Embed Size (px)
Citation preview
Gastroesophageal Reflux Disease Gastroesophageal Reflux Disease (GERD) (GERD)
• Any symptoms or esophageal mucosal damage Any symptoms or esophageal mucosal damage that results from reflux of gastric acid into the that results from reflux of gastric acid into the esophagusesophagus
• Classic GERD symptomsClassic GERD symptoms– Heartburn (pyrosis): substernal burning discomfortHeartburn (pyrosis): substernal burning discomfort– Regurgitation: bitter, acidic fluid in the mouth Regurgitation: bitter, acidic fluid in the mouth
when lying down or bending overwhen lying down or bending over
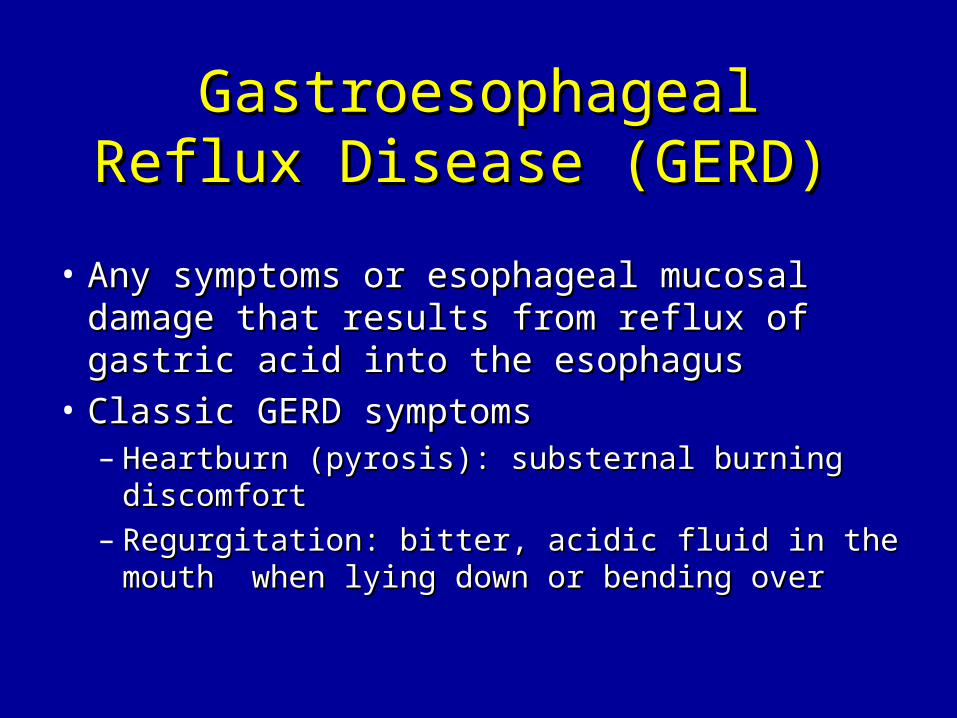
Locke et al. Gastroenterology 1997;112:1148.Locke et al. Gastroenterology 1997;112:1148.
High Prevalence of Gastroesophageal High Prevalence of Gastroesophageal Reflux Symptoms Reflux Symptoms
19.8%
59%
0%10%20%30%40%50%60%
Weekly Monthly
Frequency of heartburn and/or regurgitation
Important Reasons to Diagnose and Treat Important Reasons to Diagnose and Treat GERDGERD
• Negative impact on health-related quality of lifeNegative impact on health-related quality of life11
• Risk factor for esophageal adenocarcinomaRisk factor for esophageal adenocarcinoma22
1.1. Revicki et al. Am J Med 1998;104:252.Revicki et al. Am J Med 1998;104:252.2.2. Lagergren et al. N Engl J Med 1999;340:825.Lagergren et al. N Engl J Med 1999;340:825.
