Embed Size (px)
Citation preview

Gastroesophageal Reflux and HiatalHernia
Michael E. Höllwarth and Erich Sorantin
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
The Normal Esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Innervation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Peristalsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Lower Esophageal Sphincter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Reflux . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Upper Esophageal Sphincter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Diagnosis of Reflux . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Esophageal Passage on the X-ray . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Twenty-Four-Hour pH-Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Combined Impedance Measurement/pH-Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Manometry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Endoscopy and Histology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Diagnostic Nuclear Medicine Investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Development of Esophageal Function in Childhood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Pathological Reflux and Symptoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Newborns and Infants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Childhood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Treatment of GERD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Conservative Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Drug Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Surgical Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
M. E. Höllwarth (*)Department of Paediatric and Adolescent Surgery, MedicalUniversity of Graz, Graz, Austriae-mail: [email protected];[email protected]
E. SorantinDepartment of Pediatric Radiology, Medical University ofGraz, Graz, Austriae-mail: [email protected]
© Springer-Verlag GmbH Germany, part of Springer Nature 2020P. Puri (ed.), Pediatric Surgery,https://doi.org/10.1007/978-3-642-38482-0_95-1
1

Fundoplication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Complications of Fundoplication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Other Surgical Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Barrett’s Esophagus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Associated Diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Laryngopharyngeal Reflux . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Reflux-Associated Respiratory Tract Infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Reflux and Asthma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Reflux and Apnea Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Eosinophilic Esophagitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Hiatus Hernia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Axial Hiatus Hernia (Fig. 12) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Para-esophageal Hiatal Hernia (Fig. 13) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Conclusion and Future Directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Cross-References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
AbstractGastroesophageal reflux, caused by transientrelaxation of the lower esophageal sphincter,is the term used to describe the backflow ofgastric content into the esophagus. Pathologi-cal reflux disease is a situation in which refluxcauses major symptoms and complicationssuch as failure to thrive, disturbances of sleep,recurrent aspiration and cough predominantlyin young infants and epigastric pain, esophagi-tis, stenosis, or Barrett’s esophagus in olderchildren. A variety of diagnostic investigationsare necessary to evaluate the extent and conse-quences of pathological reflux. Conservativemanagement with different medications iswidely used. However, in children withchronic gastroesophageal disease, surgicaltherapy by fundoplication is the treatment ofchoice.
KeywordsGastroesophageal reflux · Esophagitis ·Barrett’s esophagus · Fundoplication · Hiatushernia · Eosinophilic esophagitis · Sandifersyndrome
Introduction
Gastroesophageal reflux (GER) is a physiologicalphenomenon. It occurs in persons of all agegroups and more frequently after the ingestion ofliquid food (soup) or other fluids (soft drinks,coffee, alcohol, etc.). A pathological reflux orgastroesophageal reflux disease (GERD) is con-sidered to exist when the number and/or durationof reflux events exceeds normal ranges. The inci-dence of GERD in the population is difficult todetermine, because the majority of refluxes areasymptomatic. The disease becomes clinicallyevident only when complications and theiraccompanying symptoms occur. Epidemiologicdata in adults show that approximately 20% ofthe Western population is affected, and GERD isnow the most common gastrointestinal disorder inthe Western world (Dent et al. 2005). In an Italianstudy, 12% of more than 2000 infants (less than1 year old) had clinical symptoms of reflux, butonly 1 of 210 infants older than 24 months of agedeveloped reflux disease (Vandenplas et al. 1991;Campanozzi et al. 2009). The significance of gas-troesophageal reflux or reflux disease is reflectedby 300–400 publications each year on the subject,focused on diagnostic and therapeutic aspects. Inthe following, we discuss the normal function ofthe esophagus; the development of esophageal
2 M. E. Höllwarth and E. Sorantin

function in newborns and infants; symptoms,investigation methods in patients with pathologi-cal reflux; therapeutic options and complicationsof reflux disease; and its potential late sequelae.
The Normal Esophagus
Anatomy
The esophagus is a muscular tubular organ in thedorsal mediastinum, responsible for transportingfood from the mouth or the pharynx into thestomach. The esophagus is about 8 cm long inthe newborn infant and about 25 cm long in theadult. Striated muscles are found in the upper halfof the esophagus and smooth muscles in the lowerhalf. The lumen covers a non-keratinizing multi-layered squamous epithelium with a papillarytype of basal layer. The transition to the single-layered columnar epithelium of the cardia is seenon endoscopy as an irregular line, the so-called Z-line, which partly extends in tongue-like fashioninto the esophagus and, in terms of its location,often does not exactly correspond with the ana-tomical barrier of the lower esophageal sphincter.
Within the diaphragmatic hiatus, the esopha-gus is fixed to the diaphragm by the phrenico-esophageal membrane. While the medial wall ofthe esophagus continues directly into the lessercurvature of the stomach, a type of incisure ariseson the lateral circumference in the direction of thefundus – the so-called angle of His. The lattertends to be flat on the X-ray of a newborn –because of the inferior position of the diaphragm,but in adults, it is clearly sharp-angled. At this site,there is a mucosal fold within the gastric lumen(the flutter valve), which is pressed passivelyagainst the esophagus when the gastric fundus isfilled, and thus prevents reflux (Fig. 1) (Edwards1982). The flatter the angle of His, the less devel-oped the mucosal valve mechanism; reflux canoccur more easily in this setting.
Innervation
Parasympathetic innervation of the esophagus isachieved by the vagus nerve, which courses alongthe esophagus and sends its fibers to the latter.Sympathetic innervation is achieved by postgan-glionic neurons of the sympathetic trunk. Themyenteric plexus and the submucosal plexus con-tain non-adrenergic and non-cholinergic nervesand initiate the complex activity of the esophagusthrough a number of neurotransmitters. Centralregulation is achieved in the deglutition centerlocated in the brainstem and core areas of peristal-sis connected in a serial fashion. In infants withcentral sleep apnea and in cerebral disabledpatients, disorders in the central coordination ofmotor functions of the esophagus play a majorrole in the etiology of reflux.
Peristalsis
Once food enters the esophagus, it is passed on tothe stomach by means of an orderly propulsiveperistaltic wave (pressure between 60 and100 mmHg, velocity 2–4 cm/s) (primary peristal-sis; Fig. 2). After localized distension of theesophagus, as happens during reflux of gastriccontent, a propulsive peristaltic wave is generatedlocally that returns the refluxed volume back tothe stomach (secondary peristalsis). Isolated and
Fig. 1 Typical mucosal “flutter valve” at the site of the Hisangle within the stomach (arrow). Opposite one can see apart of the cardia epithelia (star)
Gastroesophageal Reflux and Hiatal Hernia 3

disorderly non-propulsive contractions aredescribed as “tertiary peristalsis” or “pathologicalcontractions.”
Lower Esophageal Sphincter
Backward flow of the contents of the stomach intothe esophagus is prevented by the lower esopha-geal sphincter (LES). The LES pressure isbetween 12 and 15 or 25mmHg, not only in adultsbut also in neonates and infants. The length of theLES in the newborn is about 1.0 cm; in the adult, itis about 2.5–3.5 cm (Table 1) (Höllwarth 1979;Höllwarth et al. 1986; Omari et al. 2002). Whilethe pressure zone can easily be demonstrated bymanometry, a special anatomical technique ofpreparation is required to detect thickening ofthe sphincter muscle at the esophagogastric tran-sition (Liebermann-Meffert et al. 1979).
Onmanometry, the pressure zone makes it easyto exactly determine the position of the LES – and
thus the position of the lower end of the esopha-gus. The LES lies exactly within the esophagealhiatus, and the lower portion of the pressure zoneis attributed to the abdominal pressure regionwhile the upper portion is assigned to the chestpressure cavity (Fig. 3). The frequently describedcondition of an abdominal esophagus does clearlynot exist in a normal person. The diaphragmaticpinch within the hiatus also contributes to theoverall tone of the esophagogastric junction. Itcan be distinguished by manometry in cases of afixed hiatal hernia.
Reflux
An essential characteristic of the LES is that itstone becomes relaxed by propulsive peristalsiswhen food enters the esophagus. Even in a healthyperson, and even without any other motor activityin the esophagus, spontaneous relaxations occurregularly and persist for 5–10 s (transient sphinc-ter relaxation) (Mittal and Balaban 1997). Nitricoxide is involved in the timing of human esopha-geal peristalsis and is one of the neurotransmittersinvolved in the reflex arc mediating the triggeringof transient LES relaxations (Hirsch et al. 1998).Physically, this causes a shared space between thestomach and the esophagus, with the occurrenceof a typical abdominal pressure curve in theesophagus on manometry, the “common cavityphenomenon” (Fig. 4) (Butterfield et al. 1972).Due to greater abdominal pressure on the onehand, and the thoracic suction effect during inspi-ration on the other, these spontaneous relaxationsare usually accompanied by a reflux of the con-tents of the stomach and – depending on the pH ofthe contents of the stomach – to a drop, a rise, orno change in pH levels in the esophagus (Fig. 5).The refluxed volume is rapidly returned to thestomach by secondary propulsive peristalsis (vol-ume clearance). However, the pH drop is neutral-ized in a stepwise manner by saliva duringsubsequent acts of swallowing (acid clearance)(Fig. 6). In contrast to a healthy person, the num-ber and duration of spontaneous relaxations aswell as the acid clearance time rise significantlyin a person GERD, as will be described later on.
Fig. 2 Primary propulsive peristalsis after swallowing.One single irregular tertiary contraction in the distal esoph-agus (Höllwarth 2009)
4 M. E. Höllwarth and E. Sorantin

