health insurance scheme still depend on OOP payments to cover their medical
expenditures. Out of pocket payments have severe consequences for health care access and utilization
and especially catastrophic for the poorest households

35
(Onwujekwu et al, 2010). In Nigeria, private health expenditures account for 60% to 65% of total
health expenditure and 95% of private expenditure (Onwujekwe, Hanson & Uzochukwu, 2012;
Onwujekwe et al, 2011). Every year more than 150 million individuals in 44 million households face
financial catastrophe as a direct result of paying for health care and 100million individuals are pushed
into poverty by the need to pay for health care (Xu et al 2005). The incidence of catastrophic health
expenditure has been reported by some researchers in Nigeria (Onwujekwe et al, 2012; Onoka et al,
2011).
Health expenditure has been defined as catastrophic when it is greater or equal to 40% of the annual
household income remaining after subsistence needs have been met (Xu et al, 2005, Onoka et al
2011, Onwujekwe et al, 2012). Catastrophic health expenditure depletes household income and
contributes to the vicious cycle of poverty and disease. It forces poor house holds to reduce other
basic expenses such as food, shelter or their children’s education (Russell, 2004; Wagstaff & van
Doorlaer, 2003).
Direct Cost
Direct medical costs are those associated with services that patients receive, including
hospitalizations, surgery, physician visits, radiation therapy and chemotherapy/immunotherapy, and
are typically measured by insurance payments and patient out-of- pocket co-payments and
deductibles (Yabroff, 2011). Within each phase of care, the direct medical costs associated with
cancer vary significantly by cancer site. For example, a recent study reported that in the year 2010,
mean monthly net costs in the elderly were $1,923 for female breast cancer and $5,074 for female
lung cancer patients in the initial phase of care (Lund, 2011). In the continuing phase of care, mean
monthly net costs were $184 and $678, respectively. In the last year of life among patients who died

36
of cancer, mean monthly costs were $5,238 and $7,710. As illustrated in this example, net costs of
care were higher in the initial and last year of life phases of care than in the continuing phase of care
and higher for lung than breast cancer patients in every phase of care (Yabroff, Lund, Kepka and
Mariotto, 2011).
Cancer is on the rise in Nigeria but treatment costs N0.5m monthly. Cancer cases keep rising and the
cost implications of treatment are putting Nigerians on edge since the current minimum wage of
N18,000 may not be able to afford diagnosis, let alone procure the right medical service to manage
the ailment (Chiejina, 2013). Business day investigations show that an individual is likely to spend
about N67,000 for breast scan, mammogram, biopsy and other tests. An average surgery cost between
N80,000 and N150,000 while chemotherapy cost ranges between N100,000 and N500,000 (Chiejina,
2013). This is an indication that the financial burden of managing the ailment bites hard on the patient
worst if he or she is of the low financial status (Chiejina, 2013).
Indirect cost
Indirect cost of cancer are monetary losses associated with time spent receiving medical care, time
lost from other usual activities (morbidity costs), and lost productivity due to premature death
(mortality cost) (Yabroff, Lund, Kepka Mariotto, 2011). These costs are incurred by patients as
well as their caregivers and families. Since these lost opportunities are not typically reflected in
monetary transactions, the value of lost time must be approximated. Lyman (2007) opined that, death
care costs have risen dramatically over several decades, now approaching $2 trillion annually with
costs of cancer care representing approximately 10% or roughly $200 billion.
In USA, bladder cancer is responsible for 70,000 diagnosed cases and over 15,000 deaths. Once
diagnosed, patients with non-muscle invasive bladder cancer (NMIBC) are committed to a life time

37
of invasive procedures and potential hospitalization that result in substantial direct and indirect costs
amounting to nearly $4 billion per year. Mossanen and Gore, (2014); added that, this fiscal burden is
further compounded by the indirect impact on psychological health and quality of life of patients and
their families.
Huffing and Thiboldeaux (2015) reported that, in their study that 58% of patients ages 18-44 were
reported being or very seriously concerned about bankrupting their families, that, apart from the
direct costs, the impactful cost also are the less frequently mentioned collateral costs, such as loss
income due to taking time off work, the time and cost of travelling across large distances to see in-
network doctors and child care. In an effort to cover cost, patients with cancer will use money
originally set aside for other purpose e.g 37% of those affected cut their grocery expenses 48% gave
up vacations, celebrations and social events. 24% borrowed against or used money from a retirement
plan. The impact of the financial burden caused by out of pocket expenses cannot be over stated
(Huffington, 2015). There is therefore death of data on the cost of managing individuals with cancer
and the cost borne by patients/families in Nigeria, and there is therefore an urgent need to quantify the
cost of cancer and to place cancer on the policy agenda for integration into the national Health policy
and strategies so that cancer management cost will be considered to compete with other sensitive
health issues like HIV/AIDs, Tuberculosis (TB) and Malaria control (Sridhar, 2011).
The main approaches for valuing time are the human capital and the willingness-to-pay (WTP)
methods. In the human capital approach gender-and age-specific average earnings are combined with
time lost from work or years of working life lost due to premature death to estimate unrealized
earnings (Yabroff et al, 2011). WTP approaches, in contrast, incorporate both lost productivity and
the intrinsic value of life, by estimating the amount an average individual or populations of
individuals would be willing to pay for an additional year of life. Because cancer incidence and

38
mortality rates are highest in the elderly, a population less likely to be in the workforce than their
younger counterparts, these valid, but conceptually different approaches yield very different estimates
of the indirect costs of cancer (Yabroff et al, 2011).
Payment coping mechanism
Adams and Ke (2008) defined payment coping mechanisms as short term strategies used to cope
with the cost of medical care. It provides information on how individuals and house holds respond to
unpredictable illness that diminish the health status and lead to poverty because they are affected by
both payments for medical care and income losses from inability to work (health shock). Very high
health care expenditures relative to income in house holds may force house hold members to cut their
consumption of other minimum needs. This triggers the use of payment coping mechanisms to cater
for the costs of health care (Adams & Ke, 2008). Such strategies include selling of assets, borrowing,
perceived cost - saving behaviours like skipping appointment, skipping doses of drugs to make it last
longer or seeking and use of treatment from cheaper alternatives at the expense of good quality care
(Adams & Ke, 2008).
The choice of a coping strategy differs in different context among house holds in the face of
economic burden of illness and will depend on a house hold's asset base (Adams & Ke, 2008). While
such strategies may meet the short term goal of paying for treatment and minimizing costs, financing
health care with payment coping mechanisms leads to sacrificing of necessary consumptions to pay
for health care thus, pushing the house hold into deeper poverty (Adam & Ke, 2008; Chuma &
Molyneaux, 2007). The mechanisms include but not limited to the following:
Appeal for Charity/Begging
Appeal for support may be made to charitable individuals/groups to contribute towards treatment of
individual(s) with particular health problems. This appeal could come through the mass media

39
creating awareness of the need for support. It may come through group of individuals who advocate
for such supports using photograph of the person involved and presenting the picture of the problem.
They often use public address system in the streets, markets or public gathering like churches to
solicit for support. Media houses can also raise advocacy for support on behalf of the cancer patient.
Begging could also be used. The person with cancer stands at strategic places in the streets or gets to
individual(s) to ask for support to help them purchase their drugs. Individuals use appeal for support
from good-spirited individuals, members of the public, and begging among others to cope with
payment (Oyekale, et al., 2010)
Borrowing/loans
This is a mechanism where individual(s) obtain a resource to meet healthcare need to pay back when
he/she is able. Borrowing can be formal or informal. Informal borrowing exists where the resources
are given out without interest but formal one attracts interest (Oyekale et al, 2010). Borrowing, as a
coping mechanism, often attracts high rate of interest on loan, especially when they borrow from
professional money lenders. Borrowings mainly from friends and other families and taking out a loan
using collateral especially for low and middle income households and those with high in-patient
expenses are used as coping mechanisms (Adams et al, 2008). They noted that the highest income is
less likely to borrow or sell assets and that 30% of households in West Africa finance out of pocket
spending through borrowing. Kaleml (2006) asserts that coping mechanisms are not costless, Kupur
(2006) and Onwujekwe et al (2010) also identified borrowing as payment coping mechanism.

40
Sale of Assets
In short terms, when medical bills exceed a household’s income, households sell assets (Adams et al,
2008). They recognized sale of assets as a method employed to finance out-of pocket spending and
that sale of assets is popular in West Africa but not common in Zambia, Namibia and Swaziland but
about 68% of patients in Burkina Faso cope by selling assets. Distress selling of assets (land,
household mobile assets, labour) is a coping mechanism in Northern Nigeria (Oyekale and Yusuf,
2010). Onwujekwe, et al., (2010) also noted sale of household assets and sale of land as coping
mechanism in South-East Nigeria, though sale of land is said to be uncommon.
Gifts as a payment coping mechanism
Individuals or groups may be moved with compassion to give cash or kind gifts to cancer patients to
support treatment. Most times it comes from friends and relations who are aware of the person’s
problem/need. Gift is used in several sub-Saharan and south East Asian countries to support health
care. Gifts from friends, relatives and neighbours are payment coping mechanisms in Nigeria
(Tawiah, 2000; Oyekale, et al., 2010)
Savings and Cutting Down on Minimum Consumptions
Individuals could fall back on savings earmarked for other needs to cope with healthcare payment
(Tawiah, 2000; Kupur, 2006). Tawiah also noted personal savings as a means of mitigating the effect
of high cost of healthcare and cutting down on personal consumption of certain goods as a coping
mechanism for payment. Incomes and savings were noted as popular coping mechanisms in Zambia,
Cote d’ivoire, Chad and an average of 40% of West African countries cope with healthcare payment
through it (Adams & Ke, 2008). In developing countries with few government safety nets chronic

41
conditions like cancer impose heavy cost over time if regular treatment is required and if the sick are
incapacitated. This high cost triggered either cost prevention strategies (do not seek treatment or
abandon treatment or adopt relatively risky asset strategies, settle for cheaper alternatives) (Russel
2004; Oyekele et al., 2010).
In Nigeria the various coping mechanism utilized by house holds include distress sale of assets,
reduced intake of food to conserve foods, interruption of children's education, informal and formal
borrowing, charitable support from churches, gifts from friends (Oyakale & Yusuf, 2010). Others
includes installment payment, borrowing, reimbursement, off-front payment and in-kind payment
(Onwujekwe et al, 2010).
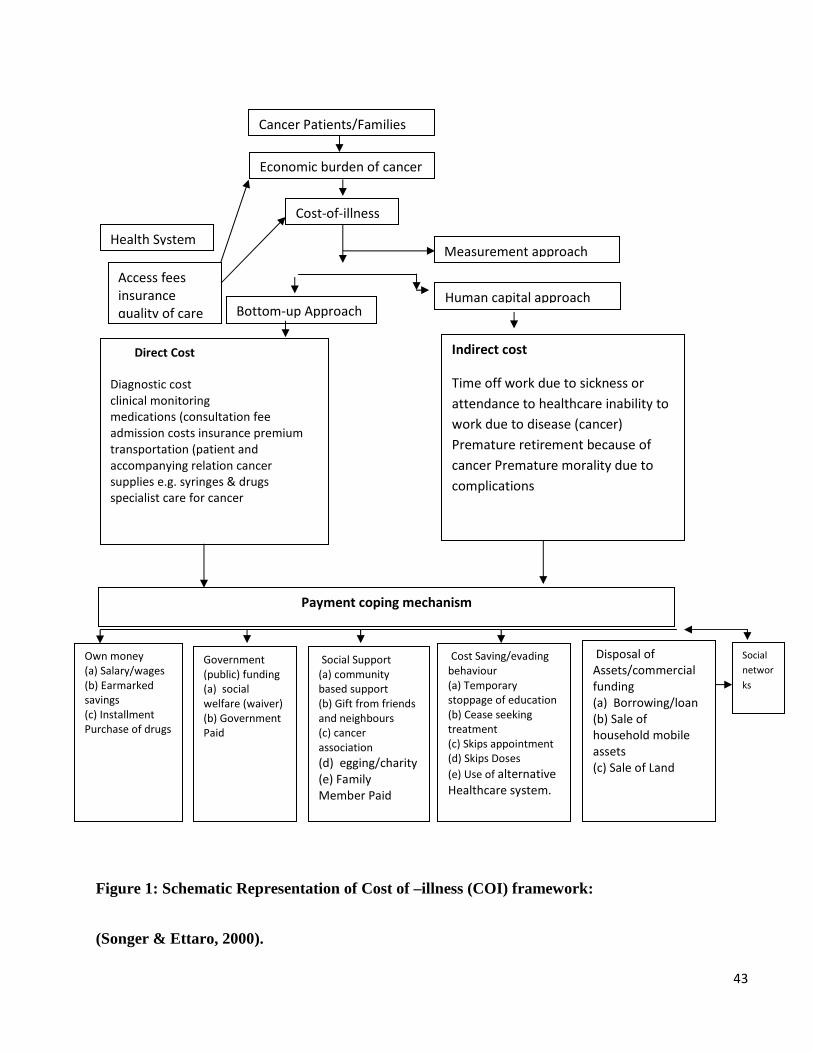
Theoretical Review
The theoretical framework related to this work is the cost-of-illness (COI) framework. It is a model
that describes the costs of specific diseases using analytical approaches. For the study on economic
burden of cancer patients this model becomes necessary to elicit the direct and indirect costs
associated with cancers. The two approaches adopted for this study are: ‘bottom-up’ approach for the
direct costs and human capital approach for indirect costs (Songer & Ettaro, 2000).
Bottom-up approach derives the direct costs by aggregating the cost units of services performed at
each encounter with the health system within a given period of time. They include costs of drugs,
investigations, admissions, consultation etc. It uses cost of service estimate and applies data to the
total number of health encounters related to the disease (cancer) to arrive at an estimate of the health
cost of the disease. These costs have attendant burdens/problems which patients need to cope with as
their treatments progress. The payment coping is focused on short term payment methods/strategies
used by cancer patients in the course of their treatment to meet up the economic demand of the
illness.

