-
8/3/2019 General Anaesthesia 1
1/46
GENERAL ANAESTHESIA
Presented by
Dr. Vishal DewalwarLecturer
-
8/3/2019 General Anaesthesia 1
2/46
Definition
A controlled state of unconsciousness
in which there is a loss of protective
reflexes, including the ability to
maintain an airway independently and
to respond appropriately to physicalstimulation. or verbal
command.
-
8/3/2019 General Anaesthesia 1
3/46
Surgery Before Anesthesia
-
8/3/2019 General Anaesthesia 1
4/46
Fun and Frolic led to early Anaesthesia
-
8/3/2019 General Anaesthesia 1
5/46
History of Anaesthesia
Joseph Priestlydiscovered N2O in 1773
Sir Humphrey Davyexperimented with
N2O, reported loss of pain, euphoria
Horace Wells in 1844 demonstrated N2O
for tooth extraction
-
8/3/2019 General Anaesthesia 1
6/46
William Morton, dentistfirst
demonstration of successful surgical
anesthesia with ether in 1846
Dr. John Snow administered chloroform to
Queen Victoria (1853)popularized
anesthesia for childbirth in UK
-
8/3/2019 General Anaesthesia 1
7/46
Goals of Anaesthesia
Hypnosis (unconsciousness)
Amnesia
Analgesia Immobility/decreased muscle tone
(relaxation of skeletal muscle)
Inhibition of nociceptive reflexes Reduction of certain
autonomic reflexes
(gag reflex, tachycardia, vasoconstriction)
-
8/3/2019 General Anaesthesia 1
8/46
Preanaesthetic evaluation
The main purpose of preoperative visit is to
assess the patients fitness for anaesthesia.
This visit allows the most suitable
anaesthetic technique to be determined, any
potential interaction between concurrentdiseases, drugs and
anaesthesia to be
anticipated and also provides reassurance to
the patient.
-
8/3/2019 General Anaesthesia 1
9/46
Anaesthetic History
Previous anaesthesia and major surgeries
Past and present medical history
- CVS, RS
- Pregnancy
Drug and allergies Personal history
- HabitsSmoking, Alcohol, Drugs
-
8/3/2019 General Anaesthesia 1
10/46
Physical Examination
Cardiovascular System
- Cardiac arrhythmias
- Blood pressure
- Peripheral veins
Respiratory System
- Asthma
- COPD`s
-
8/3/2019 General Anaesthesia 1
11/46
Nervous system
- motor or sensory impairment
Musculoskeletal system
- TMJ- Cervical spondilitis
-
8/3/2019 General Anaesthesia 1
12/46
Airway
- assessment is made in 3 stages
1. Observation of patients anatomy
2. Bedside tests
3. X- rays
-
8/3/2019 General Anaesthesia 1
13/46
1. Observation of patients anatomy- Trismus
- Retrognathia
- Position, no. and health of teeth- Size of tongue
- Deviated larynx or trachea
- Midline or lateral swelling of neck
-
8/3/2019 General Anaesthesia 1
14/46
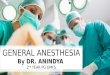
2. Bedside tests
a. Mallampati`s criteria
- view of pharyngeal
structures is noted
and graded as I-IV
-
8/3/2019 General Anaesthesia 1
15/46
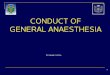
b. Thyromeatal distance
- distance between
bony point of the chin
and the prominence ofthyroid cartilage
- a distance less than
7cm suggests difficult
intubation
-
8/3/2019 General Anaesthesia 1
16/46
3. X - rays
- Lateral and AP neck X - rays are advised
- measurements can be made on lateral
X - ray of head and neck
-
8/3/2019 General Anaesthesia 1
17/46
Preanaesthetic medication
It refers to the drugs administered to facilitate theinduction
and maintenance of anaesthesia.
The 6 A`s premedication1.Anxiolysis
2.Amnesia
3.Anti-emetic
4.Antacid
5.Anti-autonomic
6.Analgesic
-
8/3/2019 General Anaesthesia 1
18/46
Aims
1. Relief of anxiety and apprehension
preoperatively and to facilitate smooth
induction.
