Embed Size (px)
Citation preview
Autopsy and Case Reports. ISSN 2236-1960. Copyright © 2018. This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium provided the article is properly cited.
a Metropolitan University of Santos (UNIMES), Hospital Guilherme Álvaro, Department of Pathology. Santos, SP, Brazil.
Gastric lethal hemorrhage due to Dieulafoy’s disease
Cesar Cilento Poncea
How to cite: Ponce CC. Gastric lethal hemorrhage due to Dieulafoy’s disease. Autops Case Rep [Internet]. 2018;8(1):e2018006. http://dx.doi.org/10.4322/acr.2018.006
Article / Autopsy Case Report
ABSTRACT
Gastric Dieulafoy’s lesion (DL) is a potentially fatal entity that causes upper digestive hemorrhage as a consequence of the erosion of an abnormal large-caliber artery in the submucosa of the gastrointestinal tract. We report the case of a 59-year-old female patient admitted to the emergency facility due to melena without any active sign of bleeding during the esophagogastroduodenoscopy. Unexpectedly, she progressed presenting a massive hematemesis followed by an irreversible cardiorespiratory arrest. The aim of this study is to draw attention to DL as a possible cause of massive and fatal digestive hemorrhage, and to describe the anatomical autopsy findings.
Keywords Stomach Diseases; Gastrointestinal Hemorrhage; Autopsy
INTRODUCTION
In 1898, Georges-Paul Dieulafoy first described the potentially life-threatening entity characterized by the abnormal presence of large-caliber arteries in the gastric submucosa, which may result in digestive hemorrhage due to the thinning and eroding of the overlying mucosa.1 Dieulafoy’s lesion (DL) occurs mainly in the stomach and, although it is difficult to determine the true incidence level, it is reported to be responsible for 1-2% of all the causes of upper gastrointestinal bleeding. Approximately one-third of lesions may manifest in other sites of the digestive tract.2
Currently, this anomalous vessel, which is also known as caliber persistent artery, is considered a vascular malformation.3 The most common morphological pattern of gastric DL is a single large arterial vessel usually in the fundus or body that penetrates the wall from the serosa, presenting as dilated at the higher portions of the submucosa.4
The main clinical features of DL result from the massive gastric hemorrhage presenting as hematemesis, melena, tachycardia, hypotension, and acute anemia, which may progress to hypovolemic shock, and eventually death.2
In adults, the most common causes of upper digestive tract bleeding are the rupture of esophageal varices secondary to portal hypertension, gastric or duodenal peptic ulcers, and gastric neoplasm. All these entities are routinely diagnosed by endoscopy.3 Endoscopy is also the most efficient method for the diagnosis of gastric DL during an active bleeding, which accounts for about 70% of the diagnoses. However, this diagnosis is not always an easy task. About 6% of the patients require three or more endoscopies to display the lesion site. In these cases, angiography or angiotomography are useful methods to confirm the diagnosis.2,5

Gastric lethal hemorrhage due to Dieulafoy’s disease
2-4 Autops Case Rep (São Paulo). 2018;8(1):e2018006
The aim of this study is to describe the pathological findings in an autopsy case of DL, rarely reported in the literature.
CASE REPORT
A 59-year-old previously healthy female patient was admitted to the emergency with melena, without any previous episodes of abdominal pain or nausea. She denied alcohol abuse, tobacco smoking, or the use of aspirin and non-steroidal anti-inflammatory drugs. At the clinical examination, she presented tachycardia and hypotension with hypothesis of upper gastrointestinal hemorrhage. The esophagogastroduodenoscopy showed moderate gastritis in the body and antrum, focal surface erosion in the body’s mucosa, but no active signs of bleeding.
The patient was hospitalized for a diagnostic work-up. Unexpectedly, the patient presented a massive hematemesis, hypovolemic shock, and irreversible cardiorespiratory arrest. Permission for autopsy was granted by her parents.
AUTOPSY FINDINGS
At the thoracic and abdominal cavities overture, a diffuse pallor of the organs was evidenced. The Letulle technique was used, where the thoracoabdominal viscera are removed en bloc, with subsequent evaluation by the pathologist.6
Numerous blood clots were found in the lumen of the stomach, small intestine, and proximal colon. The gastric body mucosa of the lesser curvature had a small erosion measuring 3 mm (Figure 1).
The dissection of the esophagus and the stomach revealed the presence of a sizable arterial branch penetrating the stomach wall in the lesser curvature of the gastric body. The anomalous arterial vessel was a branch of the left gastric artery that derived from the celiac trunk. Under the gastric serosa, the vessel was dilated and tortuous (Figure 2).