Clinical Presentations of GERDClinical Presentations of GERD
• Classic GERD Classic GERD
• Extraesophageal/Atypical GERDExtraesophageal/Atypical GERD
• Complicated GERDComplicated GERD
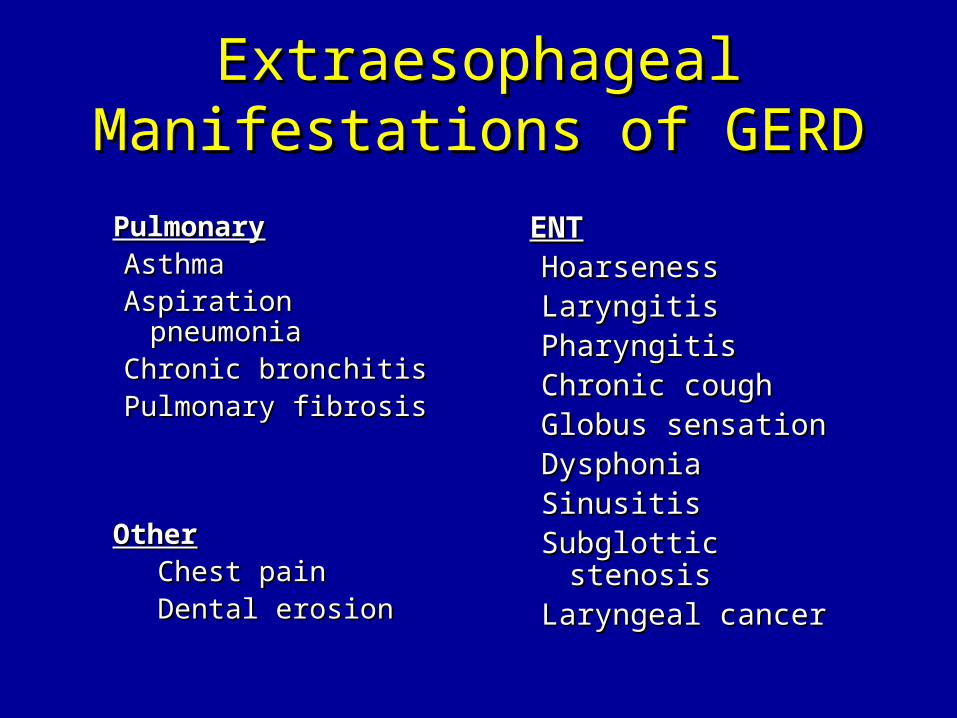
Extraesophageal Manifestations Extraesophageal Manifestations of GERDof GERD
PulmonaryPulmonaryAsthmaAsthmaAspiration pneumoniaAspiration pneumoniaChronic bronchitisChronic bronchitisPulmonary fibrosisPulmonary fibrosis
OtherOther Chest painChest pain Dental erosionDental erosion
ENTENTHoarsenessHoarsenessLaryngitisLaryngitisPharyngitisPharyngitisChronic coughChronic coughGlobus sensationGlobus sensationDysphoniaDysphoniaSinusitisSinusitisSubglottic stenosisSubglottic stenosisLaryngeal cancerLaryngeal cancer
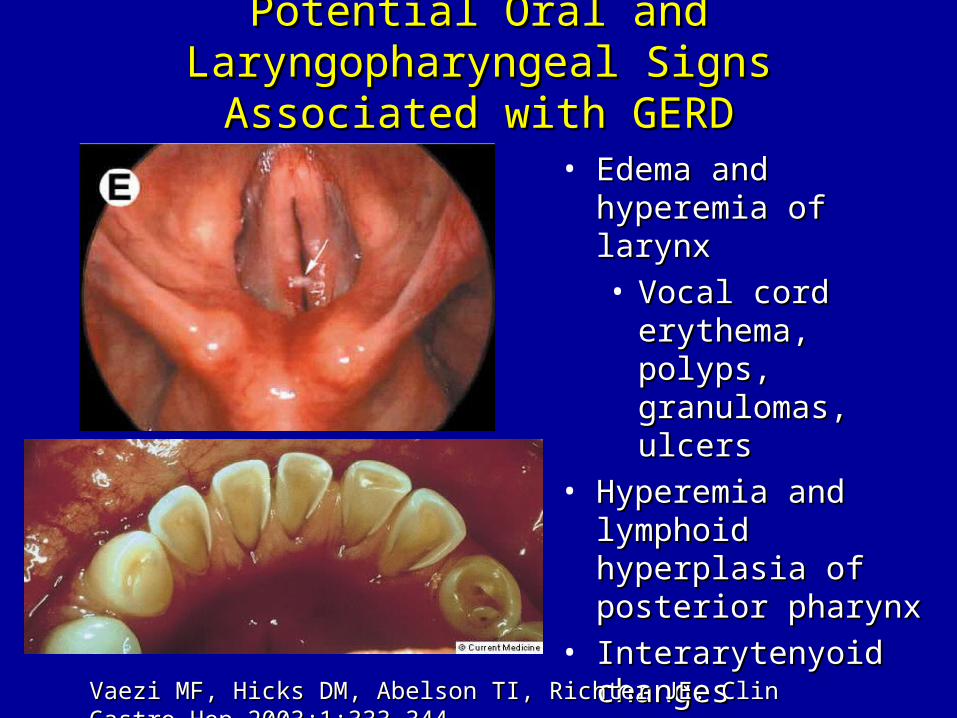
Potential Oral and Laryngopharyngeal Signs Potential Oral and Laryngopharyngeal Signs Associated with GERDAssociated with GERD
• Edema and hyperemia of Edema and hyperemia of larynxlarynx
• Vocal cord erythema, Vocal cord erythema, polyps, granulomas, polyps, granulomas, ulcersulcers
• Hyperemia and lymphoid Hyperemia and lymphoid hyperplasia of posterior hyperplasia of posterior pharynx pharynx
• Interarytenyoid changesInterarytenyoid changes
• Dental erosionDental erosion
• Subglottic stenosisSubglottic stenosis
• Laryngeal cancerLaryngeal cancer
