Embed Size (px)
Citation preview

Gastrointestinal Surgery & Peri-Operative Nutrition Support Case Study-P.L. 5/26/2015 Sodexo, Allentown Salome Rao

- 1 -
Introduction
The reason behind selecting P.L., as a patient for my case study research, was apprehension for
the patient’s extended length of stay at the facility, being supported solely by Total Parenteral
Nutrition (TPN), while not meeting her postoperative nutritional needs. This patient initially
underwent small bowel resection due to ischemic bowel that was caused by a ventral incisional
hernia. Over the following months, this surgery led to several complications, including a number
of enterocutaneous fistulas. We were increasingly concerned about the patient’s gut atrophying,
while being on long term TPN and thus researched Medical Nutrition Therapy (MNT) options to
potentially improve recovery time, advance to a regular diet and have a prompt discharge from
the hospital.
This case enabled us to explore medical nutrition therapy options to potentially accelerate
recovery time, even while on TPN. We recommended increased rates and amino acid
concentration, in order to better meet the patient’s nutritional needs. In addition, we researched
into alternative TPN formulation options, currently not being utilized in the facility where this
patient was being managed. For example, TPN formulations modified or supplemented with
additional nutrients such as omega-3 oils, Glutamine or Branched Chain Amino Acids (BCAAs)
that potentially can speed up recovery. These formulations have either been studied in a research
setting or are being utilized in other facilities and abroad. In addition, we explored whether it
was necessary for this patient to remain on TPN for such an extended time, or whether it would
have been possible to start early oral feedings and have prevented further complications. Finally,
nutrition support was an area in which I had little expertise and this was an opportunity to
investigate recent advances in peri-operative support of GI surgery.

- 2 -
Abstract
P.L was admitted to the hospital on October 5th
, 2014, with a diagnosis of strangulated recurrent
incisional ventral hernia, small bowel obstruction, ischemic and perforated bowel. The patient
was placed on IV antibiotics and underwent small bowel resection with primary anastomosis.
Post surgery the patient was placed on TPN for an extended period of time and developed
multiple complications. The patient developed peritonitis, leukopenia and sepsis, possibly due to
an infected mesh that remained within her abdomen from a previous surgery. Furthermore, she
developed multiple fistulas which were leaking externally, were operated on, but the wounds
were not spontaneously healing. Therefore, a wound vac was placed to aid in the closure of the
external wound. The patient remained on TPN throughout her four month stay at the hospital,
with minimal attempts to oral feed. After a thorough review of recent literature on peri-operative
GI management, we believe that an alternative nutrition support protocol would have been
beneficial in this patient’s recovery. A combination of oral feedings including
immunomodulators, such as arginine, glutamine, fish oils and nucleic acids, as well as an early
recovery after surgery (ERAS) protocol, would help promote wound healing, promote normal
gut function, and reduce this patient’s length of hospital stay.

- 3 -
Discussion of Medical Condition
Incarcerated Incisional Hernia
A hernia is a defect or hole that allows the protrusion of an organ or other tissue through it
(Ansari P., The Merck Manual). A previous surgical incision, that has failed to heal completely,
can result in an incisional hernia. Sometimes these also called ventral hernias, since they occur in
the front part of the body. Patients who have undergone a non-laparoscopic, open surgery have
approximately a 15% chance to develop an incisional hernia at the site of incision. Obesity
creates more pressure on the abdominal wall, compromising healing, and thus promoting
herniation of the intestine through the abdominal wall. In addition, a loop of the intestine can
become incarcerated or trapped within the opening, and could be asymptomatic, or could result
in persistent pain. On occasion, nausea, vomiting and fever can be additional symptoms. In
order to create a strong hernia repair, it is recommended to place an intra-abdominal ventral
mesh on the underside of the abdominal wall. This mesh is usually made of woven nylon, and
fuses with the abdominal wall, reinforcing the suture repair. The larger the surface area of fusion
between the abdominal wall and the mesh, the stronger the hernia repair.
Small bowel obstruction (SBO)
An obstruction is a partial or complete blockage that prevents food, fluid or gas to move through
the intestine (Nobie, B., Emedicine). Mechanical obstructions can be caused by twisting of the
intestine, hernias or intussusceptions where the intestine folds like a telescope onto itself or other
areas of the intestine. Other causes are tumors, diverticulitis or Crohn’s disease which can result
in the narrowing of the intestinal lumen. In the large intestine tumors or severe constipation
causing impacted hard stools, are the most often cause for obstruction. Post-operative small-