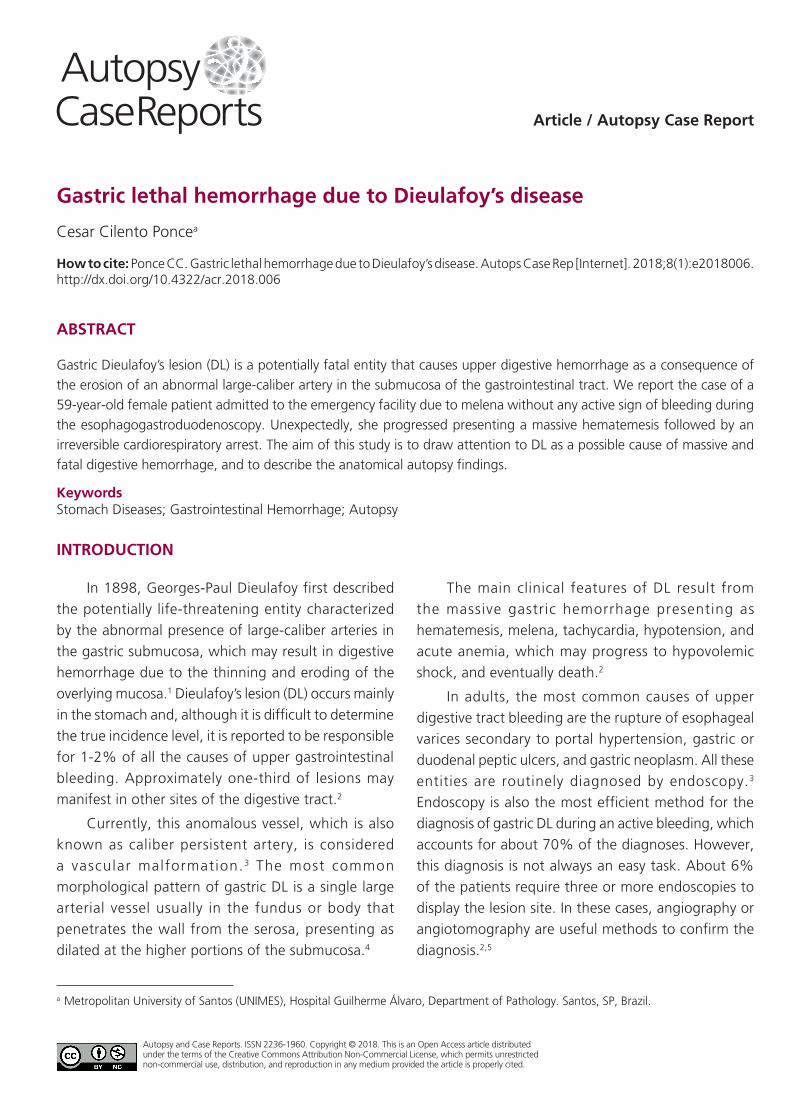
The wall sections in this region demonstrated the presence of an enlarged blood vessel that was macroscopically visible (Figure 3).
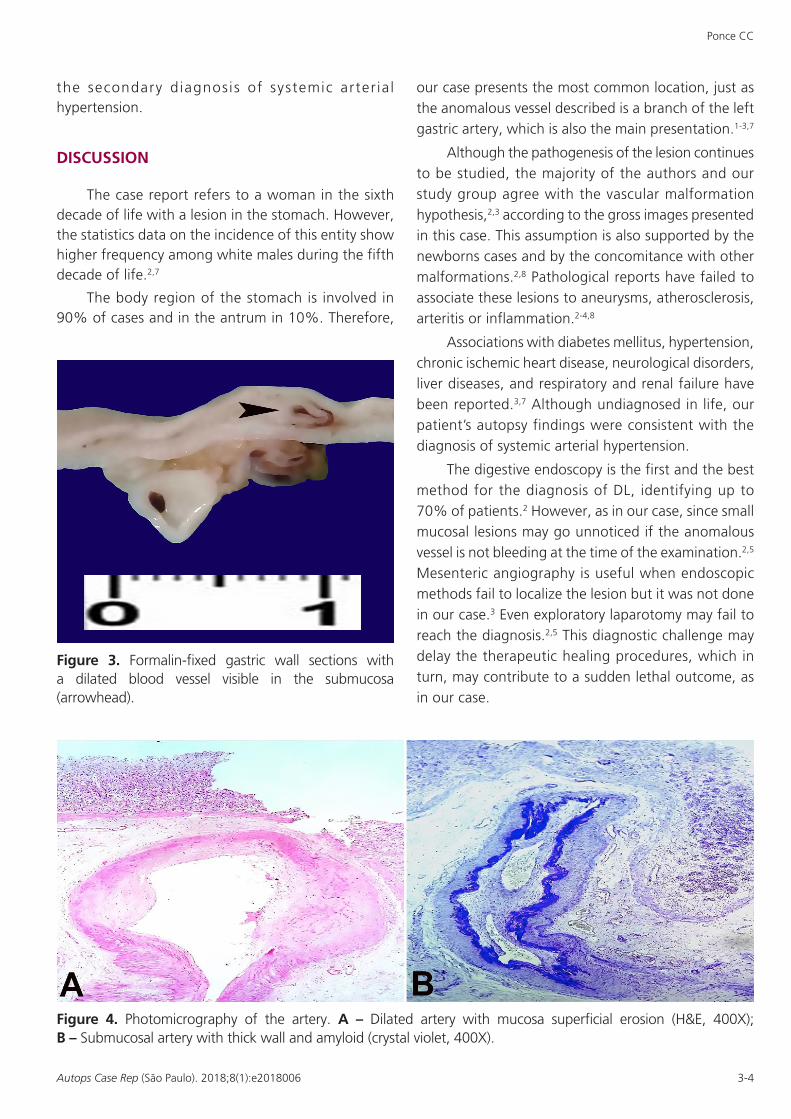
Histological sections stained with hematoxylin and eosin (H&E) revealed a dilated artery with a thick wall in the submucosa (Figure 4A). The Crystal violet stain
was positive for the detection of amyloid on the vessel
wall.3 The mucosa had mild chronic inflammation and
an erosion area (Figure 4B).
The remaining organs presented hypertrophic
cardiomyopathy and bilateral benign nephrosclerosis,
the heart weighed 490 grams (mean reference value
[mRV]; 280g) and the kidneys 130 grams/each on
average (mRV for both 240-350g), which corroborated
Figure 1. Gross view of the formalin-fixed gastric mucosa showing erosion measuring 3 mm in the gastric mucosa (arrowhead).
Figure 2. Large-Caliber and tortuous artery in the formalin-fixed serosa of the stomach.
Ponce CC
3-4Autops Case Rep (São Paulo). 2018;8(1):e2018006
the secondary diagnosis of systemic arter ia l hypertension.
DISCUSSION
The case report refers to a woman in the sixth decade of life with a lesion in the stomach. However, the statistics data on the incidence of this entity show higher frequency among white males during the fifth decade of life.2,7
The body region of the stomach is involved in 90% of cases and in the antrum in 10%. Therefore,
our case presents the most common location, just as the anomalous vessel described is a branch of the left gastric artery, which is also the main presentation.1-3,7
