Embed Size (px)
Citation preview
Research in Nursing & Health, 2009, 32, 163–176
Gender Comparisons ofPerceived Benefits of and
Barriers to Physical Activity inMiddle School Youth
Lorraine B. Robbins,1* Alla Sikorskii,2* Lauren M. Hamel,3** Tsu-Yin Wu,4{
JoEllen Wilbur5z
1Michigan State University College of Nursing, 422A West Fee Hall, East Lansing, MI 488242Michigan State University, Department of Statistics & Probability, East Lansing, MI
3Michigan State University, Health & Risk Communication Center, Department of Communication,
East Lansing, MI4Eastern Michigan University School of Nursing, Ypsilanti, MI
5Rush University College of Nursing, Chicago, IL
Accepted 25 October 2008
Abstract: Perceived benefits of and barriers to physical activity (PA)reported by 206 middle school boys and girls in a survey were compared.Only ‘‘take care of myself, stay in shape, and be healthier’’ emerged as agreater benefit for girls than boys. Among students not on a sports team, boysreported fewer barriers than girls. Among those selecting an active pursuit,boys perceived more barriers than girls. When controlling for sports teamparticipation and perceived benefits and barriers, boys reported moreminutes of vigorous PA than girls. As boys and girls reported relativelysimilar benefits of and barriers to PA, nurse counseling with both groups canfocus on the same information. Effort is particularly needed to increase PAamong girls. � 2008 Wiley Periodicals, Inc. Res Nurs Health 32:163–176, 2009
Keywords: physical activity; adolescents; exercise benefits; exercise barriers
National recommendations call for youth toengage in physical activity (PA) for at least 1 hourevery day, and most of the 1 hour or more shouldbe spent doing moderate or vigorous aerobic PA(U.S. Department of Health and Human Services,2008). Despite well-documented health benefits ofregular PA at this level of intensity (Daniels et al.,2005; Dugan, 2008), the percentage of youthachieving this objective decreases from 100% inelementary school to slightly less than 30% in high
school (Pate et al., 2002). Other researchers havedocumented decreases in PA as youth move tohigher grades (Kahn et al., 2008; Nader, Bradley,Houts, McRitchie, & O’Brien, 2008; Troianoet al., 2008). With the exception of those on sportsteams, many youth who are consistently activewhile in elementary school discontinue some, orall, of their PA during middle school (Pate et al.).Additional evidence indicates that girls are lessactive than boys (Kimm et al., 2000; Troiano
Contract grant sponsor: Michigan State University College of Nursing.Correspondence to Lorraine B. Robbins.*Assistant Professor.**PhD Candidate.{Associate Professor.zProfessor and Endowed Independence Foundation Chair in Nursing.Published online 11 December 2008 in Wiley InterScience
(www.interscience.wiley.com). DOI: 10.1002/nur.20311
�2008 Wiley Periodicals, Inc.
et al.). An understanding of middle school boys’and girls’ perceptions concerning PA is importantto develop interventions to prevent the decline inPA that occurs between the elementary and highschool years.
Although determinants of PA among youthhave not been clearly established, accumulatingliterature indicates that cognitive and affectivevariables, such as perceived benefits and barriers,are related to PA (Garcia et al., 1995; Heitzler,Martin, Duke, & Huhman, 2006; Sallis, Pro-chaska, & Taylor, 2000) and that specific percep-tions regarding these two variables differ betweengenders (Wu, Pender, & Noureddine, 2003) andamong age groups (Garcia, Pender, Antonakos, &Ronis, 1998; Nahas, Goldfine, & Collins, 2003).The primary purpose of this study was to identifyand compare perceived benefits of and barriers toPA among boys and girls of middle school age.Nurses could use this information in PA counsel-ing sessions to reinforce benefits of PA and address
barriers to PA identified as relevant by boys andgirls in this group.
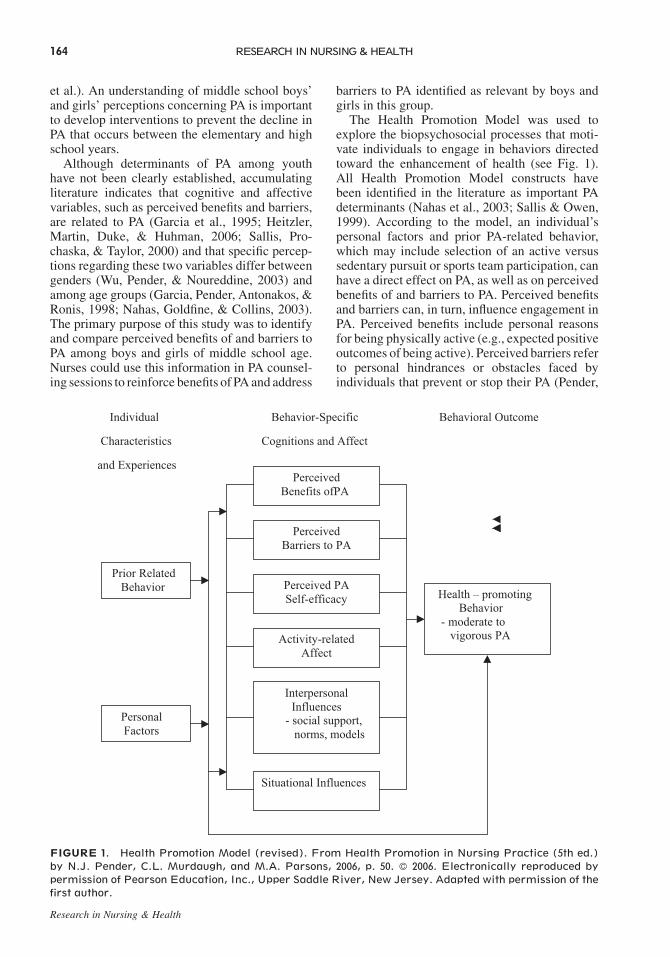
The Health Promotion Model was used toexplore the biopsychosocial processes that moti-vate individuals to engage in behaviors directedtoward the enhancement of health (see Fig. 1).All Health Promotion Model constructs havebeen identified in the literature as important PAdeterminants (Nahas et al., 2003; Sallis & Owen,1999). According to the model, an individual’spersonal factors and prior PA-related behavior,which may include selection of an active versussedentary pursuit or sports team participation, canhave a direct effect on PA, as well as on perceivedbenefits of and barriers to PA. Perceived benefitsand barriers can, in turn, influence engagement inPA. Perceived benefits include personal reasonsfor being physically active (e.g., expected positiveoutcomes of being active). Perceived barriers referto personal hindrances or obstacles faced byindividuals that prevent or stop their PA (Pender,
Research in Nursing & Health
Individual Behavior-Specific Behavioral Outcome
Characteristics Cognitions and Affect
and Experiences
PersonalFactors
PerceivedBarriers to PA
Prior RelatedBehavior
Health – promotingBehavior
- moderate tovigorous PA
PerceivedBenefits ofPA
Perceived PASelf-efficacy
Activity-relatedAffect
InterpersonalInfluences- social support,norms, models
Situational Influences
FIGURE 1. Health Promotion Model (revised). From Health Promotion in Nursing Practice (5th ed.)by N.J. Pender, C.L. Murdaugh, and M.A. Parsons, 2006, p. 50. � 2006. Electronically reproduced bypermission of Pearson Education, Inc., Upper Saddle River, New Jersey. Adapted with permission of thefirst author.
164 RESEARCH IN NURSING & HEALTH

Murdaugh, & Parsons, 2006). Guided by therelationships among these constructs as presentedin the model, we examined whether middleschool boys and girls differed regarding theinfluence of type of pursuit (active vs. sedentary)and sports team participation on perceivedbenefits of and barriers to PA. We also exploredgender differences in self-reported moderate andvigorous PA.
