Embed Size (px)
Citation preview

Annals of the Rheumatic Diseases 1986, 45, 475-483
Gastrin, gastric acid secretion, and gastric microflorain patients with rheumatoid arthritisK HENRIKSSON,' K UVNAS-MOBERG,3 C-E NORD,4 C JOHANSSON,2 ANDR GULLBERG'From the 'Department of Rheumatology and the 2Department of Medicine, Karolinska Hospital; the3Department of Pharmacology, Karolinska Institute, and the 4National Bacteriological Laboratory,Stockholm Sweden
SUMMARY The relation between the basal and stimulated gastric acid secretion, plasma gastrin,and the gastric microflora was examined in 45 patients with rheumatoid arthritis. Sixteen patients(36%) had basal achlorhydria, and of these, 10 (22%) had achlorhydria or hypochlorhydria afterstimulation with pentagastrin. The peak acid output and acidity showed inverse correlation withthe disease duration but were not associated with age or with the degree of physical disability.Hypergastrinaemia was found in nine patients (20%), of whom 6 (13%) had significant titres ofparietal cell antibody. The acidity of the peak acid output showed negative correlation withplasma gastrin. It was confirmed that the gastric secretory state is a determinant of plasma gastrinlevels and in addition influences the growth of micro-organisms in the gastric lumen. The type ofmicroflora in the non-acid stomach was similar to that found in the saliva. A subgroup of eightfemales was identified who showed low gastric acid secretion rates, positive bacterial cultures,and atlantoaxial subluxation. Gastrin- and insulin-like immunoreactivities were found in jointfluid. The concentrations reflected their plasma levels, suggesting that the peptides are notreleased at the inflammatory site, but rather that they reach synovial fluid from circulating blood.
Key words: atlantoaxial joint, gastritis-atrophic, insulin, peptides, saliva, synovial fluid.
Previous studies have shown that patients below 40years of age with rheumatoid arthritis (RA) have areduced gastric secretory capacity. 1-3 Raised plasmagastrin levels in RA were reported first by Rooney etal in 1973,4 but gastric acid secretion was notexamined. An inverse relation between gastric acidsecretion and plasma gastrin was reported in suchpatients by Rowden et al,5 but the frequency ofachlorhydria was similar to that of normal controls.In a subsequent study De Witte et al confirmed thatincreased plasma gastrin was found in patients withachlorhydria or low acid secretion and there wasalso a higher frequency of reduced gastric acidsecretion in the RA patients.6 On the other hand,hypergastrinaemia in the presence of normal pari-etal cell function has been reported in patients withRA,7 8 and this also has been reported in ex-perimental arthritis in the rat.9 "' Since gastrin maybe released from somatic nerves in animals" the
Accepted for publication 10 October 1985.Correspondence to Dr K Henriksson, Department of Rheuma-tology, Karolinska Hospital, -104 01 Stockholm, Sweden.
possibility should be considered that hypergastrin-aemia in RA may be due partly to extragastricrelease.The gastric microbial pattern is known to change
in achlorhidna,'2 '3 and it has been suggested byOlhagen,"1Gullberg,'5 and Bennett'6 that bacterialantigens or other biologically active substances fromthe gastrointestinal microflora may be of importanceas a causative or perpetuating factor in RA.The present study was designed to analyse further
the inter-relation between plasma gastrin, basal andstimulated gastric acid secretion, and gastric micro-flora in patients with rheumatoid arthritis. Deter-minations of gastrin- and insulin-like immunoreac-tivity in joint fluid in parallel with blood plasmawere also performed in order to assess possiblerelease of these peptides at the inflammatory site.
Patients and methods
PATIENTSForty five patients (21 male and 24 female) with an
475
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from
476 Henriksson, Uvnas-Moberg, Nord, Johansson, Gullberg
average age of 57 years (range 24-79) were ex-
amined. All patients had 'classical' or 'definite' RAaccording to the criteria of the American Rheuma-tism Association.17 All patients had symmetrical,peripheral arthritis; in 39 patients the arthritis was
erosive, and 44 patients were seropositive forrheumatoid factor. Sixteen had subcutaneousnodules. Thirty three patients had cervical spinesymptoms, and of these, 11 had atlantoaxial sub-luxation on x ray examination. Four of thesepatients, all female, had such severe instability thatsurgery was indicated. The mean duration of thedisease was 7-5 years (range three months to 24years) dated from the onset of symptoms. Thephysical disability of the patients was evaluated as
functional capacity and graded I to IV.'8 Twentyfour patients were in grade II and 21 in grade III.