- 4 -
bowel obstruction is also a common complication of GI and abdominal surgery, whereby fibrous
tissue, adhesions or scarring, form after surgery. Strangulated small bowel obstructions are
most commonly associated with adhesions. Postoperative adhesions can result in obstruction
within four weeks of surgery. The incidence of SBOs parallel the number of laparotomies,
currently being the preferred mode of surgery when feasible. Symptoms of SBO can be
manifested as crampy, intermittent abdominal pain, nausea, diarrhea, constipation and abdominal
distention (The Mayo Clinic). Fever and tachycardia are most often associated with intestinal
strangulation. Nasogastric decompresion is a procedure to relieve abdominal distention by
placing a nasogastric tube through the nose and into the stomach to remove trapped air or fluids
causing the swelling and discomfort. The use of nasogastric decompression has been debated
more recently (Willcuts, 2010). In the cases of partial obstruction where food and fluid can still
pass through the intestine, one may not need surgery and a low-fiber diet may be sufficient to
allow the obstruction to clear on its own. If nothing is able to pass through the intestine, a self-
expanding metal mesh stent may be utilized to expand the lumen. Surgery is often necessary,
however, to remove the section of the intestine with the blockage, especially if that section is
damaged or necrotic. Small bowel obstruction accounts for 20% of all acute surgical admissions.
With proper diagnosis and prompt treatment, the prognosis of SBO is good. If not treated in a
timely manner, however, SBOs can lead to ischaemia, rupture, sepsis and death.
Ischaemic Bowel Disease; Peritonitis
There are several potential causes of intestinal ischaemia, or decreased blood supply, to a section
of the intestine (Cleveland Clinic). As described above, the intestine can move into an
abdominal opening or hernia or get tangled within scar tissue or adhesions from past surgery.
Other reasons for bowel ischaemia are arterial or venous thrombosis, embolus or low blood

- 5 -
pressure, but these were not the case with our patient. The incarceration of the intestine within a
hernia can lead to strangulation which means that the intestine is trapped and twisted inside the
hernia (Fig. 1) and blood supply is interrupted. Strangulated hernias and small bowel
obstructions can be fatal if not attended to as soon as possible, because gangrene can develop
within hours (Merck Manuals).
The intestinal wall becomes necrotic, ruptures, and can lead to peritonitis. Peritonitis is an
inflammation of the serous membranes of the peritoneum, the membrane that lines the inner
abdominal wall and covers the inner abdominal organs, including the intestine (Mayo Clinic
Staff, The Mayo Clinic). Peritonitis is most often due to pathogenic microorganisms, such as
bacteria or fungal infections. Signs and symptoms include abdominal pain and distention, fever,
nausea and vomiting, loss of appetite, diarrhea, low urine output, thirst, and fatigue.
Spontaneous peritonitis can occur without an abdominal rupture, usually due to an
immunocompromised state, and mostly seen in patients with chronic liver disease. Injury or
trauma can also cause bacteria from other parts of the body to enter the peritoneum, resulting in
an infection. Once one has had peritonitis, they have a higher risk of developing it again, as
Figure 1.
Schematic of intestinal
strangulated hernia. The
ischaemic and necrotic part
of the intestine can be seen
protruding from the
abdominal wall.

- 6 -
compared to someone who has never had peritonitis. If peritonitis is not attended to as soon as
possible, it can extend beyond the peritoneum and cause bacteremia (bloodstream infection) and
sepsis which is infection throughout the body. Sepsis is life-theatening and can result in multiple
organ failure, septic shock and death. Patients older than 65 years have a 3-fold increase of
developing generalized peritonitis and sepsis from perforated bowel than younger patients
(Daley et al., 2015). Treatment of peritonitis most often involves the use of systemic antibiotics
and sometimes surgery. It is essential to also treat any underlying medical condition, such as a
necrotic and ruptured bowel which is leaking contents into the abdominal cavity. Surgery of the
underlying condition will be essential in order to eliminate the infection.
Small bowel resection with primary anastomosis
Small bowel resection can remove the necrotic part of the intestine and is performed under open
surgery. The necrotic part of the intestine is located and removed by clamping off the two ends
of the diseased section. Following removal of the dissected portion, the surgeon performs the
anastomosis (Fig.2). During this procedure the two healthy sides of the small intestine are re-
attached. In cases where there is not enough of the small intestine remaining, in order to reattach
the two ends, a surgeon may need to perform an ileostomy. If the section of the intestine
remaining is less than 100 cm, it can result in short bowel syndrome, but this was not the case
with our patient. In some cases a short or long-term ileostomy, as mentioned above, or a
colostomy may be necessary, but these were not procedures performed on our patient.