Upper Esophageal Sphincter
Pressure values in the upper esophageal sphincter(UES; 40–80 mmHg) are much higher than thosein the LES, which indicates that reflux into theesophagus may occur more easily than reflux into
the pharynx or the oral cavity. The UES relaxesduring the propulsion of food from the oral cavity,and strong contraction of the hypopharynx passesthe bolus with great velocity into the esophagus.However, even when reflux approaches frombelow, the UES might relax and reflux can reachthe hypopharynx, larynx, and eventually themouth.
Diagnosis of Reflux
Esophageal Passage on the X-ray
X-rays with contrast material are mainly used toinvestigate the morphology and peristaltic func-tion of the esophagus. The primary benefits of anX-ray investigation include visualization of theesophagogastric junction or evidence of a slidingor fixed hiatal hernia, assessment of the angle ofHis, the presence of an orderly or pathologicalpharyngoesophageal act of swallowing, thecourse of esophageal peristalsis, and any irregu-larities of the epithelium as signs of inflammation.Evidence of aspiration of contrast medium duringthe investigation is another important finding.Actual evidence of reflux episodes, on the otherhand, is of lesser significance because the durationof a barium esophagogram is short and an obviousreflux may occur or not occur during the fewminutes of fluoroscopy. However, indirect signsof a GERD are several: frequent air reflux duringthe investigation, a positive water siphon test(reflux after drinking a large sip of water to pro-voke reflux), and in the case of a reflux events, it
Table 1 Results of esophageal manometry: the LES pres-sure values in newborn babies and infants are alreadynormal. PS is the response of propulsive peristaltic wavesin the esophagus after 10 induced swallows. The results
show that the response is significantly lower within the first10 days of life, but thereafter it is normal with nearly8 propulsive responses out of 10 induced swallows(Höllwarth and Uray 1985)
n Age (d) LES-tone (mm HG) x� SD LES-length (mm) x� SD PS (n = 10)
Prematures (GA 30–36) 7 7–28 23.0 � 3.6 1.0 � 1.1 –
Newborns 24 1–10 20.4 � 8.0 10.7 � 0.8 5.2�
Newborns 19 11–28 21.8 � 10.0 11.0 � 0.5 7.3
Infants 20 >28 18.0 � 7.0 11.3 � 1.1 7.9�p < 0.05
Fig. 3 Slow pull-through manometry through the LES ina newborn child. DU indicates the pressure inversion froma typical stomach tracing to a typical esophageal tracing.Thus, the DU is located within the diaphragmatic hiatusand one part of the LES belongs to the abdomen and theother part to the thorax. There is no other intra-abdominalesophagus (Höllwarth 2009)
Gastroesophageal Reflux and Hiatal Hernia 5

Respiration
Stomach
Lower esophagus
Upper esophagus
Fig. 4 Spontaneouspressure inversion of theesophageal tracing to anabdominal tracing indicatesthe opening of the LES dueto a transient relaxation.This is the manometric signof reflux – the “commoncavity phenomenon”(CCP). It is alwaysterminated by a secondarypropulsive peristalsispushing the refluxedvolume back into thestomach (volume clearance)(Höllwarth 2009)
Upper esophagus
Lower esophagus
Stomach
Stomach
pH
Respiration
Fig. 5 Common cavityphenomenon with refluxand simultaneous rise of theintraesophageal pH. Thisreflux cannot be detectedwith simple pH-monitoring
6 M. E. Höllwarth and E. Sorantin

will be recorded to which height these refluxesreach in the esophagus (lower/middle/upperesophagus).
Twenty-Four-Hour pH-Monitoring
This investigation, performed on an out-patientbasis, still is the gold standard to assess esopha-geal function. The electrodes should be as thin aspossible. Glass or antimony electrodes are intro-duced through the nose and pH values arerecorded continuously on a battery-operatedrecorder. At the end of the 24-h investigation,
the saved values are evaluated by means of suit-able software. One ideally uses multichannel pro-bes and measures pH levels in the stomach, thelower esophagus, and the upper esophagus. Fall-ing pH levels in the esophagus can be correlatedwith the pH of the stomach, and the number ofrefluxes that reach the esophagus are analyzed(Semeniuk and Kaczmarski 2007).
All drops in pH below 4 with a duration of atleast 15 s (number of refluxes), the time taken forpH levels to normalize or rise back to pH 4 (refluxclearance), the number of refluxes with clearancetime longer than 5 min, and the longest reflux timeare analyzed. The type and the ingestion time offood as well as the length of time the person lies insupine position or is upright are also registered.Regrettably, laboratories use different cut-offvalues, which are partly influenced by standardvalues in adults (Table 2). The low threshold valueof 3% in infants largely fed with milk takes thebuffer effect of milk and the consequent lowernumbers of acid refluxes (accompanied by a pHdrop to below 4) into account.
There is no doubt of the fact that 24-h pH-monitoring still is the most frequently usedmethod to detect acid reflux. The weakness ofthe method, however, is that it does not demon-strate refluxes with neutral pH or mildly alkalinerefluxes accompanied by a rise in pH.
Combined Impedance Measurement/pH-Monitoring
This 24-h multichannel method of impedancemeasurement combined with pH-monitoring(pH/MII), by which voltage variations during dis-tension of the esophagus are recorded at multiplerecording points, does not merely show the pH ofrefluxes but also the direction of the bolus. Thus, itpermits measurement not only of acid refluxes butof all neutral and alkaline refluxes over a period of24 h (Fig. 7). Thus, the informative value isgreatly enhanced compared to simple pH-moni-toring (Vandenplas et al. 2007; Fukahori et al.2013; Wenzel et al. 2012). The combined MII/pH monitoring is clearly superior to pH-monitor-ing alone, especially because in young infants,
Fig. 6 Common cavity phenomenon with reflux in theupper esophagus and pH drop <3. Normalization of thepH in the esophagus after and acid reflux occurs onlystepwise by swallowing saliva (acid clearance)
Gastroesophageal Reflux and Hiatal Hernia 7

symptoms are more frequently associated withweakly acidic or neutral refluxes. In one recentstudy, acid-related parameters were significantlyrelated to MII baselines, although they did notcorrelate exactly with the endoscopic findings(van der Pol et al. 2013). However, the results ofthis study might have been influenced by thedifficult macroscopic estimation of a grade ofesophagitis, especially with lower grades. Recur-rent cough due to microaspiration of nonacidicrefluxes may play a significant role in respiratorytract infection and is a diagnostic domain of pH/MII (Blondeau et al. 2011). Furthermore, MII/pHresults have an influence on the choice of medicaltreatment since it is possible to discriminatepatients with primarily acid refluxes from thosewith nonacid refluxes needing a differentneuromodular therapy (Jodorkovsky et al. 2014).Therefore, combined impedance measurement
and pH-monitoring will probably soon replacepure pH-monitoring as the gold standard.
Manometry
Manometric investigation of esophageal functionwas a diagnostic method introduced in the late1960s, primarily to record the pressure in theLES. The general assumption at that time wasthat primarily a low LES pressure is the responsi-ble factor to allow reflux. Initial manometricinvestigations in newborns and infants appearedto confirm that the LES pressure in this age groupis extremely low. However, only when low-com-pliance perfusion pumps have been introduced,investigators were able to register relevant pres-sures values. As mentioned earlier, investigationsin the 1970s already showed that normal LESpressures are present in neonates and infants
Table 2 Cut-off values: the lower pH% value in children under 1 year of age is the result of the fact the gastric acidity isneutralized in infants who are mainly fed with milk products (see also Fig. 7) (Höllwarth 2009)
pH<4 in % Low grade % Intermediate % High grade %
<1a 3–5 5–7 >7
>1a 5–7 7–10 >10
Fig. 7 Combinedimpedance and pH-monitoring. It shows a shortreflux episode with adecrease of the pH in theesophagus and a smallincrease of the pH with thenext swallow (Höllwarth2009)
8 M. E. Höllwarth and E. Sorantin

(Höllwarth 1979). Furthermore, manometry ishighly suitable to analyze the motor functionsand peristalsis of the esophagus. Due to the lon-gitudinal contraction of the esophagus duringperistalsis, special sleeve devices have beendeveloped for sphincter pressure measurement(Dent 1976). Manometry shows that reflux ofgastric contents is rendered possible not due tolow pressures but due to spontaneous transientrelaxations of the LES. These occur much moreoften in patients with GERD and persist for asignificantly longer time. These relaxations ofthe LES are the so-called “common cavity phe-nomenon” (CCP), because the manometry trac-ings in the thoracic esophagus are of theabdominal type and return to normal only after asecondary peristalsis and closure of the LES (Fig.4) (Butterfield et al. 1972). The refluxed volume isreturned to the stomach by secondary peristalsis,whereas the drop in pH is normalized in a step-wise manner by swallowing saliva. SimultaneouspH-monitoring permits demonstration of the pHof refluxes being nonacidic, neutral, or alkaline.Thus manometry allows the investigator to drawconclusions similar to those obtained by imped-ance measurement. However, the drawback ofmanometry is the fact that, in contrast to pH-monitoring and impedance investigation, it ismotion dependent. It requires calm conditions.Therefore, it is not a suitable method for 24-hexaminations.
Endoscopy and Histology
Investigations with flexible fiberoptic endoscopesare part of the standard investigation of refluxdisease. The device is introduced into the esoph-agus under direct vision, usually down to theduodenum. Biopsy specimens are taken from theduodenum and the antrum of the stomach. In thestomach, the tip of the device is inverted to viewthe esophagogastric junction from below. In nor-mal cases, the device is closely encircled by theesophagus. At the lateral circumference, one seesthe flap valve mentioned above (Fig. 1). In con-trast, in a hiatal hernia, the diaphragmatic pinch isa little open and one obtains a clear upward view
towards the higher positioned LES. By withdraw-ing the device further, one is able to inspect theesophagogastric junction and the Z-line with thecardia monolayer epithelium more closely. Thetypical esophageal squamous epithelium issmooth and of milky red color (Grade 0).According to Savary-Miller, the grades in thepresence of esophagitis are: Grade 1: single ero-sion or exudative lesion on only one longitudinalfold; Grade 2: multiple erosions on more than onelongitudinal fold; Grade 3: circular erosion orexudative lesion; Grade 4: ulcers, strictures, orshort esophagus; and Grade 5: Barrett’ epithelium(Ollyo et al. 1986). The more sophisticated LosAngeles Classification of the severity of refluxesophagitis can also be used in children; itdescribes four grades of mucosal damage,depending on the extension between mucosalfolds (Genta et al. 2011).
It must be emphasized that the macroscopicgrading, especially with exudative lesions of theGrades 1 and 2, is affected by the impression ofthe observer and does often not well correlate withthe histological results. Therefore, it is mandatoryto take several biopsy specimens, starting 1–2 cmproximal to the Z-line and extending upward intothe upper esophagus. It is advisable to place thebiopsy specimens on a piece of cork, in appropri-ate direction, immediately after taking the speci-men, and then inserting it in formalin. An optimalspecimen consists of the entire layer of epithe-lium, including the basal cell layer. Thickeningof the basal layer and relative elongation of thepapilla (due to a thinner epithelial zone) areregarded as signs of greater cell turnover andpathological reflux. Evidence of intraepithelialeosinophils then confirms the presence of evidentesophagitis, even in the absence of correspondingsymptoms (Sherman et al. 2009). Erosions andulcerations are, by their very nature, signs ofsevere chronic esophagitis. However, the latter isnot always associated with unequivocal symp-toms in children. The presence of more than 20eosinophils per “high-power” field, on the otherhand, is a sign of another non-reflux-related aller-gic or atopic disease, i.e., so-called eosinophilicesophagitis (Furuta et al. 2007).
Gastroesophageal Reflux and Hiatal Hernia 9