One patient had undergone antrectomy for recur-
rent gastric ulcer. All patients had normal renalfunction and none of the patients had perniciousanaemia (PA).Only five patients were without medication at the
time of the study. The remaining 40 patients were
receiving non-steroidal anti-inflammatory drugs(NSAIDs). In addition, 14 patients were on main-tenance treatment with prednisolone at a daily doseof 5-10 mg and one patient received two to threeinjections of adrenocorticotrophic hormone every
week. In combination with predisolone or NSAIDs,or both, 12 patients had chloroquine and fivepatients penicillamine. Proresid, an antimitoticcytostatic agent, was given to a further three otherpatients. Thirteen patients had had only NSAIDs,i.e., first line antirheumatic drugs, during theirdisease, while the other 32 patients had been furthertreated with the aforementioned second line or thirdline drugs, or both, for at least two months.
All patients were evaluated clinically and dividedarbitrarily into three groups with low, moderate,and high disease activity respectively. Laboratoryparameters for the three groups are reported inTable 1.
PROCEDUREThe patients fasted overnight with the last medi-cation given 12-16 hours before the study.
In the morning blood for hormone analysis was
prepared in prechilled, heparinised tubes and centri-fuged at 4°C. The plasma was separated and keptfrozen at -70°C until assayed. Saliva samples were
obtained from 14 patients and cultured both aerobi-cally and anaerobically.Before swallowing a tube for the gastric secretion
test patients rinsed the mouth with an antisepticsolution of ascorbic acid, sodium bicarbonate, andcopper sulphate (Ascoxal). With the patient lying on
Table 1 Laboratory parameters in patient groups withlow, moderate, orhigh disease activity as evaluated clinically*
Disease activitvLow Moderate High(n1 =6) ( =23) (n = 16)
ESR-' (mm/lst h) 17 39 73(4-49) (1(}-95) (29-130)
CRP- (mg/I) <5 18 46(<5) (<5-34) (12-63)
Haptoglobin (g/l) 2-1 3 3 4-5(1 3-26) (18-45) (29-64)
*Values are mean and ranges."ESR=erythrocyte sedimentation rate- CRP=C reactive protein.
the left side the tube (Fg 14, Portex, England) waspositioned in such a way as to permit an optimalrecovery. Saliva was removed by suction. Afterthree 15 min collections of the basal secretion,pentagastrin 6 ig/kg (Peptavlon) was given as a sub-cutaneous injection. A further four collections ofgastric secretions were made at 15 min intervalsafter stimulation. Two to four millilitre samples ofthe gastric contents were aspirated through a sterilesyringe for culture 15 min before and 45 min afterthe pentagastrin injection.
In an additional study samples of blood and jointfluid from a further 12 patients with classical, sero-positive rheumatoid arthritis were withdrawn at thesame time for assay of gastrin and insulin concen-trations. Nine patients had fasted overnight andthree patients had had a light morning meal one totwo hours before sampling.
RADIOIMMUNOLOGICAL DETERMINATIONSGastrin levels were determined according to themethod described by Nilsson'9 using antiserum2604, a gift kindly given by Professor J Rehfeld,Copenhagen. This antiserum recognises gastrin 17and 34 and unsulphated and sulphated forms ofgastrin with the same potency. Insulin determi-nations were performed with the radioimmunoassaydescribed by Nilsson and Uvnas-Wallensten,20 withan antiserum kindly given by Professor S Efendic,Stockholm.
ANALYSES OF GASTRIC JUICEThe volume and the pH of each 15 min gastriccollection were determined. The acidity of sampleswas determined by titration with 0-1 M NaOH topH 7 (Radiometer, Copenhagen). The basal gastricacid output (BAO) is defined as the acid secretionduring 30 min before stimulation; the peak acidoutput (PAO) is defined as the sum of the two
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from

Gastric function in RA 477
highest consecutive measurements after pentagas-trin administration.