Vaezi MF, Hicks DM, Abelson TI, Richter JE. Clin Gastro Hep 2003;1:333-Vaezi MF, Hicks DM, Abelson TI, Richter JE. Clin Gastro Hep 2003;1:333-344.344.
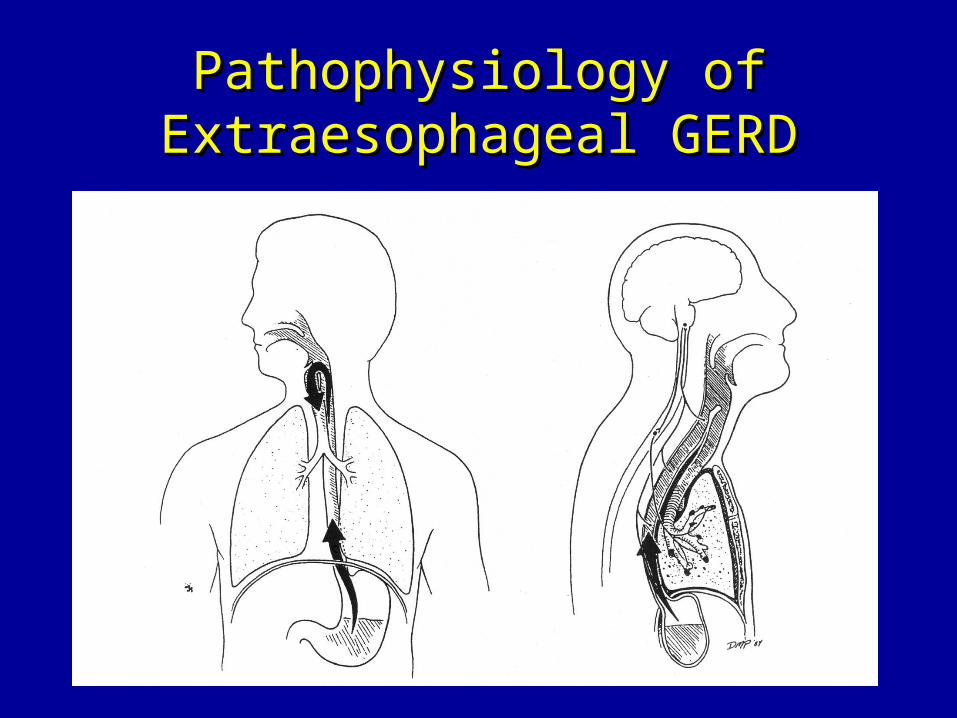
Pathophysiology of Extraesophageal Pathophysiology of Extraesophageal GERDGERD
Symptoms of Complicated GERDSymptoms of Complicated GERD
• DysphagiaDysphagia– Difficulty swallowing: food sticks or hangs Difficulty swallowing: food sticks or hangs
upup
• OdynophagiaOdynophagia– Retrosternal pain with swallowingRetrosternal pain with swallowing
• BleedingBleeding
When to Perform Diagnostic TestsWhen to Perform Diagnostic Tests
• Uncertain diagnosisUncertain diagnosis
• Atypical symptomsAtypical symptoms
• Symptoms associated with complicationsSymptoms associated with complications
• Inadequate response to therapy Inadequate response to therapy
• Recurrent symptomsRecurrent symptoms
• Prior to anti-reflux surgeryPrior to anti-reflux surgery
Diagnostic Tests for GERDDiagnostic Tests for GERD
• Barium swallowBarium swallow
• EndoscopyEndoscopy
• Ambulatory pH monitoringAmbulatory pH monitoring
• Esophageal manometryEsophageal manometry
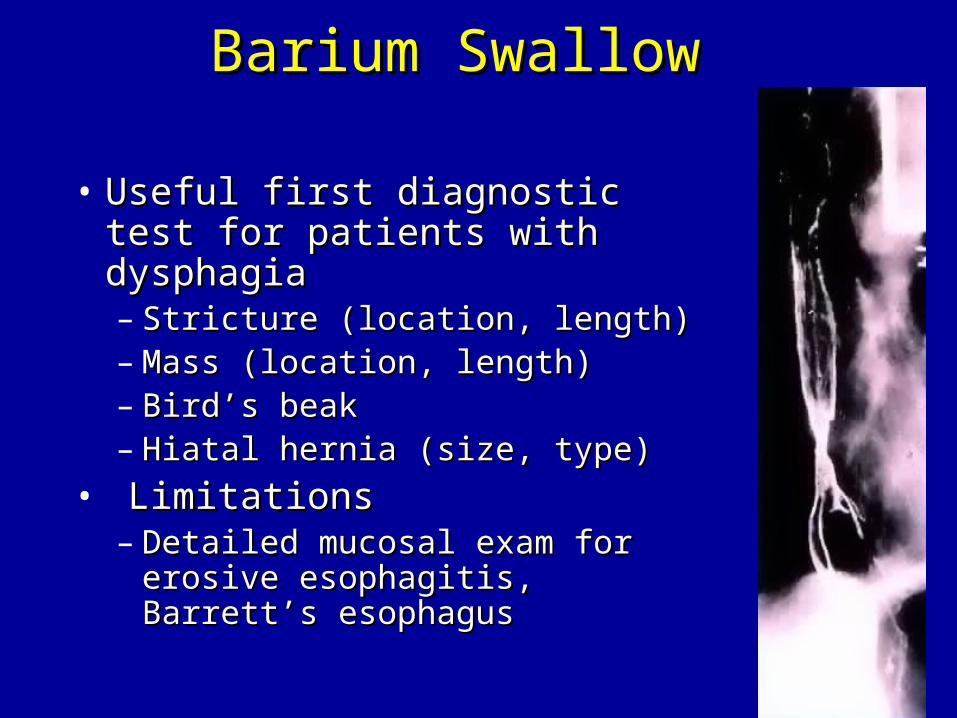
Barium SwallowBarium Swallow
• Useful first diagnostic test for Useful first diagnostic test for patients with dysphagiapatients with dysphagia– Stricture (location, length)Stricture (location, length)– Mass (location, length)Mass (location, length)– Bird’s beakBird’s beak– Hiatal hernia (size, type)Hiatal hernia (size, type)
