Embed Size (px)
Citation preview
Policy & Procedures Manual Updated: March 20, 2003 New Amended
Section Title: Benefits Administration - Adjudication & Compensation Subject: Permanent Impairment Rating Schedule Effective Date: For accidents occurring between October 1, 1996 to March 31, 2000, inclusive
GENERAL INFORMATION The Workers Compensation Act, sections 4(9) and 38 deal with impairment awards. These awards are calculated by determining a rating which represents the percentage of impairment as it relates to the whole body. The award is not related to loss of earning capacity nor is it a proxy for loss of earning capacity. A. POLICY
1. The degree of impairment will be established by the Healthcare Management Services Department of the Workers Compensation Board in accordance with this policy. The degree of impairment established by this Department can only be altered on review and approval by the Executive or Senior Director responsible subject to the normal appeal process.
2. Whenever possible, and reasonable, impairment ratings will be established strictly in accordance
with the schedule attached as appendix A. 3. In the event that the Healthcare Management Services Department feels that strict adherence
would create an injustice, or if it is felt that an impairment exists that is not covered by the schedule, Healthcare Management Services may deem it just and fair to establish an impairment rating that is not specifically covered by the schedule. In such cases they may use information other than the schedule such as the American Medical Association Guides to the Evaluation of Permanent Impairment established for a similar purpose. In such cases the award will not be official until it is reviewed and approved by the Director of Healthcare Management Services. The Healthcare Management Services Department will document the case and explain the justification for the non-scheduled award in full. Awards in excess of 20% must be reviewed and approved by the Director of Healthcare Management Services.
4. If a worker had a pre-existing condition the worker is eligible for an impairment award based
on the difference between the new combined rating and the rating assigned to the pre-existing condition. The Healthcare Management Services Department will assign a fair rating to the pre-existing condition based on the best information available.
Section Policy 40 44.90.10.03
WCB Policy 44.90.10.03 Page 2
Policy & Procedures Manual Updated: February 22, 2000 New Amended
5. Healthcare Management Services will assign an impairment rating based on file information, or
information from the attending physician, if such information is available and the impairment rating is less than 20%. Impairment ratings of 20% or greater can be confirmed without an examination if it is apparent from objective evidence, such as an x-ray of an amputated limb, what the rating should be. In other cases the worker will be asked to submit to an examination by a Healthcare Management Services physician or a physician chosen by the WCB. If the impairment rating has been appealed the rating will be performed by Healthcare Management Services or a physician ordered by the Appeal Commission.
6. The appropriate time to assess an injured worker for a permanent impairment award will be the
subject of guidelines established by the Healthcare Management Services Department. B. REFERENCES Workers Compensation Act, sections 4(9) and 38 Appendix A - Permanent Impairment Rating Schedule History: 1. Initial adoption of a permanent disability rating schedule in March, 1946. 2. Permanent Impairment Rating Schedule approved by Board Order 152/86 as a
compilation/recording of past policies, directives and practices, effective August 20, 1986. 3. Board Order 152/86 revised by Board Order 42/89 on March 15, 1989 to incorporate "minimum
awards". 4. Permanent Partial Disability Awards for Disfigurement adopted by Board Order 67/89 on April 24,
1989. 5. Policy 44.70.10 - Permanent Impairment Rating Schedule approved by Board Order 12/92 on
March 31, 1992, effective immediately for the rating of impairments after that date. Schedule revised to incorporate previously approved changes and recommendations of healthcare professionals. The majority of changes expand upon and clarify the original schedule, and reflect amendments to The Workers Compensation Act effective January 1, 1992.
6. Policy re-numbered to 44.90.10 on issue to Policy Manual. 7. Policy updated for current position and division titles, May 2, 1994. 8. Permanent Impairment Rating Schedule amended by Board Order 32/96, on September 25, 1996 to
correct specific omissions/errors and incorporate two amendments (partial loss of movement of finger, impairment of shoulder mobility) for all decisions (initial, reconsideration, and appeal) effective October 1, 1996
9. Permanent Impairment Rating Schedule amended by Board Order 6/2000 on February 22, 2000, which replaces the Hearing Impairment section for claims arising from accidents on or after April 1, 2000. Former Policy re-issued as 44.90.10.01.
10. Permanent Impairment Rating Schedule – Appendix A “Impairment of Hearing” section amended by Board Order 03/03 effective January 31, 2003. Former Policy reissued as 44.90.10.01 and 44.90.10.02.
11. September 1, 2009 policy updated to clarify effective date.

WCB Policy 44.90.10.03 Page 3
Policy & Procedures Manual Updated: February 22, 2000 New Amended
12. The policy was updated by Board Order No. 34/14 on October 30, 2014 effective January 1, 2015.
This policy was reissued as 44.90.10.03.
PERMANENT IMPAIRMENT RATING SCHEDULE
THE WORKERS COMPENSATION BOARD OF MANITOBA
A general summation of established practice, and scheduled ratings from various provincial jurisdictions, employed regularly by the Workers Compensation Board of Manitoba as guidelines for the evaluation of permanent impairment........
INDEX INTRODUCTION TO SCHEDULE............................................................................................................1 HAND (AMPUTATIONS AND LOSS OF MOBILITY)...........................................................................4 UPPER EXTREMITY (AMPUTATION AND IMPAIRED FUNCTION)................................................9 LOWER EXTREMITY (AMPUTATION AND IMPAIRED FUNCTION)............................................13 SPINE...........................................................................................................................................................16 JAW..............................................................................................................................................................17 REPRODUCTIVE AND URINARY SYSTEM.........................................................................................17 HEMOPOIETIC AND LYMPHATIC SYSTEM.......................................................................................17 GASTRO-INTESTINAL SYSTEM............................................................................................................18 IMPAIRMENT OF SPECIAL SENSES.....................................................................................................18 IMPAIRMENT OF HEARING...................................................................................................................21 VIBRATION-INDUCED WHITE FINGER DISEASE.............................................................................26 NERVOUS SYSTEM..................................................................................................................................26 BRAIN..........................................................................................................................................................28 DISFIGUREMENT......................................................................................................................................30 MYOCARDIAL INFARCTION.................................................................................................................31 RESPIRATORY (INDUSTRIAL LUNG DISEASES)..............................................................................32 PSYCHOLOGICAL....................................................................................................................................33 EVALUATION OF PSYCHIATRIC IMPAIRMENT...............................................................................40 CANCER......................................................................................................................................................41 COMBINED VALUES CHART.................................................................................................................44
APPENDIX A
- 1 -
GUIDELINES FOR PERMANENT IMPAIRMENT EVALUATION INTRODUCTION TO SCHEDULE:
The rating schedule is designed to measure the degree of permanent physical impairment of body
function following an injury for the purpose of calculating an award in accordance with Sections
4(9) and 38 of the Workers Compensation Act.
Permanent impairment is evaluated by conducting a medical examination of the worker or by
reviewing the medical history documented on file as described in the policy statement.
Evaluation of permanent impairment is made when treatment has been completed, or when, in the
opinion of the Board’s physicians, the medical condition has stabilized and no further improvement
is expected. The timing of the evaluation, therefore, varies according to the individual’s
circumstances.
Permanent impairment is measured by the following factors: loss of a part of the body; loss of
mobility in the joints; loss of function of any organs of the body identified in the schedule; and
cosmetic deformity of the body.
Currently for Manitoba Workers Compensation Board purposes, the permanent impairment
evaluation is administratively converted into an impairment award according to the Permanent
Impairment Rating Schedule.
- 2 - TYPES OF EVALUATIONS OR RATINGS:
There are two types of evaluations for permanent impairment made by the physicians who work
for the Workers Compensation Board: schedule ratings and judgement ratings.
Schedule ratings refer to the percentage values shown in this book for specific injuries. Where
the injury or impairment is straight forward, such as in cases of amputations, blindness, etc., it is
assessed at the percentage value shown.
Some types of impairment of function of the body do not lend themselves to exact
measurement. These require judgement on part of the medical examiner. Judgement ratings are
made to determine a percentage of impairment when the impairment does not fit into a specific
category of the existing schedule, but must be within the parameters as outlined in the schedule.
The figures outlined in the schedule are percentages of impairment of the total body. Multiple
injuries, due to a single accident, resulting in more than one impairment are evaluated on the
basis of the whole person, rather than by adding the individual values. This is done with the aid
of a combined values chart, as established by the American Medical Association Guides to the
Evaluation of Permanent Impairment. (See Combined Value Chart, page 54).