Five qualitative studies were found thataddressed benefits of and barriers to PA in middleschool students. Four included only girls (Grieseret al., 2006; Kientzler, 1999; Leslie et al., 1999;Taylor et al., 1999), and one involved asking boysand girls separately to talk about girls’ PA (Vu,Murrie, Gonzalez, & Jobe, 2006). Commonlyreported benefits of PA that emerged for middleschool girls in the qualitative studies were to: stayin shape (Grieser et al.; Kientzler; Leslie et al.;Taylor et al.; Vu et al.), stay healthy (Grieser et al.;Kientzler; Taylor et al.; Vu et al.), have anopportunity to socialize (Grieser et al.; Leslieet al.; Taylor et al.), have fun (Kientzler; Leslieet al.; Taylor et al.), increase energy (Grieser et al.;Vu et al.), and improve appearance (Leslie et al.;Taylor et al.). Some girls perceived being active asa benefit (Grieser et al.); others identified PA as auseful coping strategy to get things off one’s mindor relieve stress (Taylor et al.).
One barrier to middle school girls’ PA thatwas consistently noted involved feeling self-conscious or embarrassed about appearancewhile exercising. This barrier included dislikeof sweating (Grieser et al., 2006), spoiling hairand make-up (Leslie et al., 1999; Taylor et al.,1999), and shyness and low self-esteem (Vu et al.,2006). Girls identified boys as another majorbarrier due to boys’ name-calling or tauntingwhen girls are physically active (Vu et al.). Otherbarriers included dislike of certain PAs (Grieseret al.; Kientzler, 1999) and insufficient variedopportunities for girls to be active (Taylor et al.;Vu et al.). Lack of skill, interest, motivation,and time; wanting to do other things withtheir time (Vu et al.); and fear of getting hurt(Grieser et al.; Vu et al.) also emerged. Kientzler(1999) reported that the most frequently reportedbarrier among girls of middle school age wasconflict with other activities. In a quantitativestudy, researchers explored perceived barriersamong middle school girls and had findingsanalogous to those of the qualitative studies, withgirls identifying feeling self-conscious aboutappearance when exercising and lack of motiva-tion as their top barriers to PA (Robbins, Pender,& Kazanis, 2003).
We did not find any qualitative or quantitativestudies exploring perceived benefits of andbarriers to PA among middle school boys. In twoquantitative studies, boys and girls were com-pared, but in both studies the focus was on highschool students (Tappe, Duda, & Ehrnwald, 1989;Tergerson & King, 2002) and in one, only barriersto PA were considered (Tappe et al.).
In summary, information concerning middleschool girls’ perceived benefits of and barriersto PA has primarily emerged from focus groups.Quantitative studies extending or lending supportto the qualitative findings are lacking. Further-more, perceptions of middle school boys withregard to their PA have not been thoroughlyexplored, either qualitatively or quantitatively. Asa result, the literature is devoid of information tocompare boys and girls. The purpose of our studywas to begin to fill this knowledge gap byexploring whether or not middle school boysand girls differ in their perceptions. Results couldinform nurses of the extent to which counselingneeds to be gender-specific. The research ques-tions were:
1. Which benefits of and barriers to PA areperceived most commonly by middle schoolboys and girls?
2. Do middle school boys and girls differ in theirperceived benefits of and barriers to PA?
3. Do gender differences occur in perceivedbenefits of and barriers to PA between middleschool students who (a) do versus do notparticipate on a sports team and (b) select asedentary versus active pursuit?
4. After controlling for sports team participation,selection of an active versus sedentary pursuit,and perceived benefits of or barriers to PA, arethere gender differences in self-reported mod-erate and vigorous PA?
METHOD
Design
An observational cross-sectional cohort designwas used. A total of 206 middle school studentscompleted the same questionnaires at two timepoints, 2 weeks apart.
Sample
A convenience sampling strategy was used with6th, 7th, and 8th graders enrolled in a public
Research in Nursing & Health
COMPARISON OF BENEFITS AND BARRIERS / ROBBINS ET AL. 165

middle school in a Midwestern rural territoryno more than five miles from an urban area(population 22,362). The school was selectedbecause of its racially and economically diversestudent body. According to National Center forEducation Statistics (NCES, 2005-2006), 31.4%of the students in the school were AfricanAmerican, 64.1% were European American, andthe remaining students were other races. Thirty-two percent of the students were eligible for thefree or reduced-price lunch program. The school’sracial distribution reflects that of the local geo-graphic area (30.6% African American; 60.5%European American; almost 9.0% other races).The median household income in the area is$35,416 (MuniNetGuide, 2008).
One hundred five boys and 101 girls, ranging inage from 11 to 14 years old (M¼ 12.38; SD¼ .86),participated in the study. Slightly over half hadat least one parent who had graduated fromcollege. The percentage of African Americanparticipants (almost 20.0%) was lower than that ofthe school (see Table 1). The difference may haveoccurred because the NCES data collection formsdid not include a non-specific or multi-racialcategory.
Measures
Demographics. Participants responded to sin-gle item questions that addressed age, academicgrade, and race. The highest education for eitherparent or guardian was used to assess socio-economic status (Dowda, Dishman, Pfeiffer, &Pate, 2007).
Selection of an active versus sedentarypursuit. Participants responded to a single itemto identify their favorite thing to do when not inclasses at school or doing homework from a list ofeight sedentary pursuits (e.g., talking on thetelephone, watching television, shopping, playingvideo games, using the computer, reading, sittingaround or hanging out with friends, and sleeping)and one active pursuit (e.g., playing sportsor active games or exercising; 0¼ sedentary;1¼ active). In this study, strength of agreementin responses between the two testing periods wassubstantial (k¼ .70). In a previous study, in whichthe item was used (Robbins, Pis, Pender, &Kazanis, 2004), selection of an active pursuitemerged as being positively correlated withexercise frequency reported by youth in middlepuberty (p < .01).
Sports team participation. Participants respondedto a single item to indicate whether or not theywere currently on a sports team at school oroutside of school, such as those run by communitygroups Response choices were no (¼0) or yes(¼1). k of .71 indicated strong agreement betweentesting periods.
Benefits of and barriers to PA. A 10-itemPerceived Benefits Scale and 9-item PerceivedBarriers Scale (Robbins, Wu, Sikorskii, & Morley,2008) were used. Response choices for the scalesincluded: 1 (not at all true), 2 (not very true), 3(sort of true), and 4 (very true). Scores for eachparticipant were determined by computing themean of participant responses to items on eachscale. Higher scores on the Perceived Benefits andPerceived Barriers Scales corresponded with ahigher level of perceived benefits of and barriers to
Research in Nursing & Health
Table 1. Demographic Characteristics of Middle School Boys (n¼ 105) and Girls (n¼ 101)
Items Boys, n (%) Girls, n (%)
Grade6th (age 11–12) 25 (23.81) 18 (17.82)7th (age 12–13) 42 (40.00) 42 (41.58)8th (age 13–14) 38 (36.19) 41 (40.59)
RaceAfrican American 20 (19.05) 20 (19.80)European American 54 (51.43) 43 (42.56)Multi-racial 11 (10.48) 13 (12.87)Other (Asian, Hispanic or Latino, Middle
Eastern, Native American)7 (6.67) 6 (5.94)
Do not know 13 (12.38) 19 (18.81)Highest level of parent/guardian education
Did not finish or finished high school 16 (15.24) 17 (16.83)Did some college or training after high school 16 (15.24) 22 (21.78)Finished college program and has degree 56 (53.33) 51 (50.50)Do not know 17 (16.19) 11 (10.89)
166 RESEARCH IN NURSING & HEALTH

PA, respectively. Perceived Benefits Scale itemswere preceded by the phrase ‘‘A major reason forbeing physically active or exercising for me is to.’’For the Perceived Barriers Scale, each participantwas asked to ‘‘Please show how true each state-ment is regarding certain barriers or problems thatprevent or stop you from exercising, being active,or doing sports.’’ Cronbach’s alphas were .80 and.78 for the Perceived Benefits and Barriers Scales,respectively. Test-retest reliability was .70 for bothscales. Evidence of validity emerged in a priorstudy involving middle school boys and girls, inwhich mean number of days of moderate tovigorous PA was correlated positively with scoresof the Perceived Benefits Scale and negativelywith scores of the Perceived Barriers Scale(Robbins et al., 2008).