42
Below is a schematic representation of patient-based economic burden of cancer consisting of direct
and indirect costs which when articulated amounts of total cost of cancer care, with need to device
payment coping mechanism. It is expected that this framework would help in capturing the necessary
data from the cancer patients on their economic burden and their payment coping mechanism.
43
Figure 1: Schematic Representation of Cost of –illness (COI) framework:
(Songer & Ettaro, 2000).
Cancer Patients/Families
Economic burden of cancer
Cost-of-illness
Access fees
insurance
quality of care
Health System Measurement approach
Human capital approach Bottom-up Approach
Indirect cost
Time off work due to sickness or
attendance to healthcare inability to
work due to disease (cancer)
Premature retirement because of
cancer Premature morality due to
complications
Direct Cost
Diagnostic cost
clinical monitoring
medications (consultation fee
admission costs insurance premium
transportation (patient and
accompanying relation cancer
supplies e.g. syringes & drugs
specialist care for cancer
Own money
(a) Salary/wages
(b) Earmarked
savings
(c) Installment
Purchase of drugs
Government
(public) funding
(a) social
welfare (waiver)
(b) Government
Paid
Social Support
(a) community
based support
(b) Gift from friends
and neighbours
(c) cancer
association
(d) egging/charity
(e) Family
Member Paid
Cost Saving/evading
behaviour
(a) Temporary
stoppage of education
(b) Cease seeking
treatment
(c) Skips appointment
(d) Skips Doses
(e) Use of alternative
Healthcare system.
Disposal of
Assets/commercial
funding
(a) Borrowing/loan
(b) Sale of
household mobile
assets
(c) Sale of Land
Social
networ
ks
Payment coping mechanism

44
Application of Theoretical Framework
This framework was adapted from studies that have investigated the cost of illness, strategies and
economic burden of patients/families (Russell, 2004 & Akobundu, 2006).
Patients/families when challenged with cancer seek quality care from orthodox health care facilities
using access fees. Illness costs are incurred by cancer patients/family care directly and indirectly
(economic burden of cancer). The direct costs are incurred from received care while the indirect costs
represent the monetary value of productive man travelling to receive care, absent from work by
patients and family carers, premature retirement etc.
The cancer patients/families live in environment which has social resources (policies and
programmes) and network of support for healthcare payment and for coping with payment of cancer
costs on short term when 10-40% subsistence income is exceeded. These payments coping
mechanism could be through private funding (OOPS, Insurance etc), Public funding (Government
pays; exemption, general taxation etc) or donor (social support, NGOs, community based insurance
etc.). Because the social environment of cancer in Nigeria is laden with poverty, user fee is
operational and since they visit the health facilities more frequently, they could incur catastrophic
costs and may use short term measures to cope with payment. They could also mobilize resources
within and outside the family (social network) to cope with payment for cancer. Such coping
mechanisms include but are not limited to own money (earmarked savings, salaries and wages etc),
social support (gifts from friends, community support etc), disposal of assets (sale of household
assets, land), Government pays (waiver, concessional release on specific visits) use of perceived cost
saving behaviours (skipping appointments, alternative healthcare system etc). If cancer patients
finance healthcare with unfavourable coping mechanisms like disposal of assets, borrowing or

45
stoppage of children's education etc they can be pushed deeper into poverty as these could increase
costs indirectly and compromise the future economic value of the children. Some analysts assume
that a cost burden greater than or equal to 10% of income is likely to be catastrophic for cancer
patients/household. By implication, it is likely to force them to cut their consumption of other
minimum needs, trigger productive asset sales or high level of debts and reduce access to health care
and subsequent early complication of cancer. This study therefore assumes that 40% expenditure on
cancer care could be considered as catastrophic but considering socio economic inequalities it would
also assess catastrophic expenditure at 10% and 40% for the poorest socioeconomic status group and
the least poor socioeconomic status groups respectively.
Empirical Review
Zaidi, Asari and Khan (2012) carried out a study on the financial burden of cancer: estimate from
patients undergoing cancer care in a tertiary care hospital, at Aga Khan University, Hospital (AKUH)
Karachi Pakistan from March 2009 to March 2010. The study adopted a cross-sectional approach
with a sample size of 67 patients. All adult patients who had been diagnosed with either breast or
head and neck cancers for at least three months were included in the study. Patients were enrolled
from the Day-care chemotherapy and radiation therapy units. Interviews were conducted from the
patients and/or family members after written consent was taken from all participants. Data was
collected using a structured pre-tested questionnaire. Interviews were conducted by a medical student
after initial pilot testing. Questions included demographics, family income, treatment costs, insight
regarding the treatment and expectations of the patients and families. Data was analysed using
commercially available software package for social science (SPSS) version 17. All costs were
estimated as Rupees per month and later converted into dollars for analysis. The conversion rate of
2009-2010 was used and applied to other studies for comparison. Descriptive analysis was carried out

46
for patients’ demographics and clinical characteristics. Means with standard deviations were
calculated for continuous variables and proportions were calculated for categorical variables. Chi-
square test was used for Univariate analysis for significance of categorical variables in determining
perceived level of burden and cost anticipation of the treatment. Logistic regression was done for
same categorical variables in multivariate analysis. The significance level was set at 5%. Student’s t-
test was applied for multiple values of test variables. The result showed that, the mean and median
monthly income of these patients was 996.4 USD and 562.5 USD respectively. Comparatively the
mean and median monthly cost of cancer care was 1093.13 USD and 946.42 USD respectively. The
cost of the treatment either fully or partially was borne by the family in most cases (94%). The
financial burden of cancer was perceived as significant by 28 (42%) patients and unmanageable by 18
(27%) patients. This perceived level of burden was associated significantly with average monthly
income (p = <0.001). It was concluded that the financial burden of cancer care is substantial and can
be overwhelming. There is a desperate need for treatment support programmes either by the
government or other welfare organisations to support individuals and families who are already facing
a difficult and challenging situation.
Akpan-Idiok and Anarado (2014) conducted a study on the perceptions of the burden of care-giving
by informal caregivers of cancer patients attending University of Calabar Teaching Hospital, Calabar,
Nigeria using cross-sectional descriptive design with a sample size of 210 care givers providing care
to advanced cancer patients. Purposive sampling technique was used to select the care givers. The
sampling method allowed for wider coverage of the study respondents. The population included all
advanced (stage iii and iv) cancer patients in the study area. The participants of the study cut across
all ethnic groups and diversified culture from within and outside the state. Data were collected using a
research developed questionnaire and standardized Zarit Burden Interview Scale (ZBIS) with 22

47
items. Data collected were analyzed using mean, standard deviation, percentages and Chi-square test
with the help of SPSS version 18 and Predictive Analytical Software 19.0 software. The sum of
burden was achieved by adding the scores of all items with a range of 0-88 with higher scores
indicating severity (higher level) of burden. The results indicated that the caregivers were in their
youthful and active economic age, dominated by females, Christians, spouses, partners and patients.
The burden levels experienced by the caregivers were as follows: severe (46.2%), moderate (36.2%)
and trivial of no burden (17.6%). The forms of burden experienced were physical (43.4%),
psychological (43.3%,), financial (41.1%) and social (46.7%). Psychological and social forms of
burden had the highest weighed score of 228 in terms of magnitude of burden. The result further
showed that there was a significant (p = 0.001) and inverse association between caregivers’
functional ability. The level of burden also increased significantly (p = 0.000) with the duration of
care, while there was also a significant (p = 0.01) relationship between care givers’ experience of
burden and their desire to continue care giving. It was concluded that care giving role can be
enhanced by provision of interventions such as formal education programme on cancer, care giving,
oncology, home services along side with transmural care.
Asuzu and Elumelu (2013) carried out a study to assess the cancer patients’ quality of life (QOL) and
coping mechanisms in Radiotherapy Department of the University College Hospital, Ibadan. The
purpose of the study was to assess the relationship between cancer patients’ QOL dimensions and
coping strategies in the radiotherapy Department with a sample size of 237 cancer patients. Data was
collected on clinic days from all available and consenting cancer patients who were receiving
treatment at the Radiotherapy Department. The result was analyzed using mean, percentages and Chi-
square test. The result showed the respondents age range of 15-95 years with a mean age of 49.9
years. There was significant inverse relationship between physical well-being with behavioural

48
disengagement, venting, planning and self-blame (p < 0.05). Social/family well-being has significant
linear relationship with active coping, emotional support, positive reframing, instrumental support,
acceptance and religion (p < 0.05); emotional well-being has significant inverse relationship with
behavioural disengagement and self-blame (p <0.05); functional well-being has significant linear
relationship with active coping, instrumental support and acceptance (p < 0.05). It was concluded that
it is important to assess cancer patients for the kind of coping strategies they are adapting to use in
coping with their cancer burden, thereby guarding against lower QOL due to negative coping
strategies. Intervention programmes could be developed to help cancer patients adopt more positive
and effective coping strategies to improve patients’ QOL.
Mayston, Guerra, Huang, Sosa, Uwakwe, Acosta et al (2014) explored the economic and social
effects of care dependence in later life. The study used mixed methods. It was focused on two
countries in Latin America (Peru and Mexico), China and Nigeria. The study was based on 10/66
survey catchment areas in four countries; China, Peru, Mexico and Nigeria. At the baseline of the
10/66 survey, the Peru sites comprised urban catchment areas (1381 older people sampled in Lima
Cercado and San Miguel in the capital city, Lima) and rural sites (n = 552 in Cerro Azul, Imperial,
Nuevo Imperial, Quilmana, San Luis, San Vicente in Canete coastal province). In Mexico we also
sampled urban (n = 1003 in six districts in Tlalpan, Mexico City) and rural (n = 1000 in nine villages
in Morelos, a mountainous district 70 km from Mexico City) catchment areas. The urban site in
China was Xicheng, close to Tiananmen Square (n = 1160), while the rural site comprised 14 villages
in Daxing, a rural district 40 kilometres away (n = 1002). In Nigeria they sampled 1132 older people
in seven mainly rural communities in Dunukofia, Anambra State. The surveys comprised baseline
surveys of health, socioeconomic circumstances and care arrangements, to be repeated three to four