Diagnostic Nuclear MedicineInvestigations
Scintigraphic investigation methods permit obser-vation of the moving bolus through the esopha-gus, any aspiration of tracer into the lungs due toreflux, and measurement of gastric emptying timeafter standardized meals. The latter consist of asolid and a liquid portion, such as a mealconsisting of egg and water. 99mTc sulfur colloidis used as tracer. The act of swallowing is visual-ized on dynamic sequences. After setting regionsof interest (ROI), refluxes are registered and themean gastric emptying rate is documented on atime/activity curve. Investigations after 24 h per-mit the detection of tracer in the lung, providedaspiration has occurred.
Development of Esophageal Functionin Childhood
Minimal spitting, flaccid flow, or vomiting of milk– as signs of frequent gastroesophageal reflux –are observed in approximately one-half of allnewborns and young infants and are rightlydeemed normal if the child’s development is oth-erwise uneventful and satisfying. As fluids causefrequent episodes of reflux even in adults, it is nosurprise that the largely liquid diet in this phase oflife may give rise to frequent reflux. The child’ssubsequent development shows usually that thesesymptoms become rare after the first 4–6 monthsand are no longer observed at the end of12 months. Switching to pulpy and later solidfood obviously plays an important role in thisdevelopment.
As mentioned above, previously it was believedthat frequent reflux in this early phase of life iscaused by the absence or a very low tonus in theLES, and when these structures mature as the childdevelops, the enhanced LES tonus prevents reflux.In contrast, newborns and preterm infants havenormal pressures (similar to those in adults) in theLES, and that reflux in this age group is not causedby the absence of tonus in the LES but by toofrequent and prolonged transient relaxations in theLES (Höllwarth et al. 1986). As those frequent
LES relaxations are often associated with a delayof normal propulsive peristalsis in the esophagus,reflux in this age group has been regarded as theconsequence of a central delay in the developmentof motor coordination of the esophagus. An espe-cially high incidence of reflux in infants with cen-tral apnea also indicates that immature centralregulatory structures are responsible for frequenttransient relaxations in this setting (Landler et al.1990).
Most infants experience an abatement of typi-cal symptoms of reflux by the end of 12 monthsand also experience effective normalization ofesophageal function as confirmed by 24-h pH-monitoring (Orenstein et al. 2006). However, theresolution of the clinical symptoms of refluxaround the age of 1 year is not necessarily a signof better function and spontaneous normalizationof function may occur at the much later age of3–5 years, evidenced by long-term follow-up pH-monitoring (Pesendorfer et al. 1993). The prob-lem is that clinical signs of reflux after the age of1 year are rare and mild and are therefore notgiven attention until several years later, when thelate sequel of chronic pathological reflux becomeevident. Recent investigations in adults haveshown that about one-half of young adults withGERD had marked symptoms in childhood (Mar-tin et al. 2002; Gold 2006; El-Serag et al. 2007).
Pathological Reflux and Symptoms
Gastroesophageal reflux disease (GERD) in chil-dren is different in several aspects from adults. In2009, an International Consensus was publishedon the definition of GERD in the pediatric popu-lation (Sherman et al. 2009). The symptoms ofGERD depend on the patient’s age.
Newborns and Infants
In newborns and infants, reflux is a commonphenomenon as long as they are fed mainly withliquid food. A moist pillow is a typical sign thatreflux reached the mouth. However, GERD has tobe suspected when the infant fails to thrive,
10 M. E. Höllwarth and E. Sorantin

experiences recurrent respiratory infection due tomicroaspiration, shows greater irritability, rest-lessness, especially restless sleep interspersed bywake-up phases or screams, and near-miss suddeninfant death events (Vandenplas et al. 2009; Slo-cum et al. 2007). Feeding difficulties, which fre-quently accompany this condition, may disturbthe interaction between mother and child(Mathisen et al. 1999). Recurrent vomiting orregurgitation of food causes malnutrition andinsufficient weight gain. Histologic evidence ofesophagitis is rare at this age because the infant islargely fed on milk and gastric acid is sufficientlybuffered over a period of 1–2 h after the meal(Fig. 8).
Childhood
Spitting and vomiting are common signs of refluxbut become increasingly rare after the infantileage. This may mimic normalization of function.Typical symptoms include recurrent pain in theupper abdomen, but retrosternal burning, such asthat known in adults, is very rare in children.Intolerance of acid or sweet food, a sour mouthodor, gurgling sounds in the chest after eating,
recurrent respiratory tract infection, and hoarse-ness are further characteristic symptoms (Changet al. 2006; Semeniuk and Kaczmarski 2007).Asthmatic symptoms may also be caused bychronic microaspiration. A very rare but charac-teristic symptom of reflux is the Sandifer syn-drome, which is accompanied by recurrent tic-like sideways inclination of the head to the left;this may be interpreted as support of passive pre-vention of reflux (Lee et al. 1999).
The primary complication of gastroesophagealreflux is esophagitis, which is caused by frequentand excessively long relaxations of the LES withchronic acid exposure of the esophagus. Theresulting inflammation leads to microhemorrhageof mucous membranes and, in chronic cases, hem-orrhagic anemia. A significant aspect of the sub-sequent course of the disease is the fact thatinflammation of the esophagus sets a vicious cir-cle into motion, characterized by a disturbance ofsecondary peristalsis and consequent prolonga-tion of acid clearance. Furthermore, the inflamma-tion causes more numerous relaxations of the LESdue to reflux. Subsequently the inflammationspreads to deeper layers of the wall, eventuallyleading to stenosis because of simultaneous scarformation (Fig. 9). The symptoms of evident
Fig. 8 Combined manometric study and pH-monitoringafter a typical milk meal in a 4-month-old child. The linesindicate reflux episodes of different duration. The result
shows that refluxes are accompanied by a pH decrease only90 min after feeding (CCP = common cavityphenomenon)
Gastroesophageal Reflux and Hiatal Hernia 11

esophagitis in children include, in addition torecurrent pain in the upper abdomen, frequentbouts of vomiting partly tinged with blood.Chronic blood loss might lead to anemia, and thepresence of a significant stenosis can causeswallowing difficulties and regurgitation of food.
Such grave complications are rare at the pre-sent time; however, it should be noted that chil-dren with mental disabilities constitute anexception. Grave sequelae of reflux are often dis-covered late in these children because the patientsare unable to articulate their difficulties. Investi-gations have shown that the symptom of auto-aggression may be an important sign of painfulesophagitis in these children and should always betaken as a reason to investigate the presence ofreflux (Gössler et al. 2007).
Treatment of GERD
Pathological reflux may be treated by conserva-tive means or surgery. Conservative therapy ismainly considered in infants and young children,because the probability of spontaneous normali-zation of reflux is very high. Conservative treat-ment is also indicated if one wishes to gain timeand when a severe esophagitis or reflux-relatedstenosis has to be treated before a planned opera-tion. Furthermore, it is used in those rare patientswho are unable to undergo surgery.
Conservative Therapy
In InfantsAt this age, a pathological reflux is believed toexist when the child has recurrent bouts ofvomiting and fails to thrive, cannot be fed orally,experiences recurrent respiratory tract infectionand/or pain, restlessness at night, or reflux-relatednear-miss attacks. As the risk of esophagitis isvery low at this age, one may well dispense withan endoscopic investigation in the absence ofspecific indications. However, in addition to 24-h pH-monitoring or impedance investigation, anX-ray of the esophagus (and ultrasound investiga-tion of the pylorus) will be necessary to exclude
any pathology that may hinder spontaneoushealing of the reflux, such as hiatus hernia,organo-axial gastric volvulus, gastric outlet steno-sis, or hypertrophic pyloric stenosis.
Investigations have shown that lying in proneposition, possibly with a raised torso, preventsreflux most effectively. However, it also involvesa much greater risk of sudden infant death due tovomiting in sleep and apnea events. Therefore, thesupine position with a raised torso and frequentmeals with lesser quantities of food and thicken-ing the food with rice gruel is generallyrecommended (Carroll et al. 2002; Corvaglia etal. 2007; Horvath et al. 2008). In most cases, thesymptoms abate within the next few months.
Fig. 9 Esophageal stenosis due to chronic reflux withesophagitis
12 M. E. Höllwarth and E. Sorantin

