Embed Size (px)
DESCRIPTION
Citation preview

UK IBD Audit 2006
National Results for the Organisation & Process of IBD Care in the UK
Prepared by
The UK IBD Audit Steering Group on behalf of
• Association of Coloproctology of Great Britain and Ireland
• British Society of Gastroenterology • Clinical Effectiveness & Evaluation Unit,
Royal College of Physicians of London • National Association for Colitis and Crohn’s Disease
February 2007


REPORT PREPARED BY: Dr Keith Leiper Consultant Gastroenterologist, Royal Liverpool University Hospital & Clinical Director for the UK IBD Audit Mr Derek Lowe Medical Statistician, Clinical Effectiveness and Evaluation Unit, Royal College of Physicians
Mr Richard Driscoll Director, National Association for Colitis and Crohn’s Disease (NACC)
Miss Asha Senapati Consultant Surgeon, Queen Alexandra Hospital, Portsmouth
Professor Jonathan Rhodes Professor of Medicine, University of Liverpool
Mr Calvin Down IBD Audit Project Manager, Clinical Effectiveness and Evaluation Unit, Royal College of Physicians
Miss Nancy Pursey IBD Audit Project Co-ordinator, Clinical Effectiveness and Evaluation Unit, Royal College of Physicians ACKNOWLEDGEMENTS The Royal College of Physicians of London and the UK IBD Audit Steering Group (Appendix 1) thank and acknowledge all who have participated in the piloting and development of the audit since the beginning of the Project. The web based data collection tool was developed by Netsolving Ltd. Thanks are due to the many people who have participated in the UK IBD Audit 2006. It is recognised that this has involved many individuals spending time over and above an already heavy workload with no financial recompense. Thanks are also due to
• The Health Foundation who fund the UK IBD Audit • The Association of Coloproctology of Great Britain and Ireland • The British Society of Gastroenterology • The National Association for Colitis and Crohn’s Disease (NACC) • All those who contributed to organising the collection, retrieval and input of data including audit,
IT and coding staff in addition to the members of the clinical teams.


UK IBD Audit 2006 Report
CONTENTS Page Executive summary 5
Introduction 15 Aims of the Audit 15 Availability of this report in the public domain 15 Methods 16 Standards in the audit 16 Data collection tool 16 Definition of a ‘site’ 16 Recruitment 16 Selection criteria for the patient cohorts (ICD-10 codes) 17 Data reliability 17 Presentation of results 18
RESULTS
Section 1. Key National Results for England, Northern Ireland, Scotland and Wales 19
Organisation and Structure 19 Ulcerative Colitis Inpatients 20 Crohn’s Disease (inpatients & outpatients) 21 Section 2. Organisation and Structure of IBD services as at 1st June 2006 23
General Hospital Demographics 23 Inpatient activity 24 Gastroenterology services 24 Colorectal services 26 Multi-disciplinary working 26 Dietetics & Nutritional services 27 Outpatient services 28 Patient information 28 Monitoring of established immunosuppressive therapy 29 IBD support services 29 Management of Ulcerative Colitis 29 Interactions between hospital and patients and patient groups 30 Section 3. Clinical Audit: Ulcerative Colitis (Inpatient) 31 Patient demographics 31 Admission 32 Co-morbidity 33 Inpatient mortality 33 Mortality after discharge 33 Length of stay 34 Assessment: patient history 34 Assessment: severity of disease 35 Assessment: endoscopic assessment 36 Monitoring of Colitis post admission – general information 37 Monitoring of Colitis post admission – radiology 39 Medical intervention – steroid therapy 40 Medical intervention – other therapies 41

UK IBD Audit 2006 Report Medical intervention - initiating ciclosporin therapy 42 Medical intervention – monitoring ciclosporin therapy 43 Surgical intervention 44 Surgical complications 46 Discharge arrangements 46 Section 4. Clinical Audit: Crohn’s Disease (Inpatient) 48 Patient demographics 48 Admission 48 Admitting speciality 49 Inpatient mortality 50 Mortality after discharge 50 Length of stay 51 Co-morbidity 51 Medication on admission 51 Smoking status 52 Patient history 52 Assessment: severity of disease 53 Assessment: exclusion of infection 54 Assessment: documentation of sepsis 54 Assessment: imaging 55 Assessment: weight assessment & dietetic support 56 Assessment: use of anti-thrombotic therapies 57 Medical intervention - steroid therapy 57 Medical intervention – blood transfusion 57 Medical intervention – treatment initiation with anti-TNF during admission 58 Surgical intervention 58 Post-operative prophylactic therapy 60 Discharge arrangements 61 5. Clinical Audit: Crohn’s Disease (Outpatient) 62 Patient history 62 Assessment of Crohn’s activity 63 Smoking status 64 Monitoring of immunosuppressive therapy 64 Use of corticosteroids 65 Use of anti-TNF therapy 66 Appendices 1. Membership of the UK IBD Audit 2006 Steering Group 67 2. Copies of Audit Proformas 69 3. Pilot sites 92 4. List of hospitals that submitted data to the audit 93 5. List of hospitals that did not submit data to the audit 96 6. UK IBD Steering Group list of IBD Standards 97

5
UK IBD Audit 2006 Executive Summary Background The UK IBD Audit is the first UK-wide audit performed within gastroenterology. The 1st Round of the UK Inflammatory Bowel Disease Audit was conducted from September 2006 to December 2006. National audit data could support the self assessment requirements of the Healthcare Commission. Although ignored by the National Service Framework program, gastroenterological conditions are common and after cardiac and respiratory disease are the third most common reason for acute medical emergency admissions. IBD includes Crohn’s Disease and Ulcerative Colitis, different disorders, but with considerable overlap in terms of health service care. Together, they affect about 1 in 400 of the population. They present in late adolescence or early adult life so typically affect people who are trying to earn a living and/or raise a family. IBD accounts for 0.3% of absences from work in the UK with an estimated loss of £115 million in productivity per year. At least 80% of Crohn’s disease patients need surgery at some time, as do 25% of patients with ulcerative colitis. There are about 27,000 admissions per year for exacerbations of IBD and admissions are associated with significant mortality. Many deaths occur around the time of surgery and data indicates that young people are disproportionately represented amongst those deaths. Data from individual hospitals has shown a marked variation in mortality rates across the UK. The UK IBD Audit seeks to improve the quality and safety of care for IBD patients in hospitals throughout the UK by auditing individual patient care, service resources and organisation against national standards. The British Society of Gastroenterology has recently published national evidence based guidelines that cover all the clinical aspects of management of IBD. Audit Aims
1. Assess the current structure and organisation of care for those patients with IBD 2. Assess the processes and outcomes of care delivery (inpatient and outpatient) in IBD 3. Enable Trusts to compare their performance and quality of care against national standards 4. Identify resource and organisational factors that may account for variations in care 5. Facilitate, develop and institute an intervention strategy to improve quality of patient care. 6. Repeat the audit to prove that change has occurred 7. Establish measures that healthcare services can use beyond the study to compare quality of IBD
services 8. Develop a sustainability programme to maintain quality of patient care.
This report addresses aims 1, 2, 3 & 4 enabling each site to compare or benchmark their performance against national statistics. Audit Organisation The audit is a collaborative partnership between Gastroenterologists (the British Society of Gastroenterology), Colorectal Surgeons (the Association of Coloproctology of Great Britain and Ireland), Patients (the National Association for Colitis and Crohn’s Disease) and Physicians (the Royal College of Physicians of London). It is funded by a grant from the Health Foundation as part of their Engaging with Quality Initiative which aims to improve the quality of clinical care by engaging clinicians in quality improvement. The audit is a four-year, nation-wide, full cycle comparative audit with initial audit, dissemination, change implementation and re-audit.

UK IBD Audit 2006 Report
6
The audit is co-ordinated by the Clinical Effectiveness and Evaluation unit (CEEu) of the Royal College of Physicians of London. Each hospital identified a lead from their IBD service and data were collected by hospitals using a standardised method. Data collection was overseen at site level by a lead agreed within the site IBD service. The audit was guided by a multidisciplinary IBD Audit Steering Group (Appendix 1) which oversaw the preparation, conduct, analysis and reporting of the audit. Who participated? 281 acute hospitals that admit patients with Inflammatory Bowel Disease (IBD) in England, Northern Ireland, Scotland and Wales (plus the Isle of Man and the Channel Islands) were invited to take part. 200 sites submitted data (England 159, Northern Ireland 10, Scotland 14, Wales 15, Islands 2). Of these 200 sites, 12 were Trust-wide sites combining 2 hospitals with a total of 212 hospitals entering data. We aimed to get 80% of applicable Acute Hospitals in the UK - a tough but realistic target for a discipline without any previous record of national audit- and achieved 75% participation. This response was achieved through the hard work and time-commitment of clinical teams involved in the management of patients with IBD.
The audit of the organisation of IBD services was ‘as of 1st June 2006’ (together with activity data from 1st June 2005 to 31st May 2006) and 181 sites submitted data. For individual patient care, 40 consecutive inpatient case notes were audited (20 Crohn’s Disease and 20 Ulcerative Colitis) admitted from 1st June 2006 working backwards as far as 1st June 2004. For both Ulcerative Colitis (UC) and Crohn’s Disease (CD), inpatient details were audited and for CD the last outpatient visit prior to admission was audited. In total, data were collected for 2767 Ulcerative Colitis patients (from 180 sites), median (IQR) of 19 (11-20) per site, and for 2914 Crohn’s Disease patients (from 185 sites), median (IQR) of 19 (12-20) per site. Results The complete results of the audit are presented in full in this audit report. The Executive Summary focuses on the Key messages derived from the full report in the opinion of the UK IBD Audit Steering Group. Key Messages Key messages are summarised below (with histograms illustrating site variation). These include areas where improvement of care across the UK is urgently required.

UK IBD Audit 2006 Report
7
Organisation & Structure of hospital IBD Services Inpatient activity and organisation of services
• Multidisciplinary team working functions well with timetabled meetings between gastroenterologists and surgeons in 74% of sites. Joint or parallel medical-surgical clinics occur in only 47%. Comment: IBD MDT meetings should occur regularly at all sites.
• Hospitals vary considerably in their yearly inpatient activity in IBD; median (Interquartile range
[IQR]) 50 (25-105) range 1-481 for Ulcerative Colitis and 61 (30-111) range 2-609 for Crohn’s Disease. Comment: some smaller hospitals may need to interact with larger ones to provide a comprehensive inpatient IBD service.
• 44% of sites have no IBD clinical nurse specialist(s). Amongst those with specialist nurses, the
median number of sessions dedicated to IBD care is 6 per week. Comment: IBD clinical nurse specialist(s) service needs to be expanded to include all sites caring for patients with IBD.
• 33% of sites did not have a dedicated gastroenterology ward (medical or surgical). Comment: a
dedicated gastroenterology ward or ward area should be identifiable at each site.
• There are not enough toilets with a median 4.5 beds per toilet. Comment: there should be a maximum of 3 beds per toilet.
• Provision of dietetic services is poor with a median of 2 (IQR 0-5) sessions per week dedicated to
gastroenterology. Comment: IBD patient surveys show dissatisfaction with the lack of dietetic services. There needs to be improvement in the provision of these services.
• Ileo-anal pouch procedures are performed in most sites (72%) but the volume of surgery is low
(median 4 [IQR 2-7] per year). Comment: hospitals with a low volume of pouch surgery should consider referring to hospitals with a larger volume of pouch surgery.
• Only 34% of sites have a searchable IBD database. Comment: Provision of databases need to
improve across the UK to facilitate patient care (e.g. colorectal cancer surveillance, immunosuppressive therapy monitoring) and audit
Interactions between hospitals and patients and patient groups
• Open forum or other meetings with patient groups are uncommon in the UK with only 30% of sites involved in these. Comment: IBD teams should be encouraged to set up meetings with patient groups, perhaps on a regional basis.
IBD Support services
• Only 21% of sites have pathways for direct access to psychological support. Comment: direct referral pathways should be available for IBD teams to refer directly to psychological support services.

UK IBD Audit 2006 Report
8
Ulcerative Colitis Inpatients:
• 31% of patients admitted with Ulcerative Colitis are not transferred to a specialist gastroenterology ward (medical, surgical or joint). Comment: Triage systems for IBD should be established to ensure that admitted patients are under the care of the relevant specialty team.
• Inpatient mortality was 1.6% (45 patients). 25 deaths were directly related to Ulcerative Colitis,
including 15 that occurred in patients who had surgery. Comment: further analyses are being performed to investigate possible correlations with mortality.
• Stool culture was done in 59% of patients (CDT done in 47%). Comment: both stool culture and
CDT should be performed in all patients admitted with active Ulcerative Colitis.
• For new diagnoses of Ulcerative Colitis, endoscopic evaluation was done a median of 2 (IQR 1-5) days from admission. Histology was reported a median of 5 (IQR 2-7) days after endoscopic procedure. Comment: In many sites there is a delay in obtaining reported histology. For suspected new diagnosis of Ulcerative Colitis admitted to hospital, histology should be reported within 5 days of biopsies being taken.
• 40% of Ulcerative Colitis inpatients did not receive prophylactic heparin. Comment: in-patients
with Ulcerative Colitis should receive prophylactic heparin.
• For those Ulcerative Colitis patients failing to respond to high dose steroids (high CRP and high stool frequency after 3 days therapy), surgery was the next therapy in 42%, 25% had ciclosporin and 4% anti-TNF-α therapy. Comment: rescue medical therapy (ciclosporin or anti-TNF-α therapy) was infrequently used. This an area in which participation in clinical trials is needed. Functional clinical trials networks would be beneficial.
• The decision to operate was made by a consultant colorectal surgeon in 77% of elective operations
and 81% of emergency operations. 92% elective and 77% emergency operations were performed or assisted by consultant colorectal surgeons. Comment: consultant colorectal surgeons should be involved in the decision to operate and perform (or assist) operations for inflammatory bowel disease
Crohn’s Disease Inpatients:
• Smoking status was not documented in 15% of cases. Comment: smoking cessation support is an important aspect in treating people with Crohn’s Disease.
• Only 52% of patients admitted with Crohn’s Disease were weighed and only 37% were seen by a
dietitian. Comment: patients admitted with Crohn’s Disease should be weighed and seen by a dietitian.
• Prophylactic anti-thrombotic therapy was not given in 38% of cases. Comment: in-patients with
Crohn’s Disease should receive prophylactic heparin.
• For elective surgery, 12% of cases were done laparoscopically/ laparoscopically-assisted. Comment: There is marked variation geographically in the provision of laparoscopic surgery for IBD. Laparoscopic surgery should be available as an option for patients with Crohn’s Disease requiring resectional surgery.

UK IBD Audit 2006 Report
9
• In 49% of cases where resectional surgery was performed for Crohn’s Disease, post-operative
prophylactic therapy was not given. Comment: prophylactic therapy to try to reduce recurrence should be discussed with Crohn’s Disease patients having resectional surgery with anastomosis.
Crohn’s Disease Outpatient care
• Established immunosuppressive therapy was monitored by full blood count at least 3 monthly in around 90% of cases. Comment: full blood count should be monitored at least 3 monthly for all patients on established immunosuppressive therapy.
• 46% of patients receiving systemic corticosteroids received continuous therapy for more than 3
months. 12% of these received anti-TNF- therapy. Comment: Prolonged use of steroid therapy is of no benefit in maintaining remission in Crohn’s Disease, increases the risk of septic complications and is associated with an increased mortality. Prolonged use of steroids (oral prednisolone or budesonide) should be avoided.
• Only 45% of patients on systemic steroids were prescribed bone protection agents and only 18%
had bone densitometry performed within 12 months of initiation of systemic corticosteroids. Comment: there is inadequate prophylactic bone protection therapy given for patients on systemic steroids and inadequate screening for osteoporosis.
Research
• Only two Ulcerative Colitis patients failing high dose steroids participated in any clinical trial and only ten Crohn’s Disease patients were on any trial drug on admission, both <1% participation. Comment: There seems to be infrequent participation in clinical research - functional clinical trials networks would be beneficial.


UK IBD Audit 2006 Report
10
Site variation histograms for Key Indicators
Beds per lavatory on the ward. Median 4.5, Inter-Quartile Range 3.0-6.0, n=118 sites with a dedicated Gastroenterology ward. Note that two outliers have been excluded from the histogram
Gastroenterology Beds Per Lavatory14.012.010.08.06.04.02.00.0
Site
s
25
20
15
10
5
0
Number of IBD specialist nurse sessions. Median 1, Inter-Quartile Range 0-6 sessions, n=170 sites Note that one outlier has been excluded from the histogram
Sessions of Specialist Nurse time dedicated to IBD care per week2520151050
Site
s
90
80
70
60
50
40
30
20
10
0

UK IBD Audit 2006 Report
11
Number of sessions of dietetic support Median 2, Inter-Quartile Range 0-5, n=171 sites
Dietetic sessions per week dedicated to GI disorders2520151050
Site
s
60
50
40
30
20
10
0
% of IBD patients (UC or Crohn’s) with diarrhoea who had standard stool culture and CDT performed. Median 42%, Inter-Quartile Range 23-56%, n=178 sites
% stools sent for standard culture AND for CDT (UC+Crohn's patients)1009080706050403020100
Site
s
25
20
15
10
5
0

UK IBD Audit 2006 Report
12
% of IBD admissions (UC & Crohn’s cases) with prophylactic heparin Median 62%, Inter-Quartile Range 46-77%, n=179 sites
% for prophylactic heparin (UC +Crohns cases)100806040200
Site
s
20
15
10
5
0
% of operations done or assisted by a consultant colorectal surgeon (UC & Crohn’s cases) Median 83%, Inter-Quartile Range 69-95%, n=179 sites
% for consultant colorectal surgeon operating or assisting (UC+Crohns)1009080706050403020100
Site
s
50
40
30
20
10
0

UK IBD Audit 2006 Report
13
% with Bone protection agents prescribed alongside oral steroids (UC cases at discharge) Median 40%, Inter-Quartile Range 20-64%, n=179 sites
% Bone protection agents prescribed (UC)1009080706050403020100
Site
s
25
20
15
10
5
0
% of patients at any point taking oral corticosteroids for > 3 months (Crohn’s outpatient cases) Median 43%, Inter-Quartile Range 20-64%, n=175 sites
% Taking oral corticosteroids for Crohn's Disease continuously for >3M1009080706050403020100
Site
s
40
30
20
10
0
UK IBD Audit 2006 Report
14
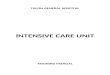
% with weight measured during admission (Crohn’s Disease inpatient cases) Median 50%, Inter-Quartile Range 31-71%, n=185 sites
% Weight measured during admission (Crohn's Disease)1009080706050403020100
Site
s
20
15
10
5
0
Next steps in the UK IBD Audit process - 2007 and beyond During 2007 multi-disciplinary regional meetings will stimulate local discussion of results and look for local solutions to identified problems. This approach is known to work but the project would like to accelerate the pace of change. A “Model” Action Plan for IBD services will be developed by the Project team and Steering Group in conjunction with hospital teams. This will be an interactive process with the IBD community nationwide. A subgroup of sites will then be selected at random to receive intensive support with action planning. It is hoped that the progress of this subgroup can be compared to the progress of other hospitals in changes to organisational structure, processes and outcome. Round 2 of the audit is planned for 2008-2009 in which both organisational and clinical care audits will be repeated. The number of questions will be reduced in the 2nd round of audit and will be largely based on the key messages above. The project hopes to see change for each of these dimensions.


UK IBD Audit 2006 Report
15
INTRODUCTION Although ignored by the National Service Framework program, gastroenterological conditions are common and after cardiac and respiratory disease are the third most common reason for acute medical emergency admissions1. IBD includes Crohn’s Disease and Ulcerative Colitis, different disorders, but with considerable overlap in terms of health service care. Together, they affect about 1 in 400 of the population. They present in late adolescence or early adult life so typically affect people who are trying to earn a living and/or raise a family. IBD accounts for 0.3% of absences from work in the UK with an estimated loss of £115 million in productivity per year2. At least 80% of Crohn’s Disease patients need surgery at some time, as do 25% of patients with ulcerative colitis. There are about 27,000 admissions per year for exacerbations of IBD3 and admissions are associated with significant mortality4. Many deaths occur around the time of surgery and data indicates that young people are disproportionately represented amongst those deaths5. The British Society of Gastroenterology has recently published national evidence based guidelines that cover all the clinical aspects of management of IBD6. In parallel a “Service and standards of Care” document has been produced that sets out the requirements that should be in place to deliver a first class service7. The latter standards are largely consensus based because as for most chronic conditions (including those covered by NICE guidelines), the evidence on care delivery is scanty. The UK IBD Audit seeks to improve the quality and safety of care for IBD patients in hospitals throughout the UK by auditing individual patient care, service resources and organisation against national standards. The project is a collaborative working partnership between the Association of Coloproctology of Great Britain and Ireland, the British Society of Gastroenterology, the National Association for Colitis and Crohn’s Disease and the Royal College of Physicians of London Clinical Effectiveness & Evaluation Unit (CEEu). The project is funded by a grant from the Health Foundation and is a four-year, nation-wide, full cycle comparative audit with initial audit, dissemination, change implementation and re-audit. Specifically, the audit aims to:
1. Assess the current structure and organisation of care for IBD 2. Assess the processes and outcomes of care delivery (inpatient and outpatient) in IBD 3. Enable Trusts to compare their performance against national standards 4. Identify resource and organisational factors that may account for observed variations in care 5. Facilitate, develop and institute an intervention strategy to improve quality of care. 6. Repeat the audit to prove that change has occurred 7. Establish measures that healthcare services can use beyond the study to compare quality of IBD
services 8. Develop a sustainability programme to maintain quality of care.
This report addresses aims 1, 2, 3 & 4 enabling each site to compare their performance against national statistics. Availability of audit reports in the public domain Individual hospital site results will not be placed in the public domain as agreed upon registration for this audit. Generic National results will be available to the Department of Health in England, the Scottish Executive Health Department, NHS Wales Department (Welsh Assembly Government) and the Department of Health, Social Services and Public Safety in Northern Ireland. More limited summary data on the first round of audit will be made available to the SHAs and PCTs and to the Healthcare Commission in England. A Concise Report of the National Results from the 1st round will be available in the public domain via the Clinical Standards section of the Royal College of Physicians external website: www.rcplondon.ac.uk
1 Pearson MG, Littler J, Davies PDO. An analysis of medical workload by speciality and diagnosis in Mersey - evidence of patient to specialist mismatch. J. Roy. Coll. Phys. 1994; 28:230-234 2Lewison G Gastroenterology in the UK: the burden of disease. PRISM/Wellcome report for the British Society of Gastroenterology. 1997 http://www.bsg.org.uk/pdf_word_docs/burden_disease.pdf3Bassi A, Dodd S, Williamson P, Bodger K. Cost of illness of inflammatory bowel disease in the UK: a single centre retrospective study. Gut. 2004;53:1471-8 4Stenner JMC, White P, Gould SR, Lim AG. Audit of the management of severe ulcerative colitis in a DGH. Gut 2001; 48:A87 5Card T, Hubbard R, Logan RF. Mortality in inflammatory bowel disease: a population-based cohort study. Gastroenterology. 2003;125:1583-90 6Agrawal A, Bundred P, Kennedy S, Leiper K, Ellis A, Morris AI, Rhodes JM. Social deprivation and mortality in Crohn’s disease. Presented British Society of Gastroenterology, Glasgow, March 2004. Gut 2004;53:A98 7 Hawthorne AB, Travis SPL and the BSG IBD Clinical Trials Network. Outcome of inpatient management of severe ulcerative colitis: a BSG IBD Clinical Trials Network Survey. Gut 2002; 50:A16

UK IBD Audit 2006 Report
16
METHODS
Standards in the audit The full proformas of questions are shown in Appendix 2. The questions are largely based on the BSG document ‘Guidelines for the management of inflammatory bowel disease in adults’ (Gut. 2004) 1. The standards listed against each data item throughout Sections 2- 5 of this report were agreed through consensus by the UK IBD Audit Steering Group unless directly stated as otherwise. A full list of the standards for this report appears as Appendix 6. The set of audit questions were developed by the UK IBD Audit Steering Group and both the questions and data collection method were assessed in extensive piloting involving data from 23 sites recruited throughout the UK (Appendix 4). These questions, subject to minor changes that might be considered by the Steering Group as standards change and new areas are considered, are to be repeated in Round 2 and will allow an assessment of change in standards over time, a high priority for hospitals.
Data collection tool Data were collected using the internet. The web tool included context specific online help including definitions and clarifications, internal logical data checks and feedback to enable more complete and accurate data. Security and confidentiality were maintained through the use of site specific codes. Sites accessed the proformas by using unique identifiers and passwords and data could be saved during as well as at the end of an input session. Definition of a ‘site’ Lead clinicians were asked to collect data on the basis of a unified service typically within a single hospital. Some institutions (7 in total) which run IBD services across two sites with the same staff completed the audit as one Trust-wide site. Recruitment
Three individuals from each hospital were approached: a lead Clinician, lead Surgeon and a lead from within their Clinical Audit Department. An overall “audit lead” from each site was then identified, following local discussion. The identified “audit lead” was responsible for the quality of data supplied by their particular site. Trust Chief Executives were alerted to the study. The target recruitment was set at 80% of Acute Hospitals in the UK that admit patients with IBD – a tough but realistic target for a discipline without any previous record of national audit. 293 acute hospitals throughout UK were initially contacted. Of these 12 said they were not eligible as they did not admit IBD patients acutely. Of the remaining 281 acute hospitals 84% (237) registered to take part, registering as 225 sites (12 of which were Trust-wide sites combining 2 hospitals). Country registration of sites was: England 176, Northern Ireland 10, Scotland 22, Wales 15 and the Islands 2 (States of Guernsey HSS & Isle of Mann DHSS). The total number of sites involved in entering data was 200, comprising data from 212 hospitals- a 75% response overall from the 281 applicable acute hospitals initially invited to participate. The data were entered between 4th September and 31st December 2006.
Each participating site was provided with an appropriate login and password and help booklets. A telephone and email helpdesk was provided by the CEEu, RCP to answer any individual queries.
The audit of the site organisation of IBD services was at 1st June 2006. Some questions related to discharges and operations during the 12 month period from 1st June 2005 to 31st May 2006. In total, organisational audit data was received for 181 sites.

