Embed Size (px)
Citation preview

Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735
Contents lists available at SciVerse ScienceDirect
Best Practice & Research ClinicalGastroenterology
3
Gastric and duodenal neuroendocrine tumours
Dermot O’Toole, MD, FRCPI, Associate Professor ofGastroenterology & Clinical Medicine a,*,Gianfranco Delle Fave, MD, PhD, Professor of Medicine b,Robert T. Jensen, MD, Chief, Cell Biology Section c
aDepartment of Gastroenterology and Clinical Medicine, St James’s Hospital and Trinity College,Dublin, IrelandbDepartment of Digestive and Liver Disease, Ospedale Sant’Andrea, Rome, ItalycDigestive Diseases Branch, NIDDK, NIH, Bethesda, MD, USA
Keywords:Neuroendocrine tumoursGastrinStomachGastric neuroendocrine tumoursDuodenal neuroendocrine tumours
* Corresponding author. Tel.: þ353 863728832.E-mail address: [email protected] (D. O’Too
1521-6918/$ – see front matter � 2013 Elsevier Lthttp://dx.doi.org/10.1016/j.bpg.2013.01.002
a b s t r a c t
Gastric neuroendocrine neoplasms (NENs) are increasing in fre-quency and have a varied spectrum with regard to histology,clinicopathologic background, stage, and prognosis. They areusually discovered incidentally, are for the most part benign andare associated with hypergastrinaemia (secondary either tochronic atrophic gastritis or rarely Zollinger–Ellison syndrome;types 1 and 2, respectively) or more rarely sporadic type 3. Ap-plications of recent staging and grading systems – namely usingKi-67 proliferative indices – (from ENETS and WHO 2010) can beparticularly helpful in further categorising these tumours. Thenatural history of Type 1 gastric carcinoids is generally (>95%)favourable and simple surveillance is usually recommended forsmall (<1 cm) T1 tumours, with local (endoscopic or surgical)resection for larger lesions. Other potential therapies such as so-matostatin analogues and gastrin receptor antagonists may offernewer therapeutic possibilities. Rarely, gastric NENs have a malig-nant course and this is usually confined to Type 2 and especiallyType 3 tumours; the latter mimic the biological course of gastricadenocarcinoma and require radical oncological therapies. Mostduodenal NENs, apart from gastrinomas (that are not dealt withhere) are sporadic and non functional. They are also increasing infrequency probably due to incidental discovery at endoscopy or
le).
d. All rights reserved.

D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735720
imaging for other reasons and this may account for their overallgood prognosis. Peri-ampullary and ampullary NENs may havea more aggressive outcome and should be carefully appraised andtreated (often with surgical resection).
� 2013 Elsevier Ltd. All rights reserved.
Introduction
Neuroendocrine-derived tumours, originally termed carcinoid tumours, are derived from enter-ochromaffin or Kulchitsky cells. The term carcinoid was first used by Oberdorfer in 1907 to describea carcinoma-like tumour, which was considered to have less malignant potential than adenocarci-nomas and which may have a broad spectrum of biological behaviours [1,2]. The term neuroendocrinetumour (NET) or neuroendocrine neoplasm (NEN) has supplanted carcinoid in the current nomen-clature, although carcinoid tumours may be considered a specific subtype of functioning neuro-endocrine tumours that produces serotonin. Gastric and duodenal NENs account for a relatively smalland heterogeneous population that differ considerably in clinicopathological, histologic differentiation,stage and prognosis. There have been important additions to the literature on gastric and duodenalNENs, largely on epidemiological and pathological aspects. However, clinical trials are rare and creatinglarge registries will be an important step to further our understanding of these tumours. This reviewseeks to present an overview of recent developments in understanding of the biology of gastric andduodenal NENs and the current approach to their classification, staging and management.
Classification, epidemiology and clinical features (Table 1)
Gastric NENs
Gastric NENs can be broadly categorised into well and poorly differentiated gastric NETS [3]. Thesetumours are subdivided into those arising from enterochromaffin cell hyperplasia due to excess gastrinstimulation (Types 1 and 2) and sporadic tumours (that may be well or poorly differentiated tumours)[4] (Table 1). Since the 1950s, there has been a marked increase in the reported incidence of gastricNENs, accounting currently for approximately 1.8% of gastric malignancies compared to 0.3% previously[5]. Age-adjusted incidence rates have shown an 800% increase in incidence in Caucasian females [5].This may reflect the increased incidence of chronic atrophic gastritis amongst females, increased ratesof PPI use or better detection and reporting. While acid suppression with PPIs has been shown toincrease gastric NEN formation in rodents [6] this has not been borne out in humans. There has been an8–9-fold increase in the incidence of gastric NENs reported in two large databases (Florida Cancer dataSystem and SEER registries) over twenty years (1981–2000) [7]. This represents an increase in the age-adjusted incidence from <0.03 per 100,000 population to 0.2. Of these tumours, the majority werelocalised (94%), with distant metastases in just 1%. Themean age of the patient populationwas 65 years(21–96 years) [7]. The most frequent gastric NENs is Type I comprising 70–80% of the total, and occurmore frequently in women (64.5%), with a mean age of presentation of 63 [2]. Yearly age-adjustedincidence is approximately 0.2 per population of 100,000 [2]. These tumours arise in patients withchronic atrophic gastritis (CAG) – thatmay be immune or non-immune-related –where the decrease ingastric pH results in compensatory hypergastrinaemia and via binding to CCK-2 receptors, ECL cellhyperplasia [8]. Gastrin signals via the CCK-2 receptor activate protein kinase C and MAP kinase tostimulate an anti-apoptotic effect in AGS-G gastric carcinoma cells stably transfected with the CCK-2receptor by inducing expression of the anti-apoptotic protein, mcl-1, and mcl-1 expression is alsoincreased in human hypergastrinaemia-associated type I gastric NETs [9]. The relationship betweenCAG and type I gastric carcinoids was recently examined in a cohort of 367 patients with CAG [10].Tumours were present at index endoscopy in nine (2.4%) patients and after 1463 person/years, sixpatients developed type I tumours (annual incidence rate, person-year of 0.4%) [10]. Hyper-gastrinaemia alone is probably insufficient for tumour development; since chronic PPI use or vagot-omy, do not appear to be associated with gastric NETs, and proposed co-factors include genetic,

