Embed Size (px)
DESCRIPTION
Saintifikasi Jamu
Citation preview

The Editors welcome submissions for possible publication in the Letters section. Authors
of letters should: • Include no more than 300 words of text, three authors, and five
references • Type with double-spacing • Send three copies of the letter, an authors’ form
(see Table of Contents for location) signed by all authors, and a cover letter describing
any conflicts of interest related to the contents of the letter.
Letters commenting on an Annals article will be considered if they are received within
6 weeks of the time the article was published. Only some of the letters received can be
published. Published letters are edited and may be shortened; tables and figures are
included only selectively. Authors will be notified that the letter has been received. If the
letter is selected for publication, the author will be notified about 3 weeks before the
publication date. Unpublished letters cannot be returned.
Annals welcomes electronically submitted letters. The Internet address is
www.acponline.org/shell-cgi/letter-article.pl.
In Defense of a Department of Geriatrics
TO THE EDITOR: Dr. Cassel writes in support of geriatric medicine(1), which has always been subsumed as a major aspect of internalmedicine. She maintains that “geriatricians . . . must have substantialknowledge of . . . psychiatry, rehabilitation, ophthalmology, audiol-ogy, gynecology, urology, orthopedics” and many other areas. I thinkher patients would best be served by referral to appropriate specialistsin those fields. No evidence is provided that the elderly are bettertreated by physicians with geriatric training. The conditions Dr.Cassel considers to be “geriatric,” such as congestive heart failure,osteoarthritis, and urinary incontinence, are not restricted to any agegroup. Nor are preventive medicine, early diagnosis of disease, andawareness of the advantages of shorter hospitalization specificallygeriatric subjects. In brief, I find no reason to expect better medicalcare in my senior state from a geriatrician than from a competentinternist.
Saul B. Gilson, MDNew York, NY 10033
Reference1. Cassel CK. In defense of a department of geriatrics. Ann Intern Med. 2000;133:
297-301. [PMID: 10929172]
IN RESPONSE: Dr. Gilson asserts that geriatric medicine has alwaysbeen subsumed as a major aspect of internal medicine. Althoughinternists see an increasingly large number of elderly patients, unfor-tunately that in itself does not mean that most internists are welltrained in the content and principles of geriatric medicine. Earlyleaders in the field of geriatrics, such as eminent internist Paul Bee-son, pointed out that the specialty of geriatric medicine as recognizedin other developed countries around the world includes a significantbody of knowledge about aging and age-related syndromes, as well asa different approach to the patient in which functional assessmentand functional goals are coupled with diagnosis and treatment. Suchleaders as Beeson and Hazzard would argue that internal medicineought to incorporate this body of knowledge and approach to care,especially in light of the aging of the population. I also share thatview and articulated it during my term as president of the AmericanCollege of Physicians. Unfortunately, however, many internists havenot had this training and are unfamiliar with functional assessmentand with recent advances in aging research. Furthermore, while thissituation is improving somewhat, there is still a great deal of room toenrich the curriculum in medical schools and internal medicine res-
idencies, making it more useful for physicians caring for patients ofadvanced age. Geriatricians do not replace the other specialties inmedicine, but they must have extensive familiarity with these otherdisciplines in order to effectively coordinate the care of the patientwho requires multiple referrals. Many internists have learned theprinciples and content of geriatric medicine through continuingmedical education courses, reading of the literature, and relationshipswith other colleagues. I suspect that Dr. Gilson’s definition of acompetent internist may be very close to my definition of a goodgeriatrician.
Christine K. Cassel, MDMount Sinai Medical CenterNew York, NY 10029
Placebo-Controlled Trials
TO THE EDITOR: I was surprised that in a series of four articlesdevoted to the ethics of placebo-controlled trials in the 19 September2000 issue of Annals, including those by Temple and Ellenberg (1,2), none referred to equipoise, a fundamental ethical and scientificprinciple of human experimentation (3). This principle states thatthe patient should be enrolled in a randomized, controlled trial onlyif there is substantial uncertainty (“equal bet”) about which of thetrial treatments would benefit a patient most (3). This principleapplies to any randomized trial, regardless of whether it is placebo-controlled. However, it is in placebo-controlled trials that we shouldbe particularly vigilant about applying the uncertainty principle (4),in light of recent empirical data suggesting that placebo arms mayindeed constitute inferior comparative therapy (5). Acknowledgingequipoise (that is, that true uncertainty about effects of competingtreatment alternatives exists) is the best mechanism available forchoosing an adequate control group. When the principle of equi-poise is applied, patients do not lose out prospectively and are notrequired to sacrifice themselves for the benefit of others (3, 4). Byamending the Declaration of Helsinki to explicitly acknowledge theprinciple of equipoise, we will remain in a position both to protectpatients’ individual rights and autonomy and to advance science byensuring that the most credible results are obtained (4). In my opin-ion, improvement in the ethics and science of clinical research willcome with further understanding of the equipoise principle—a fun-damental principle on which nearly the entire system of humanexperimentation is based (5). This discussion was sorely neglected inall four Annals articles.
Letters
62 © 2001 American College of Physicians–American Society of Internal Medicine

Benjamin Djulbegovic, MDH. Lee Moffitt Cancer Center and Research InstituteUniversity of South FloridaTampa, FL 33612
References1. Temple R, Ellenberg SS. Placebo-controlled trials and active-control trials in the
evaluation of new treatments. Part 1: ethical and scientific issues. Ann Intern Med.
2000;133:455-63. [PMID: 10975964]
2. Ellenberg SS, Temple R. Placebo-controlled trials and active-control trials in the
evaluation of new treatments. Part 2: practical issues and specific cases. Ann Intern
Med. 2000;133:464-70. [PMID: 10975965]
3. Edwards S, Lilford R, Braunholtz D, Jackson J, Hewison J, Thornton J. Ethical
issues in the design and conduct of randomised controlled trials. Health Technol
Assess. 1998;2:1-132. [PMID: 10194615]
4. Lilford RJ, Djulbegovic B. Declaration of Helsinki should be strengthened. Equi-
poise is essential principle of human experimentation [Letter]. BMJ. 2001;322:299-
300. [PMID: 11157551
5. Djulbegovic B, Lacevic M, Cantor A, Fields K, Bennett C, Adams J, et al. The
uncertainty principle and industry-sponsored research. Lancet. 2000;356:635-8.
[PMID: 10968436]
TO THE EDITOR: The debate over the ethics of randomized, place-bo-controlled trials focused on clinical settings where treatment doesnot affect the patient’s long-term health or where delay or omissionof active treatment would not increase mortality or irreversible mor-bidity (1). Unfortunately, this discussion ignored the issue of the useof a placebo in randomized, controlled trials when an effective treat-ment known to prevent reversible but highly clinically relevant mor-bidity is available. A specific example graphically makes this point.