Number of days of PA. To determine thenumber of days of PA per week, we used thefollowing single item: ‘‘In a typical or usual week,how many days do you do moderate to vigorousPA for a total of 60 minutes (1 hour) or moreper day?’’ Response choices included: (1) 0 daysper week; (2) 1 day per week; (3) 2 days per week;(4) 3 days per week; (5) 4 days per week; (6) 5 daysper week; (7) 6 or more days per week (Hagler,Calfas, Norman, Sallis, & Patrick, 2006). Test-retest reliability was .72 in our study.
Number of minutes of PA. The Child andAdolescent Activity Log (CAAL) was adaptedfrom the instrument used by Garcia, George,Coviak, Antonakos, and Pender (1997). TheCAAL consists of a list of 22 different PAs tohelp participants identify those that they hadparticipated in during the past 2 weekdays and thepast Sunday (same list used for each day). Afteridentifying their PAs for a particular day, partic-ipants reported their number of minutes ofparticipation and rated the intensity of each PA(moderate or vigorous). Content and criterionvalidity have been established and daily test-retestcorrelations (45-minute interval) ranging from.73 to .94 have been reported (Garcia et al., 1997).
Procedures
The University Biomedical and Health Institu-tional Review Board approved procedures forprotecting participants. Two physical education(PE) teachers (trained by the first author) dis-tributed envelopes, each containing a letterexplaining the study, parent/guardian consentform, and student assent form, to all interestedmiddle school boys and girls. Students wererecruited for participation during both fall and
spring semesters of a single school year. The PEteachers told the students that they or their parents/guardians should contact the researchers with anyquestions. Of the 500 students invited to partic-ipate, 262 (52.4%) returned signed consent andassent forms to their teacher.
On the Friday prior to data collection, each PEteacher followed a written protocol to inform theparticipants that they should not change their PA,but needed to remember the number of minutes ofmoderate to vigorous PA they engaged in over thenext few days because they would be asked torecall the information during data collection thenext week. Examples of moderate (e.g., fastwalking) to vigorous (e.g., running) PA, whichwas described as ‘‘moving or being active enoughso that they were breathing hard and sweating andtheir heart was beating fast,’’ were presented viapictures and demonstration to assist participantsin evaluating intensity. Participants were toldthat time used for rest or snack breaks should notbe included in their reported number of minutesof PA.
At the time of data collection prior to admin-istering the questionnaire to all consentedstudents, the first author and a research assistanttrained by the first author explained the nature ofthe study and informed the students that parti-cipation was voluntary and could be stoppedat any time without penalty. The researchersremained in the room during questionnairecompletion and responded to any questions.Participants were given the same questionnairesto complete at time 1 and again 2 weeks later fora reliability check. At both time periods, theresearchers used the written protocol to reviewexamples of moderate to vigorous PA for theparticipants. The researchers asked participants torecall the PA that they had done over the past2 weekdays and past Sunday and complete theCAAL for each of the 3 days.
During the data collection times, 56 studentsdid not complete the questionnaire due to schoolabsences (n¼ 51) or last-minute refusal (n¼ 5),resulting in a response rate of 41.2%. Completedata were collected in November 2005 (fallsemester) from 108 students and in February2006 (spring semester) from a different group of98 students.
Students completed all instruments on either aTuesday or Wednesday and reported the minutesof moderate and vigorous PA that they hadengaged in last Sunday and the past 2 weekdays(Monday and Friday; Monday and Tuesday).Although we preferred to collect all data onWednesday for the past 3 days, we were unable to
Research in Nursing & Health
COMPARISON OF BENEFITS AND BARRIERS / ROBBINS ET AL. 167
do so due to unforeseen changes in PE classactivities (e.g., student assemblies). To ensureparticipant attention to and completion of theitems, researchers read the instructions for ques-tionnaire completion along with each item to smallgroups of participants. Participants were asked toavoid progressing to the next page or instrumentuntil all items on the current page had beencompleted.
Analyses
Statistical analyses were conducted using theStatistical Package for the Social Sciences (SPSS)version 15.0 for Windows (SPSS, 2006) andStatistical Analysis Software (SAS) version 9(SAS Institute, 2002-2003). Descriptive statisticswere obtained for socio-demographic, type ofpursuit, current sports team participation, per-ceived benefits of and barriers to PA, and threePA variables (see Tables 1 and 2). t-tests, point-biserial correlations, and chi-square tests (Phi,Cramer’s V, and Pearson Chi Square) were used toexamine differences by gender.
Research Questions 1 and 2 were designedto identify and note any gender differences inPerceived Benefits and Barriers Scale items.Frequencies for the items in these scales wereobtained separately for boys and girls. To testfor gender differences in responses to the itemsof each scale, multivariate analysis of variance(MANOVA) was performed.
Research Question 3 focused on gender differ-ences in perceived benefits of and barriers to PA by
(a) sports team participation and (b) selection of anactive versus sedentary pursuit. The outcomes ofperceived benefits of and barriers to PA wererelated to the following explanatory variables:(a) gender, current sports team participation, andtheir interaction; and (b) gender, selection of anactive versus sedentary pursuit, and their interac-tion. From these regression models, least squares(LS) means by the interaction terms were calcu-lated (Searle, Speed, & Miliken, 1980). Genderdifferences in LS means were evaluated.
Research Question 4 addressed gender differ-ences in self-reported moderate and vigorousPA after controlling for sports team participationor selection of an active versus sedentary pursuit,and perceived benefits of or barriers to PA. Theoutcomes in the regression models were moderateand vigorous PA across 3 days. All statistical testswere two-sided.
RESULTS
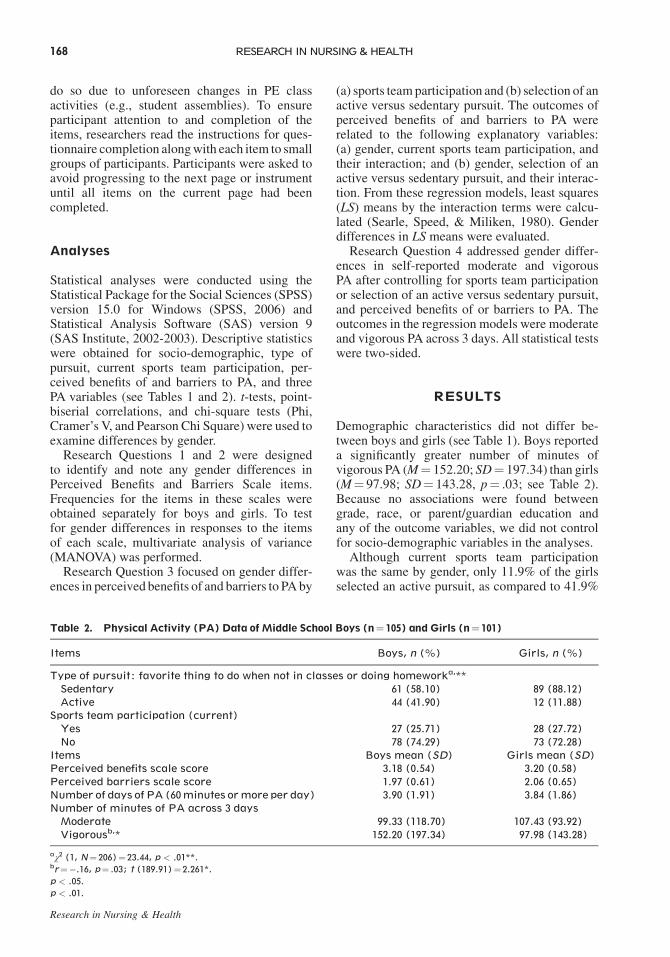
Demographic characteristics did not differ be-tween boys and girls (see Table 1). Boys reporteda significantly greater number of minutes ofvigorous PA (M¼ 152.20; SD¼ 197.34) than girls(M¼ 97.98; SD¼ 143.28, p¼ .03; see Table 2).Because no associations were found betweengrade, race, or parent/guardian education andany of the outcome variables, we did not controlfor socio-demographic variables in the analyses.