Table 1Characteristics of gastric neuroendocrine tumours.
Type 1 Type 2 Type 3
Proportion, % 70–80 5–6 14–25Gastric localisation Corpus, fundus Body, fundus, antrum AntrumEndoscopic and
morphologicalcharacteristics
Single/multiple (60%),small (<1 cm); polyploidor submucosal
Often multiple, small(<1–2 cm); polyploid(sessile)
Single, large size(>2 cm); occasionallyulcerated
Associated disorders CAG; achlorhydria Gastrinoma/MEN-1 SporadicHistology Well differentiated Well differentiated Well differentiated,
poorly differentiatedor mixed endo/exocrine
Gastrin [ [ NormalGastric pH [ Y NormalRisk of metastases, % 2–5 10–30 50–100Management - <5 mm: biopsies of the
tumour and gastric epithelium(antral and body/fundus) tolook for associated CAG andECL cell hyperplasia;
- <10 mm surveillance;- 1–2 cm (uT1 on EUS) –endoscopic resection
- >2 cm, uT2 or þ marginfollowing incompleteendoscopic resectiondiscuss surgery(wedge resection)
Treatment dictated oftenby associated gastrinomasor non functioningpancreatic tumours; iftreatment of gastric tumourrequired considerendoscopic resection/surgery
Oncological surgicalresection (partialof total gastrectomy)
Surveillance Annual or every two years; biopsiesfrom tumours and looks forassociated field defects associatedwith atrophy-metaplasia-dysplasiasequence
Surveillance specific toassociated gastrinomasand MEN-1; annual OGD
According to subtypeof tumour (at least sixmonths initially)
CAG: chronic atrophic gastritis.ECL: enterochromaffin-like.OGD: oesophagogastroduodenoscopy.MEN-1: multiple endocrine neoplasia type 1.
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 721
dietary/environmental, hormones and growth factors and bacteria. The Reg (regenerating geneproduct) 1a gene, a proliferative suppressor in response to gastrin, may be dysregulated in Type 1gastric NEN [11]. Gastric NENs are typically found during upper GI endoscopy, often incidentally (ex-plorations for non-specific symptoms or dyspepsia) or during investigations for macrocytic or irondeficiency anaemia [12–16]. The majority of Type I NENs are benign (>95%), often multiple (>60%),usually<2 cm (median diameter 5 mm) and are exclusively localised to the gastric body or fundus [17–19]. They may present in a wide variety of endoscopic/morphological aspects (Figs. 1 and 2) – sessile,firm, papules, rarely polypoid and may also be detected at biopsies (microcarcinoids, 22%) [3]. Mosttype 1 gastric NENs are WHO group G1 or G2. Their natural course remains poorly defined but overallsurvival rates are excellent; disease-specific survival approaches 100% [3]. Presence of metastases,a rare event (<5%) [3,20,21] was the only factor which influenced long-term prognosis in a series of 51cases [22]. The metastatic potential is proportional to tumour size and more deeply infiltrating tu-mours, but there is no correlation between the degree of multicentricity and metastases [22–24].Outcome even in the presence of metastases is reasonable – a 75% 5-year survival compared to 98% fornon-metastatic disease was reported [22]. Despite a relatively high frequency of these tumours thepublished experience on metastases remains relatively limited [22,25–29].
Type II gastric NENs account for 5–8% of gastric NENs, are associated with Multiple EndocrineNeoplasia type 1 (MEN-1) and Zollinger–Ellison syndrome (ZES), and have intermediate malignantpotential [30,31]. The synergy of the presence of the tumour-suppressor gene mutation on chromo-some 11 and the hypergastrinaemia of ZES associated with MEN-1 promotes the development ofgastric NENs in 23% of MEN-1 patients [32,33]. The menin tumour suppressor gene interacts with

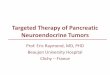
Fig. 1. a: Typical endoscopic appearance of a type 1 gastric neuroendocrine neoplasm (NEN); note the smooth adjacent mucosa ina patient with chronic atrophic gastritis.; b: A type 1 gastrin NEN with a more polypoid appearance; c: this type 1 gastric NEN hasa more intra- or submucosal aspect and is well defined on EUS (d) as a well defined hypoechoic 8 mm lesion lying within thesubmocosal layer and at a distance form the deeper layers (uT1). e: Biopsies (40 � magnification) reveal (H&E) features consistentwith a well differentiated appearance with polygonal cells with abundant pale cytoplasm; the nuclei are round/oval regular in sizeand have a granular chromatin pattern with micronucleoli. Diffuse strongly staining for chromogranin A is seen (f). The proliferativeindex (MIB-1 immunostain for Ki-67) is <2% (G1).
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735722

Fig. 2. Type 1 gastric neuroendocrine tumour that measures 12 mm in the gastric body and was a uT1 on EUS. This lesion wasresected using an EMR technique (Duette kit, Cook) following injection of a small amount of methylene blue to lift the lesion fromthe deep muscle layer. The blue deep submucosa/muscularis propria is seen in the clean base following resection (b). C: Histology (H& E) and immunohistochemistry for chromogranin A is diffusely positive (d) with a low Ki-67 proliferative indeed of 2% (insert, e).
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 723
a member of the AP-1/JunD pathway which may be co-stimulated by gastrin [34]. Type II gastriccarcinoids are estimated to be >70-fold more frequent in MEN1/ZES patients than those with sporadicZES (No MEN1), because gastric carcinoids occur in the latter group in <1% of patients [33,35]. Loss ofheterozygosity of the MEN-I gene locus on 11q13 has also been described in the other types of gastricNENs – in 17–73% of Type I tumours and 25–50% in Type III tumours [36,37]. Type II NENs displaya relatively indolent behaviour but do have a greater metastatic potential than Type I tumours, withapproximately 10–30%metastasising [30,31,38].Where Type I tumours are limited to themucosa of thebody and fundus (Figs. 1 and 2), Type II may also occur in the gastric antrum (Fig. 3).
Type III tumours represent approximately 15–20% of gastric NENs, arise sporadically and are themost aggressive gastric NEN subtype; between 50 and 100% metastasise [4,20] (Table 1). Theirdevelopment and biology is unrelated to gastrin concentration. They are frequently large (>2 cm) andlocalised in the gastric antrum (Fig. 4). They typically produce 5-hydroxytryptophan (5-HT) rather thanserotonin. Carcinoid syndrome is a rare presentation of gastric NENs (<1%) and almost exclusivelyassociated with Type III tumours with associated liver metastases. Some advocate the subdivision ofType III tumours into two groups (Type III and IV), where Type III tumours are sporadic non-functioning gastric NETs and Type IV tumours are those that are poorly differentiated or arise fromACTH or serotonin-cells or are of mixed endocrine–exocrine aetiology [22]. The clinical behaviour of allof these tumour types is similar and distinguishing them as separate types, of entities has little clinicalutility, at least from a management viewpoint. Mutation of the tumour suppressor gene p53 has beenreported to be strongly correlated with Type III tumours and functionally may play a role in stimulatingproliferation [39]. Differential gene expression signatures specific to Type III compared with Type I andII gastric NENs has also been found [40]. Of 270 genes differentially altered, CgA [41], MAGE-D2(adhesin), MTA1 (histone deacetlyase regulator) [42] b and CCN2 (growth factor) [40] can differ-entiate between Type III and I tumours.
Duodenal NENs
Duodenal NENs comprises up to 3% of all duodenal tumours [43] and almost 3% of all NEN tumoursin the pan SEER Registry (1973–1999) [44–46]. Their incidence is 0.19 in the latest SEER data set [47]. Insome studies, duodenal NENs were classified generally into five different tumour types [46,48].Duodenal NENs comprise largely gastrinomas (not dealth with here), somatostatinomas, non-

Fig. 3. Example of a Type 2 gastric neuroendocrine neoplasm (NENs) with multiple tumours of various size in the gastric body andproximal antrum (a) and in the 2nd part of the duodenum (b). At EUS of the gastric lesions, the NENs are seen (c, *) as well definedhomogeneous hypoechoic uT1 lesions. However, while a 9 mm duodenal tumour is see to be well within the T1 limits (d, *) EUSclearly demonstrates a lymph node adjacent to the duodenal wall (d, arrows).
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735724
functional tumours (that may stain for calcitonin and serotonin), duodenal gangliocytic para-gangliomas, and high-grade poorly differentiated NECs [48,49] (Table 5). Ampullary or peri-ampullarytumours may have a more aggressive behaviour and pathological expression [50–55]. The latter arefrequently associated with von Recklinghausen’s disease [49,53,56–60]. A recent review cites duodenalgastrinomas to be the most frequent (48%) followed by somatostatinomas (44%), non-functional se-rotonin-containing tumours (28%), non-functional calcitonin-containing NETs (9%) and finally raregangliocytic paragangliomas or NE carcinomas [46]. Many series include gastrinomas when consid-ering duodenal NENs and this almost certainly skews data with respect to many factors such as size,location andmetastatic potential. More than 90% of all duodenal NENs arise in the first and second partof the duodenum [49,61–64] and approximately 20% occur in the periampullary region [49]. They arecharacteristically small (mean, 1.2–1.5 cm) and [49] and>75% are<2 cm [49,53,63,65,66] (Fig. 5). Mostduodenal NENs are T1 but regional lymph node metastases has been reported to occur in 40–60% ofcases [48,49,67–69]; this contrasts with a 10% regional metastatic rate in latest SEER data [47]; again,inclusion of gastrinomasmay account for these discrepancies. Livermetastases generally occur in<10%of all patients with duodenal NENs [47,49]. Multiple tumours should lead to a suspicion of MEN-1 (thelatter is far more frequent occurring in up to 30% of tumours associated with ZES) [46,69,70].
Duodenal NENs present in the 6th decade and there is a slight male predominance (1.5/1 in latestSEER data set) [47]. These tumours are discovered incidentally (up to a third) or due to pain, bleeding oranaemia, jaundice or duodenal obstruction ordiarrhoea [46]. Obviously in duodenal NENassociatedwithgastrinoma symptoms of ZES occur and frank carcinoid syndrome can occur however it is rare (<4%).Other rare presentations include Cushing’s syndrome, acromegaly due to a GRF-secreting tumour,somatostatinoma syndrome, insulinoma, glucagonoma or due to the development of polycythaemia

