Embed Size (px)
Citation preview

GASTRIC CANCERGASTRIC CANCER
►Decreases in gastric cancerDecreases in gastric cancer have been have been attributed in part toattributed in part to refrigeration refrigeration :: increased consumption of fresh fruits and increased consumption of fresh fruits and
vegetables vegetables decreased intake of salt decreased intake of salt decreased contamination of food by decreased contamination of food by
carcinogenic compounds from the decay carcinogenic compounds from the decay of unrefrigerated meat products of unrefrigerated meat products
►Other factorsOther factors:: lower rates of chronic Helicobacter pylori lower rates of chronic Helicobacter pylori
infectioninfection►improved sanitationimproved sanitation►use of antibioticsuse of antibiotics►increased screening in some countries.1 increased screening in some countries.1

►gastric cancer is still the gastric cancer is still the second most second most common cause of cancer-related death common cause of cancer-related death in the worldin the world
► it remains difficult to cure in Western it remains difficult to cure in Western countries, primarily because countries, primarily because most most patients present with advanced disease patients present with advanced disease
►2 studies have demonstrated 2 studies have demonstrated improved improved survival with adjuvant therapysurvival with adjuvant therapy:: a US study using postoperative a US study using postoperative
chemoradiationchemoradiation a European study using preoperative and a European study using preoperative and
postoperative chemotherapy postoperative chemotherapy
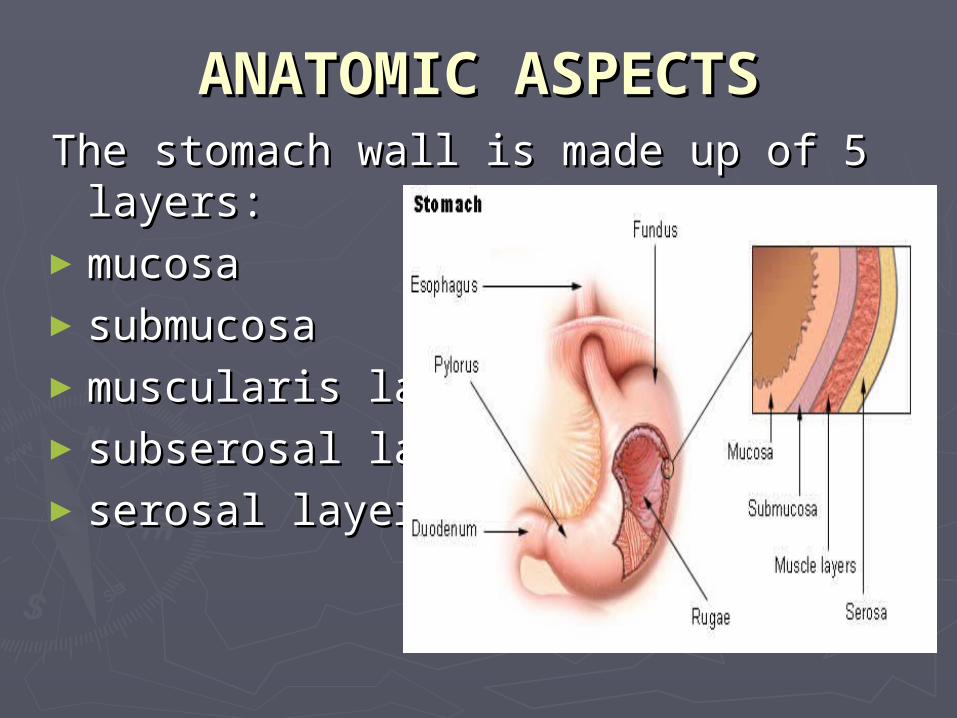
AANATOMIC ASPECTSNATOMIC ASPECTSThe stomach wall is made up of 5 The stomach wall is made up of 5
layerslayers::►mmucosaucosa►ssubmucosaubmucosa►muscularis layermuscularis layer►subserosal layersubserosal layer►serosal layer serosal layer
The site of stomach cancerThe site of stomach cancer is classified is classified on the basis of its relationship to the on the basis of its relationship to the long axis of the stomachlong axis of the stomach
►40% of cancers develop in the 40% of cancers develop in the lower lower partpart
► 40% in the 40% in the middle partmiddle part►15% in the upper part15% in the upper part►10% involve more than one part of the 10% involve more than one part of the
organ organ ►the incidence of adenocarcinoma in the incidence of adenocarcinoma in
the cardia has actually shown a the cardia has actually shown a gradual increase.gradual increase.