49
years later with the intension of going back to these households to make a detailed assessment of the
overall economic status and the use of health services by all family members. They compare
households where; an older resident became dependent between baseline and follow-up (incident
care); one or more older people were dependent at both time points (chronic care), and no older
residents had needs for care (control households) for household income, consumption, healthcare
expenditure and economic strain. In each of the four countries, six detailed household 'case studies' to
explore in more depth the economic impacts of dependence, and the social relations between
household members and others in their network is being carried out. All households meeting criteria
for incident or chronic care were selected for inclusion in the INDEPT study. In each site, control
households equivalent in number to the sum of incident and chronic care households were selected in
each site, at random from all those eligible, and batch matched to care households for the age of the
oldest resident. For each selected household, the aim is to conduct a household interview with a
suitably qualified key informant (usually the self-defined head of household), brief interviews with
each of the surviving index older people, and an informant interview for each older person to provide
an independent perspective on their health and needs for care. Data collection involved the detailed
household interviews are to be conducted masked to the household group status. Masking was not
possible in Nigeria, in which setting they conduct incidence phase interviews selecting all incident
and chronic care households, and every fourth control household for the INDEP study. The result
showed the prevalence of dependence in the baseline survey, and the care giving context for
dependent older people in the four countries (seven sites). The norm is to live with adult children or
children-in-law. Three generation households, including children under the age of 16 are common in
all sites other than urban China. Care giving is mainly done by women, although men were more
likely to be nominated as the principal carer in China. Carers often report giving up or cutting back on

50
work to care, although this arrangement was less common in Lima and Beijing, where paid carers are
often employed. Caring roles are commonly shared with other informal carers, other than in China,
where an isolated main carer seems to be the norm. Care giving, as in high income countries, is often
associated with considerable psychological strain.
Elumelu, Asuzu, and Akin-Odanye (2012) conducted a study on the impact of active coping, religion
and acceptance on quality of life of patients with breast cancer in the department of radiotherapy,
University College Hospital (UCH), Ibadan using descriptive survey design with a sample size of 110
patients with breast cancer receiving treatment at the radiotherapy clinic in UCH. Data was collected
using the Functional Assessment of Cancer Therapy-Breast (FACT-B) V, 4 Quality of life
Questionnaire (QOL) and Carver’s Brief Cope Questionnaire. Data was analyzed using mean
standard deviation and percentages. Chi-square test was used to test for association. The result most
pertinent to this study showed a significant difference between participants who used active coping,
religious coping and acceptance more than those who did not in the overall QOL (p <0.05) as well as
in some of the QOL dimensions. It was concluded that significant difference exist in the QOL of
patients with breast cancer based on the coping style they adopt. Patients with breast cancer should be
helped to adopt coping styles that would enhance their QOL.
Vicens, Zefra, Moreno-cresp, Ferrer and Marcos-Gragera (2014) carried out a study on the incidence
variation of prostrate and cervical cancer according to socio-economic level in Girona Health Region
(GHR). It was an explanatory population based study which included all the inhabitants in the GHR
in the period 1993-2006. The study population was 670,096 (339,839 were males and 330,257
females). In order to assess prostrate/cervical cancer risk, Besag, York and mobile (BYM)’s spatial-
temporal version of the model were used and four random effects were introduced: (non-spatial)

51
unstructured variability, spatial dependency, temporal dependency and spatial-temporal interaction.
As an explanatory variable, a deprivation index was introduced at the census tract level. The
percentage of the population between 45-64 years of age and over 65 was also considered as
explanatory variables. The results showed that in the case of prostate cancer, all the variables which
were introduced into the mode revealed a significant correlation with the risk, except for the second
quintile of the deprivation index. As the index increased the correlation became negative and lower.
Thus, the correlation between the relative risk and the two age bands proved to be lower, the higher
the age was. In the case of cervical cancer, only the correlation between the over 65 age band and the
relative risk was found to be statistically significant and positive. It was concluded that in the case of
prostate ca, the results obtained in the GHR are in line with similar analyses. However, in the case of
cervical cancer, no significant relationship between incidences in this location or economic status was
found.
Clegg, Reichman, Miller, Hankey, Singh, Lin, et al (2010) conducted a study on the impact of
socioeconomic status on cancer incidence and stage at diagnosis: selected findings from the
surveillance, epidemiology and end results; National Longitudinal Mortality study (NLMS) using
records of cancer patients diagnosed in 1973-2001 when residing 1 of 11 SEER registers were linked
with 26 NLMS cohorts. The total number of SEER matched cancer patients that were also members
of an NLMS cohort was 26,844, of these patients, 11464 were included in the incidence analyses and
15,357 in the late-stage diagnosis analyses. Matched patients (used in the incidence analysis) and
unmatched patients were compared by age group, sex, race, ethnicity, residence area, year of
diagnosis and cancer anatomic site. Cohort-based cancer incidence and stage of diagnosis was
evaluated. Incidence analyses were conducted for all census combined and for six major cancers

52
separately: lung and bronchus, colon/rectum, breast, prostate, uterine cervix and melanoma of the
skin as well as age specific cancer incidence rate. The result showed that men and women with less
than a high school education had elevated lung cancer rate ratio of 3.01 and 2.02 respectively, relative
to their college educated counterparts. Those with family annual income less than 12,500 U.S dollars
had incidence rates that were more than 1.7 times the lung cancer incidence rate of those with
income 50,000 U.S dollars or higher. Lower income was also associated with a statistically
significantly increased risk of distant-stage breast cancer among women and distant-stage prostate
cancer among men. It was concluded that, socioeconomic patients in incidence varied for specific
cancer while such patterns for stage were generally consistent across cancers, with late stage
diagnosis being associated with lower SEES. These findings illustrate the potential for analyzing
disparities in cancer outcomes according to a variety of individual-level socioeconomic, demographic
and health care characteristics, as well as by area measures available in the linked data base.
Adams and Ke (2008) carried out their study on coping with out-of-pocket health payment: empirical
evidence from 15 African countries (Burkina Faso, Chad, Congo, Cote d'ivoire, Ethiopia, Ghana,
Kenya, Malawi, Mali, Mauritania, Namibia, Senegal, Swaziland, Zambia, Zimbabwe) with the
purpose of providing evidence to policy-makers in designing financial health protection mechanisms
using a series of longit regression to exploit correlating with greater likelihood of selling assets,
borrowing or both to finance health care. It was a cross- sectional study which was based on a multi-
stage clustered random sample of households designed to be nationally representative. The instrument
for data collection was questionnaire which was standardized across countries to facilitate
international comparisons. Sample size ranged from 2754 in the Congo to 5276 in Malawi. The
household questionnaire was administered to the household members most knowledgeable about the
53
health employment and expenditures of the house hold. Household out-of-pocket payments for out
patient and routine expenses in local currency units were collected for a 4 weeks recall period.
Household out-of-pocket payments for inpatient services were collected for both a 4-week and a one-
week recall period.
The average partial effects for different levels of spending on inpatient care were derived by
computing the partial effects for each observation and taking the average across the sample. Data
used in the analysis were from 2002-2003 world health survey which asked how households had
finance out-of-pocket payments over the previous year. Household selling assets or borrowing money
were compared to those that financed health care from or savings. Those that used insurance were
excluded. For the analysis, a value of 1 was assigned to selling assets or borrowing money and a
value of 0 to other coping mechanisms. The findings revealed that, coping through borrowing and
selling assets ranged from 23% of households in Zambia to 68% in Burkina Faso. In general, the
highest income groups were less likely to borrow and sell assets, but coping mechanisms did not
differ strongly among lower income quintiles. Households with higher inpatient experiences were
significantly more likely to borrow and deplete assets compared to those financing outpatient care or
routine medical expenses, except in Burkina Faso, Namibia and Swaziland. In eight countries, the
coefficient on the highest quintile of inpatient spending had a p value below 0.01. It was concluded
that in most African countries, the health financing system is too weak to protect households from
health shocks. Borrowing and selling assets to finance health care are common. Formal prepayment
schemes could benefit many households and an overall social protection network could help to
mitigate the long-term effects of ill health on household well-being and support poverty reduction.

54
Marti et al (2015) conducted a study on the economic burden of cancer in the UK: a study of
survivors treated with curative intent. Patient level data were collected over a 3 month period, 12-15
months spot diagnosis to estimate the monthly societal cost incurred by cancer survivors. Self-
reported resource utilization data were obtained via the electronic patient reported outcomes from
cancer survivors system and included community based health and social care, medications, travel
costs and informal care. Health costs were retrieved through data linkage. Multivariate regression
analysis was used to examine cost predictors. The result revealed that, overall, 298 patients were
included in the analysis, including 136 breast cancer, 83 colorectal cancer and 79 prostate cancer
patients. The average monthly societal cost was 409 US dollars and was incurred by 92% of patients.
This was divided into costs to the National Health Insurance services with mean of 279 US dollars.
Patients’ out of pocket expenses mean is 40 US dollars. The cost of informal care mean is 110 US
dollar. The distribution of cost was skewed with a small number of patients incurring very high costs;
Multivariate analysis showed higher societal costs for breast cancer patients. Significant predictors of
OOP costs included age and socio-economic deprivation. It was concluded that, economic burden of
cancer survivorship is unevenly distributed in the population and that cancer survivors may still incur
substantial cost over 1 year post-diagnosis. In addition, this study illustrates the feasibility of using an
innovative online data collection platform to collect patient-reported resource utilization information.
Summary of Literature Review
The literatures reviewed provides an overview of the concept of cancer, economic burden including
the direct and indirect cost of cancer treatment and payment coping mechanism of cancer. Cost-of
illness framework was used in this study. It is suitable for this study because this framework captures
the necessary data from the cancer patients on their economic burden.

55
From empirical literature reviewed of economic burden and payment coping mechanism of cancer
patients, the financial burden of cancer care is directly on the patients and relative, the social impact
of cancer care is associated with psychological stress and the cost distribution of cancer among
different socioeconomic groups shows disparities in cancer outcomes according to a variety of
individual-level socioeconomic status.
Review of previous related studies showed that many studies were carried out on cancer, but few
were done on cost distribution of cancer among different socioeconomic groups. This study will
therefore fill the gap.

56
CHAPTER THREE
RESEARCH METHODS
This chapter focused on the research methods adopted for this study which includes: research design,
area of study, target population, sample and sampling procedure, inclusion criteria, instrument for
data collection etc.
Research Design
The research design adopted in this study was a descriptive cross-sectional survey and it involves the
description of the summary of characteristics from a given population (to observe, describe and
document) and to show the need for change. The descriptive survey allows one to describe things as
they exist in their natural setting. This is considered suitable for the phenomenon being studied
(Isangedigilis, Joshua, Asim and Ekuri, 2004).
Area of Study
Jos University Teaching Hospital (JUTH) was the area of study and it is one of the most active
tertiary hospitals in the Middle Belt. It is located in Jos East Local Government Area of Plateau State
of the North Central Zone of Nigeria. The hospital initially, Plateau State Government Hospital was
later taken over by the Federal Government of Nigeria in early 1970s. The hospital serves both self
and health system referred from the 17 local governments of Plateau State as well as its neighbouring
states – Bauchi, Taraba, Nasarawa, Benue, and parts of Kaduna State. Due to the specialist services it
renders, there is increasing patient attendance in the Oncology unit.

57
Target Population
The target population for this study were all the in and out patients receiving treatment for cancer at
the oncology clinic in Jos University Teaching Hospital, Plateau State. It was estimated that about
276 received care from the Oncology unit of the hospital in the last one year (clinic
register/admission records).
Sample
A sample size of 163 patients was determined using the formula; n = N 1+N (e)2 By (Araoye, 2004). Where; n = required sample
N = total population (sample frame)
e = error of tolerance which is 0.05 at 95% confidence level
1 = constant (Appendix 1)
In order to cater for attrition or non response, 10% provision was made giving the final sample size of
179.3 approximately 179 patients.
Inclusion Criteria
- All patients aged 18 years and above, diagnosed of cancer and are receiving treatment in Jos
University Teaching Hospital for the past 1 year either as outpatient or inpatient or within the
period of study.
- Patients who are conscious and are actively involved in the management of their condition.
- Willingness to participate in the study.
- Available at the time of study.

