Embed Size (px)
Citation preview
""""SACTIONS OF THE ROYA~ SOCI~Y OF TROPICAL MEDICINE AND HYGIENE (1986) 80, 675-68S 675
RO~AL SOCIETY OF TROPICAL MEDICINE AND HYGIENE
SymposiumManson House, Thursday, 16th January, 1986
Gastrointestinal Helminth Infections
The clinical ~ignificance of gastrointestinal helminths-a review
I G. c. COOK
Dept. of Clinical Tropi~al Medicine, Hospital for Tropical Diseases, St. Pancras Way, London NWl OPE
AbstractGastrointestinal helminths (nematodes, trematodes and cestodes) constitute some of the most
common and impo tant infective agents of mankind and are responsible for much morbidity and somemortality , Wherea many symptoms and signs are confined to the intestine and less often theassociated digestiv organs, systemic manifestations are also numerous; this applies especially toindigenous popula 'ons of developing 'Third World' countries, Using a clinical classification theseorganisms can be roadly separated into those involving the small-intestine and those which have acolo-rectal distrib tion; of the former, a minority has been causally related to intestinalmalabsorption, Cl arly, however, not all gastrointestinal helminths are associated with disease and itis important to be ble to separate these two groups; when present at high concentration and especiallyin infants and c ldren some of the least pathogenic are not, however, entirely asymptomatic,Maintenance of a high 'index of suspicion' is necessary and this applied especially to 'western'populations in wh m rapid and extensive travel to areas of the world with substandard sanitation andcontaminated food and water supplies is now common; first evidence of infection in them may resultfrom serious clinic complications. Recent advances have focussed on treatment, and especially theintroduction of th benzimidazole compounds (especially albendazole) for nematode, and praziquan-tel for cestode, in ections, Treatment of strongyloidiasis remains, however, unsatisfactory, Masselimination of gas rointestinal helminths in developing 'Third World' countries remains a majorchallenge.
infected during either brief or prolonged exposure totropical conditions; the magnitude of infection andunderlying nutritional status are therefore important.Similarly, epilepsy resulting from cerebral cysticer-cosis (Taenia solium) and large-duct biliary or pancrea-tic duct obstruction caused by Ascaris lumbricoides arerarities in European travellers who have becomeinfected, but often assume considerable clinical im-portance in the indigenous population of sometropical countries. Multiple infections too are com-mon in the 'Third World', the common 'trinity' beingascariasis, hookworm infection and trichuriasis. Thedegree to which individual parasites influence eachother requires more attention.
At a clinical level, host defence mechanisms areclearly important (ALLARDYCE & BIENENSTOCK,1984; WALKER, 1984). Whereas immunologicalmechanisms probably playa part, and there is someevidence that undernutrition interferes with this(GREENWOOD & WHITTLE, 1981), hypocWorhydria(which is a relatively common problem in developing'Third World' countries) has probably been under-estimated (COOK, 1985c). Reasonable evidence existsthat Strongyloides stercoralis, for example, is morecommon in hypochlorhydrics. Statistically, the anato-mical site of infection is usually the small-intestine,where clearly the luminal milieu is acceptable tonematodes, trematodes and cestodes alike. Larvae of
"And he was eaten ofwo s, and gave up the ghost"(Acts of the Apostles, ch pter 12, verse 23)
To the clinical gastroe terologist and physicians ingeneral, intestinal helmi ths are, with a few notableexceptions, of less than outstanding interest whencompared with their prot zoal counterparts. Of thoseinvolving the small-intes .e, the more interesting areassociated with absorptio disturbances; numerically,however, hookworm dis ase and ascariasis dominatethe picture. The major elrninths in the context ofcolo-rectal disease are th various species of schisto-Somes, but because the a ult worms reside elsewhere~i.e. , in the portal system these can hardly be termedIntestinal helminth infe tions in the true sense.
