Embed Size (px)
Citation preview
Gavin Giovannoni
Version 2.0
Disclosures
Over the last 5 years I have received personal compensation for participating in advisory boards in relation to clinical trial design, trial steering committees, and data and safety monitoring committees from: Abbvie, Atara Bio, Biogen, Canbex, Sanofi-Genzyme, Genentech, GSK, MSD, Merck-Serono, Novartis, Roche, Synthon BV and Teva.
Spoilt for choice
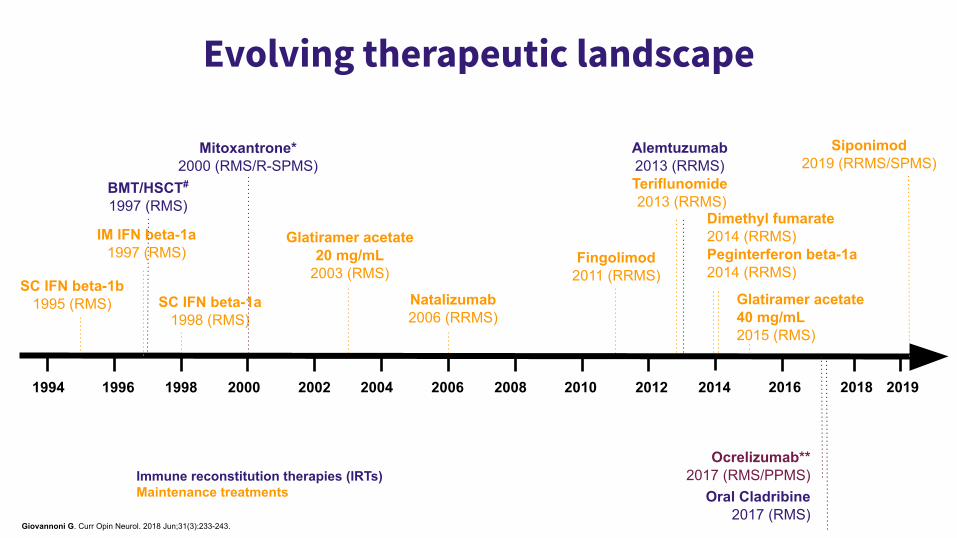
Evolving therapeutic landscape
1994 1996 20001998 2002 2004 2006 2008 2010 2012 2014
SC IFN beta-1b1995 (RMS)
IM IFN beta-1a1997 (RMS)
SC IFN beta-1a 1998 (RMS)
Natalizumab2006 (RRMS)
Glatiramer acetate20 mg/mL
2003 (RMS)Fingolimod
2011 (RRMS)
Alemtuzumab2013 (RRMS)Teriflunomide 2013 (RRMS)
2016
Dimethyl fumarate2014 (RRMS)Peginterferon beta-1a2014 (RRMS)
Glatiramer acetate40 mg/mL2015 (RMS)
Ocrelizumab**2017 (RMS/PPMS)
Oral Cladribine2017 (RMS)
2018
BMT/HSCT#
1997 (RMS)
Mitoxantrone*2000 (RMS/R-SPMS)
Immune reconstitution therapies (IRTs)Maintenance treatments
Giovannoni G. Curr Opin Neurol. 2018 Jun;31(3):233-243.
2019
Siponimod2019 (RRMS/SPMS)
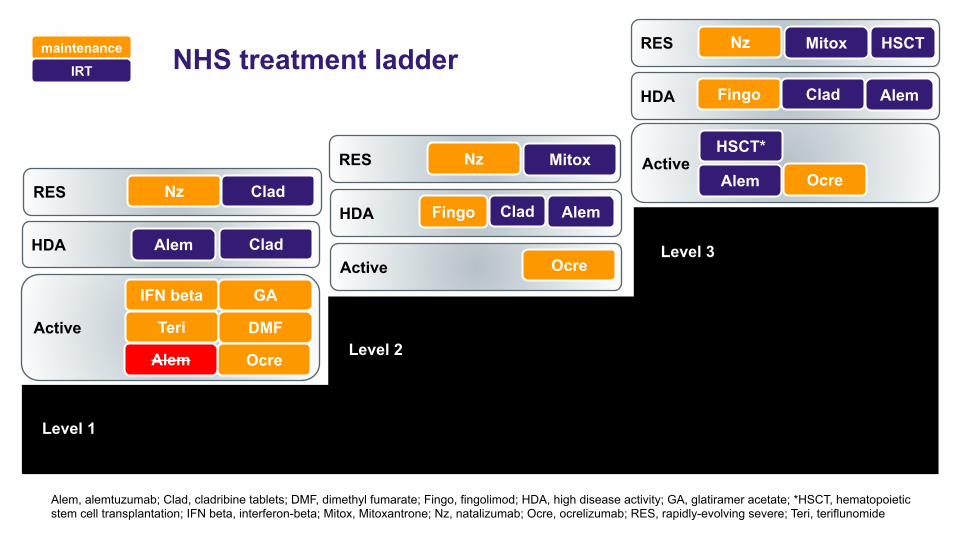
Alem, alemtuzumab; Clad, cladribine tablets; DMF, dimethyl fumarate; Fingo, fingolimod; HDA, high disease activity; GA, glatiramer acetate; *HSCT, hematopoietic stem cell transplantation; IFN beta, interferon-beta; Mitox, Mitoxantrone; Nz, natalizumab; Ocre, ocrelizumab; RES, rapidly-evolving severe; Teri, teriflunomide
NHS treatment ladder
RES Nz CladHDA Fingo Clad
Level 1
Level 2
Level 3Active Ocre
HDA Clad
HDA Fingo Clad
ActiveHSCT*
Alem OcreRES Nz Mitox
RES Nz Mitox HSCTmaintenanceIRT
Active
IFN beta
Teri
GA
DMF
Ocre
Alem
Alem
Alem
Alem
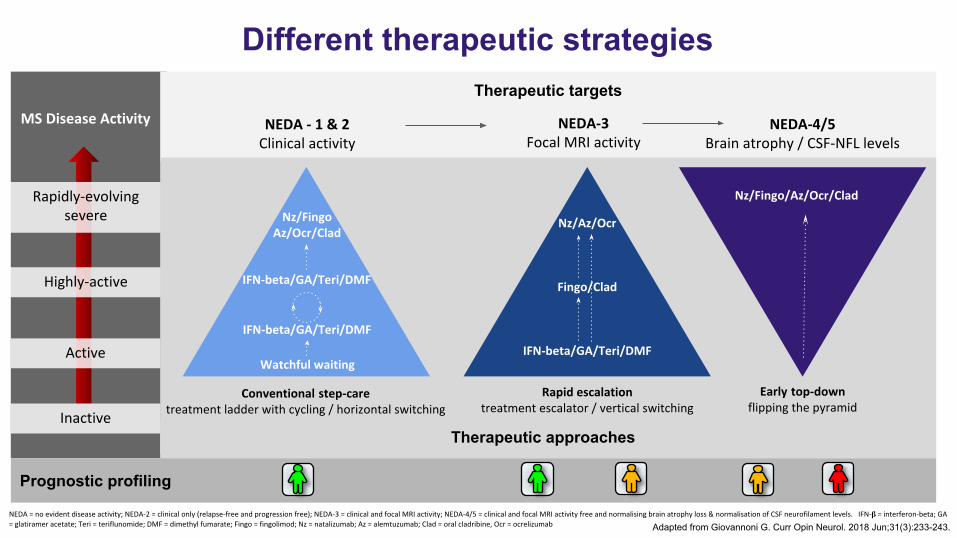
Therapeutic targets
Prognostic profiling
Different therapeutic strategies
𝛃
Therapeutic approaches
Adapted from Giovannoni G. Curr Opin Neurol. 2018 Jun;31(3):233-243.