As well, in the event of multiple injuries, the impairment rating may be enhanced in order to
reflect the cumulative functional effect. Enhancement is particularly important in dealing with
finger injuries, loss of vision, and loss of hearing; therefore, the enhancement factor has been
considered in the development of the rating schedule, for these particular conditions.
Enhancement is considered to be relevant in respect of injuries which involve mirror parts of
bilateral structures; e.g., both wrists, both knees. In these instances, an enhancement factor of
up to 50% of the lesser impairment is awarded. The ratings must not be disproportionate when
applied to the whole person and are therefore subject to the combined values chart.

- 3 -
Impairment rating for the loss of function of an extremity cannot exceed the rating allowed for
amputation of that extremity. Multiple impairments affecting a single extremity, or part thereof,
may be calculated on the basis of the combined values chart, or as a percentage loss of total
function for the extremity.
- 4 -
HAND (AMPUTATIONS AND LOSS OF MOBILITY) AMPUTATIONS:
Finger amputations are rated in accordance with the detailed hand charts (see page 8); and
partial amputations of a phalanx are rated on a judgement basis having regard to the whole
value of the phalanx and the percentage affected by amputation.
If a single finger is involved, the single finger chart is used.
For multiple finger amputations, the corresponding multiple chart is used (refer to page 8).
The charts are used by beginning at the DIP joint and assign values to the distal phalanx from
the chart corresponding to the number of fingers having impairment at or proximal to the distal
joint. Then proceeding to the PIP joint and assigning values to the middle phalanx from the
chart corresponding to the number of fingers having impairment at or proximal to the middle
phalanx. Then proceeding to the MP joint, and in a similar fashion assigning values to the
proximal phalanges.
PARTIAL LOSS OF MOVEMENT/FUNCTION:
Impairment ratings for digit injuries take into consideration loss of joint movement as well as
amputation, and the detailed hand charts are also used.
When a finger joint is ankylosed in a position of function (or in an acceptable position), the
rating is one-half of what it would be for an amputation at that level. If a joint is ankylosed in
a position that is not functional, and there is some good reason why surgical correction will not
be done, the rating could equal up to the rating for amputation of that joint.
- 5 -
The impairment rating for partial loss of movement will be proportional to the amount of
movement that is lost. In as much as there are great variations from person to person in ranges
of when there is a completely normal digit to compare with, loss of movement can be
determined by comparing the movement in the joint being examined with the movement in the
normal joint on the opposite hand.
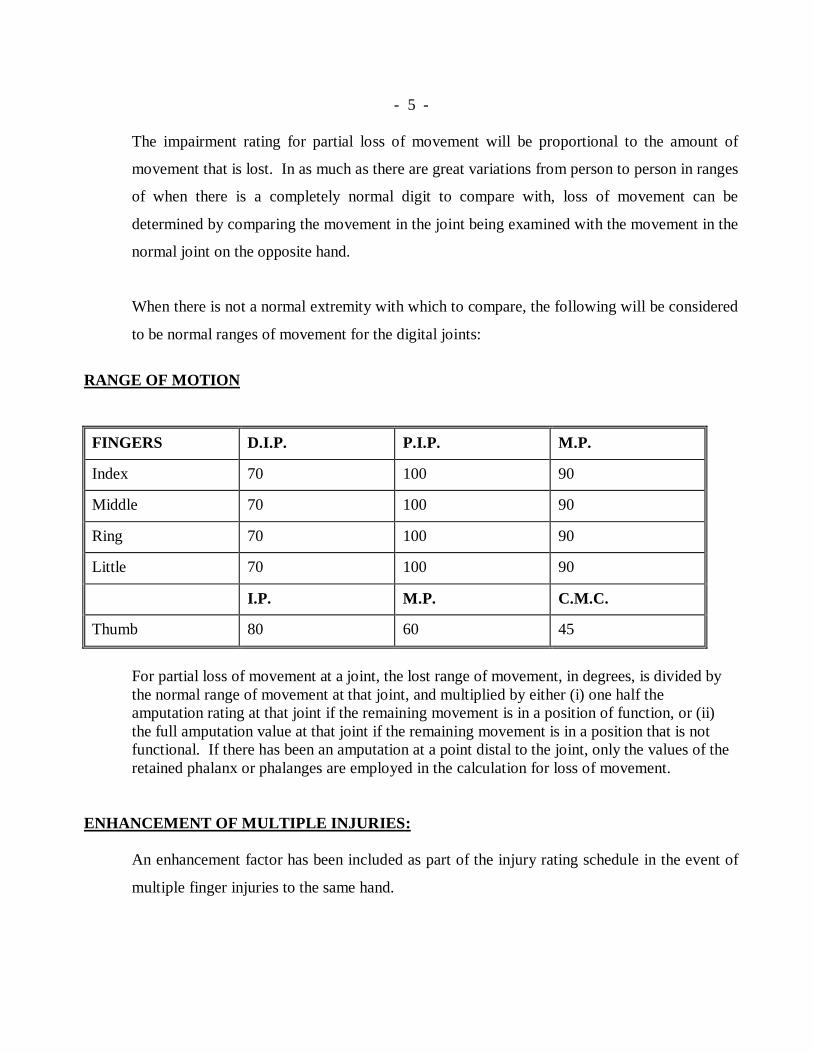
When there is not a normal extremity with which to compare, the following will be considered
to be normal ranges of movement for the digital joints:
RANGE OF MOTION
FINGERS D.I.P. P.I.P. M.P.
Index 70 100 90
Middle 70 100 90
Ring 70 100 90
Little 70 100 90
I.P. M.P. C.M.C.
Thumb 80 60 45
For partial loss of movement at a joint, the lost range of movement, in degrees, is divided by the normal range of movement at that joint, and multiplied by either (i) one half the amputation rating at that joint if the remaining movement is in a position of function, or (ii) the full amputation value at that joint if the remaining movement is in a position that is not functional. If there has been an amputation at a point distal to the joint, only the values of the retained phalanx or phalanges are employed in the calculation for loss of movement.
ENHANCEMENT OF MULTIPLE INJURIES:
An enhancement factor has been included as part of the injury rating schedule in the event of
multiple finger injuries to the same hand.
- 6 - As well, an enhancement factor of 50% of the lesser impairment is warranted in respect to
injuries which involve identical parts of bilateral structures, although the ratings must not be
disproportionate when applied to the whole person and are therefore subject to the combined
values chart.