In 1993, a randomized trial comparing oral ondansetron withplacebo demonstrated that the serotonin antagonist significantly re-duced emesis caused by moderately emetogenic cancer chemotherapy(2). However, two previously published peer-reviewed randomizedtrials had shown that dexamethasone resulted in a statistically signif-icant improvement in emesis in the same general patient population,compared with either placebo (3) or prochlorperazine (4). Thus, inthe oral ondansetron study, patients receiving placebo were exposedto a well-defined risk for considerable short-term discomfort, solelyfor the purpose of satisfying the “drug approval process”—an inex-pensive, well-tolerated, and documented effective antiemetic agentwas available at the time. Were patients entering this trial able toprovide truly “informed” consent?
No patient died as a result of participating in this phase IIIantiemetic study, and “irreversible morbidity” was not observed.However, on the basis of solid clinical data, patients entering thisstudy experienced a totally unnecessary risk for serious impairment intheir quality of life. Was this an ethical study design (4)?
Maurie Markman, MDThe Cleveland Clinic FoundationCleveland, Ohio 44195
References1. Simon R. Are placebo-controlled clinical trials ethical or needed when alternative
treatment exists? [Editorial] Ann Intern Med. 2001;133:474-5. [PMID: 10975967]
2. Beck T, Ciociola A, Jones S, Harvey W, Tchekmedyian N, Chang A, et al. Efficacy
of oral ondansetron in the prevention of emesis in outpatients receiving cyclophos-
phamide-based chemotherapy. The Ondansetron Study Group. Ann Intern Med.
1993;118:407-13. [PMID: 8439113]
3. Cassileth P, Lusk E, Torri S, DiNubile N, Gerson S. Antiemetic efficacy of dexa-
methasone therapy in patients receiving cancer chemotherapy. Arch Intern Med. 1983;
143:1347-9. [PMID: 6347109]
4. Markman M, Sheidler V, Ettinger D, Quaskey S, Mellits E. Antiemetic efficacy of
dexamethasone. Randomized, double-blind, crossover study with prochlorperazine in
patients receiving cancer chemotherapy. N Engl J Med. 1984;311:549-52. [PMID:
6379459]
5. Markman M. When regulatory requirements conflict with ethical study design: the
case of oral ondansetron. Cancer Invest. 1994;12:654-6. [PMID: 7994600]
IN RESPONSE: Dr. Djulbegovic argues that the principle of equipoisemust be of particular concern in placebo-controlled trials becauseplacebo-treated patients may be disadvantaged and should not “sac-rifice themselves for the benefit of others.” It seems important, as weemphasized in our papers, to distinguish between studies of treat-ments for serious illness and studies of symptomatic treatments. Ex-posure to placebo in the former requires genuine uncertainty aboutthe outcome. Exposure to placebo in a trial of headache, anxiety, orseasonal allergy, however, cannot reasonably be said to constitute“sacrifice” of oneself. It is, at worst, the sort of choice to defer oromit therapy that people with symptomatic conditions make everyday. Moreover, at least in the first trial carried out, there is, in fact,equipoise—uncertainty as to whether the drug or placebo will besuperior. There may be knowledge that some other treatment iseffective, but that is a different question. It should, however, beappreciated that during treatment development, studies are repli-cated and there are often multiple placebo-controlled trials of variousdoses and regimens in diverse settings and populations. These studieshelp define safe and effective use of the drug, but the favorable resultsof these trials are at least strongly suspect. Nonetheless, despite pos-sible lack of equipoise, such trials have been conducted, have beenconsidered ethical, and are valuable. In contrast, if in the course ofdrug development it becomes known that a treatment enhances sur-vival or decreases significant morbidity, relevant equipoise no longerexists and another placebo-controlled trial cannot be conducted.
Dr. Markman asks whether placebo controls are justified whereavailable therapy is “known to prevent reversible but highly clinicallyrelevant morbidity,” such as “emesis caused by moderately emeto-genic cancer chemotherapy.” He specifically questions the conduct ofa placebo-controlled trial of ondansetron in preventing emesis aftercyclophosphamide regimen–induced emesis, since dexamethasonehad been shown to be effective in that population. He asks whetherpatients in the trial gave truly informed consent and why they shouldhave endured emesis when an inexpensive existing treatment wasavailable. In this setting, Dr. Markman suggests that the appropriatecomparator was dexamethasone, not placebo, but does not statewhether these should have been noninferiority trials or superioritytrials. A superiority trial (or a trial seeking evidence of greater efficacywhen ondansetron is added to dexamethasone) would have beeninformative and interpretable, perhaps particularly desirable given
Letters
www.annals.org 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 63

dexamethasone’s low cost. An interpretable noninferiority trial, how-ever, would have required a full evaluation of all trials (not just oneor two) comparing dexamethasone with placebo. If dexamethasonehad consistently been shown to be effective (superior to placebo) indecreasing emesis, an appropriately sized equivalence–noninferioritytrial could have been informative. Despite the documented effective-ness of ondansetron in the setting of highly emetogenic chemother-apy, however, there are many situations, primarily postsurgical, inwhich ondansetron has not been consistently distinguishable fromplacebo as an antiemetic. In these situations, a comparison withdexamethasone would have been uninformative. To know whetherondansetron was effective in these cases, placebo-controlled trialswould be necessary.
Whether patients or physicians accept a trial of a particulardesign depends on the trial’s value and necessity. It may be that anactive control design is interpretable in the initial treatment of pa-tients receiving moderately or markedly emetogenic cancer chemo-therapy. This could be shown by a thorough review of experiencewith placebo-controlled trials of the proposed active control. If aconsistent benefit were established, most patients and physicianswould not want to participate in a placebo-controlled trial of a newagent, and no such trial would be needed for regulatory approval.
Robert Temple, MDSusan S. Ellenberg, PhDU.S. Food and Drug AdministrationRockville, MD 20857
Update in Infectious Diseases
TO THE EDITOR: Dr. Bartlett’s update on infectious diseases (1) wasvery much appreciated, but I was troubled by its omission of anymention of the link between antibiotic resistance and the widespreaduse of antibiotics to promote growth in livestock. Roughly one thirdof all antibiotics produced in the United States are fed to animalssolely to enhance weight gain (2). A September 1999 advertisementin Swine Practitioner boasted about a product containing a tetra-cycline, a sulfonamide, and penicillin to enhance “growth and feedefficiency”—available without a prescription. Since 1998, the Euro-pean Union has prohibited for use in animal growth promotion allantibiotics used in human medicine (3). The United States, by con-trast, allows 19 different antibiotics to be used for growth promo-tion, and of these, 7 are from classes used in human medicine (3).The economic use of antibiotics, not to cure sick animals but topromote weight gain, is especially problematic in an age of unprec-edented antibiotic resistance. Although this practice translates intocheaper meat prices, the economic advantage seems to be minimal.Denmark has banned the use of human antibiotics for growth pro-motion for 5 years and has seen productivity actually increase (3). ANational Research Council study (4) estimated that a similar ban inthe United States would increase per capita costs by $5 to $10 peryear. Use of antibiotics as growth promoters in livestock has beenlinked to the emergence of antibiotic-resistant diseases, helping the
Centers for Disease Control and Prevention to conclude that anti-microbial use in food animals is the dominant source of antibioticresistance among foodborne pathogens (5). Both the Centers forDisease Control and Prevention and the World Health Organizationhave called for an end to the use of antibiotics for growth promotionin animals. It is time for our leaders in medicine to include thisproblem in discussions about antibiotic resistance.