UK IBD Audit 2006 Report
17
For individual patient care, the case-notes were audited of 40 consecutive inpatients (20 Crohn’s Disease and 20 Ulcerative Colitis) admitted from 1st June 2006 working backwards as far as 1st June 2004 if necessary to identify the 40. This enabled outcome data to be collected for at least 3 months after the admission before the data entry period commenced in September 2006. Case identification was based on discharge diagnosis as this defined the standards a clinical team expects to be assessed against. A recent study3 showed that a large District General Hospital serving a population of 330,000 admitted 35 patients with Ulcerative Colitis and 31 patients with Crohn’s Disease over a 6 months period so the target numbers were expected to be readily achievable for most NHS Trusts. In total, data were collected for 2767 Ulcerative Colitis patients (from 180 sites), median (IQR) of 19 (11-20) per site, range.1-24 In total, data were collected for 2914 Crohn’s Disease patients (from 185 sites), median (IQR) of 19 (12-20) per site, range 2-24. Selection criteria for the patient cohorts (ICD-10 codes) For the Crohn’s Disease and Ulcerative Colitis clinical audits, case identification was based on the discharge diagnosis using the following relevant ICD codes:-
• Crohn’s Disease K50.0 (small intestine), K50.1 (large intestine), K50.8 (other), K50.9 (unspecified).
• Ulcerative Colitis K51.0 (enterocolitis), K51.1 (ileocolitis), K51.2 (proctitis), K51.3 (rectosigmoiditis), K51.4 (pseudopolyposis of colon), K51.5 (mucosal proctocolitis), K51.8 (other), K51.9 (unspecified)
A patient was to be included in the clinical audit only once, this being for the most recent admission prior to 1st June 2006. For the Organisational audit multiple admissions were to be counted for discharges and operations during the year prior to 1st June 2006. Patients were to be included in the audit if the primary reason for admission was because of IBD or symptoms that were later diagnosed as IBD and excluded if IBD was not indicated as the main reason e.g. a person with known IBD admitted because of a myocardial infarction. Day cases were to be excluded, such as for endoscopy or drug infusions or if a patient was admitted for a day but stayed overnight and was discharged the following day. Patients with a diagnosis of indeterminate Colitis were also excluded as were patients under the age of 16. Data reliability Pilot audit sites were asked to enter 20 cases (10 UC and 10 Crohn’s) and re-audit 5 cases using a different auditor. For Ulcerative Colitis, duplicate data was available for 93 patients (from 22 sites); Crohn’s Disease 91 patients (from 22 sites). These limited numbers for analysis had scope only for assessing the grey areas of judgement relating to the more common events. However, the levels of agreement (where assessable) were generally good with kappa agreement statistics of 0.60 and higher dominating the results. With Ulcerative Colitis the median (IQR) kappa value was 0.87 (0.76-0.93) n=61 data items, for Crohn’s Disease 0.80 (0.66-0.88), n=85 inpatient items and 0.69 (0.50-0.84) n=19 outpatient items. Kappa levels tended to be higher for patient characteristics and medication details than for other information which required a greater degree of scrutiny of case-notes.

UK IBD Audit 2006 Report
18
Presentation of results Wherever possible the audit question numbers have been added within tables of results to facilitate reference to the actual questions in the audit proformas in Appendix 2.
• Section 1 provides a breakdown of Key National Results by country. • Section 2 gives the national summary results for the organisational audit for all of the sites
participating in this audit. • Section 3 gives the national summary results for the audit of Ulcerative Colitis inpatients. • Sections 4 & 5 give the national summary results for the audit of Crohn’s Disease inpatients and
outpatients. National results are presented as percentages for categorical data and as median and inter-quartile range (IQR) for numerical data. Site variation is also summarized by the median and IQR and in graphical form by histogram plots.

UK IBD Audit 2006 Report
19
RESULTS
Section 1. Key National Results for England, Northern Ireland, Scotland and Wales The sites that registered were, by country: England 176, Northern Ireland 10, Scotland 22,Wales 15 The number of sites entering data into the audit (Organisational and/or Ulcerative Colitis and/or Crohn’s Disease) were: England 159, Northern Ireland 10, Scotland 14, and Wales 15. Organisation and Structure: The number of sites entering data into the organisational audit were: England 145, Northern Ireland 10, Scotland 10, and Wales 14.
England
(145)
N. Ireland
(10)
Scotland
(10)
Wales
(14) 2.1 Discharges 1/6/05 -31/5/06 with primary diagnosis of Ulcerative Colitis
Median: 55, n=133
Median: 39, n=10
Median: 62, n=9
Median: 33, n=13
2.1 Discharges 1/6/05 -31/5/06 with primary diagnosis of Crohn’s Disease
Median: 65, n=133
Median: 47, n=10
Median: 78, n=9
Median: 26, n=13
2.2 Discharges 1/6/05 -31/5/06 having had operation where primary indication was Ulcerative Colitis
Median: 14, n=126
Median: 11, n=10
Median: 10, n=9
Median: 7, n=12
2.2 Discharges 1/6/05 -31/5/06 having had operation where primary indication was Crohn’s Disease
Median: 17, n=126
Median: 20, n=10
Median: 17, n=9
Median: 9, n=12
2.3 On site ileo-anal pouch surgery ? 79% (114/144) 30% (3) 50% (5) 57% (8)
If, yes, how many between 1/6/05 and 31/5/06 Median: 4, n=109
Median: 7, n=2
Median: 2, n=5
Median: 3, n=6
3.1 Dedicated gastroenterology ward? 74% (107) 30% (3) 60% (6) 43% (6)
If yes, how many beds per lavatory on the ward Median: 4.6, n=104
Median: 5.0, n=3
Median: 2.6, n=6
Median: 4.0, n=5
3.4 IBD Nurse Specialists on site? 61% (88/144) 10% (1) 60% (6) 36% (5)
5.2 Do timetabled meetings take place between the following specialties:
Gastroenterologists & Colorectal Surgeons 82% (119) 30% (3) 30% (3) 64% (9) Gastroenterologists & Radiologists 90% (131) 70% (7) 50% (5) 64% (9)
Colorectal Surgeons & Radiologists 90% (130/144) 50% (5) 70% (7) 64% (9)
6.4 How many dietetic sessions per week are dedicated to GI disorders?
Median: 2
%None: 24% (33/138)
Median: 0.5
%None: 44% (4/9)
Median: 5
%None: 22% (2/9)
Median: 2
%None: 36% (5/14)
10.4 Existing pathways for direct access to psychological support 21% (31) 30% (3) 20% (2) 0% (0)
12.1 Does your hospital offer open forums or meetings for patients with IBD? 34% (50) 10% (1) 0% (0) 21% (3)

UK IBD Audit 2006 Report
20
Ulcerative Colitis Inpatients: The number of sites entering data into the Ulcerative Colitis audit were: England 149, Northern Ireland 10, Scotland 12, and Wales 13.
England
(2302)
N. Ireland
(158)
Scotland
(134)
Wales
(167) 1.1.9 Was the patient transferred to a specialist gastroenterology ward? (NON-ELECTIVES)
a) Medical, surgical or joint 72% (1412/1964) 44% (62/141) 54% (60/112) 63% (93/147) d) Not transferred 28% (552/1964) 56% (79/141) 46% (52/112) 37% (54/147)
1.3.1 Did the patient die during admission (ALL PATIENTS) 1.8% (42/2302) 0.6% (1/158) 0% (0/134) 1.2% (2/167)
2.2.5 Stool sample sent for Standard Stool Culture (NON-ELECTIVES) 60% (1172/1962) 57% (80/141) 46% (51/112) 57% (84/147)
2.2.6 Stool sample sent for CDT? (NON-ELECTIVES)
47% (922/1962) 47% (66/141) 36% (40/112) 50% (74/147)
2.3.3 Biopsies taken for histology at endoscopy (NON-ELECTIVES)
78% (775/995) 80% (56/70) 77% (50/65) 70% (57/81)
Days after admission that histology reports approved by histology: Median: 9 days Median: 6 days Median: 7 days Median: 9 days
3.1.1 Patient given Prophylactic heparin (ALL PATIENTS)
61% (1415/2302) 44% (69/158) 52% (70/134) 58% (97/167)
3.1.9 (high CRP) and 4.1.4 (high stool frequency) after 3 days for high dose steroids % with surgery 41% (73/178) 40% (4/10) 38% (3/8) 64% (7/11)
% with ciclosporin 27% (48/178) 10% (1/10) 25% (2/8) 27% (3/11) % with anti-TNF therapy 4% (7/178) 10% (1/10) 13% (1/8) 0% (0/11)
5.1.2 Who made the decision to operate? (ELECTIVES with surgery)
a) Consultant Colorectal Surgeon 80% (260) 65% (11) 91% (20) 65% (13) b) Consultant GI Surgeon (non-colorectal) 0.6% (2) - - - - - -
c) Consultant General Surgeon 0.6% (2) 12% (2) - - 5% (1) d) Other Consultant Surgeon 0.3% (1) - - - - - -
e) Specialist Registrar 3% (9) 6% (1) - - 5% (1) f) *Other (please specify) 3% (10) - - - - 5% (1)
Not documented 16% (54) 18% (3) 9% (2) 20% (4) 5.1.2 Who made the decision to operate? (NON-ELECTIVES with surgery)
a) Consultant Colorectal Surgeon 84% (207) 80% (16) 73% (16) 69% (20) b) Consultant GI Surgeon (non-colorectal) 4% (10) 10% (2) 5% (1) 3% (1)
c) Consultant General Surgeon 4% (11) 10% (2) 14% (3) 14% (4) d) Other Consultant Surgeon 0.8% (2) - - - - - -
e) Specialist Registrar 4% (9) - - - - - - f) *Other (please specify) 0.4% (1) - - - - 3% (1)
Not documented 3% (7) - - 9% (2) 10% (3)
UK IBD Audit 2006 Report
21
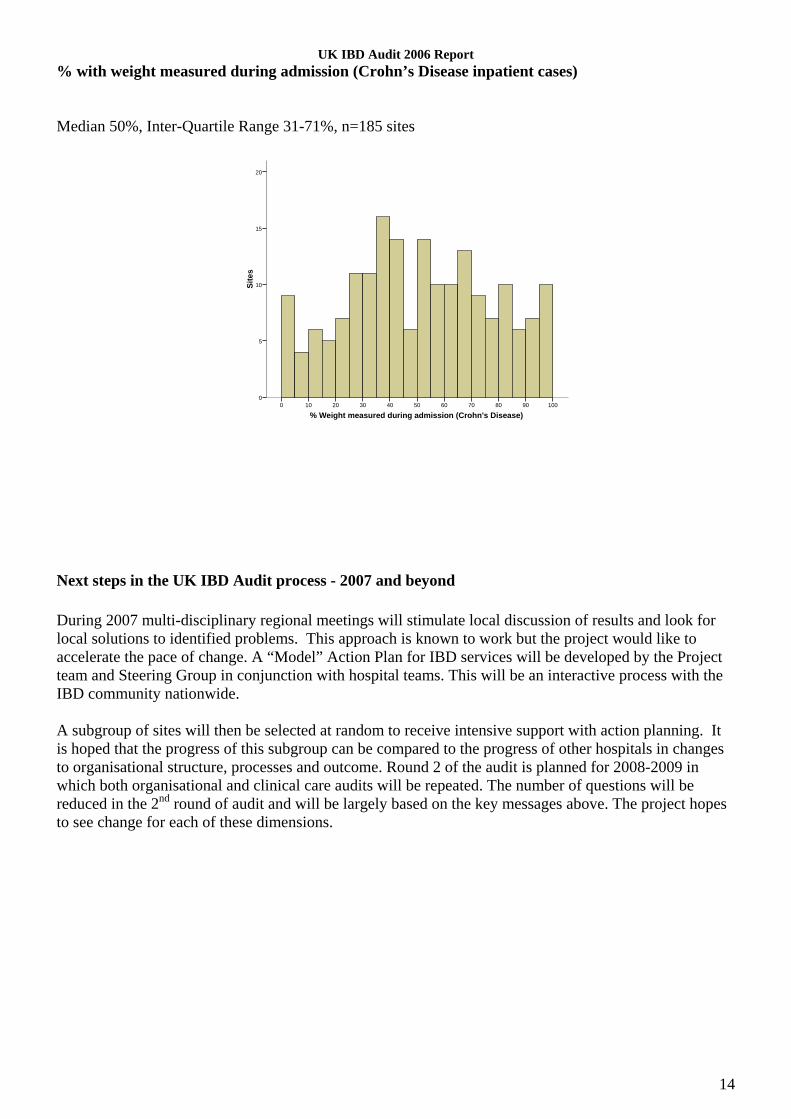
Crohn’s Disease (inpatients & outpatients): The number of sites entering data into the Crohn’s Disease audit were: England 149, Northern Ireland 10, Scotland 12, and Wales 13. England
(2384)
N. Ireland
(159)
Scotland
(169)
Wales
(194) 1.6.1 Smoking status (ALL PATIENTS)
a) Current smoker 30% (715) 38% (61) 38% (65) 35% (68) b) Lifelong non-smoker/ ex-smoker 55% (1307) 47% (74) 52% (88) 52% (101)
c) Not documented 15% (362) 15% (24) 9% (16) 13% (25) 2.2.1 Stool sample sent for Standard Stool Culture (NON-ELECTIVES with diarrhoea (2.1.1))
48% (474/995) 49% (35/71) 49% (45/92) 47% (39/83)
2.2.2 Stool sample sent for CDT (NON-ELECTIVES with diarrhoea (2.1.1)) 36% (355/992) 41% (29/71) 35% (32/92) 39% (33/84)
2.5.1 Patient weight measured during admission (NON-ELECTIVES)
52% (990/1907) 53% (70/133) 51% (76/148) 53% (86/162)
BMI measured 31% (307/990) 34% (24/70) 34% (26/76) 22% (19/86)
2.5.2 Did a dietitian visit the patient? 36% (696/1907) 38% (50/133) 41% (61/148) 39% (63/162) 2.6.1 Patient given Prophylactic heparin 63% (1506) 57% (90) 52% (88) 66% (128) 3.3.2 Evidence of chest x-ray performed in 3 months before anti-TNF- therapy? (NON-ELECTIVES with antiTNF therapy (3.3.1))
72% (68/95) 78% (7/9) 50% (5/10) 67% (4/6)
4.1.3 Which Surgeon made the decision to operate? ( ELECTIVES with surgery)
a) Consultant Colorectal Surgeon 78% (366) 60% (15) 48% (10) 65% (20) b) Consultant GI Surgeon (non-colorectal) 2% (11) - - 10% (2) 3% (1)
c) Consultant General Surgeon 2% (11) 8% (2) 14% (3) 6% (2) d) Other Consultant Surgeon - - - - - - - -
e) Specialist Registrar 2% (10) - - - - 3% (1) f) Other (please specify)* 2% (9) - - - - 3% (1)
Not documented 13% (63) 32% (8) 29% (6) 19% (6) 4.1.3 Which Surgeon made the decision to operate? (NON-ELECTIVES with surgery)
a) Consultant Colorectal Surgeon 68% (297) 50% (10) 71% (25) 66% (35) b) Consultant GI Surgeon (non-colorectal) 7% (31) 20% (4) 6% (2) 6% (3)
c) Consultant General Surgeon 8% (36) 20% (4) 17% (6) 11% (6) d) Other Consultant Surgeon 1% (5) - - - - 2% (1)
e) Specialist Registrar 10% (44) - - 3% (1) 4% (2) f) Other (please specify)* 2% (9) 5% (1) - - 6% (3)
Not documented 3% (13) 5% (1) 3% (1) 6% (3) 4.1.9i Surgery done laparoscopically/ laparoscopically-assisted? (ELECTIVES with surgery)
14% (62/450) 10% (2/21) 5% (1/21) 0% (0/29)
4.1.9i Surgery done laparoscopically/ laparoscopically-assisted? (NON-ELECTIVES with surgery)
8% (32/409) 31% (5/16) 3% (1/35) 2% (1/43)
4.3.1 Patient prescribed any of the following drugs on discharge (ELECTIVES with segmental or extended colectomy, subtotal colectomy, Ileal / Jejunal resection, or Ileocolonic resection surgery)
a) Azathioprine 21% (69/334) 29% (4/14) 14% (2/14) 21% (5/24) b) Mercaptopurine 2% (6/334) - (0/14) 7% (1/14) - (0/24)
c) Metronidazole 7% (25/334) - (0/14) - (0/14) 4% (1/24) d) 5-ASA 35% (117/334) 86% (12/14) 21% (3/14) 21% (5/24)
e) Methotrexate 1% (5/334) - (0/14) - (0/14) 4% (1/24) f) None 46% (155/334) 14% (2/14) 57% (8/14) 54% (13/24)

UK IBD Audit 2006 Report
22
England
(2384)
N. Ireland
(159)
Scotland
(169)
Wales
(194) 4.3.1 Patient prescribed any of the following drugs on discharge (NON-ELECTIVES with segmentmental extended colectomy, subtotal colectoy, Ileal / Jejunal resection, or Ileocolonic resection surgery)
a) Azathioprine 15% (50/325) 14% (2/14) 21% (6/29) 15% (6/41) b) Mercaptopurine 2% (5/325) - (0/14) - (0/29) - (0/41)
c) Metronidazole 8% (25/325) - (0/14) - (0/29) 2% (1/41) d) 5-ASA 27% (87/325) 50% (7/14) 28% (8/29) 22% (9/41)
e) Methotrexate 2% (6/335) - (0/14) - (0/29) 2% (1/41) f) None 56% (181/325) 50% (7/14) 59% (17/29) 63% (26/41)
6.4.3 How often was WBC monitoring performed? (LAST OPD before admission (6.1.1), if WBC routinely measured (6.4.2) and on Azathioprine, mercaptopurine or Methotrexate in 12 months before admission (6.4.1))
At least once a month 38% (238/625) 41% (11/27) 42% (19/45) 24% (11/46) Every 2-3 months 53% (33/625) 44% (12/27) 44% (20/45) 63% (29/46)
Less frequently 1% (8/625) - (0/27) 2% (1/45) 2% (1/46) Not documented/unable to interpret 8% (48/625) 15% (4/27) 11% (5/45) 11% (5/46)
6.5.1 Patient taking oral corticosteroids for Crohn’s Disease in 12 months before admission? ( LAST OPD (6.1.1))
56% (866/1544) 54% (49/91) 53% (54/102) 62% (77/125)
6.5.2 Any point at which patient taking oral corticosteroids continuously for more than three months (LAST OPD (6.1.1))
45% (390/866) 47% (23/49) 46% (25/54) 60% (46/77)
6.5.3 Bone protection agents prescribed alongside corticosteroids? (LAST OPD (6.1.1))
46% (398/866) 49% (24/49) 26% (14/54) 51% (39/77)
6.5.4 Bone densitometry measured within 12 months of initiation of corticosteroid therapy? (LAST OPD (6.1.1))
18% (160/866) 8% (4/49) 17% (9/54) 14% (11/77)
6.5.3 Bone protection agents prescribed alongside corticosteroids for those taking oral corticosteroids continuously for more than 3 months (6.5.2). (LAST OPD (6.1.1))
55% (214/390) 61% (14/23) 40% (10/25) 59% (27/46)

UK IBD Audit 2006 Report
23
Section 2. Organisation & Structure of IBD services as at 1st June 2006
Auditor Discipline
National (181 sites)
Consultant 78% (142) Other medical staff 15% (28)
Nurse 22% (39) Audit staff 13% (24)
Other* 6% (11)
* Other included SPR (3), Dietician (2), medical student (2), database manager, general manager, information staff, medical secretary. General Hospital Demographics Standard: Hospitals where surgery is performed for IBD should have ITU beds with 24 hr care by anaesthetists/intensivists on-site. National
(181 sites) 1.1 How many beds does your hospital have in total? Median (IQR) 540 (396-798), n=177 1.2 Does your hospital have either of the following? Acute medicine unit 98% (178) Acute surgical unit 77% (138/180) 1.3 Is there an Intensive Therapy Unit (ITU) on site? % YES 71% (128)
If yes, how many beds Median (IQR) 7 (6-10), n=126 1.4 Is there a High Dependency Unit (HDU) on site? % YES 66% (120)
If yes, is it: a) Medical 8% (9/118) b) Surgical 14% (16/118) c) Mixed 79% (93/118)
If yes, how many beds Median (IQR) 6 (4-9), n=119 1.5 Is there a combined Intensive Therapy (ITU) & High Dependency (HDU) Unit on site? % YES 25% (45)
If yes, is it: a) Medical 2% (1) b) Surgical 0% (0) c) Mixed 98% (44)
If yes, how many beds Median (IQR) 10 (8-16), n=45 There were 4 sites that did not have ITU nor HDU beds on site – these were the 4 smallest hospitals in the audit.

UK IBD Audit 2006 Report
24
Inpatient Activity Standard: 2.3 Patients undergoing surgery for ulcerative colitis should have the opportunity to have ileo-anal pouch surgery either locally (BSG Guidelines), if available, or at a regional centre. National
(181 sites) 2.1 How many patients were discharged between 1st June 2005 and 31st May 2006 with a primary diagnosis of Ulcerative Colitis
Median (IQR) Range
50 (25-105), n=167 1-481
2.1 How many patients were discharged between 1st June 2005 and 31st May 2006 with a primary diagnosis of Crohn’s Disease
Median (IQR) Range
61 (30-112), n=167 2-609
2.2 How many patients were discharged between 1st June 2005 and 31st May 2006 having had an operation where the primary indication was Ulcerative Colitis
Median (IQR) 11 (5-30), n=159
2.2 How many patients were discharged between 1st June 2005 and 31st May 2006 having had an operation where the primary indication was Crohn's Disease
Median (IQR) 16 (9-40), n=159
2.3 Do surgeons perform ileo-anal pouch surgery on site? % YES 72% (130/180) If yes, how many ileo-anal pouch operations were performed between 1st June 2005 and 31st May 2006? Median (IQR) 4 (2-7), n=122
Gastroenterology Services Standards: 3.1 Specialty triage of emergency admitted IBD patients to appropriate medical or surgical gastroenterology. 3.2 No more than 3 patients per lavatory. 3.3 At least 2 WTE Medical Gastroenterologists. 3.4 & 3.5 At least 1 IBD specialist nurse with at least 5 sessions dedicated to IBD. National
(181 sites) 3.1 Is there a dedicated Gastroenterology ward? % YES 67% (122) If yes, how many beds per lavatory on the ward Median (IQR) 4.5 (3.0-6.0), n=118
3.2 How many WTE Gastroenterologists are there on site? Median (IQR) 3 (2-4), range 1-9, n=181
3.3 How many Gastroenterology staff of the following grades are there on site?
i. Specialist Registrar (SpR) Median (IQR) 2 (1-2), n=180, 12% (21) NONE
ii. Associate Specialist Median (IQR) 0 (0-1), n=179 69% (124) NONE
3.4 How many IBD Nurse Specialists are there on site? Median (IQR) 1 (0-1), n=180 44% (80) NONE
3.5 How many sessions of Specialist Nurse time are dedicated to IBD care per week? Median (IQR) 6 (4-10), n=90/100
Range 1-50 In only 25% (30/118) of sites with a dedicated gastroenterology ward was there 3.0 or fewer beds per lavatory. In 26% (31/118) there was 6.0 or more beds per lavatory. The histogram of beds per lavatory is as follows:

UK IBD Audit 2006 Report
25
Site variation histogram: Beds per lavatory on the ward. Note that two outliers have been excluded from the histogram
Gastroenterology Beds Per Lavatory14.012.010.08.06.04.02.00.0
Site
s
25
20
15
10
5
0
Site variation histogram: Number of IBD specialist nurse sessions. Note that one outlier has been excluded from the histogram
Sessions of Specialist Nurse time dedicated to IBD care per week2520151050
Site
s
90
80
70
60
50
40
30
20
10
0

