Embed Size (px)
Citation preview
Gastrointestinal System
nutrition
S. Buckley, RN, MS
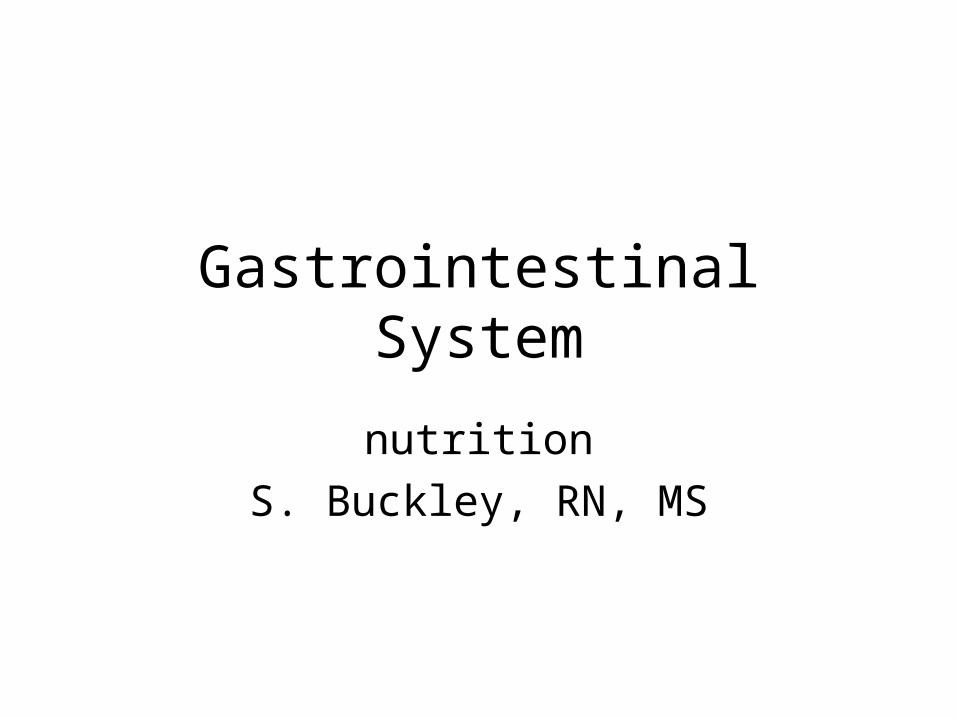
GI tract anatomy
• 30 ft. long from mouth to anus.
• Consists of mouth, esophagus, stomach, small intestine, large intestine, rectum, anus.
• Associated organs: liver, pancreas, gallbladder.
Function of GI tract
• Each part of system performs different activities.
• Ingestion and propulsion of food: mouth, pharynx, esophagus.
• Digestion and absorption: mouth, stomach, small intestine.
• Elimination: large intestine
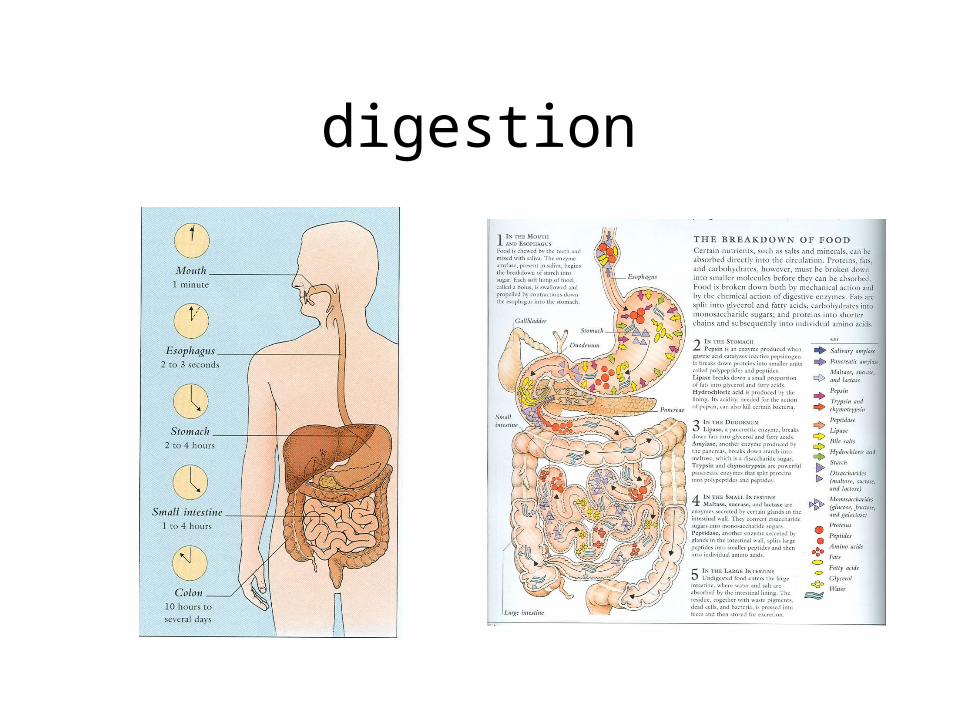
digestion
Factors affecting GI tract:
• Emotional factors: stress, anxiety..