58
Sampling Procedure
Patients were consecutively recruited in the oncology ward and as they attended the clinic. The
attendance register was used as sampling frame to select participants who met the inclusion criteria.
The clinic runs from Monday to Friday. The recruitment continued until the sample size was
completed.
Instrument for Data Collection
An interviewer administered questionnaire was used to source information from the subjects. The
questionnaire was developed from literature search on economic burden of cancer and the four stated
objectives. The questionnaire was divided into sections. Section ‘A’ demographic data. Section ‘B’
economic burden of cancer patients. Section ‘C’ payment coping mechanisms of cancer and section
‘D’ assessed household assets of the patients. The respondents were to choose and tick the options
that best described their views on the issue. A total of 26 items were generated (Appendix 11)
Validity of Instrument:
The face and content validity of the instrument was determined through the judgment of the project
supervisor and three lecturers from the Department of Nursing Sciences and one clinical expert on
oncology. They were given a copy of the instrument, purpose of the study and the research questions
to assess the relevance of content, clarity of statements and logical accuracy of the instrument. Their
suggestions were used to modify the questions.

59
Reliability of the study
A pilot test was conducted on 18 cancer patients attending cancer clinic at Bingham University
Teaching hospital Jos using split-half method. The data collected was analyzed using Spearman-
Brown coefficient which gave a reliability of 0.82. This showed that the instrument was reliable
(Appendix 111).
Ethical consideration
Ethical approval was obtained from the ethical committee of Jos University Teaching Hospital, Jos.
Informed consent was obtained from each participant prior the administration of the instrument. They
were assured that all information given will be treated confidentially (Appendix IV).
Procedure for Data Collection
With the ethical approval and letter of introduction from the Department of Nursing, administrative
permit was obtained from the Heads of units in charge of oncology clinic. Two research assistants
were trained on the purpose of the study and how to administer the instrument. The researcher and
assistants administered the questionnaire to each participant that met the inclusion criteria as they
waited to be attended to in the clinic and in the wards. Those who could not read or write were
assisted by reading out the questions to them and allowing them to respond to each question. Data
collection lasted for a period of three weeks.

60
Method of Data Analysis
The data gathered were analyzed using descriptive statistics such as frequency, percentages, mean
and standard deviation. The direct cost was derived from costs incurred in tests, drugs/medications,
insurance premium and co-payment, transportation etc, using the ‘bottom-up’ approach which was
based on individual unit of services performed. This uses average cost of service to estimate cost and
applies this data to the total number of health encounters to the disease (cancer) to arrive at an
estimate of the health cost of the disease. The indirect cost was assessed using the human capital
approach. Here, the average wage rate/replacement cost was used to input values. Productivity losses
from pre-mature death and disability as lost of earning as a surrogate daily wage rate was used for
work absence. Chi-square was used to test the association between the socioeconomic groups and
payment mechanisms utilized by the patients as well as cost distribution of different socio-economic
groups. Rejection or acceptance was based on 0.05 level of significance. All the analyses were done
using SPSS version 20.0 computer software programme. All costs were estimated in naira and
converted in dollar for analysis.

61
CHAPTER FOUR
PRESENTATION OF RESULTS
This chapter dealt with presentation of results based on the research objectives. One hundred and seventy nine
(179) questionnaires were administered, same were returned. The results are presented in tables.
Table 1: Demographic characteristics of respondents (n = 179) Demographic Characteristics F % Age 18 - 27yrs
9
5.0
28 - 37yrs 32 17.9 38 - 47yrs 64 35.8 48 - 57yrs 40 22.3 58 - 67yrs 23 12.8 68 - 77yrs 11 6.1 Minimum Age 18 Maximum Age 77 Mean + Std. Dev. 46.02 + 12.32 Sex Male
70
39.1
Female 109 60.9 Marital Status Married
115
64.2
Single 25 14.0 Divorced 12 6.7 Widowed 27 15.1 Employment Status Unemployed
52
29.1
government employed 64 35.8 private sector employed 24 13.4 self employed 26 14.5 Trader 2 1.1 Retiree 9 5.0 Farmer 1 .6 Menial labour 1 .6 Highest Educational Level Primary
22
12.3
Secondary 44 24.6 Tertiary 85 47.5 None 28 15.6 Type of Cancer breast cancer
72
40.2
cervical cancer 29 16.2 prostrate cancer 48 26.8 Colon cancer 7 3.9 lung cancer 5 2.8 Liver Carcinoma 7 3.9 Colorectal cancer 3 1.7 Gastric cancer 4 2.2 Lymph sarcoma 3 1.7 Hand cancer 1 .6

62
As presented on Table 1, the respondents’ mean age was 46.02 + 12.32 years with the minimum age
being 18 years and maximum age being 77 years. Majority 109(60.9%) of the sampled respondents
were females while 70(39.1) were males. The respondents consisted majorly of married persons
115(64.2%), 25(14%) single, 12(6.7%) divorced and 27(15.1%) widowed. Respondents that were
government employed had a higher distribution of 64(35.8%) followed by the unemployed
52(29.1%), private sector employed 24(13.45%), self employed 26(14.5%), trader 2(1.1%), retiree
9(5%) while respondents that engaged in farming and menial labour were the least 1(0.6% each). In
term of educational level, 85(47.5%) of the respondents had tertiary education as their highest
educational level, secondary 44(24.6), primary 22(12.3%) while none was 28(15.6%). A higher
percentage 40.2% (72) of the respondents had breast cancer followed by those that had prostate
cancer 48(48%), cervical cancer 29(16.2%), colon cancer 7(3.9%), lung cancer 5(2.8%), liver
carcinoma 7(3.9%), colorectal 3(1.7%), gastric cancer 4(2.2%), lymph sarcoma 3(1.7%) and only 1
(0.6%) respondent had hand cancer.
Objective 1: To assess the direct medical cost of cancer incurred by patients and their households.

63
Table 2: Direct medical cost of cancer of cancer incurred by patients and their households. (n = 179)
Items F % Duration of Treatment < 6months
53
29.6
7 to 12months 48 26.8 13 to 18months 11 6.1 19 to 24months 29 16.2 25 to 30months 6 3.4
> 31months 32 17.9 Minimum 1 Maximum 72 Mean + Std. Dev. 17.06 + 14.30 Frequency of Check-Up Weekly
23
12.8
Bi-weekly 34 19.0 Three weekly 6 3.4 Monthly 64 35.8 Six weekly 31 17.3 Eight weekly 15 8.4 Quarterly 4 2.2 Four monthly 2 1.1 Minimum Weekly Maximum Four Monthly Average Monthly
Cost of pre-diagnosis Tests < N40,000
105
58.7
N40,000 - N79,999 45 25.1 N80,000 - N119,999 23 12.8 N120,000 and above 6 3.4 Minimum 2,000 Maximum 180,000 Mean +Std Dev. 43,864.91 + 34001.25 Monthly cost of managing illness less than N40,000
129 72.1
N40,000 - N79,999 42 23.5 N80,000 - N119,999 4 2.2 N120,000 and above 4 2.2
Minimum 2,000
Maximum 180,000
Mean + Std. Dev. 30,757.95 + 27,325.82 Received Treatment from elsewhere Yes
43
24.0
No 136 76.0 Place of Treatment (n = 43) Herbal
6
14.0
Private hospital 12 27.9 Kaduna 2 4.7 Enugu 1 2.3 Nassarawa 1 2.3 Bauchi 7 16.3 Plateau 3 7.0 Benue 2 4.7 ABUTH 2 4.7 FMC Keffi 1 2.3 India 2 4.7 Kano 2 4.7 Calabar 1 2.3 Jigawa 1 2.3 Cost of Treatment (n = 43) less than N40,000
36
83.7
N40,000 - N79,999 3 7.0 N80,000 - N119,999 1 2.3 N120,000 – N179,000 0 0.0 N180,000 and above 3 7.0 Minimum 5,000 Maximum 360,000 Mean + Std. Dev. 39,952.38 + 66,841.62

64
Based on the presentation in Table 2, the minimum time (months) spent on treatment by a patient is 1
month while the maximum time is 72 months. The mean duration of treatment by a patient is 17.06 +
14.30 months. However, the duration of treatment for higher percentage 53(29.6%) of the
respondents was 6 months and below followed by those whose duration was 7 to 12 months
48(26.8%) respondents.
The minimum frequency for check-up appointment by a respondent is weekly while the maximum
frequency by a respondent is four monthly. The average frequency for check-up appointments among
the respondents is monthly.
The minimum cost of pre-diagnosis tests was N2,000 while the maximum cost was N180,000. The
average cost of pre-diagnosis tests among the patients was N43,864.91+ 34,001.25. Over half of the
patients (58.7%) spent less than N40,000 as cost of pre-diagnosis tests.
The minimum monthly cost of managing the illness among the patients was N2,000 while the
maximum monthly cost was N180,000. The mean monthly cost of managing the illness among the
patients is N30,757.95+ 27.325.82. Majority 129(72.1%) of the respondents spend less than N40,000
monthly managing the illness.
Only 43 (24%) patients have received treatment from elsewhere. Out of this number, 12 (27.9%)
received treatment from private hospitals, 6 (14%) received from herbal centres. It is worth noting
that among other patients that received treatment from other places, like different states in Nigeria, 2
(4.7%) received treatment from India. The minimum cost of treatment was N5,000 while the
maximum cost of treatment was N360,000. The average cost of treatment was N39,952.38+
66,841.62. Majority 36(83.7%) of the patients incurred less than N40,000 as cost of treatment from
these other places.
Objective 2: To assess the indirect medical cost of cancer incurred by patients and their households.

65
Table 3: Indirect medical cost of cancer incurred by patients and their households. (n = 179)
Items F % Source of Income Rent
1
0.6
Family members 24 13.4 Salary 74 41.3 Pettytrading 11 6.1 Farming 19 10.6 Business 20 11.2 Pension 8 4.5 Transporter 2 1.1 Menial Job (labour) 14 7.8 Friends and Relations 3 1.7 Artisan 3 1.7 Monthly pay/earnings < N50,000
123
68.7
N50,000 - N99,999 34 19.0 N100,000 - N149,999 12 6.7 N150,000 - N199,999 4 2.2 N200,000 - N249,999 2 1.1 N250,000 - N299,999 2 1.1 N300,000 and above 2 1.1 Minimum 2,000 Maximum 350,000 Mean + Std. Dev. 49,587.88 + 51,809.54 Days absent from work because of illness no day
109
60.9
1 - 5 days 16 8.9 6 - 10 days 17 9.5 11 - 15 days 3 1.7 16 - 20 days 34 19.0 Minimum 0 Maximum 26 Mean + Std. Dev. 7.23 + 9.78 Employment status of person accompanying for treatment Artisan
6
3.4
Civil/Public servant 75 41.9 Teaching 4 2.2 Petty trading 2 1.1 Unemployed 63 35.2 Farmer 12 6.7
Business 15 8.4
Retiree 2
1.1
Income of the person less than N50,000
31
17.3
N50,000 - N99,999 34 19.0 N100,000 - N149,999 7 3.9 N150,000 - N199,999 8 4.5 N200,000 - N249,999 3 1.7 N250,000 - N299,999 6 3.4 N300,000 and above 8 4.5 Do not know 82 45.8 Minimum 2,000 Maximum 550,000 Mean + Std. Dev. 105,159.28 + 108,342.16 Duration taken to see doctor on appointment date 30 minutes and below
24
13.4
31 - 60 minutes 50 27.9 61 - 90 minutes 4 2.2 91 - 120 minutes 44 24.6 more than 120 minutes 47 26.3 Not Sure 10 5.6 Minimum 15 min. Maximum 360 min. Mean + Std. Dev. 116 + 80.23 mins. Time taken to get to JUTH on appointment 30 minutes and below
23
12.8
31 - 60 minutes 48 26.8 61 - 90 minutes 6 3.4 91 - 120 minutes 43 24.0 more than 120 minutes 52 29.1 Not Sure 7 3.9 Minimum 1 min. Maximum 360 mins. Mean + Std. Dev. 117.24 + 76.35

66
Tables 3 and 4 addressed objective 2. As presented in Table 3, the source of income for the higher
percentage 74(41.3%) of the respondents is salary, 24(13.4%) family members, business 20(11.2%),
farming 19(10.6%), petty trading 11(6.1%), pension 8(4.5%), transporter 2(1.1%), menial job
14(7.8%), friends and relations 3(1.7%), Artisan 3(1.7%) while 1 (0.6%) respondent’s earnings is
from rent.
The minimum amount earned by a patient is N2000; the maximum amount earned by a patient is
N350,000 while the mean amount earned by a patient is N49,587.88 + 51,809.54. Majority
123(68.7%) of the respondents earn less than N50,000.
Most of the respondents 109(60.9%) have not been absent from work because of the illness. The
maximum number of days absent from work is 26 days and the mean number of days absent from
work is 7.23 + 9.78 days.
The employment status of the persons accompanying a higher percentage 75(41.9%) of patients for
treatment is civil/public servants followed by the unemployed 63(35.2%) while the least percentage
2(1.1%) are retirees. The minimum income for the persons accompanying the patient is N2,000; the
maximum is N550,000 and the mean income is N105,159.28 + 108.342.16. 82. 82(45.8%) patients do
not know how the persons accompanying them earns.
The minimum duration taken to see a doctor on appointment date is 15 minutes; the maximum
duration is 360 minutes and the mean duration is 116 + 80.23 minutes. The minimum time taken to
get to JUTH on appointment is 1 minute; the maximum time is 360 minutes while the mean time
taken to get to JUTH on appointment is 117.24 + 76.35 minutes.