UK IBD Audit 2006 Report
26
Colorectal Services Standards: 4.1 At least 2 FTE Colorectal surgeons. 4.3 & 4.4 At least 1 stoma-care nurse specialist with at least 5 sessions dedicated to stoma care. National
(181 sites) 4.1 How many WTE specialist Colorectal Surgeons are there on site? Median (IQR) 3 (2-4), n=178
5% (9) NONE 4.2 How many Colorectal staff of the following grades are there on site?
i. Specialist Registrar (SpR) Median (IQR) 2 (1-2), n=177 12% (22) NONE
ii. Associate Specialist Median (IQR) 0 (0-1), n=176 61% (107) NONE
4.3 How many Stoma Nurses are there on site? Median (IQR) 2 (1-3), n=177 4% (8) NONE
4.4 How many sessions of Stoma Nurse time are dedicated to stoma care per week? Median (IQR) 10 (7-20), n=132/169
Range 1-85 Multi-Disciplinary Working Standards: 5.1 Sites should have a searchable data-base to allow adequate audit. 5.2 A weekly multi-disciplinary meeting should take place between gastroenterologists, colorectal surgeons and radiologists. There should be regular histopathology conferences (at least 1 per month). 5.3 & 5.4 Each hospital should have a radiologist and pathologist with a special interest in gastroenterology. National
(181 sites) 5.1 Is there a searchable database of IBD patients on site? % YES 34% (62/180) 5.2 Do timetabled meetings take place between the following specialties:
i. Gastroenterologists and Colorectal Surgeons % YES 74% (134) ii. Gastroenterologists and Pathologists % YES 78% (142)
iii. Gastroenterologists and Radiologists % YES 85% (153) iv. Colorectal Surgeons and Pathologists % YES 77% (139/180) v. Colorectal Surgeons and Radiologists % YES 84% (152/180)
5.3 Is there a specialist GI Pathologist? % YES 67% (122) 5.4 Is there a specialist GI Radiologist? % YES 71% (129)
UK IBD Audit 2006 Report
27
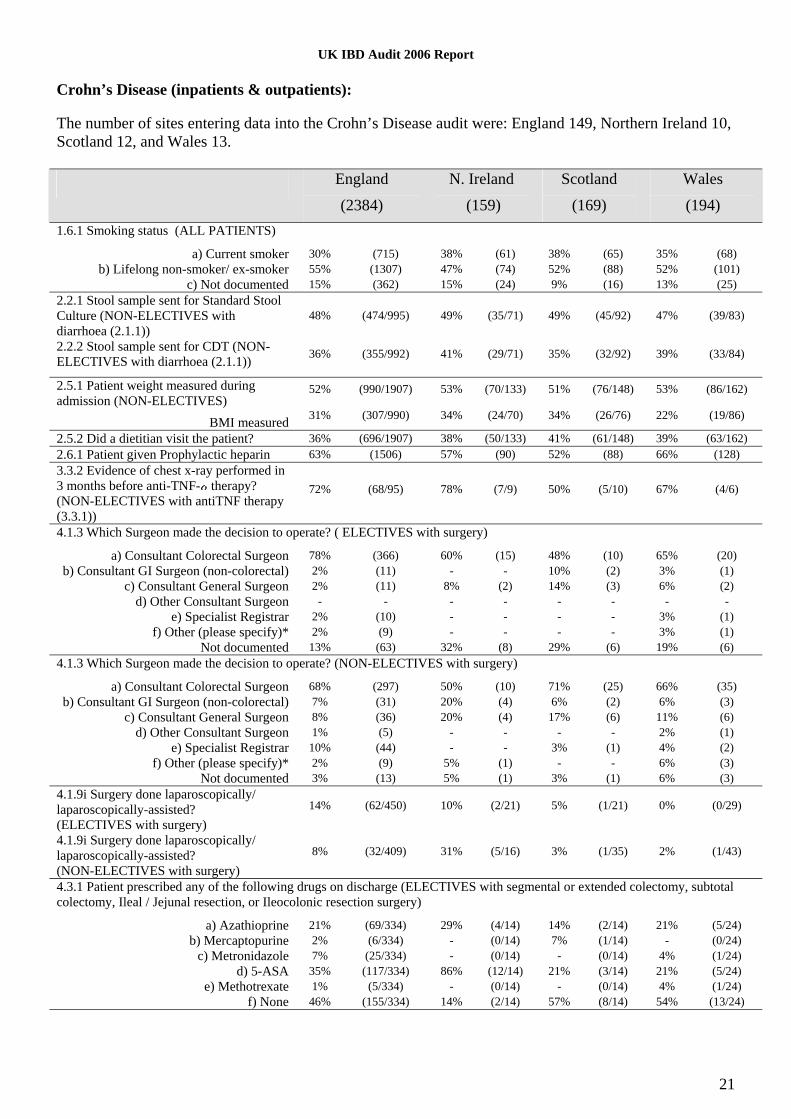
Dietetics and Nutritional Services Standards: 6.1-6.3 Each site should have a multidisciplinary nutrition team. This team should conduct ward rounds at least twice a week. 6.4 At least 5 dietetic sessions per week should be dedicated to gastroenterological diseases ( includes inpatients and outpatients). National
(181 sites) 6.1 Is there a hospital nutrition team? % YES 62% (112) 6.2 Is it a multi-disciplinary team? % YES 94% (105/112) 6.3 Does the team go on ward rounds? % YES 79% (88/112)
If yes, how frequently? %Daily 32% (28/88) 6.4 How many dietetic sessions per week are dedicated to GI disorders? Median (IQR) 2 (0-5), n=171
Site variation histogram: Number of sessions of dietetic support
Dietetic sessions per week dedicated to GI disorders2520151050
Site
s
60
50
40
30
20
10
0
UK IBD Audit 2006 Report
28
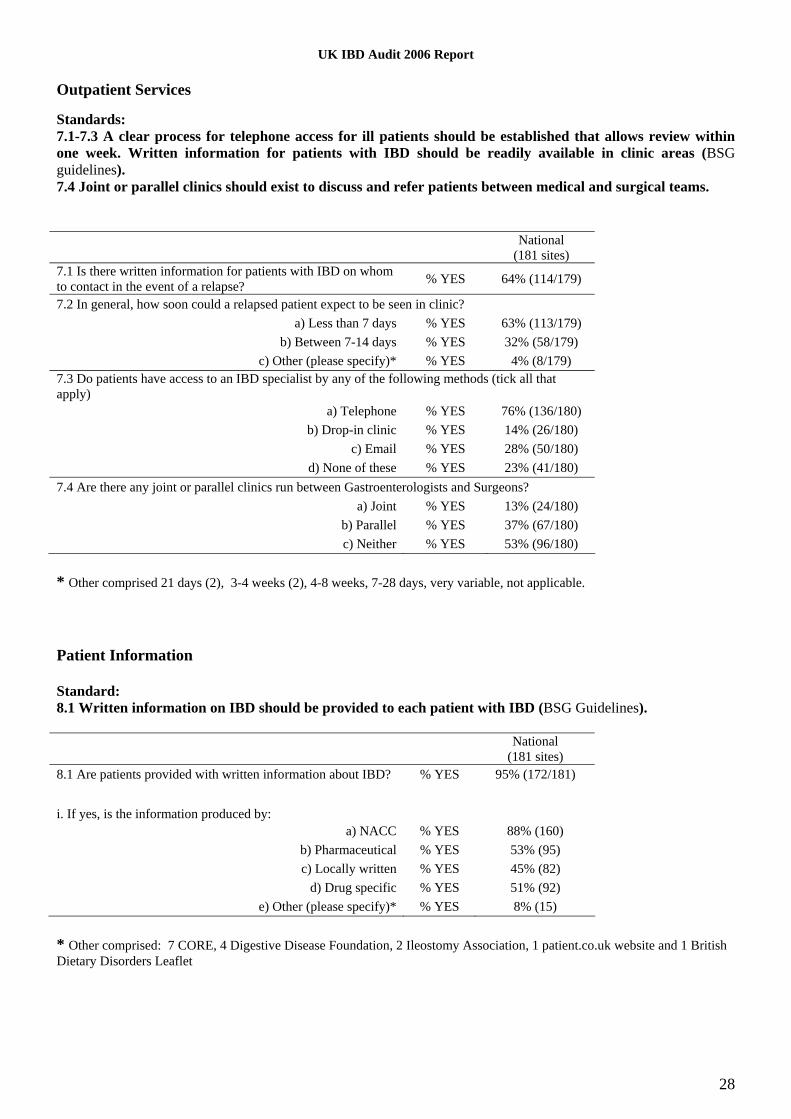
Outpatient Services Standards: 7.1-7.3 A clear process for telephone access for ill patients should be established that allows review within one week. Written information for patients with IBD should be readily available in clinic areas (BSG guidelines). 7.4 Joint or parallel clinics should exist to discuss and refer patients between medical and surgical teams. National
(181 sites) 7.1 Is there written information for patients with IBD on whom to contact in the event of a relapse? % YES 64% (114/179)
7.2 In general, how soon could a relapsed patient expect to be seen in clinic? a) Less than 7 days % YES 63% (113/179)
b) Between 7-14 days % YES 32% (58/179) c) Other (please specify)* % YES 4% (8/179)
7.3 Do patients have access to an IBD specialist by any of the following methods (tick all that apply)
a) Telephone % YES 76% (136/180) b) Drop-in clinic % YES 14% (26/180)
c) Email % YES 28% (50/180) d) None of these % YES 23% (41/180)
7.4 Are there any joint or parallel clinics run between Gastroenterologists and Surgeons? a) Joint % YES 13% (24/180)
b) Parallel % YES 37% (67/180) c) Neither % YES 53% (96/180)
* Other comprised 21 days (2), 3-4 weeks (2), 4-8 weeks, 7-28 days, very variable, not applicable. Patient Information Standard: 8.1 Written information on IBD should be provided to each patient with IBD (BSG Guidelines). National
(181 sites) 8.1 Are patients provided with written information about IBD? % YES 95% (172/181) i. If yes, is the information produced by:
a) NACC % YES 88% (160) b) Pharmaceutical % YES 53% (95) c) Locally written % YES 45% (82)
d) Drug specific % YES 51% (92) e) Other (please specify)* % YES 8% (15)
* Other comprised: 7 CORE, 4 Digestive Disease Foundation, 2 Ileostomy Association, 1 patient.co.uk website and 1 British Dietary Disorders Leaflet

UK IBD Audit 2006 Report
29
Monitoring of established immunosuppresive therapy Standard: 9.1 There should be a written policy for the mechanism of monitoring immunosuppressive therapy (National Patient Safety Agency) National
(181 sites) 9.1 How is established immunosuppresive therapy monitored? (Please tick all that apply)
a) By the GP % YES 24% (43) b) A dedicated monitoring service % YES 20% (36)
c) During clinic visits % YES 49% (88) d) A combination of primary and secondary care monitoring % YES 72% (131)
IBD Support Services Standard: 10.1 There should be regular (usually 1 or 2 per year) transition clinics involving paediatricians and adult gastroenterologists for hand over of patients to adult services. These can be done on a regional basis. National
(181 sites) 10.1 Is there a paediatric to adult handover clinic for young patients with IBD? % YES 23% (42/180) 10.2 Is a registered counsellor available to patients as part of your IBD Service? % YES 5% (9/179) 10.3 Are there any psychologists attached to the Gastroenterology service? % YES 7% (12/179)
If yes, how many sessions per month are dedicated to Gastroenterology service? Median (IQR) 4, (1-7), n=12 10.4 Do pathways exist for direct access to psychological support? % YES 21% (37/179) 10.5 Is there an acute pain management team on site? % YES 92% (166) Management of Ulcerative Colitis Standard: Written Trust guidelines should exist for the management of acute or severe colitis. National
(181 sites) 11.1 Do written trust guidelines exist for the management of acute or severe colitis? % YES 47% (84/180)
UK IBD Audit 2006 Report
30
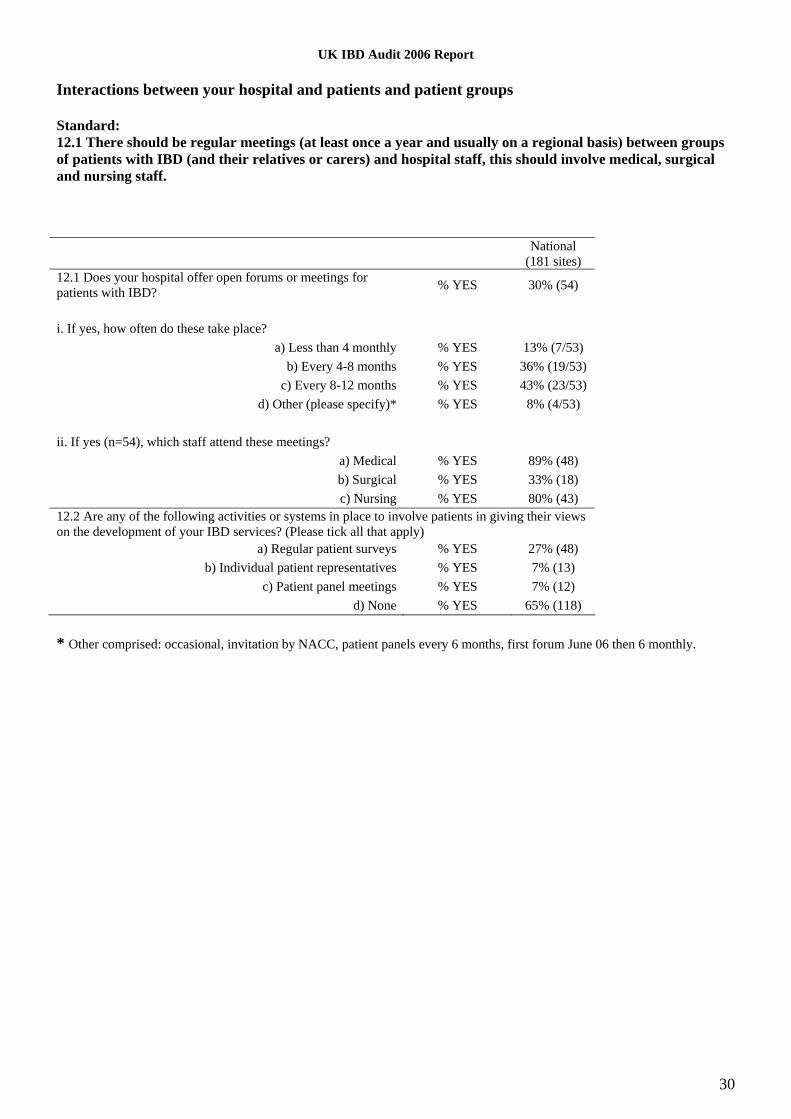
Interactions between your hospital and patients and patient groups Standard: 12.1 There should be regular meetings (at least once a year and usually on a regional basis) between groups of patients with IBD (and their relatives or carers) and hospital staff, this should involve medical, surgical and nursing staff. National
(181 sites) 12.1 Does your hospital offer open forums or meetings for patients with IBD? % YES 30% (54)
i. If yes, how often do these take place?
a) Less than 4 monthly % YES 13% (7/53) b) Every 4-8 months % YES 36% (19/53)
c) Every 8-12 months % YES 43% (23/53) d) Other (please specify)* % YES 8% (4/53)
ii. If yes (n=54), which staff attend these meetings?
a) Medical % YES 89% (48) b) Surgical % YES 33% (18) c) Nursing % YES 80% (43)
12.2 Are any of the following activities or systems in place to involve patients in giving their views on the development of your IBD services? (Please tick all that apply)
a) Regular patient surveys % YES 27% (48) b) Individual patient representatives % YES 7% (13)
c) Patient panel meetings % YES 7% (12) d) None % YES 65% (118)
* Other comprised: occasional, invitation by NACC, patient panels every 6 months, first forum June 06 then 6 monthly.

UK IBD Audit 2006 Report
31
Section 3. Clinical Audit Ulcerative Colitis (inpatient) In total, data were collected for 2767 Ulcerative Colitis patients (from 185 sites), median (IQR) of 19 (11-20) per site, range.1-24. Your site - cases. Auditor Discipline:
National (2767) % N Consultant 23 632 Other medical staff 42 1152 Nurse 28 778 Manager 0.5 15 Other (please specify)* 11 293 * Other included Clinical audit/effectiveness (158), medical student (51), SHO/SPR (36), medical secretary (21), specialist nurse (10), Patient Demographics National (2767) Median IQR Patient age* (years) 43 30-61 Derived from year of birth and year of admission
National (2767) Gender % N
Male 53 1458 Female 47 1309
When were patients admitted? 79% (2194/2767) of cases audited were admitted in the 12 month period prior to 1st June 2006. 95% (2638/2767) of cases audited were admitted in the 24 month period prior to 1st June 2006. Admission 2004 2005 2006 January 4 35 239 February 4 34 230 March 3 45 263 April 6 63 255 May 6 83 237 June 17 112 33 July 19 117 16 August 34 106 16 September 23 128 10 October 26 162 9 November 39 171 2 December 26 174 1 There were also 11 cases from 2003, 2 from 2002 and 6 from 2001 included in the audit.

UK IBD Audit 2006 Report
32
Admission Standards: 1.1.5 Patients should be transferred to the care of a medical gastroenterologist or colorectal surgeon within 24 hours of admission. 1.1.6 Patients should be seen by a consultant gastroenterologist or colorectal surgeon within 3 days of admission. 1.1.8 Patients should be seen by an IBD specialist nurse during admission. 1.1.9 Patients should be transferred to a specialist gastroenterology ward. National (2767)
% N 1.1.2 What was the source of admission to hospital?
a) General Practitioner (GP) 31% 845 b) Accident and Emergency (A&E) 27% 743 c) Outpatients Department (OPD) 37% 1019 d) Other hospital 1% 40 e) Not documented 4% 120
1.1.3 What was the duration of active colitis (new or relapse) precipitating this admission? a) Less than two weeks 34% 943 b) Two to three weeks 18% 485 c) Four to eight weeks 18% 496 d) More than eight weeks 20% 547 e) Not documented 11% 296
1.1.4 What was the primary reason for admission? a) Emergency admission for active Ulcerative Colitis 75% 2074 b) Planned admission for active Ulcerative Colitis 11% 296 c) Elective admission for surgery 14% 397
The rest of this table excludes 397 Elective admission, total n=2370 1.1.5 Which specialty was responsible for the patient's initial care 24 hours after admission?
a) Acute Medicine 31% 739 b) Gastroenterology 34% 808 c) Colorectal Surgery 10% 238 d) Geriatrics 1% 28 e) General Medicine 10% 234 f) General Surgery 13% 299 g) Other (please specify)* 1% 24
1.1.6 What date was the person first seen by a Consultant Gastroenterologist? Not Seen 20% 469 Not required 27% 128/469 Median (IQR) N If seen 1 (1-3) 1901
1.1.6 What date was the person first seen by a Consultant Colorectal Surgeon? Not Seen 65% 1545 Not required 54% 842/1545 Median (IQR) N If seen 2 (1-7) 825
1.1.8 Was patient visited by an IBD Nurse/GI Nurse specialist during admission? YES 22% 533 IN UNITS with a IBD Nurse (Organisational audit)** 36% 450/1243
1.1.9 Was the patient transferred to a specialist gastroenterology ward? a) Medical 51% 1215 b) Joint 5% 127 c) Surgical 12% 285 d) Not transferred 31% 743
* Other included paediatrics (11), Obs/Gynae (4), A&E, acute general surgery, HIV/GUM, infectious diseases, ITU, Renal, Rheumatology. ** Note that the organisational audit asked about IBD services as at 1st June 2006, whereas almost all of the clinical audit cases were prior to 1st June 2006. ,
UK IBD Audit 2006 Report
33
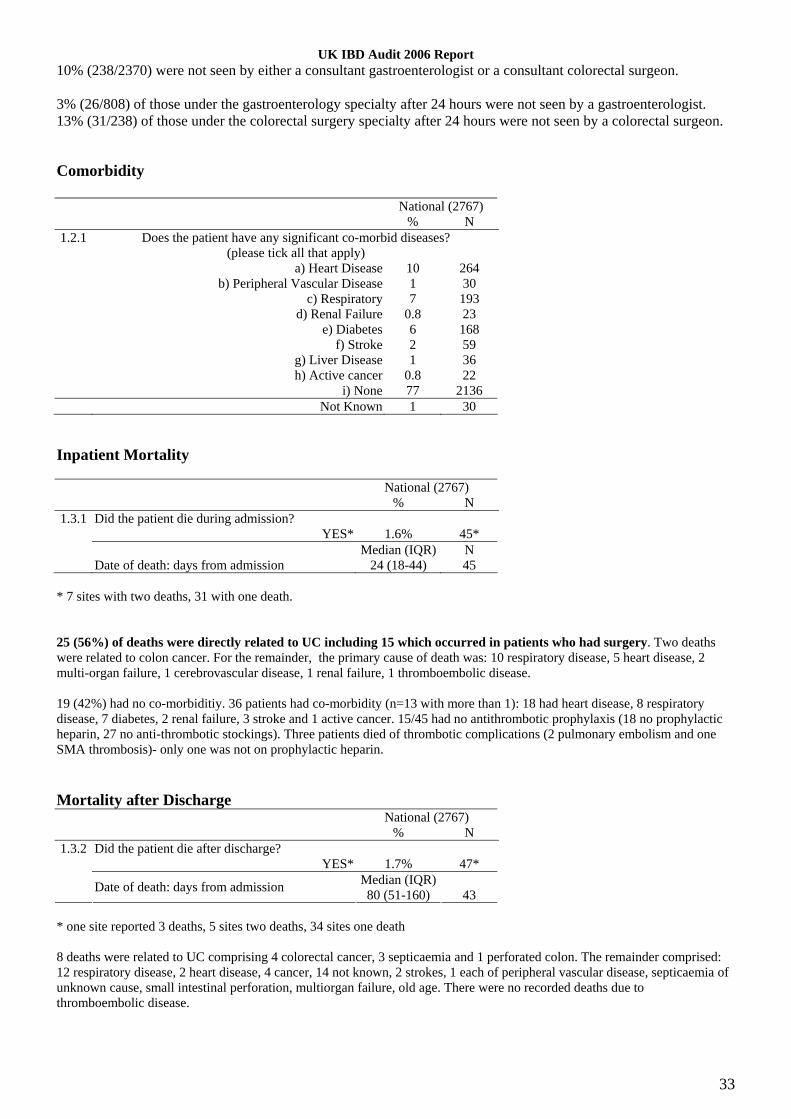
10% (238/2370) were not seen by either a consultant gastroenterologist or a consultant colorectal surgeon. 3% (26/808) of those under the gastroenterology specialty after 24 hours were not seen by a gastroenterologist. 13% (31/238) of those under the colorectal surgery specialty after 24 hours were not seen by a colorectal surgeon. Comorbidity National (2767)
% N 1.2.1 Does the patient have any significant co-morbid diseases?
(please tick all that apply) a) Heart Disease 10 264 b) Peripheral Vascular Disease 1 30 c) Respiratory 7 193 d) Renal Failure 0.8 23 e) Diabetes 6 168 f) Stroke 2 59 g) Liver Disease 1 36 h) Active cancer 0.8 22 i) None 77 2136 Not Known 1 30
Inpatient Mortality National (2767)
% N 1.3.1 Did the patient die during admission?
YES* 1.6% 45* Median (IQR) N Date of death: days from admission 24 (18-44) 45
* 7 sites with two deaths, 31 with one death. 25 (56%) of deaths were directly related to UC including 15 which occurred in patients who had surgery. Two deaths were related to colon cancer. For the remainder, the primary cause of death was: 10 respiratory disease, 5 heart disease, 2 multi-organ failure, 1 cerebrovascular disease, 1 renal failure, 1 thromboembolic disease. 19 (42%) had no co-morbiditiy. 36 patients had co-morbidity (n=13 with more than 1): 18 had heart disease, 8 respiratory disease, 7 diabetes, 2 renal failure, 3 stroke and 1 active cancer. 15/45 had no antithrombotic prophylaxis (18 no prophylactic heparin, 27 no anti-thrombotic stockings). Three patients died of thrombotic complications (2 pulmonary embolism and one SMA thrombosis)- only one was not on prophylactic heparin.
Mortality after Discharge National (2767)
% N 1.3.2 Did the patient die after discharge?
YES* 1.7% 47* Median (IQR) Date of death: days from admission 80 (51-160) 43
* one site reported 3 deaths, 5 sites two deaths, 34 sites one death 8 deaths were related to UC comprising 4 colorectal cancer, 3 septicaemia and 1 perforated colon. The remainder comprised: 12 respiratory disease, 2 heart disease, 4 cancer, 14 not known, 2 strokes, 1 each of peripheral vascular disease, septicaemia of unknown cause, small intestinal perforation, multiorgan failure, old age. There were no recorded deaths due to thromboembolic disease.

UK IBD Audit 2006 Report
34
Length of stay (Discharged) Median LOS: 8 days IQR: 5-13 days. 0-1 days: 3% (74) 0-2 days: 8% (224) 3-6 days: 26% (703) Your site: median - days.
LOS (days)1009080706050403020100
Cas
es
250
200
150
100
50
0
Assessment: Patient History National (2767)
% N 2.1.1 Did the patient have a pre-admission diagnosis of Ulcerative Colitis?
YES 83% 2303 2.1.2 Has the patient had previous admissions with Ulcerative Colitis?
YES 51% 1186/2303 Median (IQR) N
If yes, how many times in the two years prior to this admission? 1 (1-2) 1186
UK IBD Audit 2006 Report
35
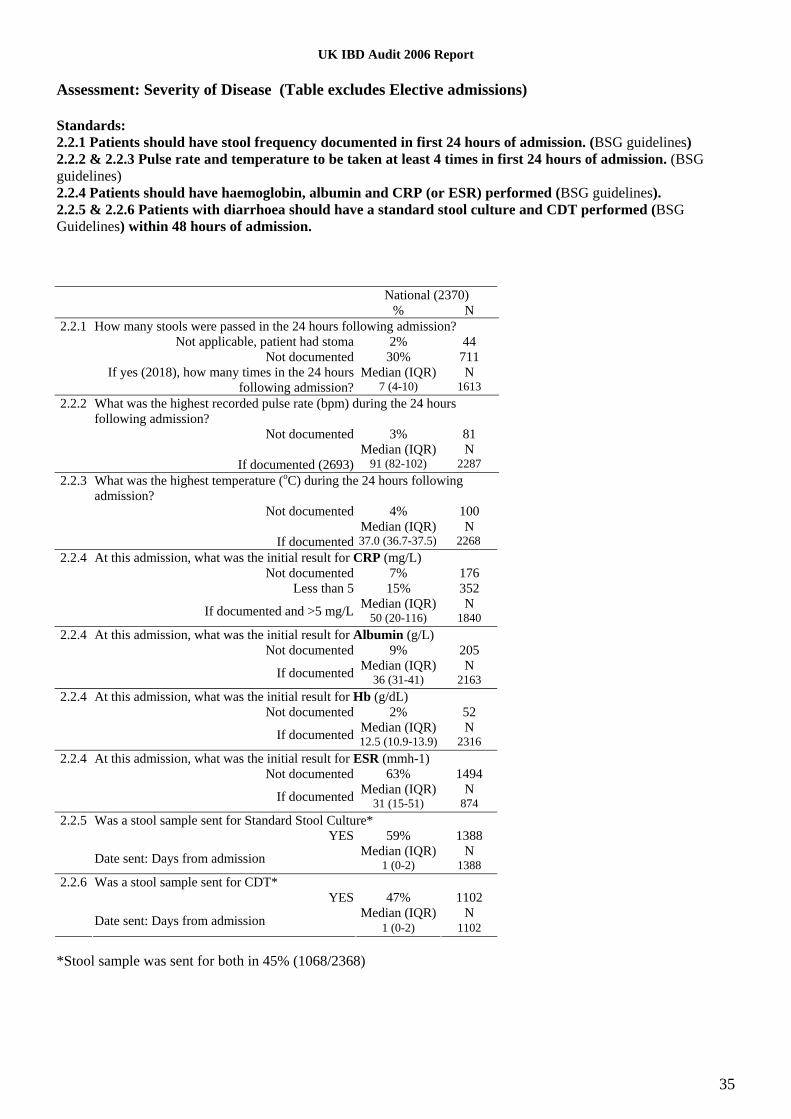
Assessment: Severity of Disease (Table excludes Elective admissions) Standards: 2.2.1 Patients should have stool frequency documented in first 24 hours of admission. (BSG guidelines) 2.2.2 & 2.2.3 Pulse rate and temperature to be taken at least 4 times in first 24 hours of admission. (BSG guidelines) 2.2.4 Patients should have haemoglobin, albumin and CRP (or ESR) performed (BSG guidelines). 2.2.5 & 2.2.6 Patients with diarrhoea should have a standard stool culture and CDT performed (BSG Guidelines) within 48 hours of admission. National (2370)
% N 2.2.1 How many stools were passed in the 24 hours following admission?
Not applicable, patient had stoma 2% 44 Not documented 30% 711 Median (IQR) N
If yes (2018), how many times in the 24 hours following admission? 7 (4-10) 1613
2.2.2 What was the highest recorded pulse rate (bpm) during the 24 hours following admission?
Not documented 3% 81 Median (IQR) N If documented (2693) 91 (82-102) 2287
2.2.3 What was the highest temperature (oC) during the 24 hours following admission?
Not documented 4% 100 Median (IQR) N If documented 37.0 (36.7-37.5) 2268
2.2.4 At this admission, what was the initial result for CRP (mg/L) Not documented 7% 176 Less than 5 15% 352 Median (IQR) N If documented and >5 mg/L 50 (20-116) 1840
2.2.4 At this admission, what was the initial result for Albumin (g/L) Not documented 9% 205 Median (IQR) N If documented 36 (31-41) 2163
2.2.4 At this admission, what was the initial result for Hb (g/dL) Not documented 2% 52 Median (IQR) N If documented 12.5 (10.9-13.9) 2316
2.2.4 At this admission, what was the initial result for ESR (mmh-1) Not documented 63% 1494 Median (IQR) N If documented 31 (15-51) 874
2.2.5 Was a stool sample sent for Standard Stool Culture* YES 59% 1388 Median (IQR) N Date sent: Days from admission 1 (0-2) 1388
2.2.6 Was a stool sample sent for CDT* YES 47% 1102 Median (IQR) N Date sent: Days from admission 1 (0-2) 1102
*Stool sample was sent for both in 45% (1068/2368)

UK IBD Audit 2006 Report
36
Assessment: Endoscopic Assessment (Table excludes Elective admissions) Standards: 2.3.1 New cases of suspected ulcerative colitis admitted to hospital should have endoscopic sigmoidoscopy confirmation within 3 days of admission. 2.3.2 Endoscopy report should contain an assessment of severity. 2.3.3 New cases of ulcerative colitis admitted to hospital should have biopsies taken for histology and these should be reported within 5 days. National (2370)
% N 2.3.1 On this admission, did patient have any of the following procedures? (Please tick all that apply)
a) Rigid sigmoidoscopy 6% 140 b) Flexible sigmoidoscopy 38% 892 c) Colonoscopy 10% 233 d) None of the above 49% 1156 Median (IQR) N Date of first procedure : days after admission 3 (1-6) 1212
2.3.2 What was the assessment of severity of inflammation (n=1212 with first procedures) a) Mild 13% 163 b) Moderate 34% 418 c) Severe 41% 499 d) Not documented 11% 132
2.3.3 Were biopsies taken for histology? 77% 939 Median (IQR) N Date histology reports approved by histology:
Days after admission* 8 (6-14) 939
*Histology reports were approved by histology: Median 5 days, IQR 2-7 days after first procedure Specifically for the 20% (464/2375) non-electives with no pre-admission diagnosis of Ulcerative Colitis: National (464)
% N 2.3.1 On this admission, did patient have any of the following procedures? (Please tick all that apply)
a) Rigid sigmoidoscopy 12% 56 b) Flexible sigmoidoscopy 67% 310 c) Colonoscopy 21% 96 d) None of the above 8% 35 Median (IQR) N Date of first procedure : days after admission 2 (1-5) 429*
* Biopsies were taken for 94% (404 of 429 with first procedures). For the 404 biopsies the median (IQR) date of histology approval was 8 days (5-13) from admission.

