Embed Size (px)
DESCRIPTION
surgery lectures slides
Citation preview

GASTRIC CANCERDone by Eman,Jumana,Dania


3
The wall of the stomach has five layers:Inner layer or lining (mucosa): Most stomach cancers begin in this layer.
Submucosa: This is the support tissue for the inner layer.
Muscle layer: Muscles in this layer contract to mix and mash the food.
Subserosa: This is the support tissue for the outer layer.
Outer layer (serosa): The outer layer covers the stomach. It holds the stomach in place.

Blood Supply

venous drainage

Lymphatic drainage of the stomach

Antrum to right gastric LN superiorly, and right gastroepiploic and subpyloric LN inferiorly.Pylorus to right gastric suprapyloric nodes superiorly and subpyloric LN around the gastroduodenal artery inferiorly.efferent lymphatics from suprapyloric lymph nodes converge on the para-aortic nodes around the coeliac axis, whereas the efferent lymphatics from the subpyloric lymph nodes pass up to the main superior mesenteric lymph nodes around the origin of the superior mesenteric artery .
Lymphatic vessels related to the cardiac orifice of the stomach communicate freely with those of the oesophagus.

Carcinoma of the stomach is a major cause of cancer mortalityWorldwide Gastric cancer is actually an eminently curable disease provided that it is detected at an appropriate stage and treated adequatelyRarely disseminates widely before it has involved the lymph nodes and, therefore, there is an opportunity to cure the disease prior to disseminationEarly diagnosis is therefore the key to success.The only treatment modality able to cure the disease is resection surgery.

1. Incidence2. There are marked variations in the incidence of gastric
cancer worldwide. 3. In the UK the incidence is approximately 15 cases per 4. 100 000 population per year, 5. in the USA 10 cases per 100 0006. and in Eastern Europe 40 cases per 100 0007. In Japan the disease is much more common, with an
incidence of approximately 70 cases per 8. 100 000 population per year, and there are small
geographical areas in China where the incidence is double that in Japan.
Gastric CA - Epidemiology

10
Gastric cancer is one of the most common cancers worldwide
Gastric cancer is the second most common cause of cancer-related death in the world, and it remains difficult to cure in Western countries , because most patients present with advanced disease
Declined rapidly over the recent few decades
Highest in Eastern Asia, Eastern Europe, and South America, while the lowest rates are in North America and parts of Africa

Etiology Gastric cancer is a multifactorial disease H. pylori Helicobacter seems to be principally
associated with carcinoma of the body and distal stomach rather than the proximal stomach.
As Helicobacter is associated with gastritis, gastric atrophy and intestinal metaplasia, the association with malignancies perhaps not surprising

RISK FACTORS1. Gender : M>F 2. Age 3. Class 4. Environmental factors5. Diet & Smoking6. H.pylori & chronic gastritis7. Adenomatous polyp8. Previous gastric surgery : Billroth 1 & 29. Pernicious anemia10. Menetriers disease11. Familial gastric cancer12. Blood group A13. Hypogammaglobulinemia

Pathology The most useful classification of gastric cancer is the
Lauren classification. In this system there are principally two forms of gastric cancer: intestinal and diffuse.
In Intestinal gastric cancer, the tumour resembles a carcinoma elsewhere in the tubular gastrointestinal tract and forms polypoid tumours or ulcers. It probably arises in areas of intestinal metaplasia.
In contrast, Diffuse gastric cancer infiltrates deeply into the stomach without forming obvious mass lesions, but spreads widely in the gastric wall. Not surprisingly, this has a much worse prognosis.
A small proportion of gastric cancers are of mixed morphology.

14
Macroscopic
Types
Proliferative Ulcerative Infiltrating
Incidence 40% 40% 20%
Site Body & fundus pylorus or lesser curvature
involve stomach diffusely
Gross cauliflower mass
Malignant ulcer infiltrates all layers
Different well moderately poorly

15
Microscopic
Adenocarcinoma Squamous cell carcinoma
Columnar cell adenocarcinoma
Colloid or mucoid adenocarcinoma
Intestinal type
Diffuse type

DIFFUSE GASTRIC CA
INTESTINAL GASTRIC CA

Gastric cancer can be divided into early gastric cancer and advanced gastric cancer. Early gastric cancer is defined as cancer limited to the mucosa and submucosa with or without lymph node involvement (T1, any N).
This can be either protruding, superficial or excavated in the Japanese classification. This type of cancer is eminently curable, and even early gastric cancers associated with lymph node involvement have five-year survival rates in the region of 90 per cent.

Site The proximal stomach is now the most common
site for gastric cancer in the West. Because so many malignancies occur at the oesophagogastric junction, and because the lower oesophagus is also a very common site of adenocarcinoma, it is artificial to separate the stomach from the oesophagus.
This high prevalence of proximal gastric cancer is not seen in Japan, where distal cancer still predominates, as it does in most of the rest of the world.

Spread of Gastric CancerDistant metastases are uncommon in the
absence of lymph node metastases. The intestinal and diffuse types of
gastric cancer spread differently. The diffuse type spreads via the submucosal and subserosal lymphatic plexus and it penetrates the gastric wall at an early stage.

