Embed Size (px)
Citation preview

Cancer Therapy: Clinical
Gene Copy Number Estimation from TargetedNext-Generation Sequencing of Prostate CancerBiopsies: Analytic Validation and ClinicalQualificationGeorge Seed1,Wei Yuan1, Joaquin Mateo1, Suzanne Carreira1, Claudia Bertan1,Maryou Lambros1, Gunther Boysen1, Roberta Ferraldeschi1,2, Susana Miranda1,Ines Figueiredo1, Ruth Riisnaes1, Mateus Crespo1, Daniel Nava Rodrigues1,Eric Talevich3, Dan R. Robinson4, Lakshmi P. Kunju4, Yi-Mi Wu4, Robert Lonigro4,Shahneen Sandhu1, Arul M. Chinnaiyan4, and Johann S. de Bono1,2
Abstract
Purpose: Precise detection of copy number aberrations (CNA)from tumor biopsies is critically important to the treatment ofmetastatic prostate cancer. The use of targeted panel next-gener-ation sequencing (NGS) is inexpensive, high throughput, andeasily feasible, allowing single-nucleotide variant calls, but CNAestimation from this remains challenging.
Experimental Design: We evaluated CNVkit for CNA identi-fication from amplicon-based targeted NGS in a cohort of 110fresh castration-resistant prostate cancer biopsies and used cap-ture-based whole-exome sequencing (WES), array comparativegenomic hybridization (aCGH), and FISH to explore the viabilityof this approach.
Results: We showed that this method produced highly repro-ducible CNA results (r ¼ 0.92), with the use of pooled germlineDNA as a coverage reference supporting precise CNA estimation.
CNA estimates from targeted NGS were comparable with WES(r ¼ 0.86) and aCGH (r ¼ 0.7); for key selected genes (BRCA2,MYC, PIK3CA, PTEN, and RB1), CNA estimation correlatedwell with WES (r ¼ 0.91) and aCGH (r ¼ 0.84) results. Thefrequency of CNAs in our population was comparable with thatpreviously described (i.e., deep deletions: BRCA2 4.5%; RB18.2%; PTEN 15.5%; amplification: AR 45.5%; gain: MYC31.8%). We also showed, utilizing FISH, that CNA estimationcan be impacted by intratumor heterogeneity and demonstrat-ed that tumor microdissection allows NGS to provide moreprecise CNA estimates.
Conclusions: Targeted NGS and CNVkit-based analyses pro-vide a robust, precise, high-throughput, and cost-effectivemethodfor CNA estimation for the delivery of more precise patient care.Clin Cancer Res; 23(20); 6070–7. �2017 AACR.
IntroductionProstate cancer is a highly heterogeneous disease with distinct
genomic underpinnings (1) and generally presents a modestnumber of single point mutations and small insertions anddeletions (indels) at approximately four per megabase (2, 3), butfrequently has large-scale copy number and structural alterations(4, 5). We recently showed that 20% to 30% of prostate tumorsbear defects in DNA repair genes that render them sensitive to
treatment with PARP inhibition, and that these are commonlymediated through deletions in these tumor suppressors (6).
High-throughput, inexpensive, multiplex biomarker assays formolecular stratification are needed to guide therapeutic choicesand support clinical trial design. Although high-coverage whole-exome or genome sequencing can reliably assess tumor genomics,cost and bioinformatic demands currently restrict their routineclinical implementation to stratify patients for treatment. Tar-geted next-generation sequencing (NGS) represents an opportu-nity for implementing genomics in clinical practice with theadvantages of a rapid turnaround time, lower cost, and the abilityto concurrently analyze multiple genes with a limited bioinfor-matic analysis burden. Existing approaches to call germline andsomatic single-nucleotide variants (SNV) and short indels fromtargeted sequencing data are well established and have led to anumber of FDA biomarker-dependent drug approvals, includingthe PARP inhibitor olaparib in the past decade (7, 8). However, inthe case of PARP inhibition for homologous recombination repairdefective cancers, screening for tumors with these DNA repairdefects relies on detecting gene copy number changes.
In this study, we identify gene copy number aberrations (CNA),based on targeted amplicon sequencing of a focused biomarkergene panel dedicated to identifyingDNA repair defects.We used a
1The Institute of Cancer Research, London, United Kingdom. 2The Royal MarsdenNHS Foundation Trust, London, United Kingdom. 3University of California SanFrancisco, San Francisco, California. 4Michigan Centre for Translational Pathol-ogy, Ann Arbor, Michigan.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corrected online February 13, 2018.