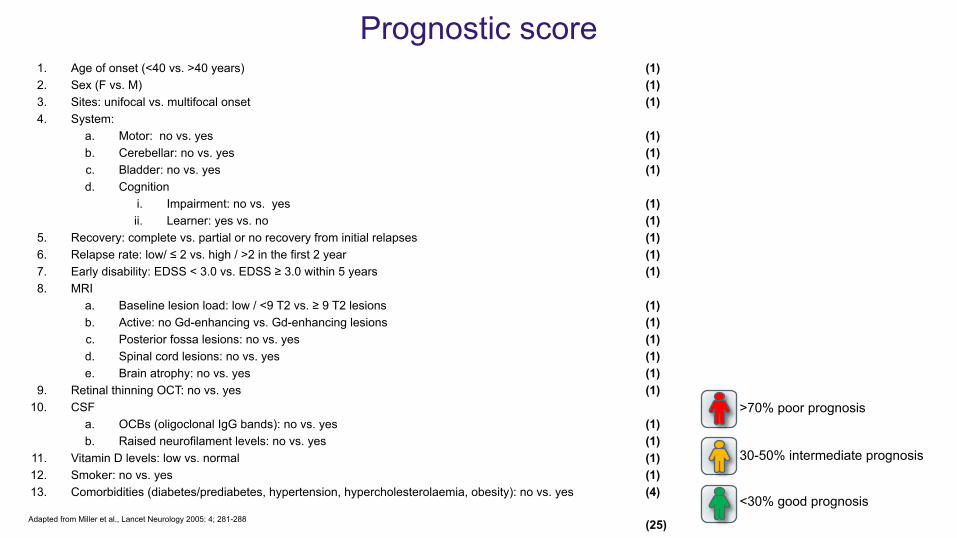
Prognostic score1. Age of onset (<40 vs. >40 years) (1)2. Sex (F vs. M) (1)3. Sites: unifocal vs. multifocal onset (1)4. System:
a. Motor: no vs. yes (1)b. Cerebellar: no vs. yes (1)c. Bladder: no vs. yes (1)d. Cognition
i. Impairment: no vs. yes (1)ii. Learner: yes vs. no (1)
5. Recovery: complete vs. partial or no recovery from initial relapses (1) 6. Relapse rate: low/ ≤ 2 vs. high / >2 in the first 2 year (1)7. Early disability: EDSS < 3.0 vs. EDSS ≥ 3.0 within 5 years (1)8. MRI
a. Baseline lesion load: low / <9 T2 vs. ≥ 9 T2 lesions (1)b. Active: no Gd-enhancing vs. Gd-enhancing lesions (1)c. Posterior fossa lesions: no vs. yes (1)d. Spinal cord lesions: no vs. yes (1)e. Brain atrophy: no vs. yes (1)
9. Retinal thinning OCT: no vs. yes (1)10. CSF
a. OCBs (oligoclonal IgG bands): no vs. yes (1)b. Raised neurofilament levels: no vs. yes (1)
11. Vitamin D levels: low vs. normal (1)12. Smoker: no vs. yes (1)13. Comorbidities (diabetes/prediabetes, hypertension, hypercholesterolaemia, obesity): no vs. yes (4)
(25)
<30% good prognosis
30-50% intermediate prognosis
>70% poor prognosis
Adapted from Miller et al., Lancet Neurology 2005: 4; 281-288
ImmunosuppressionA reduction of the activation or efficacy of the immune system
This definition refers to short-term (IRTs) and long-term persistent immunosuppression (maintenance).
For a drug to be considered an immunosuppressant it should cause:
1) significant lymphopaenia2) be associated with opportunistic infections3) reduce the antibody response to vaccines4) be associated with secondary malignancies
1) Interferon-beta2) Glatiramer acetate3) Mitoxantrone4) Natalizumab (selective compartment)5) Fingolimod, Siponimod & other S1P
modulators6) Teriflunomide7) Dimethyl fumarate8) Alemtuzumab9) Ocrelizumab (Anti-CD20)
10) Cladribine (purine analogue)
Giovannoni G. Curr Opin Neurol. 2018 Jun;31(3):233-243.
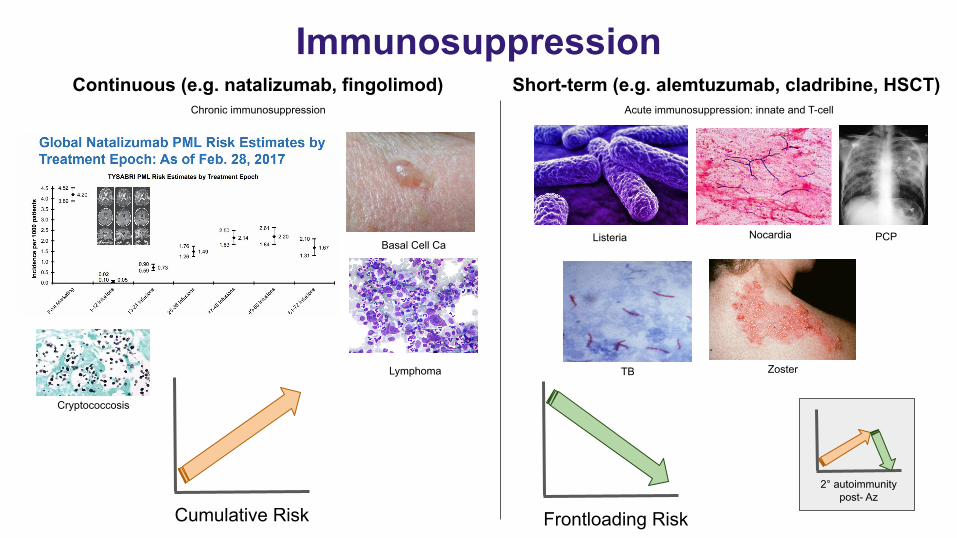
ImmunosuppressionContinuous (e.g. natalizumab, fingolimod) Short-term (e.g. alemtuzumab, cladribine, HSCT)
Basal Cell Ca
Zoster
Cumulative Risk Frontloading Risk
Listeria
TB
Nocardia PCP
Lymphoma
Cryptococcosis
2° autoimmunity post- Az
Acute immunosuppression: innate and T-cellChronic immunosuppression
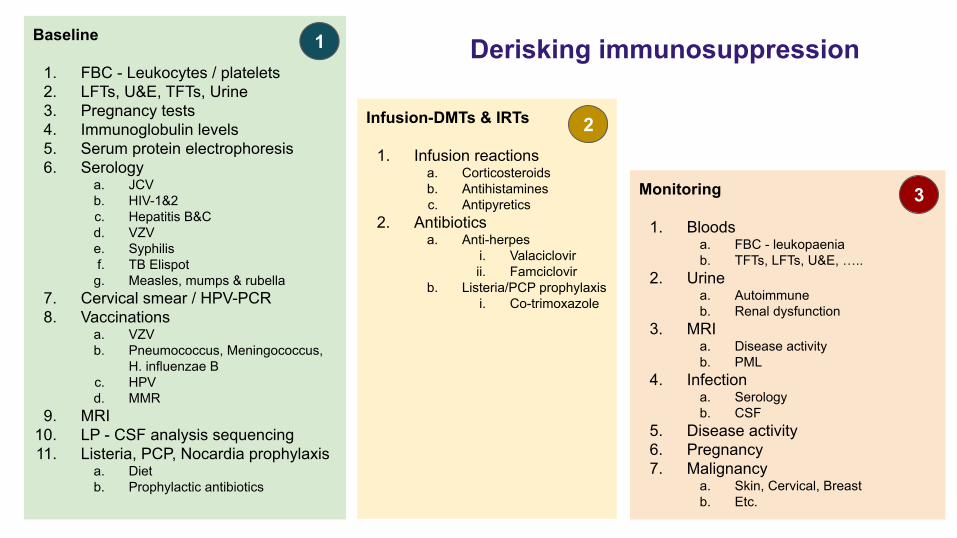
Derisking immunosuppressionBaseline
1. FBC - Leukocytes / platelets2. LFTs, U&E, TFTs, Urine3. Pregnancy tests4. Immunoglobulin levels5. Serum protein electrophoresis6. Serology
a. JCVb. HIV-1&2c. Hepatitis B&Cd. VZVe. Syphilisf. TB Elispot
g. Measles, mumps & rubella7. Cervical smear / HPV-PCR8. Vaccinations
a. VZVb. Pneumococcus, Meningococcus,
H. influenzae Bc. HPVd. MMR
9. MRI10. LP - CSF analysis sequencing11. Listeria, PCP, Nocardia prophylaxis
a. Dietb. Prophylactic antibiotics
Infusion-DMTs & IRTs
1. Infusion reactionsa. Corticosteroidsb. Antihistaminesc. Antipyretics
2. Antibioticsa. Anti-herpes
i. Valaciclovirii. Famciclovir
b. Listeria/PCP prophylaxisi. Co-trimoxazole
Monitoring
1. Bloodsa. FBC - leukopaeniab. TFTs, LFTs, U&E, …..
2. Urinea. Autoimmuneb. Renal dysfunction
3. MRIa. Disease activityb. PML
4. Infectiona. Serologyb. CSF
5. Disease activity6. Pregnancy7. Malignancy
a. Skin, Cervical, Breastb. Etc.