Direct spread penetrates the muscularis, serosa and
ultimately adjacent organsLymphatic spread by both permeation and emboli to the
affected tiers of nodes. This may be extensive, the tumour even appearing in the supraclavicular nodes (Troisier’s sign).

Blood-borne metastases first to the liver , subsequently to other organs eg;
lung and bone. Transperitoneal spread common once the tumour has reached the serosa
indicates incurability. commonly give rise to ascites. tumour ‘shelf’.
Krukenberg’s tumours Sister Joseph’s nodule Detected most effectively by laparoscopy and
cytology

22
Gastric CA - Clinically In the United States, about 25% of stomach cancer
patients present with localized disease, 31% present with regional disease, and 32% present with distant metastatic disease
NOTE : Gastric CA in cardia gives dysphagia. pylorus gives vomiting.

23
Gastric CA – Cont. Early symptoms:
Weight loss Abdominal pain (epigastric, vague and mild early in the
disease but more severe and constant as the disease progresses)
Nausea/Vomiting/Hematemesis Dysphagia (In proximal stomach or at the esophagogastric
junction) Melena Early satiety Postprandial fullness Anorexia Dyspepsia

24
Gastric CA – Cont. Late symptoms: (Due to extension)
Abdominal distention (Ascites) Pleural effusions Obstruction of the gastric outlet,
gastroesophageal junction, or small bowel Bleeding in the stomach from esophageal
varices Jaundice Headache

25
Gastric CA – Cont. Signs: (Indicate late disease)
Weight loss Ascites Hepatomegaly Sister Mary Joseph nodule Virchow nodes Irish node Blumer shelf Anemia Paraneoplastic syndromes such as dermatomyositis,
acanthosis nigricans, microangiopathic hemolytic anemia, membranous nephropathy, and hypercoagulable state

Investigation of Gastric CA CBC … anemia Stool for occult blood LFT … liver mets Electrolyte Tumor markers such as CEA and CA 19-9: Elevated CEA in 45-50% of
cases; elevated CA 19-9 in about 20% of cases
1- for diagnosis : A-Upper GI endoscope… Gold standard for Dx B-barim meal (accuracy 75% ) : lf cauliflower mass will be as irregular filling defect lf malignant ulcer Ulcer niche >2cms (small depression in hollow
organ )
26

27
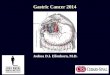
Linitis plastica of the stomach as seen on upper gastrointestinal (UGI) series
Upper gastrointestinal study reveals fixed narrowing of the entire proximal stomach (arrows) due to submucosal invasion by a
gastric cancer.
Normal upper GI series
Normal air-contrast upper gastrointestinal study showing normal
gastric folds and small intestinal anatomy, and no masses.

Endoscopy

UltrasonographyMostly use for
proximal tumor

CT

CT/PET

Laparoscopy

Investigation of Gastric CA 2-For staging : Abdominal U/S Abdominal CT Laproscopy … to detect peritoneal seeding For follow up : Tumor marker : CEA increase in 65%and indicates
extensive spread . lt is of prognostic value rather than diagnostic
CA 19-9 CA72-4 (more recent and more specific)
For preop preparations : CBC ,KFT ,LFT ,Electrolyte
33

TNM Staging International Union Against Cancer (UICC) staging of gastric cancer.
T Stage _Tis, carcinoma in situ
–T1, tumour in mucosa or submucosa –T2, tumour into/through muscularis propria
–T3, tumour through serosa –T4, tumour invading other structures


N Stage (requires at least 15 nodes to be examined)N0 No lymph nodesN1 Metastasis in 1–2 regional nodesN2 Metastasis in 3–6 regional nodesN3a Metastasis in 7–15 regional nodesN3b Metastasis in more than 15 regional nodes
M Stage –M0, no distant metastases
–M1, distant metastases(this includes peritoneum and distant lymph nodes)

STAGINGT1 N0 M0 IA T1 N1 M0T2 N0 M0 IBT1 N2 M0T2 N1 M0T3 N0 M0
IIA
T1 N3 M0T2 N2 M0T3 N1 M0T4a N0 M0
IIB
T2 N3 M0T3 N2 M0T4a N1 M0
IIIA
T3 N3 M0T4a N2 M0T4b N0–1 M0
IIIB
T4a N3 M0T4b N2–3 M0
IIICAny T Any N M IV

General treatment recommendations
**Treatment based on the following: Stage of disease.
Surgical fitness of patient . The patient’s preference.
Patient comorbidities

OperabilityEndoscopic mucosal resection (IA)Total gastrectomySubtotal gastrectomy
(In non curable cases ) Palliative surgery One of the commoner indications for palliative surgery is gastric outlet obstruction from stenosing distal gastric cancer and even in this situation the use of expandable metal mesh stents can offer better palliation in a significant proportion . Other indications is bleeding

Total gastrectomy40

Subtotal gastrectomy41

Complications of gastric surgery1. Early complication : 1-Potential complications include the usual cardiac, respiratory and wound complications that may occur in any patient undergoing abdominal surgery.2-risk of anastomotic leakage.3-Fluid collections or abscesses are common, particularly if extensive lymph node dissection has been performed.4-Afferent loop obstruction is due to a poorly constructed afferent loop and this will lead to post- prandial pain and nausea relived by vomiting.