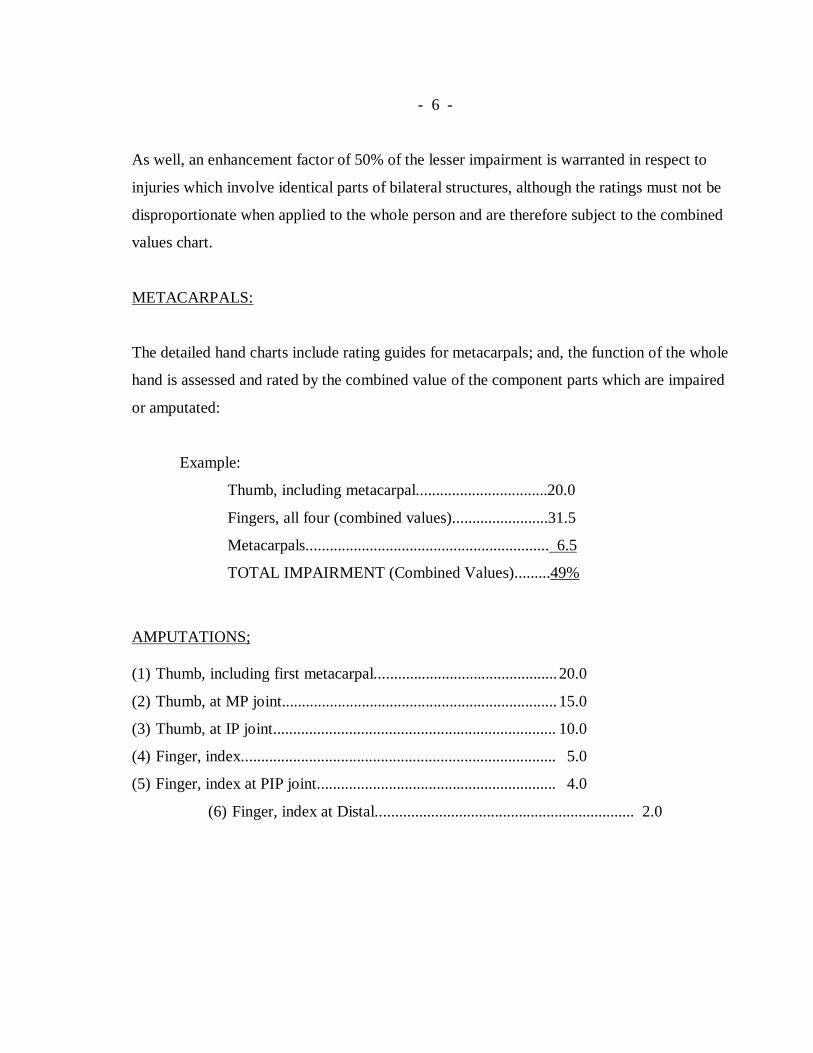
METACARPALS:
The detailed hand charts include rating guides for metacarpals; and, the function of the whole
hand is assessed and rated by the combined value of the component parts which are impaired
or amputated:
Example:
Thumb, including metacarpal.................................20.0
Fingers, all four (combined values)........................31.5
Metacarpals............................................................. 6.5
TOTAL IMPAIRMENT (Combined Values).........49%
AMPUTATIONS; (1) Thumb, including first metacarpal.............................................. 20.0
(2) Thumb, at MP joint..................................................................... 15.0
(3) Thumb, at IP joint....................................................................... 10.0
(4) Finger, index............................................................................... 5.0
(5) Finger, index at PIP joint............................................................ 4.0
(6) Finger, index at Distal................................................................. 2.0
- 7 -
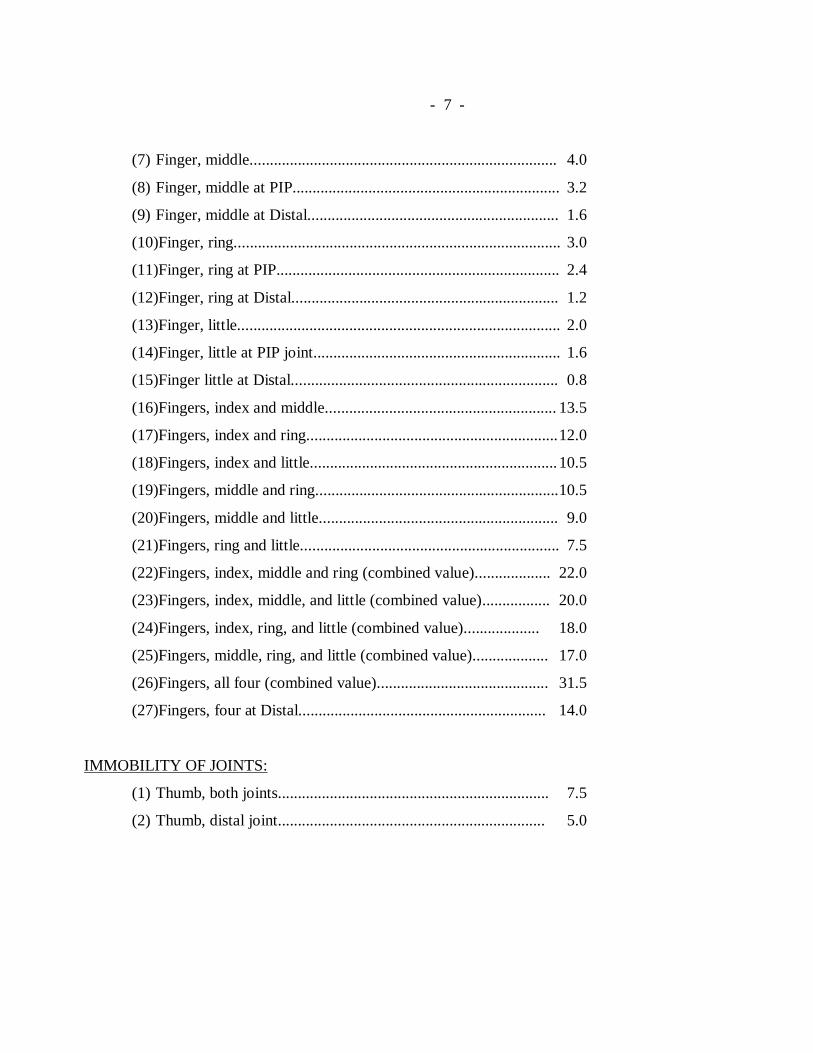
(7) Finger, middle............................................................................. 4.0
(8) Finger, middle at PIP................................................................... 3.2
(9) Finger, middle at Distal............................................................... 1.6
(10)Finger, ring.................................................................................. 3.0
(11)Finger, ring at PIP....................................................................... 2.4
(12)Finger, ring at Distal................................................................... 1.2
(13)Finger, little................................................................................. 2.0
(14)Finger, little at PIP joint.............................................................. 1.6
(15)Finger little at Distal................................................................... 0.8
(16)Fingers, index and middle.......................................................... 13.5
(17)Fingers, index and ring............................................................... 12.0
(18)Fingers, index and little.............................................................. 10.5
(19)Fingers, middle and ring............................................................. 10.5
(20)Fingers, middle and little............................................................ 9.0
(21)Fingers, ring and little................................................................. 7.5
(22)Fingers, index, middle and ring (combined value)................... 22.0
(23)Fingers, index, middle, and little (combined value)................. 20.0
(24)Fingers, index, ring, and little (combined value)................... 18.0
(25)Fingers, middle, ring, and little (combined value)................... 17.0
(26)Fingers, all four (combined value)........................................... 31.5
(27)Fingers, four at Distal.............................................................. 14.0
IMMOBILITY OF JOINTS:
(1) Thumb, both joints.................................................................... 7.5
(2) Thumb, distal joint................................................................... 5.0

- 8 -
HAND CHART
- 9 -
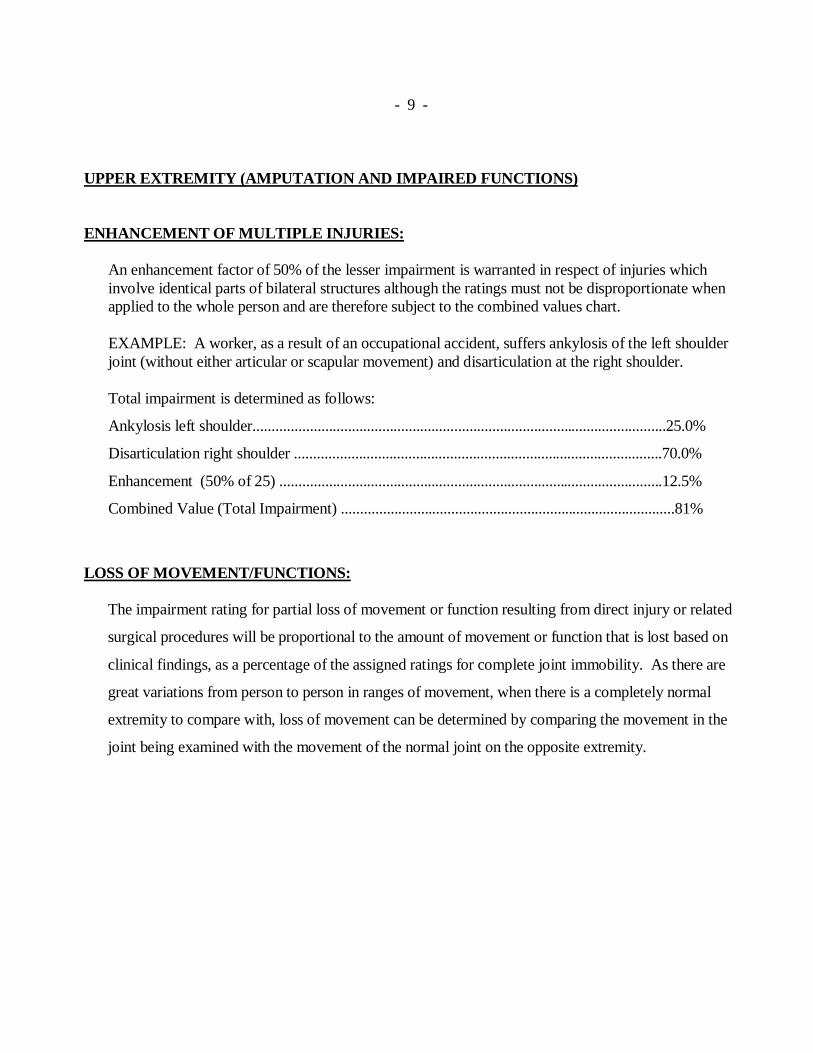
UPPER EXTREMITY (AMPUTATION AND IMPAIRED FUNCTIONS) ENHANCEMENT OF MULTIPLE INJURIES:
An enhancement factor of 50% of the lesser impairment is warranted in respect of injuries which involve identical parts of bilateral structures although the ratings must not be disproportionate when applied to the whole person and are therefore subject to the combined values chart. EXAMPLE: A worker, as a result of an occupational accident, suffers ankylosis of the left shoulder joint (without either articular or scapular movement) and disarticulation at the right shoulder.