FREQUENCYFREQUENCY
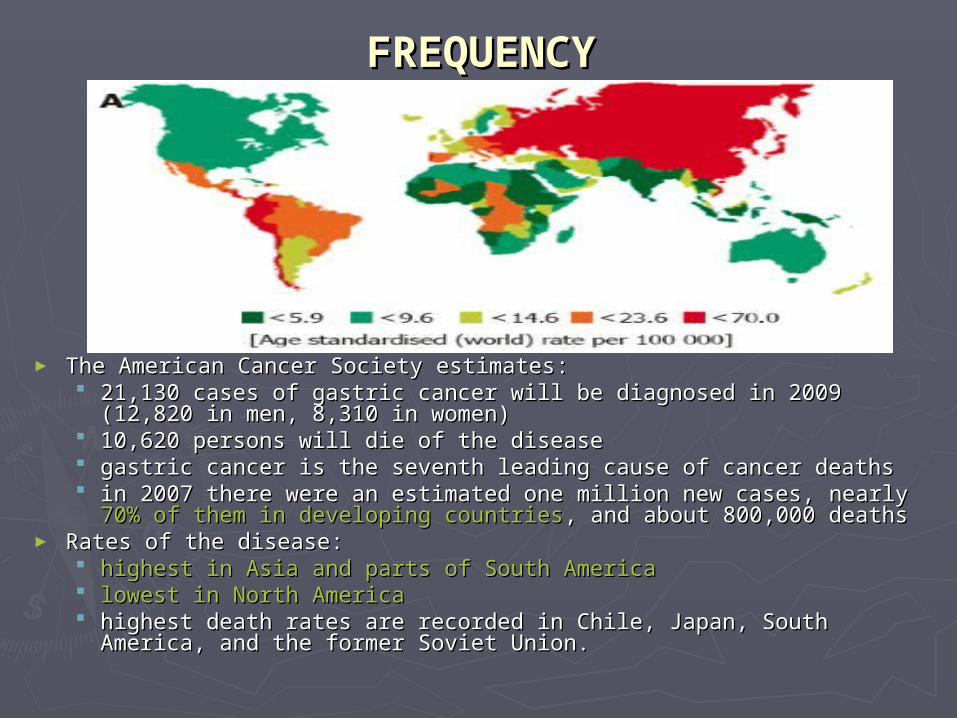
► The American Cancer Society estimatesThe American Cancer Society estimates:: 21,130 cases of gastric cancer will be diagnosed in 2009 (12,820 in 21,130 cases of gastric cancer will be diagnosed in 2009 (12,820 in
men, 8,310 in women) men, 8,310 in women) 10,620 persons will die of the disease10,620 persons will die of the disease ggastric cancer is the seventh leading cause of cancer deathsastric cancer is the seventh leading cause of cancer deaths in 2007 there were an estimated one million new cases,in 2007 there were an estimated one million new cases, nearly nearly 70% 70%
of them in developing countriesof them in developing countries, and about 800,000 deaths , and about 800,000 deaths ► Rates of the diseaseRates of the disease::
highest in Asia and parts of South Americahighest in Asia and parts of South America lowest in North Americalowest in North America highest death rates are recorded in Chile, Japan, South America, highest death rates are recorded in Chile, Japan, South America,
and the former Soviet Union.and the former Soviet Union.