Some food manufacturers offer special formulamilk to prevent reflux.
At the end of 12 months, control pH-monitor-ing should be performed even after the symptomshave apparently returned to normal, in order torule out the persistence of a pathological refluxpattern. As mentioned earlier, due to altered foodhabits, the reflux may rarely reach the mouth andtherefore remain invisible, thus mimicking theresolution of reflux. For the same reason, parents’compliance with prescribed control investigationsis usually poor. Just about 10% of children stillhave marked symptoms of reflux and require, inaddition to treatment, follow-up controls everyyear. Spontaneous normalization of esophagealfunction may occur between the age of 4 and5 years but cannot be expected to occur after thistime (Pesendorfer et al. 1993).
In Older ChildrenAs the child’s food starts to resemble that ofadults, there is an increasing quantity of acidsecretion from the stomach after meals. Therefore,the majority of postprandial refluxes are nowaccompanied by a pH reduction to below 4 and,in cases of GERD, the possibility of esophagitis isincreased. In addition to esophageal passage onX-rays and pH-monitoring/impedance measure-ment, a comprehensive investigation must includeendoscopy and biopsy. Long-term conservativetreatment is meaningful only when spontaneousnormalization is anticipated. However, spontane-ous healing, even in small babies, is unlikely tooccur after esophageal atresia, diaphragmatic her-nia, as well as in patients with severe mentaldisabilities. Thus, conservative maintenance ther-apy is advisable only in a few exceptional cases ofthese types. When no esophagitis is seen onbiopsy, a suitable diet may be sufficient – suchas avoiding acidic and sweet food or other foodscausing reflux (coffee, tea, soft drinks), taking lessfluids in the evening – and mucosal protection (e.g., Ulsal or Gaviscon). Nonacidic reflux episodesmay still occur and may lead to aspiration andchronic respiratory infection particularly insleep. Therefore, impedance measurement is anexcellent measure to determine the extent of non-acidic reflux in these patients.
In the presence of esophagitis, preoperativelythe patient should always be given drug-basedreflux treatment. In reflux-related esophageal ste-nosis, it is advisable to perform bougienage undertreatment with antacids until the condition hasnormalized. Surgery should be planned afterthese measures have been performed and thepatient’s local condition has been stabilized. Pre-operatively, the successful treatment of the steno-sis should be verified by performing esophagealbarium investigation in order to avoid postopera-tive bougienage.
Drug Therapy
The aim of drug therapy is to reduce acid exposureof the esophagus and thus avoid or treat esopha-gitis. A distinction should be made here betweendrugs that protect the mucosal surface and thosethat reduce or hinder the production of gastricjuices. Sucralfate is an aluminum complex in theform of a gel and belongs to the former group. Itimproves the symptoms of esophagitis andreduces signs of inflammation. The latter groupsof drugs that block the production of gastric juicesinclude H2 receptor antagonists or proton pumpinhibitors (PPI).
H2 receptor antagonists reduce acid secretionby blocking the H2 receptor on the surface ofparietal cells in the stomach but might fail in thepresence of gastric juice secretion induced bymeals (Donnellan et al. 2004). Thus, today theefficacy of H2 receptor antagonists is consideredto not be as effective as proton pump inhibitortherapy in GERD children (Ummarino et al.2012).
Proton pump inhibitors inhibit H+/K+-ATpasein parietal cells. Omeprazole and lanzoprazole areapproved for children (Rudolph 2003; Castellaniet al. 2014). The latter drug may even be admin-istered during the first 12 months. However, long-term treatment with PPI is associated with a higherrisk of gastrointestinal infection because it inhibitsgastric acids (Berni Canani and Terrin 2010; Loand Chan 2013).
Infants: Most milk-fed infants do not requiredrug-based treatment of reflux. However, if
Gastroesophageal Reflux and Hiatal Hernia 13

recurrent unquietness, disturbed sleep, and painare the symptoms, PPI therapy is indicated. Stud-ies in infants <1 year of age with pain-relatedsymptoms have shown that PPI reduced the num-ber of acid refluxes significantly but does notreduce the total number of refluxes (Castellani etal. 2014). Thus, respiratory tract-related symp-toms due to recurrent aspiration during sleepmay still be present. Further exceptions are infantsin which the peristalsis of the esophagus is mas-sively disturbed and acid or volume clearancetakes a very long time. This occurs in childrenwho have undergone surgery for esophageal atre-sia, especially when the lower segment had to bemobilized extensively, in children who have expe-rienced diaphragmatic hernia, those with anincompetent esophagogastric junction, as well aschildren with severe mental disorders.
Children frequently require a much higher PPIdose compared to adults (1–2 mg/kg BW). Theefficacy of gastric acid blockade must be checkedby performing pH-monitoring about 2 weeks afterthe start of therapy, as the dose may need to bemodified significantly in individual cases. Inves-tigations after long-term treatment with protonpump inhibitors in adults revealed a 30% reduc-tion in vitamin B12 levels, atrophic gastritis, andseveral weeks of acid hypersecretion after discon-tinuation of the medication. As mentioned earlier,long-term therapy with acid inhibitors in childrenis indicated only in exceptional cases, althoughpositive results have been reported in thepublished literature in this regard (Hassall et al.2007; Tolia and Boyer 2008).
Baclofen, a gamma-aminobutyric acid receptoragonist (GABA), is a new and promising thera-peutic option is the pharmacologic inhibition oftransient sphincter relaxations (Lidums et al.2000). Recent experience with baclofen in adultsand children with GERD has demonstrated a sig-nificant reduction of LES relaxations and reflux(Zhang et al. 2002; Omari et al. 2006). Baclofenreduced significantly upright refluxes as well asbelching and regurgitation in adult patients(Cossentino et al. 2012). In children with refrac-tory reflux, baclofen together with PPI signifi-cantly reduced the clinical symptoms in two-thirds of patients (Vadlamudi et al. 2013). Adverse
side effects may be drowsiness, dizziness, andfatigue.
Prokinetic drugs were used in the past toimprove peristalsis and cleansing functions ofthe esophagus. However, experience has shownthat none of these drugs (metoclopramide, cis-apride, bethanechol) had a confirmed reflux-pre-ventive effect, and the side effects maysuperimpose any positive effects. Therefore, cur-rently there are little or no indications for the useof these drugs in reflux disease (Augood et al.2003; Vandenplas et al. 2009).
Surgical Treatment
Fundoplication
The strategic principles of surgical reflux treat-ment are based on the creation of an intra-abdom-inal portion of the esophagus and complete(Nissen) or partial plication (dorsally Toupet, ven-trally Thal) of the gastric fundus around theesophagus (Nissen 1956; Toupet 1963; Thal etal. 1965). The first step requires removal of theesophagus from the hiatus in order to obtain alonger intra-abdominal portion. Therefore,approximating the crura with one or two suturesmay be required additionally to reduce the risk ofwrap herniation into the thorax. The selection offundoplication depends on the surgeon’s choice.Favorable results have been achieved with allthree methods. The current standard is laparo-scopic surgery or robot-assisted laparoscopicfundoplication (Binet et al. 2019). Whenperforming a Nissen fundoplication, the gastricfundus should be closed very loosely in circularfashion around the esophagus with just 2–3sutures so that passage is not hindered and spon-taneous vomiting is still permitted (Georgeson2006). Tovar has convincingly shown thatfundoplication with a floppy wrap is a powerfulmeans of controlling reflux in appropriatelyselected children in whom medical treatmentfails, or in symptomatic patients with specificcomorbidities such as neurologic disorders orcongenital anomalies (Tovar et al. 2007). System-atic reviews of randomized controlled trials of
14 M. E. Höllwarth and E. Sorantin

laparoscopic versus open fundoplication showeda significant lower operative morbidity, shorterpostoperative stays and a less prolonged sickleave following the endoscopic approach (Strateet al. 2008). In a randomized multicenter trial witha 5-year follow-up, antireflux surgery was moreeffective than omeprazole with respect to failurerates. However, when the dose of omeprazole wasadjusted in case of recurrent symptoms, the failurerate still revealed the superiority of surgery but thedifference was not significant (Lundell et al.2001).
The highest population-based procedure rate inthe United States (45%) was performed in infantsyounger than the age of 1 year (Lasser et al. 2006).Given the option of spontaneous maturation ofesophageal function in infants younger than theage of 1 year, concerns have been expressed aboutthe necessity of antireflux procedures. Hassaldiscussed failure rates and results offundoplication in children and recommended sur-gery only in selected patients (Hassall 2005).
Complications of Fundoplication
Fortunately, the mortality rate is low (<1%) butimmediate postoperative morbidity is around5–20% with laparoscopic surgery (Richter2013). Early complications include perforation,bleeding, and pneumothorax (Peery et al. 2012).The most common complication is recurrent
reflux with an incidence as high as 10–15% andoccurs with all three surgical procedures (Table 3)and is associated with a higher perioperative risk(Kahrilas et al. 2008). This complication is partlyrelated to natural motions in this region due to themotility of the diaphragm during respiration andbecause the esophagus is shortened during everyact of swallowing for about 5 cm in adults (Doddset al. 1974). Further known risk factors for recur-rent reflux are being aged below 6 years, thepresence of hiatus hernia, and mental disabilitiesaccompanied by frequent choking, belching,rumination and preoperative dystrophy; thesephenomena are frequently observed in childrenwith mental disabilities (Ngerncham et al. 2007).Therefore, children with mental disabilities andmarked catabolism should be fed additionallywith parenteral calories until they clearly have ananabolic metabolism (Weber 1995). Epilepsy isnot an additional risk factor for recurrent reflux inmentally disabled patients (Goessler et al. 2006;Vernon-Roberts and Sullivan 2007). Furthercauses of recurrences are inadequate closure ofthe diaphragmatic crura, short esophagus, or inad-equate mobilization of the esophagus. Commonlate complications are gas-bloat syndrome, mostlyas a consequence of the smaller gastric volume,dysphagia, postoperative pain, and diarrhea.However, most of the problems resolve spontane-ously after a few months. After a Nissenfundoplication, a temporary inability to vomitmay occur. This complication is rare after the
Table 3 Significant rate of complications is reported in the literature after long-term follow-up of surgically treatedpatients (Höllwarth 2009)
Author/year n Method Recurr. % Dysphagia % Gas bloat % Other %
Fonkalsrud 1998 7467 Nis/Thal/Toupet 7.1 – 3.6 7.0
v.d.Zee 2002 149 Endosc. Thal 5.4 – – 19.4
Pessaux 2000 1470 Nis/NisRo/Toupet 1.1 0.35 – 1.3
Zaninotto 2000 621 Nis/NisRo/Toupet 8.5 26 14.7 –
Lafullarde 2001 176 Endosc. Nis 1.7 3.9 – 7.3
Esposito 2000 289 NisRo/Toupet 2.1 1.0 – 2.4
Holzinger 2001 100 Toupet 3.0 5.0 – –
Kimber 1998 66 Nis/Thal 39.3 3.0 10.6 50.0
Subramiam 2000 109 Nis/Boix 20.0 3.0 2.0 –
Gilger 2004 178 Nis/Boix 18.0 22.7 – –
Diaz 2005 456 Nis (endo+open) 12.1 – – –
Gastroesophageal Reflux and Hiatal Hernia 15