G. Seed and W. Yuan contributed equally to this article.
Corresponding Author: Johann S. de Bono, The Institute of Cancer Research,London SM2 5NG, United Kingdom. Phone: 4420-8722-4028; Fax: 4420-8642-7979; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-17-0972
�2017 American Association for Cancer Research.
ClinicalCancerResearch
Clin Cancer Res; 23(20) October 15, 20176070
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

patient cohort of metastatic castration-resistant prostate cancer(CRPC) to explore the utility of this approach. This targetedgene panel focused on the study of 113 genes important toDNA repair machinery, including BRCA2, BRCA1, ATM, PALB2,and CDK12 as well as other important potentially actionableprostate cancer genes, including AR, SPOP, PIK3CA, PTEN,AKT1, AKT2, and MYC (1, 6).
Materials and MethodsPatient selection and sample preparation
Patient tumor (biopsies) and germline (buccal swab andsaliva) samples were collected as part of the Royal Marsdenethics committee–approved CCR2472 protocol. Samples werecollected, annotated, stored, and reviewed as described previ-ously (6). All samples were collected between July 25, 2015,and October 17, 2016.
Briefly, biopsies were paraffin embedded, DNA from biopsieswas extracted using the QIAamp DNA FFPE Tissue Kit (Qiagen),Quant-iT Picogreen High-Sensitivity double-stranded DNA(dsDNA) Assay Kits (Invitrogen, Thermo Fisher Scientific) andQC check by FFPE QC Kit (Illumina).
Targeted panel designA customized Generead v2 DNAseq Panel (Qiagen) panel was
used for library construction; the exonic regions of 113 geneswereincluded in the targeted panel, these being selected for beingpotentially actionable and/or involved in DNA damage repairprocesses and/or in prostate carcinogenesis (Supplementary TableS1; ref. 6). The panel covered 564 kb of the human genome, andeach of the 113 genes was covered by an average of 18.69 probes(SD, 13.64).
Targeted and exome sequencingTargeted amplicon sequencing was performed using the Illu-
mina MiSeq platform following the manufacturers' protocol.FASTQ files were generated using the Illumina MiSeq Reporterv2.5.1.3 (9, 10). Reads were aligned to the human referencegenome (hg19) using BWA.Whole-exome sequencing (WES)wasperformed at the University of Michigan (Ann Arbor, MI) asdescribed previously (1).
FastQC (v0.11.2) and Samtools (0.1.19) were used to assesssequencing quality. Targeted sequencing samples were excludedfrom copy number analysis on the basis of: insufficient (<0.5million) total read counts, low (<95%) percentage of properlypaired reads, and low (<99.99%) percentage of on-target reads.Exome sequencing samples were rejected if the FastQC per-basequality score for 75% of the reads was less than Q20 over the first80 bases, and alignment quality was monitored with Picard, asdescribed previously (1).
CNAsWe used the software CNVkit (v0.3.5; ref. 11) to analyze
sequencing coverage and copy number in the aligned sequencingreads from targeted amplicon sequencing of tumor and germlinesamples. Sequencing coverage of targeted regions in germlinesampleswas assessed andused to create pooled reference data thatincluded the technical variability at each covered region. Regionsthat were poorly amplified or mapped were masked from furtheranalysis. The analyses of germline samples were also performedwith CNVkit to validate sample quality. The read depths of tumorsamples were accessed, normalized (corrected for GC content,target footprint size and spacing, and repetitive sequences), andindividually compared with the reference, and the circular binarysegmentation (CBS) algorithm (12) was used to infer copynumber segments. Very small copy changes (�3bins)were treatedas artifacts. Poor samples were also identified through high (>0.8)values of the segment interquartile range (IQR), a metric for thespread of bin-level copy ratios within each segment followingapplication of the CBS algorithm. Copy number segments wereannotated to genes, and regions bearing a log2 ratio of at least�0.4 were identified as suggestive of shallow deletions or gains(11). Segments with log2 <�1.2 were classified as deep dele-tions, and those with log2 >2 were classified as amplifications.Experimental noise was identified as a log2 ratio SD of approx-imately 0.2.
WESCNAdatawere extracted fromapreviously reported Su2C-PCF dataset (1). Briefly, log2 ratios were derived on a per-genebasis from circular-binary segmented, Lowess-normalized log2transformed coverage ratio between each tumor and matchednormal sample.