MMORTALITYORTALITY/M/MORBIDITYORBIDITY► tthe he 5-year survival5-year survival rate for curative surgical rate for curative surgical
resection ranges resection ranges from 30-50% for patients with stage II from 30-50% for patients with stage II
disease disease ffrom 10-25% for patients with stage III rom 10-25% for patients with stage III
diseasedisease
► tthe operative mortality rate for patients he operative mortality rate for patients undergoing curative surgical resection at undergoing curative surgical resection at major academic centers is less than 3%major academic centers is less than 3%
RACERACE►tthe rates of gastric cancer are higher he rates of gastric cancer are higher
in in Asian and South American countriesAsian and South American countries than in the United Statesthan in the United States
► Japan, Chile, and Venezuela have Japan, Chile, and Venezuela have developed a very rigorous early developed a very rigorous early screening program that detects screening program that detects patients with early stage diseasepatients with early stage disease
► iin the n the United StatesUnited States, , Asian and Pacific Asian and Pacific IslanderIslander males and females have the males and females have the highest incidence of stomach cancer, highest incidence of stomach cancer, followed by black, Hispanic, white, followed by black, Hispanic, white, American Indian, and Inuit populations.American Indian, and Inuit populations.
SEXSEX► iin the United States, gastric cancer affects n the United States, gastric cancer affects
slightly slightly more men than womenmore men than women► the American Cancer Society estimates that in the American Cancer Society estimates that in
2009, 12,820 new cases will occur in men and 2009, 12,820 new cases will occur in men and 8,310 in women8,310 in women
► gastric cancer rates are about gastric cancer rates are about twice as high in twice as high in men as in womenmen as in women
AGEAGE► tthe median age for gastric cancer in the United he median age for gastric cancer in the United
States is States is 70 years for males70 years for males and and 74 years for 74 years for femalesfemales
► tthe gastric cancers that occur he gastric cancers that occur in younger patientsin younger patients may represent a may represent a more aggressivemore aggressive variant or may variant or may suggest a suggest a genetic predispositiongenetic predisposition to development to development of the disease.of the disease.

CAUSESCAUSESGastric cancer may often be Gastric cancer may often be multifactorialmultifactorial::► inherited predispositioninherited predisposition► environmental factorsenvironmental factors
ddietiet smokingsmoking Helicobacter pylori infectionHelicobacter pylori infection previous gastric surgeryprevious gastric surgery pernicious anemiapernicious anemia adenomatous polypsadenomatous polyps cchronic atrophic gastritishronic atrophic gastritis ggastric ulcersastric ulcers radiation exposure radiation exposure obesityobesity bbisphosphonates isphosphonates

CLINICALCLINICALHISTORYHISTORY► eearly disease has no associated symptomsarly disease has no associated symptoms► some patients with incidental complaints are some patients with incidental complaints are
diagnosed with early gastric cancerdiagnosed with early gastric cancer► mmost symptoms of gastric cancer reflect advanced ost symptoms of gastric cancer reflect advanced
disease disease ► ppatients may complain of atients may complain of
indigestion indigestion nnauseaausea vvomitingomiting ddysphagiaysphagia postprandial fullnesspostprandial fullness loss of appetiteloss of appetite mmelenaelena hhematemesisematemesis weight lossweight loss
► complications complications pathologic peritoneal and pleural pathologic peritoneal and pleural effusions effusions

PHISYCALPHISYCAL► a palpable enlarged stomacha palpable enlarged stomach with succussion splash with succussion splash► hepatomegalyhepatomegaly► periumbilical metastasis (Sister Mary Joseph nodule)periumbilical metastasis (Sister Mary Joseph nodule)► enlarged lymph nodes such as enlarged lymph nodes such as Virchow nodesVirchow nodes (ie, left (ie, left
supraclavicular) and Irish node (anterior axillary)supraclavicular) and Irish node (anterior axillary)► blumer shelf (ie, shelflike tumor of the anterior rectal blumer shelf (ie, shelflike tumor of the anterior rectal
wall) wall) ► weight lossweight loss► melena melena ► pallor from anemiapallor from anemia► Paraneoplastic syndromesParaneoplastic syndromes are poor prognostic features are poor prognostic features
dermatomyositisdermatomyositis acanthosis nigricansacanthosis nigricans circinate erythemas are poor prognostic features.circinate erythemas are poor prognostic features.