Fig. 4. Macroscopic appearance of a Type 3 gastric neuroendocrine tumour found incidentally at upper GI endoscopy. a: Endoscopyreveals a polypoid mucosal/submucosal lesion with poor lifting following saline injection; b: Endoscopic ultrasound demonstratesa hypoechoic submucosal lesion in the distal stomach 1.1 cm extending to involve the deep muscle layer (muscularis propria); c:Gross appearance following partial gastrectomy: 1.3 cm polypoid lesion; d: Transverse section shows a firm, white tumour pre-dominantly submucosal. Na this was found at histology to be a well differentiated tumour with a Ki-67 of 6% (G2) with two positivelymph nodes.
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 725
rubra vera [49,57,59,60,71–73]. PeriampullaryNENsmore frequently presentwith jaundice and aremoreoften associated with von Recklinghausen’s disease (18%) and the presence of somatostatin immunor-eactivity (25–100%); however, a clinical somatostatinoma syndrome is very rare with these tumours[49,52,53,58,74,75].
Pathology, staging systems and prognosis
Gastric and duodenal NENs typically have a solid, yellow-tan or white gross morphology. As withother NENs, histologically, the tumour cells, with faint pink granular cytoplasm and round nuclei withfewmitoses, form trabecular, glandular or rosette-shaped patterns [76]. In a series of 205 gastric NENs,191 of 193 well differentiated tumours were mainly composed of enterochromaffin-like cells, with twotumours derived from G-cells [27]. There have been case reports of enterochromaffin cell and ghrelin-producing NENs [77]. Type III gastric NETs are occasionally functional and can secrete kinins, prosta-glandins, substance P, somatostatin, insulin, corticotrophin and neuron-specific enolase. Samplinggastric and duodenal lesions is usually simple and often biopsies suffice to obtain histological proof. Forgastric NENs, biopsies of fundic non-polypoid regions should also be performed to search for atrophic

Fig. 5. a. Example of a small (<10 mm) non functioning duodenal neuroendocrine neoplasm that was confined to the mucosa andsubmucosa (b), uT1 and without regional nodes at EUS and was fully excised using an EMR technique. The final histology confirmeda well differentiated NEN (G1) with a Ki-67 <1%.
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735726
gastritis [78] and also ECL cell hyperplasia (the predisposing condition leading to Type 1 gastric NENs).In addition, a careful exploration of the stomach in cases of gastric atrophy should be made to examinefor field defects and early adenomatous changes (associated with CAG) according to guidelines[3,46,79]. In addition to standard histology with haematoxylin and eosin, staining for chromogranin Aand synaptophysin [4,80–83] should be performed. Grading is also mandated with mitotic index/10HPF and Ki-67 proliferation index calculations [84,85]. Use of the WHO classification to distinguishNEN from NEC, and G1-G3 should also be performed.
Duodenal NENs share much homology with their gastric counterparts frequently (80%) showingargyrophilic (silver staining) [58,63,66,86] and being argentaffin-negative (0–12% positive) [58,66,86].A large proportion synthesise peptides/amines that may be biologically active. Their relative frequencyis: gastrinomas (48%), somatostatinomas (43%), non-functioning serotonin-containing tumours (27%),non-functioning calcitonin-containing tumours (9%), NEC G3, and gangliocytic paragangliomas [49].Duodenal somatostatinomas localise to the periampullary region and approximately half containpsammoma bodies [49,50,58,64–66,87]. Duodenal paragangliomas contain epithelial (PP and so-matostatin cells), ganglia, and spindle cells [49,64,88]. They characteristically contain gangliocyticdifferentiation and S-100 protein-immunoreactive Schwann cells [64,88].
Prognosis and outcome
ENETS and World Health Organization 2010 grade and stage classifications (Tables 2–4) wererecently tested together with additional clinicopathologic and histologic parameters in a series of 209gastric NENs (51 G3 NECs and 15 mixed endocrine/exocrine carcinomas or poor outcome separatedfrom 143 G1 or G2 NENs) with a median follow-up of 89 months [89]. Most G1 cases had excellentprognosis, even when metastatic, whereas G2 and G3 neoplasms had worse or very severe prognosis,respectively. ENETs and WHO 2010 proliferative grading system correlated well with patient survival.Standard staging using ENETS system was not effective for well differentiated gastric NENs but mod-ifications and use of a novel T (T1a and T1b or deep submucosal) and N categories (N1, b3 nodesmetastases; N2, �3) allowed a simplified, equally informative 3-stage TNM system.
Data from the SEER registry reveals that 76% of gastric NENs are localised at time of diagnosis [47].Survival trends have also improved as an overall five-year survival of 63% was shown compared withprevious data which estimated 51% [5]. Clearly, prognosis of gastric NENs varies according to tumour

Table 2ENETS TNM staging for gastric neuroendocrine neoplasms [115].
TNM
Tdprimary tumourTX Primary tumour cannot be assessedT0 No evidence of primary tumourTis In situ tumour/dysplasia (<0.5 mm)T1 Tumour invades lamina propria or submucosa and �1 cmT2 Tumour invades muscularis propria or subserosa or >1 cmT3 Tumour penetrates serosaT4 Tumour invades adjacent structures
For any T, add (m) for multiple tumoursNdregional lymph nodesNX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
Mddistant metastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1a Distant metastasis
StageDisease stagesStage 0 Tis N0 M0Stage I T1 N0 M0Stage IIa T2 N0 M0Stage IIb T3 N0 M0Stage IIIa T4 N0 M0Stage IIIb Any T N1 M0Stage IV Any T Any N M1
a M1 specific sites defined according to Sobin and Wittekind [116].
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 727
type. Type 1 tumours, being usually well differentiated and with low Ki-67 (NET G1), generally have anexcellent prognosis and early T1 lesions managed endoscopically can achieve close to 100% survival.Size plays an important role in metastatic potential and was recently found to be a stage-independentprognostic factor (�3 cm) where only three of 94 tumours �1 cm and only one (a NEC) of 59 tumours<0.5 cm were metastatic at diagnosis or during follow-up [89]. Deep submucosal invasion or angio-lymphinvasion have also been proposed as a poorer prognostic indicator [89–92]. Liver metastases arerare. Disease recurrence is infrequent with a recent median recurrence-free survival of 24months [93];interestingly in a small proportion of patients 3% developed more aggressive tumour behaviourbecoming high grade NECs [93]. Type 2 gastric NENs, displaying intermediate grading (G1 or G2) havea metastatic rate of 10–30%; although given their association with duodenal and pancreatic NENs aspart of MEN-1-related ZES, it may be difficult to accurately identify the ‘primary’ lesion responsible formetastases. Outcome in sporadic type 3 tumours is poor with a 25–30% five-year survival rate anda metastatic rate of 50–100% [4,23,94]. Subtypes I and II of gastric NENs are associated with anapproximate 80% five-year overall survival and Type III is associated with approximately 33% five-yearsurvival.
Diagnostic tests – biological, endoscopy and imaging tests
General markers for both gastric and duodenal NENs include serum chromogranin A with orwithout neuron specific enolase (especially if a G3 NEC is suspected). In addition, functional tumoursmay also require specific relevant assay estimations (e.g., gastrin, somatostatin, PP) [3,46]. Patientswith Type 1 gastric NENs present with elevated serum gastrin (important in making the diagnosis inconjunction with achlorhydria) and serum chromogranin A and levels may be hard to correlate withdisease status and generally are not useful as part of follow-up. A diagnosis of auto-immune relatedCAG is made in the presence of anti-parietal cell or anti-intrinsic factor antibodies (present in 50% of