- 7 -
Intestinal Anastomosis
Diffuse post-operative peritoneal adhesions are connections via scar tissue between sections of
the intestine and/or the intestine and the peritoneal lining of the abdominal wall. These adhesions
form after surgery as a normal response to injury during surgery. They are beneficial in the case
of healing, but they can also cause severe and chronic abdominal pain, and potential
complications during subsequent abdominal surgeries. As mentioned above, adhesions are the
most common cause of bowel obstruction and should be suspected in any patient with a history
of prior abdominal or pelvic surgery who present symptoms of bowel obstruction. Meticulous
surgical technique and prevention of tissue damage is the first measure of prevention of
adhesions. Surprisingly , both laparoscopic and open abdominal surgeries, result in similar rates
of adhesions. During a follow-up surgery, the surgeon will try and remove as much as possible
of these adhesions, by a procedure called adhesiolysis (or enterolysis in cases where the intestine
is also involved), by cauterizing the adhesions between healthy tissues. More recently, certain
materials and pharmacologic agents have been evaluated in preventing or reducing these post-
surgical adhesions, while the initial surgery is performed. Oxidized regenerated cellulose
(Interceed) , expanded polytetrafluoroethylene (GoreTex) or hyaluronic acid sheets can act as
Figure 2. Schematic of an intestinal
anastomotic procedure.

- 8 -
barriers between organs and tissues. GoreTex sheets, however, even through more effective than
Interceed, require a second operation for removal (Farguhar et al., 2000). In addition,
polyethylene glycol (PEG), hyaluronic acid solutions and gels or icodextrin sodium, can form
liquid, as compared to solid, barriers. Convicing data on their efficacy, however, is still emerging
and according to a review by Uptodate, intraabdominal fluid solutions and antithrombotics are
not recommended because they are ineffective and potentially harmful. More reseach is essential
on the efficacy and safety for these agents.
Enterocutaneous Fistulas
Fistulas are abnormal communications or tunnels between two epithelialized surfaces and are
classified based on anatomy, physiology or etiology. The anatomies of fistulas also suggest
causation and physiological classification is based on fluid output, mostly external drainage of
enteral contents, in milliliters per day. High output fistulas, originate most often from the small
bowel and have outputs of over 500 ml per day, moderate fistulas have outputs between 200-500
ml per day and low output fistulas are more likely of colonic origin, with outputs of less than 200
ml.
With improved health conditions in modern times, the occurrence of spontaneous fistulas has
decreased dramatically, and currently post-operative fistulas account for approximately 80% of
all fistulas. These occur more frequently following cancer or IBS surgeries and lysis of
adhesions. Post-operative fistulas form within 5-6 days of operation and are associated with
fever and post-op ileus. Post-operative ileus, is failure to restore adequate bowel function post-
operatively. The treatment of fistulas involves five overlapping phases: recognition and
stabilization, investigation, decision, definitive therapy and healing (Pritts et al., 2001).

- 9 -
1. Within 24-48 hours recognize and stabilize to correct fluid and electrolyte imbalances,
control fistula drainage, ensure adequate skin care and initiate aggressive nutrition
support.
2. After 7-10 days, investigation to determine anatomy and fistula characteristics.
3. By 4-6 weeks determine the likelihood of spontaneous closure and decide course of
therapy.
4. If closure is unlikely then continue with surgical closure of the fistula, reestablish GI
continuity and secure abdominal closure.
5. Five-ten days after closure ensure long term adequate nutritional support and transition to
oral intake.
Early Recovery After Surgery (ERAS)
The ERAS protocol is a more recent approach to reduce surgical stress and enhance overall
recovery, and most of the data for this protocol have been based on GI surgery patients and has
originated in Europe. Use of ERAS protocols results in earlier return of GI function and shorter
hospital lengths of stay by 1-4 days (Walter et al., 2009). This protocol involves extensive
preoperative counseling, no bowel per-op preparation, antibiotic prophylaxis, limited
preoperative fasting, selective use of nasogastric tube and decompression, early feeding and oral
supplements, from day one of surgery, gum chewing for 30 minutes TID and early ambulation.
Gum chewing can act as sham feeding and stimulate the cephalic phase of digestion, increasing
GI secretions, increase motility and reduce post operative ileus. Select ERAS protocol
interventions that have been adapted by a number of hospitals in the US are early ambulation,
early diet progression, early removal of NGT, the overall use of the ERAS protocol is still rare in
the US (Delaney et al. 2010). This review was from five years ago, however, and currently there
may be more extensive adaptation of the protocol.