2. Amnesia for pre and post operative events.
3. Supplement analgesic action of
anaesthetics and potentiate them so thatless anaesthetic is
needed.
-
8/3/2019 General Anaesthesia 1
19/46
3. Decrease secretions and vagal stimulationcaused by
anaesthetics.
4. Antiemetic effect extending to the
postoperative period.
5. Decreases acidity and volume of gastric
acid so that it is less damage if aspirated.
-
8/3/2019 General Anaesthesia 1
20/46
Anticholinergics
ATROPINE
Atropine is the prototype drug of anticholinergic class and
is
highly selective for muscarinic receptors.
ACTION:-Blocks the muscarinic effects of acetylcholine as it
has
the same affinity for muscarinic receptors as
acetylcholine but poor intrinsic activity.
USES :- 1. Preanasesthetic medication
2.Organophosphorous poisoning
3.Bradyarrhythmias
4.Motion sickness
5.Colic and dysmenorrehea
-
8/3/2019 General Anaesthesia 1
21/46
SIDE EFECTS :-1.Dry mouth, dysphagia, constipation, paralytic
ileus
2.Urinary retention
3.Blurred vision and precipitates of glaucoma
4.Allergic dermatitis
PRECAUTIONS:-1.In elderly it precipitates glaucoma and
urinary
retention(if enlarged prostate).
2.In chronic lung diseases it dries up secretions.
DOSE :-ATROPINE SULPHATE 0.6mg/ml inj. i.m.,i.v.
6.Peptic ulcer
7.Parkinson`s disease
8.To produce mydriasis and cycloplegia
-
8/3/2019 General Anaesthesia 1
22/46
RANITIDINE
It is introduced as a non-imidazole H2 blocker.
ACTION:-1. Abolishes histamine stimulated gastric acid
secretion
and flushing.
2. Inhibits gastric H2 receptors, this reduces basal, 24
hours
and nocturnal acid secretion.
3. Has mucosal protective action.
USES:- 1.Preaneasthetic medication.
2.Peptic ulcer.
3.Esophagitis.
H2 BLOCKER
-
8/3/2019 General Anaesthesia 1
23/46
6.Gastro oesophageal reflux disease(GERD).
SIDE EFFECTS :- 1.Blood dycrasias.
2.Skin rash.
3.Leucopenia
DOSE :-300mg/day or 150mg BD
50mg i.m. or slow i.v.every 6 to 8 hrs.
TRADE NAME :- ULTEC,ZENTAC,RANITINE,ACILOC.
4.Stress ulcer
5.Zollinger- Ellision syndrome
-
8/3/2019 General Anaesthesia 1
24/46
ONDANSETRON
It is the prototype of a new class of anti emetic drugs
developed tocontrol cancer chemotherapy/radiotherapy induced
vomitting and later
found to be highly effective in postoperative nausea and
vomiting as
well.
USES:- 1.Preaneasthetic medication.
2.It is given before starting chemotherapy
especially CISPLASTIN.
SIDE EFFECTS:- 1.GI:diarrohea
.
ANTIEMETIC
-
8/3/2019 General Anaesthesia 1
25/46
DOSE : 4-8mg BD or TDS orally or i.v.
TRADE NAME:-EMESET,VOMIZ,OSETRON
2.Skin:rashes
3.Miscellaneous;headache, blurred vision,
hypokalemia, anaphylactoid reaction.
-
8/3/2019 General Anaesthesia 1
26/46
INTRAVENOUS ANAESTHETICS
INTRAVENOUS
Inducing agents Slower acting drugs
Thiopentone sodium Benzodiazepines
Propofol Diazepam
Midazolam
Dissociative anaesthesia
Ketamine
-
8/3/2019 General Anaesthesia 1
27/46
Inducing agents
These are drugs which on i.v. injection
produce loss of consciousness.
They are generally used for induction
because of rapidity of onset of action.
-
8/3/2019 General Anaesthesia 1
28/46
THIOPENTONE SODIUM
It is an ultra short acting barbiturate highly soluble in
water.