MICROBIOLOGICAL INVESTIGATIONSThe saliva specimens from 14 patients and samplesof basal and stimulated gastric secretion from 39patients were transported anaerobically to thelaboratory and prepared for microbial cultureswithin two hours after sampling. Fifty eight gastricsamples, 28 each from basal and stimulated periods,were examined both with and without manipulationof the pH. If the pH was below 4 part of the samplewas adjusted to pH 7*0 with NaOH, if above 4 to pH1*8 with HCI. The pH adjustment was madeimmediately after withdrawal of samples, whichwere thereafter identically treated.The samples were suspended in prereduced
peptone-yeast extract medium ,2I diluted, inoculatedin media, and handled as described by Heimdahland Nord.22 The aerobic agar plates were incubatedfor 24 h at 37°C and the anaerobic plates for 48 h at370C in anaerobic jars (Gas Pak, BBL, Cockeys-ville, Maryland, USA). They were then examined,and colonies were counted under a stereo-microscope.
Aerobic bacteria were identified biochemically as
described elsewhere,22 and anaerobic bacteria were
identified by biochemical tests and gas-liquidchromatography.21
STATISTICAI METHODS
Values are given as mean±SD or range. Wilcoxon'snon-parametric rank test and the X2 test were usedto test significance. Correlation coefficients werecalculated according to Spearman.
Results
GASTRIC ACID
The average basal gastric output (BAO) was
043 mmol/30 min (range 0-2-4), and the peak acidoutput (PAO) after pentagastrin administration was
7-4 mmol/30 min (range 0-23.8). The antrectomisedpatient was achlorhydric. Sixteen of the other44 patients (36%) were achlorhydric in the basalstate. Of these, four had no acid response to stimu-lation and the PAO was less than 1-30 mmol/30 minin an additional six patients. Female patients of allage groups had low average and peak gastric acidsecretion rates. The secretion rate declined with age
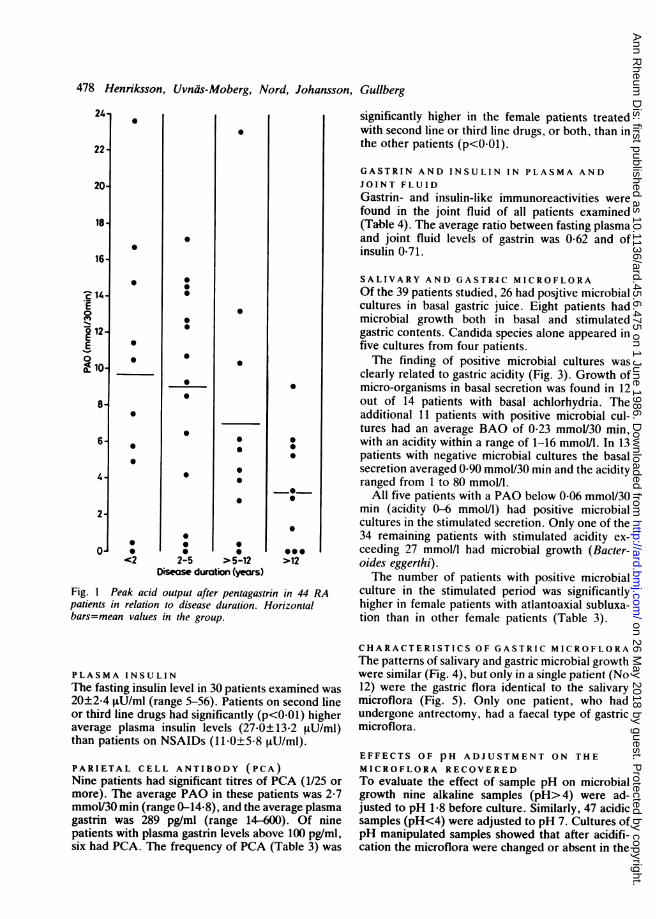
in the male patients (Table 2). The PAO (Fig. 1)was inversely proportional to disease duration(r= -0*39, n=44, p<001) but showed no correlationwith either the inflammatory activity or the degreeof physical disability.The eight female patients with atlantoaxial sub-
luxation had all received second line or third linedrugs, or both, and had significantly lower basal(p<0-02) and stimulated (p<0.01) gastric acidsecretion rates compared with those of the femalepatients without this cervical spine complication(Table 3). The four patients with severe atlantoaxialinstability had all basal achlorhydria and PAObelow 1-3 mmol/30 min. In comparison, malepatients with atlantoaxial subluxation had fewerabnormalities of gastric functions.