Toupet procedure, during which the fundus isplaced about 270� dorsally around the esophagus,as well as after the Thal procedure.
Other Surgical Methods
A rarely used method is Collis gastroplasty, dur-ing which the fundus is separated parallel to theesophagus in the angle of His by using a stapler,and the fundoplicate is then fixed to a kind ofelongated esophagus either by the Nissen or theToupet/Thal procedure. The procedure is mainlyused in cases of primary or secondary short esoph-agus (esophageal atresia or chronic esophagitis) toelongate the distance and perform thefundoplication within the abdomen (Nakahara etal. 2012).
A number of new technical methods have beenintroduced in the last few years for the treatmentof reflux in adults. However, there is a lack ofsufficient experience regarding the use of thesemethods in children (Katz 2002). Using onemethod, a type of mucosal fold is created in thecardia using a special endoscopic intraluminalstapler (EsophyX system); the fold is supposedto prevent reflux (Bell and Cardiere 2011; Chen etal. 2012). A further endoscopic method that wasused successfully in children is the so-calledStretta procedure, by which predefined thermaldamage is applied in the cardia by the use ofradio waves (Liu et al. 2005). Finally, a thirdtechnique is used: similar to injection for avesicoureteral reflux, endoscopic submucosalimplants are injected into the cardia (Enteryx) toprevent reflux (Johnson et al. 2003). Long-termexperience with these methods is lacking, and thecurrent data do not favor the use of these tech-niques (Pandolfino and Krishnan 2014).
A new, not endoscopic, technique which hasraised interest is the LINX device by which a ringof magnetic beads is placed around the esophagusduring laparoscopy (Ganz et al. 2013). Anothernon-endoscopic innovation is the implantation ofan electrical LES stimulator which is supposed toimprove the LES pressure (Rodriguez et al. 2013).
In children with mental disabilities, one shouldalways try to create conditions for oral (although
modest) nutrition. In the case of insufficient intakeof food, the fundoplication should be combinedwith a gastrostomy button so that food may besupplemented via gastrostomy. In cases of severemental disability, the patient may occasionallydevelop numerous recurrent refluxes due to exten-sive rumination. In order to preserve the option oforal feeding, it would be advisable to perform theesophagogastric dissection procedure describedby Bianchi (1997) in these patients. The stomachis severed from the esophagus and closed. Anesophagojejunostomy (as a Roux loop) is createdto preserve continuity. Thus, food taken orallyreaches the jejunum directly, and recurrentrefluxes or rumination are rendered impossible(Morabito et al. 2006).
Barrett’s Esophagus
Barrett’s esophagus is a rare complication of gas-troesophageal reflux, associated with chronicesophagitis. Raicevic and Saxena performed asystematic review of Barrett’s esophagus in chil-dren and reported that Barrett’s esophagus wasassociated with gastroesophageal reflux in 77%of patients and 10% of patients with esophagealatresia and reflux (Raicevic and Saxena 2018). Itshistological feature is replacement of the layeredsquamous epithelium of the esophagus by themetaplastic cylindrical epithelium either fromthe cardia or the intestinal tract. Therefore, a dis-tinction is made between two forms:
(a) The harmless type of metaplastic cylindricalepithelium of the cardia
(b) The problematic type, involving intestinalmetaplasia with goblet cells, associated withhigher risk of carcinoma
One explanation for the presence of cylindricalcardia-type epithelium in the esophagus is that theacid-resistant epithelium of the cardia grows morerapidly than the squamous epithelium destroyedby inflammation. Therefore, metaplasia of thecylindrical epithelium is quite frequently locatedin the close distal aspect of a stenosis caused byesophagitis and extends all the way down to the
16 M. E. Höllwarth and E. Sorantin

cardia. This condition is also referred to as anendobrachyesophagus. In contrast to the veryrare condition of a genuine brachyesophagus, inwhich the esophagus is effectively too short andthe LES lies in the chest, in an endo-brachyesophagus the cardia is in the normal ana-tomic position but the mucosa of the cardiaextends far upwards.
Intestinal metaplasia indicates the presence ofa duodenogastroesophageal reflux and intestinalepithelium has replaced the squamous epitheliumof the esophagus. In the strict sense of the term,only the second type is known as Barrett’s esoph-agus (Fig. 10). Untreated reflux of long durationin children with mental disability, esophagealatresia, chronic lung disease, or chemotherapymay lead to Barrett’s esophagus in 13% of cases(Hassall 1993).
Diagnosis: On endoscopy, one finds a ratherflesh-colored, slightly bleeding mucosa withirregular mucosal changes. These may be insularin shape or may cover wide areas in circularfashion. By injecting Lugol’s solution or indigocarmine solution, the mucosal changes can beseen better and biopsied more accurately. Thehistological investigation permits differentiationof the more harmless condition of metaplasticcardiac epithelium from intestinal metaplasiawith typical goblet cells. In cases of proven intes-tinal metaplasia, one must obtain four-quadrantbiopsy specimens at intervals of 2 cm along theesophagus (Abrams et al. 2009). The risk of
subsequent carcinoma in situ or adenocarcinomais 30- to 125-fold higher than it is in the normalpopulation. However, the interval until the occur-rence of carcinoma is 15–30 years. Amongpatients with Barrett’s esophagus, approximately2% will die within 10 years; however, patients diemore frequently from other diseases (Solayamani-Dodaran et al. 2013). Therefore, adenocarcinomaafter Barrett’s esophagus is rare in children; how-ever, individuals born preterm or small for gesta-tional age have a threefold increased risk fordeveloping Barrett’s esophagus as adults (Forsellet al. 2013).
The guidelines suggested by the AmericanCollege of Gastroenterology (Sampliner 1998)for Barrett’s esophagus (intestinal metaplasia) rec-ommend the following monitoring strategy:
(a) In case of dysplasia not demonstrated on twooccasions: control endoscopies every2–3 years
(b) In case of low-grade dysplasia demonstratedon two occasions: control endoscopies everyyear
(c) In case of high-grade dysplasia: selectiveresection or control endoscopies at 3-monthintervals
Recent consensus statement for managementof Barrett’s dysplasia and early-stage esophagealadenocarcinoma have been published (Bennett etal. 2012).
Therapy: Treatment of Barrett’s esophagus isidentical to that of chronic reflux: drug-based acidblockade and bougienage of the esophagus untilthe elimination of any stenosis that may be pre-sent, followed by fundoplication (Rees et al.2010). The presence of high-grade dysplasia oradenocarcinoma is rare in children and has beenreported only in a few isolated cases. Radio-frequency ablation is highly effective and safefor treatment of Barrett’s esophagus with dyspla-sia or early stage cancer. Continuous surveillanceis needed since a third of the patients have arecurrence within 2 years but that can again betreated endoscopically (Gupta et al. 2013;Bulsiewicz et al. 2013).Fig. 10 Histologic specimen of a Barrett’s esophagus
with intestinal metaplasia (Höllwarth 2009)
Gastroesophageal Reflux and Hiatal Hernia 17

Associated Diseases
Laryngopharyngeal Reflux
Gastroesophageal reflux is frequently reported tobe associated with laryngeal symptoms such ashoarseness, irritation of the throat, a globus sen-sation, or dysphagia. This condition is referred toas a laryngopharyngeal reflux. Reddening, ulcer-ation, or pseudopolyps on the vocal cords (Fig.11) are typical changes assigned to this conditionin cases of positive evidence of reflux. By nature,this condition is also associated with chronicmicroaspiration. In terms of differential diagnosis,other causes such as allergic diseases, smoking,injury, etc. should be ruled out. In terms of ther-apy, it would be advisable to first attempt treat-ment with PPI for 1–2 months. When thesymptom or the laryngeal condition is markedlyimproved by this measure, one may assume thatthe condition is caused be reflux. In the absence ofimprovement, the clinician must investigate fur-ther differential diagnostic options (Vaezi 2007).
Reflux-Associated Respiratory TractInfection
Reflux-associated respiratory tract infection andpneumonia may be caused by the aspiration ofacid or even nonacidic reflux (Chang et al.2006). Therefore, inquiring about this symptom
when recording a patient’s medical history is alsoimportant in children without esophagitis. Interms of differential diagnosis, other causes suchas cystic fibrosis, aspirated foreign body,malformations of the respiratory tract or thelungs should be ruled out. In patients with mentaldisabilities, recurrent respiratory tract infectionmay also be caused by disruption of pharyngoe-sophageal transport – the act of deglutition – inaddition to reflux.
The diagnosis is not easy to establish, exceptwhen aspiration is clearly seen on radiologicalinvestigation with contrast medium. Neitherbronchoalveolar lavage nor nuclear medicineinvestigations are unequivocal. On lavage, oneassesses the fat content of 100 macrophages, butthere is a wide overlap with normal controls. Anegative scintigraphic test does not rule out aspi-ration because no aspiration may have occurredspecifically during the investigation. Finally, noneof the methods provides unequivocal informationas to whether the suspected aspiration occurredduring the act of swallowing or due to reflux.
Recently, it has been shown that 24-h pH/MIImay be helpful in diagnosing reflux-associatedaspiration as a cause of chronic unexplainedcough in children (Blondeau et al. 2011). It allowsdistinguishing between acidic and nonacidicrefluxes. Both of them may be independentlyresponsible for recurrent aspiration and chroniccough. Although PPI therapy is the standard treat-ment, the chronic cough may persist due to thecontinuous aspiration of nonacidic reflux. Addi-tion of baclofen to the PPI therapy has been shownto improve the chronic cough significantly inmore than half of the patients (Xu et al. 2013).
Reflux and Asthma
Symptoms of GERD are frequently seen inasthma, but the true incidence of reflux in asth-matic children is not known (Khoshoo et al. 2003;Semeniuk and Kaczmarski 2007; Sopo et al.2009). Investigations on this subject have shownthat 25–75% of children with asthma actuallyhave a pathological reflux, but only 50% of themhave corresponding symptoms such as belching,
Fig. 11 Typical laryngeal polyp due to chronic reflux upto the pharynx/larynx
18 M. E. Höllwarth and E. Sorantin