- 10 -
Discussion of Medical Nutrition Therapy
Perioperative nutrition, includes not only post-operative care, but also nutritional assessment
before the operation, and is critical for the positive outcome of patients undergoing abdominal
surgery. According to research of patients who have undergone anastomosis, early postoperative
enteral feeding, is not only safe but also associated with significant benefits (Osland et al., 2010,
Warren et al. 2011, Lee et al., 2014). As mentioned previously, a common part of recovery after
gastrointestinal surgery is post-operative ileus, which is failure to restore adequate bowel
function. Contrary to older theories of recommending “nil by mouth” (NPO) post-operatively,
until bowel function has resumed, early initiation of oral diet has shown to improve peri-
operative management. The traditional regimen prior to GI surgery, such as small bowel
resection and anastomosis, is to follow a clear liquid diet, consisting of foods such as broths,
clear juice and water. In addition, the day before surgery a patient has been required to be NPO
(nothing by mouth) after midnight. By the second or third day after the procedure, these patients
are most often able to consume clear liquids, which will slowly be advanced to thicker liquids
and GI soft foods, as the bowel begins to return to normal function. This regimen of clear liquid
diet, even though well tolerated, it does not provide adequate nutrients for post-op recovery. A
review by Willkutts, 2010, on Pre-Op NPO and traditional post-op diet advancement, states that
bowel sounds, which are used to determine readinesss for oral intakes, are an unreliable marker
of normal bowel function, because bowel sounds may or may not be present with normal bowel
activity. She also states that feeding may be helpful in reducing post-operative ileus by
stimulating bowel motility. A prospective, randomized, controlled trial by Boelens, et al.,
(2014), showed that early enteral feedings (within 8 hours of operation) of patients undergoing
major rectal surgery, as compared to parenteral nutrition, reduced postoperative ileus. An

- 11 -
unexpected finding in this study was that the group on parenteral nutrition demonstrated
increased rates of anastomotic leakage, as compared to the group fed enterally. In addition the
mean length of hospital stay was 13 (for enterally fed) vs. 16 days for the PN patients. This
study was performed in patients undergoing surgery for rectal cancer and the authors state
uncertainty whether this would also apply to more promixal GI surgeries.
A meta-analysis of 29 trials, including 2,552 patients, showed that enteral vs. parenteral nutrition
in GI surgery was beneficial in reducing post-op infection, anastomotic leaks, intraabdominal
abcesses, and duration of hospital stay (Mazaki et al., 2008). Enteral compared to parenteral
feeding did not show benefits however, in respiratory failure or pneumonia, UTIs and wound
dehiscence. An additional meta-analysis of thirteen trials involving a total of 1,173 patients
undergoing GI surgery (Lewis et al., 2009), compared early post-operative feeding (within 24
hours of operation) with no feeding (NPO). In this meta-analysis early enteral nutrition was
associated with reduced mortality; the authors stating the mechanism not being clear. Early post
op feeding in some of these studies was associated with increased vomiting.
In summary, there are numerous studies and multiple meta-analyses reviewing those, indicating
that early postoperative feeding of patients undergoing GI surgery is associated with improved
outcomes and reduced lengths of stay in the hospital. According to a statement by Schulman and
Sawyer in an editorial in 2005, even though these studies support early post-operative feedings
following bowel surgery, it is likely that it will take several years before this will become the
accepted norm. One decade later, even though there is enough data to support the benefits, early
post-operative feedings are still not considered the routine path to proceed by after GI surgery.

