Embed Size (px)
Citation preview
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
1
Georgia Center For Cancer StatisticsKim DeWolfe, MS, CTR
11/16/2012
Proper Text Documentation
Essential Rules for Abstracting
Collaborative Staging
Tips by Cancer Site

GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
2
See 2012 NAACCR Volume II Data Dictionary/Chapter X Recommended content by section http://www naaccr org/Applications/C http://www.naaccr.org/Applications/C
ontentReader/Default.aspx?c=10
You should be able to code from your text
Enter text in appropriate sectionEnter a date in each sectionUse abbreviations from approved listAvoid copy and pasteUse lower case characters Use punctuation
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
3
When information missing from record, state it is missing
D t t i f ti f Do not repeat information from other text fields
Enter information relevant to primary site
Do NOT intermix text for simultaneous primaries
If O t f St t id t t ti f If Out of State resident at time of admit, address at dx should reflect this
For sequence >00, provide text to justify
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
4
Saves time and limits length
MUST use NAACCR approved bb i ti li tabbreviation list
DO NOT make up your own terms
Located in Volume II of NAACCR’s Standards for Cancer Registries: http://www.naaccr.org/Applications/C
ontentReader/Default aspx?c=17ontentReader/Default.aspx?c 17Appendix G
GCCR/S is providing the list on a flash drive
Xray: “…intense act related to prim lesion RUL 2.2 cm spic mass pstv m lns bilat slight act Lt midlung corresponds to sml ill-def lesions on CT susp for to sml ill def lesions on CT susp for poss mets or 2nd prim act Rt sprclv susp for met Ln”
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
5
X-ray: Chest CT 6/24/12: Primary lesion of RUL measuring 2.2 cm, described as spiculated. Positive bilateral mediastinal Lns Small ill-bilateral mediastinal Lns. Small illdefined lesion of Lt mid-lung is suspfor possible mets or 2nd primary. Activity in Rt supraclavicular region is susp for Ln mets.
PE (4/20/12): 67 yo wf presents to this facility for
lobectomy of a LLL lung primary. Patient diagnosed with
adenocarcinoma in Tallahassee FL adenocarcinoma in Tallahassee, FL via bronchoscopy.
Patient has prior hx of breast ca. Note: patient lived in Florida at time
of diagnosis. She has moved to Georgia to be closer to son.
X-ray/Scan: CT Chest/Abd/Pelvis (4/20/12): 14 mm LLL pulm nodule susp for neoplastic dz. Abd and Pelvis: No abnormalities.
CT Head (4/20/12):4.5 cm cystic mass in Lt ( ) ycerebellar hemisphere. Metasatic dz vs. hemangioblastoma.
Bone Scan(4/25/12): Scan is unremarkable with no evidence of bone mets.
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
6
Lab Tests: 06/09/2012- PSA 5.9. Postop readmission CBC, 07/31/2011, WBC 12.90, RBC 3.79, HGB 11 7 HCT 35 2 Normal diff PtHGB 11.7, HCT 35.2, Normal diff. Ptw/previous hx of positive MRSA test at X medical center, unk details.
Lab Tests: 6/9/12 PSA = 5.9 ng/ml
Procedures from which staging info is derived
List biopsies and all other surgical proceduresprocedures
Surgeon’s observationsResidual tumor Invasion of surrounding areas

GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
7
DON’T limit to TNM
Organs involved by direct extension
Site(s) of Distant Mets
Physician’s specialty and comments
Let’s review togetherNote: there is a generic text
document on your flash drive
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
8
Before you assign 999, look for a descriptor code
E l I i b t t Example: Invasive breast tumor described as microscopic focus
Correct Size code = 990
The most miscoded CS field
AVOID assigning “T nos” codes
Use best information whether clinical or pathologic
Document how the most extensive tumor established (clinical or pathologic)
Limit code 6 to tumors that are Limit code 6 to tumors that are more extensive than before neo-adjuvant therapy
Example: Tumor size larger after pre-operative chemotherapy
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
9
Many are related to one another
With no edits in place currently, be t h k th t isure to check these twice
All codes should have text to accompany it SSF 7 for Breast coded to 080 =
“Bloom-Richardson Score of 8”
Read the general instructions of your manuals
MP/H Manual 2007
Collaborative Stage Part I
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
10
Code histology and grade from the invasive component only
Exception: if grade is unknown for invasive component, you may use the in-situ grade
Record the earliest of any of these dates:
Date First Surgical ProcedureD t R di ti St t dDate Radiation Started
Date Systemic Therapy StartedDate Other Treatment Started
Primary siteRegional lymph nodes (FNA or core
bx)Di t t it t di t t l h Distant sites or to distant lymph nodes
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
11
Lung Cancer Case
FNA of Mediastinal Lymph Node f d 11/06/2012performed 11/06/2012
LUL lobecotmy 12/12/2012
Date of First Course of Treatment = 11/06/2012
Indicate if this date is estimated
Use the first date whether clinical hi t l ior histologic
Clinical must contain reportable ambiguous terms
2/2/2012 Chest CT: 5 cm RUL lung nodule suspicious for carcinoma
3/15/2012 Right Upper Lung Lobectomy: poorly differentiated Lobectomy: poorly differentiated adenocarcinoma
What is the date of diagnosis? 2/2/2012Use first date containing reportable phrase
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
12
Reportability
Staging/Involvement
Histology
Word Document on your Flash Drive
Let’s review it together
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
13
62 yo bf with 4 cm mass arising in right kidney.