vomiting, or pain in the upper abdomen. There-fore, even in asthmatic children without symp-toms of reflux, it would be advisable to perform24-h pH-monitoring. It is assumed that micro-aspiration and even acidification of the esophagusin asthmatics may trigger hyperreactivity of therespiratory tract. This also explains why drug-based reflux treatment reduces the symptoms ofasthma or causes the patient to require lower dosesof asthma therapy. In these patients, surgical treat-ment of reflux leads to clinically demonstrableimprovement of asthma symptoms in 85% ofcases (Field et al. 1999).
Reflux and Apnea Syndrome
Sudden infant death syndrome (SIDS) is the mostcommon cause of death in infants; its incidence isespecially high between the age of 2 and 4months.In the last few years, the association betweenSIDS and episodes of apnea on the one hand,and gastroesophageal reflux on the other, wasinvestigated. Diverse results were reported(Wenzl et al. 2001; Di Fiore et al. 2005; Slocumet al. 2007). Some authors demonstrated acidreflux as the cause of apnea episodes whereasothers were unable to show this association. Com-bined investigations consisting of manometry andpH-monitoring in infants with pathological sleepapnea showed frequent episodes of apnea andreflux but did not demonstrate acid refluxes asthe direct cause of apnea. Landler observed amarked delay in the growth and development ofthe motor functions of the esophagus in childrenwith “near-miss” events (Landler et al. 1990). In afurther study, it was found that infants with path-ological sleep apnea also have pathological refluxin many cases, whereas infants with primarily
pathological reflux do not experience episodes ofapnea to a remarkable extent (Table 4) (Kurz et al.1985). The investigation confirms the hypothesisthat infants with the sleep apnea syndrome (or so-called near miss events) suffer from underlyingdelayed regulatory function of the brainstem,because of which the higher centers responsiblefor esophageal motor function are also involved.On the other hand, delayed maturation of esoph-ageal motor functions is not necessarily associatedwith disorders of deeper respiratory regulationcenters. Thus, the rather frequent coincidence ofreflux and sleep apnea syndrome appears to becaused by underlying retarded maturation in bothcenters in the brainstem. In older children andadults, there is a strong evidence of a bidirectionalrelationship between GERD and sleep distur-bances, including sleep fragmentation and earlymorning awakenings (Fujiwara et al. 2013). PPItherapy in children with sleep apnea has beenshown to reduce the obstructive events signifi-cantly in some patients indicating a relationshipbetween apnea and reflux (Wasilewska et al.2012).
Eosinophilic Esophagitis
Eosinophilic esophagitis is a disease with increas-ing incidence and prevalence in children andadults affecting the esophagus by an eosinophilicinfiltration with symptoms similar to those ofreflux (Alterio et al. 2019). In children, the typicalsymptoms are refusal to eat, dysphagia, regurgi-tation of food, vomiting, and pain in the upperabdomen.With advancing age, the individual mayexperience other symptoms similar to reflux, suchas dystrophy and retrosternal pain (Dellon 2012).The cause is presumably an abnormal reaction to
Table 4 Infants with significant sleep apnea suffer oftenfrom GERD, too (*<0.05). In contrast, infants with GERDbut no sleep apneas have a normal respiration pattern
during sleep. That indicates that central sleep apneas arewithin the brainstem a complex dysfunction (Höllwarth2009)
n MA(s/min) LES-tone Reflux P:S
Controls 10 3.2 � 1.3 21.6 � 11.6 1 9.2 � 1.6
Infants with history of reflux 12 5.5 � 4.4 23.8 � 10.4 8 8.4 � 1.7
Infants with history of sleep apneas 21 13.7 � 7.9� 22.3 � 7.0 14 7.5 � 1.4
Gastroesophageal Reflux and Hiatal Hernia 19

food allergens in terms of cellular hyperreactivity(Gonsalves et al. 2012). Quite often, eosinophilicesophagitis occurs in combination with otheratopic diseases (Alterio et al. 2019).
The decisive aspect of differential diagnosisand its delineation from reflux disease are thefindings of a normal 24-h pH-monitoring and noresponse to treatment with acid blockers. X-rayinvestigation of esophageal passage reveals acircumscribed stenosis only in about 6% of chil-dren; in most cases, the stenosis does not requiredilatation. The endoscopic investigation fre-quently shows concentric rings of mucosa (similarto the trachea) and whitish, partly flaky exudates,thickened mucosal folds and, in distension of theesophagus, longitudinal folds over longer dis-tances. The diagnosis can be established when,in the presence of a normal 24-h pH-monitoring,the histological investigation shows more than 20eosinophils per “high-power” field (Furuta et al.2007). As regards therapy, foodstuffs identified asallergens on testing must be avoided. However,the symptoms improve only after 2–3 weeks inmany cases. Recommended drug therapiesinclude oral administration of methylpredniso-lone, inhaled corticosteroids, and recently alsoleukotriene receptor antagonists (Furuta et al.2007). 40% of children with eosinopholic esoph-agitis responded to proton pump inhibitor therapy(PPI), not dependend on the results of pH studies.Therefore, the beneficial use of PPI in childrenwith eosinophilic esophagitis needs further eval-uation (Dranove et al. 2009)
Hiatus Hernia
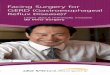
Any upward shift of portions of the stomach intoor beyond the esophageal hiatus is referred to as ahiatus hernia (HH). A distinction is made betweenaxial and para-esophageal hiatal hernias.
Axial Hiatus Hernia (Fig. 12)
On radiographs, the axial HH is either a slidingphenomenon or is fixed in the chest region. Asliding HH is much rarer in children than in
older adults (it occurs in approximately 60% ofadults). A fixed HH is occasionally seen in chil-dren with mental disability, reflux of long dura-tion, and esophagitis-related stenosis, as well asshortening of the esophagus due to scarring. Ininfants or young children with reflux disease andHH, the condition cannot be expected to resolvespontaneously. Therefore, conservative therapyhas no chances of success in this setting; surgeryis indicated in all cases.
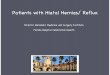
Para-esophageal Hiatal Hernia (Fig. 13)
Para-esophageal hernias are a common and typi-cal postoperative complication after fundoplica-tion. A part of the stomach slips through the hiatusinto the chest sideways, from the esophagogastricjunction located in normal position. This probablyoccurs due to failure of the hiatal pillar-sutures orfixation sutures of the stomach to the diaphragm.When a para-esophageal hernia is not combinedwith a pathological recurrent reflux and no furthersymptoms are present (such as a sensation ofpressure especially after meals as a sign of herni-ation), surgical correction is not required in everycase.
A congenital form of para-esophageal hernia isthe rare condition of an upside-down stomach in anewborn or infant. This is accompanied by moreor less complete displacement of the stomach intothe chest, with the esophagogastric junction innormal position.
Conclusion and Future Directions
Simple gastroesophageal reflux (GER) in earlyinfancy can be seen as a delay of the motor devel-opment of the esophagus with common and pro-longed lower esophageal sphincter relaxations.Spontaneous maturation occurs usually withinthe first year and conservative treatment is theappropriate therapy for most of the cases. In con-trast, chronic reflux leading to symptoms such asrecurrent spitting-up, vomiting and failure tothrive, and recurrent exposure of the esophagealmucosa to gastric acid is defined as
20 M. E. Höllwarth and E. Sorantin

gastroesophageal reflux disease (GERD). Esoph-agitis is common and replacement of the esopha-geal mucosa by gastric or intestinal epithelia maylead to Barrett’s esophagus. Conservative treat-ment with proton pump inhibitors is used to pre-vent acidic reflux. However, the number of refluxepisodes is usually not reduced and secondarysymptoms such as recurrent aspiration at night-time and respiratory infections are common.Babies with esophageal atresia, diaphragmatichernia, or severe cerebral retardation suffer oftenfrom severe reflux and surgical therapy is indi-cated in most of the patients. Fundoplication bylaparoscopy is today the best choice of treatmentfor GERD in children and adults. In recent years, anumber of endoscopic antireflux procedures havebeen proposed. Despite early promising results,
long-term quality does not withstand theestablished clinical efficacy of conservative treat-ment with PPI or fundoplication. Further technicalinnovations with implantable magnetic beads orlower esophageal sphincter stimulators are underinvestigation.
Cross-References
▶Congenital Diaphragmatic Hernia▶Esophageal Atresia▶ Innovations in Minimal Invasive Surgery▶ Principles of Minimal Invasive Surgery▶ Surgical Problems of Children with PhysicalDisabilities
Fig. 13 Para-esophageal hernia: radiological and endoscopic view
Fig. 12 Axial hiatal hernia: radiological and endoscopic view
Gastroesophageal Reflux and Hiatal Hernia 21