► Other associated abnormalitiesOther associated abnormalities also include peripheral also include peripheral thrombophlebitis and microangiopathic hemolytic thrombophlebitis and microangiopathic hemolytic anemiaanemia
DIFFERENTIAL DIAGNOSESDIFFERENTIAL DIAGNOSES
► Esophageal CanceEsophageal Cancerr► Esophageal Esophageal
StrictureStricture► EsophagitisEsophagitis►Gastric UlcersGastric Ulcers►Gastritis, AcuteGastritis, Acute►Gastritis, AtrophicGastritis, Atrophic►Gastritis, ChronicGastritis, Chronic
►Gastroenteritis, Gastroenteritis, BacterialBacterial
►Gastroenteritis, Gastroenteritis, ViralViral
► Lymphoma, Non-Lymphoma, Non-HodgkinHodgkin
►Malignant Malignant Neoplasms of the Neoplasms of the Small IntestineSmall Intestine
LABORATORY STUDIESLABORATORY STUDIES
► The goal of obtaining laboratory studies is to assist The goal of obtaining laboratory studies is to assist in determining optimal therapyin determining optimal therapy
► A complete A complete blood cell countblood cell count can identify can identify anemiaanemia, , which may be caused by which may be caused by bleeding, liver bleeding, liver dysfunction, or poor nutritiondysfunction, or poor nutrition. Approximately 30% . Approximately 30% of patients have anemia.of patients have anemia.
► Electrolyte panelsElectrolyte panels and and liver functionliver function tests also are tests also are essential to better characterize the patient's clinical essential to better characterize the patient's clinical state.state.
► Carcinoembryonic antigen (CEA)Carcinoembryonic antigen (CEA) is increased in 45- is increased in 45-50% of cases.50% of cases.
► Cancer antigen (CA) 19-9Cancer antigen (CA) 19-9 is elevated in about 20% is elevated in about 20% of cases.of cases.

IMAGING STUDIESIMAGING STUDIES► Esophagogastroduodenoscopy Esophagogastroduodenoscopy has a has a
diagnostic accuracy of 95%diagnostic accuracy of 95%