Although the pathogenesis of the lesion continues to be studied, the majority of the authors and our study group agree with the vascular malformation hypothesis,2,3 according to the gross images presented in this case. This assumption is also supported by the newborns cases and by the concomitance with other malformations.2,8 Pathological reports have failed to associate these lesions to aneurysms, atherosclerosis, arteritis or inflammation.2-4,8
Associations with diabetes mellitus, hypertension, chronic ischemic heart disease, neurological disorders, liver diseases, and respiratory and renal failure have been reported.3,7 Although undiagnosed in life, our patient’s autopsy findings were consistent with the diagnosis of systemic arterial hypertension.
The digestive endoscopy is the first and the best method for the diagnosis of DL, identifying up to 70% of patients.2 However, as in our case, since small mucosal lesions may go unnoticed if the anomalous vessel is not bleeding at the time of the examination.2,5 Mesenteric angiography is useful when endoscopic methods fail to localize the lesion but it was not done in our case.3 Even exploratory laparotomy may fail to reach the diagnosis.2,5 This diagnostic challenge may delay the therapeutic healing procedures, which in turn, may contribute to a sudden lethal outcome, as in our case.
Figure 3. Formalin-fixed gastric wall sections with a dilated blood vessel visible in the submucosa (arrowhead).
Figure 4. Photomicrography of the artery. A – Dilated artery with mucosa superficial erosion (H&E, 400X); B – Submucosal artery with thick wall and amyloid (crystal violet, 400X).