1
2
3
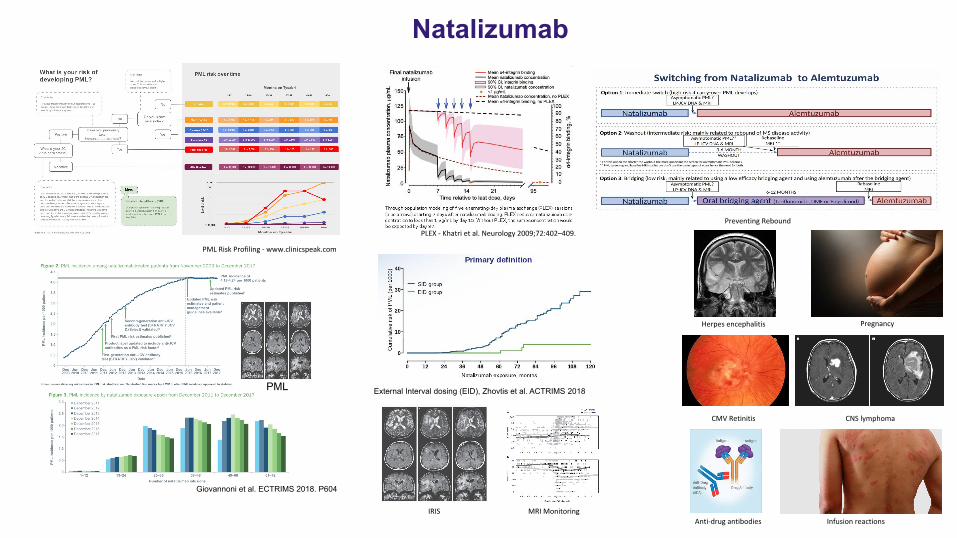
Natalizumab
PML
Giovannoni et al. ECTRIMS 2018. P604
External Interval dosing (EID), Zhovtis et al. ACTRIMS 2018
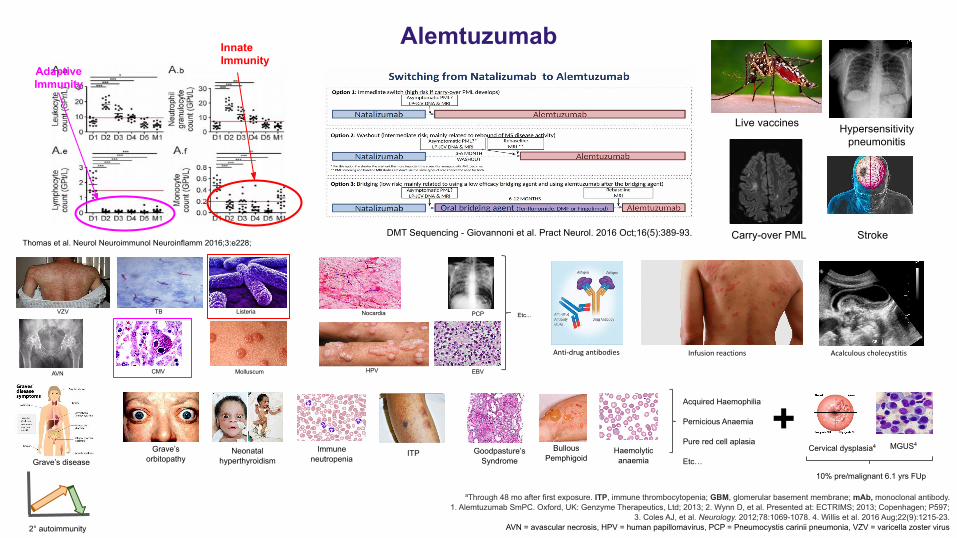
Alemtuzumab
VZV TB Listeria Nocardia
Molluscum HPVCMV EBV
PCP Etc...
Thomas et al. Neurol Neuroimmunol Neuroinflamm 2016;3:e228;
AVN
InnateImmunity
AdaptiveImmunity
aThrough 48 mo after first exposure. ITP, immune thrombocytopenia; GBM, glomerular basement membrane; mAb, monoclonal antibody.1. Alemtuzumab SmPC. Oxford, UK: Genzyme Therapeutics, Ltd; 2013; 2. Wynn D, et al. Presented at: ECTRIMS; 2013; Copenhagen; P597;
3. Coles AJ, et al. Neurology. 2012;78:1069-1078. 4. Willis et al. 2016 Aug;22(9):1215-23.AVN = avascular necrosis, HPV = human papillomavirus, PCP = Pneumocystis carinii pneumonia, VZV = varicella zoster virus
.
Haemolytic anaemia
Goodpasture’s Syndrome
ITP Bullous Pemphigoid
Immune neutropenia
Grave’s orbitopathy
Neonatal hyperthyroidism
Acquired Haemophilia
Pernicious Anaemia
Pure red cell aplasia
Etc…
Cervical dysplasia4 MGUS4
+10% pre/malignant 6.1 yrs FUp
Live vaccines Hypersensitivity pneumonitis
DMT Sequencing - Giovannoni et al. Pract Neurol. 2016 Oct;16(5):389-93. Carry-over PML
2° autoimmunity
Grave’s disease
Stroke
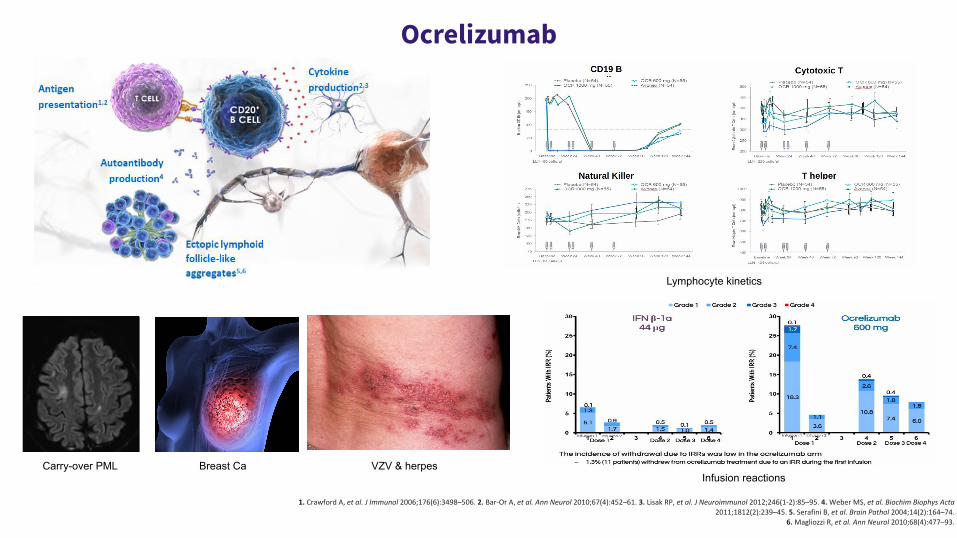
Ocrelizumab
Carry-over PML Breast Ca VZV & herpesInfusion reactions
Lymphocyte kinetics
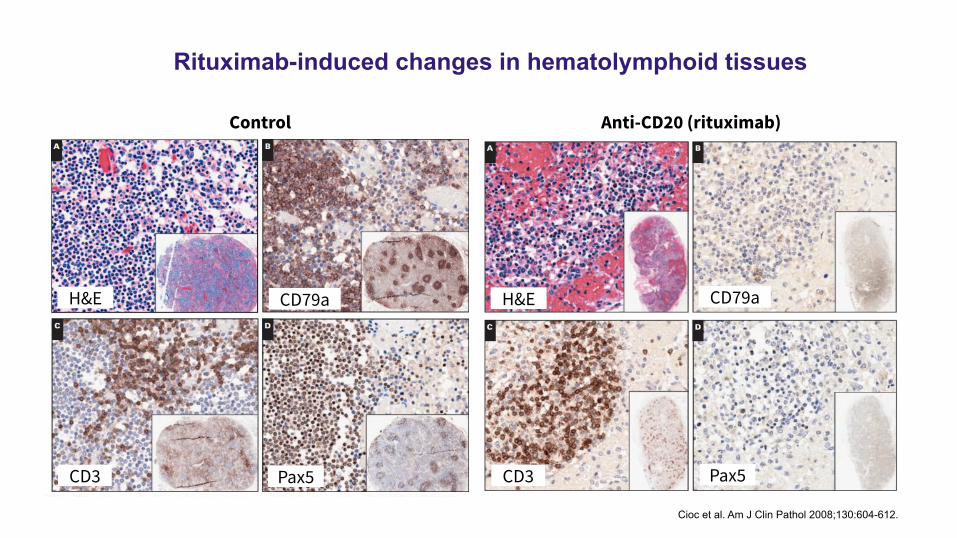
Rituximab-induced changes in hematolymphoid tissues
Control Anti-CD20 (rituximab)
H&E H&E CD79a
CD3 CD3Pax5 Pax5
CD79a
Cioc et al. Am J Clin Pathol 2008;130:604-612.