UK IBD Audit 2006 Report
37
Monitoring of Colitis – Post-Admission: General information Standards: 3.1.1 Patients should have prophylactic heparin (BSG guidelines). 3.1.3 & 3.1.4 Pulse rate and temperature to be monitored at least 4 times a day (BSG guidelines). 3.1.7 Stool frequency should be monitored daily (BSG guidelines). 3.1.8 & 3.1.10 ESR, or CRP should be monitored every 24–48 hours in severely active ulcerative colitis (BSG guidelines). National (2767)
% N 3.1.1 Patient given Prophylactic heparin 60% 1652 3.1.2 Patient given Anti-thrombotic stockings 29% 806
63% (1735) were given heparin or stockings, 37% (1039) were given neither The rest of this table excludes 399 Elective admission, total n = 2370
3.1.3 In the first seven days following admission, how often was the patient’s pulse monitored? a) 4 or more times per day 39% 930 b) 1-3 times per day 58% 1364 c) Less than once a day 1% 23 d) Not monitored 2% 51
3.1.4 In the first 7 days following admission did the patient have a persistent Tachycardia (Pulse rate >90bpm on more than one occasion in 24 hours)
YES 23% 523/2317 Median (IQR) N Days after admission 1 (0-2) 523
3.1.5 In the first seven days following admission, how often was temperature monitored? a) 4 or more times per day 35% 831 b) 1-3 times per day 61% 1452 c) Less than once a day 2% 36 d) Not monitored 2% 49
3.1.6 In the first 7 days following admission did the patient have a Fever (Temperature >37.5°C on more than one occasion in 24 hours)
YES 15% 350 Median (IQR) N Days after admission 1 (0-2) 350
3.1.7 In the first seven days following admission, how often was stool frequency monitored? a) Daily 71% 1687 b) Every 2-3 days 5% 108 c) Every 4-6 days 1% 17 d) Once a week 1% 22 e) Not applicable, stoma present 3% 62 f) Not documented 20% 472
3.1.8 In the first seven days following admission, how often was CRP monitored? a) Daily 24% 570 b) Every 2-3 days 48% 1136 c) Every 4-6 days 8% 184 d) Once 13% 308 e) Not documented 7% 170
3.1.9 At any point following the first 72-hours of steroid therapy was the patient’s CRP level reported to be greater than >45mg/L (N=2198 with CRP monitoring known)
YES 30% 658 No 65% 1418 Not documented 6% 122
3.1.10 In the first seven days following admission, how often was ESR monitored? a) Daily 4% 94 b) Every 2-3 days 16% 389 c) Every 4-6 days 6% 138 d) Once 17% 398 e) Not documented 57% 1349
In 6% (149/2370) there was no documentation of either CRP or ESR having been monitored.

UK IBD Audit 2006 Report
38
The above table is for all patients, who stayed differing lengths of time in hospital. A breakdown of results by time in hospital (0-2 days, 3-6 days and 7 or more days) is given below.
LOS (discharges/deaths) 0-2 days 3-6 days 7+days ALL N=219 N=654 N=1464 N=2370
3.1.3 In the first seven days following admission, how often was the patient’s pulse monitored? a) 4 or more times per day 27% 36% 42% 39% b) 1-3 times per day 67% 61% 55% 58% c) Less than once a day 2% 1% 1% 1% d) Not monitored 3% 2% 2% 2%
3.1.4 In the first 7 days following admission did the patient have a persistent Tachycardia (Pulse rate >90bpm on more than one occasion in 24 hours)
YES 15% 17% 26% 23% 3.1.5 In the first seven days following admission, how often was temperature monitored?
a) 4 or more times per day 20% 33% 38% 35% b) 1-3 times per day 72% 64% 59% 62% c) Less than once a day 4% 1% 1% 2% d) Not monitored 5% 1% 2% 2%
3.1.6 In the first 7 days following admission did the patient have a Fever (Temperature >37.5°C on more than one occasion in 24 hours)
YES 9% 11% 18% 15% 3.1.7 In the first seven days following admission, how often was stool frequency monitored?
a) Daily 50% 67% 76% 71% b) Every 2-3 days 3% 5% 5% 5% c) Every 4-6 days - 1% 1% 1% d) Once a week 2% 2% 1% 1% e) Not applicable, stoma present 3% 2% 3% 3% f) Not documented 42% 23% 15% 20%
3.1.8 In the first seven days following admission, how often was CRP monitored? a) Daily 18% 21% 26% 24% b) Every 2-3 days 21% 45% 54% 48% c) Every 4-6 days 2% 5% 10% 8% d) Once 33% 21% 7% 13% e) Not documented 27% 8% 4% 7%
3.1.9 At any point following the first 72-hours of steroid therapy was the patient’s CRP level reported to be greater than >45mg/L (N=2198 with CRP monitoring known)
YES 11% 18% 37% 30% No 79% 74% 59% 65% Not documented 10% 7% 4% 6%
3.1.10 In the first seven days following admission, how often was ESR monitored? a) Daily 4% 4% 4% 4% b) Every 2-3 days 6% 15% 18% 16% c) Every 4-6 days 1% 3% 8% 6% d) Once 16% 22% 14% 17% e) Not documented 73% 56% 55% 57%

UK IBD Audit 2006 Report
39
Monitoring of Colitis – Post-Admission: Radiology (Table excludes Elective admissions) Standards: 3.2.1 Patients should have a plain abdominal X-ray (BSG Guidelines) with 24 hours of admission. 3.2.2 If toxic megacolon is present the abdominal X-ray should be repeated the next day (BSG guidelines) if emergency surgery is not undertaken (BSG Guidelines). National (2370)
% N 3.2.1 Plain abdominal X-Ray performed 80% 1892
Date requested: Same day as admission 76% 1439 Next day after admission 12% 229 Later 12% 227 Date performed: Same day as request 90% 1696 Next day after request 8% 158 Later 2% 38 Date reported by Radiologist: Same day as X-Ray performed or next day 52% 604 2-3 days after X-Ray performed 14% 163 More than 3 days after X-Ray performed 34% 392
3.2.2 Was toxic megacolon present in the x-ray? (n=1892) NA 1% 28 YES 2% 37/1864 If yes, was a repeat x-ray performed? 70% 26/37 Median (IQR) N Days after admission 1 (1-3) 26
3.2.3 CT Scan of the abdomen performed 6% 147 Date requested: Same day as admission 16 24 Median (IQR) N 4 (1-13) 147 Date performed: Same day as request 54% 79 Next day after request 20% 29 Later 27% 39 Date reported by Radiologist: Same day as CT scan performed or next day 86% 126 2-3 days after CT scan performed 6% 9 More than 3 days after CT scan performed 8% 12
UK IBD Audit 2006 Report
40
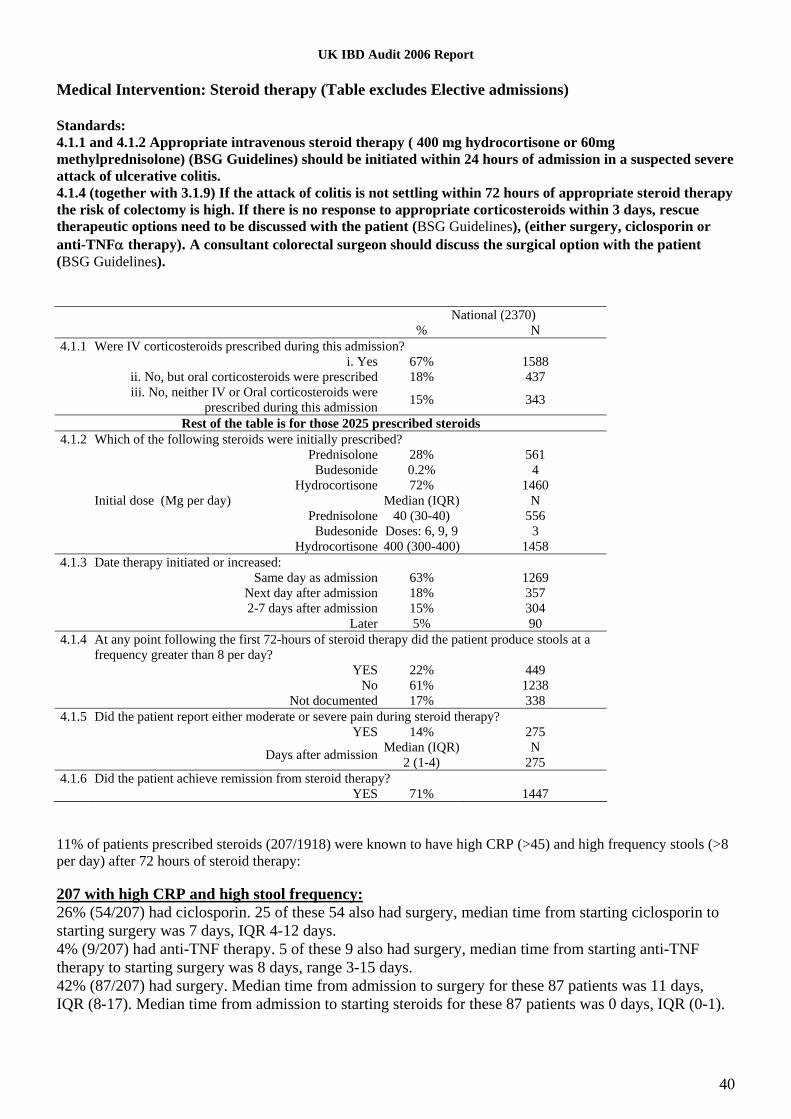
Medical Intervention: Steroid therapy (Table excludes Elective admissions) Standards: 4.1.1 and 4.1.2 Appropriate intravenous steroid therapy ( 400 mg hydrocortisone or 60mg methylprednisolone) (BSG Guidelines) should be initiated within 24 hours of admission in a suspected severe attack of ulcerative colitis. 4.1.4 (together with 3.1.9) If the attack of colitis is not settling within 72 hours of appropriate steroid therapy the risk of colectomy is high. If there is no response to appropriate corticosteroids within 3 days, rescue therapeutic options need to be discussed with the patient (BSG Guidelines), (either surgery, ciclosporin or anti-TNFα therapy). A consultant colorectal surgeon should discuss the surgical option with the patient (BSG Guidelines). National (2370)
% N 4.1.1 Were IV corticosteroids prescribed during this admission?
i. Yes 67% 1588 ii. No, but oral corticosteroids were prescribed 18% 437 iii. No, neither IV or Oral corticosteroids were
prescribed during this admission 15% 343
Rest of the table is for those 2025 prescribed steroids 4.1.2 Which of the following steroids were initially prescribed?
Prednisolone 28% 561 Budesonide 0.2% 4 Hydrocortisone 72% 1460 Initial dose (Mg per day) Median (IQR) N Prednisolone 40 (30-40) 556 Budesonide Doses: 6, 9, 9 3 Hydrocortisone 400 (300-400) 1458
4.1.3 Date therapy initiated or increased: Same day as admission 63% 1269 Next day after admission 18% 357 2-7 days after admission 15% 304 Later 5% 90
4.1.4 At any point following the first 72-hours of steroid therapy did the patient produce stools at a frequency greater than 8 per day?
YES 22% 449 No 61% 1238 Not documented 17% 338
4.1.5 Did the patient report either moderate or severe pain during steroid therapy? YES 14% 275 Median (IQR) N Days after admission 2 (1-4) 275
4.1.6 Did the patient achieve remission from steroid therapy? YES 71% 1447
11% of patients prescribed steroids (207/1918) were known to have high CRP (>45) and high frequency stools (>8 per day) after 72 hours of steroid therapy: 207 with high CRP and high stool frequency: 26% (54/207) had ciclosporin. 25 of these 54 also had surgery, median time from starting ciclosporin to starting surgery was 7 days, IQR 4-12 days. 4% (9/207) had anti-TNF therapy. 5 of these 9 also had surgery, median time from starting anti-TNF therapy to starting surgery was 8 days, range 3-15 days. 42% (87/207) had surgery. Median time from admission to surgery for these 87 patients was 11 days, IQR (8-17). Median time from admission to starting steroids for these 87 patients was 0 days, IQR (0-1).

UK IBD Audit 2006 Report
41
658 with high CRP: 14% (88/616) had ciclosporin. 40 of these 88 also had surgery, median time from starting ciclosporin to starting surgery was 7 days, IQR 3-12 days. 2% (14/616) had anti-TNF therapy. 7 of these 14 also had surgery, median time from starting anti-TNF therapy to starting surgery was 6 days, range 3-15 days. 28% (173/616) had surgery. Median time from admission to surgery for these 173 patients was 10 days, IQR (6-16). Median time from admission to starting steroids for these 173 patients was 0 days, IQR (0-1). Medical Intervention: Other Therapies (Table excludes Elective admissions) National (2370)
% N 4.2.1 Ciclosporin 6% 150
Median (IQR) N Start date: Days after admission 6 (4-10) 150 Patient achieved remission on ciclosporin therapy 55% 82
4.2.2 Anti-TNF 2% 37 Median (IQR) N Start date: Days after admission 10 (7-14) 37 Patient achieved remission on TNF therapy 54% 20
4.2.3 Clinical Trial (please specify)* 2 Start date: Days after admission 4 & 5 days Patient achieved remission from clinical trial 0% 0
4.2.4 Significant Other therapies (please specify)** 2% 42 Median (IQR) N Start date: Days after admission 3 (1-7) 42 Patient achieved remission from other therapy 50% 21
4.2.5 Surgical therapy YES 13% 318
4.2.3 *Clinical trials were: UC-CAT (1), not documented (1) 4.2.4 **Significant other therapies were: 6 Antibiotics and 2 Antivirals For n=207 with high CRP (>45) and high stool frequency (>8 per day) after 72 hours of steroid therapy having an initiation/increase data for steroids the median (IQR) time from steroid initiation to the earliest of starting either ciclosporin, anti-TNF therapy , or surgery was 8 days (5-13 days), n=119. For these patients the median (IQR) time was 6 days to starting ciclosporine, 9 days to starting anti-TNF therapy and 11 days to surgery.

UK IBD Audit 2006 Report
42
Medical Intervention: Initiating Ciclosporin Therapy (N=150) (Table excludes elective admissions) Standards: 4.3.1 Creatinine should be measured (BSG Guidelines) within the 48 hours prior to initiation of ciclosporin. 4.3.2 & 4.3.3 Magnesium and cholesterol should be measured (BSG Guidelines) within the 48 hours prior to initiation of intravenous ciclosporin. National (150)
% N 4.3.1 Pre-treatment results for Creatinine (μmol/L)
Not documented 5% 7 Median (IQR) N Results 74 (65-82) 143 Date of sample (143): 3 days or more before ciclosporin started 6% 9 2 days before ciclosporin started 8% 11 1 day before ciclosporin started 38% 55 Same day as ciclosporin started 46% 66 1-2 days after ciclosporin started 1% 2
4.3.2 Pre-treatment results for Magnesium (mEq/L) Not documented 35% 53 Median (IQR) N Results 0.9 (0.8-0.9) 97 Date of sample for intravenous ciclosporin (97): 3 days or more before ciclosporin started 12% 12 2 days before ciclosporin started 11% 11 1 day before ciclosporin started 31% 30 Same day as ciclosporin started 42% 41 1-2 days after ciclosporin started 3% 3
4.3.3 Pre-treatment results for Cholesterol (mmol/L) Not documented 47% 71 Median (IQR) N Results 3.6 (3.0-4.2) 79 Date of sample for intravenous ciclosporin (79): 3 days or more before ciclosporin started 18% 14 2 days before ciclosporin started 15% 12 1 day before ciclosporin started 24% 19 Same day as ciclosporin started 39% 31 1-2 days after ciclosporin started 4% 3
4.3.4 How was the ciclosporin initially administered? Oral 23% 35 IV 77% 115 Median (IQR) N Initial daily dose 2 (2-4) 150
When oral ciclosporin therapy was given magnesium levels were checked two or more days before therapy for 3/20, one day before for 9/20, the same day for 7/20 and the day after for 1/20. When oral ciclosporin therapy was given cholesterol levels were checked two or more days before therapy for 5/13, one day before for 5/13, the same day for 2/13 and the day after for 1/13.

UK IBD Audit 2006 Report
43
Medical Intervention: Monitoring Ciclosporin Therapy (N=150) (Table excludes Elective admissions) Standards: 4.4.1 & 4.4.2 Creatinine and FBC should be monitored daily. 4.4.3 Ciclosporin levels should be checked daily after 3 days of IV therapy. National (150)
% N 4.4.1 After Ciclosporin therapy was initiated, how often was Creatinine measured?
a) Daily 67% 100 b) Every two days 23% 35 c) Every three days 5% 8 d) Once a week 1% 2 e) Less than once a week 2% 3 f) Not documented 1% 2
4.4.2 After Ciclosporin therapy was initiated, how often was FBC (Full Blood Count) measured? a) Daily 65% 98 b) Every two days 24% 36 c) Every three days 5% 8 d) Once a week 2% 3 e) Less than once a week 2% 3 f) Not documented 1% 2
4.4.3 After three days of ciclosporin therapy, how often were serum ciclosporin levels checked? a) Daily 11% 16 b) Every two days 13% 19 c) Every three days 10% 15 d) Once a week 21% 31 e) Less than once a week 9% 14 f) Not documented 36% 55

UK IBD Audit 2006 Report
44
Surgical Interventions - 715 UC patients underwent surgery Standards: 5.1.2 Consultant colorectal surgeons should be involved with the discussion with the patient regarding the decision to operate (BSG Guidelines). 5.1.4 Patients having resectional surgery for Ulcerative Colitis should see a stoma nurse prior to the operation (BSG Guidelines). 5.1.5 & 5.1.6 Operations should be performed or assisted by a consultant colorectal surgeon. 5.1.9 ASA status should be recorded pre-operatively. Electives (397) Emergency/
Planned (318) % N % N
5.1.1 What date was the decision to operate made? Not known 16 63 4 12 Median (IQR) N Median (IQR) N Date of decision: days from admission -49 (-106 to -18) 334 7 (3-13) 306
5.1.2 Who made the decision to operate? a) Consultant Colorectal Surgeon 77% 304 81% 259 b) Consultant GI Surgeon (non-colorectal) 0.5% 2 4% 14 c) Consultant General Surgeon 1% 5 6% 20 d) Other Consultant Surgeon 0.3% 1 0.6% 2 e) Specialist Registrar 3% 11 3% 9 f) *Other (please specify) 3% 11 0.6% 2 Not documented 16% 63 4% 12
5.1.3 Median (IQR) N Median (IQR) N
Date of Surgery: days from admission 1 (1-1) 396 10 (5-15) 318
5.1.4 Patient seen by a stoma nurse during this admission 54% 213 77% 245 Median (IQR) N Median (IQR) N If yes, date first seen : days from admission 1 (0-3) 213 8 (5-15) 244
5.1.5 What was the grade of the operating surgeon? a) Consultant Colorectal Surgeon 86% 340 72% 229 b) Consultant GI Surgeon (non-colorectal) 1% 4 3% 9 c) Consultant General Surgeon 3% 10 8% 25 d) Other Consultant Surgeon 0.3% 1 0.6% 2 e) Specialist Registrar 9% 35 13% 42 f) **Other (please specify) 2% 6 3% 11
5.1.6 What was the grade of the assisting surgeon? a) Consultant Colorectal Surgeon 11% 43 7% 22 b) Consultant GI Surgeon (non-colorectal) 0.8% 3 0.6% 2 c) Consultant General Surgeon 1% 5 0.9% 3 d) Other Consultant Surgeon 2% 6 0.6% 2 e) Specialist Registrar 73% 289 66% 209 f) ***Other (please specify) 13% 50 25% 78
Consultant colorectal surgeon as either operating or assisting surgeon: Electives: 92% (363/396), Non-electives: 77% (242/316) 5.1.2 f) * Other: For elective surgery, there were 11 cases where the decision to operate was classed as ‘other’. This consisted of 1 by an Associate Specialist, 1 by Staff Grade, 1 by Senior House Officer, 1 by Consultant Gastroenterologist, 1 by Gastroenterologist and Colorectal Surgeon (grades not stated), 1 by MDT group, 1 by ‘Patient and Consultant’ (specialty not stated) and 4 by the Patient. For non-elective surgery, the decision to operate was made by a Staff Grade (2). 5.1.5 f) ** Other: The operating surgeon was indicated for elective surgery as ‘other’ for 7 cases: 1 associate specialist, 5 staff grade, and 1 not known. For non-elective surgery: 3 associate specialist, 6 staff grade and 2 Senior House Officer.