Although current sports team participationwas the same by gender, only 11.9% of the girlsselected an active pursuit, as compared to 41.9%
Research in Nursing & Health
Table 2. Physical Activity (PA) Data of Middle School Boys (n¼ 105) and Girls (n¼ 101)
Items Boys, n (%) Girls, n (%)
Type of pursuit: favorite thing to do when not in classes or doing homeworka,**Sedentary 61 (58.10) 89 (88.12)Active 44 (41.90) 12 (11.88)
Sports team participation (current)Yes 27 (25.71) 28 (27.72)No 78 (74.29) 73 (72.28)
Items Boys mean (SD) Girls mean (SD)Perceived benefits scale score 3.18 (0.54) 3.20 (0.58)Perceived barriers scale score 1.97 (0.61) 2.06 (0.65)Number of days of PA (60 minutes or more per day) 3.90 (1.91) 3.84 (1.86)Number of minutes of PA across 3 days
Moderate 99.33 (118.70) 107.43 (93.92)Vigorousb,* 152.20 (197.34) 97.98 (143.28)
aw2 (1, N¼ 206)¼ 23.44, p < .01**.br¼�.16, p¼ .03; t (189.91)¼ 2.261*.
p < .05.
p < .01.
168 RESEARCH IN NURSING & HEALTH

of the boys (p < .01; see Table 2). More than 10%of the boys reported that playing video games(24.8%) and using the computer (10.5%) weretheir favorite things to do when not in school ordoing homework. For girls, more than 10%reported shopping (25.7%), talking on the tele-phone (13.9%), sitting around and hanging outwith friends (13.9%), and using the computer(10.9%) as their favorite things to do (data notshown in tables).
Research Question 1: Benefits of andBarriers to PA Perceived by MiddleSchool Boys and Girls
As shown in Table 3, boys’ top benefits were to: (a)improve or have more athletic skills; (b) take careof myself, stay in shape, and be healthier; and (c)have a chance to play and be active. Girls top threebenefits were similar to those of boys except forthe order of the items and the inclusion of ‘‘proveto myself what I can do physically’’ in place of‘‘improve or have more athletic skills.’’ Overall,for seven of the items, boys and girls both had amean score of � 3, which indicates that eachbenefit was a reason for them to be physicallyactive. Both girls and boys gave the lowest scoresto: look better; spend time with family, friends, orteam members; and have other people see my
athletic skill or fitness. Thirty-three students(15 boys, 18 girls) wrote in an additional benefit.The most common recurring write-in benefit of PAwas weight control, which was reported by girlsonly.
The top three barriers were the same for boysand girls: (a) minor aches and pains from activity;(b) tiredness; and (c) too busy. The mean scores forall items were below 2.5 suggesting that, overall,the barriers to PA were not very true for them (seeTable 4). Twenty-five students (11 boys, 14 girls)wrote in an additional barrier to PA. The mostcommon recurring write-in barrier to PA wasasthma or trouble breathing.
Research Question 2: GenderDifferences for Items Comprising thePerceived Benefits and Barriers Scales
Significant gender differences were noted forthe MANOVA of Perceived Benefits Scale items,F(10, 195)¼ 2.46, p < .01 (data not shown intables). Follow-up t-test results for gender by itemindicated that one item, ‘‘take care of myself,stay in shape, and be healthier,’’ was a greaterperceived benefit of PA for girls than boys(p¼ .02; see Table 3). No gender differencesemerged in the MANOVA of Perceived BarriersScale items.
Research in Nursing & Health
Table 3. BenefitsofPhysicalActivityPerceivedbyMiddleSchoolBoysandGirls—MeanScoresandStandardDeviations (N¼ 206)
Scaleitem
Boys mean(SD)
Scaleitem
Girls mean(SD)
Improve or have more athletic skill 3.50 (0.87) Take care of myself, stay in shape,and be healthiera,*
3.63 (0.63)
Take care of myself, stay in shape,and be healthiera
3.41 (0.76) Have a chance to play or be active 3.42 (0.83)
Have a chance to play or be active 3.32 (0.83) Prove to myself what I can dophysically
3.37 (0.87)
Have more energy 3.28 (0.86) Have more energy 3.33 (0.92)Have fun or be part of a fun group
or activity3.18 (0.93) Improve or have more athletic skill 3.28 (0.93)
Make me happier 3.17 (0.96) Make me happier 3.26 (0.90)Prove to myself what I can do
physically3.17 (0.94) Have fun or be part of a fun group
or activity3.25 (1.04)
Look better 3.14 (0.94) Look better 2.98 (1.13)Spend time with family, friends, or
team members2.90 (0.99) Spend time with family, friends,
or team members2.95 (1.03)
Have other people see my athletic skillor fitness
2.71 (1.03) Have other people see my athleticskill or fitness
2.53 (1.11)
Scale range is 1–4. Higher mean scores denote more agreement with statement.ar¼ .16; t (199.83)¼�2.32*.
p < .05.
COMPARISON OF BENEFITS AND BARRIERS / ROBBINS ET AL. 169
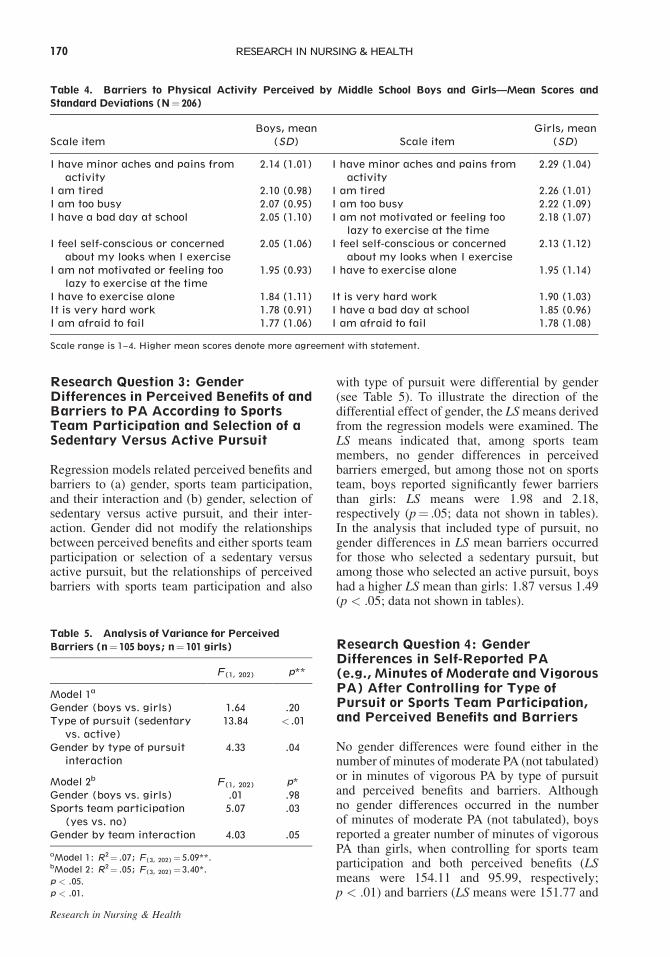
Research Question 3: GenderDifferences in Perceived Benefits of andBarriers to PA According to SportsTeam Participation and Selection of aSedentary Versus Active Pursuit
Regression models related perceived benefits andbarriers to (a) gender, sports team participation,and their interaction and (b) gender, selection ofsedentary versus active pursuit, and their inter-action. Gender did not modify the relationshipsbetween perceived benefits and either sports teamparticipation or selection of a sedentary versusactive pursuit, but the relationships of perceivedbarriers with sports team participation and also
with type of pursuit were differential by gender(see Table 5). To illustrate the direction of thedifferential effect of gender, the LS means derivedfrom the regression models were examined. TheLS means indicated that, among sports teammembers, no gender differences in perceivedbarriers emerged, but among those not on sportsteam, boys reported significantly fewer barriersthan girls: LS means were 1.98 and 2.18,respectively (p¼ .05; data not shown in tables).In the analysis that included type of pursuit, nogender differences in LS mean barriers occurredfor those who selected a sedentary pursuit, butamong those who selected an active pursuit, boyshad a higher LS mean than girls: 1.87 versus 1.49(p < .05; data not shown in tables).