Pre-vaccination
Geo
met
ric m
ean
titre
(IgG
IU/m
L)
4 weekspost-vaccination
8 weekspost-vaccination
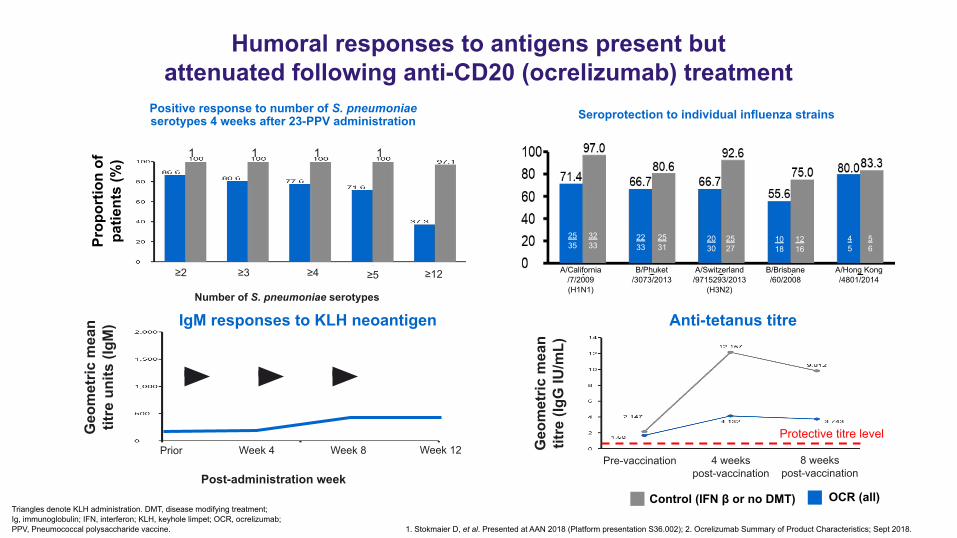
Anti-tetanus titre
Protective titre level
Triangles denote KLH administration. DMT, disease modifying treatment;Ig, immunoglobulin; IFN, interferon; KLH, keyhole limpet; OCR, ocrelizumab;PPV, Pneumococcal polysaccharide vaccine. 1. Stokmaier D, et al. Presented at AAN 2018 (Platform presentation S36.002); 2. Ocrelizumab Summary of Product Characteristics; Sept 2018.
Humoral responses to antigens present but attenuated following anti-CD20 (ocrelizumab) treatment
Positive response to number of S. pneumoniaeserotypes 4 weeks after 23-PPV administration
Number of S. pneumoniae serotypes
100
100
100
100
Prop
ortio
n of
pa
tient
s (%
)
≥2 ≥3 ≥4 ≥5 ≥12 A/California/7/2009(H1N1)
B/Phuket/3073/2013
A/Switzerland/9715293/2013
(H3N2)
B/Brisbane/60/2008
A/Hong Kong/4801/2014
2535
2233
2030
1018
45
3233
2531
2527
1216
56
Seroprotection to individual influenza strains
Post-administration week
Prior Week 4 Week 12Week 8
Geo
met
ric m
ean
titre
uni
ts (I
gM) IgM responses to KLH neoantigen
OCR (all)Control (IFN β or no DMT)
Reasoning by analogy
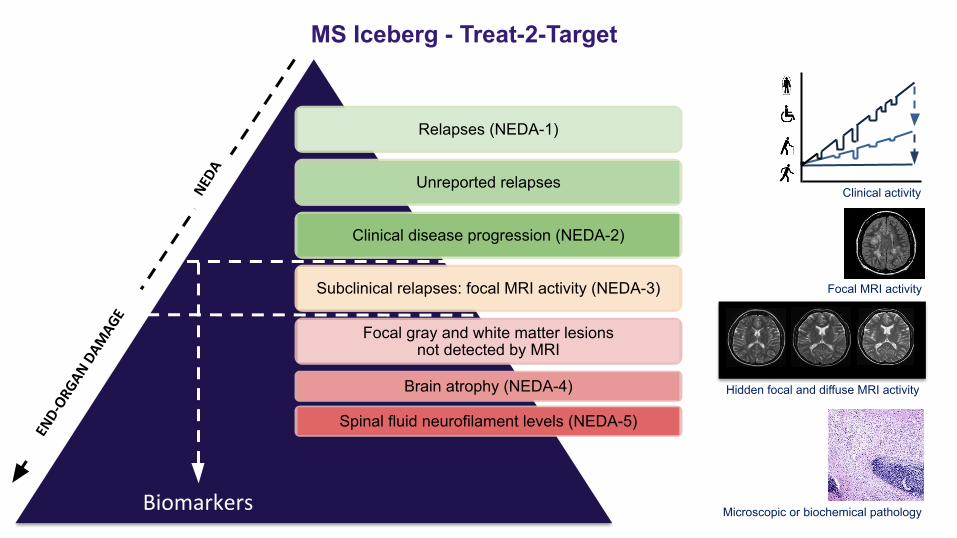
Relapses (NEDA-1)
Unreported relapses
Clinical disease progression (NEDA-2)
Subclinical relapses: focal MRI activity (NEDA-3)
Focal gray and white matter lesions not detected by MRI
Brain atrophy (NEDA-4)
Spinal fluid neurofilament levels (NEDA-5)
MS Iceberg - Treat-2-Target
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
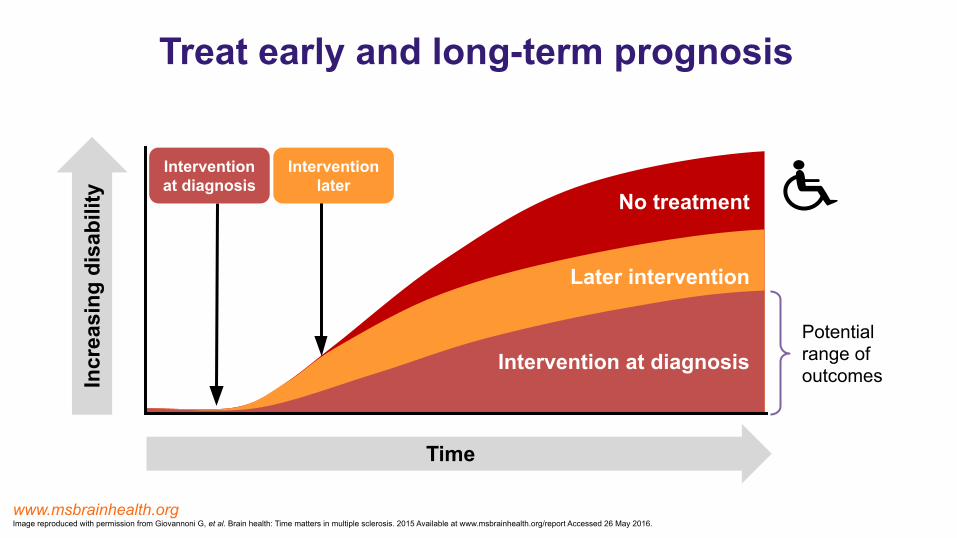
Treat early and long-term prognosis
www.msbrainhealth.orgImage reproduced with permission from Giovannoni G, et al. Brain health: Time matters in multiple sclerosis. 2015 Available at www.msbrainhealth.org/report Accessed 26 May 2016.
Incr
easi
ng d
isab
ility
Time
Intervention at diagnosis
Intervention later
Potentialrange ofoutcomes
No treatment
Later intervention
Intervention at diagnosis
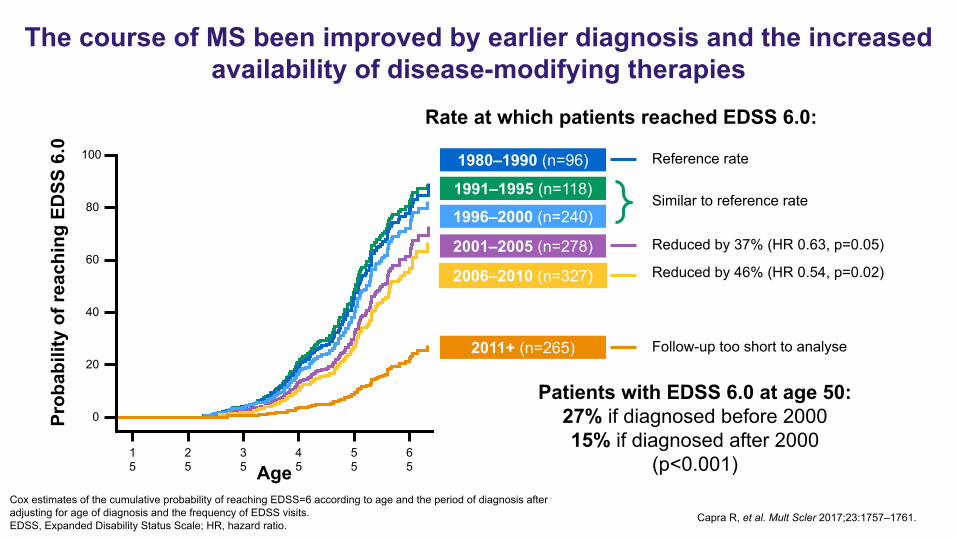
Cox estimates of the cumulative probability of reaching EDSS=6 according to age and the period of diagnosis after adjusting for age of diagnosis and the frequency of EDSS visits.EDSS, Expanded Disability Status Scale; HR, hazard ratio.