►Double-contrast upper gastrointestinal Double-contrast upper gastrointestinal series series
Barium Contrast Radiography: large crater which erodes into a mass( filling-defect) on the lesser curve, below the gastric angle.
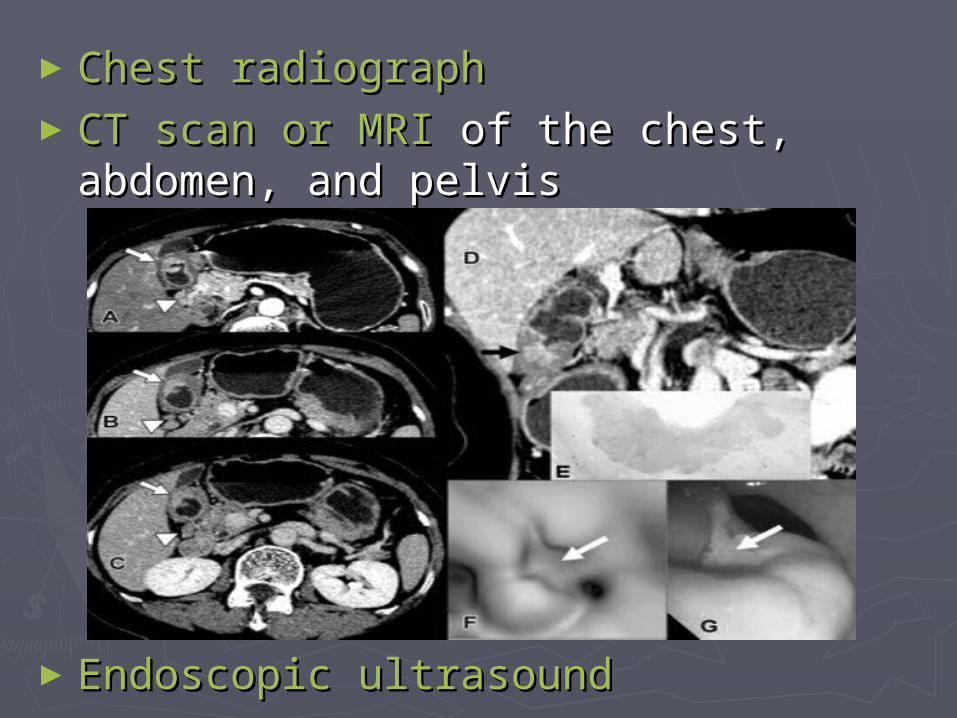
►Chest radiographChest radiograph ►CT scan or MRICT scan or MRI of the chest, abdomen, of the chest, abdomen,
and pelvis and pelvis
►Endoscopic ultrasound Endoscopic ultrasound

HISTOLOGIC FINDINGSHISTOLOGIC FINDINGS►aadenocarcinomadenocarcinoma of the stomach of the stomach
constitutes 90-95% of all gastric constitutes 90-95% of all gastric malignanciesmalignancies
► lymphomaslymphomas►ggastrointestinal stromal tumors astrointestinal stromal tumors ((2% of 2% of
gastric neoplasmsgastric neoplasms)) leiomyomas leiomyomas leiomyosarcomas leiomyosarcomas
►ccarcinoids (1%)arcinoids (1%)►adenoacanthomas (1%)adenoacanthomas (1%)►squamous cell carcinomas (1%)squamous cell carcinomas (1%) Histology of Histology of
gastric gastric cancer with signet ring cellscancer with signet ring cells

STAGINGSTAGING► Stage 0 - Tis, N0, M0Stage 0 - Tis, N0, M0► Stage IA - T1, N0 or N1, M0Stage IA - T1, N0 or N1, M0► Stage IB - T1, N2, M0 or Stage IB - T1, N2, M0 or
T2a/b, N0, M0T2a/b, N0, M0► Stage II - T1, N2, M0 or Stage II - T1, N2, M0 or
T2a/b, N1, M0 or T2, N0, M0 T2a/b, N1, M0 or T2, N0, M0 ► Stage IIIA - T2a/b, N2, M0 or Stage IIIA - T2a/b, N2, M0 or
T3, N1, M0 or T4, N0, M0T3, N1, M0 or T4, N0, M0► Stage IIIB - T3, N2, M0Stage IIIB - T3, N2, M0► Stage IV - T1-3, N3, M0 or Stage IV - T1-3, N3, M0 or
T4, N1-3, M0, or any T, any T4, N1-3, M0, or any T, any N, M1N, M1
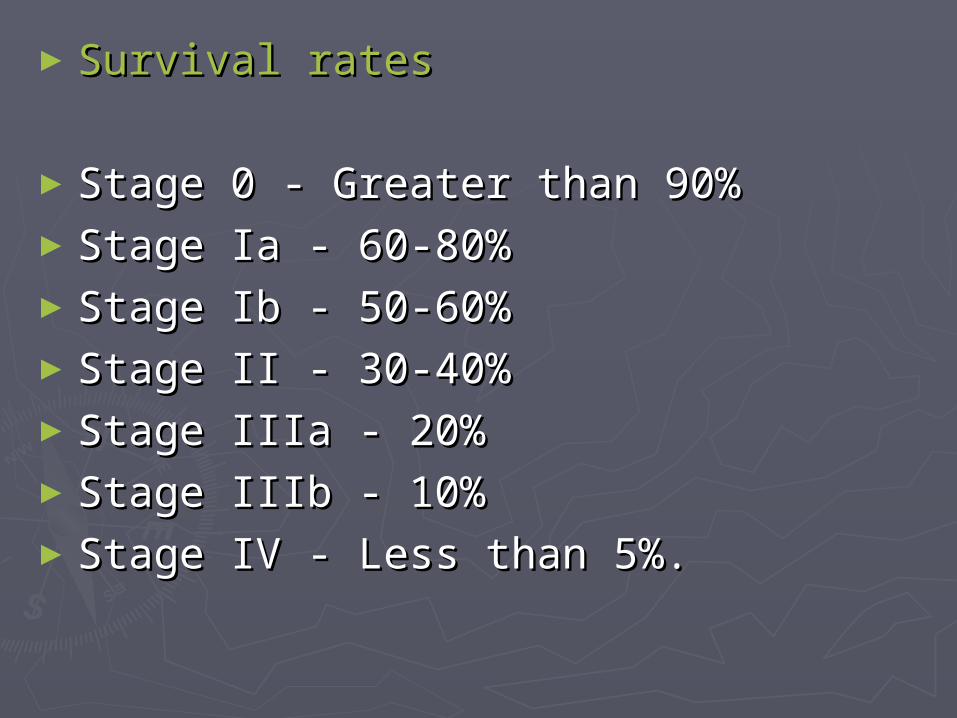
►Survival ratesSurvival rates
►Stage 0 - Greater than 90%Stage 0 - Greater than 90%►Stage Ia - 60-80%Stage Ia - 60-80%►Stage Ib - 50-60%Stage Ib - 50-60%►Stage II - 30-40%Stage II - 30-40%►Stage IIIa - 20%Stage IIIa - 20%►Stage IIIb - 10%Stage IIIb - 10%►Stage IV - Less than 5%.Stage IV - Less than 5%.