Array comparative genomic hybridizationTumor DNA from prostate cancer patients and male refer-
ence DNA from Agilent were amplified using Sigma WGA2 Kit(Sigma-Aldrich) according to the manufacturer's recommenda-tions, and the amplified DNA was quantified by the Qubitfluorometric quantitation method (Thermo Fisher Scientific).Amplified tumor DNA (500 ng) was then fluorescently labeledwith Cy5, and male reference DNA labeled with Cy3, usingthe SureTag Complete DNA Labeling Kit (Agilent Technolo-gies). Labeled DNA was subsequently hybridized utilizing theAgilent SurePrint G3 Human CGH Microarray Kit, 4 � 180 Kaccording to the manufacturer's instructions. The slides werethen scanned and analyzed using the CytoGenomics Software v4.0.3.12 (Agilent Technologies). To compare array comparativegenomic hybridization (aCGH) and NGS results, we used thelog2 ratio of the aCGH segments that overlap with genespresent in the NGS panel. Genes not part of a copy-alteredsegment were included in the analysis by using the mean log2ratio for probes, if the value was no greater than 0.25. Genes onthe X-chromosome were excluded from comparison with
Translational Relevance
Detection of oncogenic genomic aberrations has led tonovel therapeutic strategies for treating cancer. We recentlyshowed that 20% to 30% of metastatic prostate cancers havedeleterious defects in DNA repair machinery affecting genes,such as BRCA2, ATM, PALB2, BRCA1, and CDK12. Theseaberrations are associated with sensitivity to PARP inhibitors.Robust methods are needed to identify these tumor subtypes.We have previously described a targeted next-generationsequencing method that identifies single-nucleotide variantsand copy number aberrations, with precision, from formalin-fixed, paraffin-embedded tumor biopsy samples. We nowdescribe the bioinformatics pipeline for this robust high-throughput, cost-efficient, and rapid solution. We have imple-mented these methods into clinical trial protocols to enablepatient stratification.
Targeted-seq and Copy Number Analysis of CRPC Biopsies
www.aacrjournals.org Clin Cancer Res; 23(20) October 15, 2017 6071
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

results from the male reference–based panel data as a femalereference was used for aCGH.
FISHRB1 FISH was performed using a standard formalin-fixed,
paraffin-embedded (FFPE) hybridization method (13) on 3-mmFFPE tissue slices adjacent to hematoxylin and eosin sections thatwere confirmed to contain a minimum of 50 intact cells. Briefly,RB1 status was determined using Vysis LSI 13 RB1 (13q14) probe(catalog # 08L65-020; Abbott Laboratories) and a reference probeVysis 13q34 (catalog # 05N34-020; Abbott Laboratories). Nine-teen z-stacks were used to assess cell status.
ResultsMetastatic prostate cancer sample characteristics
Freshly collectedmetastatic CRPC (mCRPC)biopsies (n¼110)were collected from patients with progressing disease (Supple-mentary Table S2) and assessed for copy number changes bysequencing with our targeted panel. Germline DNA samples(buccal swab) were taken from 34 consenting patients to use asa baseline reference and for additional analyses. Tumor biopsieswere from: bone (49.1%), lymph nodes (35.5%), liver (9.1%),soft tissue disease (3.6%), and transurethral resection of theprostate (3.6%).
2 1 0 1 2
21
01
2
Exome log2 ratios
Pan
el lo
g 2 ra
tio
r : 0.91
2 1 0 1 2
21
01
2
Replicate 1 log2 ratios
Rep
licat
e 2
log 2
ratio
s
r : 0.92
2 1 0 1 2
21
01
2
Matched reference log2 ratios
Poo
led
refe
renc
e lo
g 2 ra
tios r : 0.93
2 1 0 1 2
21
01
2
Exome log2 ratios
Pan
el lo
g 2 ra
tios
r : 0.87
2 1 0 1 2
21
01
2
Array log2 ratios
Pan
el lo
g 2 ra
tios
r : 0.7
2 1 0 1 2
21
01
2
Array log2 ratios
Pan
el lo
g 2 ra
tio
r : 0.84
BRCA2MYCPIK3CAPTENRB1
A
C
E F
D
B
Figure 1.
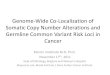
Copy number estimation results bytargeted NGS and the describedbioinformatic method were highlyreproducible. Correlations of log2 results(overplotted) shown from: replicatesamples (A; n ¼ 13); matched germlinereference (B; 25 pairs available) againstpooled germline reference. Pearsonr values presented. Comparing tools forgenerating informative log2 ratios showedthat targeted panel NGS of CRPCsproduced valid results for identification ofCNAs when compared with orthogonalmethods. Shown are correlations of log2results (overplotted) from: panel datawithexome data (C; n ¼ 13); and panel datawith aCGH results (D; n ¼ 9). Pearson rvalues depicted. CNA orthogonalvalidation focusing on selected genes oftherapeutic relevance to CRPC presentedas log2 ratios in comparison with exome(E) and aCGH (F) data from the samesamples compared with panel data. Colorsindicate gene: BRCA2 ¼ red, MYC ¼orange, PIK3CA ¼ dark blue, PTEN ¼ lightblue, and RB1 ¼ yellow. Pearson r valuesare shown.