Robert J. Lodato, MDDexter Internal MedicineDover-Foxcroft, ME 04426
References1. Bartlett J. Update in infectious diseases. Ann Intern Med. 2000;133:285-92.
[PMID: 10929170]
2. Mellon M. Antibiotic resistance: causes and cures. From a press briefing at the
National Press Club, 4 June 1999. Available at www.ucsusa.org/food/brf.cause.html.
3. Mellon M. Europe says “no” to using antibiotics to promote livestock growth.
Nucleus. 1999–2000;22:6-8.
4. The use of drugs in food animals: benefits and risks. National Research Council.
Washington, DC: National Academy Pr; 1998.
5. Mølbak K, Baggesen D, Aarestrup F, Ebbesen J, Engberg J, Frydendahl K, et al. An
outbreak of multidrug-resistant, quinolone-resistant Salmonella enterica serotype typhi-
murium DT104. N Engl J Med. 1999;341:1420-5. [PMID: 10547404]
IN RESPONSE: Dr. Lodato makes a good point regarding the contri-bution of antibiotic abuse in animals to antibiotic resistance andantibiotic-resistant infections in people. Agricultural antibiotic useseems to have been particularly important in vancomycin resistancein Europe (but not the United States), as well as fluoroquinoloneresistance in Salmonella species and Campylobacter jejuni. Neverthe-less, to keep perspective, the overuse of antibiotics in patients, par-ticularly those with viral respiratory infections, and extensive use ofbroad-spectrum antibiotics in hospitals probably account for thelion’s share of our current dilemma. Having said this, I acknowledgethat the publication by Mølbak and colleagues (1) should have mademy listing.
John G. Bartlett, MDJohns Hopkins UniversityBaltimore, MD 21287-0003
Reference1. Mølbak K, Baggesen D, Aarestrup F, Ebbesen J, Engberg J, Frydendahl K, et al. An
outbreak of multidrug-resistant, quinolone-resistant Salmonella enterica serotype typhi-
murium DT104. N Engl J Med. 1999;341:1420-5. [PMID: 10547404]
Testosterone and Resistance Training in AIDS
TO THE EDITOR: There are two points of interest in the article byGrinspoon and colleagues (1), which examined the effects of testos-terone supplementation on muscle mass and strength in patientswith AIDS cachexia. First, all patients had normal free testosteronelevels (that is, they were eugonadal). Second, the dosage of testoster-one enanthate used (200 mg/wk) was twice the physiologic replace-ment dosage.
Letters
64 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 www.annals.org

Eight published randomized, controlled trials have examinedtestosterone supplementation in men at doses that produced physi-ologic serum concentrations and assessed the effects of such supple-mentation on muscle mass and strength. Results from these trialssuggest that testosterone supplementation at these doses increasedmuscle mass and strength in hypogonadal but not eugonadal pa-tients. Testosterone doses that produced supraphysiologic concentra-tions of testosterone in eugonadal patients had inconsistent effects onmuscle. Earlier studies had several shortcomings and produced in-conclusive results (2, 3). In 1996, Bhasin and coworkers (4), in awell-designed study, reported that a supraphysiologic dosage of tes-tosterone enanthate (600 mg/wk for 10 weeks) increased muscle sizeand strength in a group of eugonadal normal men. The study byGrinspoon and colleagues reports similar findings in a group ofeugonadal men with AIDS wasting. The short-term administrationof these supraphysiologic dosages of testosterone did not cause ad-verse events in either study sample.
These two studies suggest that short-term administration of su-praphysiologic doses of testosterone may have beneficial effects ineugonadal men with wasting caused by such conditions as cancer,AIDS, or age-related sarcopenia. The safety of long-term administra-tion, however, is not known. Potential side effects include increasedhematocrit levels, stimulation of benign prostatic hypertrophy, andprostate carcinoma, as well as angry behavior.
Hosam K. Kamel, MDSaint Louis University School of MedicineSt. Louis, MO 63104
References1. Grinspoon S, Corcoran C, Parlman K, Costello M, Rosenthal D, Anderson E, et al.
Effects of testosterone and progressive resistance training in eugonadal men with AIDS
wasting. A randomized, controlled trial. Ann Intern Med. 2000;133:348-55. [PMID:
0010979879]
2. Young NR, Baker HW, Liu G, Seeman E. Body composition and muscle strength
in healthy men receiving testosterone enanthate for contraception. J Clin Endocrinol
Metab. 1993;77:1028-32. [PMID: 0008408450]
3. Friedl KE, Dettori JR, Hannan CJ Jr, Patience TH, Plymate SR. Comparison of the
effects of high dose testosterone and 19-nortestosterone to a replacement dose of tes-
tosterone on strength and body composition in normal men. J Steroid Biochem Mol
Biol. 1991;40:607-12. [PMID: 0001958561]
4. Bhasin S, Storer TW, Berman N, Callegari C, Clevenger B, Phillips J, et al. The
effects of supraphysiologic doses of testosterone on muscle size and strength in normal
men. N Engl J Med. 1996;335:1-7. [PMID: 0008637535]
IN RESPONSE: We agree with Dr. Kamel that our data demonstratea significant effect of supraphysiologic testosterone on muscle massand strength in eugonadal men with AIDS wasting. The use of tes-tosterone may therefore be considered to reverse sarcopenia in thispopulation. However, we also agree that the long-term safety ofsupraphysiologic testosterone is unknown in this population. Al-though our data do not show adverse effects on prostate-specificantigen and hematocrit levels, the study was short and the longer-term safety effects remain unknown. Furthermore, our data do sug-gest a decrease in high-density lipoprotein cholesterol level, which
may adversely affect such patients. In addition, long-term use ofhigh-dose testosterone may result in suppression of gonadal function.In contrast, we have shown that progressive resistance training in-creases muscle mass and improves levels of high-density lipoproteincholesterol. How these strategies will be best used in long-term clin-ical care remains to be determined.
