Embed Size (px)
Citation preview

Gastric surgery and NOTES
Péter LUKOVICH M.D.
Semmelweis University, Faculty of Medicine, 1st Department of Surgery

Blood supply of the stomach
and the duodenum
Celiac trunk - a. gastrica sin.
- a hepatica comm. - a. gastroepiploica d.
- a. hepatica comm. - a. gastrica d.
- a. lienalis - a. gastroepiploica sin.
- a lienalis - a. gastricae breves

Anamnesis (familiar: ulcer,cancer)
Complains (vomitus, haematemesis, anaemia (iron deficiency) disgust of meat)
Physical examination (palpable mass, Wirchow lymph node)
Contrast X-ray
Endoscopy
Endoscopic Ultrasound (EUS)
CT
Virtual endoscopy
Capsule endoscopy
Helicobacter pylori test
Scintigraphy
Lab test: Gastrin level (Zollinger-Ellison syndrome) >50-100 pg/ml
Laparoscopy, laparotomy
Examination of the stomach

Congenital dieseases of the stomach
and the duodenum
Duodenum atresia Rare, double bubble sign : X-ray
Congenital pylorus stenosis
Pancreas annulare Frequency 1:6-7000
Meckel diverticulum
Congenital hypertrophic pylorus stenosis
- Frequency: 500-700/1 birth
- First-born male infants (male/female ratio: 4-5/1)
- One of the more common causes of gastric outlet
obstruction in the neonatal period
- Manifest by projectile nonbilious vomiting between the 4th and 6th weeks
- The antiperistaltic movement of the stomach can be visualised and the hypertrophied
pylorus is palpable
Operation: Weber-Ramstedt pyloro-myotomy
Pancreas anulare
1818 Tiedemann discribed at the first time
1862 Ecker gave the name: pancreas anulare
Drey classified: (neonatal, child age,
asymptomatic and symptomatic in the adult age
Rare disease: 20 000/3
(boncolt esetek)
Male/female ratio : 1/1

In 75% with other congenital diseaeses
Down syndrom
Tracheo-oesophageal fistula
Oesophageal atresia
Anus imperforatus
Hirchsprung disease
Duodenal atresia
Meckel diverticulum
Pancreas anulare

Ulcer of the stomach and the duodenum
Etiology
1., Familiar
2., Hyperacidity (Schwartz 1910 - "Ohne saure kein Ulcus”)
Peptic ulcer is not peptic, Zollinger-Ellison syndrome
3., Decreased level of the protective factors
(pepsin and bicarbonat, prostaglandin level)
4., Blood group - "O" blood group
5., Non steroid antiinflammatory drugs (aspirin)
6., Steroid therapy
7., Helicobacter pylori infection
8., Stress
9., Damage of the blood supply of the duodenum
10., Others Curling ulcer - after burning
Cushing ulcer - after trauma of the brain

Complication of the ulcer
of the stomach and the duodenum
Perforation
Pylorus stenosis
Bleeding

Perforation of the ulcer
Complains: Usually the ulcer on the anterior wall could perforate
Epigastrial pain like thrust of the knife -
later pain in the right lower quadrant (Moynihan tunnel)
Differential diagnosis: Appendicitis!!!
Examinations:
Physical examination: free air in the abdominal cavity,
loss of the blunt of the liver (Chilaiditi syndrome!)
defanse musculaire - peritonitis
no movement of the the bowels
Nativ abdominal X-ray:
air in the abdominal cavity (under the diaphragma)
Operation: suture of the perforation (+covering with omentum)
Neumann
resection of the stomach
Minimal invasiv technic: laparo-gastroscopy

P. Lukovich
Heinecke-Mikulicz
Finney
Jaboulay
Pyloromyotomy (Aust)
Pyloroplasty

Forrest classification of the ulcer
I. active bleeding Ia: spuring bleeding
Ib: oozing bleeding
II. signs of the previous bleeding
IIa: black surface
IIb: visible stump of vessel
IIc: coagulum
III. without any sign of bleeding
Bleeding of the ulcer

Surgery: vagotomy
1. Truncal vagotomy
2. Selectiv vagotomy
3. Superselectiv vagotomy
Now it is a history!