• LimitationsLimitations– Detailed mucosal exam for erosive Detailed mucosal exam for erosive
esophagitis, Barrett’s esophagusesophagitis, Barrett’s esophagus
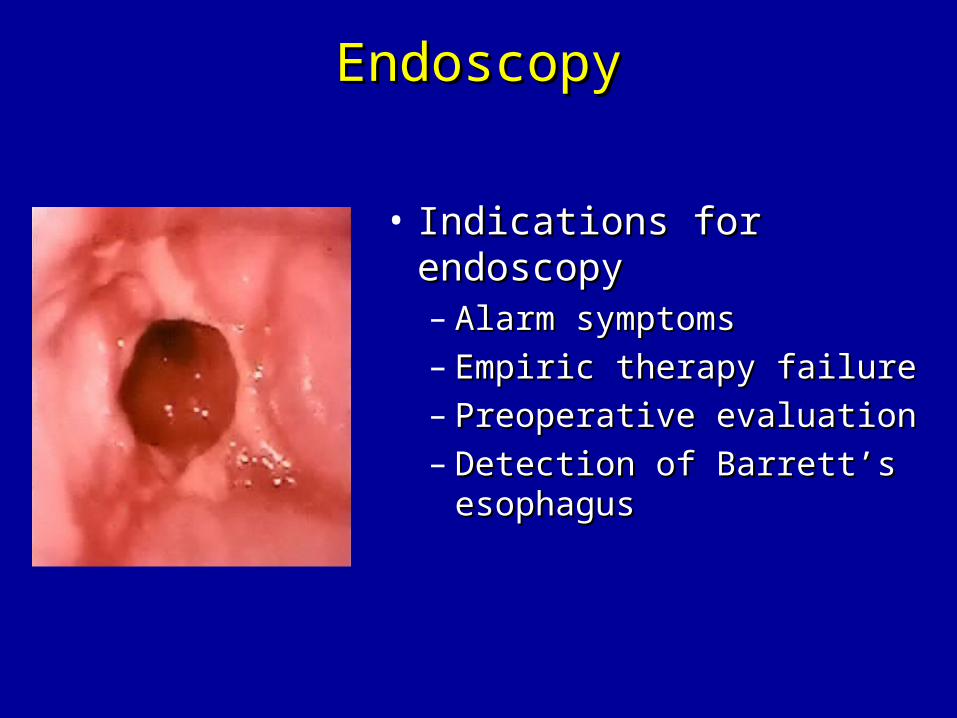
EndoscopyEndoscopy
• Indications for endoscopy Indications for endoscopy – Alarm symptomsAlarm symptoms– Empiric therapy failureEmpiric therapy failure– Preoperative evaluationPreoperative evaluation– Detection of Barrett’s Detection of Barrett’s
esophagusesophagus
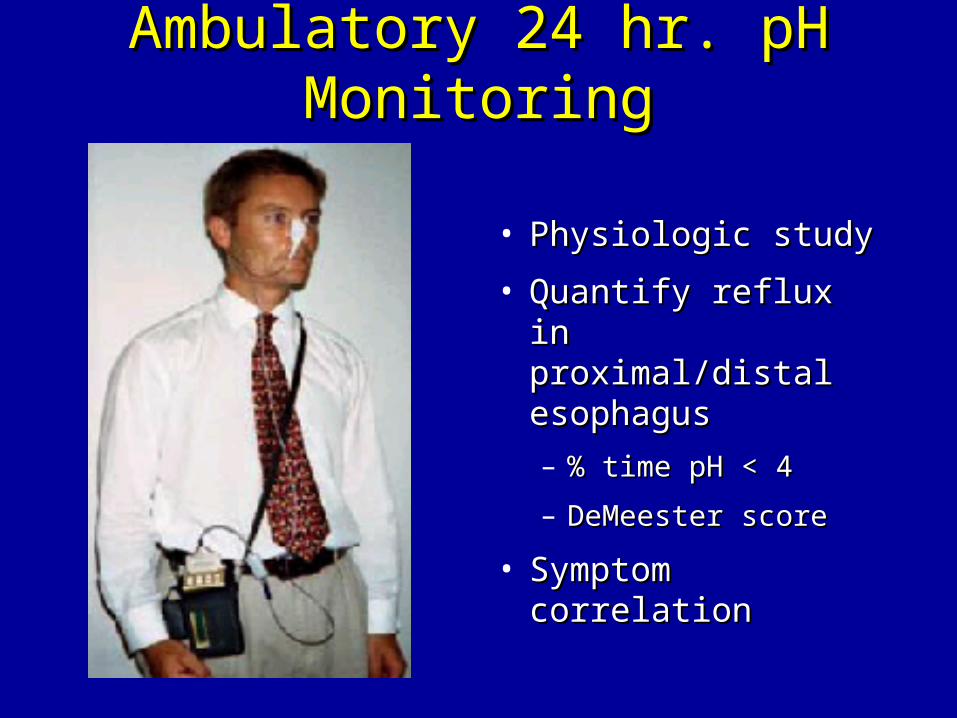
Ambulatory 24 hr. pH MonitoringAmbulatory 24 hr. pH Monitoring
• Physiologic studyPhysiologic study
• Quantify reflux in Quantify reflux in proximal/distal proximal/distal esophagusesophagus
– % time pH < 4% time pH < 4
– DeMeester scoreDeMeester score
• Symptom correlationSymptom correlation
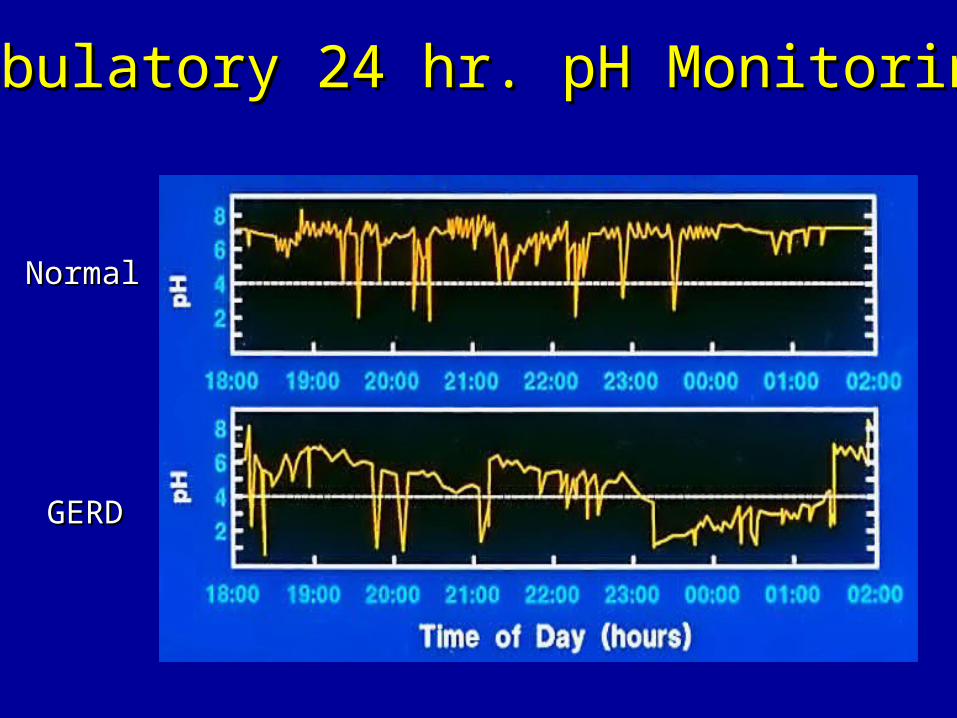
Ambulatory 24 hr. pH MonitoringAmbulatory 24 hr. pH Monitoring
NormalNormal
GERDGERD
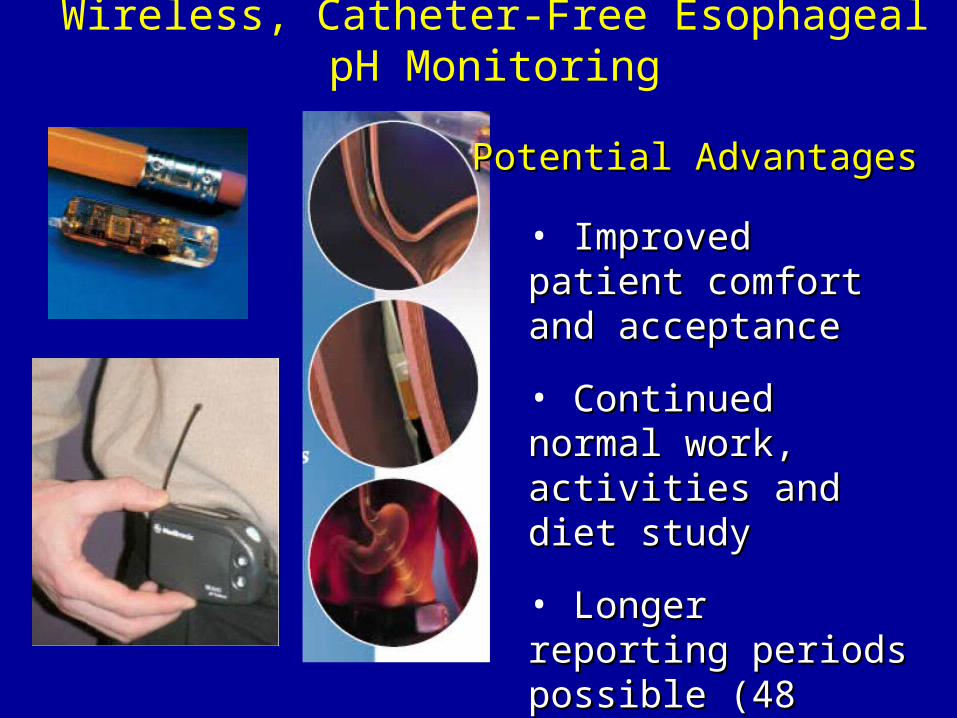
Wireless, Catheter-Free Esophageal pH Monitoring
• Improved patient Improved patient comfort and acceptancecomfort and acceptance
• Continued normal work, Continued normal work, activities and diet studyactivities and diet study