Research Question 4: GenderDifferences in Self-Reported PA(e.g., Minutes of Moderate and VigorousPA) After Controlling for Type ofPursuit or Sports Team Participation,and Perceived Benefits and Barriers
No gender differences were found either in thenumber of minutes of moderate PA (not tabulated)or in minutes of vigorous PA by type of pursuitand perceived benefits and barriers. Althoughno gender differences occurred in the numberof minutes of moderate PA (not tabulated), boysreported a greater number of minutes of vigorousPA than girls, when controlling for sports teamparticipation and both perceived benefits (LSmeans were 154.11 and 95.99, respectively;p < .01) and barriers (LS means were 151.77 and
Research in Nursing & Health
Table 4. Barriers to Physical Activity Perceived by Middle School Boys and Girls—Mean Scores andStandard Deviations (N¼ 206)
Scale itemBoys, mean
(SD) Scale itemGirls, mean
(SD)
I have minor aches and pains fromactivity
2.14 (1.01) I have minor aches and pains fromactivity
2.29 (1.04)
I am tired 2.10 (0.98) I am tired 2.26 (1.01)I am too busy 2.07 (0.95) I am too busy 2.22 (1.09)I have a bad day at school 2.05 (1.10) I am not motivated or feeling too
lazy to exercise at the time2.18 (1.07)
I feel self-conscious or concernedabout my looks when I exercise
2.05 (1.06) I feel self-conscious or concernedabout my looks when I exercise
2.13 (1.12)
I am not motivated or feeling toolazy to exercise at the time
1.95 (0.93) I have to exercise alone 1.95 (1.14)
I have to exercise alone 1.84 (1.11) It is very hard work 1.90 (1.03)It is very hard work 1.78 (0.91) I have a bad day at school 1.85 (0.96)I am afraid to fail 1.77 (1.06) I am afraid to fail 1.78 (1.08)
Scale range is 1–4. Higher mean scores denote more agreement with statement.
Table 5. Analysis of Variance for PerceivedBarriers (n¼ 105 boys; n¼ 101 girls)
F(1, 202) p**
Model 1a
Gender (boys vs. girls) 1.64 .20Type of pursuit (sedentary
vs. active)13.84 < .01
Gender by type of pursuitinteraction
4.33 .04
Model 2b F(1, 202) p*Gender (boys vs. girls) .01 .98Sports team participation
(yes vs. no)5.07 .03
Gender by team interaction 4.03 .05
aModel 1: R2¼ .07; F(3, 202)¼ 5.09**.bModel 2: R2¼ .05; F(3, 202)¼ 3.40*.
p < .05.
p < .01.
170 RESEARCH IN NURSING & HEALTH
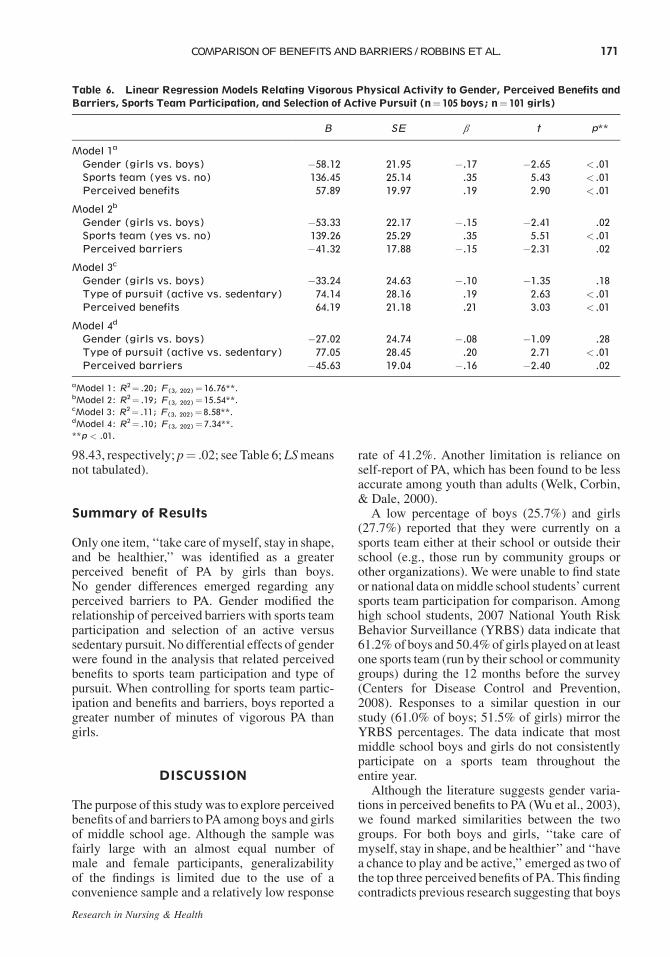
98.43, respectively; p¼ .02; see Table 6; LS meansnot tabulated).
Summary of Results
Only one item, ‘‘take care of myself, stay in shape,and be healthier,’’ was identified as a greaterperceived benefit of PA by girls than boys.No gender differences emerged regarding anyperceived barriers to PA. Gender modified therelationship of perceived barriers with sports teamparticipation and selection of an active versussedentary pursuit. No differential effects of genderwere found in the analysis that related perceivedbenefits to sports team participation and type ofpursuit. When controlling for sports team partic-ipation and benefits and barriers, boys reported agreater number of minutes of vigorous PA thangirls.
DISCUSSION
The purpose of this study was to explore perceivedbenefits of and barriers to PA among boys and girlsof middle school age. Although the sample wasfairly large with an almost equal number ofmale and female participants, generalizabilityof the findings is limited due to the use of aconvenience sample and a relatively low response
rate of 41.2%. Another limitation is reliance onself-report of PA, which has been found to be lessaccurate among youth than adults (Welk, Corbin,& Dale, 2000).
A low percentage of boys (25.7%) and girls(27.7%) reported that they were currently on asports team either at their school or outside theirschool (e.g., those run by community groups orother organizations). We were unable to find stateor national data on middle school students’ currentsports team participation for comparison. Amonghigh school students, 2007 National Youth RiskBehavior Surveillance (YRBS) data indicate that61.2% of boys and 50.4% of girls played on at leastone sports team (run by their school or communitygroups) during the 12 months before the survey(Centers for Disease Control and Prevention,2008). Responses to a similar question in ourstudy (61.0% of boys; 51.5% of girls) mirror theYRBS percentages. The data indicate that mostmiddle school boys and girls do not consistentlyparticipate on a sports team throughout theentire year.