Table 3ENETS TNM staging for duodenal, ampulla and proximal jejunum neuroendocrine neoplasms [115].
TNM
Tdprimary tumourTX Primary tumour cannot be assessedT0 No evidence of primary tumourT1 Tumour invades lamina propria or submucosa and size �1 cma
T2 Tumour invades muscularis propria or subserosa or size >1 cmT3 Tumour invades pancreas or retroperitoneumT4 Tumour invades peritoneum or other organs
For any T, add (m) for multiple tumoursNdregional lymph nodesNX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
Mddistant metastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1b Distant metastasis
StageDisease stagesStage I T1 N0 M0Stage IIa T2 N0 M0Stage IIb T3 N0 M0Stage IIIa T4 N0 M0Stage IIIb Any T N1 M0Stage IV Any T Any N M1
a Tumour limited to ampulla of Vater for ampullary gangliocytic paraganglioma.b M1 specific sites defined according to Sobin and Wittekind [116].
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735728
cases). Biological assays for associated auto-immune thyroiditis is also useful at baseline. For gastricNENs, genetic testing for hereditary tumour syndrome should only be performed in case of suspectedor established diagnosis of ZES. Germline testing for MEN-1 in patients with duodenal tumours isrestricted to cases of suspectedMEN-1, a family history suggestive of MEN-1 or withmultiple duodenaltumours (following genetic counselling).
Upper gastrointestinal endoscopy is recommended for all gastric NENs and for small (<1 cm) tu-mours is usually the only recommended imaging procedure. Here, biopsies from the dominant tumourare required, but in addition it is mandatory to sample the gastric antrum (two biopsies) and body/fundus (four biopsies) in addition to biopsies of the largest polyps [78]. Endoscopic ultrasound (EUS)enables assessment of the degree of parietal extension (invasion of the muscularis propria) andlocoregional lymph node invasion (essential in patients with gastric tumours �1 cm) and is recom-mended before resection of polyps 1–2 cm in diameter [19] (Figs. 1–4). The same principles hold truefor primary duodenal NEN, where axial endoscopy with biopsy is recommended and EUS to confirmthe diagnosis and locally stage the disease [46,95]; the latter is especially important as their size isusually small and may be localised to the submucosal and not detected on axial endoscopy. In factduodenal gastrinomas are hard to detect even with aid of EUS and combination with somatostatinreceptor scintigraphy (SRS) or 68-gallium PET-CT can increase detection rates. In cases of sporadicgastric tumours (Type 3), a more extensive imaging protocol should be performed and in addition to
Table 4ENETS Grading system for foregut tumours [115].
Grade Mitotic count (10 HPF)a Ki-67 index (%)b
G1 <2 �3G2 2–20 3–20G3 >20 >20
a 10 HPF: high power field¼ 2mm2, at least 40 fields (at 40�magnification) evaluated in areas of highestmitotic density.
b MIB1 antibody; % of 2,000 tumour cells in areas of highest nuclear labelling.

Table 5Classification duodenal neuroendocirne neoplasms (adapted from [3]).
NEN Grade 1 Benign: non-functioning,confined to mucosa-submucosa, non-angioinvasive,<1 cm in sizeGastrin-producing tumour (upper part of the duodenum)
– Serotonin (5-HT)-producing tumour– Gangliocytic paraganglioma (any size and extension, periampullary)
Benign or low-grade malignant (uncertain malignant potential):confined to mucosa-submucosa, with or without angioinvasion, or >1 cm in size
– Functioning gastrin-producing tumour (gastrinoma), sporadic or MEN-associated– Non-functioning somatostatin-producing tumour (ampullary region) with or without– Neurofibromatosis type 1 non-functioning serotonin-producing tumour
NEN Grade 2 Low-grade malignant: invasion of the muscularis propria and beyond or metastasesFunctioning gastrin-producing carcinoma (gastrinoma), sporadic or MEN-1-associated
– Non-functioning somatostatin-producing carcinoma (ampullary region) with orwithout neurofibromatosis type 1
– Non-functioning or functioning carcinoma (with carcinoid syndrome)– Malignant gangliocytic paraganglioma
NEC G3 High-grade malignant (large cell, small cell carcinoma)
D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 729
EUS (Fig. 4), axial imaging for loco-regional nodes and liver metastases is recommended along withsomatostatin receptor scintigraphy. Axial imaging with triple phase CT scan and/or MRI in conjunctionwith is recommended for large or suspicious Type 1 tumours and in all Type 2 and Type 3 gastric NENsto stage nodal, liver and bony metastases.
Treatment
a. Gastric NENs.
Surveillance, local resection
Management of gastric NENs is determined by subtype, and whether the disease is localised ormetastatic. Since the commonest subtype of gastric NEN (Type 1) usually displays a benign andindolent clinical behaviour, simple surveillance or localised endoscopic treatment modalities can beemployed for small tumours [26]: tumours <1 cm surveillance can be recommended; tumours be-tween 1 and 2 cm confined to mucosa/submucosa (guided by careful EUS appraisal – uT1) endoscopicresection is recommended with an experienced endoscopist in this field using endoscopic mucosalresection or ESD techniques (Fig. 2) to ensure complete resection. Endoscopic resection can be easilyrepeated provided tumours do not grow beyond T1 [3,96] and this strategy appears to be universallyaccepted Nonetheless, recurrences do occur and a recurrence rate in a recent series of patients treatedendoscopically was 64% (21/33) at a median of eight months and of these, 67% (14/21) had a secondrecurrence [19]. The TNM staging system uses 1 cm in size as a cut off to define T1/2 tumours, althoughthere is inconsistency in guidelines as to whether tumours between 1 and 2 cm should be treated withlocal resection. Surgery should be performed in case of involvement beyond submucosa, or positivemargin after endoscopic resection and either a local resection (e.g., wedge resection) and antrectomy ortotal gastrectomy depending on tumour histological features, invasion and localisation have beenrecommended. While antrectomy has the theoretical advantage of removing the stimulus for gastrinsecretion, this technique have become outdated by many expert groups [25] as the adequacy ofantrectomy has been questioned in the past and a simple wedge or localised excision followed byendoscopic surveillance may be more appropriate [3,8,25]. Follow-up for small tumours is annual orevery 24-month endoscopies (the latter may be appropriate for stable or non-recurring cases). Anoctreotide suppression test has been suggested as a means to assess whether type-1 gastric NENs arelikely to regress following antrectomy [97] (by assaying serum gastrin concentrations and gastriccorpus and tumour histidine decarboxylase mRNA abundances before and 72 h after the admin-istration of 25 mg/h intravenous octreotide and gastric tumour response can be assessed endoscopically