UK IBD Audit 2006 Report
45
5.1.6 f) ***Other The assisting surgeon was indicated as ‘other’ for 50 elective cases: 19 not known or not stated, 2 associate specialist, 12 staff grades, 17 F2 or Senior House Officers, 1 Senior Staff Practitioner and 1 Gynaecologist (grade not stated). For non-elective surgery 78 were indicated as ‘others’: 25 Staff Grades, 23 FY2 or Senior House officers, 7 Associate Specialists, 1 FY1, 1 Clinical Assistant and 21 not known or nor documented. Electives (397) Emergency/
Planned (318) % N % N
5.1.7 What were the indications for surgery? a) Failure of Medical Therapy 58% 229 86% 274 b) Toxic megacolon - 0 7% 22 c) Bleeding 6% 22 6% 18 d) Obstruction 2% 9 3% 8 e) High Grade Dysplasia 3% 13 0.3% 1 f) Low Grade Dysplasia 2% 8 - 0 g) Ungraded Dysplasia 2% 9 - 0 h) Cancer 1% 4 - 0 i) Perforation 0.3% 1 6% 18 j) Abscess 3% 10 0.9% 3 k) Formation of ileostomy 12% 47 2% 6 l) Other indication (please specify)* 18% 73 2% 7
5.1.8 Type of intervention: a) Subtotal colectomy 18% 73 71% 226 b) Protocolectomy 25% 101 22% 70 c) Protectomy 24% 97 1% 4 d) Ileoanal pouch with stoma 18% 71 1% 4 e) Ileoanal pouch without stoma 11% 43 0.3% 1 f) Formation of ileostomy 24% 96 44% 140 g) Other (please specify)** 11% 42 3% 9
5.1.8i Was the surgery done laparoscopically/ laparoscopically-assisted? YES 10% 37/384 5% 16/300
5.1.9 ASA status recorded pre-operatively 63% 251 66% 208 If yes, what was the status? 1 22% 56 14% 29 2 63% 159 49% 102 3 12% 31 28% 58 4 2% 4 7% 14 5 - - 1% 3 N/A 0.4% 1 1% 2
5.1.7 l) *Other comprised: 42 Ileo-anal pouch procedures, 11 Completetion Proctectomy, 2 Anal Pain, 6 Patient Choice 1 Colostomy Dysfunction, 1 Jejunostomy Closure, 1 Pouch Dysfunction 16 Not Documented 5.1.8 g) **Other comprised: 23 Ileostomy Reversals, 10 Perianal Procedures, 2 Release of adhesions, 1 Laparotomy, 1 Resection of Ileum, 1 Splenectomy, 1 Wound Exploration and 14 Unknown

UK IBD Audit 2006 Report
46
Surgical Complications Electives (397) Emergency/
Planned (318) % N % N
5.2.1 Did the patient suffer from any of these complications with their surgery? a) Wound Infection 10% 41 7% 23 b) Rectal stump complications 1% 4 1% 4 c) Intra-abdominal bleeding 1% 4 2% 7 d) Intra-abdominal sepsis 3% 12 6% 18 e) Anastomatic leakage 2% 8 1% 4 f) Stoma complications 3% 12 3% 10 g) Deep vein thrombosis (DVT) 0.5% 2 2% 5 h) Pulmonary embolus (PE) 0.3% 1 1% 4 i) Small bowel obstruction 3% 10 3% 8 j) Ileus requiring parenteral nutrition 2% 7 3% 8 k) Cardiac 0.8% 3 4% 13 l) Respiratory 4% 17 10% 31 m) Other (please specify)* 3% 11 4% 12 n) No Complications 73% 288 69% 219
5.2.1 m) *Other: For elective there were 11 complications classified as ‘other’: 2 ureteric injury, 1 ureteric obstruction, 1 acute renal failure, 1 bacteraemia (unspecified), 1 cellulitis (unspecified), 1 epidural abscess, 1 post –operative haemorrhage (unspecified), 1 pyelonephritis, 1 thrombophlebitis, 1 splenectomy (indication not stated).
For non-elective surgery there were 12 complications classified as ‘other’: 1 ureteric injury, 2 acute renal failure, 1 ‘aretic surgery’ case, 1 cellulitis (site not specified), 1 cannula related cellulitis, 2 epidural site abscess, 1 generalised seizure, 1 perforated gastric ulcer, 1 pyelonephritis, 1 sepsis (site not specified)
Discharge Arrangements Standards: 6.1.1 Patients should be followed up by a gastroenterologist or colorectal surgeon. 6.1.3 Patients discharged on oral steroids should have a steroid reduction programme stated on discharge. 6.1.4 Patients on oral steroids should be co-prescribed bone protection agents (such as calcium and vitamin D or bisphosphonates (BSG guidelines). National (2767)
% N 6.1.1 Was an appointment made for the patient to be referred back to a Gastroenterologist
YES 71% 1968 6.1.1 Was an appointment made for the patient to be referred back to a Colorectal Surgeon
YES 34% 944 6.1.2 Was the patient taking oral steroids on discharge?
YES 69% 1907 No 28% 783 N/A 3% 77
6.1.3 Was a steroid reduction programme stated on discharge (n=1907) YES 87% 1657 No 12% 225 N/A 1% 25
6.1.4 Were bone protection agents prescribed? (n=1907) YES 41% 788 No 57% 1083 N/A 2% 36

UK IBD Audit 2006 Report
47
Site variation histogram: % Bone protection prescribed Median 40%, Inter-Quartile Range 20-64%, n=179 sites
% Bone protection agents prescribed (UC)1009080706050403020100
Site
s
25
20
15
10
5
0


UK IBD Audit 2006 Report
48
Section 4. Clinical Audit: Crohn’s Disease (Inpatient) In total, data were collected for 2914 Crohn’s Disease patients (from 185 sites), median (IQR) of 19 (12-20) per site, range 2-24. Your site: - cases. Auditor Discipline:
National (2914) % N Consultant 24 686 Other medical staff 42 1228 Nurse 26 765 Manager 0.1 4 Other (please specify)* 11 313 * Other comprised: clinical audit (170), medical student (47), SpR (23), SSHO (20), Nurse specialist (15), secretary (9), PRHO (9), F1 doctor (9), staff grade doctor (5), Registrar (3), SHO (2), clinical observer (1). Patient Demographics National (2914) Median IQR N Patient age (years) 38 27-54 2914
National (2914) Gender % N Male 40 1168 Female 60 1746 When were patients admitted? 82% (2404/2914) of cases audited were admitted in the 12 month period prior to 1st June 2006. 95% (2766/2914) of cases audited were admitted in the 24 month period prior to 1st June 2006. Admission 2004 2005 2006 January 3 34 291 February 3 36 265 March 7 41 345 April 4 56 285 May 4 59 283 June 18 88 42 July 17 93 22 August 14 138 13 September 17 136 9 October 22 152 11 November 25 181 7 December 23 147 1 Also included were 12 cases from 2003, 7 from 2002 and 3 from 2001.
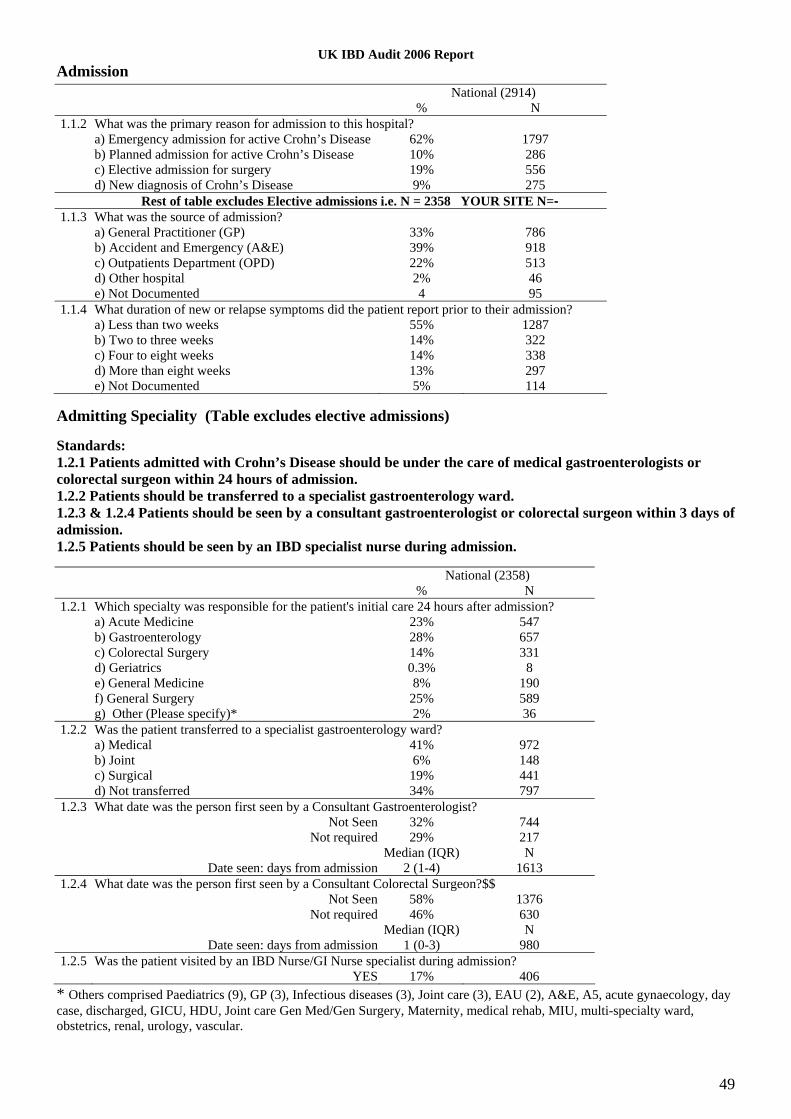
UK IBD Audit 2006 Report
49
Admission National (2914)
% N 1.1.2 What was the primary reason for admission to this hospital?
a) Emergency admission for active Crohn’s Disease 62% 1797 b) Planned admission for active Crohn’s Disease 10% 286 c) Elective admission for surgery 19% 556 d) New diagnosis of Crohn’s Disease 9% 275 Rest of table excludes Elective admissions i.e. N = 2358 YOUR SITE N=-
1.1.3 What was the source of admission? a) General Practitioner (GP) 33% 786 b) Accident and Emergency (A&E) 39% 918 c) Outpatients Department (OPD) 22% 513 d) Other hospital 2% 46 e) Not Documented 4 95
1.1.4 What duration of new or relapse symptoms did the patient report prior to their admission? a) Less than two weeks 55% 1287 b) Two to three weeks 14% 322 c) Four to eight weeks 14% 338 d) More than eight weeks 13% 297 e) Not Documented 5% 114
Admitting Speciality (Table excludes elective admissions) Standards: 1.2.1 Patients admitted with Crohn’s Disease should be under the care of medical gastroenterologists or colorectal surgeon within 24 hours of admission. 1.2.2 Patients should be transferred to a specialist gastroenterology ward. 1.2.3 & 1.2.4 Patients should be seen by a consultant gastroenterologist or colorectal surgeon within 3 days of admission. 1.2.5 Patients should be seen by an IBD specialist nurse during admission. National (2358)
% N 1.2.1 Which specialty was responsible for the patient's initial care 24 hours after admission?
a) Acute Medicine 23% 547 b) Gastroenterology 28% 657 c) Colorectal Surgery 14% 331 d) Geriatrics 0.3% 8 e) General Medicine 8% 190 f) General Surgery 25% 589 g) Other (Please specify)* 2% 36
1.2.2 Was the patient transferred to a specialist gastroenterology ward? a) Medical 41% 972 b) Joint 6% 148 c) Surgical 19% 441 d) Not transferred 34% 797
1.2.3 What date was the person first seen by a Consultant Gastroenterologist? Not Seen 32% 744 Not required 29% 217 Median (IQR) N Date seen: days from admission 2 (1-4) 1613
1.2.4 What date was the person first seen by a Consultant Colorectal Surgeon?$$ Not Seen 58% 1376 Not required 46% 630 Median (IQR) N Date seen: days from admission 1 (0-3) 980
1.2.5 Was the patient visited by an IBD Nurse/GI Nurse specialist during admission? YES 17% 406
* Others comprised Paediatrics (9), GP (3), Infectious diseases (3), Joint care (3), EAU (2), A&E, A5, acute gynaecology, day case, discharged, GICU, HDU, Joint care Gen Med/Gen Surgery, Maternity, medical rehab, MIU, multi-specialty ward, obstetrics, renal, urology, vascular.

UK IBD Audit 2006 Report
50
14% (331/2358) were not seen by either a consultant gastroenterologist or a consultant colorectal surgeon. 6% (37/657) of those under the gastroenterology specialty after 24 hours were not seen by a gastroenterologist. 7% (24/331) of those under the colorectal surgery specialty after 24 hours were not seen by a colorectal surgeon. Inpatient Mortality National (2914)
% N 1.3.1 Did the patient die during admission?
YES* 1.2% 36 Median (IQR) N Date of death: days from admission 20 (10-67) 36
*25 of the 36 deaths (69%) were judged directly related to Crohn’s Disease, including 14 patients who died after surgery for Crohn’s Disease. The remainder comprised 7 respiratory infections, 1 heart disease, 1 CDT diarrhoea, 1 ‘old age’ and 1 unknown cause of death. 12 had no co-morbidity. 24 with co-morbidity (11 had >1) consisting of 16 heart disease, 8 respiratory disease, 5 peripheral vascular disease, 2 diabetes, 2 renal failure, 2 liver disease. 10/36 had no antithrombotic prophylaxis (11 no prophylactic heparin, 22 no anti-thrombotic stockings) Mortality after Discharge National (2914)
% N 1.3.2 Did the patient die after discharge?
YES* 1.3% 36/2820 Median (IQR) Date of death: days from admission 138 (51-229) 35
*Of the 36 patients who died 13 may have been related directly to CD: 2 peritonitis, 3 colon or small bowel cancer, 2 pulmonary embolism, 2 bowel obstruction, 2 toxic megacolon, 2 ‘exacebation of Crohn’s disease’. Of the other 23 the cause of death comprised: 4 respiratory, 2 heart disease, 1 cancer, 9 not known, 2 liver disease, one each of intracerebral haemorrhage, renal failure, gastric perforation, general deterioration and tuberculous meningitis.
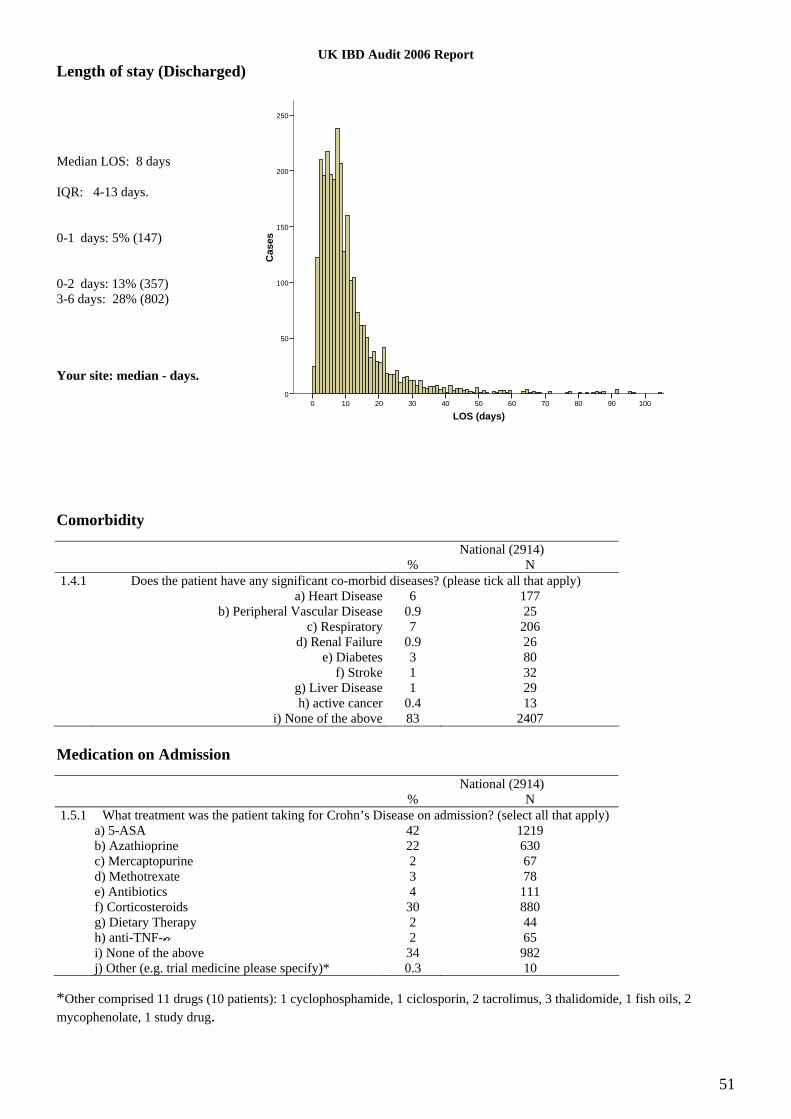
UK IBD Audit 2006 Report
51
Length of stay (Discharged) Median LOS: 8 days IQR: 4-13 days. 0-1 days: 5% (147) 0-2 days: 13% (357) 3-6 days: 28% (802) Your site: median - days.
LOS (days)1009080706050403020100
Cas
es
250
200
150
100
50
0
Comorbidity National (2914)
% N 1.4.1 Does the patient have any significant co-morbid diseases? (please tick all that apply)
a) Heart Disease 6 177 b) Peripheral Vascular Disease 0.9 25 c) Respiratory 7 206 d) Renal Failure 0.9 26 e) Diabetes 3 80 f) Stroke 1 32 g) Liver Disease 1 29 h) active cancer 0.4 13 i) None of the above 83 2407
Medication on Admission National (2914)
% N 1.5.1 What treatment was the patient taking for Crohn’s Disease on admission? (select all that apply)
a) 5-ASA 42 1219 b) Azathioprine 22 630 c) Mercaptopurine 2 67 d) Methotrexate 3 78 e) Antibiotics 4 111 f) Corticosteroids 30 880 g) Dietary Therapy 2 44 h) anti-TNF- 2 65 i) None of the above 34 982 j) Other (e.g. trial medicine please specify)* 0.3 10
*Other comprised 11 drugs (10 patients): 1 cyclophosphamide, 1 ciclosporin, 2 tacrolimus, 3 thalidomide, 1 fish oils, 2 mycophenolate, 1 study drug.

UK IBD Audit 2006 Report
52
Smoking Status Standard: 1.6.1 Smoking status should be documented (BSG guidelines) and smoking cessation support should be offered. National (2914)
% N 1.6.1 What is the smoking status of the patient?
a) Current smoker 31 911 b) Lifelong non-smoker/ ex-smoker 54 1574 c) Not documented 15 429
Patient History National (2914)
% N 1.7.1 Did the patient have a pre-admission diagnosis of Crohn’s Disease?
YES 86 2493 1.7.2 What is the extent of the disease?
a) Small bowel 23 663 b) Colonic 23 667 c) Ileo-colonic 39 1142 d) Perianal 3 76 e) Not known 8 228 f) Other (mainly combinations of a to d above) 5 138
1.7.3 Has patient had previous admissions to your hospital with Crohn’s Disease in the last 2 years? YES 52 1305/2493 If yes, how many times in the two years prior to this admission? Once 54 704 Twice 25 325 More than twice 21 270

UK IBD Audit 2006 Report
53
Assessment: Severity of Disease (Table excludes elective admissions) Standards: 2.1.1 Patients should have stool frequency documented in the first 24 hours following admission. 2.1.5 Patients should have haemoglobin, albumin and CRP (or ESR) performed in the first 24 hours following admission. National (2358)
% N 2.1.1 Was diarrhoea recorded as a symptom upon admission?
YES 52% 1236 No 42% 987 Patient has Stoma 6% 135
2.1.2 How many stools were passed in the 24 hours following admission? Not documented 39% 486/1236 Median (IQR) N If documented 5 (3-9) 750
2.1.3 What was the highest recorded pulse rate (bpm) during the 24 hours following admission? Not documented 4% 106 Median (IQR) N If documented 90 (80-104) 2252
2.1.4 What was the highest recorded temperature (oC) during the 24 hours following admission? Not documented 5% 125 Median (IQR) N If documented 37.0 (36.7-37.5) 2234 Did the patient have a fever (temperature >37.5°C on more than one occasion in 24 hours) within
the first 7 days of admission? YES 17% 403 No 76% 1785 Not documented 7% 170
2.1.5 At this admission, what was the initial result for CRP (mg/L) Not documented 9% 222 Less than 5 14% 329 Median (IQR) N If documented and >5 mg/L 55 (20-129) 1807
2.1.5 At this admission, what was the initial result for Albumin (g/L) Not documented 11% 251 Median (IQR) N If documented 37 (31-42) 2107
2.1.5 At this admission, what was the initial result for Hb (g/dL) Not documented 3% 66 Median (IQR) N If documented 12.6 (11.1-14.1) 2292
2.1.5 At this admission, what was the initial result for ESR (mmh-1) Not documented 69% 1636 Median (IQR) N If documented 28 (13-52) 722

UK IBD Audit 2006 Report
54
Assessment: Exclusion of Infection (Table excludes elective admissions) Standards: 2.2.1 & 2.2.2 Patients with diarrhoea should have a standard stool culture and CDT performed within 48 hours of admission. National (1236 with
diarrhoea)) % N
2.2.1 Was a stool sample sent for Standard Stool Culture* YES 47% 586/1236 Median (IQR) N Date sent: Days from admission 1 (0-2) 584
2.2.2 Was a stool sample sent for CDT* YES 36% 444/1236 Median (IQR) N Date sent: Days from admission 1 (0-3) 444
*Stool sample sent for both in 35% (432/1236)
Assessment: Documentation of Sepsis (Table excludes elective admissions) Standards: 2.3.1 & 2.3.2 Patients with fever (>37.5° C on two occasions) should have blood cultures performed. National (403)
% N 2.3.1 Were antibiotics given? N=403 with fever (2.1.4)
YES 75 303 No 24 96 Not documented 1 4
2.3.2 Were blood cultures taken? N=403 with fever YES 54 216 If yes, were the cultures Positive 7 15 If yes, were the cultures Negative 93 201

UK IBD Audit 2006 Report
55
Assessment: Imaging Standards: 2.4 For suspected abdominal sepsis, imaging should be performed within 48 hours of request and reported within 24 hours of being done. National (2914)
% N 2.4.1 Ultrasound Scan performed 15% 432
Date requested: Same day as admission 30% 129 Median (IQR) N 1 (0-4) 432 Date performed: Performed same day as request 53% 227 1-2 days after request 36% 157 3-5 days after request 8% 36 6 or more days after request 3% 11 Date reported: Same day as performed 78% 338 1-2 days after performed 14% 61 3-5 days after performed 4% 17 6 or more days after performed 4% 16
2.4.2 CT Scan of the abdomen performed 17% 506 Date requested: Same day as admission 28% 140 Median (IQR) N 1 (0-5) 506 Date performed: Performed same day as request 42% 212 1-2 days after request 40% 202 3-5 days after request 14% 70 6 or more days after request 4% 21 Date reported: Same day as performed 65% 330 1-2 days after performed 23% 117 3-5 days after performed 8% 40 6 or more days after performed 4% 19
2.4.3 MRI performed 2% 72 Date requested: Same day as admission 21% 15 Median (IQR) N 3 (1-7) 72 Date performed: Performed same day as request 28% 20 1-2 days after request 27% 19 3-5 days after request 25% 18 6 or more days after request 20% 14 Date reported: Same day as performed 39% 28 1-2 days after performed 24% 17 3-5 days after performed 21% 15 6 or more days after performed 15% 11
2.4.4 Abscess found during imaging YES 11% 113 No 81% 807 NA 8% 76 If drainage was undertaken (113) , was it: a) Surgical 71% 80 b) Radiological 25% 28 Not documented 4 5

UK IBD Audit 2006 Report
56
Assessment: Weight Assessment and Dietetic Support (Table excludes elective admissions) Standards: 2.5.1 Patients should be weighed (BSG Guidelines) and BMI calculated. 2.5.2 Non-elective admissions should be seen by a dietician. 2.5.3 Nutritional support should be provided for malnourished patients (BSG Guidelines). National (2358)
% N 2.5.1 Was the patient’s weight measured during admission?
YES 52% 1223 BMI measured 31% 377/1223
2.5.2 Did a dietitian visit the patient? YES 37% 874
2.5.3 Was dietary treatment initiated? YES 31% 728 Crohn’s-specific dietary therapy prescribed 43% 313/728
2.5.4 Was parenteral nutrition required? YES 6% 144
Site variation histograms: % weight measured during admission Median 50%, Inter-Quartile Range 31-71%, n=185 sites
% Weight measured during admission (Crohn's Disease)1009080706050403020100
Site
s
20
15
10
5
0

UK IBD Audit 2006 Report
57
Assessment: Use of anti-thrombotic therapies Standard: 2.6.1 Patients should have prophylactic heparin (BSG guidelines). National (2914)
% N 2.6.1 Was the patient given:
i. Prophylactic heparin 62% 1814 ii. Anti-thrombotic stockings 36% 1049
35% (1018/2914) had neither prophylactic heparin nor anti-thrombotic stockings.
Medical Intervention: Steroid therapy (Table excludes elective admissions) National (2358)
% N 3.1.1 Were IV corticosteroids prescribed during this admission?
i. Yes 44% 1034 ii. No, but oral corticosteroids were administered 23% 535 iii. No, neither IV or Oral corticosteroids were
administered 33% 789
3.1.2 Which of the following steroids were initially prescribed? (n=1569 on steroids) Prednisolone 36% 562 Budesonide 4% 59 Hydrocortisone 60% 948 Initial dose (Mg per day) Median (IQR) N Prednisolone 40 (30-40) 562 Budesonide 9 (9-9) 59 Hydrocortisone 400 (300-400) 948
3.1.3 Date therapy initiated or increased: (n=1570 on steroids) Same day as admission 54% 846 Next day after admission 20% 312 2-7 days 18% 288 Later 8% 118
Medical Interventions: Blood Transfusion Standard: 3.2.1 Patients with a haemoglobin level of less than 10g/dL should be considered for blood transfusion or iron infusion. National (2914)
% N 3.2.1 What was the patient’s lowest recorded Hb level during admission?
Median (IQR) N 11.2 (9.7-12.7) 2897
3.2.2 Was a blood transfusion given during admission? YES 12% 355

UK IBD Audit 2006 Report
58
Medical Intervention: Initiation of Treatment with anti-TNF- During Admission Standard: 3.3.2 All patients given anti-TNF-α for the first time should have a chest X-ray within the previous 3 months (Joint Tuberculosis Committee of the BTS in conjunction with the BSG and British Society of Rheumatology). National (2358)
% N 3.3.1 Anti-TNF- therapy given during this admission
YES 5% 111/2201 Median (IQR) N Start date: Days after admission 7 (3-14) 111
3.3.2 Is there evidence of a chest x-ray performed in the three months prior to the initiation of anti-TNF- therapy?
YES 70% 84/120 Median (IQR) N Start date of chest x-ray : Days after admission 1 (0-6) 84
Surgical Interventions Standards: 4.1.3 Consultant colorectal surgeons should be involved with the discussion with the patient regarding the decision to operate (BSG Guidelines). 4.1.4 Patients having resectional surgery for Crohn’s Disease should see a stoma nurse prior to operation (BSG Guidelines). 4.1.6 & 4.1.7 Operation should be performed or assisted by a consultant colorectal surgeon. 4.1.10 Patients should have ASA status documented prior to surgery.
Electives (547) Non-Electives (545) % N % N
4.1.2 What date was the decision to operate made? Not known 15% 84 4% 20 Median (IQR) N Median (IQR) N Date of decision: days from admission -28 (-57 to -9) 463 2 (0-7) 525
4.1.3 Which Surgeon made the decision to operate? a) Consultant Colorectal Surgeon 75% 411 67% 367 b) Consultant GI Surgeon (non-colorectal) 3% 14 7% 40 c) Consultant General Surgeon 3% 18 10% 54 d) Other Consultant Surgeon - - 1% 6 e) Specialist Registrar 2% 11 9% 47 f) Other (please specify)* 2% 10 2% 13 g) Not documented 15% 83 3% 18
4.1.4 Patient seen by a stoma nurse during this admission 24% 133 32% 172 Median (IQR) N Median (IQR) N If yes, date first seen : days from admission 1 (0-3) 131 6 (2-13) 172
4.1.5 Median (IQR) N Median (IQR) N
Date of Surgery: days from admission 1 (1-1) 547 4 (1-10) 545
4.1.6 What was the grade of the operating surgeon? a) Consultant Colorectal Surgeon 78% 427 60% 325 b) Consultant GI Surgeon (non-colorectal) 3% 15 6% 32 c) Consultant General Surgeon 3% 18 10% 57 d) Other Consultant Surgeon - - 0.7% 4 e) Specialist Registrar 14% 78 19% 103 f) Other (please specify)** 2% 9 4% 24
4.1.7 What was the grade of the assisting surgeon? a) Consultant Colorectal Surgeon 12% 64 8% 41 b) Consultant GI Surgeon (non-colorectal) 0.5% 3 2% 10 c) Consultant General Surgeon 2% 9 2% 9 d) Other Consultant Surgeon 0.4% 2 0.4% 2 e) Specialist Registrar 65% 358 62% 336 f) Other (please specify)*** 20% 111 27% 147