• Longer reporting periods Longer reporting periods possible (48 hours)possible (48 hours)
• Maintain constant probe Maintain constant probe position relative to SCJposition relative to SCJ
Potential AdvantagesPotential Advantages
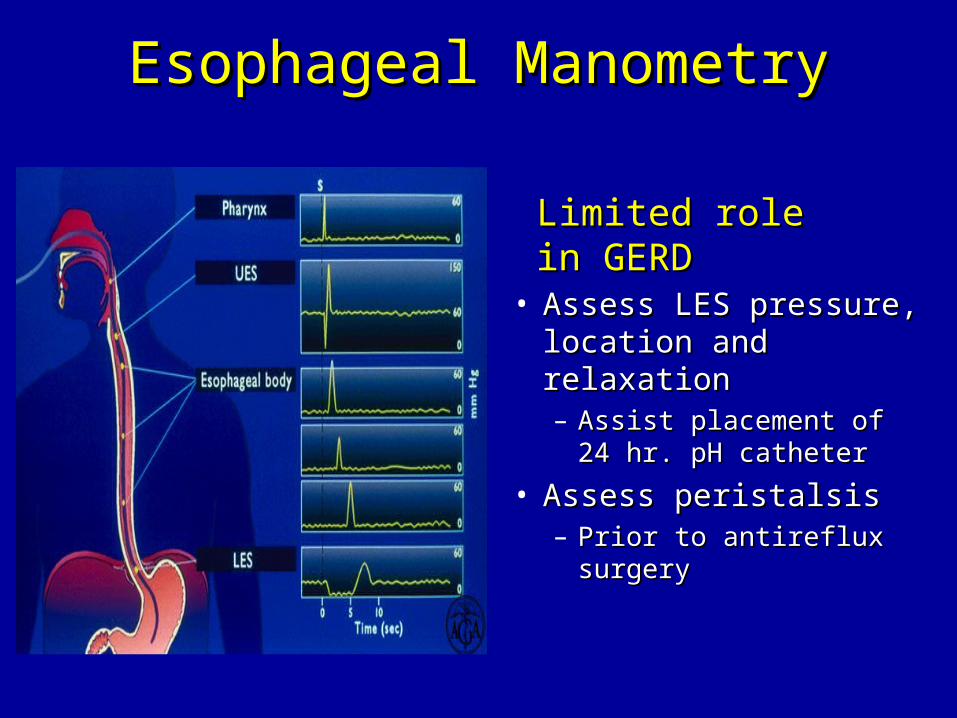
Esophageal ManometryEsophageal Manometry
• Assess LES pressure, Assess LES pressure, location and relaxationlocation and relaxation– Assist placement of 24 hr. Assist placement of 24 hr.
pH catheterpH catheter
• Assess peristalsisAssess peristalsis– Prior to antireflux surgery Prior to antireflux surgery
Limited role in GERDLimited role in GERD

Treatment Goals for GERDTreatment Goals for GERD
• Eliminate symptomsEliminate symptoms
• Heal esophagitisHeal esophagitis
• Manage or prevent complicationsManage or prevent complications
• Maintain remissionMaintain remission
Lifestyle Modifications are Lifestyle Modifications are Cornerstone of GERD TherapyCornerstone of GERD Therapy
• Elevate head of bed 4-6 inches Elevate head of bed 4-6 inches • Avoid eating within 2-3 hours of bedtimeAvoid eating within 2-3 hours of bedtime• Lose weight if overweightLose weight if overweight• Stop smokingStop smoking• Modify dietModify diet
– Eat more frequent but smaller mealsEat more frequent but smaller meals
– Avoid fatty/fried food, peppermint, chocolate, Avoid fatty/fried food, peppermint, chocolate, alcohol, carbonated beverages, coffee and teaalcohol, carbonated beverages, coffee and tea