- 12 -
In the cases where oral or enteral feedings are not being tolerated, then parenteral nutrition will
be necessary. Alternatively, oral, enteral and parenteral routes may be best used in combination
to achieve the best nutritional status (Woodcock et al. 2001).
Formulation Approaches
In addition to introducing early enteral nutrition postoperatively, the composition of the enteral
formula is also important. Immunonutrition is defined as enteral nutrition composed of at least
two of the three components: the amino acids Arginine and/or Glutamine, Omega-3 fatty acids
and nucleic acids, otherwise referred to as immunomodulators. According to a review by
Moskovitz and Kim, 2004, perioperative enteral diets containing immunomodulators, taken 5
days pre-operatively, decreased postoperative infections and length of hospital stay. More
recently, a review by Braga M., (2012) summarized the results of several meta-analyses and
concluded that perioperative immunonutrition should be implemented in patients undergoing
elective GI surgery, because of data showing reductions of post-op morbidity and lower costs to
the healthcare system. Braga recommends that larger trials are required before recommending
the same for head and neck surgeries. An additional meta-analysis of immune-modulating
nutrition of patients undergoing major open abdomen elective GI surgery by Marimuthu et al.
2012, concludes that immunotherapy was beneficial for reducing postoperative complications,
infectious and non-infectious, and reduced hospital length of stay (LOS). The feeding formulas
used by these studies were IMPACT®, STRESSON, RECONVAN and ALITRA Q and were
provided pre and post operatively for 5-7 days, most of which were administered pre-operatively.
According to Nestle Health Science, in a prospective randomized clinical trial of GI cancer
surgery patients, those who received IMPACT formula perioperatively had a 57% lower
complication rate vs. control (p<0.02) and well as reduced mean LOS. Complications noted were

- 13 -
respiratory and wound infections and anastomotic leaks. IMPACT® is a formula supplemented
with Arginine, n-3 fatty acids (EPA and DHA) and nucleotides and is available for oral
consumption and as a tube feeding formulation.
Lipids have traditionally been used in nutrition support, to provide calories, building blocks and
essential fatty acids, and have been based on n-6 lipids such as soybean oil. The type of lipid,
however, used in nutritional formulations, may affect levels of inflammation. More recently the
addition of fish oils has been shown to be beneficial additions to enteral as well as parenteral
nutrition. Immune function and inflammatory pathways are enhanced, thus improving outcomes
and reducing length of stay in ICU and the hospital. Furthermore, pre-operative nutrition support
may be even more beneficial than post operatively. Allternatively, if omega-3 oils are not
available, to avoid the immunoppresive effects of omega-6 lipid formulations, it is recommended
to provide PN without lipids during the first week of therapy.
Enhanced Recovery After Surgery (ERAS) protocol/ Carbohydrate loading
As previously described, this protocol makes use of early feedings peri-operatively, with very
limited pre-operative fasting. Solids are allowed until six hours prior to surgery and clear liquids
up until two hours before surgery. Oral supplements are provided 2-3 times a day from the day
of surgery until normal oral intakes are achieved. An additional component of the ERS protocol
involves the use of high-carbohydrate glucose drinks pre-operatively (Akbarshahi et al, 2008).
This approach has been shown to reduce the impact of surgical stress to the patient and involves
the consumption oof 800 ml of a 12.6 gm carbohydrate /100 ml the night before surgery and 400
ml of the same solution 2-3 hours prior to surgery. Benefits include reduced post-operative

- 14 -
thirst, less hunger, reduced anxiety. Additional effects are reduced post-operative insulin
resistance, reduced glycosylation of muscle and preserved lean body mass.
Glutamine
Given that our patient was on TPN for extended periods of time, an alternative approach would
be to supplement her TPN with Glutamine to promote GI and fistula wound healing. According
to a review by McClave et al., (2013), supplementing PN with parenteral glutamine is
recommended to maintain gut integrity from the serosal side, and serve as a systemic antioxidant.
Many of the studies showing positive results have used the glutamine dipeptide, however, which
is currently not available in the US. L-Glutamine, which is available in North America is
unstable, of limited solubility and limited for clinical use.
A most recent approach presented by Nutricia at the New Jersey Dietetic Association meeting,
on May 13, 2015, was the use of citrulline to promote wound healing. Citrulline is a safe means
of providing arginine for nitric oxide production which is essential for wound healing. Nutricia
recommends citrulline in tandem with Arginine as a strategy to promote wound healing under
conditions requiring additional arginine. In addition Citrulline is better tolerated than Arginine
with no GI distress up to 15 gm/dose.

- 15 -
Presentation of the patient
Pt Initials: P.L. D.O.B: 11/12/1947 Age: 67 Sex: F
Admit Date: 10/5/2014 Discharge Date: 02/12/2015
Diagnosis:
Strangulated Ventral Hernia
Perforation of Bowel
S/P Small Bowel Resection
Peritonitis
Recurrent Enterocutaneous Fistula
Sepsis
Severe Anemia of Iron Deficiency
Hypertension
Hypothyroidism
Leukopenia
Past Med hx:
Sixty seven year old African American female with complex past abdominal surgical history.
The patient is also with a past medical history significant for obesity, GERD, hypertension,
hypothyroidism, diabetes and congestive heart failure. This patient has had a
choledochoduodenostomy, cholecystectomy and a ventral hernia repair with partial small bowel
obstruction in 2012. In 2013 the patient had exploratory laparotomy, four abdominal wall
hernias and extensive enterolysis to repair dense peritoneal adhesions.
Family hx: Non-contributory
Social Hx: She is a non-smoker, non-drinker; Born in Aruba; Lives with her brother;
Unemployed; Drinks Socially; No recent travel