It must be prepared freshly before injection.
ACTION :- Its undissociated form has high lipid solubility &
enters
brain almost instantaneously to produce unconsciousness
in 15-20 sec & last till 10-20 min.
USES :- 1.Inducing agent along with anaesthetic.
2. Rapid control of convulsions.
3. Gradual i.v. infusion of subanaesthetic doses can be
used to facilitate verbal communication with psychiatric
patient.
-
8/3/2019 General Anaesthesia 1
29/46
ADVERSE EFFECTS:- 1. Laryngosparm when respiratory
secretions
or other irritants are present.
2. Shivering & delirium.3. Post operative pain.
CONTRAINDICATION:- Acute intermittent porphyria.
N.B. :- Succinylcholine & thiopentone react
chemically should not be mixed in the
same syringe.
DOSE :- 3-5 mg/kg as a 2.5% solution.
TRADE NAME :- PENTOTHAL, INTRAVAL SODIUM.
PROPOFOL
-
8/3/2019 General Anaesthesia 1
30/46
PROPOFOL
It is an oily liquid introduced recently as a 1% emulsion for
i.v.
induction & short duration anaesthesia.
ACTION :- Unconsciousness after propofol injection occurs in
15-45sec & lasts for 15min.
USES :- 1.Inducing agent; particularly for out patient
surgery.
2. In subaneasthetic doses; used for sedation in
intensive care units.
SIDE EFFECTS :- 1. Pain during injection.
2. Dose dependent respiratory depression.
DOSE :- 2mg/kg bolus i.v. for induction
9mg/kg/hr for maintenance.
-
8/3/2019 General Anaesthesia 1
31/46
SLOWER ACTING DRUGS
BENZODIAZEPINES
In addition to preanaesthetic medication; BZDs are now
frequentlyused for inducing, maintaining and supplementing
anaesthesia.
ACTION :-Injected i.v. produce sedation, amnesia and
thenunconsciousness in 10-15 minutes. If no other
anaesthetic or opioid is given, the patient becomes
responsive in 1 hr but amnesia persists for 2-3 hr
and sedation for 6 hr or more.
USES :-1. Sedative and Hypnotic.
-
8/3/2019 General Anaesthesia 1
32/46
2. Muscle Relaxant
3. Preanaesthetic Medication
4. Alcohol Withdrawal
5. Anxiety Neurosis
6. Petit-mal, Psychomotor and Status Epilepticus.SIDE EFFECTS:-
1. Drowsiness
2. Ataxia
3. Respiratory Depression4. Hypotension
-
8/3/2019 General Anaesthesia 1
33/46
MIDAZOLAM
Water Soluble
Non IrritatingFaster and Shorter Acting
3 Times more potent than Diazepam
-
8/3/2019 General Anaesthesia 1
34/46
KETAMINE
It induces a so called Dissociative Anaesthesia
- profound analgesia,immobility, amnesia with light sleep and
feeling of dissociation from
ones own body and the surroundings.
ACTION:- It acts within a minute and recovery starts after
10-15
minutes, but patient remains amnesic for 1-2 hrs.
USES :-1.Recommended for Operations on head and neck.
2.In patients who have bled.
3.In Asthmatics (relieves bronchopasm).
4.In burn dressings.
-
8/3/2019 General Anaesthesia 1
35/46
SIDE EFFECTS :- 1. Emergence Delirium
2. Hallucinations
3. Involuntary Movements
DOSE :- 1-4(average 2)mg/kg i.v. or
6.5-13(average10)mg/kg i.m.
TRADE NAME :- KETAMIN, KETLAR.
-
8/3/2019 General Anaesthesia 1
36/46
SKELETAL MUSCLE RELAXANTS
Skeletal muscle relaxants are drugs that act peripherally at the
neuro
muscular junction/muscle fibre itself or centrally in the
cerebrospinal
axis to reduce muscle tone and/or cause paralysis.