Gastric lethal hemorrhage due to Dieulafoy’s disease
4-4 Autops Case Rep (São Paulo). 2018;8(1):e2018006
Based on the literature and morphological aspects of this case, some procedures were fundamental for establishing the final diagnosis. The option for the Letulle autopsy technique was favorable,6 because it allowed the opening of the esophagus and the stomach through the great curvature, and the duodenum, with extensive exposure of the mucosa. This enabled a thorough examination and search for the cause of the bleeding. It was necessary to carefully wash the gastric mucosa to remove the adhered clots, which were hindering the detailed view. After this procedure, a small eroded area in the mucosa of the gastric body was evident, and was accompanied by an anomalous vessel – the origin of which was rendered after the dissection of the main arterial branches of the stomach. The anatomical knowledge of gastric irrigation was the cornerstone for the final diagnosis of gastric Dieulafoy’s disease. Considering the rarity of this lesion, fewer than 140 papers published and the few autopsy cases reports, we focused on the morphological aspects.3,9,10
The lack of awareness of the existence of DL in this case may have delayed the diagnosis, which resulted an unfavorable clinical course. The inclusion of Dieulafoy’s disease in the differential causes of obscure bleeding in all age groups, and in any location of the gastrointestinal tract, is the first step in establishing this often-difficult diagnosis and in avoiding its complications.
REFERENCES
1. Karamanou M, Fiska A, Demetriou T, Androutsos G. Dieulafoy (1839-1911) and the first description
of “exulceratio simplex.”. Ann Gastroenterol. 2011;24(3):188-91. PMid:24713721.
2. Baxter M, Aly EH. Dieulafoy’slesion: currenttrends in diagnosis and management. Ann R Coll Surg Engl. 2010;92(7):548-54. PMid:20883603. http://dx.doi.org/10.1308/003588410X12699663905311.
3. Gurzu S, Copotoiu C, Molnar C, Azamfirei L, Jung I. Lethalgastrichemorrhagefrom a caliber-persistent artery of the antrum: a branch of the rightgastricartery. Hippokratia. 2014;18(2):172-6. PMid:25336884.
4. Chaer R, Helton WS. Dieulafoy’s disease. J Am Coll Surg. 2003;196(2):290-6. PMid:12595057. http://dx.doi.org/10.1016/S1072-7515(02)01801-X.
5. Schmulewitz N, Baillie J. Dieulafoy lesions: a review of 6 years of experience at a tertiary referral center. Am J Gastroenterol. 2001;96(6):1688-94. PMid:11419815. http://dx.doi.org/10.1111/j.1572-0241.2001.03922.x.
6. Culora G, Roche W. Simple method for necropsy dissection of the abdominal organs after abdominal surgery. J Clin Pathol. 1996;49(9):776-9. PMid:9038770. http://dx.doi.org/10.1136/jcp.49.9.776.
7. Senger JL, Kanthan R. The evolution of Dieulafoy’s lesion since 1897: then and now- ajourney through the lens of a pediatric lesion with literature review. Gastroenterol Res Pract. 2012;2012:1. PMid:22474434. http://dx.doi.org/10.1155/2012/432517.
8. Polonkai E, Nagy A, Csízy I, et al. Pyloric atresia associated with Dieulafoy lesion and gastric dysmotility in a neonate. J Pediatr Surg. 2011;46(10):e19-23. PMid:22008357. http://dx.doi.org/10.1016/j.jpedsurg.2011.06.015.
9. Christoffersen RK, Nielsen TS, Vesterby A. Dieulafoy lesion of the esophagus causing massive upper gastrointestinal bleeding and death: a case report. Am J Forensic Med Pathol. 2012;33(2):186-7. PMid:21659839. http://dx.doi.org/10.1097/PAF.0b013e318221be16.
10. Saur K. The solitary exulceratio simplex (Dieulafoy) causing a severe acute gastric bleeding. Chirurg. 1973;44(7):293-9. PMid:4542250.
Conflict of interest: None
Financial support: None
Submitted on: November 20th, 2017 Accepted on: December 22nd, 2017
Correspondence Cesar Cilento Ponce Hospital Guilherme Álvaro - Department of Pathology - Metropolitan University of Santos (UNIMES) Av. Vicente de Carvalho, 65, 72 – Santos/SP – Brazil CEP: 11045-501 Phone: +55 (13) 3202-1375 [email protected]










![Gastrointestinal bleeding from Dieulafoy’s lesion ... · hematemesis and melena[9]. For example, in a review of 177 cases, 51% presented with hematemesis and melena, 28% of patients](https://img.pdfslide.net/doc/110x75/60621e43b491de54ad247179/gastrointestinal-bleeding-from-dieulafoyas-lesion-hematemesis-and-melena9.jpg)