D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735730
following subsequent antrectomy). A positive test is not always predictive of tumour response toantrectomy [98].
Other medical therapies
Somatostatin analogues (SSA) are known to be potent inhibitors of gastrin secretion [99] from Gcells and thus reducing ECL cell hyperplasia. They have been demonstrated to be effective in decreasingthe size and number of Type 1 and 2 gastric NENs [21,100,101]. Complete disappearance of the tumourshas been reported in up to 70% and with significant reduction in gastrin levels [100]. Use of SSA cannotbe universally recommended, for what many believe to be a slow-growing indolent tumours (that arefrequently readily controllable using surveillance/endoscopic resection for enlarging tumours); how-ever their use in certain situations needs to be examined (tumours with slightly more aggressivebehaviour) [102]. Rebound growth following interruption of SSA therapy has also been suggested atmedium term follow-up in a small cohort of patients [103]. SSA cannot be recommended in patientswith sporadic Type 3 tumours where full oncological resection (partial or total gastrectomy) withadequate lymph node clearance is the treatment of choice following adequate preoperative staging. ForG1 and G2 tumours with advanced but limited disease (e.g., limited liver metastases) amenable tosurgery, SSA therapy should be considered following multidisciplinary consultation.
Gastrin (CCK-B) antagonist – several gastrin and CCKB receptor antagonists have been tested to tryto effect acid-related stimulation over the last 2 decades. Recently netazepide (YF476), a peripheralCCK-B (gastric) inhibitor has been shown to be a potent inhibitor of gastric acid secretion with rapidonset and a prolonged duration. Inhibition of CCK-B receptors with this agent has been found toproduce potent ECL-cell inhibition and the development of hypergastrinemia induced G-cell hyper-plasia. In Rodents netazepide has anti-tumour effects in various rodent models of gastric carcino-genesis driven by hypergastrinaemia [104–106]. A first report on this agent in patients with Type 1gastric NENs was recently published [107]. Here eight patients with multiple Type 1 gastric NENs anda background of CAG were treated orally once daily for 12 weeks in an open-label, pilot trial. Thetherapy was well tolerated and all experience a reduction in the number and size of their largest NENSerum chromogranin A reduced to normal levels at three weeks and remained so until 12 weeks, buthad returned to pre-treatment levels at 24 weeks. ECL hyperplasia and serum gastrin were unchangedby therapy (perhaps related to GAC present in these patients) [107]. Further data are required tosubstantiate CCKB inhibition as a possible targeted treatment of hypergastrinaemia-induced type 1gastric NEN but certainly this opens a new potential pathway to target.
b. Duodenal NENs
Curative resection is possible in themajority of patients with duodenal NENs as only 9% have [47,49]distant metastases at diagnosis [3,6,7,94,98,99,107]. Functional tumours can be treated using SSA tocontrol symptoms prior to considering surgery. Small (<1 cm) T1 tumours can be excised eitherendoscopically (EMR or ESD) or surgically (formal resections including pancreatico-duodenectomy(PD), duodenectomy and local excision) [46,55,66,108–110]. Therapies for curative resection shouldbe based on the localisation of the tumour and ease at which therapies can be applied as well as stagingextent and underlying tumour grade. Tumours close to or involving the ampulla could in theory becured by local excision and lymph node clearance/sampling but as no correlation between the tumoursize and the presence of malignancy [50,54,55,111] has been described an oncological resection(usually pancreaticoduodenectomy) is generally recommended.
Treatment of advanced disease
Treatment choices and strategies in cases of advanced inoperable stage 3 or 4 disease are similarwhether dealing with gastric or duodenal NENs and depend on the following considerations: presenceof symptoms, the differentiation and grade of the tumour and the slope or velocity of tumour growth[112,113]. Patients with symptoms due to hormonal hypersecretion often benefit from SSA and theseagents should be started early. Moreover, SSA have been shown to exert anti-proliferative effects in

D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 731
localised gastric NENs [21,100] however, data on therapeutic effects in the presence of advanced dis-ease is not available. However, like in other gastrointestinal NENs, SSA may be of value in subgroups ofpatients with slowly progressive low proliferative NET (G1) of gastroduodenal origin although specificdata are required to corroborate this. As gastro-duodenal NENs often fell into subgroups of trials onother foregut tumours (especially pancreatic) other possible chemotherapeutic options for well dif-ferentiated (G1, G2) gastro-duodenal NENs include systemic chemotherapy with streptozotocin-basedregimens, perhaps temozolamide, and newer molecular targeted therapies including sunitinib andeverolimus. However, data on the efficacy of such therapies is lacking due to the small numbers ofpatients treated with advanced gastro-duodenal NENs treated. Loco-regional therapies includingtrans-arterial hepatic (chemo)-embolisation, radiofrequency or microwave ablation or radio-embolisation may be used to treat well differentiated hepatic-predominant disease. Peptide receptorradionuclide therapy with lutetium-177- or yttrium-90-labelled SSA [112–114] may be useful in casesof octreotide-positive tumours although again there is not extensive experience specific to gastro-duodenal NENs.
Conclusion
While gastric NENs are increasing in frequency data are needed to support optimal treatmentstrategies especially for Type 1 tumours. While endoscopic follow-up is generally recommended andappears acceptable for the majority of patients with gastric Type 1 tumours (combined with localresection as tumours get larger) this could carry could some risk and is expensive and leads to repeatedexaminations and patient inconvenience. Use of SSA (or other agents targeting perhaps the gastrinreceptor) may be beneficial in some situations but has to be tested in large prospective studies. Our aimshould be to accurately balance between under and over-treatment to avoid unnecessary side effectsand high costs. Better stratification of tumour risk should permit a tailored approach to therapy. Type 2gastric NENs are managed within the context of MEN-1 associated with ZES and oncological resectionshould be considered for Type 3 tumours. Most duodenal NENs can be resected locally with theexception of ampullary and peri-ampullary lesions that usually require oncological resection due to themore aggressive patterns of behaviour.
Practice points
� Type 1 gastric neuroendocrine neoplasms are usually small and often multiple and developon a background of atrophic gastritis (auto-immune or not) are by far the most frequentgastric NET;
� Endoscopic surveillance of type 1 NENs is recommended for small tumours (<1 cm) andendoscopic resection for lesion >1 cm is recommended but requires expertise endoscopictechniques (EMR or ESD);
� Duodenal NENs are rare outside of gastrinomas and usually have a good prognosis, beingsmall and limited to the superficial layers (T1), rendering local therapy possible.
Research agenda
� Distinction between gastric and duodenal NENs liable to be more agressive and metastasisemerits evaluation;
� Detailed studies on the mechanism and durability of somatostatin analogue therapy as anti-proliferative agents in gastric type 1 NENs are required;
� Role and mechanism of CCK/gastrin receptor inhibition in gastric NENs opens excitingresearch possibilities