PLASMA GASTRINThe average fasting plasma gastrin level was 112pg/ml (range 2 to > 600) and exceeded 100pg/ml in nine patients. There was no sex differ-ence, and correlations with age or disease durationwere absent. There was a statistically signifi-cant inverse relationship between log plasmagastrin and PAO (r=-0-51, n=37, p<0-(1) andeven more impressively with the acidity of the peaksecretion (Fig. 2). Female patients who had beentreated with second line or third line drugs, or both,had significantly higher plasma gastrin levels thanfemale patients treated only with NSAIDs (p<0-05).
Table 2 Basal (BAO) and peak (PAO) stimulated gastric acid secretion in 44 RA patients according to age and sex (theantrectomised patient excluded)
Patients of age (years): All patients
<50 50-60 >60
Female 0-26±0-29* 0-29+0-39 0-42±0-70 0-31±0-45BAO (mmol/30 min) (6)* (11) (6) (23)
Male 1-10±1-20 0-45±0-57 0-38±0-63 0-55±0-74(4) (I 1) (6) (21)
Femalc 6-2+5-4 6-2±5-5 4-6±6-3 5-8±5-5PAO (mmoU30 min) (6) (I1) (6) (23)
Male 94±5-1 11-5+7-7 5-2+4-5 9-3+6-8(4) (I 1) (6) (21)
*Values arc mcan + SD; No of patients given in parentheses.
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from
478 Henriksson, Uvnas-Moberg, Nord, Johansson, Gullberg
24
22
20
18
16
2 14
0
g12-E0E 10-
8-
6-
4-
01
0
0
0
0
0
0
0
<42
0
0
0
0
0
0
0
0
0
0
0
2-5 > 5-12Disease duration (years)
0
0
~0~
-0
00
>12
Fig. 1 Peak acid output after pentagastrin in 44 RApatients in relation to disease duration. Horizontalbars=mean values in the group.
PLASMA INSULINThe fasting insulin level in 30 patients examined was20±2-4 tLU/ml (range 5-56). Patients on second lineor third line drugs had significantly (p<0-01) higheraverage plasma insulin levels (27.0±13-2 t%U/ml)than patients on NSAIDs (11-0±5-8 ,uU/ml).
PARIETAL CELL ANTIBODY (PCA)Nine patients had significant titres of PCA (1/25 ormore). The average PAO in these patients was 2-7mmol/30 min (range 0-14-8), and the average plasmagastrin was 289 pg/ml (range 14-600). Of ninepatients with plasma gastrin levels above 100 pg/ml,six had PCA. The frequency of PCA (Table 3) was
significantly higher in the female patients treatedwith second line or third line drugs, or both, than inthe other patients (p<0-01).
GASTRIN AND INSULIN IN PLASMA ANDJOINT FLUIDGastrin- and insulin-like immunoreactivities werefound in the joint fluid of all patients examined(Table 4). The average ratio between fasting plasmaand joint fluid levels of gastrin was 0-62 and ofinsulin 0-71.
SALIVARY AND GASTR4C MICROFLORAOf the 39 patients studied, 26 had positive microbialcultures in basal gastric juice. Eight patients hadmicrobial growth both in basal and stimulatedgastric contents. Candida species alone appeared infive cultures from four patients.The finding of positive microbial cultures was
clearly related to gastric acidity (Fig. 3). Growth ofmicro-organisms in basal secretion was found in 12out of 14 patients with basal achlorhydria. Theadditional 11 patients with positive microbial cul-tures had an average BAO of 0-23 mmol/30 min,with an acidity within a range of 1-16 mmol/l. In 13patients with negative microbial cultures the basalsecretion averaged 0-90 mmol/30 min and the acidityranged from 1 to 80 mmol/l.
All five patients with a PAO below 0-06 mmol/30min (acidity 0-6 mmol/l) had positive microbialcultures in the stimulated secretion. Only one of the34 remaining patients with stimulated acidity ex-ceeding 27 mmol/l had microbial growth (Bacter-oides eggerthi).The number of patients with positive microbial
culture in the stimulated period was significantlyhigher in female patients with atlantoaxial subluxa-tion than in other female patients (Table 3).
CHARACTERISTICS OF GASTRIC MICROFLORAThe patterns of salivary and gastric microbial growthwere similar (Fig. 4), but only in a single patient (No12) were the gastric flora identical to the salivarymicroflora (Fig. 5). Only one patient, who hadundergone antrectomy, had a faecal type of gastricmicroflora.