►Spread patternsSpread patterns Cancer of the stomach can Cancer of the stomach can spread directly, via lymphatics, or spread directly, via lymphatics, or
hematogenously.hematogenously. Direct extensionDirect extension into the into the omenta, pancreas, diaphragm, omenta, pancreas, diaphragm,
transverse colon or mesocolon, and duodenumtransverse colon or mesocolon, and duodenum is common. is common. If the lesion extends beyond the gastric wall to a If the lesion extends beyond the gastric wall to a free free
peritonealperitoneal (ie, serosal) surface, then peritoneal involvement is (ie, serosal) surface, then peritoneal involvement is frequent.frequent.
The visible gross lesion frequently underestimates the true The visible gross lesion frequently underestimates the true extent of the disease.extent of the disease.
The abundant The abundant lymphatic channelslymphatic channels within the submucosal and within the submucosal and subserosal layers of the gastric wall allow for easy microscopic subserosal layers of the gastric wall allow for easy microscopic spread.spread.
The submucosal plexus is prominent in the esophagus and the The submucosal plexus is prominent in the esophagus and the subserosal plexus is prominent in the duodenum, allowing subserosal plexus is prominent in the duodenum, allowing proximal and distal spread.proximal and distal spread.
Lymphatic drainage is through numerous pathways and can Lymphatic drainage is through numerous pathways and can involve involve multiple nodal groups (eg, gastric, gastroepiploic, multiple nodal groups (eg, gastric, gastroepiploic, celiac, porta hepatic, splenic, suprapancreatic, celiac, porta hepatic, splenic, suprapancreatic, pancreaticoduodenal, paraesophageal, and paraaortic lymph pancreaticoduodenal, paraesophageal, and paraaortic lymph nodes)nodes)
Hematogenous spreadHematogenous spread commonly results in commonly results in liver metastasesliver metastases..