Surgery: resection of the stomach
Billroth-I resection Billroth-II resection

Surgery: resection of the stomach (Billroth-I)

of the stomach
and
the small bowel
Surgery: resection of the stomach (Billroth II)
Gastric cancer:
Incidence of the gastric cancer
decreased in USA
increase in Japan, Chile, Iceland
Peak of incidence in the 5th decade in the life
Male/female ratio: 2/1

Gastric cancer: epidemiology
Feeding: salt, qualitiy of the drinking water
Smoking
Precancerous diseases:
Polyps: hyperplastic adenomatous polyps
suggested:endoscopic polypectomy or surgical resection
Ulcus chronicum
Atrophic gastritis: Type A (anaemia perniciosa)
antibody against the parietal cells
localized into the fundus
Type B (local irratation of the foods)
localized into the fundus and the antrum
Dysplasia
Menetrier gastritis: suggested: preventiv gastrectomy
After Billroth II resection: bile reflux - after 15-20 yrs of the op

Gastric cancer: clinical presentation
Abdominal pain 66%
Weight loss more than 10% 50%
Nausea, vomiting 32%
GI bleeding 23%
Dysphagia 23%
Mass 36%
Tenderness 20%
Anaemia 42%
Hypoproteinaemia 26%

Gastric cancer: lymphnode metasteses
Kompartment I Kompartment II Kompartment III

Gastric cancer: pathology
Macroscopical appareance:
Bormann calssification
Histological classification:
adenocarcinoma
mucinous adenocarcinoma
round cell carcinoma
planocellular carcinoma
Localisation: antrum: 55%
corpus 35%
cardia 5%
linitis plastica 5%
Gastric cancer: TNM classification
T (primer tumor)T1 infiltration of the lamina propria
T2 infiltration of the subserosa
T3 involve the serosa
T4 involve the surronding organs (pancreas, colon, spleen, diaph)
N (regional lymph nodes)N0 no lymph node metastasis
N1 metastasis in the perigastric lymph nodes(distance <3 cm)
N2 metastasis in the perigastric lymph nodes(distance >3 cm)
Wirchow lymph node
M (distant metastases)Krukenberg tumor

Operation of the stomach cancer
Gastrectomy and - regional lyphadenectomy
- omentectomy
- splenectomy (if there is metastasis in the hilum)
- if it is necessery resection of the colon or pancreas
Antrectomy: small tumor
Reconstruction
after gastrectomy

Gastric cancer: 5 year survival rates
Carcinoma in situ (2%) 100%
Stage I (6%) 43%
Stage II (9%) 42%
Stage III (17%) 6%
Stage IV (67%) 0%
Liver 35-40%
Colon 35-40%
Klatskin 20-30%
Oesophagus 10-20%
Pancreas 8-15%
Gallbladder 0-5%
Stomach 20-25%
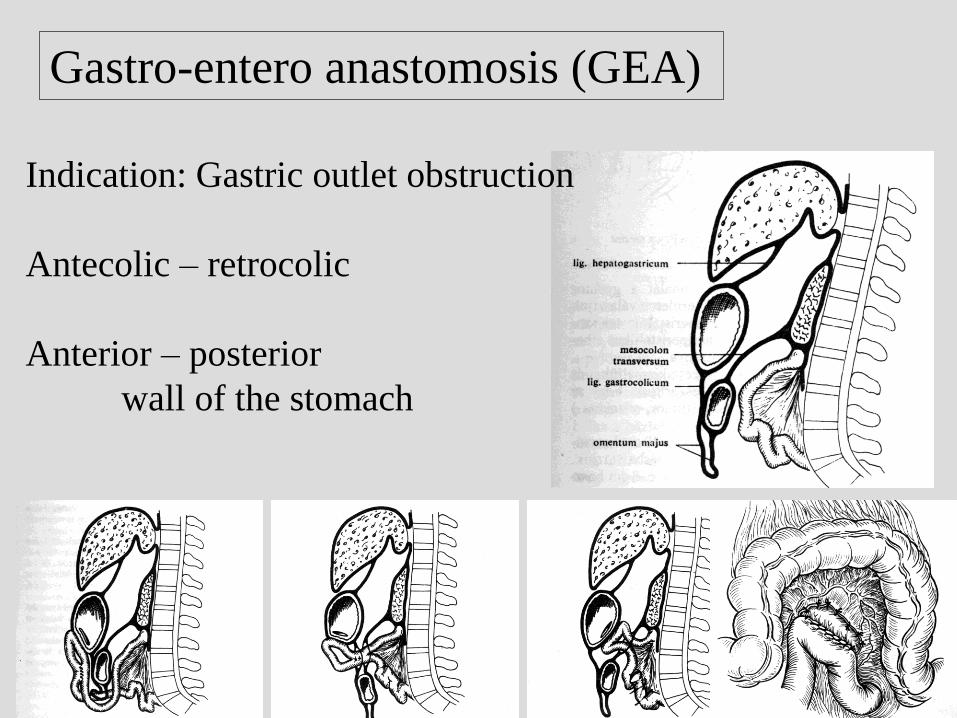
Gastro-entero anastomosis (GEA)
Indication: Gastric outlet obstruction
Antecolic – retrocolic
Anterior – posterior
wall of the stomach

P. Lukovich
Indications:
- obstruction of the oesophagus
- feeding problem
(coma, muscle diseases)
Local anaesthesia (high risk patients!)
Surgical gastrostomy
Witzel (1891)
Kader (1896) (Stamm-Senn)
Percutan endoscopic gastrostomy (PEG)