Steven K. Grinspoon, MDHarvard Medical SchoolBoston, MA 02108
Garlic for Total Cholesterol Reduction
TO THE EDITOR: To investigate “the effect of garlic on total choles-terol level in persons with elevated levels,” Stevinson and colleagues(1) performed a thorough meta-analysis of trials conducted withgarlic supplements. Such an undertaking assumes that consumptionof garlic supplements and consumption of garlic cloves result insimilar levels of active compounds in the body. However, no clinicaltrial has yet used a garlic supplement that has demonstrated bioavail-ability of the probable active compounds of garlic. This is a crucialpoint because considerable evidence indicates that most of garlic’seffect on cholesterol reduction is due to allicin (2), a compound thatis readily present when garlic is chopped or crushed but that must beenzymatically formed in the body from alliin when dried garlic isconsumed in supplement form. This transformation by alliinase can-not be assumed to take place without bioavailability studies, sincealliinase is inactivated immediately by gastric acid and in 1 hour byintestinal proteases (3). Unlike many other brands, the brand used in10 of the 13 trials that qualified for inclusion in this meta-analysisdoes not use a coating that protects alliinase from exposure to gastricacid. Because of this, in vivo allicin formation depends on gastric pHand gastric emptying time and is therefore in considerable doubt.The second powder supplement included in the analysis was pre-pared by spray-drying, a process that results in loss of most of thealliin. Of the two studies that used allicin-derived garlic oils, the onethat showed no effect (4) used an unusual solid form of the oil thathas since been demonstrated to have low bioavailability in a 48-hourbreath test (5). The conclusions derived from this meta-analysis canbe applied only to the particular supplement brands used in thestudies and not to garlic itself.
Larry D. Lawson, PhDPlant Bioactives Research InstituteOrem, UT 84058
References1. Stevinson C, Pittler MH, Ernst E. Garlic for treating hypercholesterolemia. A meta-
analysis of randomized clinical trials. Ann Intern Med. 2000;133:420-9. [PMID:
0010992573]
2. Lawson LD. Garlic: a review of its medicinal effects and indicated active com-
pounds. In: Lawson LD, Bauer R, eds. Phytomedicines of Europe: Chemistry and
Biological Activity. American Chemical Society Symposium Series 691. Washington,
DC: American Chemical Soc; 1998:176-209.
Letters
www.annals.org 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 65

3. Jansen H, Muller B, Knobloch K. Characterization of an alliin lyase preparation
from garlic (Allium sativum). Planta Med. 1989;55:434-9.
4. Berthold HK, Sudhop T, von Bergmann K. Effect of a garlic oil preparation on
serum lipoproteins and cholesterol metabolism: a randomized controlled trial. JAMA.
1998;279:1900-2. [PMID: 0009634262]
5. Lawson LD. Effect of garlic on serum lipids [Letter]. JAMA. 1998;280:1568.
[PMID: 0009820256]
IN RESPONSE: Dr. Lawson rightly points out that the results of ourmeta-analysis refer only to the use of garlic supplements and not theconsumption of garlic per se. The question of interest was whethergarlic supplements reduce cholesterol levels in patients with elevatedlevels to the extent that these supplements might be considered atreatment option for hypercholesterolemia, as suggested by previousdata (1). This question is a pertinent one, given that garlic supple-ments are marketed for that purpose. Our results indicated that sup-plements probably do not reduce total cholesterol levels to a clini-cally meaningful degree, but clearly this does not imply that eatinggarlic does not have health benefits. As discussed in our paper, sys-tematic reviews of herbal medicines invariably combine data derivedfrom different preparations. This can be problematic, not least be-cause of the lack of bioavailability data for the possible active com-pounds of garlic. Dr. Lawson has presented interesting data to sug-gest that the conflicting results of clinical trials may be related to thequality and coating of the tablets (2). Although he points out thatunlike other brands, the tablets used in most of the trials included inour analysis were not enteric-coated, it is worth noting that theefficacy of these other brands has not been demonstrated in rigorousclinical trials. It could also be mentioned that unlike other research,our work in this area is independent of commercial interests.
Clare Stevinson, BSc, MScMax H. Pittler, MDEdzard Ernst, MD, PhD, FRCP(Edin)University of ExeterExeter EX2 4NT, United Kingdom
References1. Warshafsky S, Kamer RS, Sivak SL. Effect of garlic on total serum cholesterol. A
meta-analysis. Ann Intern Med. 1993;119:599-605. [PMID: 0008363171]
2. Lawson L. Tablet quality: a major problem in clinical trials with garlic supplements
[Abstract]. Forsch Komplementarmed Klass Naturheilkd. 2000;7:45.
Wine and Mortality
TO THE EDITOR: If wine drinkers experience lower mortality ratesthan drinkers of beer and spirits (1), it may be because these bever-ages affect body tissue distribution differently. Two cross-sectionalstudies in the United States have reported that beer and spirit con-sumption was positively associated but wine consumption was in-versely (or nonsignificantly) associated with the waist-to-hip ratioamong men and women in young adulthood (2) and middle age (3).These beverage-specific associations persisted after adjustments forseveral factors, including age, education, smoking, and body massindex. An elevated waist-to-hip ratio might be the result of relative
enlargement of the upper body (waist) or relative reduction in thesize of the lower body.
Our 10-year follow-up of 44 080 middle-aged healthy whitewomen (4) explored how regular consumption ($5 days per weekreported across a 10-year interval) of these three alcohol types wasassociated with risk for weight gain in the waist and in the periphery(predominantly hips and thighs). Compared with nonconsumers,regular drinkers of wine, beer, and spirits had similar, nonsignificantlikelihoods of weight gain in the waist, with odds ratios of approxi-mately 1.0, but the beverage-specific groups differed notably in thelikelihood of weight gain in the periphery. Regular wine drinkingwas not associated with peripheral weight gain. However, womenwho regularly drank beer or spirits had a reduced likelihood of pe-ripheral weight gain (odds ratios, 0.59 [95% CI, 0.43 to 0.81] and0.54 [CI, 0.44 to 0.65], respectively).
These consistent findings suggest that the apparent advantage ofwine drinking might be related to the preservation of muscle oradipose tissue in the lower extremities. Large hips and thighs may beprotective (5). Whether these differential effects are related to thealcoholic beverage itself or to behaviors associated with its consump-tion remains to be determined.
Henry S. Kahn, MDNational Center for Chronic Disease Prevention
and Health PromotionAtlanta, GA 30341-3717
References1. Grønbaek M, Becker U, Johansen D, Gottschau A, Schnohr P, Hein H, et al. Type
of alcohol consumed and mortality from all causes, coronary heart disease, and cancer.
Ann Intern Med. 2000;133:411-9. [PMID: 10975958]
2. Slattery M, McDonald A, Bild D, Caan B, Hilner J, Jacobs D, et al. Associations of
body fat and its distribution with dietary intake, physical activity, alcohol, and smoking
in blacks and whites. Am J Clin Nutr. 1992;55:943-9. [PMID: 1570801]
3. Duncan B, Chambless L, Schmidt M, Folsom A, Szklo M, Crouse J, et al. Associ-
ation of the waist-to-hip ratio is different with wine than with beer or hard liquor
consumption. Atherosclerosis Risk in Communities Study Investigators. Am J Epide-
miol. 1995;142:1034-8. [PMID: 7485048]
4. Kahn H, Tatham L, Heath C. Contrasting factors associated with abdominal and
peripheral weight gain among adult women. Int J Obes Relat Metab Disord. 1997;21:
903-11. [PMID: 9347409]
5. Kahn H. Why are large legs protective? [Letter] Am J Clin Nutr. 1997;66:712-3.
[PMID: 9280198]
IN RESPONSE: Dr. Kahn adds to the long list of possible explana-tions for the apparent beneficial effect of wine compared with beerand spirits on morbidity and mortality. His opinions are of greatinterest. However, I doubt that the beverage-specific differences inwaist-to-hip ratio can explain some, if any, of this effect. First, al-though there truly do seem to be differences, as found in the twostudies mentioned by Dr. Kahn, they would need to be quite large(larger than those reported) to be able to explain our findings. Sec-ond, we did consider body weight in the analyses, but since partici-pants who did not drink wine had a mean body mass index of 26kg/m2 and those who did had a body mass index of 25 kg/m2, it had
Letters
66 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 www.annals.org

no effect on mortality, as can be seen in our Table 1. Third, theapparent added beneficial effect of wine in our study seemed to applymainly to death from cancer and not to death from coronary heartdisease, which is much more strongly associated with increases inwaist-to-hip ratio.