EFFECTS OF pH ADJUSTMENT ON THEMICROFLORA RECOVEREDTo evaluate the effect of sample pH on microbialgrowth nine alkaline samples (pH> 4) were ad-justed to pH 1-8 before culture. Similarly, 47 acidicsamples (pH<4) were adjusted to pH 7. Cultures ofpH manipulated samples showed that after acidifi-cation the microflora were changed or absent in the
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from

Gastric function in RA 479
Table 3 Laboratory findings in 45 RA patients with or without atlantoaxial subluxation (AAS) and treatment with orwithout second line or third line drugs, or both (>two months)
First line drugs only Second line or third line drugs, or both
Females Males Females with Females without Males(n=8) (n=5) ASS (n=8) ASS (n=8) (n=16)*
Mean age, years (range) 53 (38-62) 55 (49-59) 56 (24-77) 60 (47-73) 57 (34-79)Mean disease duration, (range) 5 (0-5-18) 2 (0-5-6) 9 (2-21) 9 (0-25-24) 8 (0-25-23)Basal achlorhydriat 2/8 2/5 7/8 2/8 4/16BAO, mmol/30 min (mean±SD) 0-62±0-59 0-42±0-52 0-04±0-12t 025±0-31 0-65±0-79PAO <1-3 mmol/30 mint 2/8 1/5 6/8 1/8 2/16PAO, mmol/30 min (mean±SD) 9-0±5-9 10-0±9-0 1-3±2-01 6-4±4-9 9-0±2-3Plasma gastrin > 100 pg/mlt 0/7 1/3 4/7" 3/8 1/12Parietal cell antibodyt 0/8 1/5 5/8 2/8 1/16Positive bacterial cultures in
stimulated periodt 0/8 0/5 5/6' 1/6 2/14
*Three patients with AAS.'Number of patients.tp<0-02, lp<0-01 v all other female patients.'Me antrectomised patient excluded.
majority of those tested (Table 5). Similar resultswere obtained by alkalisation of samples beforeculture. In the samples of changed microflora afterpH adjustment Lactobacillus species (Lactobacillusacidophilus or Lactobacillus plantarum) dominated.
600-
300-
E 100-a.
a 50-cm0~
20-
10
0
0
0
0
0 0
0 0
0 0
0 @0
0
*00
0
0
0
I.:
0
0
* 2
0 50 100Peak acidity (mmol/l)
Fig. 2 The acidity of the peak secretion plotted against thelogarithm of the plasma gastrin level (r=-0-69, n=37,p<O0OOI)
Discussion
This study first confirms an association between thegastric secretory state and plasma gastrin levels andsecond demonstrates growth of micro-organisms inthe gastric lumen in female patients with severerheumatoid arthritis.More than one third of the patients had basal
achlorhydria and almost one fourth were achlorhyd-ric or had very low acid response after stimulation.This is in agreement with earlier studies.' 2 3 6 Shortet al found that gastric achlorhydria was significantlymore frequent in RA patients below 40 years of age,in particular among female patients.2 Thus RA infemales is apparently associated with the develop-ment of achlorhydria early in life. In addition, thesecretory state of the patients showed positivecorrelation with the duration of the disease, whereascorrelation with age was absent.As observed previously 4 6 8 a large number of RA
patients had raised plasma gastrin values. Thegastrin levels correlated inversely with the acidsecretory status, an observation which is in agree-ment with the study by De Witte et al.6 In a fewpatients in this series a high plasma gastrin coexistedwith normal gastric acidity. This combination hasbeen reported previously by Rooney et al both inRA patients7 and in experimental arthritis in therat." In the experimental series there seemed to becorrelation between plasma gastrin and severity ofinflammation, but any causative relation remains tobe proved. Other peptides, such as substance p,23may also vary with the degree of inflammation. Thegastrin- and insulin-like immunoreactivities in joint
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from

480 Henriksson, Uvnas-Moberg, Nord, Johansson, Gullberg
Table 4 Concentrations of gastrin and insulin in plasma and joint fluid taken simultaneously in fasting subjects (patientsNos 1-9) and at variable times after food intake (patients Nos 1012)
Patient No Gastrin (pgltnl) Gastrin ratio Insulin (4U/mli Insulin ratiojoittlplasna - jointlplasma
Plasma Joinit Plasma Joint
1 6600 210 0 35 11 6 0-55 Fasting2 430 26) 0-60 14 9 0(64 Fasting3 364 314 0-86 12 5 0-42 Fasting4 106 44 (o42 18 15 0-83 Fasting5 95 75 0(79 19 30 158 Fasting6 88 48 155 12 9 075 Fasting7 39 38 0)97 38 18 0(47 Fasting8 38 23 0(60 18 9 0550 Fasting9 41 18 0(44 25 16 0-64 Fasting10 48 86 1 79 53 20 0 38 Postprandial (1-2 h)11 5 44 8.8 17 0(29 Postprandial (1-2 h)12 147 86 0-59 160 17 0 11 Postprandial (I h)
fluid from the patients appear to reflect the plasmalevels. It is thus likely that the peptides reach thejoints from circulating blood.