UK IBD Audit 2006 Report
59
Consultant colorectal surgeon as either operating or assisting surgeon: Electives: 87% (475/547), Non-electives: 65% (353/545) *Other comprised: for elective surgery, 1 associate specialist, 2 Staff Grade, 1 clinical assistant, 4 consultant gastroenterolgist, 1 GI surgeon (grade not specified), 1 gynaecologist (grade not specified). For emergency surgery, others comprised 2 associate specialists, 3 staff grade, 1 F2/Senior House Officer, 4 consultant gastroenterolgists, 3 not known.
** Other comprised: for elective surgery, 2 associate specialist, 4 Staff Grade, 1 locum consultant (specialty not specified) and 2 not known. For emergency surgery, others comprised 5 associate specialist, 11 staff grade, 4 F2/Senior House Officer, 4 not known.
*** Other comprised: for elective surgery, 7 associate specialist, 31 Staff Grade, 1 clinical fellow, 32 FY2/SHO, 6 nurse practitioners, 1 medical student, 1 Specialist GP, 1 Trainee (grade not stated) and 31 not known/not required.
For emergency surgery, others comprised 4 associate specialists, 24 staff grade, 58 F2/Senior House Officer, 1 FY1, 2 Clinical Fellow, 2 nurse practitioners, 1 radiologist (grade not specified), 55 not known.
Electives (547) Non-electives
(545) % N N N
4.1.8 What were the indications for surgery? a) Failure of Medical Therapy 44% 239 23% 123 b) Obstruction 42% 232 38% 208 c) Intra-abdominal Abscess 6% 31 17% 95 d) Intra-abdominal fistula 10% 57 9% 50 e) Stoma complications 2% 10 0.6% 3 f) Perineal disease 7% 40 9% 47 g) Toxic megacolon 0.2% 1 0.9% 5 h) Bleeding 0.7% 4 1% 8 i) Dysplasia 0.5% 3 - - j) Cancer 2% 10 0.2% 1 k) Perforation 0.2% 1 10% 52 l) Other (please specify)* 8% 45 8% 46
4.1.9 Type of intervention $$: a) Segmental/Extended Colectomy 11% 60 12% 67 b) Subtotal Colectomy 8% 43 10% 57 c) Protocolectomy 6% 31 2% 9 d) Stricturoplasty 8% 43 6% 30 e) Ileal/Jejunal Resection 13% 72 17% 93 f) Resection of Intra-abdominal Fistula 5% 28 4% 24 g) Protectomy 6% 33 0.7% 4 h) Ileocolonic Resection 40% 220 38% 208 i) Drainage of abscess 3% 17 12% 65 j) Formation of ileostomy or colostomy 10% 53 12% 68 k) Revision of Stoma 6% 33 1% 8 l) Perineal procedure 4% 22 5% 27 ml) Other intervention (please specify)** 4% 20 11% 59
4.1.9i Was the surgery done laparoscopically/ laparoscopically-assisted? YES 12% 65/521 8% 39/505
4.1.10 ASA status recorded pre-operatively 64% 349 60% 327 If yes, what was the status? 1 26% 90 27% 88 2 61% 213 57% 186 3 12% 41 11% 36 4 0.6% 2 4% 12 5 0.3% 1 0.6% 2 N/A 0.6% 2 0.9% 3
$$ Total is more than 100% because multiple procedures performed at same operation For elective surgery 14% (51/366) of elective segmental/extended colectomy, subtotal colectomy, ileal/jejunal resections or ileocolonic resections were done laparoscopically or were laparoscopically assisted.
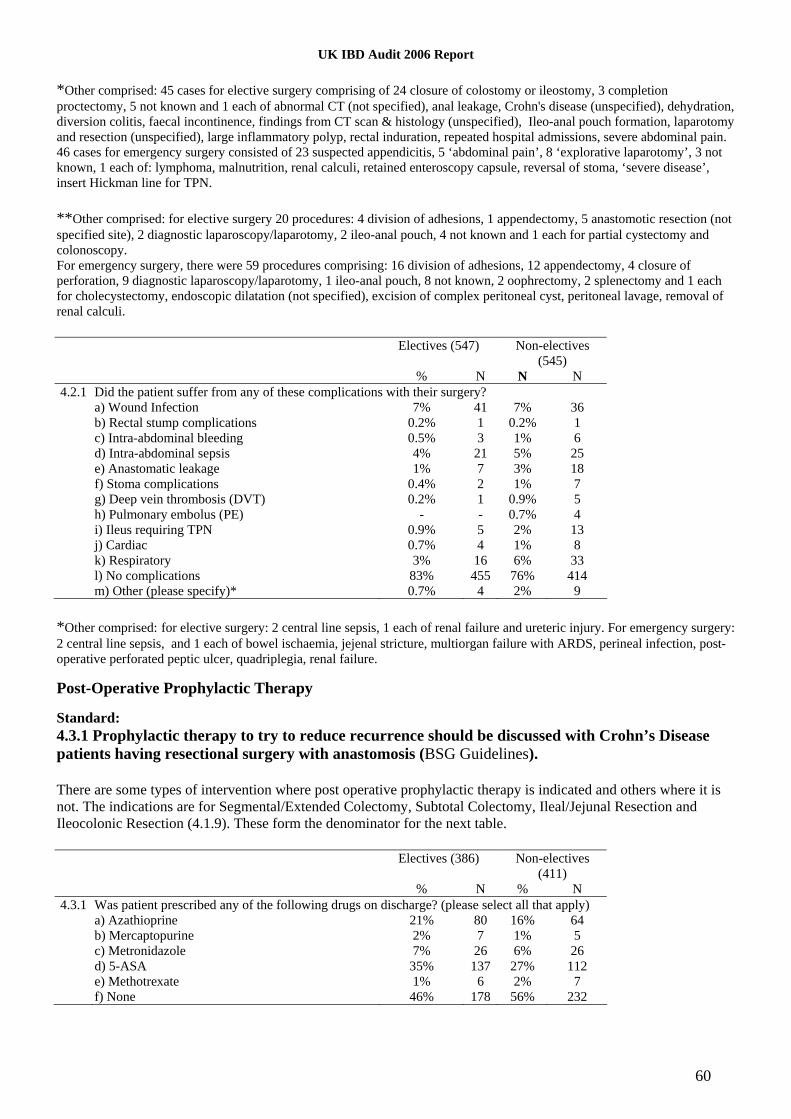
UK IBD Audit 2006 Report
60
*Other comprised: 45 cases for elective surgery comprising of 24 closure of colostomy or ileostomy, 3 completion proctectomy, 5 not known and 1 each of abnormal CT (not specified), anal leakage, Crohn's disease (unspecified), dehydration, diversion colitis, faecal incontinence, findings from CT scan & histology (unspecified), Ileo-anal pouch formation, laparotomy and resection (unspecified), large inflammatory polyp, rectal induration, repeated hospital admissions, severe abdominal pain. 46 cases for emergency surgery consisted of 23 suspected appendicitis, 5 ‘abdominal pain’, 8 ‘explorative laparotomy’, 3 not known, 1 each of: lymphoma, malnutrition, renal calculi, retained enteroscopy capsule, reversal of stoma, ‘severe disease’, insert Hickman line for TPN. **Other comprised: for elective surgery 20 procedures: 4 division of adhesions, 1 appendectomy, 5 anastomotic resection (not specified site), 2 diagnostic laparoscopy/laparotomy, 2 ileo-anal pouch, 4 not known and 1 each for partial cystectomy and colonoscopy. For emergency surgery, there were 59 procedures comprising: 16 division of adhesions, 12 appendectomy, 4 closure of perforation, 9 diagnostic laparoscopy/laparotomy, 1 ileo-anal pouch, 8 not known, 2 oophrectomy, 2 splenectomy and 1 each for cholecystectomy, endoscopic dilatation (not specified), excision of complex peritoneal cyst, peritoneal lavage, removal of renal calculi. Electives (547) Non-electives
(545) % N N N
4.2.1 Did the patient suffer from any of these complications with their surgery? a) Wound Infection 7% 41 7% 36 b) Rectal stump complications 0.2% 1 0.2% 1 c) Intra-abdominal bleeding 0.5% 3 1% 6 d) Intra-abdominal sepsis 4% 21 5% 25 e) Anastomatic leakage 1% 7 3% 18 f) Stoma complications 0.4% 2 1% 7 g) Deep vein thrombosis (DVT) 0.2% 1 0.9% 5 h) Pulmonary embolus (PE) - - 0.7% 4 i) Ileus requiring TPN 0.9% 5 2% 13 j) Cardiac 0.7% 4 1% 8 k) Respiratory 3% 16 6% 33 l) No complications 83% 455 76% 414 m) Other (please specify)* 0.7% 4 2% 9
*Other comprised: for elective surgery: 2 central line sepsis, 1 each of renal failure and ureteric injury. For emergency surgery: 2 central line sepsis, and 1 each of bowel ischaemia, jejenal stricture, multiorgan failure with ARDS, perineal infection, post-operative perforated peptic ulcer, quadriplegia, renal failure. Post-Operative Prophylactic Therapy Standard: 4.3.1 Prophylactic therapy to try to reduce recurrence should be discussed with Crohn’s Disease patients having resectional surgery with anastomosis (BSG Guidelines). There are some types of intervention where post operative prophylactic therapy is indicated and others where it is not. The indications are for Segmental/Extended Colectomy, Subtotal Colectomy, Ileal/Jejunal Resection and Ileocolonic Resection (4.1.9). These form the denominator for the next table. Electives (386) Non-electives
(411) % N % N
4.3.1 Was patient prescribed any of the following drugs on discharge? (please select all that apply) a) Azathioprine 21% 80 16% 64 b) Mercaptopurine 2% 7 1% 5 c) Metronidazole 7% 26 6% 26 d) 5-ASA 35% 137 27% 112 e) Methotrexate 1% 6 2% 7 f) None 46% 178 56% 232

UK IBD Audit 2006 Report
61
Discharge Arrangements Standards: 5.1.1 & 5.1.2 Patients should be followed up by a gastroenterologist or colorectal surgeon. 5.1.3 Patients discharged on oral steroids should have a steroid reduction programme stated on discharge. 5.1.4 Patients on oral steroids should be co-prescribed bone protection agents (such as calcium and vitamin D or bisphosphonates) (BSG guidelines). National (2914)
% N 5.1.1 Was an appointment made for the patient to be referred back to a Gastroenterologist
YES 78% 2268 5.1.1 Was an appointment made for the patient to be referred back to a Colorectal Surgeon
YES 42% 1220 5.1.2 Was the patient taking oral steroids on discharge?
YES 56% 1628 No 42% 1214 N/A 2% 72
5.1.3 Was a steroid reduction programme stated on discharge? (N=1628 on steroids) YES 80% 1305 No 17% 275 N/A 3% 48
5.1.4 Were bone protection agents prescribed? (N=1628 on steroids) YES 40% 645
An appointment was made to refer back to both a gastroenterologist and a colorectal surgeon for 26% (745/2914), and there was no appointment to either for 6% (171/2914).

UK IBD Audit 2006 Report
62
Section 5. Clinical Audit: Crohn’s Disease (Outpatient) Patient History Standard: 6.1.3 Continuity of care in hospital outpatient visits matters to patients - patients dislike seeing different individuals at each visit (BSG guidelines). Patients should be offered the opportunity to see an IBD specialist (nurse or doctor) at last once a year. National (2914)
% N 6.1.1 Has patient had previous outpatient visits for Crohn’s Disease at this hospital in last 12 months?
YES 64% 1866 6.1.2 How many times was the patient reviewed for their Crohn’s Disease in an outpatient’s clinic in the
12 months prior to the start date of this admission? Median (IQR) N 4 (2-5) 1866
6.1.3 Approximately how many times was the patient seen by the following staff in the 12 months prior to the start date of this admission? (If the patient was seen by more than one of the following staff in a single clinic visit please count each staff member individually)*
Median (IQR) N Consultant 2 (1-4) 1866 IBD Nurse Specialist 0 (0-0) 1866 Specialist Registrar 0 (0-1) 1866 SHO 0 (0-0) 1739
* For 91% (1699/1866) of cases patient was seen by a consultant, in 24% (455/1866) by an IBD specialist nurse, in 41% (767/1866) by a specialist registrar and in 12% (209/1739) by a SHO. The rest of the outpatient results are for those who were said to have had a previous outpatient visit in the last 12 months (i.e Q6.1.1 = YES, n=1866). About 5% of these had outpatient dates after the date of the audited admission and whilst some of these reflect mistyping of year (eg 2006 instead of 2005) most appear to reflect a misinterpretation of the question as being last outpatient visit per se rather than last outpatient visit before the audited admission. As the nature of the outpatient visit is unlikely to change then all 1866 have been included.
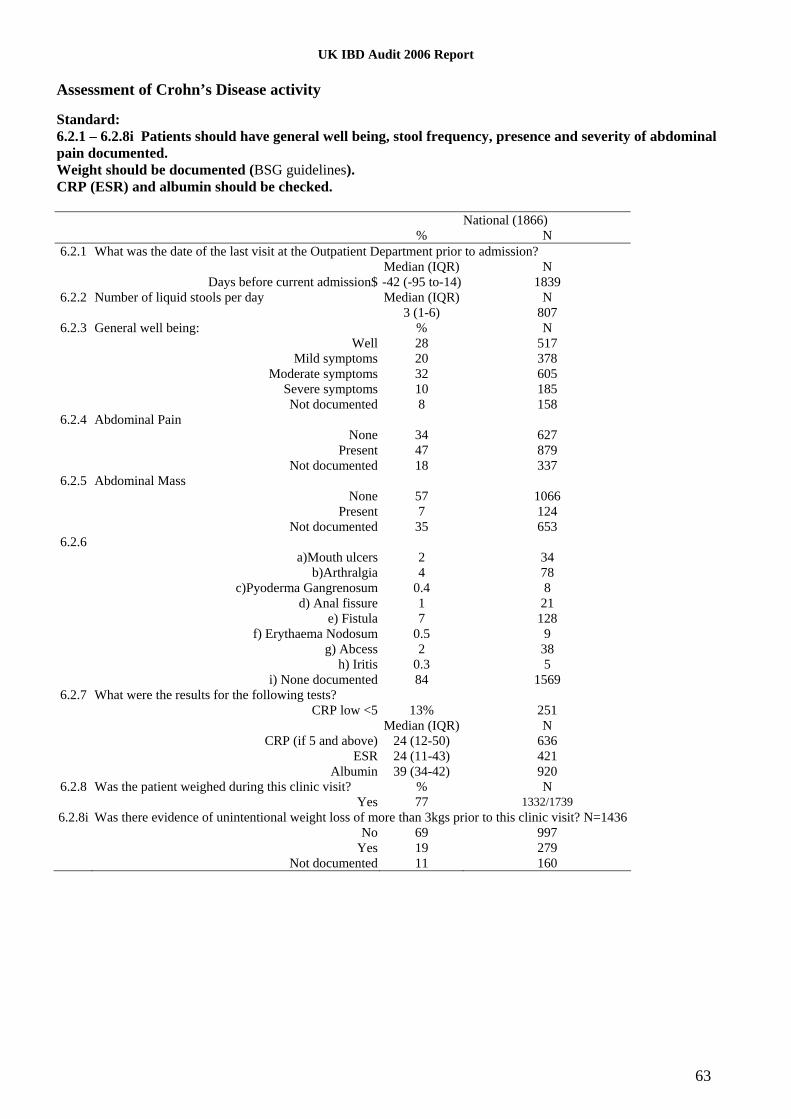
UK IBD Audit 2006 Report
63
Assessment of Crohn’s Disease activity Standard: 6.2.1 – 6.2.8i Patients should have general well being, stool frequency, presence and severity of abdominal pain documented. Weight should be documented (BSG guidelines). CRP (ESR) and albumin should be checked. National (1866)
% N 6.2.1 What was the date of the last visit at the Outpatient Department prior to admission?
Median (IQR) N Days before current admission$ -42 (-95 to-14) 1839
6.2.2 Number of liquid stools per day Median (IQR) N 3 (1-6) 807
6.2.3 General well being: % N Well 28 517 Mild symptoms 20 378 Moderate symptoms 32 605 Severe symptoms 10 185 Not documented 8 158
6.2.4 Abdominal Pain None 34 627 Present 47 879 Not documented 18 337
6.2.5 Abdominal Mass None 57 1066 Present 7 124 Not documented 35 653
6.2.6 a)Mouth ulcers 2 34 b)Arthralgia 4 78 c)Pyoderma Gangrenosum 0.4 8 d) Anal fissure 1 21 e) Fistula 7 128 f) Erythaema Nodosum 0.5 9 g) Abcess 2 38 h) Iritis 0.3 5 i) None documented 84 1569
6.2.7 What were the results for the following tests? CRP low <5 13% 251 Median (IQR) N CRP (if 5 and above) 24 (12-50) 636 ESR 24 (11-43) 421 Albumin 39 (34-42) 920
6.2.8 Was the patient weighed during this clinic visit? % N Yes 77 1332/1739
6.2.8i Was there evidence of unintentional weight loss of more than 3kgs prior to this clinic visit? N=1436 No 69 997 Yes 19 279 Not documented 11 160

UK IBD Audit 2006 Report
64
Smoking Status
Standard: 6.3.1 Smoking status should be documented (BSG guidelines) and smoking cessation support should be offered. National (1866)
% N 6.3.1 What was the smoking status of the patient during this clinic visit?
a) Current smoker 25 467 b) Lifelong non-smoker/ex-smoker 41 766 c) Not documented 34 633
Monitoring of immunosuppressive therapy Standard: 6.4.2 – 6.4.3 Full blood count should be monitored at least 3 monthly for patients on established immunosuppressive therapy (BSG guidelines). National (1866)
% N 6.4.1 Was patient taking any of these drugs in the 12 months prior to the start date of this admission?
Azathioprine 35% 662 Mercaptopurine 4% 81 Methotrexate 6% 103 None of these 57% 1060
6.4.2 Was the patient’s white blood cell (WBC) count routinely measured? (denominator comprises those on any of the three drugs in 6.4.1, n=806)
YES 92% 743/806 6.4.3 How often was WBC monitoring performed? (743)
At least once a month 38% 279 Every 2-3 months 53% 392 Less frequent than 3 monthly 1% 10 Not documented 8% 62
6.4.4 Did patient’s WBC fall below 3x109 at any time during 12 months before this admission? YES 4% 28/743
6.4.5 If the white blood cell count was less than 3.0x109 what action was taken? Reduced dose 14% 4 Stopped drug 71% 20 No action taken 14% 4
6.4.6 What was the outcome of the reduced white blood cell count? No sequelae (resolved) 96% 27 Treatment required (e.g. prophylactic antibiotics) - - Admission 4% 1

UK IBD Audit 2006 Report
65
Use of Corticosteroids Standards: 6.5.2 Prolonged use of steroid therapy is of no benefit in maintaining remission in Crohn’s Disease, increases the risk of septic complications and is associated with an increased mortality. Prolonged use of steroids (> 3 months oral prednisolone or budesonide) should be avoided. 6.5.3 Patients on oral steroids should be co-prescribed bone protection agents (BSG Guidelines). National (1866)
% N 6.5.1 Was the patient taking oral corticosteroids for their Crohn’s Disease in the 12 months prior to
the start date of this admission? YES 56% 1047
6.5.2 Was there any point at which the patient was taking oral corticosteroids continuously for more than three months?
YES 46% 484/1047 6.5.3 Were bone protection agents prescribed alongside corticosteroids?
YES 45% 475/1047 6.5.4 Was bone densitometry measured within 12 months of initiation of the corticosteroid therapy?
YES 18% 184/1047 Of those who were on corticosteroids for > 3 months 45% (219/484) were not on bone protection agents Site variation histogram: % patients at any point taking oral corticosteroids for > 3 months Median 43%, Inter-Quartile Range 20-64%, n=175 sites
% Taking oral corticosteroids for Crohn's Disease continuously for >3M1009080706050403020100
Site
s
40
30
20
10
0

UK IBD Audit 2006 Report
66
Use of anti-TNF- therapy Standards: 6.6.1 Patients initiated on infliximab should have severely active Crohn’s Disease (NICE guidance). 6.6.5 All patients receiving infliximab therapy should be on concomitant immunosuppressive therapy if tolerated (BSG Guidelines). 6.6.7 Infliximab treated patients should have a documented chest X-ray within 3 months prior to first treatment (Joint Tuberculosis Committee of the BTS in conjunction with the BSG and British Society of Rheumatology). National (1866)
% N 6.6.1 Did the patient receive anti-TNF- therapy in the 12 months prior admission?
YES 8% 131/1739 6.6.2 Was anti-TNF- therapy initiated at any point in the 12 months prior to the start date of this
admission? YES 78% 102/131
6.6.3 Did the patient have severely active Crohn’s Disease at the time anti-TNF- therapy was initiated?
YES 82% 84/102 6.6.4 What was the CRP prior to the first anti-TNF-
transfusion on record? Median (IQR) N
33 (13-78) 58 Low <5 13 Not documented 31
6.6.5 Was the patient on immunosuppressive therapy at this time? YES 72% 73/102 If NO, is there any evidence that patient was intolerant of these immunosuppressive
therapies? YES 45% 13/29
6.6.6 Was fistulating disease the primary reason for the decision to initiate anti-TNF- therapy? YES 26% 27/102
6.6.7 Did the patient have a chest X-ray to exclude TB in the three months prior to initiation of anti-TNF- therapy?
YES 86% 88/102 Of those who were on corticosteroids for > 3 months (Q6.5.2), 12% (55/448) received anti-TNF- therapy in the 12 months prior admission

Appendix 1
UK IBD Audit 2006 Steering Group
Chair Dr Keith Leiper, Consultant Gastroenterologist, Royal Liverpool University Hospital
Association of Coloproctology of Great Britain and Ireland Mr Ian Finlay, Consultant Colorectal Surgeon, Glasgow Royal Infirmary
Association of Coloproctology of Great Britain and Ireland Professor Neil Mortensen, Professor of Colorectal Surgery, Oxford Radcliffe Hospitals NHS Trust
Association of Coloproctology of Great Britain and Ireland Miss Asha Senapati, Consultant Surgeon, Queen Alexandra Hospital, Portsmouth
British Dietetic Association Ms Miranda Lomer, Locum Consultant Dietitian in Gastroenterology, Guy's and St Thomas' NHS Foundation Trust
British Society of Gastroenterology Dr Ian Arnott, Consultant Gastroenterologist, Western General Hospital, Edinburgh
British Society of Gastroenterology Dr Tim Harding, Consultant Gastroenterologist, Lagan Valley Hospital
British Society of Gastroenterology Dr Chris Probert, Consultant Gastroenterologist, Bristol Royal Infirmary
British Society of Gastroenterology Professor Jonathan Rhodes, Professor of Medicine, University of Liverpool
British Society of Gastroenterology Mrs Chris Romaya, Executive Secretary
British Society of Gastroenterology Dr Simon Travis, Clinical Director of Gastroenterology & Endoscopy, Oxford Radcliffe Hospitals NHS Trust
IBD Do Once and Share Dr Ian Shaw, Consultant Gastroenterologist, Gloucestershire Royal Hospital
National Association for Colitis and Crohn’s Disease (NACC) Mr Richard Driscoll, Director (NACC)
Royal College of Nursing Ms Allison Nightingale, IBD Specialist Nurse, Addenbrooke’s Hospital
Royal College of Physicians Dr Iain Buchan, Director & Senior Lecturer in Public Health Informatics, Northwest Institute for Bio-Health Informatics
Royal College of Physicians Mr Calvin Down, Project Manager, UK IBD Audit
Royal College of Physicians Dr Barney Hawthorne, Consultant Gastroenterologist, Cardiff and Vale NHS Trust
UK IBD Audit 2006 Steering Group

Royal College of Physicians Ms Jane Ingham, Director of Clinical Standards
Royal College of Physicians Dr Jonathan Potter, Clinical Director, Clinical Effectiveness and Evaluation Unit
Royal College of Physicians Professor Michael Pearson, Clinical Director (former), Clinical Effectiveness and Evaluation Unit
Royal College of Physicians Miss Nancy Pursey, Project Co-ordinator, UK IBD Audit
Royal College of Physicians Ms Anil Seiger, Manager, Clinical Effectiveness and Evaluation Unit
Royal Pharmaceutical Society of Great Britain Ms Jackie Eastwood, Senior Specialist Gastroenterology Pharmacist, St. Mark’s Hospital
UK IBD Audit 2006 Steering Group

UK IBD Audit 2006 Organisation and Structure Proforma 69
UK IBD Audit 2006 Organisation and Structure Proforma
The Organisation & Structure Proforma relates to your IBD Services as at 1st June 2006
Auditor Discipline: a) Consultant b) Other medical staff c) Nurse d) Audit staff
e) Other (please specify):
1 General Hospital Demographics 1.1
How many beds does your hospital have in total?
1.2 Does your hospital have either of the following? i. Acute medicine unit Yes No
ii. Acute surgical unit Yes No
1.3 Is there an Intensive Therapy Unit (ITU) on site? Yes No
i. If yes, how many beds?
1.4 Is there a High Dependency Unit (HDU) on site? Yes No
i. If yes is it: a) Medical b) Surgical c) Mixed
ii. If yes, how many HDU beds?
1.5 Is there a combined Intensive Therapy (ITU) & High Dependency (HDU) Unit on site? Yes No
i. If yes is it: a) Medical b) Surgical c) Mixed
ii. If yes, how many combined Intensive Therapy (ITU) & High Dependency (HDU) beds
2 Inpatient Activity
2.1
How many patients were discharged between 1st June 2005 and 31st May 2006 with a primary diagnosis of:
i Ulcerative Colitis
ii Crohn’s Disease 2.2
How many patients were discharged between 1st June 2005 and 31st May 2006 having had an operation where the primary indication was:
i Ulcerative Colitis
ii Crohn's Disease
2.3 Do surgeons perform ileo-anal pouch surgery on site? Yes No
i. If yes, how many ileo-anal pouch operations were performed between 1st June 2005 and 31st May 2006?