Total impairment is determined as follows:
Ankylosis left shoulder.............................................................................................................25.0%
Disarticulation right shoulder .................................................................................................70.0%
Enhancement (50% of 25) .....................................................................................................12.5%
Combined Value (Total Impairment) ........................................................................................81%
LOSS OF MOVEMENT/FUNCTIONS:
The impairment rating for partial loss of movement or function resulting from direct injury or related
surgical procedures will be proportional to the amount of movement or function that is lost based on
clinical findings, as a percentage of the assigned ratings for complete joint immobility. As there are
great variations from person to person in ranges of movement, when there is a completely normal
extremity to compare with, loss of movement can be determined by comparing the movement in the
joint being examined with the movement of the normal joint on the opposite extremity.
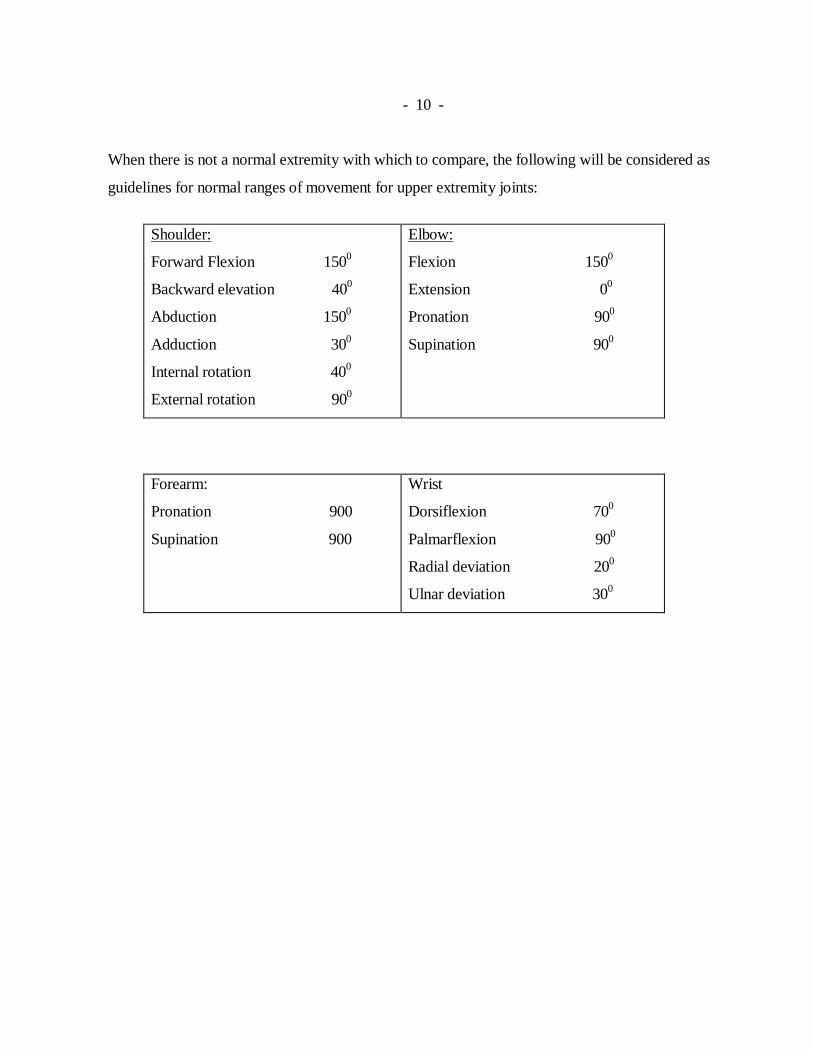
- 10 - When there is not a normal extremity with which to compare, the following will be considered as
guidelines for normal ranges of movement for upper extremity joints:
Shoulder:
Forward Flexion 1500
Backward elevation 400
Abduction 1500
Adduction 300
Internal rotation 400
External rotation 900
Elbow:
Flexion 1500
Extension 00
Pronation 900
Supination 900
Forearm:
Pronation 900
Supination 900
Wrist
Dorsiflexion 700
Palmarflexion 900
Radial deviation 200
Ulnar deviation 300
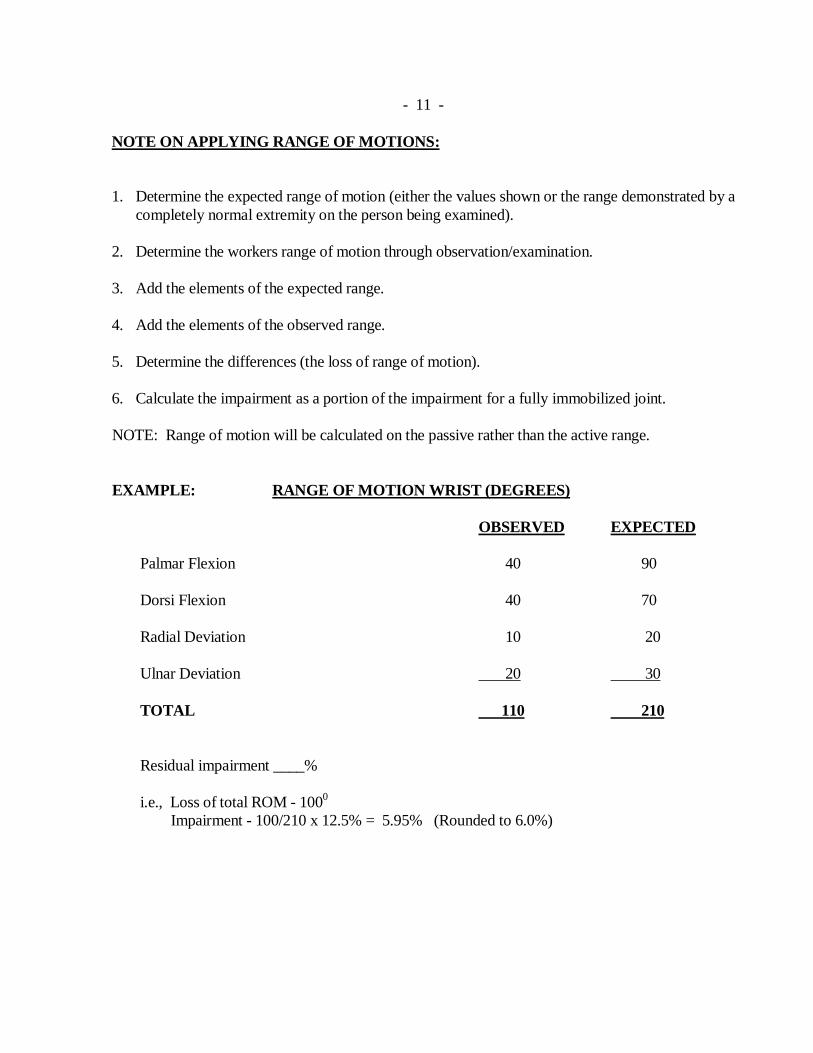
- 11 - NOTE ON APPLYING RANGE OF MOTIONS: 1. Determine the expected range of motion (either the values shown or the range demonstrated by a
completely normal extremity on the person being examined). 2. Determine the workers range of motion through observation/examination. 3. Add the elements of the expected range. 4. Add the elements of the observed range. 5. Determine the differences (the loss of range of motion). 6. Calculate the impairment as a portion of the impairment for a fully immobilized joint.