Seed et al.
Clin Cancer Res; 23(20) October 15, 2017 Clinical Cancer Research6072
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

CNA estimation reproducibilityAccurately assessing the depth of coverage of genes can be
biased by high GC content and repetitive regions (11, 14), so wefirst evaluated CNA reproducibility on a per-gene basis betweentechnical replicates. Thirteen sampleswere sequenced induplicateto assess technical variation; 12 of these duplicate datasets includ-ed repeated library preparation from the same DNA extraction,while one involved resequencing of the same library twice.
We identified 15 genes that produced less concordant resultsbetween replicates, including five genes with insufficient numberof targeted regions (four or less probes) per gene (NRAS, NFKBIA,FANCF, FAM46C, CDKN1B), and 10 (MAP2K2, CDKN2A, HRAS,RECQL4, NOTCH1, FGFR3, STK11, TSC2, SMARCA4, AXIN1)that contained repetitive or polymorphic exonic regions thatimpeded accurate read alignment and possessed high coveragevariability (Supplementary Fig. S1). These genes were excludedfrom downstream CNA analyses.
Following removal of the aforementioned genes, CNA esti-mates between duplicates showed high correlation (Pearsonr correlation coefficient ¼ 0.92; Fig. 1A). All genes with deepdeletions (log2 ratio, <�1.2) or amplifications (log2 ratio > 2) hada similar (at least �0.4) CNA estimation replicated in the dupli-cate sample. A total of 95% of samples with a log2 ratio change ofat least �0.4 had a similar result in the duplicate.
A matched germline sample is commonly used for identifyingdeviations in coverage ratios, so we sought to compare this withour pooled reference approach. For the pooled reference, wesequenced 34 unmatched germline samples and assessed thedepth of coverage as described previously (11). Regions with lowvariability were identified in the pooled reference and used toweight downstreamCNA estimates (11). This approach produceda highly similar result (overall Pearson r¼ 0.93) when comparedwith the CNA estimation approach using a matched normal asreference,whenmatchednormal sampleswere available (Fig. 1B);however, the CNA estimation confidence score (IQR value) wasimproved when using pooled germline samples (paired t testP ¼ 0.05). This was in line with other reports (14) that indicatedthat using pooled germline sequencing data as reference offered arobust method to identify gene CNAs.
CNA validation by exome sequencing and aCGHWe cross-compared copy number log2 ratios for all evaluable
genes on the targeted panel with log2 ratios generated by exomesequencing (n ¼ 13; Fig. 1C), resulting in a Pearson r correlationcoefficient of 0.86. Moreover, all the genes with a log2 ratio <�1.2by targeted sequencing, in keepingwith putative "deep" deletions,exhibited a similar (at least�0.4) result in the exome sequencing.For example, one sample bore AR amplification (log2 ratio 5.7 intargeted NGS and 4.91 in WES) alongside WRN deletion (�1.53vs. �1.17) and ATM deletion (�0.68 vs. �0.56). We also com-pared log2 ratios from aCGH segments (n ¼ 9) with gene copynumber estimations by panel NGS among the genes covered byboth platforms and found log2 ratios were also concordant (Fig.1D), with a Pearson r value of 0.7.
We then sought to further validate copynumber calls for specificgenes of clinical relevance, such as BRCA2, MYC, PIK3CA, PTEN,and RB1 (Fig. 1E and F). For these genes, we found that our panelproduced results highly concordant with exome sequencing andaCGH data, with Pearson r values of 0.91 and 0.84, respectively.All clinically relevant deletions of BRCA2 in samples with exomeor aCGH data were also identified in our panel results (Table 1).
CNA profiles in CRPCIn the analyses of this cohort of advanced prostate cancer
samples, the prevalence of the CNAs detected with this assaywas consistent with that of previously reported studies(Fig. 2). CNAs of AR (amplification; log2 > 2) were found in45.5% (50/110) of tumor samples. Broad deletions of chro-mosome 13 (1) involving the shared loss of BRCA2 and RB1were detected as previously described with 23 of 26 (88%)samples with any BRCA2 loss also having some loss of RB1,while overall 23 of 66 (34.8%) samples with RB1 loss had lossof BRCA2 (Fig. 2A).