Capra R, et al. Mult Scler 2017;23:1757–1761.
The course of MS been improved by earlier diagnosis and the increased availability of disease-modifying therapies
100
80
60
40
20
0
15
25
35
45
55
65Age
Similar to reference rate
Reduced by 37% (HR 0.63, p=0.05)
Reduced by 46% (HR 0.54, p=0.02)
Follow-up too short to analyse
Patients with EDSS 6.0 at age 50:27% if diagnosed before 200015% if diagnosed after 2000
(p<0.001)
1991–1995 (n=118)
1980–1990 (n=96)
1996–2000 (n=240)
2001–2005 (n=278)
2006–2010 (n=327)
2011+ (n=265)
Reference rate
Prob
abili
ty o
f rea
chin
g ED
SS 6
.0
Rate at which patients reached EDSS 6.0:
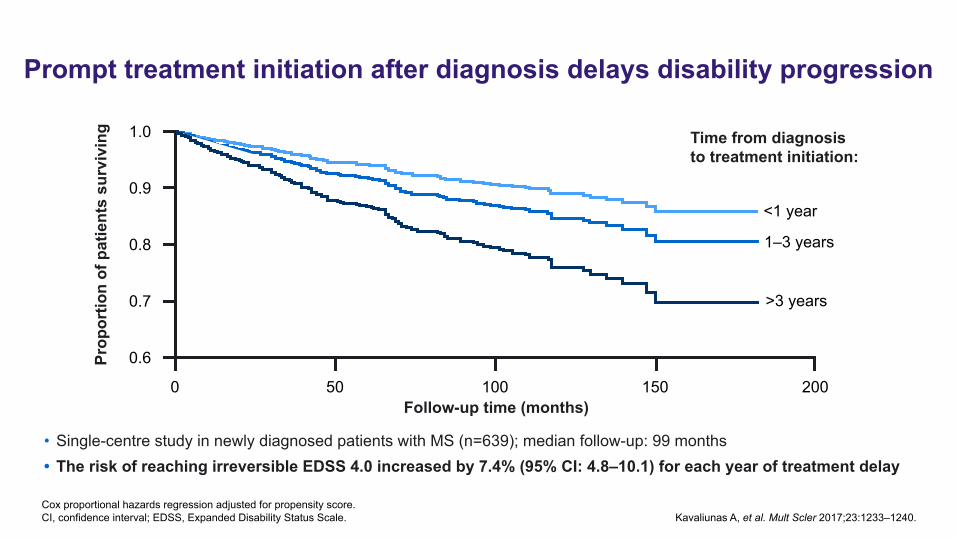
Cox proportional hazards regression adjusted for propensity score.CI, confidence interval; EDSS, Expanded Disability Status Scale. Kavaliunas A, et al. Mult Scler 2017;23:1233–1240.
Prompt treatment initiation after diagnosis delays disability progression
0.6
0.7
0.8
0.9
1.0
Prop
ortio
n of
pat
ient
s su
rviv
ing
0 50 100 150 200Follow-up time (months)
<1 year
1–3 years
>3 years
Time from diagnosis to treatment initiation:
• Single-centre study in newly diagnosed patients with MS (n=639); median follow-up: 99 months• The risk of reaching irreversible EDSS 4.0 increased by 7.4% (95% CI: 4.8–10.1) for each year of treatment delay
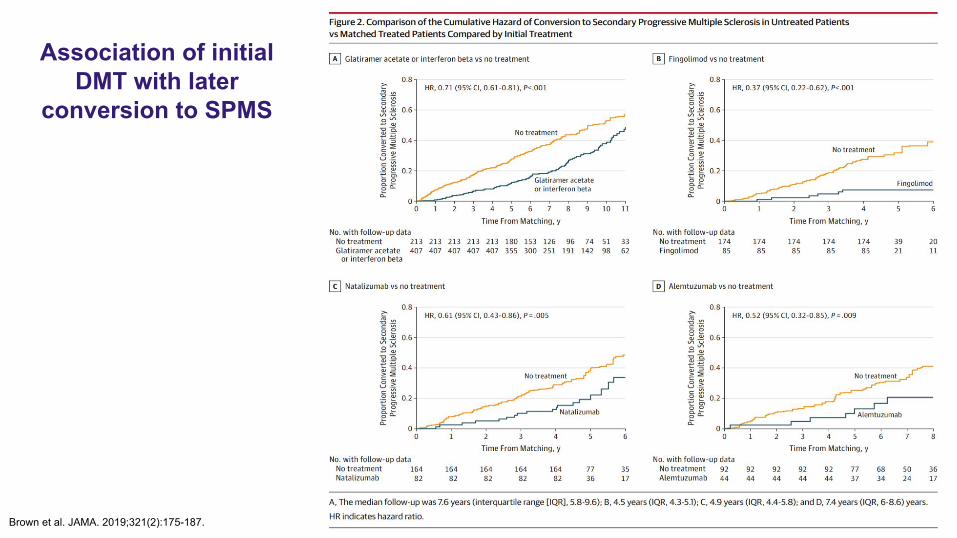
Association of initial DMT with later
conversion to SPMS
Brown et al. JAMA. 2019;321(2):175-187.
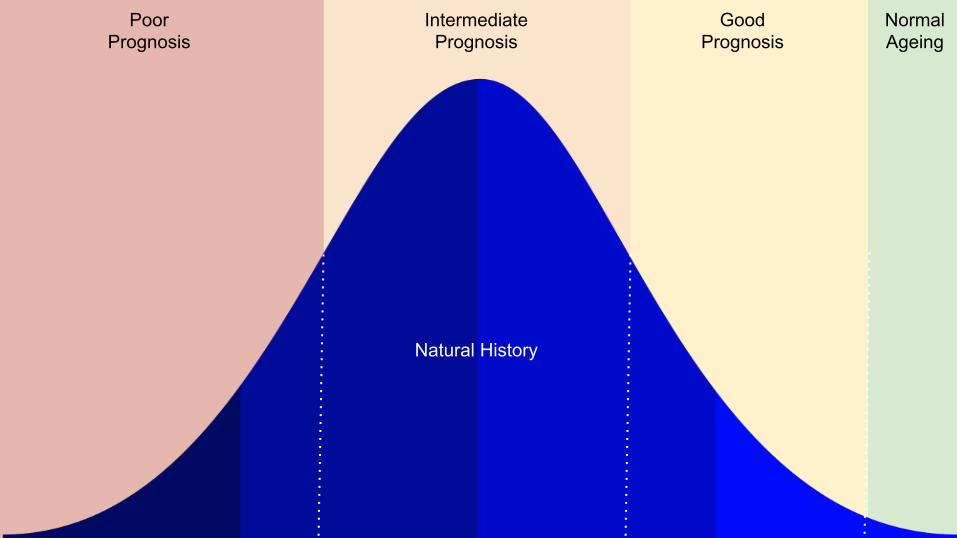
PoorPrognosis
IntermediatePrognosis
GoodPrognosis
NormalAgeing
Natural History
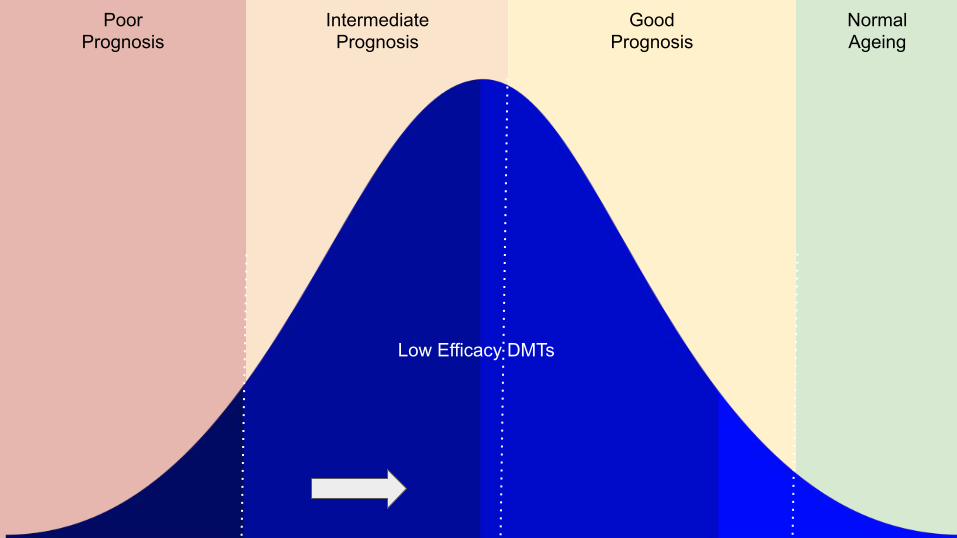
PoorPrognosis
IntermediatePrognosis
GoodPrognosis
NormalAgeing
Low Efficacy DMTs
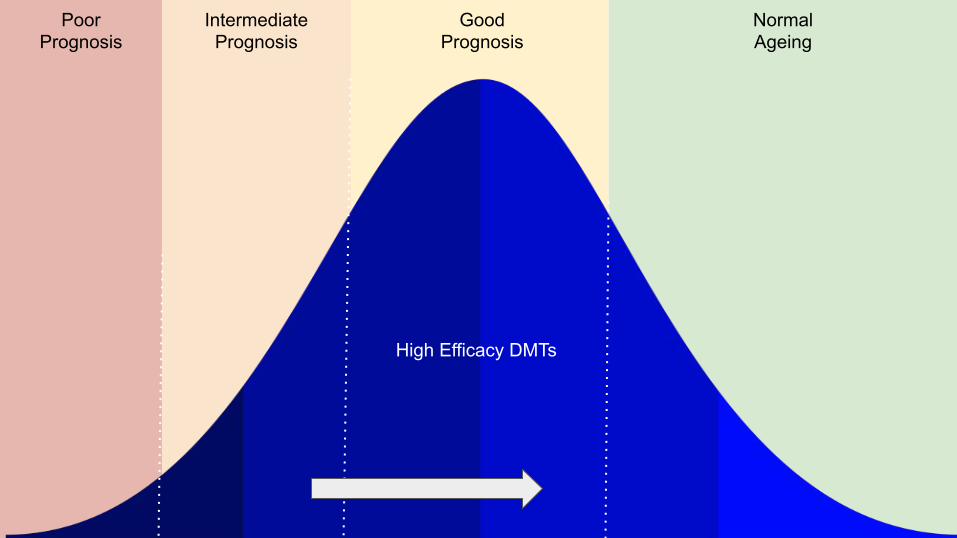
PoorPrognosis
IntermediatePrognosis
GoodPrognosis
NormalAgeing
High Efficacy DMTs
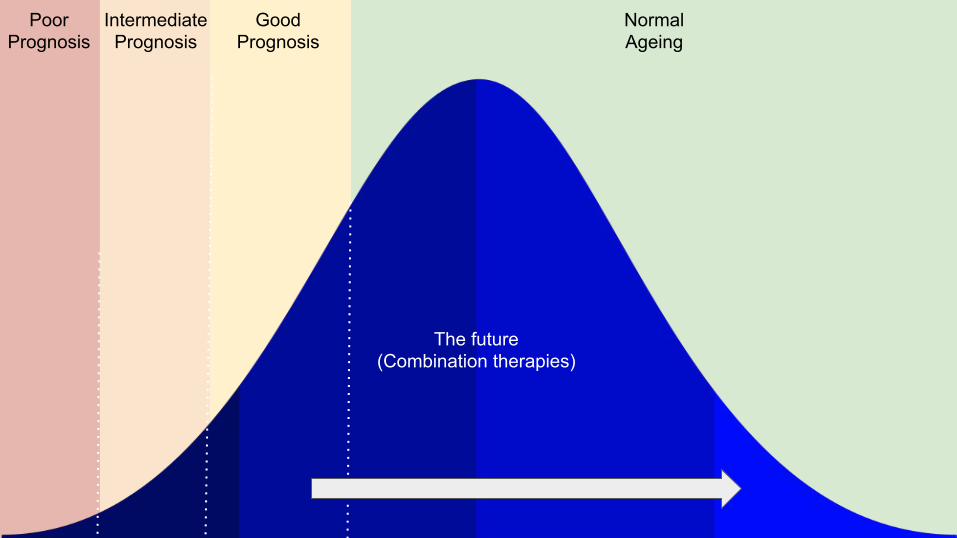
PoorPrognosis
IntermediatePrognosis
GoodPrognosis
NormalAgeing
The future(Combination therapies)
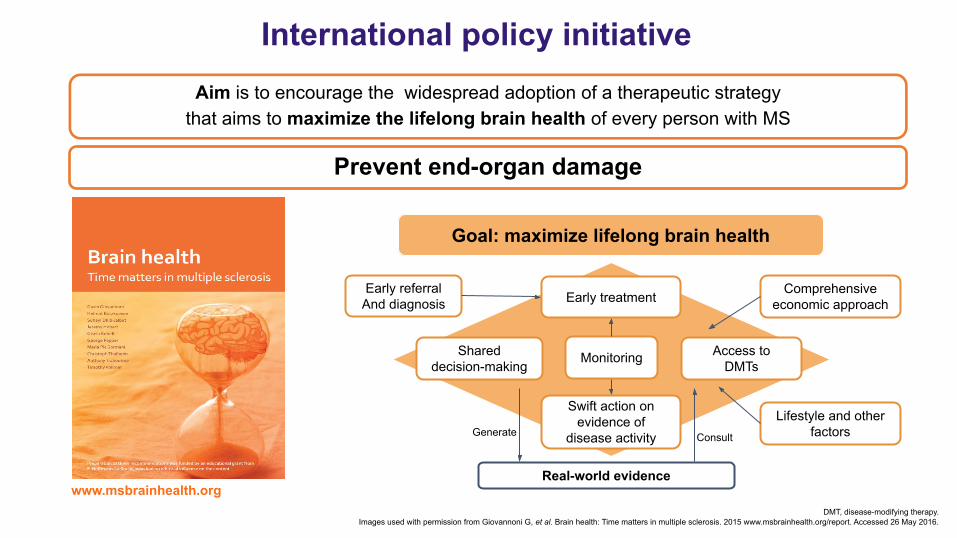
International policy initiative
www.msbrainhealth.orgDMT, disease-modifying therapy.
Images used with permission from Giovannoni G, et al. Brain health: Time matters in multiple sclerosis. 2015 www.msbrainhealth.org/report. Accessed 26 May 2016.