• OTC medications prnOTC medications prn
Acid Suppression Therapy for GERDAcid Suppression Therapy for GERD
HH22-Receptor Antagonists-Receptor Antagonists
(H(H22RAs)RAs)
Cimetidine (TagametCimetidine (Tagamet®®))
Ranitidine (ZantacRanitidine (Zantac®®))
Famotidine (PepcidFamotidine (Pepcid®®))
NizatidineNizatidine (Axid (Axid®®))
Proton Pump InhibitorsProton Pump Inhibitors (PPIs)(PPIs)
Omeprazole (PrilosecOmeprazole (Prilosec®®))Lansoprazole (PrevacidLansoprazole (Prevacid®®))Rabeprazole (AciphexRabeprazole (Aciphex®®))Pantoprazole (ProtonixPantoprazole (Protonix®®))Esomeprazole (Nexium Esomeprazole (Nexium ®®) )
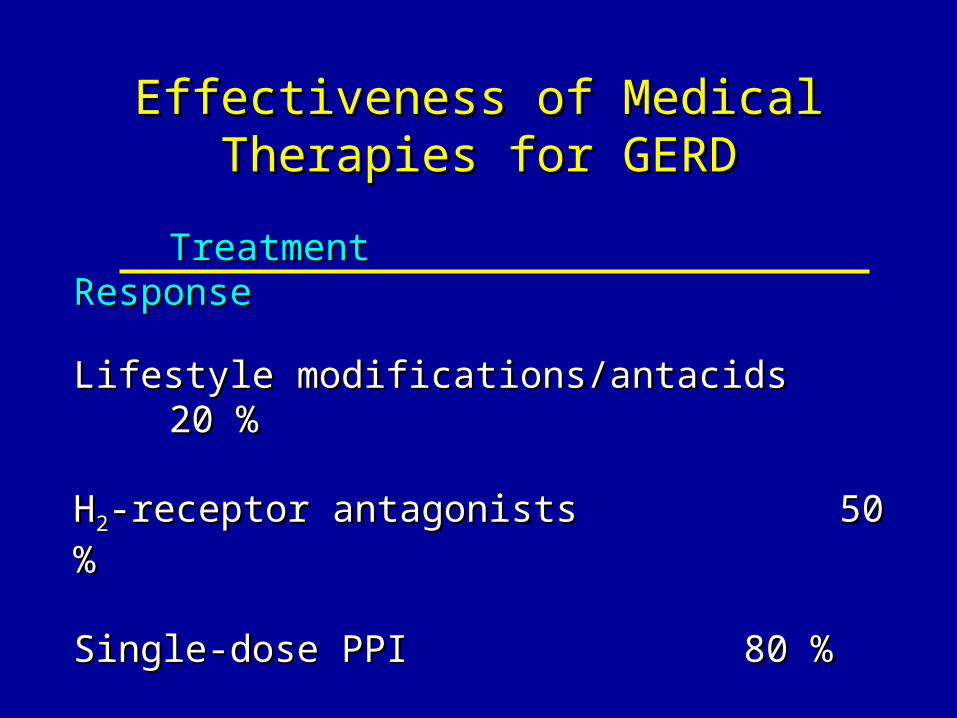
Effectiveness of Medical Therapies for Effectiveness of Medical Therapies for GERDGERD
TreatmentTreatment ResponseResponse
Lifestyle modifications/antacidsLifestyle modifications/antacids 20 %20 %
HH22-receptor antagonists-receptor antagonists 50 %50 %
Single-dose PPI Single-dose PPI 80 %80 %
Increased-dose PPIIncreased-dose PPI up to 100 %up to 100 %
Treatment Modifications for Treatment Modifications for Persistent SymptomsPersistent Symptoms
• Improve complianceImprove compliance
• Optimize pharmacokineticsOptimize pharmacokinetics
– Adjust timing of medication to 15 – 30 minutes Adjust timing of medication to 15 – 30 minutes before meals (as opposed to bedtime)before meals (as opposed to bedtime)