67
Table 4: Indirect Medical Cost of Care
( n =179)
Indirect Costs Minimum Maximum Mean Std. Dev. Minutes taken to get to JUTH on appointment date 1.00 360.00 117.24 76.35 Time taken to see doctor on each appointment date 15.00 360.00 116.00 80.24 Days absent from work because of sickness within the last one month
.00 26.00 7.27 9.78
Monthly Patients’ Total Income 1500.00 1040000.00 65978.74 104036.97 Monthly Patients’ Total Expenditure 800.00 600000.00 43916.28 56070.33 Monthly earnings of Person accompanying patient 2000.00 550000.00 105159.28 108342.16 Patient’s Monthly Loss .00 661818.18 10852.60 52987.13 Accompanying Persons’ Monthly Loss .00 177272.73 7914.73 20676.63 Total Monthly Loss .00 693636.36 18126.27 66559.08 Patient’s Annual Loss .00 7941818.18 130231.25 635845.62 Accompanying Persons’ Annual Loss .00 2127272.73 94976.75 248119.61 Total Annual Loss .00 8323636.36 217515.19 798708.95 Patient’s Annual Loss as % of Annual Income .00 106.06 11.38 19.13 Patient’s Annual Loss as % of Annual Expenditure .00 5484.68 50.06 421.98
Table 4 showed that patients spent a mean time of 117.24+ 76.35 minutes to JUTH on appointment
date. The mean length time of 116 + 80.24 minutes was spent by a patient in trying to see the doctor
on each appointment. The mean number of days absent from work by the patients is 7.27 + 9.78.
The mean monthly patients’ total income was N65,978.74 + 104,036.97 and the mean monthly
patients’ expenditure was N43,916.28 + 56,070.33. The mean monthly earnings of persons
accompanying patients was N105,159.28 + 108,342.16.
The mean patients’ monthly loss was N10,852.60 + 52,987.13; the accompanying persons’ monthly
loss was N7,914.73 + 20,676.63; the mean total monthly loss was N18,126.27 + 66,559.08; the mean
patients’ annual loss is N130,231.25 + 635,845.62; the mean accompanying persons’ annual loss is
N94,976.75 + N248,119.61 and the mean total annual loss was N217,515.19 + 798,708.95. The
mean patients’ annual loss as a percentage of their mean annual income was 11.38 + 19.13% while as
a percentage of their mean annual expenditure was 50.06 + 421.98.

68
Objective 3: Estimate the cost distribution among different socio-economic groups.
Table 5: Household Assets and social status of the respondents. Asset F % Radio 147 82.1 Television 144 80.4 Air Conditioner 15 8.4 Bicycle 20 11.2 Motorcycle 16 8.9 Car 59 33.0 Fridge 56 31.3 Generator 38 21.2 Gas Cooker 31 17.3 Electric Fan 56 31.3 Washing Machine 5 2.8 Microwave Oven 12 6.7 Personal Computer 18 10.1 Social Status Status Poorest 142 79.3 Poorer 28 15.6 Least poor 9 5.0 Total 179 100.0
Tables 5 and 6 addressed objective 3. Based on Table 5, Radio 147(82.1%) and Television
144(80.4%) were the household assets owned by most of the patients while washing machine 5(2.8%)
was the household asset owned by the fewest number of patients. In determining the socio-economic status of the patients, ownership of radio, television, bicycle and
electric fan was scored 1; ownership of motorcycle, fridge, generator, gas cooker, washing machine,
microwave oven and personal computer were scored 2 while the ownership of air conditioner and car
was scored 3. Based on the highest total score was 24 and the least score was 0. Patients that scored
from 0 to 7 were termed to be the poorest; patients that scored 8 to 15 were termed to be poorer while
patients that scored 16 and above were termed to be the least poor.

69
Data on social status showed that 142 (79.3%) patients were ranked the poorest, 28 (15.6%) patients
are ranked poorer while 9 (5%) patients are ranked least poor.
Table 6: Monthly Income and Expenditure among different socioeconomic groups.
( n =179) Mean monthly income Minimum Maximum Mean Std. Dev.
Wages/salaries 5000.00 1040000.00 73963.6015 122644.76874
Farming/gardening 833.33 100000.00 18455.8557 21427.18515 Petty trading 2000.00 60000.00 10437.5000 12186.33634 Small and medium scale enterprises 3500.00 100000.00 25236.8421 25600.76411 Large scale enterprises 100000.00 250000.00 137500.0000 75000.00000
Rent 1666.67 166666.67 23565.1047 34393.57375 Pasturing 10000.00 50000.00 23000.0000 17175.56404 Allowances from children/relations 2000.00 80000.00 23978.2609 20362.80829 Security guards 0 0 0 0Housekeeping/housewifery 1500.00 10000.00 6100.0000 3781.53408 Transport business 5000.00 180000.00 52000.0000 73194.94518 Pension 10000.00 45000.00 28250.0000 13593.59093 Other sources 1000.00 50000.00 11013.8892 14433.83677 Total Income 1500 1040000.00 65978.7426 104036.9676
Mean Monthly Expenditure Items Minimum Maximum Mean Std. Dev. Food (purchased) 100.00 100000.00 11793.9189 11803.11977 Food (produced by your family if it were bought how much will it cost)
416.67 100000.00 11235.9570 16627.68651
Clothing 416.67 50000.00 6409.0044 9337.31740
Rent 333.33 80000.00 7531.4330 12737.93447
Healthcare 500.00 100000.00 15448.0676 16987.80396 Cooking fuel 100.00 28000.00 3825.4098 4209.81614 Educational expenses 833.33 200000.00 16696.3468 26598.17722 Durable Household Goods 2000.00 18000.00 6142.8571 5928.14112 Community welfare 200.00 10000.00 2417.9488 2147.64426 Transportation 500.00 50000.00 6608.5714 9042.64843 Others expenses 1000.00 20000.00 5636.3636 5371.64271 Total Expenses 800 600000.00 43916.2794 56070.32647
Table 6 showed that the minimum average monthly total income of the patients was N1,500 while
the maximum average monthly total income of the patients was N1,040,000. The mean monthly total
income of the patients was N65,978.74 + 104,036.97. The minimum average monthly total expenses

70
of the patients was N800, the maximum mean monthly total expenses is N600,000 while the mean
monthly total expenses was N43,916.28 + 56,070.33.
Objective 4: Identify the payment coping mechanism utilized by different socio-economic groups
Objective 4: Identify the payment coping mechanism utilized by different socio-economic groups
Table 7: Payment Coping Mechanism and Ease in paying for cancer management
(n = 179) Payment Mechanism F %
Own money (salary, earnings, savings) 141 78.8
Borrowed money/loan 49 27.4
Sale of household mobile assets 3 1.7
Sales of lands 22 12.3
Community based support 8 4.5
Gift from friends and neighbours 53 29.6
Cancer association 2 1.1
Temporary stoppage of children’s education 3 1.7
Family members 84 46.9
Social welfare/social worker (waiver) 1 0.6
Skips appointments 4 2.2
Use alternative healthcare system 0 0.0
Other mechanisms
4 2.2
*Multiple responses were allowed
Difficulty in paying for cancer management
Very easy 14 7.8
Fairly easy 49 27.4 Difficult 61 34.1 Very difficult 55 30.7

71
Table 7 revealed that the payment coping mechanism utilized by most patients were, patients own
money (i.e. salary, earnings and/or savings) 141(78.8%), payment by family members was
84(46.9%). Result also revealed that 14 (7.8%) patients found it very easy in paying for their cancer
management, 49 (27.4%) patients find it fairly easy, 61 (34.1%) patients find it difficult while 55
(30.7%) patients find it very difficult in paying for their cancer management.
Hypothesis 1: There will be no significant difference in the cost distribution of cancer treatment
among different socio-economic groups.

72
Table 8: Difference in Cost Distribution among Socio-Economic Groups (n = 179) N Mean Std. Deviation Minimum Maximum F Sig.
Minutes taken to get to JUTH on appointment date
poorest 137 119.09 78.22 1.00 360.00
.761 .469 poorer 26 101.92 65.99 20.00 240.00 least poor 9 133.33 76.65 30.00 240.00 Total 172 117.24 76.35 1.00 360.00
Time taken to see doctor on each appointment date
poorest 134 119.40 85.10 15.00 360.00
.589 .556 poorer 26 101.73 49.82 30.00 180.00 least poor 9 106.67 78.10 30.00 240.00 Total 169 116.00 80.24 15.00 360.00
Days absent from work because of sickness within the last one month
poorest 142 7.13 9.63 .00 26.00
1.064 .347 poorer 28 9.07 10.81 .00 26.00 least poor 9 3.78 8.57 .00 26.00 Total 179 7.27 9.78 .00 26.00
Monthly Patients’ Total Income
poorest 132 42549.50 43958.16 1500.00 301666.67
19.728 .000 poorer 26 149169.87 205642.81 15000.00 1.04E+006 least poor 9 169277.78 131310.59 30000.00 403500.00 Total 167 65978.74 104036.97 1500.00 1.04E+006
Monthly Patients’ Total Expenditure
poorest 136 39135.42 57751.95 800.00 600000.00
2.531 .083 poorer 27 59284.57 41277.49 9333.33 165000.00 least poor 9 70055.56 58529.31 10000.00 168333.33 Total 172 43916.28 56070.33 800.00 600000.00
Monthly earnings of Person accompanying patient
poorest 74 81681.76 92899.63 2000.00 550000.00
10.377 .000 poorer 20 166300.00 110446.99 40000.00 450000.00 least poor 3 276666.67 175023.81 100000.00 450000.00 Total 97 105159.28 108342.16 2000.00 550000.00
Patient’s Monthly Loss
poorest 135 5641.35 14792.10 .00 112424.24
4.138 .018 poorer 26 37697.54 129406.50 .00 661818.18 least poor 9 11469.33 22674.01 .00 61136.36 Total 170 10852.60 52987.13 .00 661818.18
Accompanying Persons’ Monthly Loss
poorest 111 5530.12 13028.98 .00 72222.22
5.236 .006 poorer 22 12838.00 21565.99 .00 78787.88 least poor 8 27462.12 62326.43 .00 177272.73 Total 141 7914.73 20676.63 .00 177272.73
Total Monthly Loss
poorest 111 9707.01 24922.97 .00 165454.55
4.652 .011 poorer 21 54284.38 152224.52 .00 693636.36 least poor 8 40028.41 80045.57 .00 216666.67 Total 140 18126.27 66559.08 .00 693636.36
Patient’s Annual Loss
poorest 135 67696.24 177505.22 .00 1.35E+006
4.138 .018 poorer 26 452370.50 1552878.05 .00 7.94E+006 least poor 9 137631.87 272088.08 .00 733636.36 Total 170 130231.25 635845.62 .00 7.94E+006
Accompanying Persons’ Annual Loss
poorest 111 66361.49 156347.81 .00 866666.67
5.236 .006 poorer 22 154056.01 258791.86 .00 945454.55 least poor 8 329545.45 747917.21821 .00 2.13E+006 Total 141 94976.75 248119.60536 .00 2.13E+006
Total Annual Loss
poorest 111 116484.11 299075.63937 .00 1.99E+006
4.652 .011 poorer 21 651412.54 1826694.18092 .00 8.32E+006 least poor 8 480340.91 960546.86528 .00 2.60E+006 Total 140 217515.19 798708.95225 .00 8.32E+006
Patient’s Annual Loss as % of Annual Income
poorest 135 11.25 19.54660 .00 106.06
.523 .594 poorer 26 13.81 18.78328 .00 63.64 least poor 9 6.34 13.35071 .00 39.39 Total 170 11.38 19.12719 .00 106.06
Patient’s Annual Loss as % of Annual Expenditure
poorest 135 17.46 50.87918 .00 518.88
2.917 .057 poorer 26 231.98 1071.91017 .00 5484.68 least poor 9 13.55 25.38946 .00 67.15 Total 170 50.06 421.97594 .00 5484.68
significance level =0.05