Aim is to encourage the widespread adoption of a therapeutic strategy that aims to maximize the lifelong brain health of every person with MS
Prevent end-organ damage
Goal: maximize lifelong brain health
Early referralAnd diagnosis Early treatment Comprehensive
economic approach
Monitoring
Swift action onevidence of
disease activity
Real-world evidence
Access to DMTs
Shareddecision-making
Lifestyle and other factorsGenerate Consult
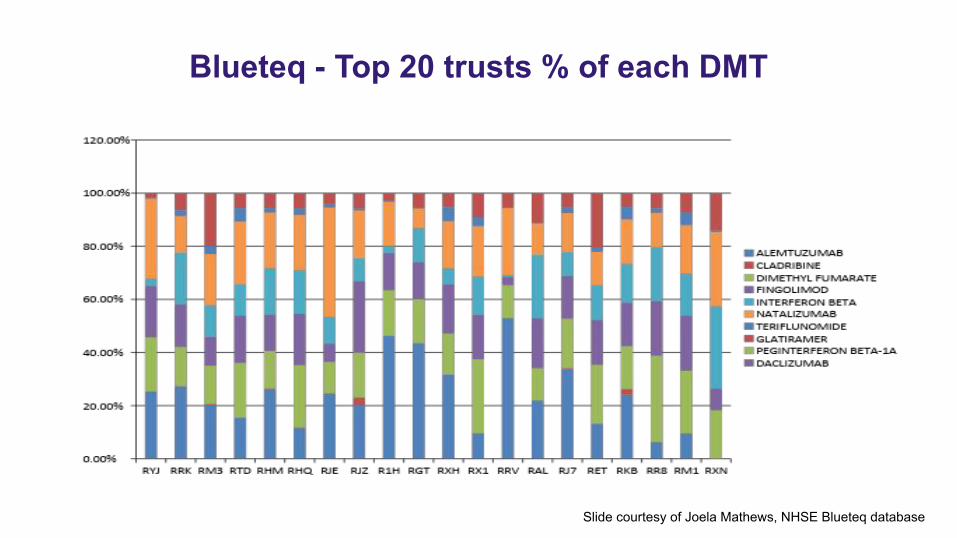
Blueteq - Top 20 trusts % of each DMT
Slide courtesy of Joela Mathews, NHSE Blueteq database
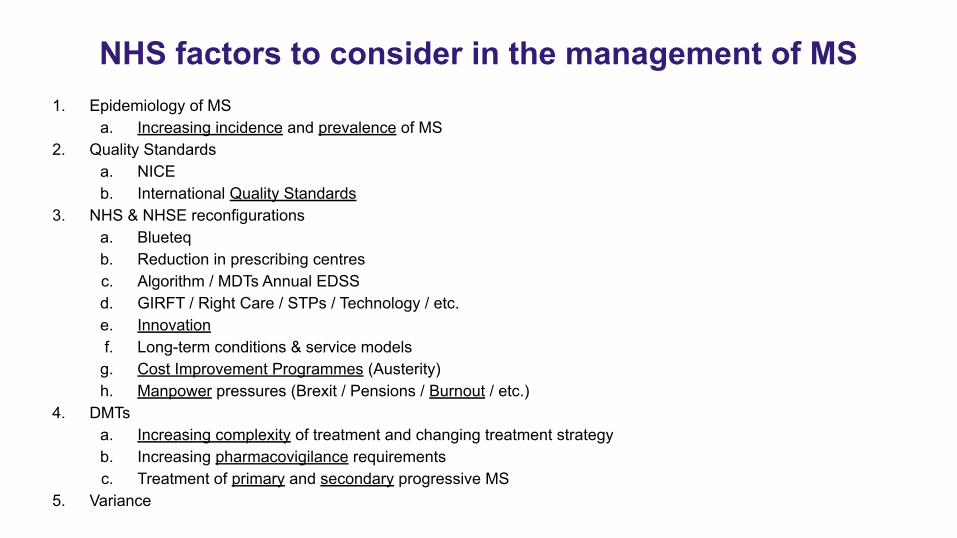
NHS factors to consider in the management of MS1. Epidemiology of MS
a. Increasing incidence and prevalence of MS2. Quality Standards
a. NICEb. International Quality Standards
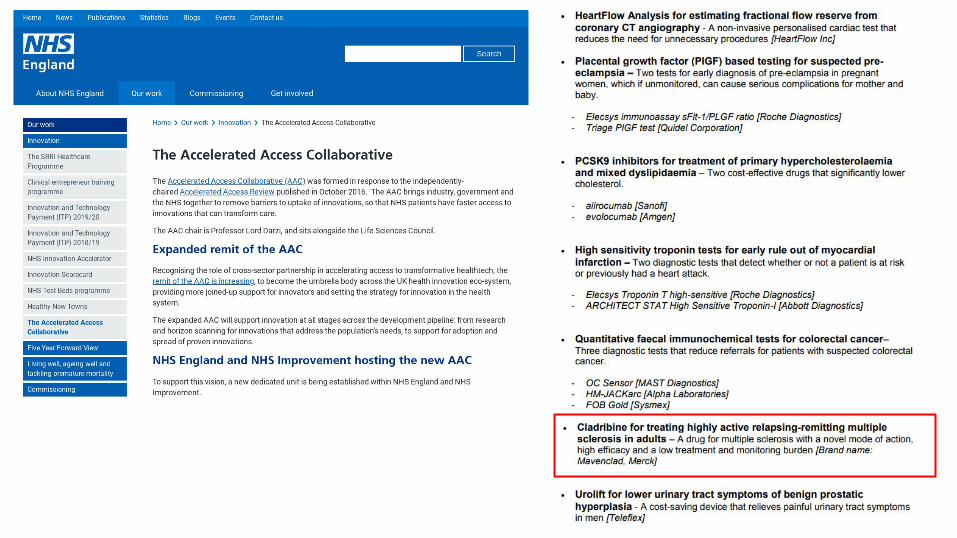
3. NHS & NHSE reconfigurationsa. Blueteqb. Reduction in prescribing centresc. Algorithm / MDTs Annual EDSSd. GIRFT / Right Care / STPs / Technology / etc.e. Innovationf. Long-term conditions & service models
g. Cost Improvement Programmes (Austerity)h. Manpower pressures (Brexit / Pensions / Burnout / etc.)
4. DMTsa. Increasing complexity of treatment and changing treatment strategyb. Increasing pharmacovigilance requirementsc. Treatment of primary and secondary progressive MS
5. Variance

Holistic management of MS

2000 Olympics Cycling Medals
2004 Olympics Cycling Medals
1996 Olympics Cycling Medals
Dave Brailsford - marginal gains
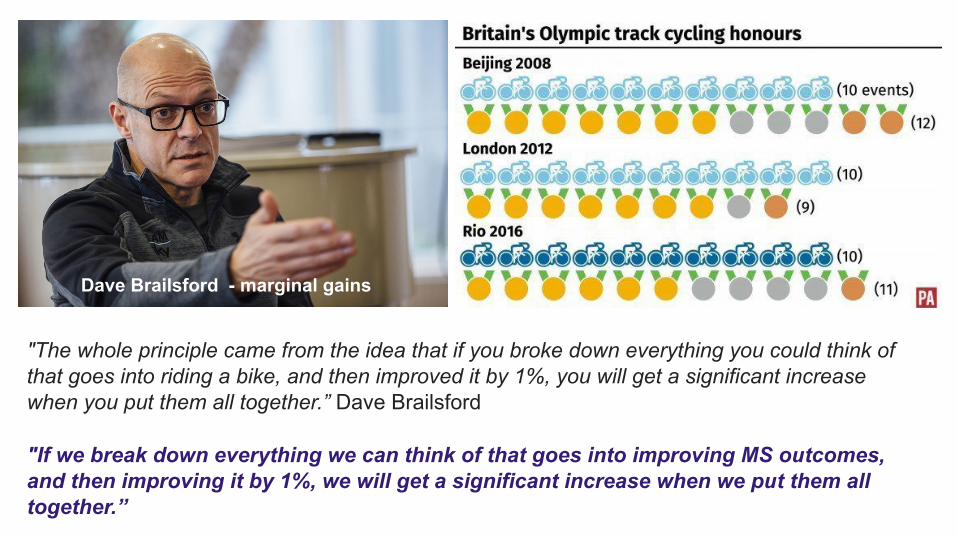
"If we break down everything we can think of that goes into improving MS outcomes, and then improving it by 1%, we will get a significant increase when we put them all together.”
"The whole principle came from the idea that if you broke down everything you could think of that goes into riding a bike, and then improved it by 1%, you will get a significant increase when you put them all together.” Dave Brailsford
Dave Brailsford - marginal gains
*
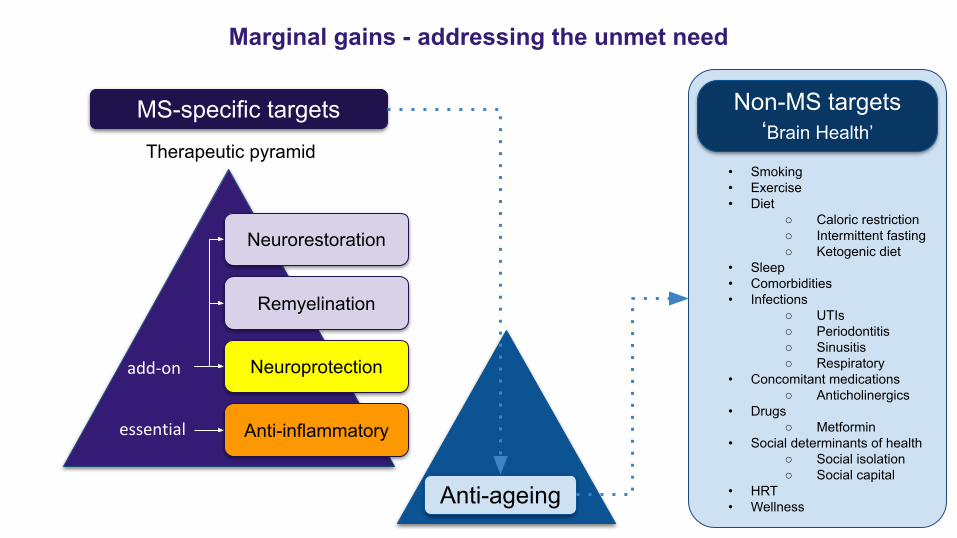
Marginal gains - addressing the unmet need
Therapeutic pyramid• Smoking• Exercise• Diet
○ Caloric restriction○ Intermittent fasting○ Ketogenic diet
• Sleep• Comorbidities• Infections
○ UTIs○ Periodontitis○ Sinusitis○ Respiratory
• Concomitant medications○ Anticholinergics
• Drugs○ Metformin
• Social determinants of health○ Social isolation○ Social capital
• HRT• Wellness
Anti-inflammatory
Neuroprotection
Remyelination
Neurorestoration
Anti-ageing
MS-specific targets Non-MS targets‘Brain Health’
Holistic management of MS
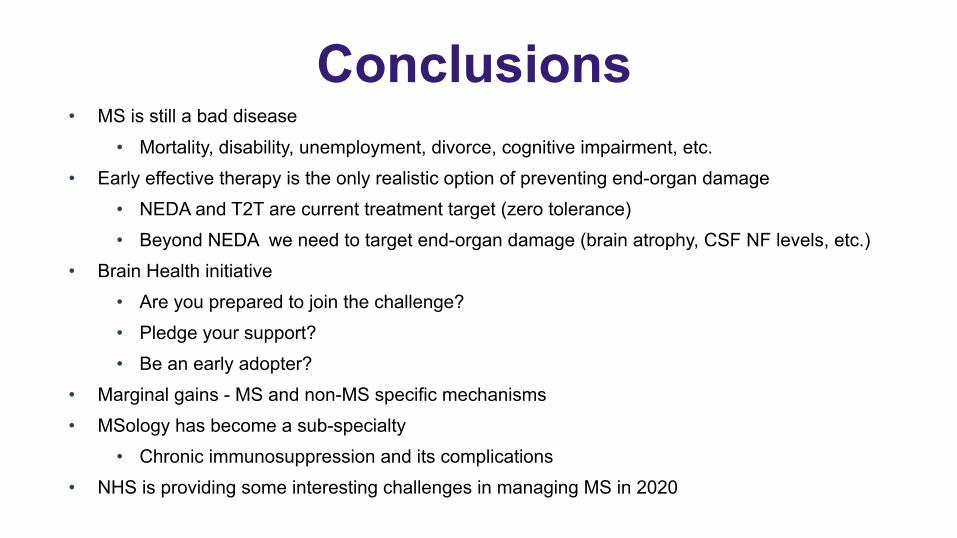
Conclusions• MS is still a bad disease
• Mortality, disability, unemployment, divorce, cognitive impairment, etc.• Early effective therapy is the only realistic option of preventing end-organ damage
• NEDA and T2T are current treatment target (zero tolerance)• Beyond NEDA we need to target end-organ damage (brain atrophy, CSF NF levels, etc.)