Overall, the evaluation of the deep deletions of commonlyaberrant CRPC genes revealed results in keeping with previousreports from two recent studies of CRPC genomics (1, 15); PTENgenomic deep deletions were detected in 17 of 110 (15.5%),BRCA2deepdeletion in 5of110 (4.5%), andRB1deepdeletion in9of 110 (8.2%)CRPC samples. In addition, gain of theMYC locuswas found in 36 of 110 samples (32.7%). We found that the copynumber alteration frequencies in our cohort were in line withexpected CRPC frequencies.
Exploring tumor purity and heterogeneityTo further explore how tumor purity altered the capacity of the
assay todetectCNAs,wepursued the serial dilutionof tumorDNAacquired from a sample estimated by pathology review as having80% tumor content, with same-patient germline DNA. Thissample harbored a somatic, BRCA2 homozygous deletion
Table 1. Validation of BRCA2 results from targeted panel CNV analysis witheither whole-exome sequencing or array comparative genome hybridization(log2 ratios are shown)
NOTE: Colors indicate direction of shift away from 0, with losses represented byblue and gains represented by red.
Targeted-seq and Copy Number Analysis of CRPC Biopsies
www.aacrjournals.org Clin Cancer Res; 23(20) October 15, 2017 6073
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

(independently confirmed WES). We then sequenced the result-ingdilutions (Fig. 3A) and found that homozygous deletionswereeasily distinguishable with tumor content purities >60% and thatclonal CNAs were detectable with purity as low as 30%.
We also performedmicrodissection of a tumor biopsy (pathol-ogist tumor purity estimate, �40%) bearing borderline BRCA2homozygous deletion (log2 ratio of �1.15) and resequenced the
resulting tumor-enriched sample (purity estimate, �80%). Thisstep further shifted theCNAestimates away fromnormal,with thelog2 ratio for BRCA2 dropping to �2.82, an unambiguous dele-tion (Fig. 3B).
The log2 copy ratios estimated from sequencing a bulkof cells, as in our protocol, can be biased by tumor sampleheterogeneity. To assess this relationship, we performed FISH
Figure 2.
A, Binned heatmap of copy number aberrations for all evaluated (n ¼ 110) samples with colors defined by log2 ratio thresholds (dark blue, <�1.2; light blue,<�0.4; pink,>0.4; red,>2). Rows and columns clustered by complete Euclidean distance for visualization purposes only. Commonly deletedgenes, such asPTEN, RB1,and BRCA2, cluster toward the left, while commonly amplified genes, such as AR, MYC, BRAF, and KRAS, trend to the right. Genes that are closely located inchromosomal coordinates (e.g., CHEK2 and NF2, BLM and MAP2K1, RB1 and BRCA2) often share similar copy number aberrations. B, Scatter plot showingthat the percentage of samples with specific copy-number changes in our targeted sequencing cohort was similar to two recently published studies of CNAs inCRPC (1, 15). Colors indicate type of aberration (red ¼ amplification, pink ¼ gain, blue ¼ deletion). Shape of points indicate study data source. Data were derivedfrom copy number frequency data publicly available from cBioPortal (21, 22), retrieved on November 17, 2016.
Seed et al.
Clin Cancer Res; 23(20) October 15, 2017 Clinical Cancer Research6074
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

assays of the RB1 gene, counting the number of cells where eachcopy number (0 through 3þ) was observed (Fig. 3C). Ourresults showed an association between the proportion of cellswith 1 or 0 copies of RB1 (hemizygous or homozygous dele-tion) and putative copy loss inferred from our targetedsequencing panel (unpaired t test P ¼ 0.02, n ¼ 18, df ¼15.884). However, the full complexity of aneuploidy in indi-vidual tumor cells is masked by bulk tissue sequencing, whicheffectively averages the estimated DNA content across all cellsin a sample. FISH analyses revealed that many tumor samplescontained a mixture of cells with different copy numberchanges at the RB1 locus, in highly heterogeneous cell popula-tions (Supplementary Fig. S2).
DiscussionThe ability to rapidly, inexpensively, and accurately identify
cancers with actionable genomic defects in tumor biopsies is nowbecoming critically important for advanced prostate cancer care.
We have previously shown that a proportion of metastatic CRPCshave DNA repair defects and are sensitive to treatment with PARPinhibitors (6), with emerging studies of platinum-based che-motherapies also indicating important antitumor activity inthis population (16). These and other data support furtherstudies of genomic stratification for treatment selection ofpatients suffering from mCRPC. Here, we demonstrate the ana-lytic validation and clinical use of a targetedNGS assay that allowsfor copy number screening for predictive biomarkers of response,enabling the integration ofmore precise patient stratification intotrial design.