Morten Grønbaek, MD, DrMedSci, PhDCopenhagen University HospitalDK-1399 Copenhagen K, Denmark
Smoking and Abnormalities in Renal Function
TO THE EDITOR: Pinto-Sietsma and colleagues recently reportedthat cigarette smoking is associated with albuminuria in nondiabeticpersons (1). They refer to the known adverse effects of smoking indiabetic patients that were previously reported in the literature. Theirreferences, however, are entirely to studies of patients with type 1diabetes mellitus. Smoking has not consistently been found to be animportant risk factor for nephropathy in patients with type 2 diabe-tes mellitus, which accounts for 90% of the 16 million cases ofdiabetes in the United States (2, 3).
We would also like to comment on the association betweensmoking and nephropathy in type 2 diabetes mellitus, which we havereported in a recent article (4). In our study, the multivariate oddsratio for nephropathy was 1.61 (95% CI, 1.01 to 2.58) in smokerswith type 2 diabetes mellitus who were enrolled in the AppropriateBlood Pressure Control in Diabetes trial.
Diabetic nephropathy continues to be the leading cause of end-stage renal disease. In patients with diabetes, aggressive blood pres-sure control, newly defined as a value less than 130/80 mm Hg, is animportant cornerstone of any successful program to prevent diabetes-related complications (5). Impressive evidence continues to mountfrom several clinical trials that show marked benefits from aggressiveblood pressure reduction. In addition, since approximately 25% ofall diabetic patients smoke, finding another potential hazard associ-ated with smoking gives physicians further impetus to strongly en-courage smoking cessation in order to attenuate the rate of decline inrenal function. The exact pathophysiologic basis for this associationis currently unknown. Smoking may contribute to decline in renalfunction through its effect on cytokine-transforming growth factorand renal hypertrophy or through an effect on glomerular ischemiaand elevations of plasma endothelin-1 levels.
Philip S. Mehler, MDRaymond Estacio, MDDenver HealthDenver, CO 80204
References1. Pinto-Sietsma S, Mulder J, Janssen W, Hillege H, de Zeeuw D, de Jong P. Smoking
is related to albuminuria and abnormal renal function in nondiabetic persons. Ann
Intern Med. 2000;133:585-91. [PMID: 11033585]
2. Lee E, Lee V, Lu M, Lee J, Russell D, Yeh J. Incidence of renal failure in NIDDM.
The Oklahoma Indian Diabetes Study. Diabetes. 1994;43:572-9. [PMID: 8138063]
3. Meigs J, Singer D, Sullivan L, Dukes K, D’Agostino R, Nathan D, et al. Metabolic
control and prevalent cardiovascular disease in non-insulin-dependent diabetes mellitus
(NIDDM): The NIDDM Patient Outcome Research Team. Am J Med. 1997;102:
38-47. [PMID: 9209199]
4. Mehler P, Jeffers B, Biggerstaff S, Schrier R. Smoking as a risk factor for nephrop-
athy in non-insulin-dependent diabetics. J Gen Intern Med. 1998;13:842-5. [PMID:
9844083]
5. Bakris G, Williams M, Dworkin L, Elliott W, Epstein M, Toto R, et al. Preserving
renal function in adults with hypertension and diabetes: a consensus approach. Na-
tional Kidney Foundation Hypertension and Diabetes Executive Committees Working
Group. Am J Kidney Dis. 2000;36:646-61. [PMID: 10977801]
TO THE EDITOR: Pinto-Sietsma and colleagues (1) found that smok-ing was associated with albuminuria and abnormal renal function innondiabetic patients. This fine report adds to a body of evidenceshowing that tobacco smoking causes structural and functional ab-normalities in the kidneys, increases the risks for primary and sec-ondary renal disease, hastens end-stage renal failure, and worsens theoutcome for patients receiving dialysis and for recipients of kidneytransplants (2). However, neither Pinto-Sietsma and colleagues norother recent authors have cited early studies that strongly suggestedthat the kidneys were a target for the adverse effects of tobacco smoking.
Researchers in the 1800s observed effects of tobacco and nico-tine on renal structure and function. By the early 1900s, reviews oftobacco-related diseases included information that linked cigarettesmoking and renal dysfunction (3, 4). In the famous 1964 Report ofthe Surgeon General’s Advisory Committee on Smoking and Health(5), among prospective studies in which mortality ratios (MRs) fornephritis were analyzed, the median MRs among smokers andformer smokers were 1.5 and 1.1, respectively. These MRs, althoughunadjusted for passive smoking, were similar to median MRs forcoronary artery disease (MR, 1.7), cancer of the kidney (MR, 1.4),and cerebrovascular disease (MR, 1.3). The relationships betweentobacco smoking and these vascular and neoplastic diseases have beenstudied extensively over the past 35 years; however, despite 100years’ worth of evidence about the adverse effects of tobacco smokeand nicotine on the kidneys, the findings in the 1964 report werelargely ignored.
One can only speculate why researchers failed to investigate therenal effects of smoking until recently. The good news is that activeresearch into basic mechanisms and therapeutic interventions relatedto tobacco smoking and kidney disease has finally begun (2).
Stephen J. Jay, MDIndiana University School of MedicineIndianapolis, IN 46202
References1. Pinto-Sietsma S, Mulder J, Janssen W, Hillege H, de Zeeuw D, de Jong P. Smoking
is related to albuminuria and abnormal renal function in nondiabetic persons. Ann
Intern Med. 2000;133:585-91. [PMID: 11033585]
2. Sessa A, Conte F, Meroni M, Battini G, eds. Cigarette Smoking and the Kidney.
Series: Contributions to Nephrology, vol. 130. New York: Karger; 2000.
3. Kellogg JH. Tobaccoism. Battle Creek, MI: Modern Medicine Publishing; 1922.
Letters
www.annals.org 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 67

4. Lickint F. Tabak und Organismus; Handbuch der gesamten Tabakkunde. Stuttgart:
Hippokrates; 1939.