73
Findings from the table showed that ,earnings of persons accompanying patients had varied
significantly among the socioeconomic groups (p = 0.00), as well as patients’ monthly loss (p =
0.018), accompanying persons’ monthly loss (p = 0.006), total monthly loss (p = 0.011), patients’
annual loss (p = 0.018), accompanying persons’ annual loss (p = 0.006) , total annual loss (p = 0.011)
, minutes taken to get to JUTH on appointment date (p = 0.469), time taken to see doctor on each
appointment date (p = 0.556), days absent from work because of sickness within the last one month (p
= 0.347), monthly patients’ total expenditure (p = 0.083). However, Patients’ annual loss as
percentage of annual income (p = 0.594) and patients’ annual loss as percentage of annual
expenditure (p = 0.057) did not vary significantly.
Hypothesis 2
There will be no significant difference between the payment coping mechanisms utilized by cancer patients and the
different socio-economic groups.

74
Table 9: Difference between Payment mechanisms Utilized by cancer patients and different
Socio-economic groups (n=-179)
Variables N Mean Std. Deviation
Minimum Maximum F Sig.
Own money (salary, earnings, savings)
Poorest 142 .7535 .43249 .00 1.00
2.669 .072 Poorer 28 .8929 .31497 .00 1.00 least poor 9 1.0000 .00000 1.00 1.00 Total 179 .7877 .41008 .00 1.00
Borrowed money/loan
Poorest 142 .3310 .47223 .00 1.00
6.040 .003 Poorer 28 .0714 .26227 .00 1.00 least poor 9 .0000 .00000 .00 .00 Total 179 .2737 .44713 .00 1.00
Sale of household mobile assets
Poorest 142 .0211 .14432 .00 1.00
.393 .676 Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .0168 .12873 .00 1.00
Sales of lands
Poorest 142 .1549 .36312 .00 1.00
3.335 .038 Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .1229 .32925 .00 1.00
Community based support
Poorest 142 .0423 .20188 .00 1.00
.449 .639 Poorer 28 .0714 .26227 .00 1.00 least poor 9 .0000 .00000 .00 .00 Total 179 .0447 .20721 .00 1.00
Gift from friends and neighbours
Poorest 142 .3028 .46110 .00 1.00
2.175 .117 Poorer 28 .3571 .48795 .00 1.00 least poor 9 .0000 .00000 .00 .00 Total 179 .2961 .45781 .00 1.00
Cancer association
Poorest 142 .0141 .11826 .00 1.00
.260 .771 Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .0112 .10541 .00 1.00
Temporary stoppage of children’s education
Poorest 142 .0211 .14432 .00 1.00
.393 .676 Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .0168 .12873 .00 1.00
Family members
Poorest 142 .4648 .50052 .00 1.00
.069 .934 Poorer 28 .5000 .50918 .00 1.00 least poor 9 .4444 .52705 .00 1.00 Total 179 .4693 .50045 .00 1.00
Social welfare/social worker (waiver)
Poorest 142 .0070 .08392 .00 1.00
.129 .879 Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .0056 .07474 .00 1.00
Skips appointments
Poorest 142 .0282 .16604 .00 1.00
.527 .591 Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .0223 .14822 .00 1.00
Use alternative healthcare system
Poorest 142 .0000 .00000 .00 .00
. . Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .0000 .00000 .00 .00
Other mechanisms
Poorest 142 .0282 .16604 .00 1.00
.527 .591 Poorer 28 .0000 .00000 .00 .00 least poor 9 .0000 .00000 .00 .00 Total 179 .0223 .14822 .00 1.00

75
Findings from the table revealed that borrowed money/loan had (p = 0.003), sales of land (p =
0.038), patients own money had (p = 0.072), sale of household mobile assets (p = 0.676), community
based support (p = 0.639), gifts from friends and neighbours (p = 0.117), cancer association (p =
0.771), temporary stoppage of children’s education (p = 0.676), family members (p = 0.934), social
welfare worker (p = 0.879), skips appointments (p = 0.591) and other payment mechanisms (p =
0.591).
Summary of Findings
The major findings of the study were;
Mean cost of pre-diagnosis test was N43,864.91 + 34001.25;
Mean monthly cost of managing illness was N30,757.95 + 27,325.82;
Mean cost of treatment using other treatment centres was N39,952.38 + 66,841.62;
Majority (79.3%) respondents were ranked among the poorest;
Mean monthly total income of the patients is N65,978.74 + 104,036.97;
Mean monthly total expenses was N43,916.28 + 56,070.33;
Mean time spent to JUTH on appointment date was 117.24 + 76.35 minutes;
Mean time spent by a patient in trying to see the doctor on each appointment was 116 + 80.24
minutes;
Mean number of days absent from work by the patients was 7.27 + 9.78;
The mean monthly patients’ total income was N65,978.74 + 104,036.97;
The mean monthly patients’ expenditure was N43,916.28 + 56,070.33;
The mean monthly earnings of persons accompanying patients was N105,159.28 + 108,342.16;
The mean patients’ monthly loss was N10,852.60 + 52,987.13;
76
The accompanying persons’ monthly loss was N7,914.73 + 20,676.63;
The mean total monthly loss is N18,126.27 + 66,559.08;
The mean patients’ annual loss was N130,231.25 + 635,845.62;
The mean accompanying persons’ annual loss was N94,976.75 + N248,119.61;
The mean total annual loss was N217,515.19 + 798,708.95;
The mean patients’ annual loss as a percentage of their mean annual income was 11.38 + 19.13%
while as a percentage of their mean annual expenditure was 50.06 + 421.98;
Payment coping mechanism utilized by most (78.8%) of the patients was their own money (i.e.
salary, earnings and/or savings) and payment by family members (46.9).
There was a significant difference between the socio-economic status and monthly patients’ total
income (p = 0.00), monthly earnings of persons accompanying patients (p = 0.00), patients’ monthly
loss (p = 0.018), accompanying persons’ monthly loss (p = 0.006), total monthly loss (p = 0.011),
patients’ annual loss (p = 0.018), accompanying persons’ annual loss (p = 0.006) and total annual loss
(p = 0.011)
There was a significant difference between socio-economic groups and borrowed money/loan (p =
0.003) and sales of land (p = 0.038) used as payment coping mechanisms.

77
CHAPTER FIVE
DISCUSSION OF FINDINGS
In this chapter, findings of the study were discussed. Report on the findings were done under:
discussion of the major findings, implications of the findings, limitations of the study, suggestions for
further studies, summary of the study, conclusions and recommendations.
Direct medical cost of cancer incurred by patients and their households.
The findings of this study revealed that the direct medical cost of cancer incurred by patients and their
household was high, (mean N30,757.95 + 27,325.82). This high cost of managing cancer by the
respondents was compounded by out of pocket payment (OOP) considered to be high for an average
Nigerian. The findings agree with that of Walsh and Crumbie (2007) who observed that, when a
patient is diagnosed with cancer, the financial resources of the family may be affected by the loss of
ability to work and the needs of the family may be neglected. John and Ross, (2009) also align with
the result of this study by stating that cancer consumes a lot of funds in the developed world where a
reasonable percentage of their budget goes to health. Similarly, the findings conform with the
assertion of Onwujekwu, Uzochukwu, ObikezeOkonkwo, Ochonwa, Onoka et al (2010) who opined
that cancer patients in developing countries like Nigeria play a large share of the health care cost out
of pocket (OOPs) due to lack of financial risk protection mechanisms. Cancer exerts a heavy financial
economic burden on individuals, national and society at large. It affects quality of life, not only of the
patient and their immediate families but also society. High medical cost seen in the treatment of
cancer poses a barrier to seeking health care.

78
Indirect medical cost of cancer incurred by patients and their households.
Findings from this study showed that the indirect cost incurred by patients and their household were;
time taken to see a doctor on days of appointment and time utilized by the patient to get to the
hospital. Edelson (2007) supports the findings of this study by noting that patients spend long hours
seeking and undergoing treatment. He observed that most patients spent an average of 99 hours
getting care during illness, while others may spend about 488 and 512 hours of care respectively.
Dorland, Hardecki, Hess, Memahan, (2014) observed that, waiting time for cancer patients
appointment are sometimes long. This can be stressful. How long these patients wait depends on
factors such as when the clients checked in with clerical staff and wait time can be driven by the
numbers of patients in the clinic area at one time.
Cost distribution among different socio-economic groups.
Findings revealed that majority (79.3%) of the respondents were in the poorest group. They had a
minimum income of 833.3 while the least poor were (5.0%) and they had a maximum income of
100,000.00. The findings of this study agree with the report of clegg et al (2010) who observed that
men and women with less than a high school education had elevated lung cancer rate ratio of 3.01 and
2.02 respectively, relative to their college educated counterparts. Those with family annual income
less than 12,500 U.S dollars had incidence rates that were more than 1.7 times the lung cancer
incidence rate of those with income 50,000 U.S dollars or higher.

79
Similarly Rusell, (2004) and Akobundu (2006) supports the findings of this study by stating that, 40%
expenditure on cancer care could be considered as catastrophic but considering socio-economic
inequalities it would also assess catastrophic expenditure at 100% and 40% for the poorest socio-
economic and the least poor socio-economic status group respectively. These authors also noted that
socio-economic status of patients varied for specific cancer while such patterns for stage were
generally consistent across cancers with latter state diagnosis being associated with lower SES. There
is a disparity in cancer outcome according to a variety of individual socio-economic, demographic
and health care characteristics, as well as by area measured available in the linked data base. This
author also agreed with the findings of this study by nothing that those families with annual income
less than 12,500 U.S dollars had incidence rates that were more than 1.7 times the lung cancer
incidence rate of those with income 50,000 U.S dollars or higher.
The findings are also in line with Wright et al (2011) who reported in their study that racial and ethnic
minorities, particularly those in impoverished urban communities, have higher colorectal cancer
morbidity and mortality rates as a result of the cost of treatment, and there is lower rates of
recommended colorectal cancer treatment among African American patients compared with their
white counterparts.
The payment coping mechanisms utilized by different socio-economic groups
The findings of the study showed that the major coping mechanisms utilized by different socio-
economic groups were; patients own money (salary, earnings, savings) and payment by family
members. Most of the respondents have difficulty in paying for cancer treatment.