2 .Late complication:
Late complications are due to changes in the anatomy and the physiology of the upper gastrointestinal tract.The complications include reflux gastritis and/or esophagitis, dumping syndromes, diarrhea and nutritional deficiencies. Most of the problems are most marked in the few months after surgery and most fade within about one year.*** Dumping refers to an array of gastrointestinal and vasomotor symptoms attributed to rapid gastric emptying. The symptoms include fullness, abdominal pain, nausea, vomiting and diarrhea. The vasomotor symptoms are due to rapid fluid shifts into the bowel lumen, and are the typical symptoms of hypovolemia. ‘Late’ dumping is due to an insulin surge soon after a meal, followed by reactive hypoglycemia. The treatment of dumping is dietary. Patients should eat small frequent meals, try to separate dry foods from liquids, and avoid simple sugars. The severity of symptoms settles with time.

Other treatment modalities
Because of the failure of radical surgery to cure advanced gastric cancer, there has been interest in the use of radiotherapy and chemotherapy.
RadiotherapyThe routine use of radiotherapy is controversial as the results of clinical trials are inconclusive. There are a number of radiosensitive tissues in the region of the gastric bed, which limits the dose that can be given. Radiotherapy has a role in the palliative treatment of painful bony metastases.

ChemotherapyGastric cancer may respond well to combination cytotoxic chemotherapy and neoadjuvant chemotherapy improves the outcome following surgery. Therefore, most patients should have chemotherapy before surgery .
Chemotherapy for advanced disease is palliative.

GIST Previously named leiomyoma and leiomyosarcoma They are tumors of mesenchymal origin. observed equally in males and females. The tumors are associated with a mutation in the
tyrosine kinase c-kit oncogene. GIST comprise 1–3 % of all gastrointestinal neoplasia. The biological behavior of these tumors is
unpredictable but size and mitotic index are the best predictors of metastasis.
Peritoneal and liver metastases are most common. LN METS IS RARE

Symptoms:they are noticed incidentally at endoscopyOr it leading to bleeding if the mucosa overlying the tumor ulceratesNon specific symptoms if large in size .Diagnosis:Because the mucosa overlying the tumor is normal, endoscopic biopsy can be uninformative unless the tumor has ulcerated. Targeted biopsy by endoscopic ultrasound is more helpful .

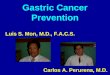
Computed tomography of the upper abdomen showinga 3.5 cm gastrointestinal stromal tumour arising from the gastric wall.

treatmentsurgery is the primary mode of treatment. Smaller tumors can be treated by wedge excision although the incidence of the condition is unclear
Larger tumors may require a gastrectomy or duodenectomy but lymphadenectomy is not required. Larger tumors which require multivisceral resection may be better treated with three to six months of imatinib prior to operation as this will usually radically reduce the size and vascularity of the tumors.
Adjuvant imatinib for large resected tumors of high malignant potential should probably be continued indefinitely.

The prognosis of advanced metastatic GIST has been dramatically improved with imatinib chemotherapy but resection of metastases, especially from the liver, still has an important role.

Gastric lymphoma primary gastric lymphoma V.S generalized
lymphomatous process.
the incidence of gastric lymphoma seems to be increasing.
Primary gastric lymphoma accounts for approximately 5 % of all gastric neoplasms.
most common in the sixth decade the presentation is no different from gastric cancer, the
common symptoms being pain, weight loss and bleeding. Primary gastric lymphomas are B cell derived, the tumor
arising from the mucosa-associated lymphoid tissue (MALT).

At an early stage, the disease takes the form of a diffuse mucosal thickening, which may ulcerate.
Diagnosis is made as a result of the endoscopic biopsy.
Following diagnosis, adequate staging is necessary, primarily to establish whether the lesion is a primary gastric lymphoma or part of a more generalized process. CT scans of the chest and abdomen and bone marrow aspirate are required, as well as a full blood count


the treatment of primary gastric lymphoma is somewhat controversial, it seems most appropriate to use surgery alone for the localized disease process.
No benefit has been shown from adjuvant chemotherapy, although some oncologists contend that primary gastric lymphoma can be treated by chemotherapy alone. Chemotherapy alone is appropriate for patients with systemic disease.
Lymphocytes are not found to any degree in normal gastric mucosa, but are found in association with Helicobacter infection. It has also been shown that early gastric lymphomas may regress and disappear when the Helicobacter infection is treated.

Gastric involvement with the diffuselymphoma
These patients are treated with chemotherapy, sometimes with dramatic and rapid responses. Surgeons are frequently asked to deal with the complications of gastric involvement.
The two common complications are bleeding and perforation. Both may occur at presentation, but more usually may follow the chemotherapy when there is rapid regression and necrosis of the tumor. These operations can be technically very challenging and normally require gastrectomy





![[Ghiduri][Cancer]Gastric Cancer](https://img.pdfslide.net/doc/110x75/55cf9399550346f57b9de771/ghiduricancergastric-cancer.jpg)