NOTE: Range of motion will be calculated on the passive rather than the active range. EXAMPLE: RANGE OF MOTION WRIST (DEGREES) OBSERVED EXPECTED
Palmar Flexion 40 90 Dorsi Flexion 40 70 Radial Deviation 10 20 Ulnar Deviation 20 30 TOTAL 110 210 Residual impairment ____% i.e., Loss of total ROM - 1000 Impairment - 100/210 x 12.5% = 5.95% (Rounded to 6.0%)
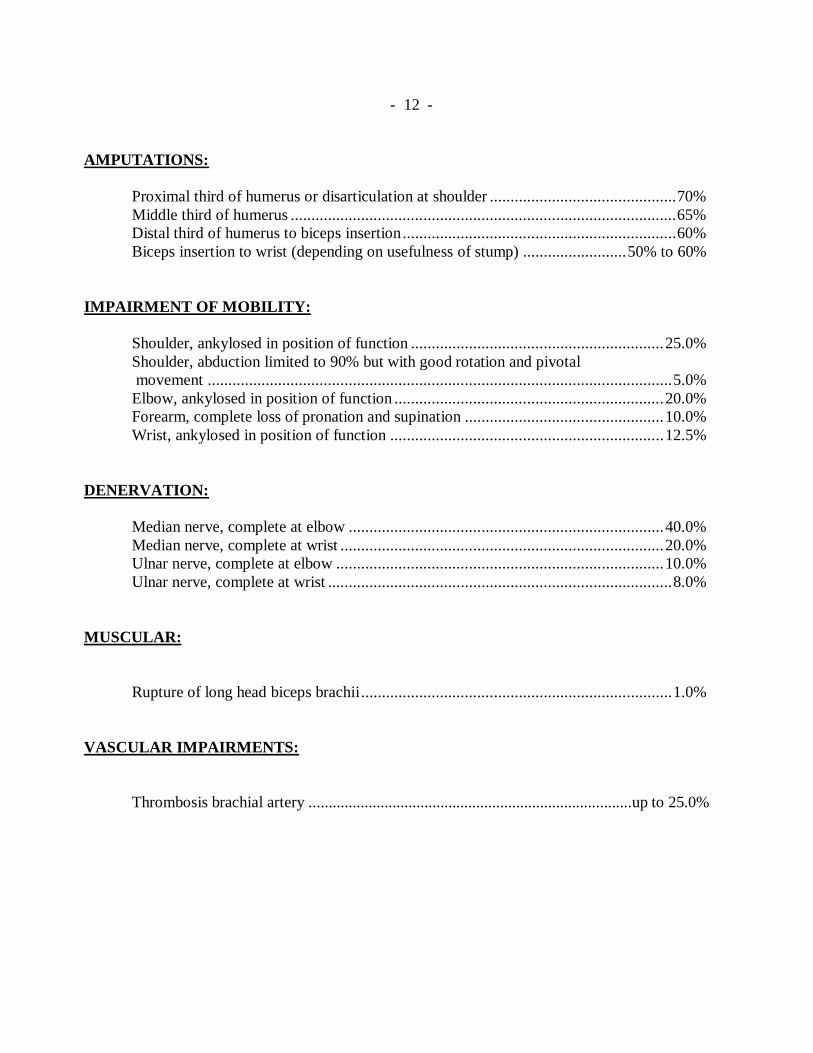
- 12 - AMPUTATIONS: Proximal third of humerus or disarticulation at shoulder ............................................. 70% Middle third of humerus ............................................................................................. 65% Distal third of humerus to biceps insertion .................................................................. 60% Biceps insertion to wrist (depending on usefulness of stump) ......................... 50% to 60% IMPAIRMENT OF MOBILITY: Shoulder, ankylosed in position of function ............................................................. 25.0% Shoulder, abduction limited to 90% but with good rotation and pivotal movement ................................................................................................................ 5.0% Elbow, ankylosed in position of function ................................................................. 20.0% Forearm, complete loss of pronation and supination ................................................ 10.0% Wrist, ankylosed in position of function .................................................................. 12.5% DENERVATION: Median nerve, complete at elbow ............................................................................ 40.0% Median nerve, complete at wrist .............................................................................. 20.0% Ulnar nerve, complete at elbow ............................................................................... 10.0% Ulnar nerve, complete at wrist ................................................................................... 8.0% MUSCULAR: Rupture of long head biceps brachii ........................................................................... 1.0% VASCULAR IMPAIRMENTS:
Thrombosis brachial artery .................................................................................up to 25.0%
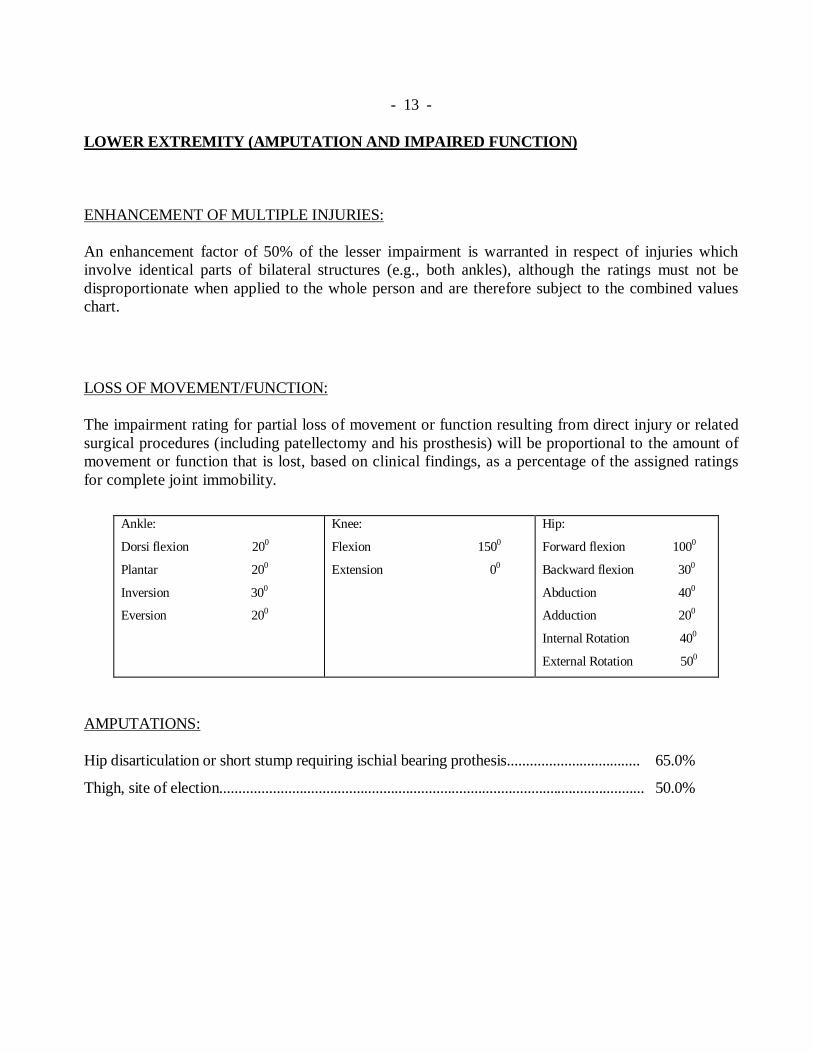
- 13 - LOWER EXTREMITY (AMPUTATION AND IMPAIRED FUNCTION) ENHANCEMENT OF MULTIPLE INJURIES: An enhancement factor of 50% of the lesser impairment is warranted in respect of injuries which involve identical parts of bilateral structures (e.g., both ankles), although the ratings must not be disproportionate when applied to the whole person and are therefore subject to the combined values chart.
LOSS OF MOVEMENT/FUNCTION: The impairment rating for partial loss of movement or function resulting from direct injury or related surgical procedures (including patellectomy and his prosthesis) will be proportional to the amount of movement or function that is lost, based on clinical findings, as a percentage of the assigned ratings for complete joint immobility.