Raised gastrin levels together with PCA inachlorhydric patients are suggestive of a type A
24 igastritis. This type is associated with various organspecific autoimmune diseases. Atrophic changes ofthe gastric mucosa have been reported previously in
patients with RA25 26 and are common in Sjogren'ssyndrome.27 The same combination of increasedplasma eastrin and PCA is seen in perniciousanaemia. It is noteworthy that not a single patientin the present study had manifest PA or reducedplasma levels of vitamin B12, which is in accordancewith earlier studies.27 28A majority of patients with basal achlorhydria or
Stimulated period
0
0
isI:IS
SS
00
No growth Growth of Growth ofbacteria candida
No growth
Fig. 3 The relation between gastric acidity (mmolll) andbasal and stimulated periods.
occurrence of micro-organisms in gastric secretion during
0
0
8-
6-
0E
2-
0-
00
-16
-14
-12
10>_.c
-8 33
-6
-4
-2
-0
0
160
@I0rS.0
WilL
Growth ofbacteria
*000
Growth ofcandida
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from

Micro-organisms
StaphylocciStreptococcia-StreptococciEnterococciE. CoiKlebsiellaHaemophius
Salivarysecretiona .
Boo.ones
so-
*0e*-0
Lactobacilli *womon
Peptococci U
ClostridiaBifidobcact.Propionibact.EubacteriaVeillonella
*
on
U
Gastric secretionQk^cnl Ctfimf dedtlVasal :)UMUCReu
very low gastric acidity had micro-organisms in thestomach, as evaluated by positive cultures of basal
* * gastric secretion, whereas none of the patients with::00:::0 00. acid secretion in the basal period had a positive* * bacterial culture. This is in agreement with earlier* studies of gastric microflora. t2 13 Similar microflora* f were found in saliva and gastric secretion, and a
000faecal type of flora was found only in an antrecto-mised patient.
*nnn *n Interestingly, the gastric contents became sterileo000 when patients responded to pentagastrin with acid* secretion. The slightest in vivo acidification of the
* Table 5 Effect ofpH adjustments on the microflora in 56gastric samples. Alkaline samples (pH> 4) were adjustedto pH 18 and acid samples (pH<4) were adjusted to pH 7
~~~~~before cultureBacteroides on 0000 *o
Fusobacteria No 0
Candida *0
* Gastric acid secretion less than 1.30 (mmol/30min)o Gastric acid secretion more than 1.30 (mmol/30min)* Salivary secretion
Fig. 4 The different micro-organisms cultivated fromsaliva and gastric secretion (basal and stimulated) andtheir relation to acid secretion.
Original sample After pH adjustment
Acidification (n=9) Alkalisation (n=47)
Chaniged Negative Changed Negativeflora flora
Positive 4 5 5 7Negative 0 0 4 31
Patients NoMicro-organismsStaphylococciStreptococcia-StreptococciEnterococciE. Coi
KlebsielkaHaemop~lus
LactobaciUiPeptococciClostridiaBifidobact.
Propionibact.EubacteriaVeillonellaBacteroides
FusobacteriaCandida
No growth
1 2 3 4 5 6 7 8 9 10 11 12 13 14
0
0
0
I a
U a
IN
U
0
0
U
U.0
U
o
:
U
o
.
0 0 00
a
U
0 0
U
a a
0
U
0
U
U
U
U
a
.
* a
U
U
U
0
.
a . I
o
* Salivary secretion * Basal secretion o Stimulated secretionFig. 5 The relation between the micro-organisms in salivary and gastric secretion (basal and stimulated) in each patient.
Gastric function in RA 481
a
a
U
0 0
In a* a
* 0
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from

482 Henriksson, Uvnas-Moberg, Nord, Johansson, Gullberg
stomach was effective in eliminating microbialgrowth as opposed to in vitro pH manipulation.Microbial overgrowth of the non-acid stomach maythus be cleared away even by minute amounts ofsecreted acid. The possibility of the concomitantrelease of other antimicrobial agents should also beconsidered.