Most reviews of this s bject are orientated aroundtaxonomic parasitologica classification (WHO, 1981;GILLES, 1984; GOLDS ITH & MARKELL, 1984;VARIYAM & BANWELL 1984). In common withseveral recent reviews ( OK, 1980, 1981, 1985a, b,c,.d, 1986) the clinical. portance of these helminthswIll be the dominant th me in this review. Clearlyt~eir importance varies and emphases are quitedifferent in developing' hird World' compared withwesternized countries. hereas hypochromic, iron-?eficient anaemia is num rically extremely importantID hookworm infections i the former it rarely causessuch problems in expatr ates who have usually been
676 SY MPOSIU M-GASTROINTESTINAL HELMINTH INFECTIONS
Anis his (see below) sometimes involve the stomach,as d es S. stercoralis in the hypochlorhydric subject(Co K, 1985c). Only a minority of helminths producecolo rectal pathology; in that situation nematodes aredo 'nant whilst cestodes are absent.
A though present throughout the world, low stan-dar s of sanitation (FEACHEM et al., 1983) and poorsoci -economic conditions are obvious predisposingfact rs to infection. Direct or indirect (e.g., as nightsoil) deposition of faecal material on to the ground isthe ajor factor responsible for infection. Therefore,rate of infection are often much higher in tropicalcom ared with non-tropical countries. Climatic in-flue ces-heat and humidity-per se are also relevant,Effe t on working capacitY is difficult to assess; manyof t e heaviest infections are in children. Managementcan be summarized: (i) environmental, includingsani ation-use of soil disinfectants etc., (ii) healthedu ation, (iii) chemotherapy, which can be separatedinto treatment of an individual, of the communitY(ma s treatment, selective chemotherapy, andtarg ted population chemotherapy), and (iv) aware-ness and participation in control by the local com-mu 'ty. An example of a control strategy for hook-wor infection (and consequent hypochromicanae .a) has been outlined (GILLES, 1985). Althoughthes aspects of control are important and must beapp ed concurrently (especially in the 'ThirdWor d'), this review will focus on clinical aspects,incl ding chemotherapy of the individual.
Sign cance of intestinal helminths in the 'Third World'T e more important intestinal helminth infections
caus major human illness in the 'Third World'(HA L et al., 1982; UDONSI, 1983; ELKINS, 1984;FAG, 1985). Rarely are accurate figures of infectionrate( ) available. One estimate of world incidencerates for infection is: hookworm one billion, round-wor 1.3 billion, strongyloids 90 million, whipworm750 llion, threadworm >500 million, (JANSSENS,1985 , Host susceptibilitY and number of reinfectionsper nit time are obviously important in pathogenic-ity. epeated and intensive infection is of paramountimp rtance in determining clinical significance, e.g.,in h okworm anaemia (LATHAM et al., 1982) andschi tosomiasis; although most individuals have lightinfec ions only, a minoritY harbour heavy loads.
C rebral cysticercosis, resulting from Taenia soliuminfec ions, is a locat problem and has been recently
ov
th
proc
th
laJ
an
pelit
m
so
m
D
oc
(SIWJ
st:
syes
nt
m
a
in
m
is
it(
ra
(0
ti(
pl
so
ec
PEec
ID
m
prth
th
fu
ac
m
lS
dt
0'
ly
fu
d(
cc
ti(
ca
gf
df
C}ar
ar
st
til
d1
UI
is
cc
re
rep.orted from W~st I~ian, after a. gift of pigs from BaliwhIch was heavIly mfected wI!h larval Cysticercuscellulosae. Severe burns resultIng from fits withsubsequent falls into fires caused significant mortalityIntestinal capillariasis caused a major problem in th~late 1960s in the Philippines after the infection hadnewly been introduced there.
Significance of intestinal helminths in the 'western' worldAlthough infection with some intestinal helminths
(e.g., hookworm, Ascaris, Trichuris, etc.) is notuncommon in travellers from the UK to the tropicsintensity of infection is usually not sufficiently high t~produce significant clinical symptoms and signs,Infections are usually revealed by routine screeningtests. However, over the last few years the importanceof parasitic infections-including helminths-has be-come apparent in the presence of immunosuppression(WONG, 1984). Although intestinal parasitoses areimportant in human HTL V III (LA V) infections,helminths are of minor importance compared withprotozoa. During the last few years, awareness thatpersisting Strongyloides stercoralis infection-causedby continuous autoinfection-can cause chronic intes-tinal and dermatological symptoms has been clearlydocumented (see below); immunosuppressed patientsare especially prone to a potentially fatal syndrome ofhyperinfection with this parasite.