Peripherally acting Centrally acting
muscle relaxants muscle relaxants
*Non Depolarizing blockers *Mephenesin group
Pancuronium Chlorzoxazone
d-Tubocurarine *Benzodiazepines
*Depolarizing blockers Diazepam and others
Succinylcholine *GABA Derivative
Baclofen
Comparative features of central and peripheral muscle
relaxants:-
-
8/3/2019 General Anaesthesia 1
37/46
Comparative features of central and peripheral muscle
relaxants:
Centrally acting Peripherally acting
1.Decrease muscle tone without 1.Cause muscle paralysis,
reducing voluntary action. Voluntary movements lost.
2.Selectively inhibit polysynaptic 2.Block neuromuscular
reflexes in CNS. transmission.
3.Cause CNS depression. 3.No effect on CNS.
4.Given orally sometimes 4.Practically always given
parenterally. i.v.
5.Used in chronic spastic condition, 5.Used for short term
purposes
acute muscle spasms,tetanus. (surgical procedures).
-
8/3/2019 General Anaesthesia 1
38/46
MECHAISM OF ACTION
NON-DEPOLARIZING BLOCKERS(COMPETITIVE)-
They combine with the receptors on the motor end-plate and
thus
block the action of acetylcholine by competitive blockade.
DEPOLARIZING BLOCKERS(NON-COMPETITIVE)-
Depolarize muscle end-plates by opening Na-channels & thus
act as
partial agonist of acetylcholine.
-
8/3/2019 General Anaesthesia 1
39/46
SUCCINYLCHOLINE
Commonly used muscle relaxant for passing tracheal tube.
Induces rapid, complete and predictable paralysis with
spontaneous recovery in 5min.
DOSE :- 50mg/ml injection, 2ml ampule.
TRADE NAME:- MIDARINE.
-
8/3/2019 General Anaesthesia 1
40/46
PANCURONIUM
Synthetic steroidal compound.
Provides good cardiovascular stability.
Seldom induces flushing, bronchospasm or cardiac
arrhythmias.
Relatively inexpensive.
Reversal often required due to its long duration of action.
DOSE :- 2mg/ml in 2ml amp.
TRADE NAME:- PAVULON, PANCONIUM.
-
8/3/2019 General Anaesthesia 1
41/46
ATRACURIUM
4 times less potent than pancuronium & shorter acting.
Inactivation in plasma by spontaneous non-enzymatic
degradation
(HOFFMANN ELIMINATION).
DOSE :- 10mg/ml injection in 2.5ml vial.
TRADE NAME:- TRACRIUM.
ANALGESICS
-
8/3/2019 General Anaesthesia 1
42/46
ANALGESICS
DICLOFENAC SODIUM
It is non-opioid analgesic , anti-pyeretic non-steroidal
anti-inflammatory drug.
ACTION :- It inhibits synthesis and has short lasting
antiplatelet action.
USES :-1. Post-traumatic and postoperative
inflammatory conditions-affords quick relief ofpain and
edema.
2. Rheumatoid & osteoarthritis, bursitis.
3. Ankylosing spondylitis.
-
8/3/2019 General Anaesthesia 1
43/46
SIDE EFFECTS :-1.Epigastric pain, nausea.
2.Headache, dizziness,rashes.
DOSE :- 50 mg TDS
75 mg deep i.m.
TRADE NAME :- VOVERAN, DICLONAC.
-
8/3/2019 General Anaesthesia 1
44/46
PENTAZOCINE
It is the first opioid agonistantagonist to be used as an
analgesic.
ACTION :- 1. Raises pain threshold & modifies
emotional reaction to pain.
2.Inhibits transmission of impulses across
the pain pathways in CNS.
USES :-1. Potent analgesic with low addiction
liability.
SIDE EFFECTS :- 1. Respiratory depression.
2. Hallucinations and unpleasant dreams.
3. Pulmonary & systemic hypertension.
-
8/3/2019 General Anaesthesia 1
45/46
DOSE :- 50-100 mg orally.
30-60 mg i.m. , s.c.
TRADE NAME :- FORTWIN, MERIWYN, SOSEGON.
-
8/3/2019 General Anaesthesia 1
46/46
THANK YOU