In a comparative study of various rheumaticdisorders Rooney et al found hypergastrinaemiaonly in patients with rheumatoid arthritis.29 Ed-strom reported in 1939 that gastric achlorhydria inRA patients was associated with high diseaseactivity and disturbed peripheral circulation withneuropathic disturbances.' This investigation re-ported that the secretory anomaly of the stomachdisappeared in a number of RA patients, whoexperienced parallel improvements in generalclinical condition, joint swelling, and peripheralcirculation. It was concluded that the depressedsecretion must be a phenomenon secondary to therheumatic tissue process.
In this study the gastric acid secretion ratesshowed no clear correlation with the clinical diseaseactivity, but the PAO tended to be lower in patientswith high inflammatory activity. A subgroup offemale patients who had been treated with secondline or third line drugs, or both, and with atlanto-axial subluxation had lower basal and stimulatedacid secretion rates, higher frequency of PCA, andpositive bacterial cultures compared with femaleswithout this complication. Such subluxation is morecommon in females3" and indicates a destructiveform of RA.3' The gastric mucosa changes andatlantoaxial subluxation in the female patientsstudied may both be consequences of a severerheumatic disease, but the possibility should also beconsidered that disturbances in the gastrointestinalflora may influence the course of the disease. Therole of antirheumatic medication in the pathogenesisof gastric changes in RA is unclear.
Biologically active substances derived from gas-trointestinal contents or from imbalance in peptidehormone systems, or both, may be of significance inthe pathogenesis of RA. As there seem to be anassociation between destructive RA and low gastricacid secretion it seems important to study furtherthe mechanisms and the consequences of thesedisturbances in the gastric secretory functions.
These investigations wcre supportcd by grants from the SwedishSociety against Rheumatism, the King Gustaff V 8() vear Foun-dation. and the Swedish Medical Rcscarch Council.
References
1 Edstrom G. Magensekretion und Grundumsatz bei den chronis-chen rheumatischen Arthritiden. Acta Med Scand 1939; 99:228-56.
2 Short C L. Bauer W. Reynolds W E. Gastric aciditv. In:Rheutnatoid arthritin. Cambridge. Massachusetts: HarvardUniversity Prcss. 1957: 361-6.
3 Olhagen B. Intestinal Clostridiumin perfringens in arthritis andallied conditions. In: Dumonde D C. ed. Itnfectiont antdimnmnunologs in rheutnatmc diseases. Oxford: Blackwell. 1976:141.
4 Roones P J. Vincc J. Kenncdv A C. ei al. Hvpergastrinacmia in
rhcumatoid arthritis: diseasc or iatrogenesis? Br MecdJ 1973: ii:752-3
5 Rowvden D R. Tavlor I L. Richter J A. Pinals R S. Levine R A.Is hypergastrinaemia associated with rheumatoid arthritis. Gut1978: 19: 1064-7.
6 De Wittc T J. Geerdink P J. Lamers C B. Boerhooms A M.Van der Korst J K. Hypochlorhydria and hvpergastrinaemia in
rheumatoid arthritis. Antn Rheiwn Dis 1979: 38: 14-7.7 Roonev P J. Kenneds A C. Gray G H. Sturrock R D.Buchanan K D. Dick W C. Scrum immunorcactive gastrin in
rheumatoid arthritis. Antn Rheu,n Dis 1976: 35: 24-50).8 Altomonte L. Sommella L. Negrini A P. Palumbo P. Magaro-M. Greco A V. Serum gastrin in rheumatoid arthritis. MineriaMed 1982: 73: 1761-3.
9 Rooncs P J. Dick W C. Buchanan K D. Imric R C. An animalmodel to studs the rclationship between immunoreactivegastrin and inflarmmatorv arthritis. Natlre 1973., 246: 497-8.
1() Rooncs P J. Dick W C. lmric R C. Turner D. Buchanain K D.Ardill J. On the rclationship between gastrin. gastric secretion.and adjusant arthritis in rats. Antnt Rheu,n Dis 1978: 37: 432-5.
11 Uvnas-Wallensten K. Uvsnas B. Release of gastrin on stimu-
lation of the sciatic and brachial nerses of the cat. Acta PhYsiolScand 1978: 103: 349-51.