Ourmethod reliably estimates gene copynumber changes fromamplicon-based targeted NGS with the acquired results beingcomparable with widely used assays, including exome sequenc-ing, aCGH, digital droplet PCR, and FISH (17). Critically, the dataprocessing time for this panel-based CNA estimation is substan-tially shorter of that for exome sequencing and can be easilycompleted even with a personal computer. In addition, we haveconfirmed that using pooled germline samples as a reference can
Figure 3.
A, Serial dilution of a tumor sample with matched germline DNA and resequencing highlights functional limits of copy number detection. Homozygously deleted(BRCA2, PTEN – dark blue), hemizygously deleted (RB1 – light blue), copy-neutral (SPOP – gray), and copy-gained (PIK3CA – pink) genes are shown. B,Microdissection of a biopsy to enrich tumor content emphasizes a BRCA2 deletion, as the segment log2 ratio (orange line) shifts from �1.15 to �2.82. Alsoshown are individual exon-level copy ratios (blue points), from which the segment is assigned. C, Stacked bar plot showing RB1-FISH results for 18 samples(50 cells each), with colors indicating observable copies of RB1 for individual cells. Navy, 0 copies; light blue, 1 copy; white, 2 copies; pink, >2 copies. Black bar,samples that had a deletion of any kind reported by our targeted NGS protocol.
www.aacrjournals.org Clin Cancer Res; 23(20) October 15, 2017 6075
Targeted-seq and Copy Number Analysis of CRPC Biopsies
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

produce equivalent and robust results to utilizing matched nor-mal samples. This feature provides the possibility of diagnosingpatients with only tumor samples for whom germline DNA is notavailable, and can dramatically reduce the overall sequencingcosts of large studies.
This approach is currently being applied in the TOPARP-B(NCT01682772) study as part of an ongoing attempt to clinicallyqualify DNA repair pathway aberrations as a predictive biomarkerfor treatment with PARP inhibition with olaparib (16). However,this assay has utility beyond this study. The gene panel we utilizedcovers several key genomic aberrations that are of emerginginterest as possible clinical predictive biomarkers that may beactionable in prostate cancer, including loss of PTEN, gain ofPIK3CA (both may sensitize tumors to PI3K/AKT pathway inhi-bition; refs. 18, 19), and amplification of MYC (MYC-driventumors have been reported to sensitize to AURA and BET inhi-bition and can result in replication stress; ref. 20). Prospectivelyidentifying tumors bearing these CNAs and other deleteriousmutations, utilizing such validated methods, is likely to becomecritically important in defining future treatment strategies for thiscommonest of male cancers.
We explored the functional limits of assessing CNAs and foundthat our pipeline can confidently estimate deletion when tumorcontent is reduced to 60% (homozygous and heterozygous). Astumor content decreases, the pipeline struggles to differentiatebetween homozygous and heterozygous deletions, and we esti-mate that interpreting results from sampleswith<30%puritymaybe extremely challenging for targeted NGS panels. We haveshown, however, that the use of microdissection to enrich tumorcontent offers a possible solution to resolve these issues.
This approach also suffers from the nature of amplicon-basedNGS, including difficulty identifying precise breakpoints, veryfocal gains or deletions, unequal amplification among genes,and coverage variation across polymorphic repeat regions. Fur-thermore, because the number of SNVs identified in targetedpanels will be much lower when compared with exome orwhole-genome sequencing, SNV allele frequencies may not besufficient to assist with copy number estimation or to detect allelicimbalance.
It is important to note that we did not systematically comparesoftware tools in this study and that different clinical require-mentswill require individual optimizations. As thefield develops,other software tools will emerge to improve the precision of CNAidentification in targeted sequencing, and independent valida-tions will be critical in guiding further work.
In conclusion, we have described the validation and clinicalapplication of an assay evaluating 100 genes utilized to assessboth deleterious tumor gene copy number, and mutations, fromtargeted NGS of prostate cancer samples from the most common
metastatic sites, including bone biopsies. We have validated theseresults by orthogonal methods, including not only exomesequencing, but also aCGH and FISH. Such targeted panel NGSassays are likely to become central to future patient care in cancertherapy.
Disclosure of Potential Conflicts of InterestS. Sandhu is a consultant/advisory board member for Amgen, Bristol-Myers
Squibb, and Janssen. J.S. de Bono is a consultant/advisory board member forAstraZeneca. No potential conflicts of interest were disclosed by the otherauthors.