Although the literature suggests gender varia-tions in perceived benefits to PA (Wu et al., 2003),we found marked similarities between the twogroups. For both boys and girls, ‘‘take care ofmyself, stay in shape, and be healthier’’ and ‘‘havea chance to play and be active,’’ emerged as two ofthe top three perceived benefits of PA. This findingcontradicts previous research suggesting that boys
Research in Nursing & Health
Table 6. Linear Regression Models Relating Vigorous Physical Activity to Gender, Perceived Benefits andBarriers, Sports Team Participation, and Selection of Active Pursuit (n¼ 105 boys; n¼ 101 girls)
B SE b t p**
Model 1a
Gender (girls vs. boys) �58.12 21.95 �.17 �2.65 < .01Sports team (yes vs. no) 136.45 25.14 .35 5.43 < .01Perceived benefits 57.89 19.97 .19 2.90 < .01
Model 2b
Gender (girls vs. boys) �53.33 22.17 �.15 �2.41 .02Sports team (yes vs. no) 139.26 25.29 .35 5.51 < .01Perceived barriers �41.32 17.88 �.15 �2.31 .02
Model 3c
Gender (girls vs. boys) �33.24 24.63 �.10 �1.35 .18Type of pursuit (active vs. sedentary) 74.14 28.16 .19 2.63 < .01Perceived benefits 64.19 21.18 .21 3.03 < .01
Model 4d
Gender (girls vs. boys) �27.02 24.74 �.08 �1.09 .28Type of pursuit (active vs. sedentary) 77.05 28.45 .20 2.71 < .01Perceived barriers �45.63 19.04 �.16 �2.40 .02
aModel 1: R2¼ .20; F(3, 202)¼ 16.76**.bModel 2: R2¼ .19; F(3, 202)¼ 15.54**.cModel 3: R2¼ .11; F(3, 202)¼ 8.58**.dModel 4: R2¼ .10; F(3, 202)¼ 7.34**.
**p < .01.
COMPARISON OF BENEFITS AND BARRIERS / ROBBINS ET AL. 171

view intrinsic fulfillment (e.g., brought about bythe activity itself) as most important, whereasgirls value extrinsic rewards or outcomes (Biddle& Armstrong, 1992; Burrows, Eves, & Cooper,1999). The finding that ‘‘take care of myself, stayin shape, and be healthier’’ and ‘‘improve or havemore athletic skill’’ were the most importantbenefits of PA among girls and boys, respectively,is consistent with qualitative studies involvingboys (Allison et al., 2005) and girls (Burrowset al.; Grieser et al., 2006; Vu et al., 2006) and onequantitative study with high school students(Tergerson & King, 2002).
The three items least likely to be perceived asbenefits of PA were identical for the two groups.The fact that one of these items included‘‘spending time with family, friends, and teammembers’’ was surprising in lieu of the importanceplaced on the social benefits of PA emphasized byyouth (O’Dea, 2003), particularly among girls(Grieser et al., 2006), and the fact that literaturefocusing on health-related behaviors among youthemphasizes the importance of peers (Zakarian,Hovell, Hofstetter, Sallis, & Keating, 1994). Oneplausible explanation is that this age group isstriving to gain independence from parents(Radzik, Sherer, & Neinstein, 2002) and, as aresult, may have been negatively influenced by theinclusion of ‘‘family’’ in the item. Anotherpossibility for the finding is that boys and girlsvalue ‘‘having fun with others’’ more than justspending time with others (Allison et al., 2005;Burrows et al., 1999; O’Dea), the latter of whichcan be accomplished through mechanisms otherthan PA.
Although making an impression on others wasperceived as an important benefit of PA amonghigh school boys participating in focus groups(Allison et al., 2005), ‘‘having other people see myathletic skill or fitness’’ emerged last in impor-tance for the middle school boys, as well as thegirls in our study. Perhaps this benefit is moresalient for older boys and less so for girls oryounger boys, although sufficient evidence islacking to support this contention.
Although ‘‘take care of myself, stay in shape,and be healthier’’ emerged as one of the top threebenefits of PA for boys and girls, the item’s meanscore was significantly lower for boys than girls.One plausible reason for this discrepancy is thatboys view health benefits in terms of appearance(looking attractive, fit, and healthy to impressothers) rather than caring for oneself to maintainpersonal health (Allison et al., 2005). Although ahigher mean score for girls than boys was expectedfor the barrier item ‘‘I am self-conscious about my
looks when I exercise’’ (Robbins et al., 2003), nogender differences occurred. Some support forthis finding was achieved from focus groups withmale youth, who identified personal physical andpsychological characteristics, such as being over-weight or too short for certain activities or lackingconfidence, as barriers to PA (Allison et al.).
The finding that ‘‘I am tired’’ and ‘‘I am toobusy’’ emerged among the top three barriers toPA supported similar results from numerouspreviously conducted studies involving youth(Kimm et al., 2006; Tappe et al., 1989; Tergerson& King, 2002). The top barrier, ‘‘I have minoraches and pains from PA,’’ was a notable deviationfrom the reported literature because, to ourknowledge, this problem has never been specifi-cally cited as a major barrier. In focus groupsconducted with middle school girls, however, themost commonly stated negative aspect of PA wasthe potential for injury or getting hurt. For thesegirls, injuries included minor discomforts, such assore muscles (Grieser et al., 2006). As boys alsoidentified minor aches and pains from PA as a topbarrier, addressing this issue with youth of this agemay prove fruitful.
Being too tired or busy are commonly reportedas top barriers among high school students, whomust commit a considerable amount of timeto school work, after-school jobs, and variousresponsibilities (Allison et al., 2005; Dwyer et al.,2006; Kubik, Lytle, & Fulkerson, 2005). Onepossible reason underlying the emergence of thesebarriers for the middle school students in this studymay be their preferred involvement in time-consuming sedentary pursuits. For example, useof the Internet is increasingly becoming a concerndue to the rapid diffusion of Broadband andgreater availability of information technology atschool and home (Koezuka et al., 2006).
Only a few boys and girls reported a benefit orbarrier not already listed as a scale item. Parentalinfluence on their children’s PA was not evidentfrom the write-in responses. Besides providingencouragement for PA (Duncan, Duncan, &Strycker, 2005), parents serve as role models andare central in organizing and funding theirchildren’s PAs (Davison, Cutting, & Birch, 2003).For example, a middle school student with aworking single parent or dual working parentsmay be instructed to stay inside rather than outsidewithout supervision. As a result, parents caninfluence their children’s perceptions of thebenefits of and barriers to PA and, ultimately,facilitate or hinder the behavior.
Findings were similar for the effects of theenvironment, with no participant identifying any
Research in Nursing & Health
172 RESEARCH IN NURSING & HEALTH

of the barriers frequently noted in the literature(e.g., bad weather or lack of equipment or trans-portation) as major impediments to PA (Yin,Hanes, et al., 2005; Yin, Moore, et al., 2005).Either the idea that the environment and familycan facilitate or encumber PA may not yet bereadily discernible to youth of middle school age,or another investigative approach may be neededto specifically elucidate related barriers. Forexample, in focus group discussions, middleschool girls (Vu et al., 2006) and high school boys(Allison et al., 2005) reported that costs or fees andlimited access or opportunities for PA, as well astelevision watching, served as barriers to their PA.The high school boys also added that their useof the computer and Internet greatly diminishedany time available for PA.
Although a negative relationship betweensedentary behaviors and PA is certainly plausible,results from a quantitative study of high schoolgirls indicated no association between eitherinteractive media use (e.g., Internet surfing andvideo games) or television watching and PA,despite a significant relationship between inter-active media use and both percent body fat andbody mass index (Schneider, Dunton, & Cooper,2007). In addition, a recent report based upon datafrom the 2003 National Survey of Children’sHealth showed that recreational computer usewas related to obesity among 12- to 17-year-oldadolescents (Singh, Kogan, Van Dyck, & Siah-push, 2008). Research with diverse subgroups ofadolescents is recommended to further examineand deconstruct these associations.