D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735732
Conflict of interest statement
There is no conflict of interest pertaining to this paper.
References
[1] Modlin IM, Moss SF, Chung DC, Jensen RT, Snyderwine E. Priorities for improving the management of gastro-enteropancreatic neuroendocrine tumors. J Natl Cancer Inst 2008;100:1282–9.
[2] Modlin IM, Moss SF, Oberg K, Padbury R, Hicks RJ, Gustafsson BI, et al. Gastrointestinal neuroendocrine (carcinoid) tu-mours: current diagnosis and management. Med J Aust 2010;193:46–52.
[3] Fave G, Kwekkeboom DJ, Van Cutsem E, Rindi G, Kos-Kudla B, Knigge U, et al. ENETS Consensus Guidelines for themanagement of patients with gastroduodenal neoplasms. Neuroendocrinology 2012;95:74–87.
[4] Rindi G, Luinetti O, Cornaggia M, Capella C, Solcia E. Three subtypes of gastric argyrophil carcinoid and the gastricneuroendocrine carcinoma: a clinicopathologic study. Gastroenterology 1993;104:994–1006.
[5] Modlin IM, Lye KD, Kidd MA. 50-year analysis of 562 gastric carcinoids: small tumor or larger problem? Am J Gastro-enterol 2004;99:23–32.
[6] Ono M, Sato H, Kazumori H, Yuki M, Rumi MA, Ortega-Cava CF, et al. Effect of a gastrin/cholecystokinin B receptorantagonist, S-0509, on the omeprazole-induced proliferation of gastric mucosa in rats. J Lab Clin Med 2003;142:364–71.
[7] Hodgson N, Koniaris LG, Livingstone AS, Franceschi D. Gastric carcinoids: a temporal increase with proton pumpintroduction. Surg Endosc 2005;19:1610–2.
[8] Delle Fave G, Capurso G, Annibale B, Panzuto F. Gastric neuroendocrine tumors. Neuroendocrinology 2004;80(Suppl. 1):16–9.
[9] Pritchard DM, Berry D, Przemeck SM, Campbell F, Edwards SW, Varro A. Gastrin increases mcl-1 expression in type Igastric carcinoid tumors and a gastric epithelial cell line that expresses the CCK-2 receptor. Am J Physiol GastrointestLiver Physiol 2008;295:G798–805.
[10] Vannella L, Lahner E, Annibale B. Risk for gastric neoplasias in patients with chronic atrophic gastritis: a critical reap-praisal. World J Gastroenterol 2012;18:1279–85.
[11] Higham AD, Bishop LA, Dimaline R, Blackmore CG, Dobbins AC, Varro A, et al. Mutations of RegIalpha are associated withenterochromaffin-like cell tumor development in patients with hypergastrinemia. Gastroenterology 1999;116:1310–8.
[12] Borch K, Renvall H, Liedberg G. Gastric endocrine cell hyperplasia and carcinoid tumors in pernicious anemia. Gastro-enterology 1985;88:638–48.
[13] Stockbrugger RW, Menon GG, Beilby JO, Mason RR, Cotton PB. Gastroscopic screening in 80 patients with perniciousanaemia. Gut 1983;24:1141–7.
[14] Modlin IM, Gilligan CJ, Lawton GP, Tang LH, West AB, Darr U. Gastric carcinoids. The Yale experience. Arch Surg 1995;130:250–5 [discussion 255–256].
[15] Thomas RM, Baybick JH, Elsayed AM, Sobin LH. Gastric carcinoids. An immunohistochemical and clinicopathologic studyof 104 patients. Cancer 1994;73:2053–8.
[16] Marignani M, Delle Fave G, Mecarocci S, Bordi C, Angeletti S, D’Ambra G, et al. High prevalence of atrophic body gastritisin patients with unexplained microcytic and macrocytic anemia: a prospective screening study. Am J Gastroenterol 1999;94:766–72.
[17] O’Toole D. Current trend: endocrine tumors of the stomach, small bowel, colon and rectum. Gastroenterol Clin Biol 2006;30:276–91.
[18] Crosby DA, Donohoe CL, Fitzgerald L, Muldoon C, Hayes B, O’Toole D, et al. Gastric neuroendocrine tumours. Dig Surg2012;29:331–48.
[19] Merola E, Sbrozzi-Vanni A, Panzuto F, D’Ambra G, Di Giulio E, Pilozzi E, et al. Type I gastric carcinoids: a prospective studyon endoscopic management and recurrence rate. Neuroendocrinology 2011;95:207–13.
[20] Rindi G, Azzoni C, La Rosa S, Klersy C, Paolotti D, Rappel S, et al. ECL cell tumor and poorly differentiated endocrinecarcinoma of the stomach: prognostic evaluation by pathological analysis. Gastroenterology 1999;116:532–42.
[21] Thomas D, Tsolakis AV, Grozinsky-Glasberg S, Fraenkel M, Alexandraki K, Sougioultzis S, et al. Long-term follow-up ofa large series of patients with type 1 gastric carcinoid tumors. Data from a multicenter study. Eur J Endocrinol 2013 Jan17;16(2):185–93.
[22] Borch K, Ahren B, Ahlman H, Falkmer S, Granerus G, Grimelius L. Gastric carcinoids: biologic behavior and prognosis afterdifferentiated treatment in relation to type. Ann Surg 2005;242:64–73.
[23] Rappel S, Altendorf-Hofmann A, Stolte M. Prognosis of gastric carcinoid tumours. Digestion 1995;56:455–62.[24] Solcia E, Rindi G, Buffa R, Fiocca R, Capella C. Gastric endocrine cells: types, function and growth. Regul Pept 2000;93:
31–5.[25] Gladdy RA, Strong VE, Coit D, Allen PJ, Gerdes H, Shia J, et al. Defining surgical indications for type I gastric carcinoid
tumor. Ann Surg Oncol 2009;16:3154–60.[26] Schindl M, Kaserer K, Niederle B. Treatment of gastric neuroendocrine tumors: the necessity of a type-adapted treatment.
Arch Surg 2001;136:49–54.[27] Rindi G, Bordi C, Rappel S, La Rosa S, Stolte M, Solcia E. Gastric carcinoids and neuroendocrine carcinomas: pathogenesis,
pathology, and behavior. World J Surg 1996;20:168–72.[28] Dakin GF, Warner RR, Pomp A, Salky B, Inabnet WB. Presentation, treatment, and outcome of type 1 gastric carcinoid
tumors. J Surg Oncol 2006;93:368–72.[29] Jordan Jr PH, Barroso A, Sweeney J. Gastric carcinoids in patients with hypergastrinemia. J Am Coll Surg 2004;199:552–5.[30] Norton JA, Melcher ML, Gibril F, Jensen RT. Gastric carcinoid tumors in multiple endocrine neoplasia-1 patients with
Zollinger-Ellison syndrome can be symptomatic, demonstrate aggressive growth, and require surgical treatment. Surgery2004;136:1267–74.

D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 733
[31] Norton JA, Warren RS, Kelly MG, Zuraek MB, Jensen RT. Aggressive surgery for metastatic liver neuroendocrine tumors.Surgery 2003;134:1057–63 [discussion 1063–1055].
[32] Debelenko LV, Emmert-Buck MR, Zhuang Z, Epshteyn E, Moskaluk CA, Jensen RT, et al. The multiple endocrine neoplasiatype I gene locus is involved in the pathogenesis of type II gastric carcinoids. Gastroenterology 1997;113:773–81.
[33] Berna MJ, Annibale B, Marignani M, Luong TV, Corleto V, Pace A, et al. A prospective study of gastric carcinoids andenterochromaffin-like cell changes in multiple endocrine neoplasia type 1 and Zollinger-Ellison syndrome: identificationof risk factors. J Clin Endocrinol Metab 2008;93:1582–91.
[34] Agarwal SK, Kennedy PA, Scacheri PC, Novotny EA, Hickman AB, Cerrato A, et al. Menin molecular interactions: insightsinto normal functions and tumorigenesis. Horm Metab Res 2005;37:369–74.
[35] Peghini PL, Annibale B, Azzoni C, Milione M, Corleto VD, Gibril F, et al. Effect of chronic hypergastrinemia on humanenterochromaffin-like cells: insights from patients with sporadic gastrinomas. Gastroenterology 2002;123:68–85.
[36] Modlin IM, Lye KD, Kidd M. Carcinoid tumors of the stomach. Surg Oncol 2003;12:153–72.[37] D’Adda T, Keller G, Bordi C, Hofler H. Loss of heterozygosity in 11q13-14 regions in gastric neuroendocrine tumors not
associated with multiple endocrine neoplasia type 1 syndrome. Lab Invest 1999;79:671–7.[38] Gilligan CJ, Lawton GP, Tang LH, West AB, Modlin IM. Gastric carcinoid tumors: the biology and therapy of an enigmatic
and controversial lesion. Am J Gastroenterol 1995;90:338–52.[39] Safatle-Ribeiro AV, Ribeiro Jr U, Corbett CE, Iriya K, Kobata CH, Sakai P, et al. Prognostic value of immunohistochemistry in
gastric neuroendocrine (carcinoid) tumors. Eur J Gastroenterol Hepatol 2007;19:21–8.[40] Kidd M, Modlin IM, Eick GN, Camp RL, Mane SM. Role of CCN2/CTGF in the proliferation of Mastomys enterochromaffin-
like cells and gastric carcinoid development. Am J Physiol Gastrointest Liver Physiol 2007;292:G191–200.[41] Kidd M, Modlin IM, Mane SM, Camp RL, Shapiro MD. Q RT-PCR detection of chromogranin A: a new standard in the
identification of neuroendocrine tumor disease. Ann Surg 2006;243:273–80.[42] Kidd M, Modlin IM, Mane SM, Camp RL, Eick GN, Latich I, et al. Utility of molecular genetic signatures in the delineation
of gastric neoplasia. Cancer 2006;106:1480–8.[43] Attanoos R, Williams GT. Epithelial and neuroendocrine tumors of the duodenum. Semin Diagn Pathol 1991;8:149–62.[44] Williams ED, Sandler M. The classification of carcinoid tum ours. Lancet 1963;1:238–9.[45] Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003;97:934–59.[46] Jensen RT, Rindi G, Arnold R, Lopes JM, Brandi ML, Bechstein WO, et al. Well-differentiated duodenal tumor/carcinoma
(excluding gastrinomas). Neuroendocrinology 2006;84:165–72.[47] Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after “carcinoid”: epidemiology of and
prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008;26:3063–72.[48] Kloppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO clas-
sification. Ann N Y Acad Sci 2004;1014:13–27.[49] Hoffmann KM, FurukawaM, Jensen RT. Duodenal neuroendocrine tumors: classification, functional syndromes, diagnosis
and medical treatment. Best Pract Res Clin Gastroenterol 2005;19:675–97.[50] Hatzitheoklitos E, Buchler MW, Friess H, Poch B, Ebert M, Mohr W, et al. Carcinoid of the ampulla of Vater. Clinical
characteristics and morphologic features. Cancer 1994;73:1580–8.[51] Walton GF, Gibbs ER, Spencer GO, Laws HL. Carcinoid tumors of the ampulla of Vater. Am Surg 1997;63:302–4.[52] Bornstein-Quevedo L, Gamboa-Dominguez A. Carcinoid tumors of the duodenum and ampulla of vater: a clin-
icomorphologic, immunohistochemical, and cell kinetic comparison. Hum Pathol 2001;32:1252–6.[53] Witzigmann H, Loracher C, Geissler F, Wagner T, Tannapfel A, Uhlmann D, et al. Neuroendocrine tumours of the duo-
denum. Clinical aspects, pathomorphology and therapy. Langenbecks Arch Surg 2002;386:525–33.[54] Clements WM, Martin SP, Stemmerman G, Lowy AM. Ampullary carcinoid tumors: rationale for an aggressive surgical
approach. J Gastrointest Surg 2003;7:773–6.[55] Hartel M, Wente MN, Sido B, Friess H, Buchler MW. Carcinoid of the ampulla of Vater. J Gastroenterol Hepatol 2005;20:
676–81.[56] Taccagni GL, Carlucci M, Sironi M, Cantaboni A, Di Carlo V. Duodenal somatostatinoma with psammoma bodies: an
immunohistochemical and ultrastructural study. Am J Gastroenterol 1986;81:33–7.[57] Swinburn BA, Yeong ML, Lane MR, Nicholson GI, Holdaway IM. Neurofibromatosis associated with somatostatinoma:
a report of two patients. Clin Endocrinol (Oxf) 1988;28:353–9.[58] Burke AP, Federspiel BH, Sobin LH, Shekitka KM, Helwig EB. Carcinoids of the duodenum. A histologic and immuno-
histochemical study of 65 tumors. Am J Surg Pathol 1989;13:828–37.[59] Soga J, Yakuwa Y. Somatostatinoma/inhibitory syndrome: a statistical evaluation of 173 reported cases as compared to
other pancreatic endocrinomas. J Exp Clin Cancer Res 1999;18:13–22.[60] Green BT, Rockey DC. Duodenal somatostatinoma presenting with complete somatostatinoma syndrome. J Clin Gas-
troenterol 2001;33:415–7.[61] Weichert 3rd RF, Roth LM, Krementz ET, Hewitt RL, Drapanas T. Carcinoid-islet cell tumors of the duodenum. Report of
twenty-one cases. Am J Surg 1971;121:195–205.[62] Lasson A, Alwmark A, Nobin A, Sundler F. Endocrine tumors of the duodenum. Clinical characteristics and hormone
content. Ann Surg 1983;197:393–8.[63] Stamm B, Hedinger CE, Saremaslani P. Duodenal and ampullary carcinoid tumors. A report of 12 cases with pathological
characteristics, polypeptide content and relation to the MEN I syndrome and von Recklinghausen’s disease (neuro-fibromatosis). Virchows Arch A Pathol Anat Histopathol 1986;408:475–89.
[64] Capella C, Riva C, Rindi G, Usellini L, Chiaravalli A, Solcia E. Endocrine tumors of the duodenum and upper jejunum. Astudy of 33 cases with clinico-pathological characteristics and hormone content. Hepatogastroenterology 1990;37:247–52.
[65] Burke AP, Sobin LH, Federspiel BH, Shekitka KM, Helwig EB. Carcinoid tumors of the duodenum. A clinicopathologic studyof 99 cases. Arch Pathol Lab Med 1990;114:700–4.
[66] Soga J. Endocrinocarcinomas (carcinoids and their variants) of the duodenum. An evaluation of 927 cases. J Exp ClinCancer Res 2003;22:349–63.