Ankle:
Dorsi flexion 200
Plantar 200
Inversion 300
Eversion 200
Knee:
Flexion 1500
Extension 00
Hip:
Forward flexion 1000
Backward flexion 300
Abduction 400
Adduction 200
Internal Rotation 400
External Rotation 500
AMPUTATIONS: Hip disarticulation or short stump requiring ischial bearing prothesis................................... 65.0%
Thigh, site of election................................................................................................................ 50.0%
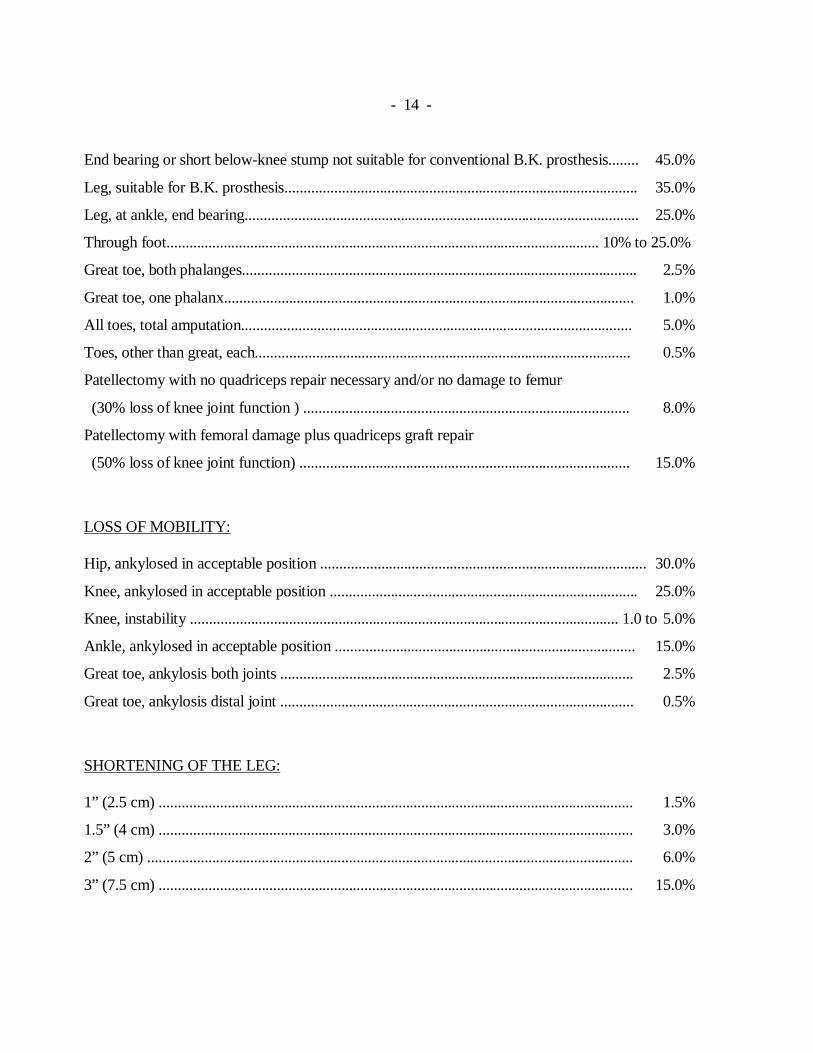
- 14 - End bearing or short below-knee stump not suitable for conventional B.K. prosthesis........ 45.0%
Leg, suitable for B.K. prosthesis............................................................................................. 35.0%
Leg, at ankle, end bearing........................................................................................................ 25.0%
Through foot.................................................................................................................. 10% to 25.0%
Great toe, both phalanges........................................................................................................ 2.5%
Great toe, one phalanx............................................................................................................ 1.0%
All toes, total amputation....................................................................................................... 5.0%
Toes, other than great, each................................................................................................... 0.5%
Patellectomy with no quadriceps repair necessary and/or no damage to femur
(30% loss of knee joint function ) ...................................................................................... 8.0%
Patellectomy with femoral damage plus quadriceps graft repair
(50% loss of knee joint function) ....................................................................................... 15.0%
LOSS OF MOBILITY: Hip, ankylosed in acceptable position ...................................................................................... 30.0%
Knee, ankylosed in acceptable position ................................................................................. 25.0%
Knee, instability ................................................................................................................. 1.0 to 5.0%
Ankle, ankylosed in acceptable position ............................................................................... 15.0%
Great toe, ankylosis both joints ............................................................................................. 2.5%
Great toe, ankylosis distal joint ............................................................................................. 0.5%
SHORTENING OF THE LEG: 1” (2.5 cm) ............................................................................................................................. 1.5%
1.5” (4 cm) ............................................................................................................................. 3.0%
2” (5 cm) ................................................................................................................................ 6.0%
3” (7.5 cm) ............................................................................................................................. 15.0%
- 15 - DENERVATION: Peroneal nerve, complete ...................................................................................................... 12.0% VASCULAR IMPAIRMENTS: Deep thrombosis of thigh and leg ........................................................................................ 10.0%
- 16 - SPINE
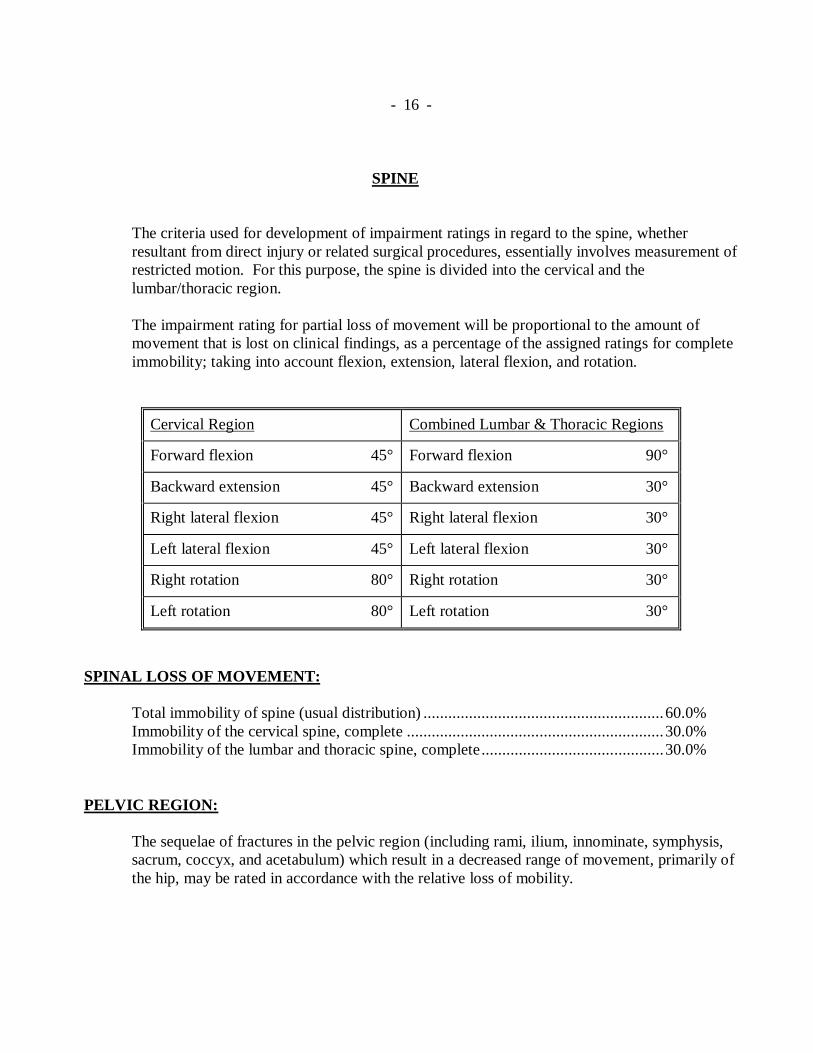
The criteria used for development of impairment ratings in regard to the spine, whether resultant from direct injury or related surgical procedures, essentially involves measurement of restricted motion. For this purpose, the spine is divided into the cervical and the lumbar/thoracic region. The impairment rating for partial loss of movement will be proportional to the amount of movement that is lost on clinical findings, as a percentage of the assigned ratings for complete immobility; taking into account flexion, extension, lateral flexion, and rotation.
Cervical Region Combined Lumbar & Thoracic Regions
Forward flexion 45° Forward flexion 90°
Backward extension 45° Backward extension 30°
Right lateral flexion 45° Right lateral flexion 30°
Left lateral flexion 45° Left lateral flexion 30°
Right rotation 80° Right rotation 30°
Left rotation 80° Left rotation 30°
SPINAL LOSS OF MOVEMENT: Total immobility of spine (usual distribution) .......................................................... 60.0% Immobility of the cervical spine, complete .............................................................. 30.0% Immobility of the lumbar and thoracic spine, complete ............................................ 30.0% PELVIC REGION:
The sequelae of fractures in the pelvic region (including rami, ilium, innominate, symphysis, sacrum, coccyx, and acetabulum) which result in a decreased range of movement, primarily of the hip, may be rated in accordance with the relative loss of mobility.