– Allows for high blood level to interact with Allows for high blood level to interact with parietal cell proton pump activated by the mealparietal cell proton pump activated by the meal
• Consider switching to a different PPI Consider switching to a different PPI
GERD is a Chronic Relapsing ConditionGERD is a Chronic Relapsing Condition
• Esophagitis relapses quickly after cessation Esophagitis relapses quickly after cessation of therapyof therapy– > 50 % relapse within 2 months> 50 % relapse within 2 months– > 80 % relapse within 6 months> 80 % relapse within 6 months
• Effective maintenance therapy is imperativeEffective maintenance therapy is imperative
Complications of GERDComplications of GERD
• Erosive/ulcerative esophagitisErosive/ulcerative esophagitis
• Esophageal (peptic) strictureEsophageal (peptic) stricture
• Barrett’s esophagusBarrett’s esophagus
• AdenocarcinomaAdenocarcinoma
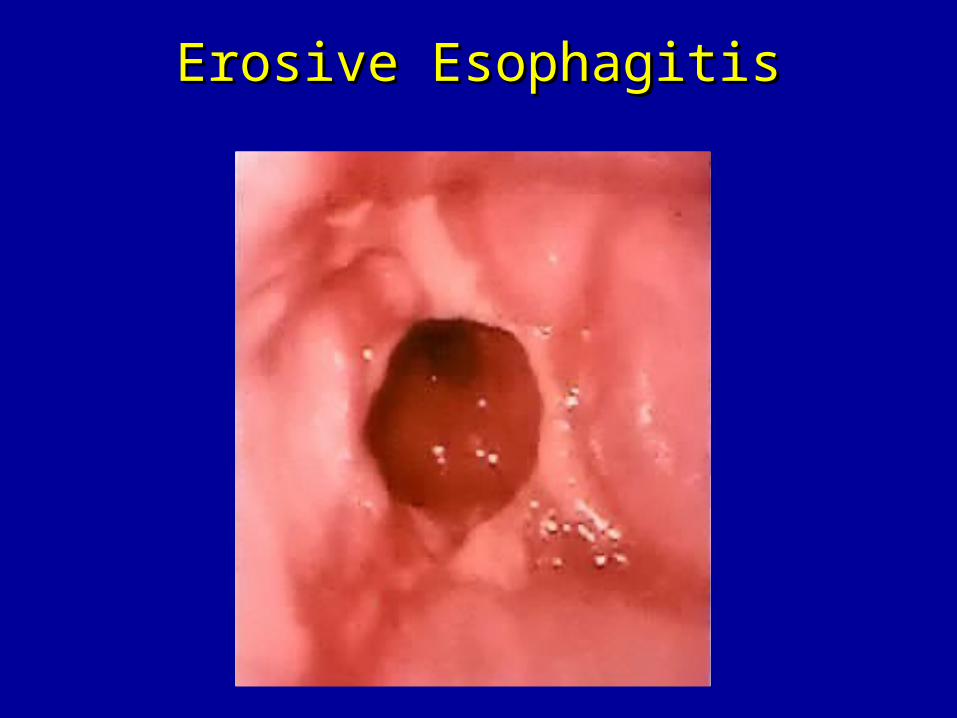
Erosive EsophagitisErosive Esophagitis
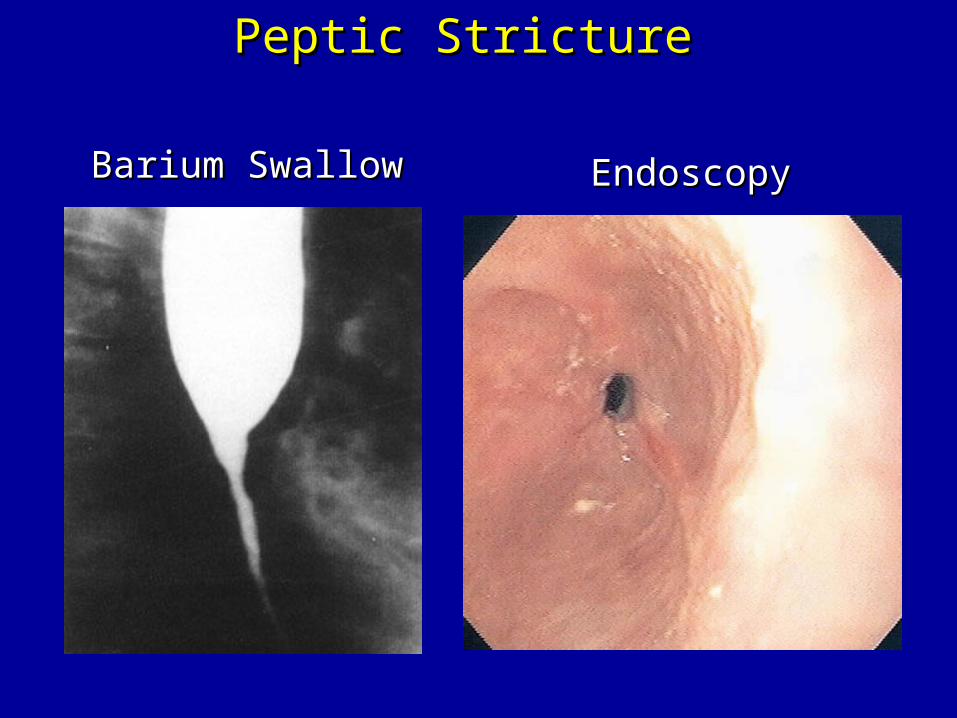
Peptic StricturePeptic Stricture
Barium SwallowBarium Swallow EndoscopyEndoscopy
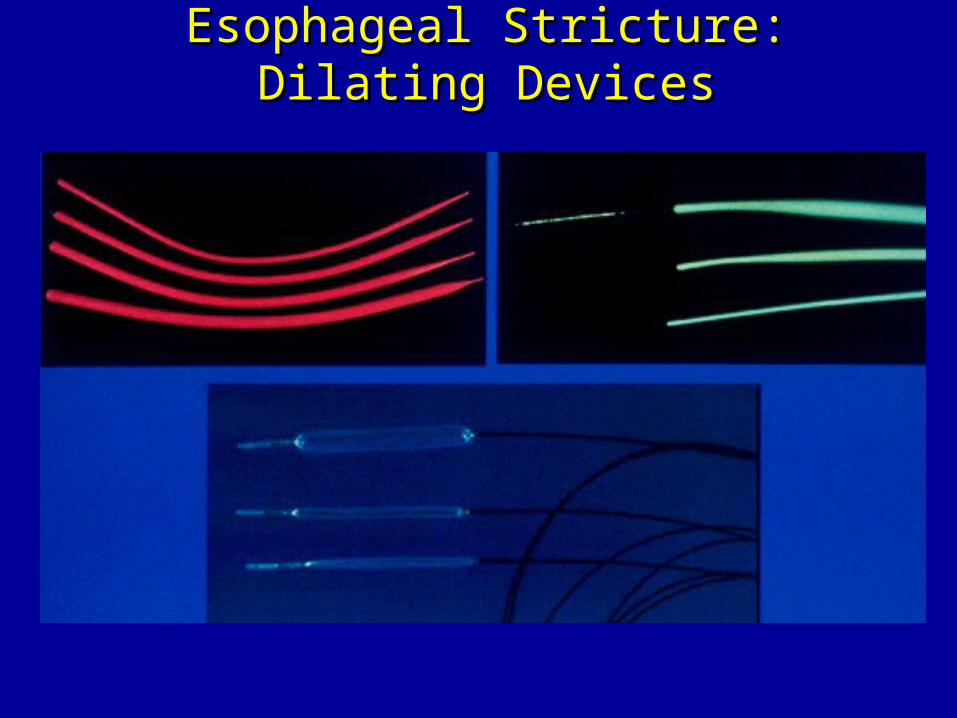
Esophageal Stricture: Dilating DevicesEsophageal Stricture: Dilating Devices
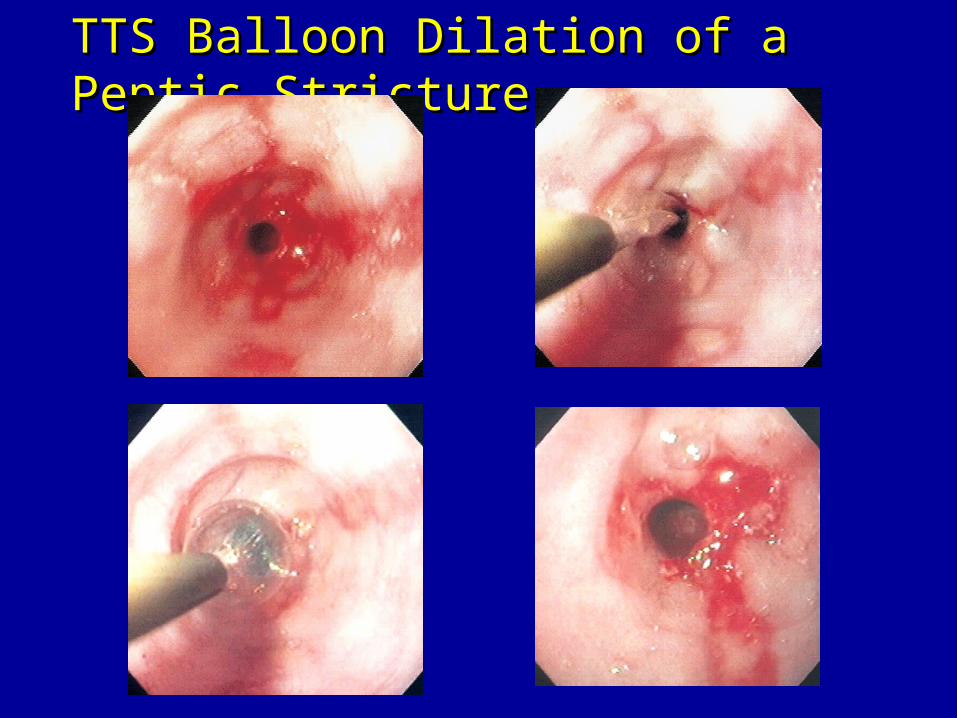