80
The findings conform with the assertion of Adams and Ke (2008) who found that very high health
care expenditures relative to income in households may force house hold members to cut their
consumption of other minimum needs. This triggers the use of payment coping mechanisms to cater
for the costs of health care. Such strategies include selling of assets, borrowing , perceived cost,
saving behaviours like skipping appointment, skipping doses of drugs to make it last longer or
seeking and use of treatment from cheaper alternatives at the expense of good quality. In the same
vein Omolawa, (2013) found in his work that the choice of a coping strategy differs in different
context among households in the face of economic burden of illness and will depend on a house
hold’s asset base. While such strategies may meet the short term goal of paying for treatment and
minimizing costs, financing health care with payment coping mechanism leads to sacrificing of
necessary consumptions to pay for health care thus, pushing the house hold into deeper poverty. The
mechanisms include but not limited to the following, appeal for charity/begging, borrowing/loans,
gifts, savings and cutting down on minimum consumptions.
Onwujekwe, (2010) agrees with the findings of this work by asserting that in Nigeria, the various
coping mechanisms utilized by households in the treatment of cancer patients include distress scale of
assets, reduced intake of food to conserve funds, interruption of children’s education, informal and
formal borrowing, charitable support from churches, gifts from friends while on the same note,
Oyekale and Yusuf (2010) support by including other coping mechanisms such installment payment,
borrowing, reimbursement, off front payment and in kind payment. This is so because the treatment is
expensive and payment is borne out of pocket (OOP) by the patients.

81
Implications of the findings to Nursing Practice
- The economic burden of cancer patients in this study is very high for the patients. This would
lead to increasing poverty and poor rate of development as the productive age group is mostly
affected within this region. The disease will progress rapidly in the patients with attendant
poor quality of life, increase morbidity, mortality and productivity loses.
- Medical technology is increasingly costly in most fields of clinical medicine. Oncology has
not been spared from issues related to cost, in part resulting from the tremendous scientific
progress that has led to new tools for diagnosis, treatment and follow up of patients. Nurses
represent a critical link among patients, support groups and insurance companies. Thus, it is
imperative for the nurse practitioner to understand the role and value of cancer therapies and
help remove financial barriers for patients. An understanding of the basics of cost analysis is
an essential tool in the struggle to impact health-care and policy change.
- The study identified payment coping mechanisms utilized by patients as patients own money
and payment from family members. This could be burdensome for families. There is therefore
the need for the nurse to provide guidance for the patient seeking available financial
assistance. It is imperative to work in tandem with the social workers, case manager, to find
financial support for medications. This may also include over all financial assistance to offset
medical, living and transportation expenses.
- The nurse has the obligation to act as patients’ best advocate to seek individual funding where
it can be found.

82
Conclusion
Based on the findings of this study, the following conclusions were made;
The direct medical cost of cancer incurred by patients and their household was high.
The indirect medical cost of cancer incurred by patients and their household were; time taken to see a
doctor on days of appointment and time utilized by the patient to get to the hospital.
It was concluded that, majority of the respondents were in the poorest group.
The major coping mechanisms utilized by patients were; patients own money (salary, earnings
savings) and payment by family members.
There was a significant difference between socio-economic groups and payment strategies utilized by
cancer patients.
There was a significant difference in the cost distribution of different socio-economic groups.
Recommendations
Cancer patients need financial assistance in order to cope with the cost of their treatment, since
majority of them in this study are poor.
There is need for government to intervene by subsidizing the cost of cancer treatment.
There is need for the formation of strong cancer Association in Plateau State so that cancer patients
could pool their resources together as a strong social support to help themselves.
The cost of managing cancer is high. Nigeria Cancer Association should be aware of this so that
advocacy for cancer patients could be made through appropriate channel for support.
The government and None Governmental Associations need to be involved in cancer care.
Research should be intensified to find cure for cancer thereby reducing the cost.

83
Limitation of the study
It was difficult for the researcher to convince some of the cancer patients to participate in the study.
Another constraint was the issue of industrial unrest prior to the time of data collection. This led to
delay in data collection as some of the patients had not reported for follow up care.
Asset based information was observed to be sensitive to some respondents who felt they were
audited. Few opted out of the study being angry with the government whom they said received their
votes but failed to do so much towards alleviating their sufferings.
The technicality of the analysis of this work was time consuming and also capital intensive and
distressing.
Suggestions for further studies
There is need to carry out more studies on the economic burden and payment coping mechanisms of
cancer patients in other places different from this area of study.
The researcher also suggests that the National Assembly should legislate on the inclusion of cancer
care in the National Health Insurance Scheme.
Summary of the study
This work was carried out to determine the economic burden of cancer patients and payment coping
mechanism in Jos University Teaching Hospital (JUTH), Plateau state. The study was designed to
determine the;
(1) Direct medical cost of cancer incurred by patients and their households in JUTH.
(2) Indirect medical cost of cancer incurred by patients and their households in JUTH
(3) The cost distribution among different socio-economic groups

84
(4) The payment coping mechanism utilized by different socio-economic groups.
Literature was reviewed under conceptual, and empirical studies which were based under the
objectives of the study. The research design was descriptive survey. Respondents were consecutively
recruited, a sample size of 179 respondents who attended Jos University Teaching Hospital Plateau
state was used for the study. A validated questionnaire was used to collect data, data obtained was
subjected to descriptive and inferential statistics in form of chi-square test of association. Major
findings of the study showed that the direct medical cost of cancer incurred by patients and their
household was high (mean monthly cost = 30, 757. 97± 27, 325.82). the indirect medical cost
incurred by patients and their household were; time taken to see a doctor on days of appointment and
time utilized by the patient to get to the hospital. Majority (79.3%) of the respondents were in the
poorest group, they had a minimum income of 833.3 while the least poor were (5.0%) and they had a
minimum income of 100.000.00 . the major coping mechanisms utilized by different socio-economic
group were, patients own money (salary, earnings, savings) and payment by family members. There
is a significant difference between the socio-economic status and monthly patients total income (P =
0.00), monthly earnings of persons accompanying patients (P = 0.00), patients’ monthly loss (P =
0.018), accompanying persons’ monthly loss (P = 0.006), total monthly loss (P = 0.011), patients’
annual loss (P = 0.018), accompanying persons’ annual loss (P = 0.006) and total annual loss (P =
0.011) there is no significant difference in the socio-economic status of the patients and minutes
taken to get to JUTH on appointment date (P = 0.409), time taken to see doctor on each appointment
date (P = 0.556), days absent from work because of sickness within the last one month (P = 0.347)
monthly patients’ total expenditure (P = 0.083), patients’ annual loss as percentage of annual income
(P = 0.594) and patients’ annual loss as percentage of annual expenditure (P = 0.057).

85
REFERENCE
Adam, L., & Ke, X. (2008). Coping with Out-of-Pocket Payment for Healthcare Payment: Empirical evidence from 15 West African Countries.http://www.who.int/healthinfor/survey/en/. Accessed 8/2/2015.
Adebamowo, C.A, (2007). Cancer in Nigeria – Life after Cancerhttp:// progressreport. cancer.gov/doc-detail.asp?pid=1&did=2007&chid=75&coid=726&mid. Assessed June, 2012
Adewale, O.A; Lawal, O.O;Ade-sunkanmi (2008). Evaluation of Patients adherence to chemotherapy
for breast Cancer. African Journal of Health Sciences, 15(1) pg 22-27 http://www.bioline.org.br/pdf?jh08005.AccessedApril,12- 2011.
Adewole, I. (2011). Cancer Treatment: Why there are few Success Stories from Nigeria. Nigerian
Health Journal 16(16) p44.http:/ nigerianhealthjournal. com/?p=759economist burden/ financing+ of+cancer+ treatment+in+ Nigeria &ct= dnk Accessed 17 July,2011.
Akpan-Idiok P.A and Anarado A.N (2014). Perceptions of the burden of care-giving by informal caregivers of cancer patients attending University of Calabar Teaching Hospital, Calabar, Nigeria. The pan African Medical journal: 18 (159): 189-229
Asuzu C. C. and Elumelu T.N. (2013). Assessing the cancer patients’ quality of life and coping mechanisms in Radiotherapy Department of the University College Hospital, Ibadan. Journal of Psycho-Oncology; 22 (10).10-15
Axios International (2009) Cancer Treatment and Care in Developing countries: Paris: http://graphics.eiu.com/marketing/ptf/eiuLIVESTRONGGlobalCancerBurden. ptf – Assessed June 2012
Beaulieu N, Bloom D and Bloom R. (2009). Breaking away: The global burden of cancer-challenges and opportunities. A report from the Economist Intelligence unit USA.
Boyle P, Levin B (2008), World Cancer Report Lyon International Agency for Research on Cancer. 368:629-630
Burke, K.M; Mohn-Brown, E.I and Eby, L (2011). Medical-Surgical Nursing Care. Boston: Pearson edu.inc.
Chiejina A, (2013). Business Day-business day online.http://www.com/2013/04/cancer-on-the-rise-but-treatment-costs-n0-5m-monthly-in-nigeria/. Accessed on the September 26th, 2015

86
Clegg L.X, Reichman M.E, Miller B.A, Hankey B.F, Singh G.K, Lin Y.D, Goodman M.T, Lynch C.F, Schwartz S.M, Chen V.W, Bernstein L., Gomez S.L, Graff J.J, Lin C.C, Johnson N.J and Edwards B.K (2010). The impart of socioeconomic status on cancer incidence and stage at diagnosis: selected findings from the surveillance, epidemiology and end results; National Longitudinal Mortality study. U.S: National centre for information.
Dorland, L, Hardecki, C, Hess, B, Memaham, C. (2014). A Guide to Cancer infusion therapy. www.med.umich.edu/cancer/.../what-to- Access 8/12/2015.
Edelson E.D. (2007) Patients’ Lost time Boosts cost of Cancer care. Consumer Healthy day.com/cancer. Information-s/mis-cancer-news-102/patients-lost-time-boost-cost-of-cancer-care-600556.htm. Accessed 8/12/2015.
Elumelu T.N. Asuzu C.C and Akin-Odanye E.O (2012). Impact of active coping, religion and acceptance on quality of life of patients with breast cancer in the department of radiotherapy, UNH, Ibadan. BMJ support palliative care: 5(2): 1136.
Fasoranti T.O, (2011). Combating breast in Nigeria; the need for comprehensive screening programs.
http://www.gamji.com/article600/News7489htm.Accessed12/9/2011. Global Cancer Facts & Figures (2011) Adanta: American Cancer Society. 2011
http://www.Cancer.org/acs/groups/content/@epidemiologysurveilance/documents/acsp-027766.pdf.Accessed 19/11/2015.
Global Cancer Facts and Figures 2nd ed. Atlanta: American Cancer Society; (2011) http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-027766.ptf.Assessed 09/05/2011
Groot MT, Rob Baltussen, Carin A. Uyl-de Groot, Benjamin O. Anderson, MD,Gabriel N. Hortobagyi, MD, (2006). Costs and healthEffects of Brezast Cancer Interventions in Epidemiologically Different Regions of Africa, North America, and Asia. The Breast Journal, 12 (1): 90.98)
Huffingto and Thiboleaux K, (2015. Financial toxicity must become part of the conversation Retrieved from http://wwwhuffpost.com/us/entry/7110766 Accessed on September 24th, 2015).
Isangedihi, A.,Joshua, M., Asim, A. &Ekuri, E.(2004). Fundamentals of Research and Statistics, Calabar: University Press.