Immigrant populations, however, not infrequentlyharbour intestinal helminths, many being nematodes,Schistosomiasis also is by no means uncommon in theminor ethnic groups in the UK. Cerebral cysticercosisis encountered as a rare complication of Taenia soliuminfection.
Helminths of the small-intestineI. Infections not associated with malabsorption
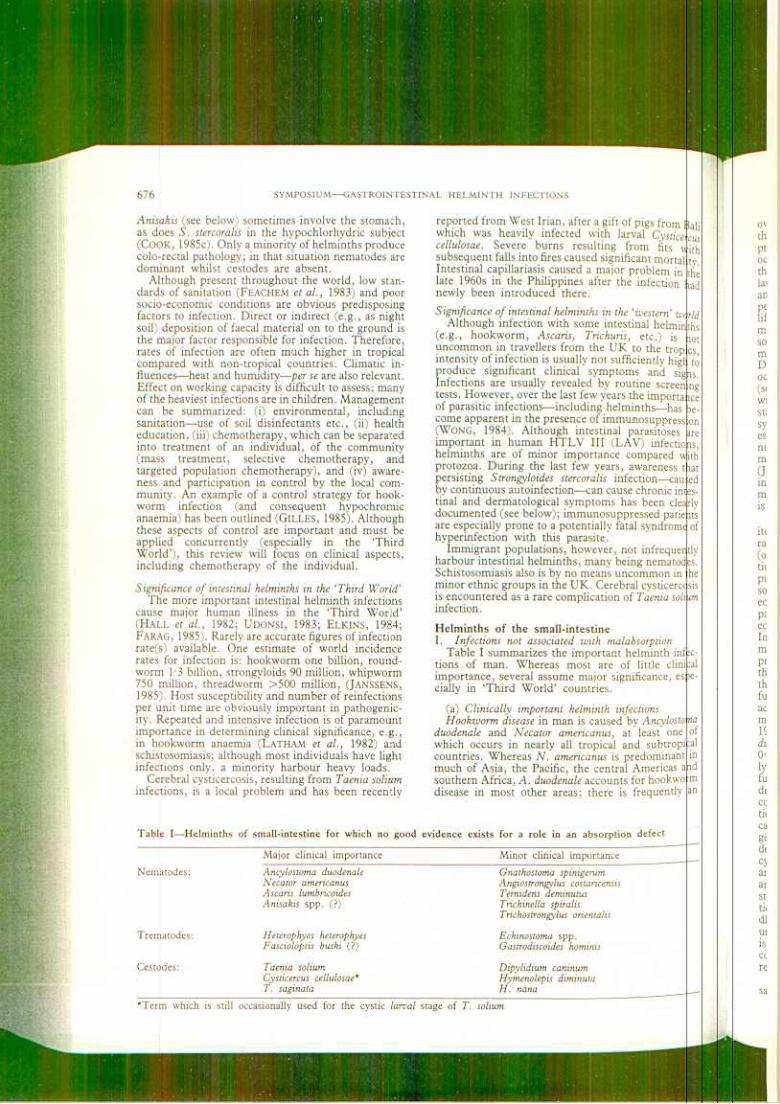
Table I summarizes the important helminth infec-tions of man. Whereas most are of little clinicalimportance, several assume major significance, espe-cially in 'Third World' countries.
(a) Clinically important helminth infectionsH ookworm disease in man is caused by Ancylostoma
duodenale and Necator americanus, at least one, ofwhich occurs in nearly all tropical and SUbtrOPIC,alcountries. Whereas N. americanus is predominant IDmuch of Asia, the Pacific, the central Americas andsouthern Africa, A. duodenale accounts for hookwormdisease in most other areas; there is frequently an
Tab If I-Helminths of small-intestine for which no good evidence exists for a role in an absorption defect
Major clinical importance Minor clinical importance
Nem~todes: Ancylostoma duodenaleNecator americanusAscaris lumbricoidesAnisakis spp. (?)
Gnathostoma spinigerumAngiostrongylus costaricensisT ernidens deminutusTrichinella spiralisTrichostrongylus orienlalis
Echinosloma spp.Gastrodiscoides hominis
Dipylidium caninumHymenolepis diminutaH. nana
Tre~atodes:
Cestqdes:
~
H eterophyes heterophyesF asciolopsis buski (?)