D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735734
[67] Weber HC, Venzon DJ, Lin JT, Fishbein VA, Orbuch M, Strader DB, et al. Determinants of metastatic rate and survival inpatients with Zollinger-Ellison syndrome: a prospective long-term study. Gastroenterology 1995;108:1637–49.
[68] Norton JA, Alexander HR, Fraker DL, Venzon DJ, Gibril F, Jensen RT. Does the use of routine duodenotomy (DUODX) affectrate of cure, development of liver metastases, or survival in patients with Zollinger-Ellison syndrome? Ann Surg 2004;239:617–25 [discussion 626].
[69] Gibril F, Schumann M, Pace A, Jensen RT. Multiple endocrine neoplasia type 1 and Zollinger-Ellison syndrome: a pro-spective study of 107 cases and comparison with 1009 cases from the literature. Medicine (Baltimore) 2004;83:43–83.
[70] Jensen RT. Management of the Zollinger-Ellison syndrome in patients with multiple endocrine neoplasia type 1. J InternMed 1998;243:477–88.
[71] Amano S, Hazama F, Haebara H, Tsurusawa M, Kaito H. Ectopic ACTH-MSH producing carcinoid tumor with multipleendocrine hyperplasia in a child. Acta Pathol Jpn 1978;28:721–30.
[72] Zyromski NJ, Kendrick ML, Nagorney DM, Grant CS, Donohue JH, Farnell MB, et al. Duodenal carcinoid tumors: howaggressive should we be? J Gastrointest Surg 2001;5:588–93.
[73] Wang HY, Chen MJ, Yang TL, Chang MC, Chan YJ. Carcinoid tumor of the duodenum and accessory papilla associated withpolycythemia vera. World J Gastroenterol 2005;11:3794–6.
[74] Dayal Y, Tallberg KA, Nunnemacher G, DeLellis RA, Wolfe HJ. Duodenal carcinoids in patients with and without neuro-fibromatosis. A comparative study. Am J Surg Pathol 1986;10:348–57.
[75] Hatzaras I, Palesty JA, Abir F, Sullivan P, Kozol RA, Dudrick SJ, et al. Small-bowel tumors: epidemiologic and clinicalcharacteristics of 1260 cases from the connecticut tumor registry. Arch Surg 2007;142:229–35.
[76] Soga J, Tazawa K, Aizawa O, Wada K, Tuto T. Argentaffin cell adenocarcinoma of the stomach: an atypical carcinoid?Cancer 1971;28:999–1003.
[77] Papotti M, Cassoni P, Volante M, Deghenghi R, Muccioli G, Ghigo E. Ghrelin-producing endocrine tumors of the stomachand intestine. J Clin Endocrinol Metab 2001;86:5052–9.
[78] Annibale B, Azzoni C, Corleto VD, di Giulio E, Caruana P, D’Ambra G, et al. Atrophic body gastritis patients withenterochromaffin-like cell dysplasia are at increased risk for the development of type I gastric carcinoid. Eur J Gastro-enterol Hepatol 2001;13:1449–56.
[79] Dinis-Ribeiro M, Areia M, de Vries AC, Marcos-Pinto R, Monteiro-Soares M, O’Connor A, et al. Management of precan-cerous conditions and lesions in the stomach (MAPS): guideline from the European Society of Gastrointestinal Endoscopy(ESGE), European Helicobacter Study Group (EHSG), European Society of Pathology (ESP), and the Sociedade Portuguesade Endoscopia Digestiva (SPED). Endoscopy 2012;44:74–94.
[80] Solcia E, Bordi C, Creutzfeldt W, Dayal Y, Dayan AD, Falkmer S, et al. Histopathological classification of nonantral gastricendocrine growths in man. Digestion 1988;41:185–200.
[81] Cattan D, Roucayrol AM. Fundic endocrinopathy in fundic atrophic gastritis with achlorhydria. II–Carcinoid tumors.Gastroenterol Clin Biol 1991;15:36C–40C.
[82] Bordi C, Yu JY, Baggi MT, Davoli C, Pilato FP, Baruzzi G, et al. Gastric carcinoids and their precursor lesions. A histologic andimmunohistochemical study of 23 cases. Cancer 1991;67:663–72.
[83] Lehy T, Cadiot G, Mignon M, Ruszniewski P, Bonfils S. Influence of multiple endocrine neoplasia type 1 on gastricendocrine cells in patients with the Zollinger-Ellison syndrome. Gut 1992;33:1275–9.
[84] Rindi G, Arnold R, Bosman FT. Nomenclature and classification of neuroendocrine neoplasms of the digestive system. In:Bosman FT, Carneiro F, Hruban RH, Theise ND, et al., editors. WHO classification of tumors of the digestive system. Lyon:IARC; 2010.
[85] Solcia E, Klöppel G, Sobin LH. Histological typing of endocrine tumours. New York: Springer; 2000.[86] Alumets J, Sundler F, Falkmer S, Ljungberg O, Hakanson R, Martensson H, et al. Neurohormonal peptides in endocrine
tumors of the pancreas, stomach, and upper small intestine: I. An immunohistochemical study of 27 cases. UltrastructPathol 1983;5:55–72.
[87] Heymann MF, Hamy A, Triau S, Miraille E, Toquet C, Chomarat H, et al. Endocrine tumors of the duodenum. A study of 55cases relative to clinicopathological features and hormone content. Hepatogastroenterology 2004;51:1367–71.
[88] Barbareschi M, Frigo B, Aldovini D, Leonardi E, Cristina S, Falleni M. Duodenal gangliocytic paraganglioma. Report ofa case and review of the literature. Virchows Arch A Pathol Anat Histopathol 1989;416:81–9.
[89] La Rosa S, Inzani F, Vanoli A, Klersy C, Dainese L, Rindi G, et al. Histologic characterization and improved prognosticevaluation of 209 gastric neuroendocrine neoplasms. Hum Pathol 2012;42:1373–84.
[90] Kumashiro R, Naitoh H, Teshima K, Sakai T, Inutsuka S. Minute gastric carcinoid tumor with regional lymph nodemetastasis. Int Surg 1989;74:198–200.
[91] Xie SD, Wang LB, Song XY, Pan T. Minute gastric carcinoid tumor with regional lymph node metastasis: a case report andreview of literature. World J Gastroenterol 2004;10:2461–3.
[92] Soga J. Early-stage carcinoids of the gastrointestinal tract: an analysis of 1914 reported cases. Cancer 2005;103:1587–95.[93] Bordi C. Gastric carcinoids. Ital J Gastroenterol Hepatol 1999;31(Suppl. 2):S94–97.[94] Gough DB, Thompson GB, Crotty TB, Donohue JH, Kvols LK, Carney JA, et al. Diverse clinical and pathologic features of
gastric carcinoid and the relevance of hypergastrinemia. World J Surg 1994;18:473–9 [discussion 479–480].[95] Dalenback J, Havel G. Local endoscopic removal of duodenal carcinoid tumors. Endoscopy 2004;36:651–5.[96] Ichikawa J, Tanabe S, Koizumi W, Kida Y, Imaizumi H, Kida M, et al. Endoscopic mucosal resection in the management of
gastric carcinoid tumors. Endoscopy 2003;35:203–6.[97] Higham AD, Dimaline R, Varro A, Attwood S, Armstrong G, Dockray GJ, et al. Octreotide suppression test predicts ben-
eficial outcome from antrectomy in a patient with gastric carcinoid tumor. Gastroenterology 1998;114:817–22.[98] Murugesan SV, Steele IA, Dimaline R, Poston GJ, Shrotri M, Campbell F, et al. Correlation between a short-term intra-
venous octreotide suppression test and response to antrectomy in patients with type-1 gastric neuroendocrine tumours.Eur J Gastroenterol Hepatol.
[99] Ruszniewski P, Laucournet H, Elouaer-Blanc L, Mignon M, Bonfils S. Long-acting somatostatin (SMS 201-995) in themanagement of Zollinger-Ellison syndrome: evidence for sustained efficacy. Pancreas 1988;3:145–52.