• Physical factors: diet, alcohol, caffeine, cigarette smoking, fatigue, organic diseases.
• Emotional and physical factors may be manifested by anorexia, epigastric and abdominal pain, diarrhea, constipation.
Stomach
• Function is to store food, mix food with gastric secretions, and empty contents into small intestine. Absorbs only small amounts of water, alcohol, electrolytes and certain drugs.
• Usual length of time food in stomach: 3-4 hrs.
Stomach
• Chief cells secrete pepsinogen (antecedent of pepsin-the chief enzyme of gastric juice which converts proteins into peptones).
• Parietal cells secrete hydrochloric acid, water and intrinsic factor (increases absorption of vitamin B complex).
Small intestine
• Functions are digestion and absorption.
• Digestion completed in small intestine, where carbohydrates and fats are broken-down.
• ~23 ft. long, extends from pylorus to ileocecal valve. Composed of duodenum, jejunum, ileum.
Small intestine
• Physical presence of chyme (food mixed with gastric secretions) stimulates motility and secretions.
• Secretions include bile from biliary tract, CCK (cholecystokinin) produced by the duodenal mucosa, pancreatic enzymes.
Large intestine
• Function is absorption of water and electrolytes, elimination (forms feces and serves as reservoir)
• 4 parts: cecum (and appendix), colon (ascending colon on the right side, transverse, descending colon on the left side, sigmoid), rectum, anus.
defecation
• Reflex action involving voluntary and involuntary control.
Liver
• 4 functions: manufacture (production and excretion of bile), storage(glucose as glycogen, vitamins and minerals), transformation and excretion (phagocyte system-breakdown of RBC’s, WBC’s and bacteria) of a number of substances involved in metabolism.
Biliary tract
• Gallbladder and duct system. Functions to concentrate and store bile.
Pancreas
• Both exocrine and endocrine functions.
• Exocrine: contributes to the process of digestion by secreting pancreatic enzymes (amylase and others).
• Endocrine: secretion of insulin, glucagons, somatostatin, polypeptide.
Nutrition
• Problems present in all age groups, cultures and socioeconomic classes in all parts of world.
• caregivers can act as educator and resource person can have influence on information and practices of patients and their families.
Factors affecting nutrition and diet
• Attitudes
• Cultural and/or religious preferences
• Economic factors
• State of health
• Psychological issues
obesity
• 2nd leading cause of preventable death in U.S.
• 65.2 % of U.S adults are overweight• Etiology; genetic, environmental• Methods of measurement;
BMI-weight/height (p.974) 18-24• Classifications of body fat distribution• (gynoid/pear), (android/apple)
obesity
• Influences: culture, economics, habits, socialization, exercise pattern, work shift
• Diets: calorie in/calorie out.• Changes: less exercise, larger portions,
more carbohydrates.• Health consequences: diabetes,
cardiovascular problems, respiratory, musculoskeletal, Gerd, liver problems.
Essential components of nutrition
• Carbohydrates:chief source of energy, 4kcal/gm.
• Fats: major source of energy,form of insulation, stored in adipose tissue, 9kcal/gm.
• Proteins:essential for tissue growth and repair, maintenance, body regulatory functions, energy production, 4kcal/gm.
Nutrition and diet
• New information constantly influences percentages of components in diets.
• Daily caloric requirements influenced by bodybuild, gender, age, physical activity, level of physical and emotional health.
Nutritional needs
• Infants and children differ from adults: first months of life, the infant’s GI tract and kidneys are not functionally mature and are limited in kinds and quantities of nutrients needed. Metabolic rate of infants is higher and they have smaller nutritional reserve than adults.
Adolescent nutritional needs
• Vulnerable time for development of nutritional deficiencies due to rapid growth and bodily changes.