Taenia soliumCysticercus cellulosae*T. saginata
*Terln which is still occasionally used for the cystic larval stage of T. solium
G. C. COOK 677
overlap (HIM & P TEL, 1984). In parts of India andthe Philippines, A ceylanicum infection is also aproblem. Filarifor larvae penetrate intact skin withoccasional producti n of 'ground itch'-usually onthe feet of children (oral infection is also possible);larvae are easily k. ed by freezing and desiccation,and therefore signifi ant rainfall (usually >50 inchesper year) is require for their survival. The humanlife-cycle of the para ite results in the development ofmature adult worm in the duodenum and jejunumsome four to five w eks after initial infection; theymay still be present some five years or more later .During this initial p ase systemic manifestations areoccasionally encoun ered during tissue penetration(see below). Individ als can be divided into (i) thosewith a few adult wor s and no symptoms (the 'carrierstate'), and (ii) thos with many worms and severesymptoms and sign of hookworm disease. Oneestimate of sympto atology is ~s follows: wormnumbers, one to 25 il, 25 to 100 mild, loo to 500moderate, 500 to 1,000 severe; >1,000 extreme(JANSSENS, 1985). Cu rent knowledge of many factorsinvolved in the hos -parasite equilibrium containsmany deficiencies; th role of immunity in reinfectionis unknown,
Clinical manifestati ns include, therefore, 'grounditch' (pruritus) at the ite of initial infection (which israre); secondary inf ction of the localized lesion(oedema, erythema d a vesicular or papular erup-tion) is unusual. O casionally, but not often, apulmonary reaction ( ith bronchospasm) is trouble-some; minute, haem rrhages are accompanied byeosinophilic and leuc cy tic infiltration. Abdominalpain, diarrhoea (rarely with blood and mucus) and aneosinophilia may occu .Serum IgE may be elevated.In the small intestine, the adult worms attach to themucosa and cause .croscopic blood and serumprotein loss but not s'gnificant enterocyte damage;therefore malabsorpti is not a feature. Althoughthere is some evidence or a duodenitis (COOK, 1985a)further work is requ' ed. The clinical picture inadvanced disease is d minated by an iron-deficientmicrocytic anaemia d hypoproteinaemia (WHO,1981). Rate of blood 1 ss for N. americanus and A.duodenale is of the ord r of 0.03 to 0.05 and 0.16 to0.34 mI per worm per ay (WHO, 1981), respective-ly; however, a good de of iron is reabsorbed in thefunctional reserve of small-intestine. Clearly thedegree of anaemia is dependent on dietary ironcontent, body iron rese ves, and intensity and dura-tion of infection; the ances of a heavy infectioncausing severe anaemia therefore vary in differentgeographical locations. A mixed anaemia (folatedepletion being concurr ntly present, as in pregnan-cy) with megaloblastosis also sometimes occurs. Theanaemia may be accomp ied by systemic symptoms,and cardiovascular deco pensation can occur at a lates~age although in 'Thir World' countries presenta-Uon with haemoglobin c ncentrations of 1.0 to 2.0gdl-l in the absence of s' ns of cardiac failure is not~ncommon (COOK, 1980 .Although depigmentationIS common, koilonychia is very unusual in tropicalcOuntries. Oedema is a f rther clinical manifestation,resulting from hypoalbu naemia.
Diagnosis is by iden .fication of ova in faecalsamples (preferably usin a concentration technique)
or of adult worms in duodenal aspirates or jejunalbiopsy samples.