UK IBD Audit 2006 Organisation and Structure Proforma 70
3 Gastroenterology Services
3.1 Is there a dedicated Gastroenterology ward? Yes No
i. If yes, how many beds per lavatory on the ward? .
3.2 How many WTE Gastroenterologists are there on site? .
3.3 How many Gastroenterology staff of the following grades are there on site?
i. Specialist Registrar (SpR)
ii. Associate Specialist
3.4 How many IBD Nurse Specialists are there on site? .
3.5
How many sessions of Specialist Nurse time are dedicated to IBD care per week? N/A
4 Colorectal Services
4.1 How many WTE specialist Colorectal Surgeons are there on site? . 4.2 How many Colorectal staff of the following grades are there on site?
i. Specialist Registrar (SpR)
ii. Associate Specialist
4.3 How many Stoma Nurses are there on site? . 4.4
How many sessions of Stoma Nurse time are dedicated to stoma care per week? N/A
5 Multi-Disciplinary Working
5.1 Is there a searchable database of IBD patients on site? Yes No
5.2 Do timetabled meetings take place between the following specialties:
i. Gastroenterologists and Colorectal Surgeons Yes No
ii. Gastroenterologists and Pathologists Yes No
iii. Gastroenterologists and Radiologists Yes No
iv. Colorectal Surgeons and Pathologists Yes No
v. Colorectal Surgeons and Radiologists Yes No
5.3 Is there a specialist GI Pathologist? Yes No
5.4 Is there a specialist GI Radiologist? Yes No

UK IBD Audit 2006 Organisation and Structure Proforma 71
6 Dietetics and Nutritional Services
6.1 Is there a hospital nutrition team? Yes No
6.2 Is it a multi-disciplinary team? Yes No
6.3 Does the team go on ward rounds? Yes No
i. If yes, how frequently? Daily Weekly Other (please specify):
6.4 How many dietetic sessions per week are dedicated to GI disorders?
7 Outpatient Services 7.1
Is there written information for patients with IBD on whom to contact in the event of a relapse? Yes No
7.2 In general, how soon could a relapsed patient expect to be seen in clinic?
a) Less than 7 days b) Between 7-14 days c) Other (please specify):
7.3 Do patients have access to an IBD specialist by any of the following methods (tick all that apply)
a) Telephone b) Drop-in clinic c) Email d) None of these
7.4 Are there any joint or parallel clinics run between Gastroenterologists and Surgeons?
a) Joint b) Parallel c) Neither
8 Patient Information
8.1 Are patients provided with written information about IBD? Yes No
i. If yes, is the information produced by: a) NACC b) Pharmaceutical
c) Locally written d) Drug specifice) Other (please
specify)
9 Monitoring of established immunosuppresive therapy
9.1 How is established immunosuppresive therapy monitored? (Please tick all that apply)
a) By the GP c) During clinic visits
b) A dedicated monitoring service
d) A combination of primary and secondary care
monitoring
10 IBD Support Services 10.1 Is there a paediatric to adult handover clinic for young patients with IBD? Yes No
10.2 Is a registered counsellor available to patients as part of your IBD Service? Yes No
10.3 Are there any psychologists attached to the Gastroenterology service? Yes No
i. If yes, how many sessions per month are dedicated to the Gastroenterology service? .
10.4 Do pathways exist for direct access to psychological support? Yes No
UK IBD Audit 2006 Organisation and Structure Proforma 72
10.5 Is there an acute pain management team on site? Yes No
11 Management of Ulcerative Colitis 11.1
Do written trust guidelines exist for the management of acute or severe colitis? Yes No
12 Interactions between your hospital and patients and patient groups
12.1 Does your hospital offer open forums or meetings for patients with IBD? Yes No
i. If yes, how often do these take place? a) Less than 4 monthly
c) Every 8-12 months
b) Every 4-8 months d) Other (please specify)
ii. Which staff attend these meetings? a) Medical b) Surgical c) Nursing
12.2
Are any of the following activities or systems in place to involve patients in giving their views on the development of your IBD services? (Please tick all that apply)
a) Regular patient surveys c) Patient panel meetings e) Other
b) Individual patient representatives d) None

UK IBD Audit 2006 Ulcerative Colitis Proforma
73
UK IBD Audit 2006 Ulcerative Colitis Proforma
Pre-section: Patient Demographics
A Auditor Discipline: a) Consultant b) Other medical staff c) Nurse d) Manager
e) Other (please specify):
B Patient Audit Number: Assigned by system
C What year was the patient born?
D Gender: Male Female
E What are the first 2 to 4 letters/numbers of the patient's postcode?
Section 1: Admission/Mortality
1.1 Admission
1.1.1 What was the date of admission to this hsopital? / / 1.1.2 What was the source of admission to this hospital?
a) General Practitioner (GP) b) Accident and Emergency (A&E)
c) Outpatients Department (OPD) d) Other hospital
e) Not documented
1.1.3 What was the duration of active colitis (new or relapse) precipitating this admission?
a) Less than two weeks b) Two to three weeks
c) Four to eight weeks d) More than eight weeks
e) Not documented
1.1.4 What was the primary reason for admission?
a) Emergency admission for active Ulcerative Colitis c) Elective admission for surgery
b) Planned admission for active Ulcerative Colitis
1.1.5 Which specialty was responsible for the patient's initial care 24 hours after admission?
a) Acute Medicine b) Gastroenterology c) Colorectal Surgery
d) Geriatrics e) General Medicine f) General Surgery
g) Other (please specify)
UK IBD Audit 2006 Ulcerative Colitis Proforma 74
1.1.6
What date was the person first seen by a Consultant Gastroenterologist? / /
Not Seen
Not required
1.1.7
What date was the patient first seen by a Consultant Colorectal Surgeon? / /
Not seen
Not required
1.1.8
Was the patient visited by an IBD Nurse/GI Nurse specialist during admission? Yes No
1.1.9 Was the patient transferred to a specialist gastroenterology ward?
a) Medical b) Joint c) Surgical d) Not transferred
1.2 Comorbidity 1.2.1 Does the patient have any significant co-morbid diseases? (please tick all that apply)
a) Heart Disease b) Peripheral Vascular Disease
c) Respiratory d) Renal Failure
e) Diabetes f) Stroke
g) Liver Disease h) active cancer
i) None
1.3 Discharge/Mortality
1.3.1 Did the patient die during admission? Yes No
i. Date of death / /
ii. Cause of death
iii. Date of discharge / /
1.3.2 Did the patient die after discharge? Yes No Not known
i. Date of Death
/ /Not known
ii. Cause of death:
Section 2: Assessing the extent of UC 2.1 Patient History
2.1.1 Did the patient have a pre-admission diagnosis of Ulcerative Colitis? Yes No
2.1.2 Has the patient had previous admissions with Ulcerative Colitis? Yes No
i. If yes, how many times in the two years prior to this admission?

UK IBD Audit 2006 Ulcerative Colitis Proforma 75
2.2 Severity of Disease 2.2.1
How many stools were passed in the 24 hours following admission? Not documented
Not applicable, patient had stoma
2.2.2
What was the highest recorded pulse rate during the 24 hours following admission? bpm
Not documented
2.2.3
What was the highest temperature recorded during the 24 hours following admission? . °C
Not documented
2.2.4 At this admission, what was the initial result for:
i. CRP
mg/L
Less than 5 Not documented
ii. Albumin
g/L
Not documented
iii. Hb .
g/dL
Not documented
iv. ESR
mmh-1
Not documented
2.2.5 Was a stool sample sent for Standards Stool Culture?
Yes No
i. Date sent: / /
2.2.6 Was a stool sample sent for CDT? Yes No i. Date sent: / /
2.3 Endoscopic Assessment 2.3.1 On this admission, did the patient have any of the following procedures? (Please tick all that apply)
a) Rigid sigmoidoscopy b) Flexible Sigmoidoscopy c) Colonoscopy
d) None of the above
i. Date of first procedure: / / 2.3.2 What was the assessment of severity of inflammation?
a) Mild b) Moderate c) Severe d) Not documented
2.3.3 Were biopsies taken for histology? Yes No
i. Date histology reports approved by histopathology: / /

UK IBD Audit 2006 Ulcerative Colitis Proforma 76
Section 3: Monitoring of Colitis – Post-Admission 3.1 General information
3.1.1 Was the patient given: Prophylactic heparin Yes No
3.1.2 Was the patient given: Anti-thrombotic stockings Yes No
3.1.3 In the first seven days following admission, how often was the patient’s pulse monitored?
a) 4 or more times per day b) 1-3 times per day c) Less than once a day
d) Not monitored
3.1.4
In the first 7 days following admission did the patient have a persistent Tachycardia (Pulse rate >90bpm on more than one occasion in 24 hours) Yes No
i. If yes, date recorded / /
3.1.5 In the first seven days following admission, how often was temperature monitored?
a) 4 or more times per day b) 1-3 times per day c) Less than once a day
d) Not monitored 3.1.6
In the first 7 days following admission did the patient have a Fever (Temperature >37.5°C on more than one occasion in 24 hours) Yes No
i. If yes, date recorded / /
3.1.7 In the first seven days following admission, how often was stool frequency monitored?
a) Daily b) Every 2-3 days c) Every 4-6 days
d) Once a week e) Not applicable,
stoma present f) Not documented
3.1.8 In the first seven days following admission, how often was CRP monitored?
a) Daily b) Every 2-3 days c) Every 4-6 days
d) Once e) Not documented
3.1.9
At any point following the first 72-hours of steroid therapy was the patient’s CRP level reported to be greater than >45mg/L
Yes No missing
3.1.10 In the first seven days following admission, how often was ESR monitored?
a) Daily b) Every 2-3 days c) Every 4-6 days
d) Once e) Not documented
UK IBD Audit 2006 Ulcerative Colitis Proforma 77
3.2 Monitoring of Colitis – Radiology 3.2.1
Was a plain abdominal X-Ray performed? Yes i. Date requested / /
No ii. Date performed / /
iii. Date reported by
Radiologist / /
iv. Date not reported by
Radiologist
3.2.2 Was toxic megacolon present in the x-ray? Yes No NA
i. If yes, was a repeat x-ray performed? Yes No
ii. Date performed
/ /3.2.3
Was a CT Scan of the abdomen performed? Yes i. Date requested / /
No ii. Date performed / /
iii. Date reported / / Section 4: Medical Interventions 4.1 Steroid therapy
4.1.1 Were IV corticosteroids prescribed during this admission? i. Yes
ii. No, but oral corticosteroids were prescribed
iii. No, neither IV or Oral corticosteroids were prescribed during this admission
4.1.2 Which of the following steroids were initially prescribed? (see help notes)
Prednisolone Budesonide
Hydrocortisone
i. Initial dose Mg/day
4.1.3 Date therapy initiated or increased: / /
4.1.4 At any point following the first 72-hours of steroid therapy did the patient produce stools at a frequency greater than 8 per day? Yes No
Not documented
4.1.5 Did the patient report either moderate or severe pain during steroid therapy? Yes
No
i. Date recorded: / /4.1.6 Did the patient achieve remission from steroid therapy? Yes No
UK IBD Audit 2006 Ulcerative Colitis Proforma 78
4.2 Other Therapies Which other therapies did the patient receive?
4.2.1 Ciclosporin
i. Start Date / /
ii. Did the patient achieve remission on ciclosporin therapy? Yes No
4.2.2 Anti TNF
i. Start Date / /
ii. Did the patient achieve remission on TNF therapy? Yes No
4.2.3 Clinical Trial (please specify)
i. Start Date / /
ii. Did the patient achieve remission from the clinical trial? Yes No
4.2.4 Significant Other therapies
(please specify) i. Start Date / /
ii. Did the patient achieve remission on other therapy? Yes No
4.2.5 Surgical therapy
4.3 Initiating Ciclosporin Therapy
What were the pre-treatment results for:
4.3.1 Creatinine μmol/L i. Date sample taken: / / Not Documented
4.3.2 Magnesium mEq/L i. Date sample taken: / /
Not Documented
4.3.3 Cholesterol mmol/L i. Date sample taken: / / Not Documented
4.3.4 How was the ciclosporin initially administered? Oral IV
i. What was the initial daily dose? Mg/Kg
4.4 Monitoring Ciclosporin Therapy After Ciclosporin therapy was initiated, how often were each of the following measured?
4.4.1 Creatinine
a) Daily b) Every two days c) Every three days
d) Once a week e) Less than once a week f) Not documented

UK IBD Audit 2006 Ulcerative Colitis Proforma 79
4.4.2 FBC (Full Blood Count)
a) Daily b) Every two days c) Every three days
d) Once a week e) Less than once a week f) Not documented4.4.3 After three days of ciclosporin therapy, how often were serum ciclosporin levels checked?
a) Daily b) Every two days c) Every three days
d) Once a week e) Less than once a week f) Not documented
Section 5: Surgical Interventions 5.1 Surgical Therapy
5.1.1 What date was the decision to operate made? / / Not Known
5.1.2 Who made the decision to operate? a) Consultant Colorectal Surgeon b) Consultant GI Surgeon (non-colorectal)
c) Consultant General Surgeon
d) Other Consultant Surgeon
e) Specialist Registrar
f) Other (please specify)
5.1.3 What was the date of surgery? / /5.1.4 Was the patient seen by a stoma nurse during this admission? Yes No
i. If yes, what date was the patient first seen by a stoma nurse? / /
5.1.5 What was the grade of the operating surgeon? a) Consultant Colorectal Surgeon b) Consultant GI Surgeon (non-colorectal)
c) Consultant General Surgeon
d) Other Consultant Surgeon
e) Specialist Registrar
f) Other Surgeon (please specify)
5.1.6 What was the grade of the assisting surgeon? a) Consultant Colorectal Surgeon b) Consultant GI Surgeon (non-colorectal)
c) Consultant General Surgeon
d) Other Consultant Surgeon
e) Specialist Registrar
f) Other (please specify)
5.1.7 What were the indications for surgery?
a) Failure of Medical Therapy e) High Grade Dysplasia i) Perforation
b) Toxic megacolon f) Low Grade Dysplasia j) Abscess
c) Bleeding g) Ungraded Dysplasiak) Formation of ileostomy
d) Obstruction h) Cancerl) Other indication
(please specify)
UK IBD Audit 2006 Ulcerative Colitis Proforma 80
5.1.8 Type of intervention: a) Subtotal colectomy e) Ileoanal pouch without stoma
b) Protocolectomy f) Formation of ileostomy
c) Protectomy g) Other (please specify)
d) Ileoanal pouch with stoma 5.1.8i
Was the surgery done laparoscopically/ laparoscopically-assisted? Yes No
5.1.9 Was the ASA status recorded pre-operatively? Yes No
i. If yes, what was the status? 1 2 3 4 5 N/A 5.2 Surgical Complications
5.2.1 Did the patient suffer from any of these complications with their surgery?
a) Wound Infection i) Small bowel obstruction
b) Rectal stump complications j) Ileus requiring parenteral nutrition
c) Intra-abdominal bleeding k) Cardiac
d) Intra-abdominal sepsis l) Respiratory
e) Anastomatic leakage m) Other (please specify)
f) Stoma complications n) No Complications
g) Deep vein thrombosis (DVT)
h) Pulmonary embolus (PE)
Section 6: Discharge Arrangements 6.1 Discharge Arrangements
6.1.1 Was an appointment made for the patient to be referred back to a:
i. Gastroenterologist Yes No
ii. Colorectal Surgeon Yes No
6.1.2 Was the patient taking oral steroids on discharge? Yes No N/A6.1.3
Was a steroid reduction programme stated on discharge? Yes No N/A
6.1.4 Were bone protection agents prescribed? Yes No N/A

UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 81
UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma
Pre-section: Patient Demographics
A Auditor Discipline: a) Consultant b) Other medical staff c) Nurse d) Manager
e) Other (please specify):
B Patient Audit Number: Assigned by system
C What year was the patient born?
D Gender: Male Female
E
What are the first 2 to 4 letters/numbers of the patient's postcode?
Section 1: Admission/Mortality 1.1 Admission
1.1.1 What was the date of admission to this hospital? / /
1.1.2 What was the primary reason for admission to this hospital?
a) Emergency admission for active Crohn’s Disease d) New diagnosis of Crohn’s Disease
b) Planned admission for active Crohn’s Disease
*If none of the options can be chosen please disregard this patient’s notes and choose the next case to enter
c) Elective admission for surgery
1.1.3 What was the source of admission? a) General Practitioner (GP) b) Accident and Emergency (A&E)
c) Outpatients Department (OPD) d) Other hospital
e) Not Documented
1.1.4 What duration of new or relapse symptoms did the patient report prior to their admission?
a) Less than two weeks b) Two to three weeks
c) Four to eight weeks d) More than eight weeks
e) Not Documented

UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 82
1.2 Admitting Speciality
1.2.1 Which specialty was responsible for the patient's initial care 24 hours after admission?
a) Acute Medicine e) General Medicine
b) Gastroenterology f) General Surgery
c) Colorectal Surgery g) Other (Please specify)
d) Geriatrics
1.2.2 Was the patient transferred to a specialist gastroenterology ward?
a) Medical b) Joint c) Surgical d) Not transferred 1.2.3
What date was the person first seen by a Consultant Gastroenterologist? / /
Not Seen
Not required
1.2.4 What date was the patient first seen by a
Consultant Colorectal Surgeon? / /
Not Seen
Not required
1.2.5
Was the patient visited by an IBD Nurse/GI Nurse specialist during admission? Yes No
1.3 Discharge/Mortality
1.3.1 Did the patient die during admission? Yes No
i. Date of death / / ii. Cause of death:
iii. Details of death: (max of 1000 chars)
iv. Date of discharge / /
1.3.2 Did the patient die after discharge? Yes No Not known
i. Date of death / / Not known
ii. Cause of death
1.4 Co-morbidity
1.4.1 Does the patient have any important co-morbid diseases? (please select all that apply)
a) Heart Disease f) Stroke
b) Peripheral Vascular Disease g) Liver Disease
c) Respiratory disease h) Active Cancer
d) Renal Failure i) None of the above
e) Diabetes 1.5 Medication on Admission
1.5.1 What treatment was the patient taking for Crohn’s Disease on admission? (select all that apply) a) 5-ASA f) Corticosteroids
b) Azathioprine g) Dietary Therapy
c) Mercaptopurine h) anti-TNF-
d) Methotrexate i) None
e) Antibiotics j) Other (e.g. trial medicine
please specify) 1.6 Smoking Status
1.6.1 What is the smoking status of the patient?
a) Current smoker c) Lifelong non-smoker/
ex-smoker
c) Not documented
1.7 Patient History
1.7.1 Did the patient have a pre-admission diagnosis of Crohn’s Disease? Yes No
1.7.2 What is the extent of the disease?
a) Small bowel only b) Colonic c) Ileo-colonic d) Perianal
e) Not known f) Other (please specify)
1.7.3 Has the patient had previous admissions to your hospital with Crohn’s Disease in the last two years? Yes No
i. If yes, how many times in the two years prior to this admission?
UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 83

UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 84
Section 2: Assessing the Severity of Crohn’s Disease 2.1 Severity of Disease
2.1.1 Was diarrhoea recorded as a symptom upon admission? Yes No Patient has Stoma
2.1.2 How many stools were passed in the 24 hours following admission?
Not documented
2.1.3 What was the highest recorded pulse rate during the 24 hours following admission? bpm
Not documented
2.1.4 What was the highest temperature recorded during the 24 hours following admission? . °C
Not documented
i. Did the patient have a fever (temperature >37.5°C on more than one occasion in 24 hours) within the first 7 days of admission Yes No
Not documented
2.1.5 Following admission, what was the initial result for:
i. CRP
Mg/L
Less than 5
Not documented
ii. Albumin g/L Not documented
iii. Hb . g/dL Not documented
iv. ESR mm/h-1 Not documented
2.2 Exclusion of Infection 2.2.1 Was a stool sample sent for Standard Stool Culture?
Yes No
i. Date sent: / /
2.2.2 Was a stool sample sent for CDT? Yes No i. Date sent: / /
2.3 Documentation of Sepsis
2.3.1 Were antibiotics given? Yes No Not documented
2.3.2 Were blood cultures taken? Yes No
i. Were the cultures: Positive Negative

UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 85
2.4 Imaging 2.4.1
Was an Ultrasound Scan performed? Yes i. Date requested / /
No ii. Date performed / /
iii. Date reported / /2.4.2
Was a CT Scan of the abdomen performed? Yes i. Date requested / /
No ii. Date performed / /
iii. Date reported / /
2.4.3 Was an MRI performed? Yes i. Date requested / /
No ii. Date performed / /
iii. Date reported / /2.4.4
Was an abscess found during imaging? Yes No
i. If drainage was undertaken, was it: a) Surgical b) Radiological
2.5 Weight Assessment and Dietetic Support
2.5.1 Was the patient’s weight measured during admission? Yes No
i. Was BMI measured? Yes No
2.5.2 Did a dietitian visit the patient? Yes No
2.5.3 Was dietary treatment initiated? Yes No
i. Was Crohn’s-specific dietary therapy prescribed? Yes No
2.5.4 Was parenteral nutrition required? Yes No 2.6 Use of anti-thrombotic therapies
2.6.1 Was the patient given: i. Prophylactic heparin Yes No
ii. Anti-thrombotic stockings Yes No
Section 3: Medical Interventions 3.1 Steroid Therapy
3.1.1 Were IV corticosteroids administered during this admission? i. Yes
ii. No, but oral steroids were administered iii. No, neither IV or Oral corticosteroids were administered

3.1.2 Which of the following steroids were prescribed?
a) Prednisolone
b) Budesonide
c) Hydrocortisone
i. Initial Dose Mg/day
3.1.3 Date therapy initiated or increased: / / 3.2 Blood Transfusion
3.2.1 What was the patient’s lowest recorded Hb level during admission? . g/dL
3.2.2 Was a blood transfusion given during admission? Yes No 3.3 Initiation of Treatment with anti-TNF- During Admission
3.3.1 Was anti-TNF- therapy given during this admission? Yes No
i. If yes, what date was the anti-TNF- therapy initiated? / /3.3.2
Is there evidence of a chest x-ray performed in the three months prior to the initiation of anti-TNF- therapy? Yes No
i. If yes, what was the date of the chest x-ray? / /
Section 4: Surgical Interventions 4.1 Surgical Therapy
4.1.1 Did the patient have surgery on this admission? Yes No
4.1.2 What date was the decision to operate made? / / Not known
4.1.3 Which Surgeon made the decision to operate? a) Consultant Colorectal Surgeon b) Consultant GI Surgeon (non-colorectal)
c) Consultant General Surgeon
d) Other Consultant Surgeon
e) Specialist Registrar
f) Other (please specify)
4.1.4 Was the patient seen by a stoma nurse during this admission? Yes No
If yes, what date was the patient first seen by a stoma nurse? / /
4.1.5 What was the date of surgery? / /
UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 86

UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 87
4.1.6 What was the grade of the operating surgeon?
a) Consultant Colorectal Surgeon b) Consultant GI Surgeon (non-colorectal)
c) Consultant General Surgeon
d) Other Consultant Surgeon
e) Specialist Registrar
f) Other (please specify)
4.1.7 What was the grade of the assisting surgeon? a) Consultant Colorectal Surgeon b) Consultant GI Surgeon (non-colorectal)
c) Consultant General Surgeon
d) Other Consultant Surgeon
e) Specialist Registrar
f) Other (please specify)
4.1.8 What were the indications for surgery ? a) Failure of Medical Therapy e) Stoma complications i) Dysplasia
b) Obstruction f) Perineal disease j) Cancer
c) Intra-abdominal Abscess g) Toxic megacolon k) Perforation
d) Intra-abdominal fistula h) Bleeding l) Other (please
specify) 4.1.9
Type of intervention: (Please select all that apply)
a) Segmental/Extended Colectomy e) Ileal/Jejunal
Resection i) Drainage of abscess
b) Subtotal Colectomy f) Resection of Intra-
abdominal Fistulaj) Formation of ileostomy
or colostomy
c) Protocolectomy g) Protectomy k) Revision of Stoma
d) Stricturoplasty h) Ileocolonic
Resection l) Perineal procedure
l) Other intervention (please specify)
4.1.9i Was the surgery done laparoscopically/ laparoscopically-assisted? Yes No
4.1.10 Was the ASA status recorded pre-operatively? Yes No
If yes, what was the status? 1 2 3 4 5 N/A

UK IBD Audit 2006 Crohn’s Disease Inpatient Proforma 88
4.2 Surgical Complications
4.2.1 Did the patient suffer from any of these complications following their surgery? (select all that apply)
a) Wound Infection e) Anastomotic leakage i) Ileus requiring TPN
b) Rectal stump complications f) Stoma complications j) Cardiac
c) Intra-abdominal bleeding g) Deep vein thrombosis (DVT) k) Respiratory
d) Intra-abdominal sepsis h) Pulmonary embolism (PE) l) No complications
m) Other (please specify) 4.3 Post-Operative Prophylactic Therapy
4.3.1 Was the patient prescribed any of the following drugs on discharge? (please select all that apply)
a) Azathioprine b) Mercaptopurine c) Metronidazole
d) 5-ASA e) Methotrexate f) None
g) Other (please specify) Section 5: Discharge Arrangements 5.1 Discharge Arrangements
5.1.1 Was an appointment made for the patient to be referred back to a:
i. Gastroenterologist Yes No
ii. Colorectal Surgeon Yes No
5.1.2 Was the patient taking oral steroids on discharge? Yes No N/A
5.1.3 Was a steroid reduction programme stated on discharge? Yes No N/A
5.1.4 Were bone protection agents prescribed? Yes No

UK IBD Audit 2006 Crohn’s Disease Outpatient Visits
Proforma
6.1 Patient History
6.1.1
Has the patient had previous outpatient visits for Crohn’s Disease at this hospital in the last 12 months? Yes No
6.1.2 How many times was the patient reviewed for their Crohn’s Disease in an outpatient’s
clinic in the 12 months prior to the start date of this admission?
6.1.3
Approximately how many times was the patient seen by the following staff in the 12 months prior to the start date of this admission? (If the patient was seen by more than one of the following staff in a single clinic visit please count each staff member individually)
i. Consultant ii. IBD Nurse Specialist iii. Specialist Registrar iv. SHO 6.2 Assessment of Crohn’s Activity
6.2.1
What was the date of the last visit at the Outpatient Department prior to admission? (If the last visit was the one which initiated the admission ignore it and use the previous one) / /
6.2.2
Number of liquid stools per day: Not documented
6.2.3 General well being: Well Mild symptoms Moderate symptoms Severe symptoms Not documented
6.2.4 Abdominal Pain: None Present Not documented
6.2.5 Abdominal Mass None Present Not documented
Mouth ulcers Arthralgia
Pyoderma Gangrenosum
6.2.6
Did the patient report any of the following complications at this clinical visit? Anal fissure
Fistula Erythaema Nodosum
UK IBD Audit 2006 Crohn’s Disease Outpatient Visits Proforma 89