• Brain Health initiative• Are you prepared to join the challenge?• Pledge your support?• Be an early adopter?
• Marginal gains - MS and non-MS specific mechanisms• MSology has become a sub-specialty
• Chronic immunosuppression and its complications• NHS is providing some interesting challenges in managing MS in 2020

www.ms-res.org
www.clinicspeak.com
Back-up slides
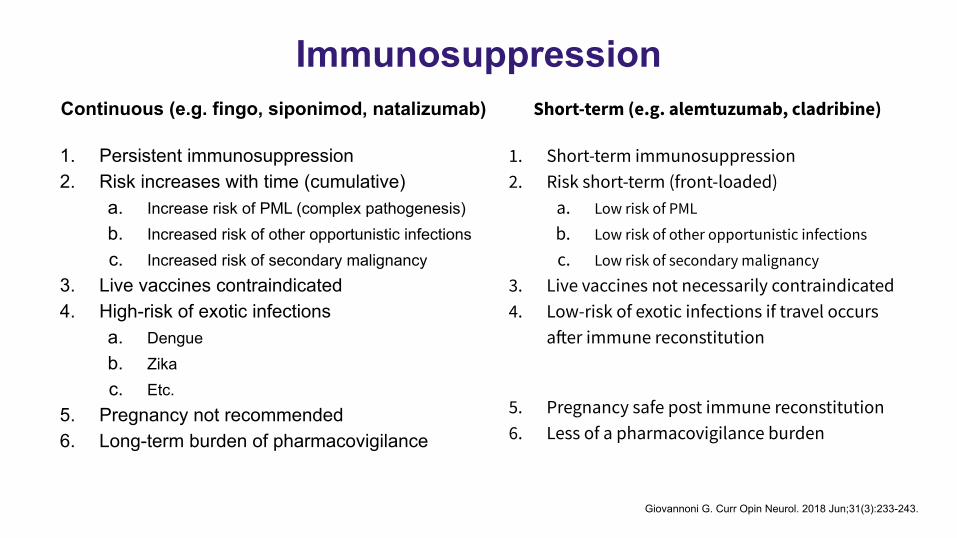
ImmunosuppressionContinuous (e.g. fingo, siponimod, natalizumab)
1. Persistent immunosuppression2. Risk increases with time (cumulative)
a. Increase risk of PML (complex pathogenesis)b. Increased risk of other opportunistic infectionsc. Increased risk of secondary malignancy
3. Live vaccines contraindicated4. High-risk of exotic infections
a. Dengueb. Zikac. Etc.
5. Pregnancy not recommended6. Long-term burden of pharmacovigilance
Short-term (e.g. alemtuzumab, cladribine)
1. Short-term immunosuppression2. Risk short-term (front-loaded)
a. Low risk of PML
b. Low risk of other opportunistic infections
c. Low risk of secondary malignancy
3. Live vaccines not necessarily contraindicated4. Low-risk of exotic infections if travel occurs
after immune reconstitution
5. Pregnancy safe post immune reconstitution6. Less of a pharmacovigilance burden
Giovannoni G. Curr Opin Neurol. 2018 Jun;31(3):233-243.
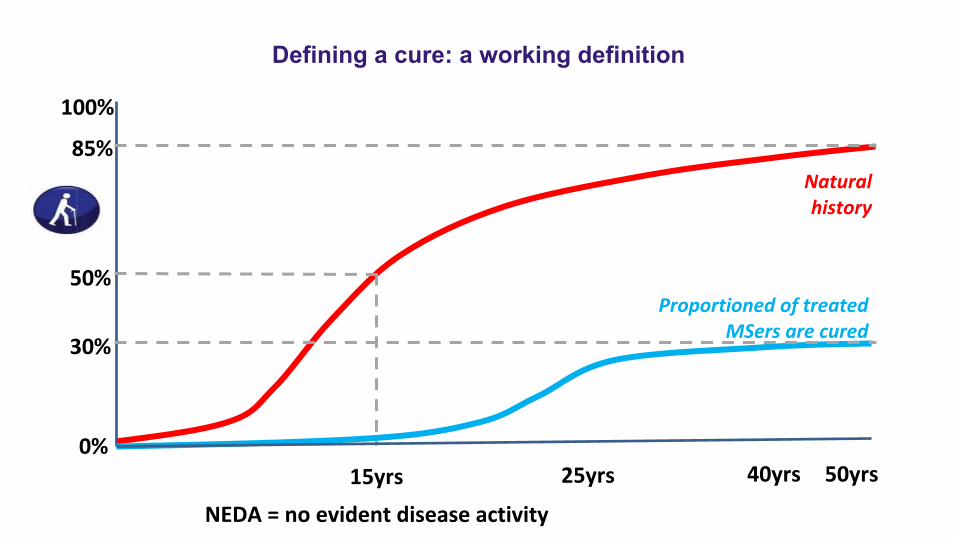
Defining a cure: a working definition
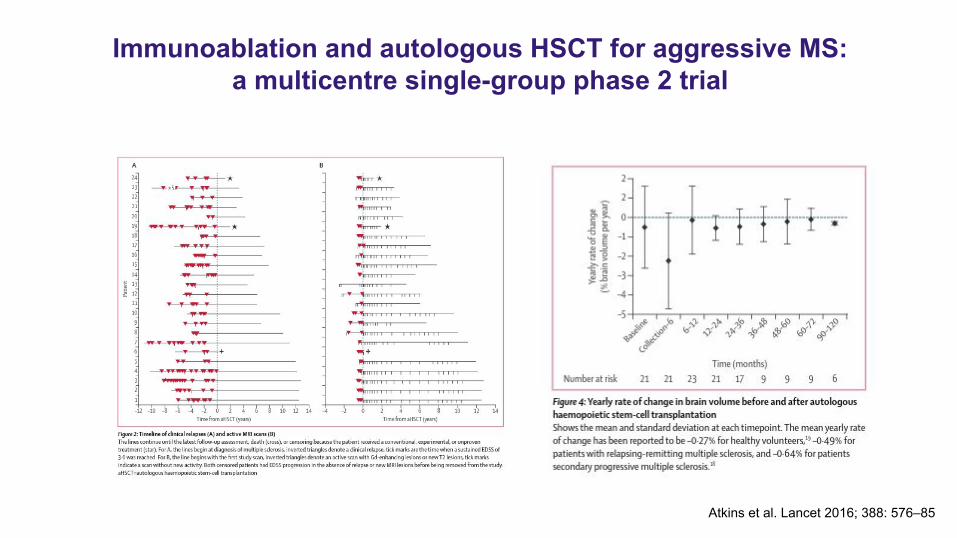
Immunoablation and autologous HSCT for aggressive MS: a multicentre single-group phase 2 trial
Atkins et al. Lancet 2016; 388: 576–85