- 16 -
P.L. was presented to the hospital with severe abdominal pain that had been present for two days
and was hypokalemic with a potassium value of 2.0. A CT scan of the abdomen and pelvis
demonstrated a possible strangulated incisional recurrent hernia and ischemic bowel. A
laparotomy was performed which revealed an incisional ventral hernia, peritonitis, which
presented no foul smell, and ischemia of the intestine, due to strangulation within the hernia.
The patient’s abdominal cavity was irrigated with 10 L of warm sterile saline. The small
intestine appeared normal from the ligament of Treitz to the ileocecal valve. The right and left
colon could not be visualized, as they were covered under adhesions. The mesh that was present
on the anterior abdominal wall was well incorporated into the wall and was left untouched by the
surgeon. The hernia was repaired and a ¼ in Penrose drain was left subcutaneously.
After extensive enterolysis was performed to remove intestinal adhesions, a 1.5 inch ischemic
segment of the small intestine was isolated, which per physician’s notes, was strangulated within
the patient’s hernia. This segment had a 1.5 cm perforation and intestinal content was leaking
into the abdominal cavity. This ischemic and damaged part of the intestine was resected and
primary stapled anastomosis was performed.
The patient was placed in ICU on IV antibiotics, and hyperalimentation via TPN.
One month later fecal material was draining from the lower end of the incision. The patient was
diagnosed to have incurred a fistula and underwent an enterocutaneous fistulectomy. During this
surgery the infected mesh was explanted. One month later the patient underwent an exploratory
laparotomy to close the enterocutaneous fistula, which was not healing, and was treated by
application of a wound vac.

- 17 -
Table 1. Patient Medications
Medication
Brand Name
Generic
Name
Indication(s) Food/Drug
Interaction(s)
Nutritional
Implication(s)
Augmentin Amoxicillin/
Clavulanic Acid
Antibiotic none Abdominal
discomfort
N/V/D
Protonix Pantoprazole Proton pump
inhibitor,
GERD
none Risk of
hypomagnesemia,
hyperglycemia
Synthroid Levothyroxine Hypothyroidism none Weight loss, N/V/D
Bacid Lactobacillus
Acidophilus
Probiotic, replaces
intestinal flora,
controls diarrhea
none Contains milk
products-Potential for
milk/lactose allergy
Zofran Ondansetron Antiemetic
Prevent post op
N/V
Food
increases
medicine
absorption
Diarrhea/constipation
Norvasc Amlodipine Antihypertensive Grapefruit
juice
Edema
Mag-Ox Magnesium
Oxide
Antacid none D/N
High Mg,
Low protein, Ca, K

- 18 -
10/5/14 12/28/14 2/10/15
Na 140 138 136
K 2.9 3.5 5.3H
BUN 13 18 12
CR 0.6 1.1H 0.9
HA1c --- 6.5H ---
Glucose 247H 160H 115
H/H --- 9.7L/29.6L 8.9L/28.7L
CO2 31 24 24
GFR >60 53L >60
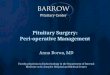
Figure 3. Patient BMI decreased by 21.5% over the patient’s stay at the hospital, from a
classification of Obese II to Obese I.
20
25
30
35
40
10/12/2014 11/12/2014 12/12/2014 1/12/2015
BM
I
Change in Patient BMI over Time
P.L.’s lab values are WNL except
for some indication for anemia,
with H/H trending low. Pt blood
glucose values improved during her
stay. According to her GFR values
her kidney function is normal.
P.L. was hypokalemic when she
was fist admitted to the hospital,
but her potassium values were
brought to slightly above normal by
the end of her hospital stay.
Table 2. Laboratory Values