5. Summary of the Report of the Surgeon General’s Advisory Committee on Smoking
and Health. U.S. Surgeon General’s Advisory Committee on Smoking and Health.
Washington, DC: U.S. Department of Health, Education, and Welfare; 1964.
IN RESPONSE: We appreciate the interest in our recent article onsmoking and renal abnormalities in nondiabetic persons. As Drs.Mehler and Estacio point out, smoking has been found to haveadverse effects on renal function not only in patients with type 1diabetes mellitus but also in those with type 2 diabetes mellitus (1).We agree with their plea that physicians should strongly encouragecessation of smoking in patients with type 2 diabetes mellitus. Ourfinding that smoking is also associated with both albuminuria andrenal function changes in patients without diabetes argues that smok-ing has renal effects independent of the diabetic setting. It adds toour knowledge about the mechanism of albuminuria. Increased uri-nary albumin excretion seems to be a phenomenon related not onlyto diabetes and hypertension but also to smoking, central obesity(Pinto-Sietsma SJ, Navis G, Janssen WM, de Zeeuw D, Gans RO,de Jong PE. A central body fat distribution is related to renal abnor-malities. Unpublished data), and the use of oral contraceptives andhormone replacement therapy (2). This may partly explain why mi-croalbuminuria may also be found in 5% to 6% of nondiabetic andnonhypertensive persons.
We thank Dr. Jay for drawing attention to the medical litera-ture as early as 1922. At that time, it indeed was already reportedthat smoking could cause Bright disease, known in those days ascongestion, degeneration, and damage of the kidney. Furthermore, itwas described that tobacco induced a pronounced contraction of thevessels of the kidney (3). These and other historical data, as pointedout by Dr. Jay, underline the importance and difficulties of thestruggle for smoking cessation. Microalbuminuria is thought to be anearly marker for worsened renal and cardiovascular prognosis. There-fore, our finding that patients who stopped smoking no longer hadan increased risk for microalbuminuria argues for a more aggressiveand intensive approach to encourage smoking cessation in patientswith microalbuminuria, both those with diabetes and those without.
Sara-Joan Pinto-Sietsma, MDWilbert M.T. Janssen, MD, PhDPaul E. de Jong, MD, PhDUniversity Hospital Groningen9713 GZ Groningen, the Netherlands
References1. Mehler P, Jeffers B, Biggerstaff S, Schrier R. Smoking as a risk factor for nephrop-
athy in non-insulin-dependent diabetics. J Gen Intern Med. 1998;13:842-5. [PMID:
9844083]
2. Monster TBM, Janssen WMT, de Jong PE, de Jong-den Berg LTW. Oral contra-
ceptives and hormone replacement therapy are associated with microalbuminuria. Arch
Intern Med. [In press]
3. Kellogg JH. Tobaccoism. Battle Creek, MI: Modern Medicine Publishing; 1922.
Kava Hepatotoxicity
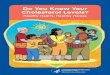
TO THE EDITOR: Phytotherapeutic preparations for sleep and anxi-ety disorders that contain kava-lactones are available over the counterin many countries. A 33-year-old woman took the drug Laitan(Schwabe Pharma AG, Kuessnacht, Switzerland) (210 mg of kava-lactones daily) for 3 weeks. The patient reported intake of no otherdrugs except the homeopathic medication Exsepta (Tentan AG, Roth-rist, Switzerland). Two months later, she restarted use of the kavapreparation. After another 3 weeks, 1 day after intake of 60 g ofalcohol, she developed malaise, loss of appetite, and jaundice. Levelsof aminotransferases, bilirubin, and alkaline phosphatase were ele-vated 60-, 15- and 3-fold, respectively (aspartate aminotransferase,40.8 mkat/L [2450 U/L]; alanine aminotransferase, 40.5 nkat/L[2430 U/L]; total bilirubin, 399 mmol/L [23 mg/dL]; alkaline phos-phatase, 4.98 mkat/L [299 U/L]). Prothrombin time was normal.Tests for autoantibodies and results of viral serologic tests were neg-ative, except for low titers of Epstein–Barr virus IgM. Liver biopsyshowed infiltrated portal tracts, bridging necroses, destruction of in-terlobular bile ducts, and canalicular cholestasis (Figure). Liver en-zyme levels returned to normal within 8 weeks after withdrawal ofLaitan. A lymphocyte transformation test (1) performed after recov-ery indicated strong and concentration-dependent T-cell reactivity toLaitan (stimulation index, 13.2) but not Exsepta. Phenotyping ofcytochrome P4502D6 activity with debrisoquine showed that thepatient was a poor metabolizer. We also performed phenotyping in apatient who had had positive results on a rechallenge test (3) andfound that she was a poor metabolizer of debrisoquine. Since thelocal prevalence of CYP2D6 deficiency is 9% (4), the probabilitythat two consecutive patients are deficient is less than 0.01%.
Figure. Liver biopsy specimen showing an inflamedportal tract.
A mixed cellular infiltrate is dominated by lymphocytes, exhibits eosin-ophil granulocytes and activated macrophages, and involves an interlob-ular bile duct (hematoxylin–eosin stain; original magnification, 3 175).
Letters
68 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 www.annals.org

The histologic findings and the results of the lymphocyte trans-formation test are compatible with an immune-mediated reaction,possibly mediated through a reactive metabolite. In humans, kava-lactones are metabolized through hydroxylation (2), but the involvedenzymes have not been identified. The present data strongly suggestthat kava preparations may be hepatotoxic and that CYP2D6 defi-ciency is a risk factor, as is the antianginal agent perhexiline (5).
Stefan Russmann, MDBernhard H. Lauterburg, MDUniversity of Bern3010 Bern, Switzerland
Arthur Helbling, MDInselspital3010 Bern, Switzerland
References1. Nyfeler B, Pichler WJ. The lymphocyte transformation test for the diagnosis of
drug allergy: sensitivity and specificity. Clin Exp Allergy. 1997;27:175-81. [PMID:
0009061217]
2. Duffield AM, Jamieson DD, Lidgard RO, Duffield PH, Bourne DJ. Identification
of some human urinary metabolites of the intoxicating beverage kava. J Chromatogr.
1989;475:273-81. [PMID: 0002777959]
3. Strahl S, Ehret V, Dahm HH, Maier KP. [Necrotizing hepatitis after taking herbal
remedies]. Dtsch Med Wochenschr. 1998;123:1410-4. [PMID: 0009856112]
4. Schmid B, Bircher J, Preisig R, Kupfer A. Polymorphic dextromethorphan metab-
olism: co-segregation of oxidative O-demethylation with debrisoquin hydroxylation.