Although the literature indicates that perceivedbenefits of Nahas et al. (2003) and barriers to PA(Nahas et al.; Sallis et al., 2000) are related toyouth PA in general, we found that both percep-tions were related to vigorous, but not moderate,PA. Perhaps boys and girls either had difficultyunderstanding the meaning of PA at a moderatelevel of intensity or perceived that moderatePA involves low exertion, and therefore, is notsufficient for achieving the important benefits ofbeing in shape (cited by girls) and improvingathletic skills (cited by boys). Some barriers thatimpede vigorous PA participation may not preventinvolvement at a lower level of intensity.
Consistent with the Health Promotion Model(Pender et al., 2006), prior related behavior had anindirect influence on PA through perceptions ofbarriers. Among those students selecting an activepursuit, boys perceived more barriers to PA thangirls. However, among those not on a sports team,girls reported higher barriers than boys. Ourfindings lend support to this theoretical proposi-
tion and underscore the need to assist girls notinvolved in organized sports to overcome barriersto PA. Prior to making any definitive conclusions,further examination of these relationships withvaried population groups is warranted.
With regard to perceived benefits of PA, theassociation with sports team participation andselection of an active pursuit did not differ bygender. Although gender differences were notexplored by Heitzler et al. (2006), their findingsindicated that, among youth aged 9–13 years,perceived benefits or positive outcome expec-tations were related to participation in bothorganized (e.g., sports lessons or teams) andfree-time PA. Although more research is neededbefore definitive conclusions can be drawn,findings from both studies underscore the impor-tance of continuing to explore the role thatperceived benefits play in interventions directedat increasing PA among boys and girls of middleschool age. The significant indirect relationshipbetween perceived barriers and PA in this studysupports the need to address the barriers to PAas well.
Based on the findings, we have some recom-mendations for future work in this area. A fruitfulapproach may be to use two separate items whenemploying the Perceived Benefits Scale to assesssocial reasons for engaging in PA (one focusing onspending time with family and another similaritem focusing on friends and team members).More in-depth exploration is also needed regard-ing middle school students’ perceptions of beingtoo tired or busy for PA in order to identify reasonsunderlying the salience of this barrier. Whether ornot personal issues take precedence over environ-mental barriers cannot be determined from ourdata, but deserves exploration (Tappe et al., 1989;Zabinski, Saelens, Stein, Hayden-Wade, & Wilf-ley, 2003).
The item related to selection of an active versussedentary pursuit included one active and eightsedentary response choices, thus, the likelihood ofselecting a sedentary response was probably high.Allowing youth to list their top three favoritepursuits as opposed to limiting them to selectingone of the nine response choices may result in amore accurate depiction of their overall interest inbeing either sedentary or active. In addition, werecommend using objective, as well as subjective,measures of PA in future studies. Longitudinalstudy of the perceived benefits of and barriers toPA and their relationship to other PA-relatedvariables can provide valuable insight regardingchange over time or across developmental periodsand potential amenability to behavior change.
Research in Nursing & Health
COMPARISON OF BENEFITS AND BARRIERS / ROBBINS ET AL. 173
NURSING IMPLICATIONS
Nurses in schools and primary care settings caninform middle school students and their parentsabout national recommendations for moderate tovigorous PA and encourage middle school stu-dents to continue sports participation or engage inother PAs. Nurses can share information aboutbenefits of and barriers to PA identified as relevantby this age group and recommend specificindividualized strategies to overcome majorbarriers. Ways to direct counseling to addresspriority issues are important in lieu of thelimited time available for anticipatory guidancein practice settings. As both boys and girlsreported relatively similar benefits of and barriersto PA, conversations with both groups can focuson the same information. For example, the nursecan suggest ways to improve athletic skills anddeal with aches and pains, explore environmentalbarriers and reasons underlying ‘‘being too tired’’for PA, and discuss time management strategies.Information from this study can guide nursesin the provision of developmentally appropriatecounseling to assist boys and girls of middleschool age in achieving national recommenda-tions for moderate to vigorous PA.
REFERENCES
Allison, K.R., Dwyer, J.J.M., Goldenberg, E., Fein,A., Yoshida, K.K., & Boutilier, M. (2005). Maleadolescents’ reasons for participating in physicalactivity, barriers to participation, and suggestions forincreasing participation. Adolescence, 40, 155–170.
Biddle, S., & Armstrong, N. (1992). Children’s physicalactivity: An exploratory study of psychologicalcorrelates. Social Science & Medicine, 34, 325–331.
Burrows, C., Eves, F., & Cooper, D. (1999). Children’sperceptions of exercise—Are children mini-adults?Health Education, 99(2), 61–69.
Centers for Disease Control and Prevention. (2008).Surveillance summaries: Youth risk behaviorsurveillance—United States, 2007. Morbidity andMortality Weekly Report, 57. (No. SS-4. pp. 1–131).Atlanta, GA: Author.
Daniels, S.R., Arnett, D.K., Eckel, R.H., Gidding, S.S.,Hayman, L.L., & Kumanyika, S., et al. (2005).Overweight in children and adolescents: Pathophysi-ology, consequences, prevention, and treatment.Circulation, 111, 1999–2012.
Davison, K.K., Cutting, T.M., & Birch, L.L. (2003).Parents’ activity-related parenting practices predictgirls’ physical activity. Medicine & Science in Sports& Exercise, 35, 1589–1595.
Dowda, M., Dishman, R.K., Pfeiffer, K.A., & Pate, R.R.(2007). Family support for physical activity in girls
from 8th to 12th grade in South Carolina. PreventiveMedicine, 44, 153–159.
Duncan, S.C., Duncan, T.E., & Strycker, L.A. (2005).Sources and types of social support in youth physicalactivity. Health Psychology, 24(1), 3–10.
Dugan, S.A. (2008). Exercise for preventing childhoodobesity. Physical Medicine and Rehabilitation Clin-ics of North America, 19, 205–216.
Dwyer, J.J.M., Allison, K.R., Goldenberg, E.R., Fein,A.J., Yoshida, K.K., & Boutilier, M.A. (2006).Adolescent girls’ perceived barriers to participationin physical activity. Adolescence, 41(161), 75–89.
Garcia, A.W., George, T.R., Coviak, C., Antonakos, C.,& Pender, N.J. (1997). Development of the child/adolescent activity log: A comprehensive andfeasible measure of leisure-time physical activity.International Journal of Behavioral Medicine, 4,323–338.
Garcia, A.W., Norton Broda, M.A., Frenn, M., Coviak,C., Pender, N.J., & Ronis, D.L. (1995). Gender anddevelopmental differences in exercise beliefs amongyouth and prediction of their exercise behavior.Journal of School Health, 65, 213–219.
Garcia, A.W., Pender, N.J., Antonakos, C.L., & Ronis,D.L. (1998). Changes in physical activity beliefs andbehaviors of boys and girls across the transition tojunior high school. Journal of Adolescent Health, 22,394–402.
Grieser, M., Vu, M.B., Bedimo-Rung, A.L., Neumark-Sztainer, D., Moody, J., & Young, D.R., et al.(2006). Physical activity, attitudes, preferences, andpractices in African American, Hispanic, andCaucasian girls. Health Education & Behavior,33(1), 40–51.
Hagler, A.S., Calfas, K.J., Norman, G.J., Sallis, J.F., &Patrick, K. (2006). Construct validity of physicalactivity and sedentary behaviors staging measuresfor adolescents. Annals of Behavioral Medicine, 31,186–193.
Heitzler, C.D., Martin, S.L., Duke, J., & Huhman, M.(2006). Correlates of physical activity in a nationalsample of children aged 9–13 years. PreventiveMedicine, 42, 254–260.
Kahn, J.A., Huang, B., Gillman, M.W., Field, A.E.,Austin, S.B., Colditz, G.A., et al. (2008). Patterns anddeterminants of physical activity in U.S. adolescents.Journal of Adolescent Health, 42, 369–377.
Kientzler, A.L. (1999). Fifth- and seventh-grade girls’decisions about participation in physical activity. TheElementary School Journal, 99(5), 391–414.