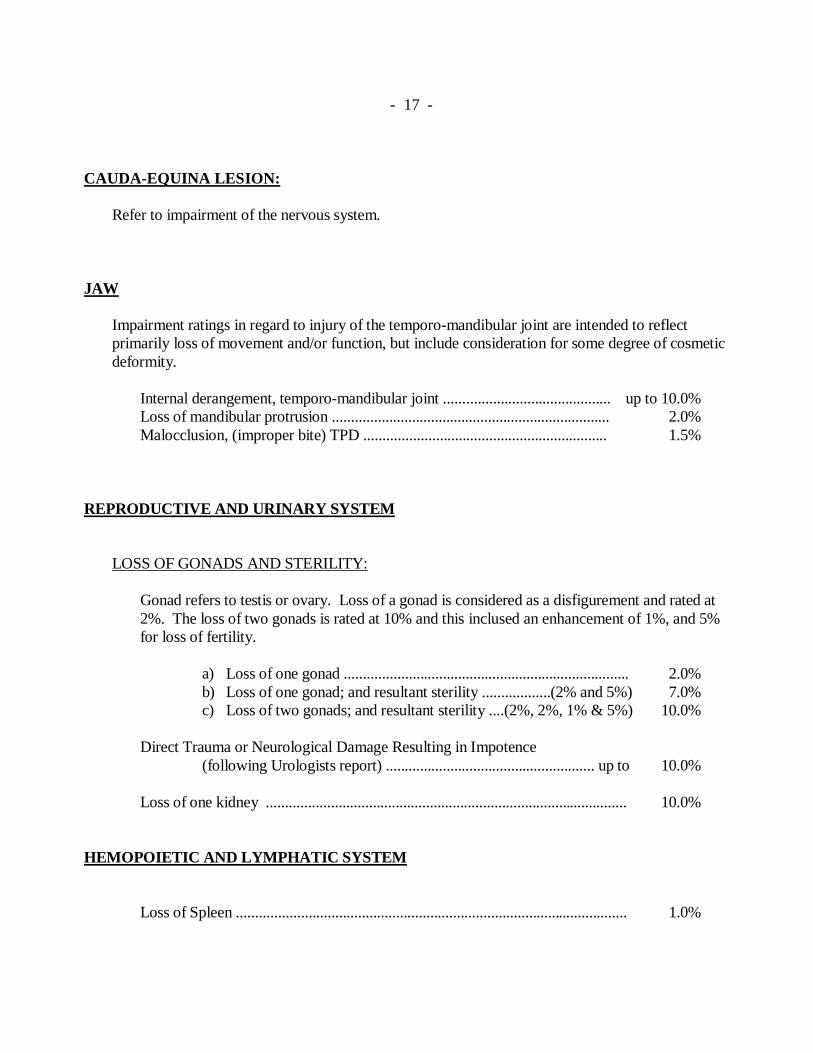
- 17 - CAUDA-EQUINA LESION:
Refer to impairment of the nervous system.
JAW Impairment ratings in regard to injury of the temporo-mandibular joint are intended to reflect primarily loss of movement and/or function, but include consideration for some degree of cosmetic deformity.
Internal derangement, temporo-mandibular joint ............................................ up to 10.0% Loss of mandibular protrusion ......................................................................... 2.0% Malocclusion, (improper bite) TPD ................................................................ 1.5%
REPRODUCTIVE AND URINARY SYSTEM LOSS OF GONADS AND STERILITY:
Gonad refers to testis or ovary. Loss of a gonad is considered as a disfigurement and rated at 2%. The loss of two gonads is rated at 10% and this inclused an enhancement of 1%, and 5% for loss of fertility.
a) Loss of one gonad ........................................................................... 2.0% b) Loss of one gonad; and resultant sterility ..................(2% and 5%) 7.0% c) Loss of two gonads; and resultant sterility ....(2%, 2%, 1% & 5%) 10.0%
Direct Trauma or Neurological Damage Resulting in Impotence (following Urologists report) ....................................................... up to 10.0% Loss of one kidney ............................................................................................... 10.0%
HEMOPOIETIC AND LYMPHATIC SYSTEM Loss of Spleen ....................................................................................................... 1.0%
- 18 -
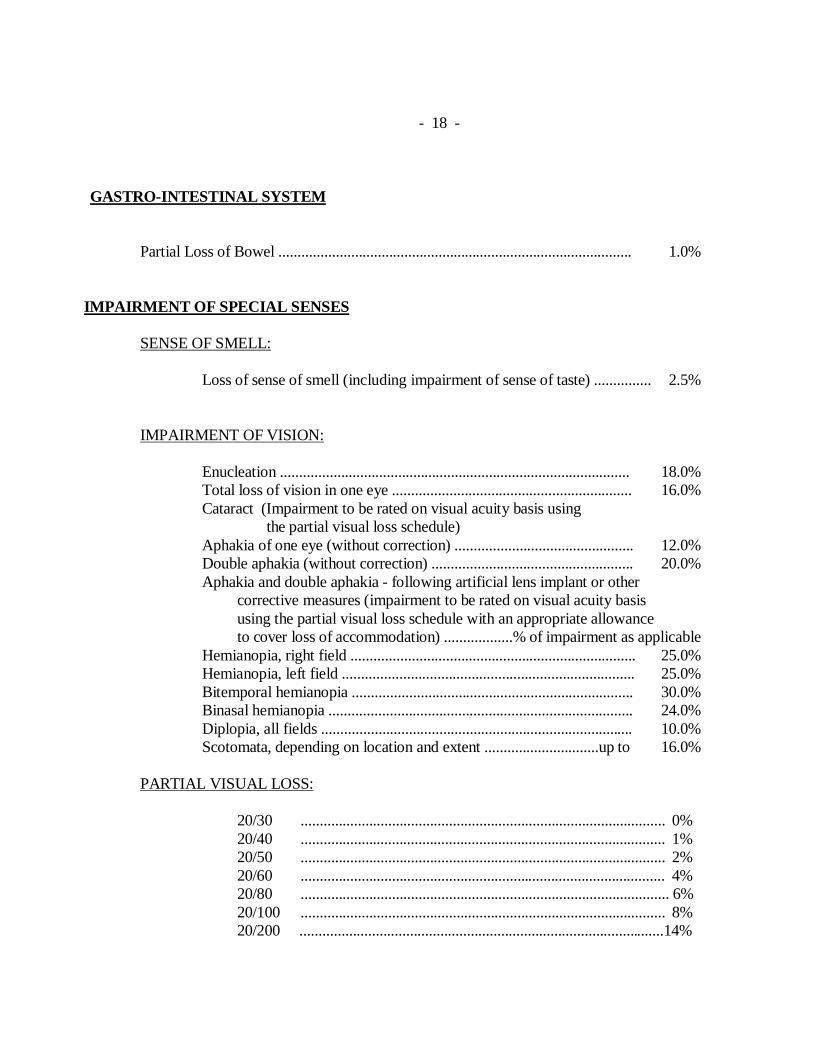
GASTRO-INTESTINAL SYSTEM Partial Loss of Bowel ............................................................................................. 1.0%
IMPAIRMENT OF SPECIAL SENSES SENSE OF SMELL:
Loss of sense of smell (including impairment of sense of taste) ............... 2.5%
IMPAIRMENT OF VISION:
Enucleation ............................................................................................ 18.0% Total loss of vision in one eye ............................................................... 16.0% Cataract (Impairment to be rated on visual acuity basis using the partial visual loss schedule) Aphakia of one eye (without correction) ............................................... 12.0% Double aphakia (without correction) ..................................................... 20.0% Aphakia and double aphakia - following artificial lens implant or other corrective measures (impairment to be rated on visual acuity basis using the partial visual loss schedule with an appropriate allowance to cover loss of accommodation) ..................% of impairment as applicable Hemianopia, right field ........................................................................... 25.0% Hemianopia, left field ............................................................................. 25.0% Bitemporal hemianopia .......................................................................... 30.0% Binasal hemianopia ................................................................................ 24.0% Diplopia, all fields .................................................................................. 10.0% Scotomata, depending on location and extent ..............................up to 16.0%