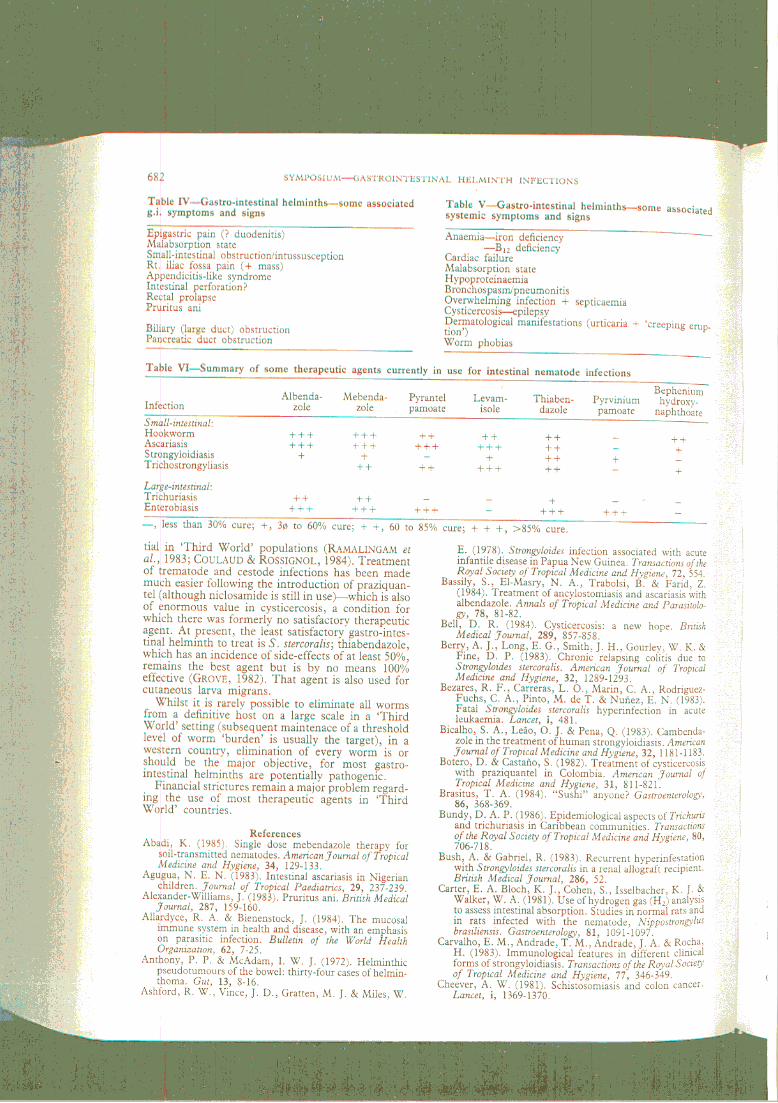
Treatment is straightforward, provided financialconstrictions allow the purchase of an effectiveanthelmintic. Whereas mebendazole and albendazole(CLINE et al., 1984) are probably the most effective(both have broad-spectrum anthelmintic activity) theyare too costly for many 'Third World' countries wheretetrachlorethylene has to be used. Anaemia should betreated with an oral iron preparation, e.g. ferroussulph~e--(rately is .an injectable iron preparationneeeSsary) and, even In severe anaemia, blood transfu-sion should be avoided for fear of precipitation ofcardiac failure (COOK, 1980); if folate depletion ispresent concurrently, oral supplements are indicated.
Ascaris: The large roundworm, Ascaris lumbricoides,is one of man's common parasites (MANNI, 1984). A.suum is morphologically identical and can also maturein man. Although infection is most common in thedeveloping 'Third World' (MARTIN et al., 1983), itoccasionally occurs in European countries includingthe UK (Lancet, 1985a). Occasional cases have beenreported in people who have not visited the tropics orsubtropics, and the reasons for this have beensummarized: (i) holiday travel abroad, (ii) infectionacquired from immigrants, (ill) imported vegetablesor fruit as a source, and (iv) contact with pigs andacquisition of an A. suum infection (LoRD & BUL-LOCK, 1982). A recent estimate in a world context is7800 million (Lancet, 1985a).
Ova (which are resistant to cold and disinfectants)are ingested by man from faecally contaminated soiland, after hatching in the small-intestine, minutelarvae are liberated which penetrate blood and lymphvessels in the gut wall; some are carried to the liver viathe portal circulation, whilst others pass through thethoracic duct. Present understanding of host im-munological mechanisms involved in ascariasis has
, been reviewed (WHO, 1981). When they reach thelungs (4 to 16 days after infection) they perforate thealveolae and severe pulmonary symptoms (Ascarispneumonia) may ensue; Loeffler's syndrome consistsof fever, productive cough, eosinophilia and radiog-raphic evidence of pulmonary infiltration. At the endof their life-cycle they reach the small-intestine, wherematuration takes place.