References
Abrams JA, Kapel RC, Lindberg GM, et al. Adherence tobiopsy guidelines for Barrett’s esophagus surveillancein the community setting in the United States. ClinGastroenterol Hepatol. 2009;7:736–42.
Alterio T, Cardile S, Trayers C, et al. Eosinophilic esoph-agitis in children: current knowledge to open new hori-zons. Scand J Gastroenterol. 2019;54(7):822–9.
Augood C, MacLennan S, Gilbert RE, et al. Cisapridetreatment for gastro-oesophageal reflux in children.Cochrane Database Syst Rev. 2003;4:1–19.
Bell RC, Cardiere GB. Transoral rotationalesophagogastric fundoplication: technical, anatomical,and safety considerations. Surg Endosc.2011;25:2387–99.
Bennett C, Vakil N, Bergman J, et al. Consensus statementsfor management of Barrett’s dysplasia and early-stageesophageal adenocarcinoma, based on a Delphi pro-cess. Gastroenterology. 2012;143:336–46.
Berni Canani RB, Terrin G. Gastric acidity inhibitors andthe risk of intestinal infections. Curr OpinGastroenterol. 2010;26:31–5.
Bianchi A. Total esophagogastric dissociation: an alterna-tive approach. J Pediatr Surg. 1997;32:1291–4.
Binet A, Fourcade L, Amar S, et al. Robot-assisted laparo-scopic fundoplications in pediatric surgery: experiencereview. Eur J Pediatr Surg. 2019;29(2):173–8.
Blondeau K, Mertens V, Dupont L, et al. The relationshipbetween gastroesophageal reflux and cough in childrenwith chronic unexplained cough using combinedimpedance-pH-manometry recordings. PediatrPulmonol. 2011;46:286–94.
Bulsiewicz WJ, Kim HP, Dellon ES, et al. Safety andefficacy of endoscopic mucosal therapy with radio-frequency ablation for patients with neoplastic Barrett’sesophagus. Clin Gastroenterol Hepatol.2013;11:636–42.
Butterfield DG, Struthers JE, Showalter BS. A test ofgastroesophageal sphincter competence. The commoncavity test. Am J Dig Dis. 1972;17:415–21.
Campanozzi A, Boccia G, Pensabene L, et al. Prevalenceand natural history of gastroesophageal reflux: pediat-ric prospective study. Pediatrics. 2009;123:779–83.
Carroll A, Garrison MM, Christakis DA. A systematicreview of nonpharmacological and nonsurgical thera-pies for gastroesophageal reflux in infants. Arch PediatrAdolesc Med. 2002;156:109–13.
Castellani C, Huber-Zeyringer A, Saxena AK, et al. Omep-razole for reflux in infants: effectiveness determined byimpedance-pH monitoring. Pediatr Surg Int.2014;30:381–5.
Chang AB, Lasserson TJ, Gaffney J, et al. Gastro-oesophageal reflux treatment for prolonged nonspecificcough in children and adults. Cochrane Database SystRev. 2006;4:1–46.
Chen S, Jarboe MD, Teitelbaum DH. Effectiveness of atransluminal endoscopic fundoplication for the
treatment of pediatric gastroesophageal reflux disease.Pediatr Surg Int. 2012;28:229–34.
Corvaglia L, Rotatori R, Ferlini M, et al. The effect of bodypositioning on gastroesophageal reflux in prematureinfants: evaluation by combined impedance and pHmonitoring. J Pediatr. 2007;151:591–6.
Cossentino MJ, Mann K, Armbruster SP, et al. Random-ized clinical trial: the effect of baclofen in patients withgastro-oesophageal reflux – a randomized prospectivestudy. Aliment Pharmacol Ther. 2012;35:1036–44.
Dellon ES. Diagnosis and management of eosinophilicesophagitis. Clin Gastroenterol Hepatol.2012;10:1066–78.
Dent J. A new technique for continuous sphincter pressuremeasurement. Gastroenterology. 1976;71:263–7.
Dent EL, Serag HB, Wallander MA, et al. Epidemiology ofgastro-oesophageal reflux disease: a systematic review.Gut. 2005;54:710–7.
Di Fiore JM, Arko M, Whitehouse M, et al. Apnea is notprolonged by acid gastroesophageal reflux in preterminfants. Pediatrics. 2005;116:1059–63.
Dodds WJ, Stewart ET, Hogan WJ, et al. Effect of esoph-ageal movement on intraluminal esophageal pressurerecording. Gastroenterology. 1974;67:592–600.
Donnellan C, Preston C, Moayyedi P, et al. Medical treat-ments for the maintenance therapy of refluxoesophagitis and endoscopic negative reflux disease.Cochrane Database Syst Rev. 2004;4:1–58.
Dranove JE, Horn DS, Davis MA, et al. Predictors ofresponse to proton pump inhibitor therapy among chil-dren with significant esophageal eosinophilia. J Pediatr.2009;154:96–100.
Edwards DAW. The anti-reflux mechanism, its disordersand their consequences. Clin Gastroenterol.1982;11:479–96.
El-Serag HB, Richardson P, Pilgrim P, et al. Determinantsof gastroesophageal reflux disease in adults with ahistory of childhood gastroesophageal reflux disease.Clin Gastroenterol Hepatol. 2007;5:696–701.
Field SK, Gary CM, Gelfand AJ, et al. The effects ofantireflux surgery on asthmatics with gastroesophagealreflux. Chest. 1999;116:766–74.
Forsell L, Cnattingius S, Bottai M, et al. Increased risk ofBarrett’s esophagus among individuals born preterm orsmall for gestational age. Clin Gastroenterol Hepatol.2013;11:790–4.
Fujiwara Y, Arakawa T, Fass R. Gastroesophageal refluxand sleep. Gastroenterol Clin N Am. 2013;42:57–70.
Fukahori S, Asagiri K, Ishii S, et al. Pre-and postoperativeevaluation of gastroesophageal reflux and esophagealmotility in neurologically impaired children using com-bined pH-multichannel intraluminal impedance mea-surement. Pediatr Surg Int. 2013;29:545–51.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilicesophagitis in children and adults: a systemic reviewand consensus recommendation for diagnosis and treat-ment. Gastroenterology. 2007;133:1342–63.
22 M. E. Höllwarth and E. Sorantin

Ganz RA, Peters JH, Horgan S, et al. Esophageal sphincterdevice for gastroesophageal reflux disease. N Engl JMed. 2013;368:719–27.
Genta RM, Spechler SJ, Kielhorn AF. The Los Angelesand Savary-Miller systems for grading esophagitis:utilization and correlation with histology. Dis Esopha-gus. 2011;24:10–7.
Georgeson KE. Gastroesophageal reflux and hiatal hernia.In: Puri P, Höllwarth M, editors. Pediatric surgery,Springer Atlas series. Berlin/Heidelberg/New York:Springer; 2006. p. 49–60.
Goessler A, Huber-Zeyringer A, Hoellwarth ME. Doesepilepsy influence the outcome of antireflux proceduresin neurologically impaired children. Pediatr Surg Int.2006;22:485–90.
Goessler A, Schalamon J, Huber-Zeyringer A, et al. Gas-troesophageal reflux and behaviour in neurologicallyimpaired children. J Pediatr Surg. 2007;42:1486–90.
Gold BD. Is gastroesophageal reflux disease really a life-long disease: do babies who regurgitate grow up to beadults with GERD complications. Am J Gastroenterol.2006;101:641–4.
Gonsalves AN, Yang GY, Doerfler B, et al. Elimination dieteffectively treats eosinophilic esophagitis in adults;food reintroduction identifies causative factors. Gastro-enterology. 2012;142:1451–9.
Gupta M, Iyer PG, Lutzke L, et al. Recurrence of esopha-geal intestinal metaplasia after endoscopic mucosalresection and radiofrequency ablation of Barrett’sesophagus: results from a US Multicenter Consortium.Gastroenterology. 2013;145:79–86.
Hassall E. Barrett’s esophagus: new definitions andapproaches in children. J Pediatr Gastroenterol Nutr.1993;16:345–64.
Hassall E. Outcomes of fundoplication: cause for concern,newer options. Arch Dis Child. 2005;90:1047–52.
Hassall E, Kerr W, El-Serag H. Characteristics of childrenreceiving proton pump inhibitors continuously for up to11 years duration. J Pediatr. 2007;150:262–7.
Hirsch DP, Holloway RH, Tytgat GN, et al. Involvement ofnitric oxide in human transient lower esophagealsphincter relaxations and esophageal primary peristal-sis. Gastroenterology. 1998;115:1374–80.
Höllwarth ME. Entwicklung der Speiseröhrenfunktion beiNeugeborenen – eine manometrische Untersuchung.Z Kinderchir. 1979;27:201–15.
Höllwarth M. Gastroösophagealer Reflux undErkrankungen des Magens. In: von Schweinitz D, UreB, editors. Kinderchirurgie. 2nd ed. Berlin/Heidelberg:Springer; 2009.
Höllwarth ME, Uray E. Physiology and pathophysiologyof the esophagus in childhood. Pediatr Surg Int.1985;18:1–13.
Höllwarth ME, Uray E, Pesendorfer P. Esophagealmanometry. Pediatr Surg Int. 1986;1:177–83.
Horvath A, Dziechciarz P, Szajewska H. The effect ofthickened-feed interventions on gastroesophagealreflux in infants: systematic review and meta-analysis
of randomized controlled trials. Pediatrics. 2008;112:e1268–77.
Jodorkovsky D, Price JC, Kim B, et al. Multichannelintraluminal impedance-pH testing is clinically usefulin the management of patients with gastroesophagealreflux symptoms. Dig Dis Sci. 2014;23. Epub ahead ofprint.
Johnson DA, Ganz R, Aisenberg J, et al. Endoscopicimplantation of Enteryx for treatment of GERD: 12-month results of a prospective, multicenter trial. Am JGastroenterol. 2003;98:1921–30.
Kahrilas PJ, Shaheen NJ, Vaezi MF, et al. American Gas-troenterological Association medical position state-ment on the management of gastroesophageal refluxdisease. Gastroenterology. 2008;135:1383–91.
Katz PO. Gastroesophageal reflux disease: new treatments(review). Rev Gastroenterol Disord. 2002;2:66–74.
Khoshoo V, Le T, Haydel RM Jr, et al. Role of GER inolder children with persistent asthma. Chest.2003;123:1008–13.
Kurz R, Höllwarth ME, Fasching G, et al. Combineddisturbance of respiratory regulation and esophagealfunction in early infancy. Prog Pediatr Surg.1985;18:52–61.
Landler U, Höllwarth ME, Uray E, et al. Esophageal func-tion in infants with sudden infant death risk. KlinPädiatr. 1990;202:37–42.
Lasser MS, Liao JG, Burd RS. National trends in the use ofantireflux procedures for children. Pediatrics.2006;118:1828–35.
Lee WS, Beattie RM, Meadows M, et al. Gastro-oesophageal reflux: clinical profiles and outcome.J Paediatr Child Health. 1999;35:568–71.
Lidums I, Lehmann A, Checklin H, et al. Control of tran-sient lower esophageal sphincter relaxations and refluxby the GABAB agonist baclofen in normal subjects.Gastroenterology. 2000;118:7–13.
Liebermann-Meffert D, Allgöwer M, Schmid P, et al. Mus-cular equivalent of the lower esophageal sphincter.Gastroenterology. 1979;76:31–8.
Liu DC, Somme S, Mavrelis PG, et al. Stretta as the initialantireflux procedure in children. J Pediatr Surg.2005;40:148–52.
LoW-K, ChanWW. Proton pump inhibitor use and the riskof small bacterial overgrowth: a meta-analysis. ClinGastroenterol Hepatol. 2013;11:483–90.
Lundell L, Miettinen P, Myrvold HE, et al. Continued (5year) followup of a randomized clinical study compar-ing antireflux surgery and omeprazole in gastroesoph-ageal reflux disease. J Am Coll Surg.2001;192:172–81.
Martin AJ, Pratt N, Kennedy DJ, et al. Natural history andfamilial relationship of infants spilling to 9 years of age.Pediatrics. 2002;109:1061–7.
Mathisen B, Worall I, Masel J, et al. Feeding problems ininfants with gastro-oesophageal reflux disease: a con-trolled study. J Paediatr Child Health. 1999;35:163–9.
Mittal RK, Balaban DH. The esophagogastric junction.N Engl J Med. 1997;336:924–32.
Gastroesophageal Reflux and Hiatal Hernia 23