CT Abd: Large mass in right kidney consistent with renal cell carcinomaconsistent with renal cell carcinoma
Patient’s diagnostic work-up stopped after imaging studies performed and no treatment given
Is this case reportable?
Yes, due to the phrase: “consistent with renal cell carcinoma” in the radiology report
Ambiguous Diagnosis Code = 1 (diagnosed by ambiguous term only)
Surgeon describes a large colon mass kissing the adjacent duodenum
D thi l i l th Does this colon mass involve the duodenum?
No, kissing is not a term on the involvement list
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
14
Pathology report for lung primary states: Non-small cell lung cancer suspicious for adenocarcinoma
Assign Adenocarcinoma histology Assign Adenocarcinoma histology code
“Suspicious for” is on the reportable ambiguous list
Use information in pathology report over other sources
V i b it d t it d Varies by site, data item, and situation
Consult site specific coding guidelines
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
15
Step 1: Look for site specific coding guidelines for data field in question SEER’s Appendix C and CS Schemas If no rules apply proceed to Step 2 If no rules apply proceed to Step 2
Step 2: Refer to general coding instructions by data item Found in FORDS, SEER, and CS Part I
Use reports in the following order (resected sites):
1 O ti t ith g ’ 1. Operative report with surgeon’s description
2. Pathology report3. Imaging
Fuhrman grade
Nuclear grade
Terminology (well diff, mod diff)
Histologic grade (grade 1, grade 2)
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
16
Refer to Breast Clock
Code multiple tumors to C50.9
Code large tumors to C50.8 If span over >1 quadrant
Don’t forget combination codes Infiltrating ductal ca with another
component
Code invasive component onlyCode invasive component onlyOften insitu and invasive cancer
present
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
17
Tissue Expander NOT a type of tissue reconstruction
A i i l t d Assign implant code
Code the intent
Scope of Regional Lymph Nodes code 2, 6, or 7 when sentinel node
mentioned in the operative report and/or pathology report(s)and/or pathology report(s)
Use operative report as primary source
New Coding Instructions for 2012 cases
Do not code a hilar or mediastinal mass as primary unless stated as such
Clearly document radiology findingsClearly document radiology findingsMost often your best source for CS staging
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
18
Mass, enlargement, or adenopathy in the hilum or mediastinum
Considered regional lymph node involvement
Understand clinically apparent vs. inapparent disease
H l d id if C d 150 i Helps you decide if Code 150 is correct for CS Extent
DRE does not mention a palpable tumor, mass or nodule
Negative imaging studies
MD statement of T1c