Children are frequently infected (AGUGUA, 1983;EL-MASRY et al., 1983), and growth may be affected(Nutr. Rev., 1981, 1983). However, as with hook-worm infections, no conclusive evidence for interfer-ence with malabsorption has been demonstrated(Nutrition Reviews, 1983). Adult A. lumbricoides cancause obstruction at various sites. A mass of worms(up to 1000) can produce small-intestinal obstruction-usually at the ileal level. Whilst volvulus,intussusceptIon, gangrene of the small-intestine,appendicitis and intestinal perforation have all beenreported (COOK, 1980), obstruction to the biliarysystem and pancreatic duct are especially importantcomplications. Biliary ascariasis is especially impor-tant in childhood (LLOYD, 1981). In a prospectivestudy in India, 40 (36.7%) of 109 patients with biliaryand pancreatic disease had evidence of ascariasis as anaetiological agent (KHUROO & ZARGAR, 1985); in 90%symptomatic treatment and anthelmintics led to cure,whilst four required surgery .If the technique is
68~ SYMPOSIUM-GASTROINTESTINAL HELMINTH INFECTIONS
in olved. Prolonged severe diarrhoea complicated byhy okalaemia and cardiac arrest has also beendo umented (KANE et at., 1984); the precise mechan-is of the absorptive defect is unclear .The relatedsp cies S. fuettebomi also causes severe malabsorp-ti n, especially in children (COOK, 1980). Mostre orts are from Zambia (HIRA & PATEL, 1984) andP ua New Guinea (ASHFORD et at., 1978). Radiolo-gi al changes during barium studies of the small-in estine can be striking. Diagnosis is by finding1 vae and sometimes ova in faecal samples. Alterna-ti ely the 'Enterotest' (string-test) by which theor anism can be recovered from jejunal fluid is av uable diagnostic technique (PENALBA et at., 1984).S rological diagnosis is also useful (GROVE & BLAIR,1 81; SATO et at., 1985). During tissue invasion ane inophilia (which may be gross) may accompany the'a ergic' manifestations which include an itchye thematous and/or urticarial rash, and pulmonaryin olvement. An important complication is over-w elming infection (IGRA-SIEGMAN et at., 1981;G NTA, 1984; HARPER et at., 1984) which can occurin immunosuppressed people (SHELHAMER et at.,1 82)-i.e. those receiving corticosteroids, and othersw th acute leukaemia (BEZARES et at., 1983), lympho-
s, leprosy, systemic lupus erythematosis, renalsplants (BUSH & GABRIEL, 1983), malnutrition,
e .(HOOPER et at., 1982; CARVALHO et at., 1983).T e disease can also be a problem in geriatric practice( ALZER et at., 1982). A Gram-negative septicaemiaa sociated with this syndrome, which has multi-organ.volvement, can prove fatal if treatment is not..tiated promptly; a paralytic ileus is often present. A
gh incidence of human T -cell leukaemia virus( TL V) has been reported in S. stercoratis carriers( AKADA et at., 1984); this is probably merely ar flection of a general impairment of immunity in thep esence of chronic infection with this parasite (GILL
BELL, 1984). As an experimental model of strongy-1 idiasis, Nippostrongytus brasitiensis infections in ther t have proved of considerable value (CARTER et at.,I 81). Treatment is with thiabendazole; mebendazolei an alternative agent which is of some value( RAVAK et at., 1983) and claims for cambendazole
ve also been made (BICALHO et at., 1983).Capillariasis is confined to the northern Philippinesd Thailand (SINGSON et at., 1975). As with S.
s ercoratis infections, autoinfection can occur andalabsorption, which may be gross, can lead to
t: talities within a couple of months or so. The diseasei contracted by consuming raw fresh-water fish; a
sh-bird cycle might be important epidemiologically( ROSS & BASACA-SEVILLA, 1983). Men of 20 to 50ears of age are especially predisposed, and the
disease can be epidemic with auntreated. As with s .worms can be -fiU1cosa, but other sections of the
best therapeutic agent available, although thiabenda-zole is also effective.
Metagonimus yokagawai infections
There is however some evidence, ,they can produce a malabsorptive state; further workis required.