Abcess Iritis None documented Other
i. CRP Not documented
6.2.7
What were the results for the following tests? ii. ESR
Not documented
iii. Albumin
Not documented
6.2.8
Was the patient weighed during this clinic visit? Yes No
Yes No Not documented 6.2.8ii
Was there evidence of unintentional weight loss of more than 3kgs prior to this clinic visit?
6.3 Smoking Status at first visit
6.3.1 What was the smoking status of the patient during this clinic visit? a) Current smoker c) Not documented b) Lifelong non-smoker/ex-smoker
6.4 Monitoring of immunosuppressive therapy 6.4.1
Was the patient taking any of these drugs in the 12 months prior to the start date of this admission?
Azathioprine Mercaptopurine Methotrexate None of these
6.4.2 Was the patient’s white blood cell (WBC) count routinely measured?
Yes
No
6.4.3 How often was WBC monitoring performed?
At least once a month Every 2-3 months Not documented Other
6.4.4
Did the patient’s WBC fall below 3x109 at any time during the 12 months prior to the start date of this admission?
Yes No Not known
6.4.5 If the white blood cell count was less than 3.0x109 what action was taken? Reduced dose Stopped drug No action taken
6.4.6 What was the outcome of the reduced white blood cell count?
No sequelae (resolved) Treatment required (e.g. prophylactic antibiotics) Admission
UK IBD Audit 2006 Crohn’s Disease Outpatient Visits Proforma 90
6.5 Use of Corticosteroids
6.5.1
Was the patient taking oral corticosteroids for their Crohn’s Disease in the 12 months prior to the start date of this admission? Yes No
6.5.2
Was there any point at which the patient was taking oral corticosteroids continuously for more than three months? Yes No
6.5.3 Were bone protection agents prescribed alongside corticosteroids? Yes No
6.5.4
Was bone densitometry measured within 12 months of initiation of the corticosteroid therapy? Yes No
6.6 Use of anti-TNF- therapy 6.6.1
Did the patient receive anti-TNF- therapy in the 12 months prior admission? Yes No
If yes
6.6.2
Was anti-TNF- therapy initiated at any point in the 12 months prior to the start date of this admission? Yes No
6.6.3
Did the patient have severely active Crohn’s Disease at the time anti-TNF- therapy was initiated? Yes No What was the CRP prior to the first anti-TNF- transfusion on record? mg/L 6.6.4
Not documented
6.6.5 Was the patient on immunosuppressive therapy at this time? Yes No If no, is there any evidence that the patient was intolerant of these
immunosuppressive therapies? Yes No
6.6.6 Was fistulating disease the primary reason for the decision to initiate anti-TNF- therapy? Yes No
6.6.7 Did the patient have a chest X-ray to exclude TB in the three months prior to initiation of anti-TNF- therapy? Yes No
UK IBD Audit 2006 Crohn’s Disease Outpatient Visits Proforma 91


Appendix 3 Pilot Sites
Addenbrooke's Hospital Bristol Royal Infirmary Causeway Hospital Chesterfield & North Derbyshire Royal Hospital Gloucestershire Royal Hospital Guy's & St Thomas' NHS Foundation Trust - (Guy's & St Thomas' Hospitals Combined) Hope Hospital John Radcliffe Hospital King George Hospital Lagan Valley Hospital Llandudno General Hospital Royal Berkshire Hospital Royal Glamorgan Hospital Royal Gwent Hospital Royal Liverpool University Hospital Royal London Hospital Royal United Hospital Sheffield Teaching Hospitals NHS Foundation Trust (Royal Hallamshire Hospital & Northern General Hospital Combined) Taunton & Somerset Hospital Torbay Hospital University Hospital of Wales, Cardiff University Hospital, Aintree Western General Hospital
---------------------------------------------------------------------------------------------------------------------------- Appendix 3 UK IBD Audit 2006 – Pilot Sites
92


---------------------------------------------------------------------------------------------------------------------------- Appendix 4 UK IBD Audit 2006 - Hospitals that submitted data to the audit
93
Appendix 4 Hospitals that submitted data to the audit
England East Midlands Chesterfield & North Derbyshire Royal Hospital Derby Hospitals NHS Foundation Trust - (Derby City General Hospital & Derbyshire Royal Infirmary Combined) Leicester General Hospital Leicester Royal Infirmary Lincoln County Hospital Louth County Hospital Nottingham City Hospital Pilgrim Hospital Queen's Medical Centre East of England Addenbrooke's Hospital Basildon Hospital Bedford Hospital Broomfield Hospital Colchester General Hospital Hemel Hempstead General Hospital Hinchingbrooke Hospital Ipswich Hospital James Paget Hospital Lister Hospital Luton & Dunstable Hospital Norfolk & Norwich University Hospital Queen Elizabeth Hospital, King's Lynn Watford General Hospital West Suffolk Hospital London Barnet General Hospital Ealing Hospital Epsom General Hospital Guy's & St Thomas' NHS Foundation Trust - (Guy's & St Thomas' Hospitals Combined) Hammersmith Hospitals NHS Trust - (Charing Cross & Hammersmith Hospitals Combined) Hillingdon Hospital Homerton University Hospital King George Hospital King's College Hospital Kingston Hospital Mayday Hospital Oldchurch Hospital Princess Royal University Hospital, Orpington Royal Free Hospital Royal London Hospital
St George's Hospital St Mark's Hospital St Mary's Hospital, London University College Hospital University Hospital, Lewisham West Middlesex Hospital Whipps Cross University Hospital Whittington Hospital North East Bishop Auckland General Hospital Darlington Memorial Hospital Freeman Hospital Friarage Hospital Hexham General Hospital James Cook University Hospital North Tyneside General Hospital Queen Elizabeth Hospital, Gateshead Royal Victoria Infirmary South Tyneside District Hospital Sunderland Royal Hospital University Hospital of Hartlepool University Hospital of North Durham University Hospital of North Tees Wansbeck General Hospital North West Arrowe Park Hospital Blackpool Victoria Hospital Burnley District General Hospital Countess of Chester Hospital Cumberland Infirmary Fairfield General Hospital Furness General Hospital Hope Hospital Lancashire Teaching Hospital NHS Foundation Trust - (Chorley & South Ribble Hospital and Royal Preston Hospital Combined) Leighton Hospital Macclesfield District General Hospital North Manchester General Hospital Rochdale Infirmary Royal Albert Edward Infirmary Royal Blackburn Hospital Royal Bolton Hospital Royal Liverpool University Hospital Royal Oldham Hospital

Southport District General Hospital Stepping Hill Hospital Tameside General Hospital University Hospital, Aintree University Hospitals of Morecambe Bay NHS Trust (Royal Lancaster Infirmary & Westmorland General Hospital Combined) Warrington District General Hospital West Cumberland Hospital Whiston Hospital Wythenshawe Hospital South Central John Radcliffe Hospital Milton Keynes General Hospital North Hampshire Hospital Royal Berkshire Hospital Southampton University Hospitals NHS Trust - (Royal South Hants Hospital & Southampton General Hospital Combined) South East Coast Darent Valley Hospital East Surrey Hospital Eastbourne District General Hospital Frimley Park Hospital Kent & Canterbury Hospital Kent & Sussex Hospital Princess Royal Hospital, Haywards Heath Queen Elizabeth The Queen Mother Hospital Royal Surrey County Hospital Royal Sussex County Hospital St Peter's Hospital St Richard's Hospital William Harvey Hospital Worthing Hospital South West Bristol Royal Infirmary Cheltenham General Hospital Derriford Hospital Dorset County Hospital Frenchay Hospital Gloucestershire Royal Hospital Great Western Hospital North Devon District Hospital Poole General Hospital Royal Bournemouth Hospital Royal Devon & Exeter Hospital Royal United Hospital Salisbury District General Hospital Taunton & Somerset Hospital Torbay Hospital Weston General Hospital
Yeovil District Hospital West Midlands Alexandra Hospital Birmingham Heartlands Hospital City Hospital, Birmingham George Eliot Hospital Hereford County Hospital Manor Hospital New Cross Hospital Queen's Hospital, Burton Russells Hall Hospital Sandwell General Hospital Shrewsbury & Telford Hospital NHS Trust - (Princess Royal Hospital, Telford & Royal Shrewsbury Hospital Combined) Solihull Hospital Staffordshire General Hospital University Hospital Birmingham NHS Foundation Trust (Queen Elizabeth Hospital, Birmingham & Selly Oak Hospital Combined) Walsgrave Hospital Warwick Hospital Worcestershire Royal Hospital Yorkshire and The Humber Airedale General Hospital Bradford Royal Infirmary Calderdale Royal Hospital Dewsbury & District Hospital Diana, Princess of Wales Doncaster Royal Infirmary Harrogate District Hospital Huddersfield Royal Infirmary Hull Royal Infirmary Leeds General Infirmary Mid Yorkshire Hospitals NHS Trust (Pinderfields General Hospital & Pontefract General Infirmary Combined) Rotherham District General Hospital Scarborough Hospital Scunthorpe General Hospital Sheffield Teaching Hospitals NHS Foundation Trust - (Northern General Hospital & Royal Hallamshire Hospital Combined) St James's University Hospital York Hospital Northern Ireland Eastern Health and Social Services Board Belfast City Hospital Downe Hospital Lagan Valley Hospital Mater Hospital
---------------------------------------------------------------------------------------------------------------------------- Appendix 4 UK IBD Audit 2006 - Hospitals that submitted data to the audit
94

Royal Victoria Hospital Ulster Hospital
Northern Health and Social Services Board Causeway Hospital United Hospitals Health & Social Services Trust (Antrim Hospital & Whiteabbey Hospital Combined) Western Health and Social Services Board Altnagelvin Area Hospital Sperrin Lakeland Health & Social Care NHS Trust (Erne Hospital & Tyrone County Hospital Combined) Scotland NHS Borders Borders General Hospital NHS Dumfries & Galloway Dumfries & Galloway Royal Infirmary NHS Forth Valley Stirling Royal Infirmary NHS Greater Glasgow & Clyde Inverclyde Royal Hospital Vale of Leven Hospital NHS Highland Belford Hospital Caithness General Hospital Raigmore Hospital NHS Lanarkshire Hairmyres Hospital Monklands District General Hospital Wishaw General Hospital NHS Lothian St John's Hospital at Howden Western General Hospital NHS Tayside Ninewells Hospital
Wales Mid & West Wales Bronglais General Hospital Neath Port Talbot Hospital Princess of Wales Hospital Singleton Hospital Withybush General Hospital North Wales Glan Clwyd Hospital Llandudno General Hospital Wrexham Maelor Hospital Ysbyty Gwynedd Hospital South East Wales Caerphilly & District Miner's Hospital Llandough Hospital Prince Charles Hospital Royal Glamorgan Hospital Royal Gwent Hospital University Hospital of Wales, Cardiff Islands Noble's Hospital, Isle of Man Princess Elizabeth Hospital, Guernsey
---------------------------------------------------------------------------------------------------------------------------- Appendix 4 UK IBD Audit 2006 - Hospitals that submitted data to the audit
95


Appendix 5 Hospitals that were invited to take part in the audit but did not participate
Aberdeen Royal Infirmary Ashford Hospital Barnsley District Hospital Bassetlaw District General Hospital Central Middlesex Hospital Chase Farm Hospital Chelsea & Westminster Hospital Clatterbridge Hospital Craigavon Area Hospital Crawley Hospital Daisy Hill Hospital Dr Gray's Hospital Glasgow Royal Infirmary Good Hope Hospital Halton General Hospital Harold Wood Hospital, Romford Hospital of St Cross Jersey General Hospital Kettering General Hospital Leigh Infirmary Lorn and Islands District General Hospital Medway Maritime Hospital Mid Ulster Hospital Middlesex Hospital Montagu Hospital Morriston Hospital Nevill Hall Hospital Newark Hospital Newham University Hospital North Middlesex Hospital Northwick Park Hospital Ormskirk & District General Hospital Papworth Hospital Perth Royal Infirmary Peterborough District Hospital Pontefract General Infirmary Prince Philip Hospital Princess Alexandra Hospital, Harlow Royal Cornwall Hospital Royal Hampshire County Hospital Seacroft Hospital Selly Oak Hospital Southern General Hospital Southmead Hospital St Mary's Hospital Stobhill General Hospital Stoke Mandeville Hospital
Tyrone County Hospital Victoria Hospital Victoria Infirmary West Cornwall Hospital West Wales General Hospital Western Infirmary Western Isle Hospital Westmorland General Hospital Wexham Park Hospital Whiteabbey Hospital Wycombe Hospital
---------------------------------------------------------------------------------------------------------------------------- Appendix 5 UK IBD Audit 2006 – Non Participating Hospitals
96


Appendix 6
UK IBD Audit 2006 National Report – List of IBD Standards Unless directly referenced as otherwise the following standards have been agreed through consensus by the UK IBD Audit Steering Group. The numbers next to each standard relate to the corresponding question from the UK IBD Audit 2006 proformas (Organisation & Structure, Ulcerative Colitis inpatient, Crohn’s Disease inpatient & outpatient).
Organisation & Structure of IBD services General Hospital Demographics Standard: Hospitals where surgery is performed for IBD should have ITU beds with 24 hr care by anaesthetists/intensivists on-site (UK IBD Audit Steering Group). Inpatient Activity Standard: 2.3 Patients undergoing surgery for ulcerative colitis should have the opportunity to have ileo-anal pouch surgery (1BSG guidelines) either locally, if available, or at a regional centre. Gastroenterology Services Standards: 3.1 Specialty triage of emergency admitted IBD patients to appropriate medical or surgical gastroenterology (UK IBD Audit Steering Group). 3.2 No more than 3 patients per lavatory (UK IBD Audit Steering Group). 3.3 At least 2 WTE Medical Gastroenterologists (UK IBD Audit Steering Group). 3.4 & 3.5 At least 1 IBD specialist nurse with at least 5 sessions dedicated to IBD (UK IBD Audit Steering Group). Colorectal Services Standards: 4.1 At least 2 FTE Colorectal surgeons (UK IBD Audit Steering Group). 4.3 & 4.4 At least 1 stoma-care nurse specialist with at least 5 sessions dedicated to stoma care (UK IBD Audit Steering Group). Multi-Disciplinary Working Standards: 5.1 Sites should have a searchable data-base to allow adequate audit (UK IBD Audit Steering Group). 5.2 A weekly multi-disciplinary meeting should take place between gastroenterologists, colorectal surgeons and radiologists (UK IBD Audit Steering Group). There should be regular histopathology conferences (at least 1 per month) (UK IBD Audit Steering Group). 5.3 & 5.4 Each hospital should have a radiologist and pathologist with a special interest in gastroenterology (UK IBD Audit Steering Group).
97
UK IBD Audit Report 2006 List of IBD Standards
Dietetics and Nutritional Services Standards: 6.1-6.3 Each site should have a multidisciplinary nutrition team (UK IBD Audit Steering Group). This team should conduct ward rounds at least twice a week (UK IBD Audit Steering Group). 6.4 At least 5 dietetic sessions per week should be dedicated to gastroenterological diseases ( includes inpatients and outpatients) (UK IBD Audit Steering Group). Outpatient Services Standards: 7.1 – 7.3 A clear process for telephone access for ill patients should be established that allows review within one week. Written information for patients with IBD should be readily available in clinic areas (BSG guidelines). 7.4 Joint or parallel clinics should exist to discuss and refer patients between medical and surgical teams (UK IBD Audit Steering Group). Patient Information Standard: 8.1 Written information on IBD should be provided to each patient with IBD (BSG Guidelines). Monitoring of established immunosuppresive therapy Standard: 9.1 Should be a written policy for the mechanism of monitoring immunosuppressive therapy (2National Patient Safety Agency) IBD Support Services Standard: 10.1 There should be regular (usually 1 or 2 per year) transition clinics involving paediatricians and adult gastroenterologists for hand over of patients to adult services (UK IBD Audit Steering Group). These can be done on a regional basis (UK IBD Audit Steering Group). Management of Ulcerative Colitis Standard: 11.1 Written Trust guidelines should exist for the management of acute or severe colitis (UK IBD Audit Steering Group).
98

UK IBD Audit Report 2006 List of IBD Standards
Interactions between your hospital and patients and patient groups Standard: 12.1 There should be regular meetings (at least once a year and usually on a regional basis) between groups of patients with IBD (and their relatives or carers) and hospital staff, this should involve medical, surgical and nursing staff (UK IBD Audit Steering Group).
Ulcerative Colitis (inpatient) Admission Standards: 1.1.5 Patients should be transferred to the care of a medical gastroenterologist or colorectal surgeon within 24 hours of admission (UK IBD Audit Steering Group). 1.1.6 Patients should be seen by a consultant gastroenterologist or colorectal surgeon within 3 days of admission (UK IBD Audit Steering Group). 1.1.8 Patients should be seen by an IBD specialist nurse during admission (UK IBD Audit Steering Group). 1.1.9 Patients should be transferred to a specialist gastroenterology ward (UK IBD Audit Steering Group). Assessment: Severity of Disease Standards: 2.2.1 Patients should have stool frequency documented in first 24 hours of admission (BSG guidelines). 2.2.2 & 2.2.3 Pulse rate and temperature to be taken at least 4 times in first 24 hours of admission. (BSG guidelines) 2.2.4 Patients should have haemoglobin, albumin and CRP (or ESR) performed (BSG guidelines). 2.2.5 & 2.2.6 Patients with diarrhoea should have a standard stool culture and CDT performed (BSG guidelines) within 48 hours of admission (UK IBD Audit Steering Group). Assessment: Endoscopic Assessment Standards: 2.3.1 New cases of suspected ulcerative colitis admitted to hospital should have endoscopic sigmoidoscopy confirmation within 3 days of admission (UK IBD Audit Steering Group). 2.3.2 Endoscopy report should contain an assessment of severity (UK IBD Audit Steering Group). 2.3.3 New cases of ulcerative colitis admitted to hospital should have biopsies taken for histology and these should be reported within 5 days (UK IBD Audit Steering Group).
99

UK IBD Audit Report 2006 List of IBD Standards
Monitoring of Colitis – Post-Admission: General information Standards: 3.1.1 Patients should have prophylactic heparin (BSG guidelines). 3.1.3 and 3.1.4 Pulse rate and temperature monitored at least 4 times a day (BSG guidelines). 3.1.7 Stool frequency should be monitored daily (BSG guidelines). 3.1.8 and 3.1.10 ESR, or CRP should be monitored every 24–48 hours in severely active ulcerative colitis (BSG guidelines). Monitoring of Colitis – Post-Admission: Radiology Standards: 3.2.1 Patients should have a plain abdominal X-ray (BSG guidelines) with 24 hours of admission (UK IBD Audit Steering Group). 3.2.2 If toxic megacolon is present the abdominal X-ray should be repeated the next day if emergency surgery is not undertaken (BSG guidelines). Medical Intervention: Steroid therapy Standards: 4.1.1 and 4.1.2 Appropriate intravenous steroid therapy ( 400 mg hydrocortisone or 60mg methylprednisolone) (BSG guidelines) should be initiated within 24 hours of admission (UK IBD Audit Steering Group) in a suspected severe attack of ulcerative colitis. 4.1.4 (together with 3.1.9) If the attack of colitis is not settling within 72 hours of appropriate steroid therapy the risk of colectomy is high. If there is no response to appropriate corticosteroids within 3 days, rescue therapeutic options need to be discussed with the patient (BSG guidelines)(either surgery, ciclosporin or anti-TNFα therapy). A consultant colorectal surgeon should discuss the surgical options with the patient (BSG guidelines). Medical Intervention: Initiating Ciclosporin Therapy Standards: 4.3.1 Creatinine should be measured (BSG guidelines) within the 48 hours (UK IBD Audit Steering Group) prior to initiation of ciclosporin . 4.3.2 and 4.3.3 Magnesium and cholesterol should be measured (BSG guidelines) within the 48 hours (UK IBD Audit Steering Group) prior to initiation of intravenous ciclosporin. Medical Intervention: Monitoring Ciclosporin Therapy Standards: 4.4.1 and 4.4.2 Creatinine and FBC should be monitored daily (UK IBD Audit Steering Group). 4.4.3 Ciclosporin levels should be checked daily after 3 days of IV therapy (UK IBD Audit Steering Group).
100

UK IBD Audit Report 2006 List of IBD Standards
Surgical Interventions Standards: 5.1.2 Consultant colorectal surgeons should be involved with the discussion with the patient regarding the decision to operate (BSG guidelines). 5.1.4 Patients having resectional surgery for Ulcerative Colitis should see a stoma nurse prior to the operation (BSG guidelines) 5.1.5 and 5.1.6 Operations should be performed or assisted by a consultant colorectal surgeon (UK IBD Audit Steering Group). 5.1.9 ASA status should be recorded pre-operatively (UK IBD Audit Steering Group). . Discharge Arrangements Standards: 6.1.1 Patients should be followed up by a gastroenterologist or colorectal surgeon (UK IBD Audit Steering Group). 6.1.3 Patients discharged on oral steroids should have a steroid reduction programme stated on discharge (UK IBD Audit Steering Group. 6.1.4 Patients on oral steroids should be co-prescribed bone protection agents (such as calcium and vitamin D or bisphosphonates (BSG guidelines).
Crohn’s Disease (inpatient) Admitting Speciality Standards: 1.2.1 Patients admitted with Crohn’s Disease should be under the care of medical gastroenterologists or colorectal surgeon within 24 hours of admission (UK IBD Audit Steering Group). 1.2.2 Patients should be transferred to a specialist gastroenterology ward (UK IBD Audit Steering Group). 1.2.3 and 1.2.4. All patients should be seen by a consultant gastroenterologist or colorectal surgeon within 3 days of admission (UK IBD Audit Steering Group). 1.2.5 All patients should be seen by an IBD specialist nurse during admission (UK IBD Audit Steering Group). Smoking Status Standard: 1.6.1 Smoking status should be documented (BSG guidelines) and smoking cessation support should be offered. Assessment: Severity of Disease Standards: 2.1.1 Patients should have stool frequency documented in the first 24 hours following admission (UK IBD Audit Steering Group). 2.1.5 Patients should have haemoglobin, albumin and CRP (or ESR) performed in the first 24 hours following admission (UK IBD Audit Steering Group).
101
UK IBD Audit Report 2006 List of IBD Standards
Assessment: Exclusion of Infection Standards: 2.2.1 & 2.2.2 Patients with diarrhoea should have a standard stool culture and CDT performed within 48 hours of admission (UK IBD Audit Steering Group). Assessment: Documentation of Sepsis Standards: 2.3.1 & 2.3.2 Patients with fever (>37.5° C on two occasions) should have blood cultures performed (UK IBD Audit Steering Group). Assessment: Imaging Standards: 2.4 For suspected abdominal sepsis, imaging should be performed within 48 hours of request and reported within 24 hours of being done (UK IBD Audit Steering Group). Assessment: Weight Assessment and Dietetic Support Standards: 2.5.1 Patients should be weighed (BSG guidelines) and BMI calculated (UK IBD Audit Steering Group). 2.5.2 Non-elective admissions should be seen by a dietician (UK IBD Audit Steering Group). 2.5.3 Nutritional support should be provided for malnourished patients (BSG guidelines) Assessment: Use of anti-thrombotic therapies Standard: 2.6.1 Patients should have prophylactic heparin (BSG guidelines). Medical Interventions: Blood Transfusion Standard: 3.2.1 Patients with a haemoglobin level of less than 10g/dL should be considered for blood transfusion or iron infusion (UK IBD Audit Steering Group). Medical Intervention: Initiation of Treatment with anti-TNF- during admission Standard: 3.3.2 All patients given anti-TNF-α for the first time should have a chest X-ray within the previous 3 months (3Joint Tuberculosis Committee of the BTS in conjunction with the BSG and British Society of Rheumatology).
102

UK IBD Audit Report 2006 List of IBD Standards
Surgical Interventions Standards: 4.1.3 Consultant colorectal surgeons should be involved with the discussion with the patient regarding the decision to operate (BSG guidelines). 4.1.4 Patients having resectional surgery for Crohn’s Disease should see a stoma nurse prior to operation (BSG guidelines). 4.1.6 & 4.1.7 Operation should be performed or assisted by a consultant colorectal surgeon (UK IBD Audit Steering Group). 4.1.10 Patients should have ASA status documented prior to surgery (UK IBD Audit Steering Group). Post-Operative Prophylactic Therapy Standard: 4.3.1 Prophylactic therapy to try to reduce recurrence should be discussed with Crohn’s Disease patients having resectional surgery with anastomosis (BSG guidelines).
Discharge Arrangements Standards: 5.1.1 and 5.1.2 Patients should be followed up by a gastroenterologist or colorectal surgeon (UK IBD Audit Steering Group). 5.1.3 Patients discharged on oral steroids should have a steroid reduction programme stated on discharge (UK IBD Audit Steering Group). 5.1.4 Patients on oral steroids should be co-prescribed bone protection agents (such as calcium and vitamin D or bisphosphonates (BSG guidelines).
Crohn’s Disease (outpatient)
Patient History Standard: 6.1.3 Continuity of care in hospital outpatient visits matters to patients - patients dislike seeing different individuals at each visit (BSG guidelines). Patients should be offered the opportunity to see an IBD specialist (nurse or doctor) at last once a year. Assessment of Crohn’s Activity Standard: 6.2.1 – 6.2.8i Patients should have general well being, stool frequency, presence and severity of abdominal pain documented (UK IBD Audit Steering Group). Weight should be documented (BSG guidelines). CRP (ESR) and albumin should be checked (UK IBD Audit Steering Group). Smoking Status Standard: 6.3.1 Smoking status should be documented (BSG guidelines) and smoking cessation support should be offered (UK IBD Audit Steering Group).
103

UK IBD Audit Report 2006 List of IBD Standards
Monitoring of immunosuppressive therapy Standard: 6.4.2 – 6.4.3 Full blood count should be monitored at least 3 monthly for patients on established immunosuppressive therapy (BSG guidelines) Use of Corticosteroids Standards: 6.5.2 Prolonged use of steroid therapy is of no benefit in maintaining remission in Crohn’s Disease, increases the risk of septic complications and is associated with an increased mortality. Prolonged use of steroids (> 3 months oral prednisolone or budesonide) should be avoided. 6.5.3 Patients on oral steroids should be co-prescribed bone protection agents (BSG guidelines) Use of anti-TNF- therapy Standards: 6.6.1 Patients initiated on infliximab should have severely active Crohn’s Disease (4NICE guidance). 6.6.5 All patients receiving infliximab therapy should be on concomitant immunosuppressive therapy if tolerated (BSG guidelines). 6.6.7 Infliximab treated patients should have a documented chest X-ray within 3 months prior to first treatment (Joint Tuberculosis Committee of the BTS in conjunction with the BSG and British Societies of Rheumatology). References 1Carter MJ, Lobo AJ, Travis SP; IBD Section, British Society of Gastroenterology. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2004;53 Suppl 5:V1-16 2National Patient Safety Agency 3Ormerod LP ,Milburn HJ,Gillespie S,et al.BTS recommendations for assessing risk and for managing M tuberculosis infection and disease in patients due to start anti-TNF alpha treatment. Thorax Published Online First:29 July 2005.doi: 10.1136/thx.2005.046797. 4NICE
104