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
19
Clinician documents “tumor”, “mass”, or “nodule” findings from DRE
Tumor is palpable or visible by imaging
Physical exam will be only source you can use to determine inapparent tumor vs. apparent tumorUnless the managing
clinician/urologist considers the imaging reliable for staging
To Code SSF6 (CRM), you must mention it in your text
Use code 999 if not mentioned in path or stated as “Margins, NOS”
Look for mesentery or radial termIf the CRM is involved (positive), use
code 000
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
20
If right hemi-colectomy performed, do not automatically assign site code C18.2 (ascending colon)
Use your source priority rules here1. Surgeon’s statement2. Pathology report3. Imaging
CS Extension often miscoded
Avoid using the 400, nos code ( t i th h ll )(extensive through wall, nos)
Adipose tissue is considered connective tissue
Sigmoidectomy path report: invasive adenocarcinoma, poorly diff, involving pericolic p y , g padipose tissue, invades musclaris propria into serosal adipose tissue
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
21
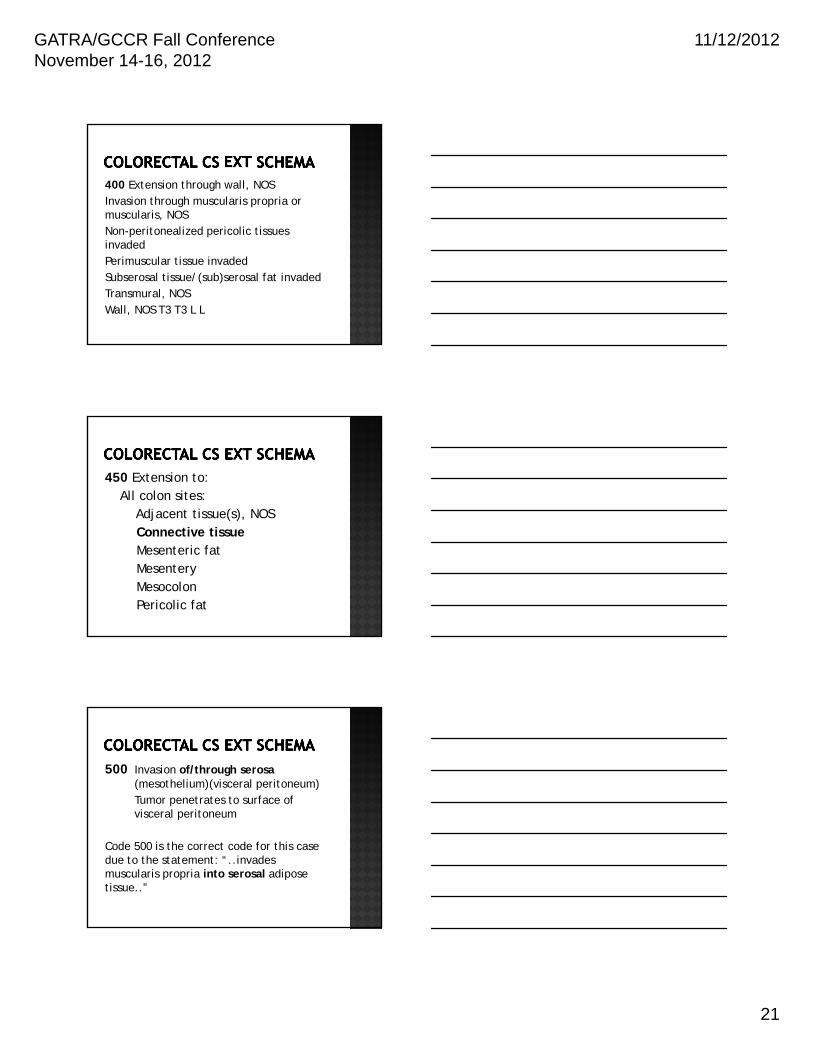
400 Extension through wall, NOSInvasion through muscularis propria or muscularis, NOSNon-peritonealized pericolic tissues Non peritonealized pericolic tissues invadedPerimuscular tissue invadedSubserosal tissue/(sub)serosal fat invadedTransmural, NOSWall, NOS T3 T3 L L
450 Extension to:All colon sites:
Adjacent tissue(s), NOSConnective tissueMesenteric fatMesentery MesocolonPericolic fat
500 Invasion of/through serosa (mesothelium)(visceral peritoneum) Tumor penetrates to surface of visceral peritoneump
Code 500 is the correct code for this case due to the statement: “..invades muscularis propria into serosal adipose tissue..”
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
22
Multiple tumors should be coded to C67.9 and not C67.8
Pay attention to TURB findings to assign the best site code
MD doesn’t state primary site of origin
Consider clinical presentation
Consider histology type if biopsy performed
Abstracting is a challenge
Proper use of text is importantp p
Abstract one site at time
Use your site specific rules and guidelines in SEER Appendix C
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
23
“If it wasn't hard, everyone would do it. It's
h h d h the hard that makes it great.”
Tom Hanks
Facility Oncology Registry Standards (FORDS): Revised for 2012
SEER Program Coding and Staging Manual 2012
SEER Appendix C – Site Specific Coding Modules
2012 NAACCR Volume II Version 13: Chapter X, Data Dictionary
Collaborative Staging, v.02.04, Parts I and II
GATRA/GCCR Fall Conference November 14-16, 2012
11/12/2012
24
Editing Staff at Georgia Center for Cancer Statistics
Judy Andrews, CTRPh lli Wil CTRPhyllis Wilson, CTR





