Although Diphyllobothrium latum, the fish tape-worm, can occasionally induce vitamin Bl2 malab-sorption (with resultant megaloblastic anaemia) this isan unusual event. Adult worms measure up to 10metres in length. Although this infection, which isacquired through ingestion of raw fish includingsalmon (RUTTENBER et al., 1984), is often consideredto be confined to cold areas, e.g., Finland, and in, ' in
tropical countries.
symptoms occasionally occur .from symptoms associated with anaemia.Bl2 deficiency probably results from abetween helminth and host, and is not thereforestrictly an example of helminth-induced malabsorp,tion. In severe disease, subacute combined degenera-tion of the spinal cord has been reported. Ova andproglottides are detected in faecal samples. Niclosa-mide and praziquantel are of value in treatment.
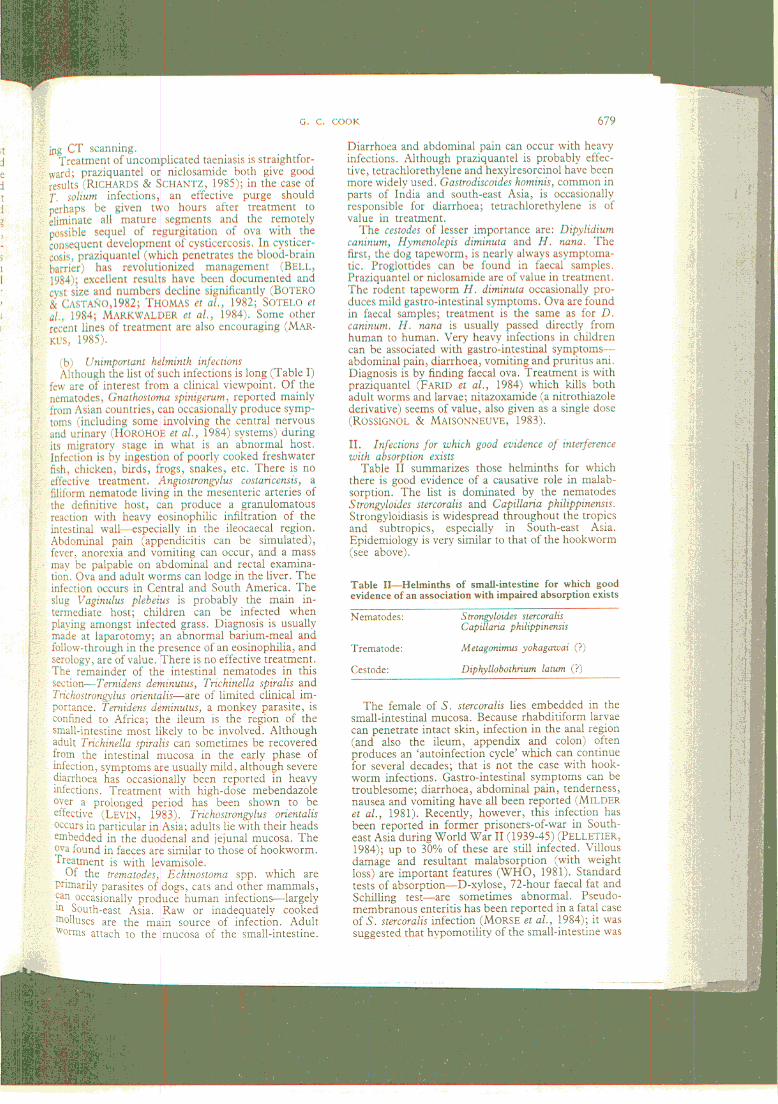
Although suggestive evidence has been produced,there is no clear evidence of small-intestinal disease inSchistosoma mansoni infections (FEDAIL & GADIR,1985).