D. O’Toole et al. / Best Practice & Research Clinical Gastroenterology 26 (2012) 719–735 735
[100] Grozinsky-Glasberg S, Kaltsas G, Gur C, Gal E, Thomas D, Fichman S, et al. Long-acting somatostatin analogues are aneffective treatment for type 1 gastric carcinoid tumours. Eur J Endocrinol 2008;159:475–82.
[101] Manfredi S, Pagenault M, de Lajarte-Thirouard AS, Bretagne JF. Type 1 and 2 gastric carcinoid tumors: long-term follow-up of the efficacy of treatment with a slow-release somatostatin analogue. Eur J Gastroenterol Hepatol 2007;19:1021–5.
[102] Massironi S, Sciola V, Spampatti MP, Peracchi M, Conte D. Gastric carcinoids: between underestimation and overtreat-ment. World J Gastroenterol 2009;15:2177–83.
[103] Jianu CS, Fossmark R, Syversen U, Hauso O, Fykse V, Waldum HL. Five-year follow-up of patients treated for 1 year withoctreotide long-acting release for enterochromaffin-like cell carcinoids. Scand J Gastroenterol 2011;46:456–63.
[104] Martinsen TC, Kawase S, Hakanson R, Torp SH, Fossmark R, Qvigstad G, et al. Spontaneous ECL cell carcinomas in cottonrats: natural course and prevention by a gastrin receptor antagonist. Carcinogenesis 2003;24:1887–96.
[105] Takaishi S, Cui G, Frederick DM, Carlson JE, Houghton J, Varro A, et al. Synergistic inhibitory effects of gastrin and his-tamine receptor antagonists on helicobacter-induced gastric cancer. Gastroenterology 2005;128:1965–83.
[106] Kidd M, Siddique ZL, Drozdov I, Gustafsson BI, Camp RL, Black JW, et al. The CCK(2) receptor antagonist, YF476, inhibitsMastomys ECL cell hyperplasia and gastric carcinoid tumor development. Regul Pept 2010;162:52–60.
[107] Fossmark R, Sordal O, Jianu CS, Qvigstad G, Nordrum IS, Boyce M, et al. Treatment of gastric carcinoids type 1 with thegastrin receptor antagonist netazepide (YF476) results in regression of tumours and normalisation of serum chromog-ranin A. Aliment Pharmacol Ther;36:1067–75.
[108] Norton JA, Doppman JL, Jensen RT. Curative resection in Zollinger-Ellison syndrome. Results of a 10-year prospectivestudy. Ann Surg 1992;215:8–18.
[109] Norton JA, Jensen RT. Resolved and unresolved controversies in the surgical management of patients with Zollinger-Ellison syndrome. Ann Surg 2004;240:757–73.
[110] Mullen JT, Wang H, Yao JC, Lee JH, Perrier ND, Pisters PW, et al. Carcinoid tumors of the duodenum. Surgery 2005;138:971–7 [discussion 977–978].
[111] Makhlouf HR, Burke AP, Sobin LH. Carcinoid tumors of the ampulla of Vater: a comparison with duodenal carcinoidtumors. Cancer 1999;85:1241–9.
[112] O’Toole D, Rindi G, Plockinger U, Wiedenmann B. ENETS consensus guidelines for the management of patients with raremetastases from digestive neuroendocrine tumors: rationale and working framework. Introduction. Neuroendocrinology2010;91:324–5.
[113] Pavel M, Baudin E, Couvelard A, Krenning E, Oberg K, Steinmuller T, et al. ENETS consensus guidelines for the man-agement of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut,and unknown primary. Neuroendocrinology;95:157–76.
[114] Kwekkeboom DJ, Teunissen JJ, Bakker WH, Kooij PP, de Herder WW, Feelders RA, et al. Radiolabeled somatostatin analog[177Lu-DOTA0, Tyr3]octreotate in patients with endocrine gastroenteropancreatic tumors. J Clin Oncol 2005;23:2754–62.
[115] Rindi G, Kloppel G, Alhman H, Caplin M, Couvelard A, de Herder WW, et al. TNM staging of foregut (neuro)endocrinetumors: a consensus proposal including a grading system. Virchows Arch 2006;449:395–401.
[116] Sobin LH, Wittekind C, editors. TNM classification of malignant tumours. New York: Wiley-Liss; 2002.