87
John, R. M. and Ross (2009). American Association for Cancer Research: studies estimate the Economic Burden of Career. http://www.Medicalnewstoday.com/articles/197891.php Accessed April, 20 2010.
Kanavas,P. (2006). The rising burden of cancer in the developing world: Annals of Oncology 17 (8): 15-23
Ke, X., Evans, D., and Carrin, G. (2007). Designing health financing policy towards universal coverage. Bull World Health Organ. 2007 (88): 653
Lemone, P; Burke, K and Banldoff, G. (2008). Medical-Surgical Nursing: Critical thinking in Patient Care . London: Pearson edu.inc.
Lyman, G. H., Coster, L. E, Kuderer N. M., et al (2007). Economics of cancer care. Journal of Oncology practice: 3(3): 113-114 .
Marti J. et al (20015). The economic burden of cancer in the UK; a study of survivors treated with curative intent. Retrieved from http://www.ncbi.nlm.gov/pubmed/26087260.Accessed on September, 25th, 2015.
Mathers, C.D and Loncar, D. (2006) Projections Of Global Mortality and Burden of Disease 2002 to 2030. PLoS Medicine ; 3(11):442
Mayston R, Guerra M, Huang Y, Sosa A. L, Uwakwe R, Acosta I --- (2014) Exploring the economic and social effects of care dependence in later life: protocol for the 10/66 research group INDEP study. Springerplus 28 (3).:111-115.
Mehta, A. (2012). Global Cancer Burden Shifting to Developing Countries. Pharmanews .34(10): 10 Merie-Nelly M (2013). 100 million Nigerian destitute fact: A jet and bulletproof bloated government
in total disconnect. Retrieved from www.http://ends-ng/100m-nigerian-destitute-fac..Accessed on September 24th, 2015.
Mossanen M, and Gore J.L (2014). The burden of bladder cancer care: direct and indirect cost. European Association of Urology 24(5): 487-91
Okoye, I. (2010). Training Manual for NYSC Cancer Prevention Advocates. Nigeria: WHO
Omolara, K.A. (2011). Feasible Cancer control strategies for Nigeria: mini review American Journal
of tropical medicine and public health 1 (1):1-10
88
Onoka, C.A, Onwujekwe, O. E, Hanson, K., and Uzochukwu, B. S (2011) Examining catastrophic health expenditure in Nigeria. Tropical Medicine and International Health, 6(10): 1334-1441.
Onwujekwe, O. E., Onoka, C. A., Hanson, K., and Uzochukwu, B. (2011) Examining Catastrophic health expenditure at variable thresholds using household consumption expenditure dairies. Tropical Medicine and International Health, 16 (10) 1334-1341.
Onwuasigwe C, (2010). Disease transition in Sub-Saharan Africa: the case of non-communicable disease in Nigeria. 54th inaugural lecture: 46-102
Osborn, K.S, Wrae, C.E, Watson and Holleran, R. (2014). Medical-surgical; Nursing-preparation for
practice New York San Francisco: Pearson educ.Inc.
Rebin K, Yabroff Y, Lund J, Kepka D and Mariotto A (2011). Economic burden of cancer in the US: Estimates projections and future reseach. Cancer epidemiol biomarkers pre 2010 Retrieved from http://www ncbi.n/m.nih.gov/pubmed/21980008. Accessed on September 24th, 2015.
Songer, T.J; Ettaro (200). The economics of diabetes project. The cost of diabetes. national centre for
chronic disease prevention and health promotion, Atlant: CDC.
Vicens G.R, Zefra M.S, Moreno-cresp J, Ferrer B.C.S, and Marcos-Gragera R. (2014). Incidence variation of prostrate and cervical cancer according to socio-economic level in Girona Health Region. Biomed central journals: 10 (14): 1074
Walsh, M. and Crumbie, A. (2007).Watson’s Clinical Nursing and Related Sciences. Philadelphia:
Bailliere Tindall Elsevier Ltd.
World Health Organization (2008). The Impact of Cancer - Nigeria. Retrieved from http://www.who.int/infobase/report.aspx Assessed on 10/06/2011
World Health Assembly (2008). Strategies for the prevention and control of NCDS and its related action plan. Vision 2020. Geneva: WHO
Wright, G.E, Borlow, W.E, Green, P, Balwin, L. Taphn. S.H. (2011). Differences Among the Elderly in the treat costs of colorectal cancer. www.ncbi.n/m.nih.gov/pmc/articles/pmc3124338/
Zaidi A.A, Asari T.Z, and Khan A. (2012). The financial burden of cancer: estimate from patients undergoing cancer care in a tertiary care hospital. International Journal of Equity Health 11(60):11-60

89
APPENDIX I
Sample size
A sample size calculated for this study is 163 and a provision for attrition out of 10% will be made,
which will result in a final sample size of 179, determined using the formula:
n = N (Araoye, 2004)
1+N (e)2
n = required sample
N = total population (sample frame)
e = error of tolerance which is 0.05 at 95%conficience level
1 = constant
Given N= 276
n= 276
1+276 (0.05)2
= 276
1+276 x 0.0025
= 276
1+0.69
= 276
1.69
=163.31
Therefore 163+10% attrition rate = 179.3
Approximately 179 patients.

90
APPENDIX II
QUESTIONNAIRE
Department of Nursing Sciences
Faculty of Health Science and
Technology University of Nigeria
Enugu Campus
Date
Dear Respondents,
I am a post graduate student of the above named institution conducting a research project on
‘Economic burden of cancer patients and payment coping mechanism in Jos University
Teaching Hospital (JUTH), Plateau State, Nigeria’.
Any information given will be used for academic purposes and confidentiality is assured.
Thank you for your expected cooperation.
Yours faithfully,
GAJI, Luka Dung

91
INSTRUCTION: Please answer the following questions as sincerely as possible the way it applies to
you.
SECTION A: SOCIODEMOGRAPHIC DATA
1. What is your age? _______________________________________
2. Sex: Male [ ] Female [ ]
3. Marital status: (a) married [ ] (b) single [ ] (c) divorced [ ]
(d) widowed [ ] (e) widower [ ]
4. Employment status: (a) Unemployed [ ] (b) Government employed [ ] (c) Private sector
employed [ ] (d) Self-employed [ ] (e) others (specify)________________
5. Highest educational level (a) Primary [ ] (b) Secondary [ ] (c) Tertiary [ ] (d) None [ ]
6. What type of cancer were you diagnosed of?
(a) Breast cancer [ ] (b) Cervical cancer [ ] (c) Prostrate cancer [ ] (d) Others
specify_______________________________________
SECTION B: ECONOMIC BURDEN OF CANCER
DIRECT COSTS:
7. How long have you been receiving treatment for cancer in JUTH Jos? (please
specify)__________________
8. How often do you come for check-up appointment?
(a) Weekly [ ] (b) 2 weekly [ ] (c) 4 weekly [ ] (d) 6 weekly [ ] (e) 8
weekly [ ]
92
9. How much did it cost you to run all the tests before you were diagnosed to have
cancer? _____________________________________________
10. How much does it cost you in a month in the course of managing the illness?
_______________________________________________
11. Did you receive treatment for cancer elsewhere within the last one year?
(a) Yes [ ] (b) No [ ]
12. If yes, please state the place where you received the treatment? ____________________
13. If yes, please state the costs incurred for your treatment monthly in that place? __________
INDIRECT COSTS:
14. What are your sources of income? __________________________
15. What is your monthly pay/earnings from these sources? __________________________
16. How many days have you been absent from work because of this sickness within
the last one month? __________________________________
17. What is the employment status of the person that accompanies you for treatment
regularly? ___________________________________________
18. What are his/her monthly earnings? ______________________
19. How long does it take you to see your doctor on each appointment date? ________
20. How many minutes does it take you to get to JUTH on appointment date? ___________

93
SECTION C: PAYMENT COPING MECHANISM
21. How have you been coping with payment for your cancer treatment?
(a) Own money (salary, earnings, saving) [ ] (b)borrowed money/loan [ ] (c) sale of household
mobile assets [ ] (d) sale of lands [ ] (e) community based support [ ] (f) gift from friends and
neighbours [ ] (g) cancer association [ ] (h) temporary stoppage of children’s education [ ] (i)
family member [ ] (j) social welfare/social worker (waiver) [ ] (k) skips appointments [ ] (l) use
alternate healthcare system [ ] (m) others
(specify)________________________________________________
SECTION D: RESPONDENTS SOCIO-ECONOMIC STATUS
Household assets holdings: below are list of household assets, please indicate those owned by your
family.
22. Which of the following does your family have?
(a) Radio [ ] (b) Television [ ] (c) Air conditioner [ ] (d) Bicycle [ ]
(e) Motorcycle [ ] (f) Car [ ] (g) Fridge [ ] (h) Generator [ ] (i) Gas cooker
[ ] (j) electric fan [ ] (k) Washing machine [ ] (l) Microwave oven [ ] (m) personal
computer [ ]
94
RESPONDENTS’ INCOME
23. How much do you earn from the following sources?
Sources Period codes (e.g.monthly) Amount receivable (₦)
Wages/ Salaries
Farming/gardening
Petty trading
Small and medium scale enterprises
Large scale enterprises
Rent
Pasturing
Allowances from children/relation
Security guards
Housekeeping/housewifery
Transport business
Pension
Others (specify)
Total
RESPONDENTS’ EXPENDITURE
24. How much do you spend on the following items?
Sources Period codes (e.g. monthly)
Amount spent(₦)
Add up later(annual expenditure)
(a) food (purchased)
(b) food (produced by your family if it were bought how much will it cost)
(c) clothing
(d) rent
(e) healthcare
(f) cooking fuel
(g) educational expenses
(h) durable household goods (specify)
(i) community welfare
(j) transportation
(k) others (specify)
Total

95
25. How easy/ difficult is it for you in paying for your cancer management?
(a) Very easy [ ]
(b) Fairly easy [ ]
(c) Difficult [ ]
(d)Very difficult [ ]
26. Suggest ways you think you could be assisted to cope with the burden of cancer and payment for
healthcare?
_______________________________________________________________________________
_______________________________________________________________________________
________________________________________

96
APPENDIX 111
SPLIT HALF TEST USING SPEARMAN-BROWN COEFFICIENT
Reliability case processing summary
N %
Cases Valid
Exclude
d(a)
Total
26
0
26
100.0
.0
100.0
List wise deletion based on all in the variables procedure
Reliability Statistics
Spearman-Brown Coefficient Equal Length
Unequal Length
.816
.816
As presented in the table, the spearman-Brown Coefficient is 0.816. Therefore, the reliability of the
research instrument is strong.
Intraclass Correlation Coefficient
Intraclass correlation (a)
95% confidence interval
F test with True value 0
Lower
Bound
Upper
Bound
Value Dfi Df2 Sig
Single
measures
.114(b)
.776( c)
.062
.642
.209
.877
4.467
4.467
29.0
29.0
754
754
.000
.000
The intraclass correlation coefficient is 0.776. This shows that the instrument is reliable.

97
APPENDIX IV

98
APPENDIX V
SUBJECT INFORMED CONSENT FORM
Instruction to researcher or research assistants
Please read the introductory statement to the respondent. His/her response will determine whether
you should proceed with the administration of the questionnaire.
Introduction
Dear respondent,
You are being invited to participate in this study on Economic Burden and Payment Coping
Mechanism of Cancer Patient in JUTH Plateau State being conducted by a Masters Degree student of
Department of Nursing Sciences, University of Nigeria, Enugu Campus.
Findings may identify the economic burden and payment coping mechanism of cancer patients. This
can be used as a basis for making relevant recommendations for health policies and legislation on
interventions to improve situations of cancer patients in order to prevent complications through
allocation of resources based on unmet needs, guide the development of strategic plan, and monitor
community based interventions. Findings will serve as a sign for necessary interventions by health
care providers towards an improved management of cancer patients.
The present study asks about your socio-demographic data, economic burden, cost distribution among
different socio-economic groups and payment coping mechanism. You will be presented with a copy

99
of questionnaire and require to kindly give true answer to the questions. The researcher or a research
assistant will interview you using the contents of the questionnaire and record your responses. This
information will help the researcher to determine your economic burden and payment coping
mechanism.
The exercise will not cause any harm to you. Every information given, reports or publications of the
results of this study shall not bear your name. You are free to accept or decline to be involved in this
study, and to leave the study at any time.
If you are willing to participate, please fill in the following form.
Consent from respondent
I understand that a study is being conducted on Economic Burden and Payment Coping Mechanism
of Cancer Patient in JUTH Plateau State. The researcher requested my consent to participate in the
study.
I was informed that every information I give will be treated as confidential, that the exercise will not
cause any physical or social harm to me and that I am free to accept or decline to be involved in the
study.
I was given opportunity to ask questions and answers were given to me.
I hereby give my free consent to participate in the study.
………………………………………………. ……………………………… Respondent’s signature/thumbprint Date

100
……………………………………………….. …………………………… Witness signature Date ……………………………………………….. …………………………… Researcher’s signature Date If you have any question or problem, contact:
The Secretary, Ethical Committee
Jos University Teaching Hospital Plateau State.
Through
Dr. Ijeoma Okoronkwo (The Supervisor)
Department of Nursing Sciences
University of Nigeria, Enugu Campus.
08063581297
Researcher’s contact address is
Plateau State College of Nursing
and Midwifery, Vom.
Phone: 08157566819
Thank you.
Gaji, Luka Dung (Researcher)