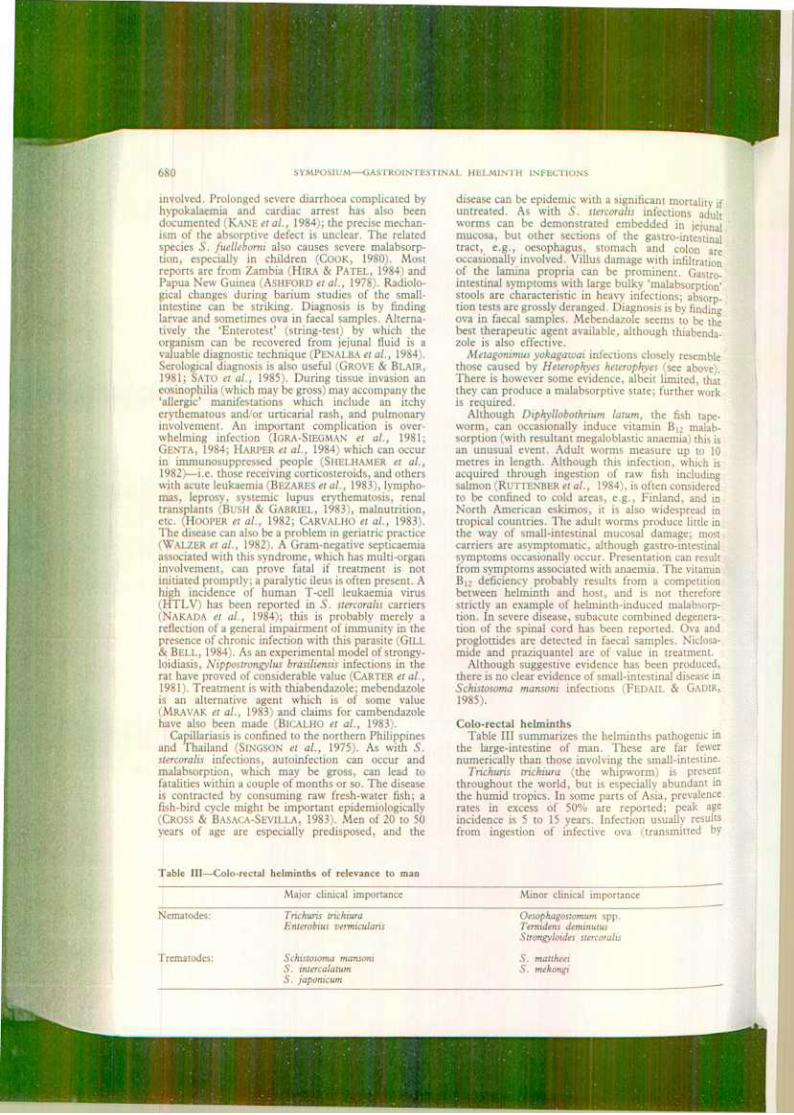
Colo-rectal helminthsTable III summarizes the helminths pathogenic in
the large-intestine of man. These are far fewernumerically than those involving the small-intestine.
Trichuris trichiura (the whipworm) is prese?tthroughout the world, but is especially abundant Inthe humid tropics. In some parts of Asia, prevalencerates in excess of 50% are reported; peak ageincidence is 5 to 15 years. Infection usually resultsfrom ingestion of infective ova (transmitted by
able IlI-Colo-rectal helminths of relevance to man
Major clinical importance Minor clinical importance
*ematodes Trichuris trichiuraEnterobius vermicularis
Oesophagostomum spp.T ernidens deminutusStrongyloides stercoralis
S. mauheeiS. mekongi
Schistosoma mansoniS. intercalatumS. japonicum
trematodes:








![HELMINTH PARASITES IN MAMMALSparasite.org.au/para-site/text/helminth-checklist.pdf · HELMINTH PARASITES IN MAMMALS ... Subclass: EUTHERIA [placental mammals] ... NEM:Asc Ascaris](https://img.pdfslide.net/doc/110x75/5ad4fa137f8b9a5d058c90e9/helminth-parasites-in-parasites-in-mammals-subclass-eutheria-placental-mammals.jpg)

![HELMINTH PARASITES IN MAMMALS - Australian …parasite.org.au/para-site/text/helminth.pdf · HELMINTH PARASITES IN MAMMALS ... Subclass: EUTHERIA [placental mammals] ... NEM:Asc Ascaris](https://img.pdfslide.net/doc/110x75/5b78c38f7f8b9a331e8c41aa/helminth-parasites-in-mammals-australian-helminth-parasites-in-mammals-.jpg)


