Clin Pharmacol Ther. 1985;38:618-24. [PMID: 0004064464]
5. Morgan MY, Reshef R, Shah RR, Oates NS, Smith RL, Sherlock S. Impaired
oxidation of debrisoquine in patients with perhexiline liver injury. Gut. 1984;25:1057-
64. [PMID: 0006479680]
Medication Assistance Programs
TO THE EDITOR: Prescription medications are the most rapidly ex-panding component of national health care expenses. Ninety billiondollars were spent on prescription drugs in 1998, and this number isprojected to increase to $171 billion by 2007, representing 8% oftotal national health care expenditures (1). Approximately 16% ofthe U.S. population does not have health insurance, and a greaterpercentage has health insurance that does not include a prescriptionmedication benefit (2). Therefore, it is becoming increasingly diffi-cult for some segments of the population to purchase the prescrip-tion drugs that they need.
Many pharmaceutical companies offer assistance by providingfree or reduced-cost medications to patients who meet specific finan-cial criteria. A wide range of medications for many indications areprovided in these programs. Drugs may be provided free, or patientsmay be required to pay a fee or shipment charge. Medications aresupplied by direct delivery to the patient or physician, or the patientmay be issued a benefit card or voucher that must be presented at apharmacy. The amount of medications given and the length of timethat a patient may be enrolled vary.
Physician involvement is necessary for patient enrollment in
these programs, so clinicians must be informed about them to in-crease patient access to medications. Information concerning medi-cation assistance programs sponsored by pharmaceutical companiescan be obtained from a variety of sources, including PharmaceuticalResearch and Manufacturers of America, such publications as Reim-bursement Assistance Programs Sponsored by the Pharmaceutical Indus-try and the Directory of Prescription Drug Patient Assistance Programs,and various Internet sites (3, 4). However, the best source of infor-mation about assistance programs and specific details concerningpatient eligibility and program enrollment is the manufacturer of themedication.
Of course, these programs are not the solution to this universalproblem of medication access, and it is important to note that theyoperate at the discretion of the pharmaceutical company and may there-fore be terminated at any time. Nonetheless, it is equally importantto be aware of their existence as a possible source for medications.The Appendix Table, available on the Annals Web site (www.annals.org), provides an extensive listing of many medications whose man-ufacturers offer medication assistance programs (5).
Marie A. Chisholm, PharmDJoseph T. DiPiro, PharmDUniversity of Georgia College of PharmacyAthens, GA 31062Medical College of GeorgiaAugusta, GA 30912-2450
References1. Smith S, Freeland M, Heffler S, McKusick D. The next ten years of health spend-
ing: what does the future hold? The Health Expenditures Projection Team. Health Aff
(Millwood). 1998;17:128-40. [PMID: 0009769576]
2. Current population reports. Health insurance coverage, 1998. Bureau of the Census.
Washington, DC: Government Printing Office; 1999.
3. Windisch P, Webb J. Reimbursement assistance programs sponsored by the phar-
maceutical industry. Chicago: University Health System Consortium Services Corpo-
ration; 1997.
4. Directory of Prescription Drug Patient Assistance Programs 1999–2000. Washing-
ton, DC: Pharmaceutical Research and Manufacturers of America; 1999.
5. The top 200 prescriptions for 1998 by number of US prescriptions dispensed.
Available at http://www.rxlist.com/98top.htm.
Acute Renal Failure Related to High-Dose Celecoxib
TO THE EDITOR: A 57-year-old woman developed acute renal failureon 6 July 2000. She had been prescribed celecoxib, 200 mg/d, 10months earlier for symptomatic osteoarthritis and had been followedwith bimonthly visits thereafter. Her baseline creatinine and bloodurea nitrogen (BUN) levels were normal at 88 mmol/L (1.0 mg/dL)and 3.9 mmol/L (11 mg/dL), respectively. In the last half of June2000, her orthopedist doubled the daily celecoxib dose to 400 mg.Two weeks later, on 6 July 2000, she presented with marked depen-dent edema and markedly elevated blood pressure (160/110 mmHg). Creatinine and BUN levels were elevated at 265 mmol/L (3.0mg/dL) and 15.4 mmol/L (43 mg/dL), respectively. Celecoxib ther-
Letters
www.annals.org 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 69

apy was discontinued on 7 July 2000, and a complete work-up foracute renal failure was begun on 14 July 2000. Results of thework-up were negative, and renal function returned to normal;creatinine and BUN levels decreased to 88 mmol/L (1.0 mg/dL) and6.8 mmol/L (19 mg/dL), respectively. Edema and hypertension alsoresolved.
A MEDLINE search for celecoxib and acute renal failure re-vealed only two cases, reported by Perazella and Eras in May 2000(1). This is the second report and the third case involving this seriousproblem with a widely used drug. In February 1999, Moreland andSt. Clair (2) reviewed the use of analgesics, including the new cyclo-oxygenase-2 inhibitors, for pain management in patients with rheu-matic diseases; the notorious renal side effects of nonsteroidal anti-inflammatory drugs (NSAIDs) were also reviewed. In December1999, Brater (3) reviewed the effects of NSAIDs on renal function,with a focus on cyclooxygenase-2 inhibitors. All NSAIDs seem toshare nephrotoxic side effects, including decreased sodium excretion,decreased potassium secretion, and decreases in renal perfusion. Pre-liminary data suggest that cyclooxygenase-2 inhibitors also affect re-nal prostaglandins. It now seems that these shared renal effects alsoinclude acute renal failure and that they are dose related.
Mark G. Graham, MDJefferson Medical CollegePhiladelphia, PA 19107
References1. Perazella MA, Eras J. Are selective COX-2 inhibitors nephrotoxic? Am J Kidney Dis.
2000;35:937-40. [PMID: 0010793030]
2. Moreland LW, St Clair EW. The use of analgesics in the management of pain in
rheumatic diseases. Rheum Dis Clin North Am. 1999;25:153-91, vii. [PMID:
0010083963]
3. Brater DC. Effects of nonsteroidal anti-inflammatory drugs on renal function: focus
on cyclooxygenase-2-selective inhibition. Am J Med. 1999;107:65S-71S. [PMID:
0010628595]
Usefulness of Online Mendelian Inheritance in Man inClinical Practice
TO THE EDITOR: The concomitant growth of genetic research andinformation technology has given birth to electronic genetic data-bases, the utility of which should not go unnoticed by medical prac-titioners. Online Mendelian Inheritance in Man (OMIM), a data-base of human genes and genetic diseases maintained by JohnsHopkins School of Medicine, is freely accessible on the Internet(1, 2). The OMIM gene map is a table of loci of inherited disordersarranged in order. We report a case illustrating the usefulness ofOMIM in clinical practice.
A 37-year-old congenitally deaf and mute man presented to ourservice with bacterial pneumonia. His history was significant forchronic renal failure secondary to primary hyperoxaluria, which wasdiagnosed when he was 26 years of age. Initial work-up also revealeddilated cardiomyopathy and severe hypothyroidism of uncertaincause. In addition, over an 11-year period, the patient had multiple
thromboembolic events, including deep venous thromboses, atrio-venous graft thromboses, and pulmonary emboli, that were due toprotein C deficiency. Of note, several of the patient’s family mem-bers are also deaf and mute. Aware that protein C deficiency wasassociated with a single gene defect, we used the OMIM gene map toascertain the location of this gene and to determine whether possibledefects in neighboring loci were associated with the other diseaseentities present in our patient. The search revealed that the long armof chromosome 2 (2q) includes loci associated with protein C defi-ciency (2q13-14); type 1 primary hyperoxaluria (2q36-37); type 16autosomal dominant deafness (2q23-24.3); congenital hypothyroid-ism due to thyroid dysgenesis or hypoplasia (2q12-14); and dilatedcardiomyopathy types 1H, 1G, and 1I (2q14-22, q31, and q35,respectively) (1). A defect affecting 2q may have accounted for thecomplex clinical picture in our patient.