Authors' ContributionsConception and design: G. Seed, W. Yuan, J. Mateo, S. Carreira, G. Boysen,S. Miranda, S. Sandhu, A.M. Chinnaiyan, J.S. de BonoDevelopment of methodology: G. Seed, S. Carreira, S. Miranda, E. Talevich,S. Sandhu, A.M. Chinnaiyan, J.S. de BonoAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.):G. Seed, J.Mateo, S.Carreira, C. Bertan, R. Ferraldeschi,M. Crespo, D.N. Rodrigues, D.R. Robinson, Y.-M. Wu, S. Sandhu, J.S. de BonoAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): G. Seed, W. Yuan, J. Mateo, S. Carreira, M. Lambros,D.N. Rodrigues, E. Talevich, D.R. Robinson, L.P. Kunju, Y.-M. Wu, R. Lonigro,J.S. de BonoWriting, review, and/or revision of themanuscript:G. Seed,W. Yuan, J.Mateo,S. Carreira, M. Lambros, G. Boysen, S. Miranda, I. Figueiredo, R. Riisnaes,D.N. Rodrigues, E. Talevich, R. Lonigro, S. Sandhu, A.M. Chinnaiyan, J.S. de BonoAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): G. Seed, I. Figueiredo, D.N. Rodrigues, J.S. deBonoStudy supervision: W. Yuan, J.S. de Bono
AcknowledgmentsWe thank the staff at the Prostate Targeted TherapyGroup and all the patients
who agreed to participate in this study.
Grant SupportThis study was supported by Cancer Research UK, Prostate Cancer UK, and
the Stand Up To Cancer – Prostate Cancer Foundation Prostate Dream TeamTranslational Research Grant (grant number: SU2C-AACR-DT0712). Researchgrant administered by the American Association for Cancer Research, theScientific Partner of SU2C. Support was also provided by an ExperimentalCancer Medicine Centre grant and a Medical Research Council/Prostate CancerUK and PCF Young Investigator Award to J. Mateo. G. Seed was supported by aProstate Cancer UK PhD studentship (TLD-S15-006), and G. Boysen wassupported by a Marie Curie International Incoming Fellowship (625792). Thisstudy was also supported by research funding from the EU FP7 project CTCTrap#305341.
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received April 4, 2017; revised June 1, 2017; accepted July 19, 2017;published OnlineFirst July 27, 2017.
References1. Robinson D, Van Allen EM, Wu YM, Schultz N, Lonigro RJ, Mosquera JM,
et al. Integrative clinical genomics of advanced prostate cancer. Cell2015;161:1215–28.
2. Baca SC, Prandi D, Lawrence MS, Mosquera JM, Romanel A, Drier Y, et al.Punctuated evolution of prostate cancer genomes. Cell 2013;153:666–77.
3. Barbieri CE, Baca SC, LawrenceMS, Demichelis F, Blattner M, Theurillat JP,et al. Exome sequencing identifies recurrent SPOP, FOXA1 and MED12mutations in prostate cancer. Nat Genet 2012;44:685–9.
4. Mitchell T, Neal DE. The genomic evolution of human prostate cancer.Br J Cancer 2015;113:193–8.
5. GrassoCS,WuYM, RobinsonDR,Cao X,Dhanasekaran SM, KhanAP, et al.The mutational landscape of lethal castration-resistant prostate cancer.Nature 2012;487:239–43.
6. Mateo J, Carreira S, Sandhu S, Miranda S, Mossop H, Perez-Lopez R, et al.DNA-repair defects andolaparib inmetastatic prostate cancer.NEngl JMed2015;373:1697–708.
Clin Cancer Res; 23(20) October 15, 2017 Clinical Cancer Research6076
Seed et al.
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

7. Ledermann J, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G, et al.Olaparib maintenance therapy in patients with platinum-sensitiverelapsed serous ovarian cancer: a preplanned retrospective analysis ofoutcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol2014;15:852–61.
8. Fong PC, Boss DS, Yap TA, Tutt A, Wu P, Mergui-Roelvink M, et al.Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA muta-tion carriers. N Engl J Med 2009;361:123–34.
9. Ong M, Carreira S, Goodall J, Mateo J, Figueiredo I, Rodrigues DN, et al.Validation and utilisation of high-coverage next-generation sequencingto deliver the pharmacological audit trail. Br J Cancer 2014;111:828–36.
10. Carreira S, Romanel A, Goodall J, Grist E, Ferraldeschi R, Miranda S, et al.Tumor clone dynamics in lethal prostate cancer. Sci Transl Med 2014;6:254ra125.
11. Talevich E, Shain AH, Botton T, Bastian BC. CNVkit: genome-wide copynumber detection and visualization from targeted DNA sequencing.PLoS Comput Biol 2016;12:e1004873.
12. Olshen AB, Venkatraman ES, Lucito R, Wigler M. Circular binary segmen-tation for the analysis of array-based DNA copy number data. Biostatistics2004;5:557–72.