- 19 -
Nutrition Care
After the initial surgery of resection and anastomosis, the surgeon prescribed a TPN regime
(Table 4). This patient had an excellent appetite and did not have any complications with her
upper GI. In addition, the segment of the bowel resected was very small (1.5 in). We were
therefore uncertain why an oral GI soft diet, had not been prescribed. Extended periods on TPN
can result in gut atrophy and for this reason, utilizing the gut ASAP after surgery is
recommended, as previously described. The patient also presented with a Stage 2 Sacral
pressure ulcer, further increasing her protein requirements. The patient complained of taste
changes while on TPN; this may sometimes be a side effect of TPN. The RD recommended
increases in nutrition support rates, and amounts of amino acid and calories, as seen in Table 4.
In addition the RD recommended initiation of oral feedings, but the recommendations did not go
into effect. Table 5 shows the RD nutrition diagnosis and recommendations for intervention.
After three months on TPN, the patient’s PICC line clogged and was shifted to PPN. The
patient was advised to allow the surgeon to insert another central catheter, since the PPN line
could not be a long term option for nutrition ssupport. After explaining the importance of
adequate protein and energy, the patient was convinced and a central PICC line was placed.
As can be seen in Figure 3, patient’s BMI decreased from 39 (Obese II) to 30.6 (Obese I),
indicating that the patient’s caloric intake was not meeting her nutritional needs. Even through
the patient’s BMI was I the obese range when admitted to the hospital, the purpose of her stay
was not to reach a normal BMI, but to support her nutritional needs by improving gut function
and wound healing. We need to consider, however, that the patient had some generalized edema,
and part of the weight loss may have been contributed by loss of fluid. The patient was not on

- 20 -
diuretics, however. A combination nutrition support of some oral nutrition with
immunomodulators such as IMPACT ®
pre-and post-operatively, in addition to the TPN, may
have promoted healing and reduced length of hospital stay.
Table 3. Nutrition Needs Assessment –based on 84 Kg
Calories Protein Fluid
2,268 KCal 101 gm 2,100 ml
@
27 Kcal/Kg
@
1.2 gm/Kg
@
25 ml/Kg
Table 4.
Nutrition supplied by TPN ordered by Physician compared to RD recommendations
Physician
Recommendations
Carbohydrate
D 20%
Protein
AA 8.5%
Lipid
20%
Rate
@ 63 ml/hr
Total
680 KCal 255 Kcal 500 KCal 1,361 KCal
64 gm
Dietitian
Recommendations
Carbohydrate
D 20%
Protein
AA 10%
Lipid
20% (250 ml)
Rate
@ 84 ml/hr
Total
1360 KCal 400 Kcal 500 KCal 2,260 KCal
100 gm

- 21 -
Table 5. Nutrition Diagnosis
PES Statement:
1. Inadequate oral intake related to Pt NPO as evidenced by Pt on TPN
2. Increase protein needs related to wound healing as evidenced by surgical wound,
enterocutaneous fistula and Stage 2 pressure ulcer.
Interventions:
i. Recommend increasing TPN rate from 63 ml/hr to 84 ml/hr to better meet nutritional
needs
ii. Recommend increasing Amino Acid concentration from 8.5% to 10 %, Dextrose from
10% to 50% (2350 Kcal, 100 gm Pro), to better meet nutritional needs
iii. Recommend wean off TPN when able to meet >50% estimated needs by PO intake.
iv. Recommend advance diet to clear liquids, Vital AF1.2 supplement, Full Liquids to GI
soft/Low Fiber, 2 GM Na, to goal regular Diet, 2 GM Na.

- 22 -
Summary
P.L. was presented to the hospital with an incarcerated ventral hernia, which resulted in
strangulation and small bowel obstruction. After anastomosis surgery and extensive enterolysis
the patient developed fistulas which did not heal spontaneously. The author believes that this
may have been prevented if an alternative peri-operative nutrition protocol had been followed.
Recent research has shown that pre-operative nutrition support involving immunomodulators
such as arginine, glutamine, omega-3 fatty acids and nucleotides, can promote healing and
reduce hospital stay. In addition early enteral feeding can promote GI motility and prevent gut
atrophy. After a four month stay at the hospital and the application of wound vac to heal the
enterocutaneous fistula stomas, the patient was advanced to clear liquids, followed by a low
fiber, GI soft diet and discharged. Three months later the patient was presented to the hospital
with facial and hand paresthesias which was diagnosed as transient ischemic attack. During that
hospital visit the patient was placed on a cardiac, 2 gm sodium diet, indicating that she could
tolerate a normal texture oral diet at this time. The patient’s condition improved and was
discharged after one day.