Electronic genetic databases are a valuable diagnostic tool forthe clinician and may suggest appropriate follow-up for patients andfamilies.
Bara Mouradi, BSUniversity of California, Irvine, Medical CenterHuntington Beach, CA 92646
Brian S. Andrews, MD, PhDUniversity of California, Irvine, Medical CenterOrange, CA 92868
References1. Online Mendelian Inheritance in Man (OMIM). McKusick-Nathans Institute for
Genetic Medicine, Johns Hopkins University (Baltimore, MD) and National Center
for Biotechnology Information, National Library of Medicine (Bethesda, MD). 2000.
Available at www.ncbi.nlm.nih.gov/omim/.
2. Hamosh A, Scott AF, Amberger J, Valle D, McKusick VA. Online Mendelian
Inheritance in Man (OMIM). Hum Mutat. 2000;15:57-61. [PMID: 0010612823]
Idiopathic Thrombocytopenic Purpura in a 101-Year-OldWoman
TO THE EDITOR: A 101-year-old woman, born on 25 December1898, presented to our institution with a 2-day history of generalweakness and presyncope. The platelet count was 0.0014 3 109
cells/L, hemoglobin and leukocyte counts were normal, and reviewof the peripheral smear revealed no clumping or schistocytes. Fivemonths before admission, the patient had a normal platelet count.Her medical history was significant only for hypertension and glau-coma. She was taking calcium carbonate, hydrochlorothiazide, lisin-opril, docusate, doxazosin, and acetaminophen and had not receivedany recent transfusions or intravenous fluids. Physical examinationrevealed several areas of ecchymoses and petechia on her trunk andupper extremities; lymphadenopathy and hepatosplenomegaly werenot present. Findings on computed tomography of the head, serumchemistry tests, and coagulation studies were normal. A presumptivediagnosis of immune thrombocytopenia was made.
The patient received one six-pack of multidonor platelets and1 g of intravenous methylprednisolone, and her platelet count in-
Letters
70 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 www.annals.org

creased to 0.011 3 109 cells/L. She was hospitalized and treated withmethylprednisolone and intravenous immunoglobulin (2 g/kg ofbody weight over 5 days). On the fourth hospital day, her plateletcount increased to 0.115 3 109 cells/L. She was discharged on thefifth hospital day with a prednisone taper. At her 3-month follow-upvisit, the platelet count was 0.209 3 109 cells/L. After 1 year offollow-up, the patient remains healthy with a normal complete bloodcount and no other medical problems.
The annual incidence of idiopathic thrombocytopenic purpuraranges from 1 to 13 per 100 000 persons (1). It usually occurs inwomen in their second and third decades of life (2). To our knowl-edge, our patient is the oldest described patient with this disorder.Previously, the oldest described patient was 89 years of age (3). Arecent observational study (4) suggests that the incidence of the dis-order in adults increases with age. As patients live longer, our patientmay be the first of many presenting with idiopathic thrombocytope-nic purpura in the second century of life.
Kevin K. Chung, MDLouis R. Macareo, MDTeresa A. Coleman, MDDwight D. Eisenhower Army Medical CenterAugusta, GA 30905
References1. Diagnosis and treatment of idiopathic thrombocytopenic purpura: recommenda-
tions of the American Society of Hematology. The American Society of Hematology
ITP Practice Guideline Panel. Ann Intern Med. 1997;126:319-26. [PMID:
0009036806]
2. Mueller-Eckhardt C. Idiopathic thrombocytopenic purpura (ITP): clinical and
immunologic considerations. Semin Thromb Hemost. 1977;3:125-59. [PMID:
0000322289]
3. Weiss GB, Klock JC, Richardson HB. Idiopathic thrombocytopenic purpura in the
elderly [Letter]. Lancet. 1975;1:411-2. [PMID: 0000046576]
4. Frederiksen H, Schmidt K. The incidence of idiopathic thrombocytopenic purpura
in adults increases with age. Blood. 1999;94:909-13. [PMID: 0010419881]
Correction: Physicians and Joint Negotiation
In the position paper “Physicians and Joint Negotiations” (1), thethird position contained an inadvertent error regarding collectivenegotiations by residents. The correct policy position that was ap-proved by the Board of Regents of the American College of Physi-cians–American Society of Internal Medicine on 17 July 1999 isprovided below and should be substituted for the position in italicsthat appeared on the top of page 790. Both the abstract and theconclusion of the paper should also be modified accordingly.
Physicians-in-training should have means available tocommunicate with their program directors and supervisors
to address and resolve concerns about patient care, sti-pends, hours, and other working conditions. Educationalcontent should remain the purview of the appropriate Res-idency Review Committee (RRC) and program directors,and should not be subject to negotiations.
The second paragraph of the abstract should be corrected toomit the phrase “collective bargaining is not appropriate for residentphysicians” and should read as follows:
The College states that employed physicians shouldcontinue to have negotiating rights. It maintains, despite arecent decision by the National Labor Relations Board,that physicians in residency training are protected by ac-creditation requirements for programs of graduate medicaleducation, and educational content should not be subjectto negotiations.
The following revision is also necessary in the conclusion. Thesentence “Residents have other mechanisms available to them thatare more appropriate than collective bargaining in the educationalenvironment” should read as follows:
Residents have other mechanisms available to them toresolve disputes in the educational environment.
These changes do not represent a change in American Collegeof Physicians–American Society of Internal Medicine policy.
Jack Ginsburg, MPEAmerican College of Physicians–American Society of Internal MedicinePhiladelphia, PA 19106
Reference1. Physicians and joint negotiations. American College of Physicians–American Society
of Internal Medicine. Ann Intern Med. 2001;134(9 Pt 1):780-2. [PMID: 11329239]
Correction: Risk Factors for Coronary Heart Disease in Men18 to 39 Years of Age
In a recent article on risk factors for coronary heart disease in 18- to39-year-old men (1), the first line of the figure legend should read“Receiver-operating characteristic curves for prediction of fatal coro-nary heart disease in young men over 20 years,” not “Receiver-oper-ating characteristic curves . . . in young men older than 20 years of age.”
Reference1. Navas-Nacher EL, Colangelo L, Beam C, Greenland P. Risk factors for coronary
heart disease in men 18 to 39 years of age. Ann Intern Med. 2001;134:433-9. [PMID:
11255518]
Letters
www.annals.org 3 July 2001 Annals of Internal Medicine Volume 135 • Number 1 71