Morabito A, Lall A, Piccolo RL, et al. Totalesophagogastric dissociation: 10 years’ review.J Pediatr Surg. 2006;41:919–22.
Nakahara Y, Aoyama K, Goto T, et al. Modified Collis-Nissen procedure for pure long-gap esophageal atresia.J Pediatr Surg. 2012;47:262–6.
Ngerncham M, Barnhart DC, Haricharan RN, et al. Riskfactors for recurrent gastroesophageal reflux diseaseafter fundoplication in pediatric patients: a case-controlstudy. J Pediatr Surg. 2007;42:1478–85.
Nissen R. A simple operation for control of reflux esoph-agitis. Schweiz Med Wochenschr. 1956;81(Suppl20):590–2.
Ollyo JB, Savary M, Levi F. Esophagitis caused bystenosing reflux: importance of endoscopy for diagno-sis and surveillance. Schweiz Rundsch Med Prax.1986;75:1528–30.
Omari TI, Barnett CP, Benninga MA, et al. Mechanism ofgastroesophageal reflux in preterm and term infantswith reflux disease. Gut. 2002;51:475–9.
Omari TI, Benninga MA, Sansom L, et al. Effect of baclo-fen on esophagogastric motility and gastroesophagealreflux in children with gastroesophageal reflux disease:a randomized controlled trial. J Pediatr.2006;149:468–74.
Orenstein SR, Shalaby TM, Kelsey SF, et al. Natural his-tory of infant reflux esophagitis: symptoms and mor-phometric histology during one year withoutpharmacotherapy. Am J Gastroenterol. 2006;101:628–40.
Pandolfino JE, Krishnan K. Do endoscopic antireflux pro-cedures fit in the current treatment paradigm of gastro-esophageal reflux disease? Clin Gastroenterol Hepatol.2014;12:544–54.
Peery AF, Dellon ES, Lund J, et al. Burden of gastrointes-tinal disease in the United States: 2012 update. Gastro-enterology. 2012;143:1051–187.
Pesendorfer P, Höllwarth ME, Uray E. Long-term follow-up in infants with pathological gastroesophageal reflux.Klin Pädiatr. 1993;205:363–6.
Raicevic M, Saxena AK. Barrett’s esophagus in children:what is the evidence? World J Pediatr. 2018;14(4):330–4.
Rees JRE, Lao-Sireix P, Wong A, et al. Treatment ofBarrett oesophagus. Cochrane Database Syst Rev.2010;1:1–59.
Richter JE. Gastroesophageal reflux disease treatment: sideeffects and complications of fundoplication. ClinGastroenterol Hepatol. 2013;11:465–71.
Rodriguez L, Rodriguez P, Gomez P, et al. Electrical stim-ulation therapy of the lower esophageal sphincter issuccessful in treating GERD: final result of open-labelprospective trial. Surg Endosc. 2013;27:1038–92.
Rudolph CD. Are proton pump inhibitors indicated for thetreatment of gastroesophageal reflux in infants andchildren? J Pediatr Gastroenterol Nutr. 2003;37(Suppl):S60–4.
Sampliner RE. Practice guidelines on the diagnosis, sur-veillance, and therapy of Barrett’s esophagus. The
Practice Parameters Committee of the American Col-lege of Gastroenterology. Am J Gastroenterol.1998;93:1028–32.
Semeniuk J, Kaczmarski M. 24-hour esophageal pH-mon-itoring in children suspected of gastroesophageal refluxdisease: analysis of intraesophageal pH monitoringvalues recorded in distal and proximal channel at diag-nosis. World J Gastroenterol. 2007;13:5108–15.
Sherman PM, Hassal E, Fagundes-Neto U, et al. A global,evidence-based consensus on the definition of gastro-esophageal reflux disease in the pediatric population.Am J Gastroenterol. 2009;104:1278–95.
Slocum C, Hibbs AM, Martin RJ, et al. Infant apnea andgastroesophageal reflux: a critical review and frame-work for further investigation. Curr Gastroenterol Rep.2007;9:219–24.
Solayamani-Dodaran M, Card TR, West J. Cause-specificmortality of people with Barrett’s esophagus comparedwith the general population: a population based cohortstudy. Gastroenterology. 2013;144:1375–82.
Sopo SM, Radzik D, Calvani M. Does treatment withproton pump inhibitors for gastroesophageal reflux dis-ease (GERD) improve asthma symptoms in childrenwith asthma and GERD? A systematic review.J Investig Allergol Clin Immunol. 2009;19:1–5.
Strate U, Emmermann A, Fibbe C, et al. Laparoscopicfundoplication: Nissen versus Toupet two-year out-come of a prospective randomized study of 200 patientsregarding preoperative esophageal motility. SurgEndosc. 2008;22:21–30.
Thal AP, Hatafuku T, Kurtzman R. New operation for distalesophageal stricture. Arch Surg. 1965;90:464–72.
Tolia V, Boyer K. Long-term proton pump inhibitor use inchildren: a retrospective review of safety. Dig Dis Sci.2008;53:385–93.
Toupet A. Technique d’esophago-gastroplastie avecphreno-gastropexiedans la cure radicals deshernieshiatales et comme complement de l’operationde Heller dans les cardiospasmes. Mem Acad Chir.1963;89:394–9.
Tovar JA, Luis AL, Encinas JL, et al. Pediatric surgeonsand gastroesophageal reflux. J Pediatr Surg.2007;42:277–83.
Ummarino D, Miele E, Masi P, et al. Impact of anti-secretory treatment on respiratory symptoms of gastro-esophageal reflux disease in children. Dis Esophagus.2012;25:671–7.
Vadlamudi NB, Hitch MC, Dimmitt RA, et al. Baclofen forthe treatment of pediatric GERD. JPGN.2013;57:808–12.
Vaezi MF. Sore throat and a red hypopharynx: is it reflux?Clin Gastroenterol Hepatol. 2007;5:1379–82.
van der Pol RJ, Loots CM, Peeters L, et al. Outcomes ofendoscopy and novel pH-impedance parameters inchildren: is there a correlation? JPGN.2013;56:196–200.
Vandenplas Y, Goyvaerts H, Helven R. Gastroesophagealreflux, as measured by 24-hour pH-monitoring, in 509
24 M. E. Höllwarth and E. Sorantin

healthy infants screened for risk of sudden infant deathsyndrome. Pediatrics. 1991;88:834–40.
Vandenplas Y, Salvatore S, Devreker T, et al. Gastro-oesophageal reflux disease: oesophageal impedanceversus pH monitoring. Acta Paediatr. 2007;96:956–62.
Vandenplas Y, Rudolph CD, Di Lorenzo C, et al. Pediatricgastroesophageal reflux clinical practice guidelines:joint recommendations of the North American Societyfor Pediatric Gastroenterology, Hepatology, and Nutri-tion (NASPGHAN) and the European Society for Pedi-atric Gastroenterology, Hepatology, and Nutrition(ESPGHAN). J Pediatr Gastroenterol Nutr.2009;49:498–547.
Vernon-Roberts A, Sullivan PB. Fundoplication versuspost-operative medication for gastro-oesophagealreflux in children with neurological impairment under-going gastrostomy (review). Cochrane Database SystRev. 2007;1:1–13.
Wasilewska A, Semeniuk J, Cudowska P, et al. Respiratoryresponse to proton pump inhibitor treatment in childrenwith obstructive sleep apnea syndrome and gastro-esophageal reflux. Sleep Med. 2012;13:824–30.
Weber TR. A prospective analysis of factors influencingoutcome after fundoplication. J Pediatr Surg.1995;30:1061–4.
Wenzel TG, Benninga MA, Loots CM, et al. Indications,methodology, and interpretation of combined esopha-geal impedance-pHmonitoring in children: ESPGHANEURO-PIG standard protocol. J Pediatr GastroenterolNutr. 2012;55:230–4.
Wenzl TG, Schenke S, Peschgens T, et al. Association ofapnea and non-acid gastroesophageal reflux in infants:investigations with intraluminal impedance technique.Pediatr Pulmonol. 2001;31:144–9.
Xu X-H, Yang Z-M, Chen Q, et al. Therapeutic efficacy ofbaclofen in refractory gastroesophageal reflux-inducedchronic cough. World J Gastroenterol.2013;19:4368–92.
Zhang Q, Lehmann A, Rigda R, et al. Control of transientlower oesophageal sphincter relaxations and reflux bythe GABAB agonist baclofen in patients with gastro-oesophageal reflux disease. Gut. 2002;50:19–24.
Gastroesophageal Reflux and Hiatal Hernia 25