• Extreme concern with body images and social pressure often affect diet.
• Teenage girls prone to fad diets as means of weight control, which may not be nutritionally sound.
Older adults nutritional needs
• Decreases in lean body mass, metabolic rate and physical activity, thus, decreased caloric needs.
• Individuals often affected by economic factors, poor dentition, lack of social setting, medical conditions, anorexia.
Diet related issues
• Vegetarian diets-can lead to problems associated with protein and iron deficiencies.
• Vitamins:• Water-soluble:C and B, excreted via urine. High
levels of C can be associated with formation of uric acid stones.
• Fat-soluble:A,D, E, K. Can accumulate to toxic levels.
Constipation
• Decrease in frequency of BM from what is normal for individual.
• Etiology-insufficient dietary fiber or water, environment, ignoring urge to defecate, organic causes, medications.
• Complications-hemorrhoids, diverticulosis, abdominal discomfort, malaise
Education (regarding constipation)
• Increase fiber-broccoli, apples, carrots, squash, bran)
• Increase fluids -3 quarts/day
• Exercise-at least 3x week
• Establish regular time to defecate
• Avoid laxatives and enemas
Malnutrition
• May be excess, deficit or imbalance in essential components of a balanced diet.
• Most common in developing countries with inadequate food sources, poor economic conditions or lack of education regarding nutrition.
Malnutrition-Types
• Protein-calorie-most common cause of undernutrition, results from primary (nutritional needs not met as a result of poor eating habits), or secondary (alteration or defect in ingestion, digestion, absorption or metabolism)
Malnutrition terms
• Marasmus-deficiency in caloric and protein intake leading to generalized loss of body fat and muscle.
• Kwarshiorkor-deficiency of protein intake that is superimposed on a catabolic event (GI obstruction, surgical treatment, cancer, medications, malabsorption syndromes, infectious diseases)
malnutrition
• Up to 50% of surgical patients may be malnourished
• Factors that increase potential for development of malnutrition: inability to swallow, cognitive issues, surgery, radiation, chemotherapy, burns, draining wounds, renal or liver disease, hemorrhage, bone fractures, malabsorption, infectious diseases such as TB and AIDS.
Collaborative careManagement of malnutrition
• Hospitalization-determination of etiology
• Treatment of infections secondary to compromised immune status
• Diet high in calories and protein (oral or enteral, or parenteral options)
• Correction of fluid and electrolytes
• Social/psychological support
Nutritional disorders
• Malabsorption syndrome-impaired absorption of nutrients from GI tract. May result from insufficient enzymes or reduced bowel surface that leads to deficiencies.
• Symptoms-steatorrhea-bulky, fatty, stools that float.
• Lactose intolerance-intolerance of milk-based products.
• Symptoms-flatulence, cramping, “acid stomach”.
Anorexia/bulimia
• Specific psychiatric diagnosis-characterized by refusal to maintain body weight to greater than 85% of expected for age and height.
• Key feature-concern about body image
• Most common in girls and women and higher economic status.
complications
• Amenorrhea, bradycardia, hypotension, hair loss, constipation, edema with altered fluid balance, cardiac complications, malignant arrhythmias, emotional problems.
Anorexia
• Often common in adolescent girls
• Restrictive eating habits, secretive
• Usually long-standing behavior, familial tendencies
• Use of laxatives and enemas common
bulimia
• Bulimia-gorging and purging, usually associated with normal weight. Food becomes obsession and addiction.
• Self-induced vomiting causes physical problems of: dental issues, swollen glands, sore throat, electrolyte imbalances, dehydration.
Treatment(anorexia/bulimia)
• Nutritional and psychological support
• Hospitalization may be necessary for severe physical complications-tube or parenteral feedings may be utilized, but only as temporary intervention (not a cure for anorexia nervosa).
obesity
• Now in epidemic proportions. • Problems associated when more than 20% over
ideal body weight.• Associated problems-cardiovascular and
respiratory problems, vascular (hypertension), diabetes, gallstone formation, sleep apnea, emotional issues, degenerative joint disease, fatty liver infiltrates.
Collaborative care
• When no organic cause, should be considered chronic, complex illness.
• Plan of care should focus on weight loss with multipronged approach: dietary intake, physical activity, behavioral-cognitive modification, medication option.
Surgical intervention
• Gastric bypass technique of choice for morbidly obese.
• Postoperative care: nutritional, psychological support, wound monitoring, respiratory assessment, NG tube management, pain management.