12 Gras J D A. Shincr M. Influence of gastric p11 on geastric andjejunal flora. Guit 1967: 8: 574-81.
13 Drasatr B S. Shiner M. McLeod G M. Studies on the intestinalflora: I. The bacterial flora of the gastrointcstinal tract in
hcalths and achlorhvdric pcrsons. GastroenteroloiY, 1969: 56:71-9.
14 Olhagcn B. Mansson 1. Intcstinal Clostridiumn perfriniigensi in
rhcumattoid arthritis and othcr collagcn discases. Acta MedcScatid 1968: 184: 395-4)2.
15 Gullbcrg R. Possiblc rolc of alterations of the intcstinal flora in
rhcumatoid arthritis. Rhelumnatol Rehabil 1978: suppl: 5-1(0.16 Bcnnctt J C. The infcctious etiology of rheumatoid arthritis.
Art/1r'tis Rheuon 1978: 21: 531-8.17 Ropcs M W. Bennctt G A. Cobbs S. Jacox R. Jcssar R A.
Revision of diagnostic criteria for rheumatoid airthritis. BullRhelutiDois 1958:X 9: 175-6.
18 Steinbrockcr 0. Tracgcr C 11, Battcrman R C. Thcrapcuticcriteria in rheumatoid arthritis. JAMA 1949: 140: 659-62.
19 Nilsson G. Incrcased plasma gastrin lcvels in connection withinhihition of gastric acid rcsponses to sharm fceding followingbulhar pcrfusion with acid in dogs. Scanid J Gastrocnterol 1975:10: 273-7.
20 Nilsson G. Uvnas-Wallensten K. Effect of teasing, shamfeeding and feeding on plasma insulin concentrations in dogs.In: Radioimmunoassav: methodology and applications inphysiology and in clinical studies. Stuttgart: Thieme. 1974: 91-7.(Commemorative Issue for Salomon A Berson.)
21 Holdeman L V, Cato E. Moore W E C. In: Anaerobelaboratory manual. 4th ed. Blacksburg. Virginia: VirginiaPolytechnic Institute and State University. 1977.
22 Hcimdahl A. Nord C E. Effect of phenoxymethylpenicillin andclindamycin on the oral, throat and faecal microflora of man.Scand J In,fect Dis 1979: tI: 233-42.
23 Levinc J D. Clark R. Devor M. Helms C. Moskowitz M A.Basbatum A I. Intraneuronal substance P contributes to theseveritv of cxperimental arthritis. Science 1984: 226: 547-9.
24 Strickland R G, Mackay. I R. A reappraisal of the nature and
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from

Gastric function in RA 483
significance of chronic atrophic gastritis. Am J Dig Dis 1973; 18:426-40.
25 Louyot P, Tamisier J N, Jeanpierre J, Pourel J, Zannetti A,Bertrand P. Le comportement gastrique au cours des rhuma-tismes inflammatoires sous incidence medicamenteuse. RevRhum Mal Osteoartic 1974; 41: 725-32.
26 Marcolongo R, Bayeli P F, Montagnani M. Gastrointestinalinvolvement in rheumatoid arthritis: a biopsy study. J Rheuma-tol 1979; 6: 163-73.
27 Maury C P J, Tornroth T, Teppo A-M. Atrophic gastritis inSjogren's syndrome: morphologic, biochemical and immuno-logic findings. Arthritis Rheum 1985; 28: 388-94.
28 Pitcher C S, Lindsay D J, Hill A G S. Absorption of vitamin B12in rheumatoid arthritis. Ann Rheum Dis 1970; 29: 533-6.
29 Rooney P J, Grennan D M, Sturrock R D, Brooks P M, DickW C. Serum immunoreactive gastrin: specificity for rheumatoidarthritis, bimodality of distribution, and failure of effect of anti-inflammatory drugs. Ann Rheum Dis 1976; 35: 40-5.
30 Winfield J, Cooke D, Brook A S, Corbett M. A prospectivestudy of the radiological changes in the cervical spine in earlyrheumatoid disease. Ann Rheum Dis 1981; 40: 109-14.
31 Bland J H. Rheumatoid arthritis of the cervical spine. JRheumatol 1974; 1: 31942.
on 26 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.45.6.475 on 1 June 1986. Dow
nloaded from
























![Atube catcher[1]](https://img.pdfslide.net/doc/110x75/545737fbaf7959c6788b8b3c/atube-catcher1.jpg)