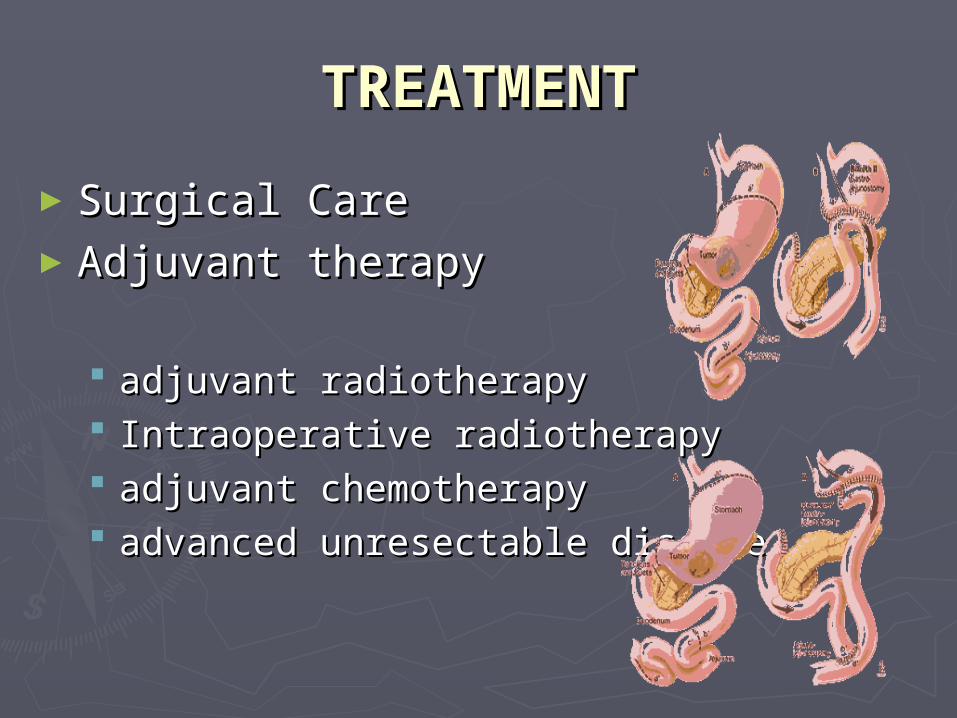
TREATMENTTREATMENT
►Surgical CareSurgical Care►Adjuvant therapy Adjuvant therapy
adjuvant radiotherapy adjuvant radiotherapy Intraoperative radiotherapy Intraoperative radiotherapy adjuvant chemotherapy adjuvant chemotherapy advanced unresectable disease advanced unresectable disease
COMPLICATIONSCOMPLICATIONS► ddirect mortality rate within 30 days after a surgical irect mortality rate within 30 days after a surgical
procedure for gastric cancer has been reduced procedure for gastric cancer has been reduced substantially over the last 40 years substantially over the last 40 years
► mmost major centers report a direct ost major centers report a direct mortality rate of 1-mortality rate of 1-2%2%
► eearly postoperative complicationsarly postoperative complications include include anastomotic failure, bleeding, ileus, transit anastomotic failure, bleeding, ileus, transit failure at the anastomosis, cholecystitis (often failure at the anastomosis, cholecystitis (often occult sepsis without localizing signs), occult sepsis without localizing signs), pancreatitis, pulmonary infections, and pancreatitis, pulmonary infections, and thromboembolism thromboembolism
► ffurther surgery may be required for anastomotic leaksurther surgery may be required for anastomotic leaks► llate mechanicophysiologic complicationsate mechanicophysiologic complications include include
dumping syndrome, vitamin B-12 deficiency, reflux dumping syndrome, vitamin B-12 deficiency, reflux esophagitis, and bone disorders, especially esophagitis, and bone disorders, especially osteoporosisosteoporosis
► postgastrectomy patients often are postgastrectomy patients often are immunologically immunologically deficientdeficient, as measured by blastogenic and delayed , as measured by blastogenic and delayed cutaneous hypersensitivity responses.cutaneous hypersensitivity responses.





![[Ghiduri][Cancer]Gastric Cancer](https://img.pdfslide.net/doc/110x75/55cf9399550346f57b9de771/ghiduricancergastric-cancer.jpg)