Kimm, S.Y.S., Glynn, N.W., Kriska, A.M., Fitzgerald,S.L., Aaron, D.J., Similo, S.L., et al. (2000).Longitudinal changes in physical activity in a biracialcohort during adolescence. Medicine & Science inSports & Exercise, 32, 1445–1454.
Kimm, S.Y.S., Glynn, N.W., McMahon, R.P., Voorhees,C.C., Striegel-Moore, R.H., & Daniels, S.R. (2006).Self-perceived barriers to activity participationamong sedentary adolescent girls. Medicine &Science in Sports & Exercise, 38, 534–540.
Research in Nursing & Health
174 RESEARCH IN NURSING & HEALTH
Koezuka, N., Koo, M., Allison, K.R., Adlaf, E.M.,Dwyer, J.J.M., Faulkner, G., et al. (2006). Therelationship between sedentary activities and phys-ical inactivity among adolescents: Results from theCanadian Community Health Survey. Journal ofAdolescent Health, 39, 515–522.
Kubik, M.Y., Lytle, L., & Fulkerson, J.A. (2005). Fruits,vegetables, and football: Findings from focus groupswith alternative high school students regarding eatingand physical activity. Journal of Adolescent Health,36, 494–500.
Leslie, J., Yancey, A., McCarthy, W., Albert, S.,Wert, C., Miles, O., et al. (1999). Development andimplementation of a school-based nutrition andfitness promotion program for ethnically diversemiddle-school girls. Journal of the American DieteticAssociation, 99, 967–970.
MuniNetGuide. (2008). Retrieved June 8, 2008, fromhttp://www.muninetguide.com/states/.
Nader, P.R., Bradley, R.H., Houts, R.M., McRitchie,S.L., & O’Brien, M. (2008). Moderate-to-vigorousphysical activity from ages 9 to 15 years. JAMA, 300,295–305.
Nahas, M.V., Goldfine, B., & Collins, M.A. (2003).Determinants of physical activity in adolescents andyoung adults: The basis for high school and collegephysical education to promote active lifestyles. ThePhysical Educator, 60, 42–56.
National Center for Education Statistics. (2005-2006). Public school data 2005-2006 school year.Retrieved November 14, 2008, from http://nces.ed.gov/globallocator.
O’Dea, J.A. (2003). Why do kids eat healthful food?Perceived benefits of and barriers to healthfuleating and physical activity among children andadolescents. Journal of the American DieteticAssociation, 103, 497–501.
Pate, R.R., Freedson, P.S., Sallis, J.F., Taylor, W.C.,Sirard, J., Trost, S.G., et al. (2002). Compliance withphysical activity guidelines: Prevalence in a popula-tion of children and youth. Annals of Epidemiology,12, 303–308.
Pender, N.J., Murdaugh, C.L., & Parsons, M.A. (2006).Health promotion in nursing practice. Upper SaddleRiver, NJ: Pearson Prentice Hall.
Radzik, M., Sherer, S., & Neinstein, L.S. (2002).Psychosocial development in normal adolescents.In: L. Neinstein (Ed.), Adolescent health care: Apractical guide. (4th ed., pp. 52–58). Philadelphia:Lippincott Williams & Wilkins.
Robbins, L.B., Pender, N.J., & Kazanis, A.S. (2003).Barriers to physical activity perceived by adolescentgirls. Journal of Midwifery & Women’s Health, 48,206–212.
Robbins, L.B., Pis, M.B., Pender, N.J., & Kazanis, A.S.(2004). Physical activity self-definition among ado-lescents. Research and Theory for Nursing Practice,18, 317–330.
Robbins, L.B., Wu, T.Y., Sikorskii, A., & Morley, B.(2008). Psychometric assessment of the AdolescentPhysical Activity Perceived Benefits and Barriers
Scales. Journal of Nursing Measurement, 16(2), 98–112.
Sallis, J.F., & Owen, N. (1999). Physical activity& behavioral medicine. Thousand Oaks, CA:Sage.
Sallis, J.F., Prochaska, J.J., & Taylor, W.C. (2000). A.review of correlates of physical activity of childrenand adolescents. Medicine & Science in Sports &Exercise, 32, 963–975.
SAS Institute. (2002-2003). SAS software, version 9 ofthe SAS System for Windows. Cary, NC: Author.
Schneider, M., Dunton, G.F., & Cooper, D.M. (2007).Media use and obesity in adolescent females. Obesity,15, 2328–2335.
Searle, S.R., Speed, F.M., & Miliken, G.A. (1980).Population marginal means in the linear model: Analternative to least squares means. The AmericanStatistician, 34, 216–221.
Singh, G.K., Kogan, M.D., Van Dyck, P.C., & Siahpush,M. (2008). Racial/ethnic, socioeconomic, and behav-ioral determinants of childhood and adolescentobesity in the United States: Analyzing independentand joint associations. Annals of Epidemiology, 18,682–695.
SPSS. (2006). SPSS 15.0 for Windows. Chicago, IL:Author.
Tappe, M.K., Duda, J.L., & Ehrnwald, P.M. (1989).Perceived barriers to exercise among adolescents.Journal of School Health, 59, 153–155.
Taylor, W.C., Yancey, A.K., Leslie, J., Murray, N.G.,Cummings, S.S., & Sharkey, S.A., et al. (1999).Physical activity among African American andLatino middle school girls: Consistent beliefs,expectations, and experiences across two sites.Women & Health, 30(2), 67–82.
Tergerson, J.L., & King, K.A. (2002). Do perceivedcues, benefits, and barriers to physical activity differbetween male and female adolescents? Journal ofSchool Health, 72, 374–380.
Troiano, R.P., Berrigan, D., Dodd, K.W., Masse, L.C.,Tilert, T., & McDowell, M. (2008). Physical activityin the United States measured by accelerometer.Medicine & Science in Sports & Exercise, 40, 181–188.
U.S. Department of Health and Human Services.(2008). Physical activity guidelines for Americans.Washington, DC: Author.
Vu, M.B., Murrie, D., Gonzalez, V., & Jobe, J.B. (2006).Listening to girls and boys talk about girls’ physicalactivity behaviors. Health Education & Behavior, 33,81–96.
Welk, G.J., Corbin, C.B., & Dale, D. (2000). Measure-ment issues in the assessment of physical activity inchildren. Research Quarterly for Exercise and Sport,71, S59–S73.
Wu, T.Y., Pender, N., & Noureddine, S. (2003). Genderdifferences in the psychosocial and cognitive corre-lates of physical activity among Taiwanese adoles-cents: A structural equation modeling approach.International Journal of Behavioral Medicine, 10,93–105.
Research in Nursing & Health
COMPARISON OF BENEFITS AND BARRIERS / ROBBINS ET AL. 175

Yin, Z., Hanes, J., Moore, J.B., Humbles, P., Barbeau,P., & Gutin, B. (2005). An after-school physicalactivity program for obesity prevention in children:The Medical College of Georgia FitKid Project.Evaluation & The Health Professions, 28(1),67–89.
Yin, Z., Moore, J.B., Johnson, M.H., Barbeau, P.,Cavnar, M., Thornburg, J., et al. (2005). The MedicalCollege of Georgia FitKid project: The relationsbetween program attendance and changes in out-
comes in year 1. International Journal of Obesity, 29,S40–S45.
Zabinski, M.F., Saelens, B.E., Stein, R.I., Hayden-Wade, H.A., & Wilfley, D.E. (2003). Overweightchildren’s barriers to and support for physical activity.Obesity Research, 11, 238–246.
Zakarian, J.M., Hovell, M.F., Hofstetter, C.R., Sallis,J.F., & Keating, K.J. (1994). Correlates of vigorousexercise in a predominately low SES and minority highschool population. Preventive Medicine, 23, 314–321.
Research in Nursing & Health
176 RESEARCH IN NURSING & HEALTH





