TTS Balloon Dilation of a Peptic StrictureTTS Balloon Dilation of a Peptic Stricture
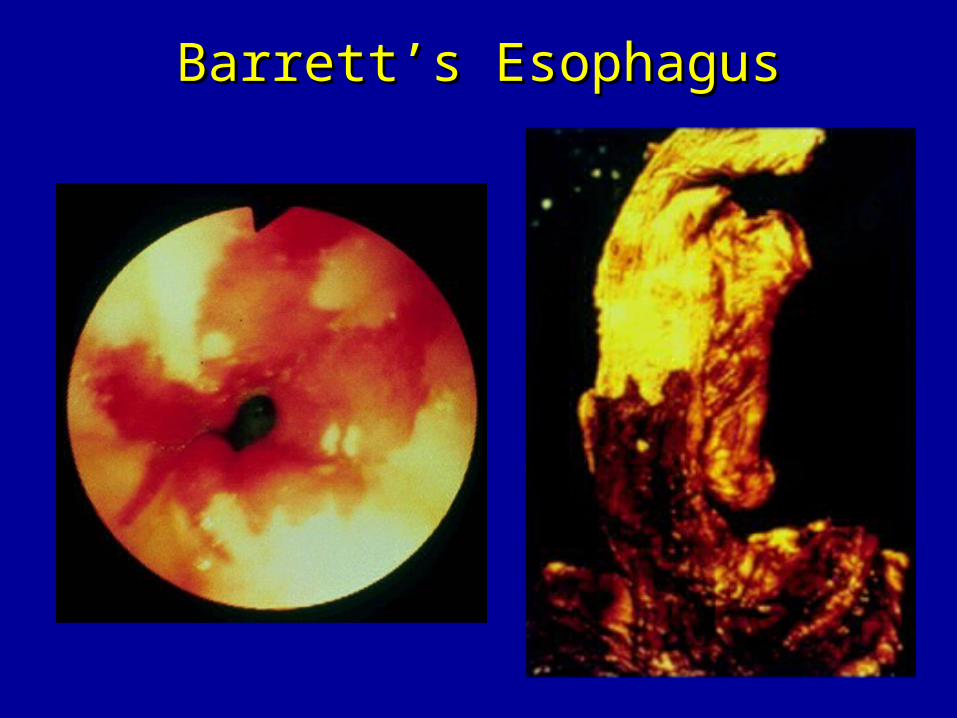
Barrett’s EsophagusBarrett’s Esophagus
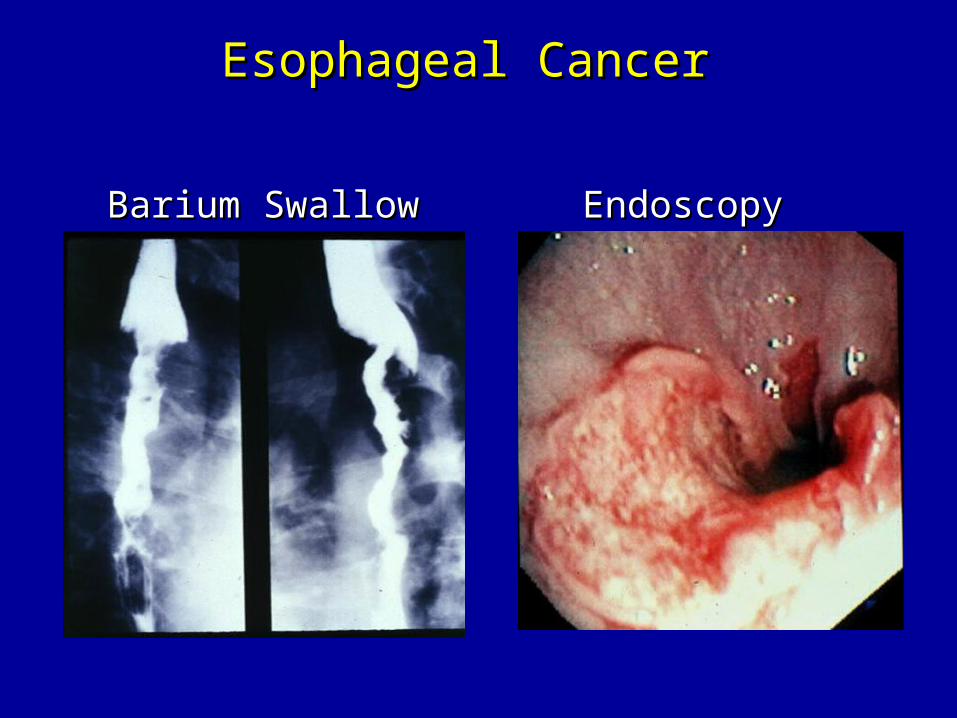
Esophageal CancerEsophageal Cancer
Barium SwallowBarium Swallow EndoscopyEndoscopy
When to Discuss Anti-Reflux When to Discuss Anti-Reflux Surgery with PatientsSurgery with Patients
• Intractable GERD – rareIntractable GERD – rare– Difficult to manage stricturesDifficult to manage strictures– Severe bleeding from esophagitisSevere bleeding from esophagitis– Non-healing ulcersNon-healing ulcers
• GERD requiring long-term PPI-BID in a GERD requiring long-term PPI-BID in a healthy young patient healthy young patient
• Persistent regurgitation/aspiration symptomsPersistent regurgitation/aspiration symptoms• Not Barrett’s esophagus aloneNot Barrett’s esophagus alone
Endoscopic GERD Therapy Endoscopic GERD Therapy
• Endoscopic antireflux therapiesEndoscopic antireflux therapies– Radiofrequency energy delivered to the LESRadiofrequency energy delivered to the LES
• Stretta procedureStretta procedure– Suture ligation of the cardiaSuture ligation of the cardia
• Endoscopic plicationEndoscopic plication– Submucosal implantation of inert material in Submucosal implantation of inert material in
the region of the lower esophageal sphincterthe region of the lower esophageal sphincter• EnteryxEnteryx