13. Ferraldeschi R, Nava Rodrigues D, Riisnaes R, Miranda S, Figueiredo I,Rescigno P, et al. PTEN protein loss and clinical outcome from castration-resistant prostate cancer treated with abiraterone acetate. Eur Urol 2015;67:795–802.
14. Grasso C, Butler T, Rhodes K, Quist M, Neff TL, Moore S, et al. Assessingcopy number alterations in targeted, amplicon-based next-generationsequencing data. J Mol Diagn 2015;17:53–63.
15. Kumar A, Coleman I, Morrissey C, Zhang X, True LD, Gulati R, et al.Substantial interindividual and limited intraindividual genomic diversityamong tumors from men with metastatic prostate cancer. Nat Med2016;22:369–78.
16. Cheng HH, Pritchard CC, Boyd T, Nelson PS, Montgomery B. Biallelicinactivation of BRCA2 in platinum-sensitivemetastatic castration-resistantprostate cancer. Eur Urol 2016;69:992–5.
17. Strom CM, Rivera S, Elzinga C, Angeloni T, Rosenthal SH, Goos-Root D,et al. Development and validation of a next-generation sequencing assayfor BRCA1 and BRCA2 variants for the clinical laboratory. PLoS One2015;10:e0136419.
18. Yamamoto Y, De Velasco MA, Kura Y, Nozawa M, Hatanaka Y, Oki T,et al. Evaluation of in vivo responses of sorafenib therapy in a preclin-ical mouse model of PTEN-deficient of prostate cancer. J Transl Med2015;13:150.
19. Park H, Kim Y, Sul JW, Jeong IG, Yi HJ, Ahn JB, et al. Synergistic anticancerefficacy of MEK inhibition and dual PI3K/mTOR inhibition in castration-resistant prostate cancer. Prostate 2015;75:1747–59.
20. Delmore JE, Issa GC, Lemieux ME, Rahl PB, Shi J, Jacobs HM, et al. BETbromodomain inhibition as a therapeutic strategy to target c-Myc. Cell2011;146:904–17.
21. Gao J, Aksoy BA, Dogrusoz U, Dresdner G, Gross B, Sumer SO, et al.Integrative analysis of complex cancer genomics and clinical profiles usingthe cBioPortal. Sci Signal 2013;6:pl1.
22. Cerami E,Gao J,DogrusozU,Gross BE, Sumer SO, Aksoy BA, et al. The cBiocancer genomics portal: an open platform for exploring multidimensionalcancer genomics data. Cancer Discov 2012;2:401–4.
www.aacrjournals.org Clin Cancer Res; 23(20) October 15, 2017 6077
Targeted-seq and Copy Number Analysis of CRPC Biopsies
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972

Correction
Correction: Gene Copy Number Estimationfrom Targeted Next-Generation Sequencingof Prostate Cancer Biopsies: AnalyticValidation and Clinical Qualification
In the original version of this article (1), the name of the 20th author, Arul M.Chinnaiyan, is incorrect. The namehasnowbeen corrected in the recent onlineHTMLand PDF versions of the article. The authors regret this error.
Reference1. Seed G, YuanW,Mateo J, Carreira S, Bertan C, LambrosM, et al. Gene copy number estimation from
targeted next-generation sequencing of prostate cancer biopsies: analytic validation and clinicalqualification. Clin Cancer Res 2017;23:6070–7.
Published first May 1, 2018.doi: 10.1158/1078-0432.CCR-18-0457�2018 American Association for Cancer Research.
ClinicalCancerResearch
Clin Cancer Res; 24(9) May 1, 20182234

2017;23:6070-6077. Published OnlineFirst July 27, 2017.Clin Cancer Res George Seed, Wei Yuan, Joaquin Mateo, et al. Clinical QualificationSequencing of Prostate Cancer Biopsies: Analytic Validation and Gene Copy Number Estimation from Targeted Next-Generation
Updated version
10.1158/1078-0432.CCR-17-0972doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2017/07/25/1078-0432.CCR-17-0972.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/23/20/6070.full#ref-list-1
This article cites 22 articles, 3 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/23/20/6070.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/23/20/6070To request permission to re-use all or part of this article, use this link
Research. on September 11, 2020. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 27, 2017; DOI: 10.1158/1078-0432.CCR-17-0972







![Higher expression of cell division cycle-associated protein 5 … · HCC is characterized by increased genomic instability with extensive copy number alterations [18, 19]. To identify](https://img.pdfslide.net/doc/110x75/604ed000492ea15fc104150d/higher-expression-of-cell-division-cycle-associated-protein-5-hcc-is-characterized.jpg)