- 23 -
References
Ansari, P. Hernials of the abdominal wall.
http://www.merckmanuals.com/professional/gastrointestinal-disorders/acute-abdomen-and-
surgical-gastroenterology/hernias-of-the-abdominal-wall
Nobie, Brian et al. Small Bowel Obstruction. http://emedicine.medscape.com/article/774140-
overview
Mayo Clinic Staff. Intestinal Obstruction. http://www.mayoclinic.org/diseases-
conditions/intestinal-obstruction/basics/definition/con-20027567
Cleveland Clinic. Intestinal Ischemic Syndrome.
http://my.clevelandclinic.org/services/heart/disorders/pad/visceralischemiasyndrome
Mayo Clinic Staff. The Mayo Clinic. http://www.mayoclinic.org/diseases-
conditions/peritonitis/basics/definition/con-20032165
Willcutts, Kate. "NUTRITION ISSUES IN GASTROENTEROLOGY, SERIES# 90 Pre-op
NPO and Traditional Post-op Diet Advancement: Time to Move On."Practical
Gastroenterology 34.12 (2010): 16-27.
Daley Brian J, MD, MBA, FACS, FCCP, CNSC; Chief Editor: Julian Katz, MD Peritonitis and
Abdominal Sepsis http://emedicine.medscape.com/article/180234-overview
Farquhar, C., et al. "Barrier agents for preventing adhesions after surgery for subfertility." The
Cochrane Library (1999).

- 24 -
Pritts, T. A., D. R. Fischer, and J. E. Fischer. "Postoperative enterocutaneous fistula." Surgical
Treatment. Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt Verlag (2001).
Walter, C. J., et al. "Enhanced recovery in colorectal resections: a systematic review and
meta‐analysis1." Colorectal Disease 11.4 (2009): 344-353.
Delaney, Conor P., et al. "Association of surgical care practices with length of stay and use of
clinical protocols after elective bowel resection: results of a national survey." The American
Journal of Surgery 199.3 (2010): 299-304.
Osland, Emma, et al. "Early Versus Traditional Postoperative Feeding in Patients Undergoing
Resectional Gastrointestinal Surgery A Meta-Analysis." Journal of parenteral and enteral
nutrition 35.4 (2011): 473-487.
Warren, Jeremy, Varun Bhalla, and Gail Cresci. "Postoperative diet advancement surgical
dogma vs evidence-based medicine." Nutrition in Clinical Practice 26.2 (2011): 115-125.
Lee, Seung Hwan, et al. "Effects of Early Enteral Nutrition on Patients After Emergency
Gastrointestinal Surgery: A Propensity Score Matching Analysis."Medicine 93.28 (2014): e323.
Boelens, Petra G., et al. "Reduction of postoperative ileus by early enteral nutrition in patients
undergoing major rectal surgery: prospective, randomized, controlled trial." Annals of
surgery 259.4 (2014): 649-655.
Mazaki, Takero, and Kiyoko Ebisawa. "Enteral versus parenteral nutrition after gastrointestinal
surgery: a systematic review and meta-analysis of randomized controlled trials in the English
literature." Journal of Gastrointestinal Surgery 12.4 (2008): 739-755.

- 25 -
Lewis, Stephen J., Henning K. Andersen, and Steve Thomas. "Early enteral nutrition within 24 h
of intestinal surgery versus later commencement of feeding: a systematic review and meta-
analysis." Journal of Gastrointestinal Surgery 13.3 (2009): 569-575.
Schulman, Alison Saalwachter, and Robert G. Sawyer. "Have you passed gas yet? Time for a
new approach to feeding patients postoperatively." Practical Gastroenterology 29.10 (2005): 82.
Woodcock, Nicholas P., et al. "Enteral versus parenteral nutrition: a pragmatic
study." Nutrition 17.1 (2001): 1-12.
Moskovitz, David N., and Young-In Kim. "Does perioperative immunonutrition reduce
postoperative complications in patients with gastrointestinal cancer undergoing
operations?." Nutrition reviews 62.11 (2004): 443-447.
Braga, Marco. "Perioperative immunonutrition and gut function." Current Opinion in Clinical
Nutrition & Metabolic Care 15.5 (2012): 485-488.
Marimuthu, Kanagaraj, et al. "A meta-analysis of the effect of combinations of immune
modulating nutrients on outcome in patients undergoing major open gastrointestinal
surgery." Annals of surgery 255.6 (2012): 1060-1068.
Akbarshahi B. Andersson M., Nordén, H. and R. Andersson. "Perioperative nutrition in elective
gastrointestinal surgery–potential for improvement?." Dig Surg25 (2008): 165-174.
McClave, Stephen A., et al. "Appropriate use of parenteral nutrition through the perioperative
period." Journal of Parenteral and Enteral Nutrition 37.5 suppl (2013): 73S-82S.