PARTIAL VISUAL LOSS:
20/30 ................................................................................................ 0% 20/40 ................................................................................................ 1% 20/50 ................................................................................................ 2% 20/60 ................................................................................................ 4% 20/80 ................................................................................................. 6% 20/100 ................................................................................................ 8% 20/200 ................................................................................................14%
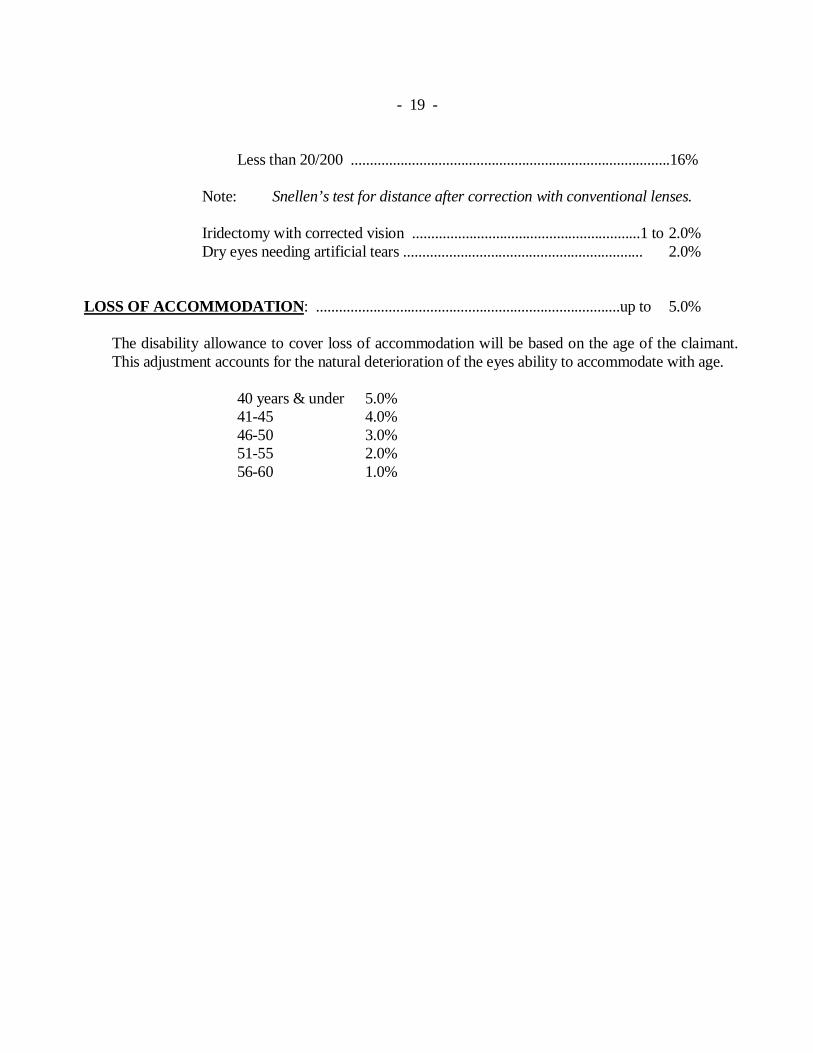
- 19 - Less than 20/200 ....................................................................................16%
Note: Snellen’s test for distance after correction with conventional lenses. Iridectomy with corrected vision ............................................................1 to 2.0% Dry eyes needing artificial tears ............................................................... 2.0%
LOSS OF ACCOMMODATION: ................................................................................up to 5.0%
The disability allowance to cover loss of accommodation will be based on the age of the claimant. This adjustment accounts for the natural deterioration of the eyes ability to accommodate with age.
40 years & under 5.0% 41-45 4.0% 46-50 3.0% 51-55 2.0% 56-60 1.0%
- 20 -
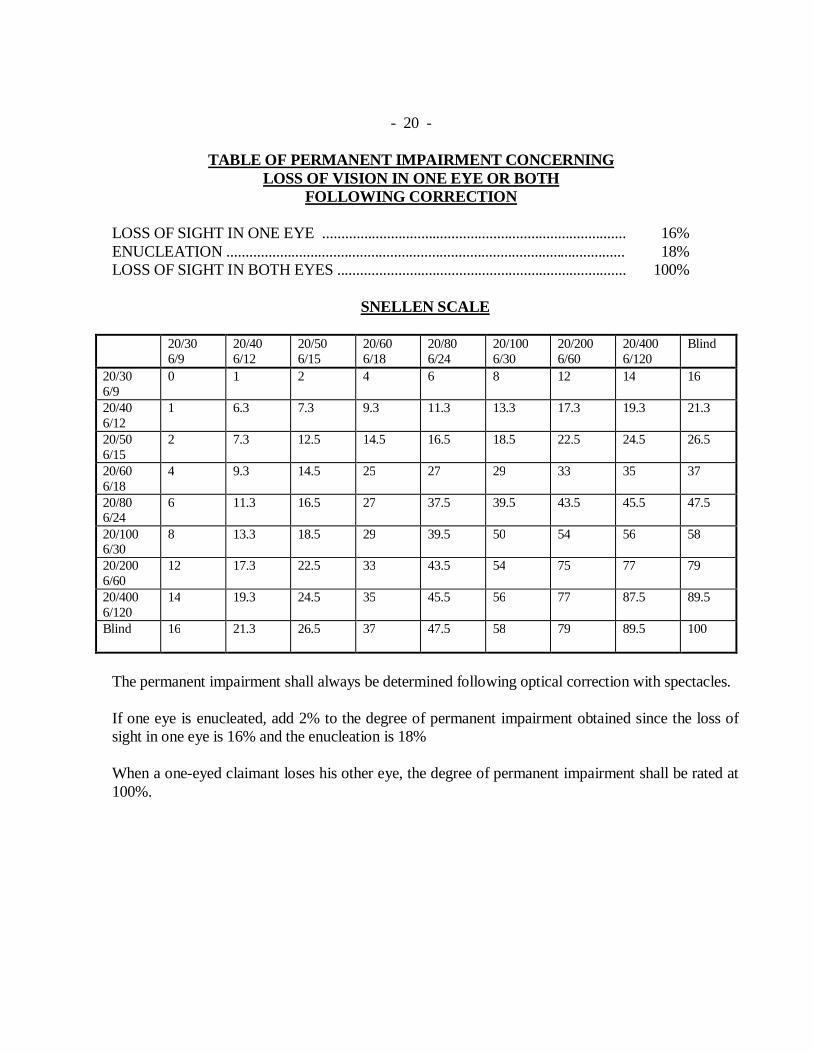
TABLE OF PERMANENT IMPAIRMENT CONCERNING
LOSS OF VISION IN ONE EYE OR BOTH FOLLOWING CORRECTION
LOSS OF SIGHT IN ONE EYE ................................................................................ 16% ENUCLEATION ......................................................................................................... 18% LOSS OF SIGHT IN BOTH EYES ............................................................................ 100%
SNELLEN SCALE
20/30 6/9
20/40 6/12
20/50 6/15
20/60 6/18
20/80 6/24
20/100 6/30
20/200 6/60
20/400 6/120
Blind
20/30 6/9
0 1 2 4 6 8 12 14 16
20/40 6/12
1 6.3 7.3 9.3 11.3 13.3 17.3 19.3 21.3
20/50 6/15
2 7.3 12.5 14.5 16.5 18.5 22.5 24.5 26.5
20/60 6/18
4 9.3 14.5 25 27 29 33 35 37
20/80 6/24
6 11.3 16.5 27 37.5 39.5 43.5 45.5 47.5
20/100 6/30
8 13.3 18.5 29 39.5 50 54 56 58
20/200 6/60
12 17.3 22.5 33 43.5 54 75 77 79
20/400 6/120
14 19.3 24.5 35 45.5 56 77 87.5 89.5
Blind
16 21.3 26.5 37 47.5 58 79 89.5 100
The permanent impairment shall always be determined following optical correction with spectacles. If one eye is enucleated, add 2% to the degree of permanent impairment obtained since the loss of sight in one eye is 16% and the enucleation is 18% When a one-eyed claimant loses his other eye, the degree of permanent impairment shall be rated at 100%.
- 21 –
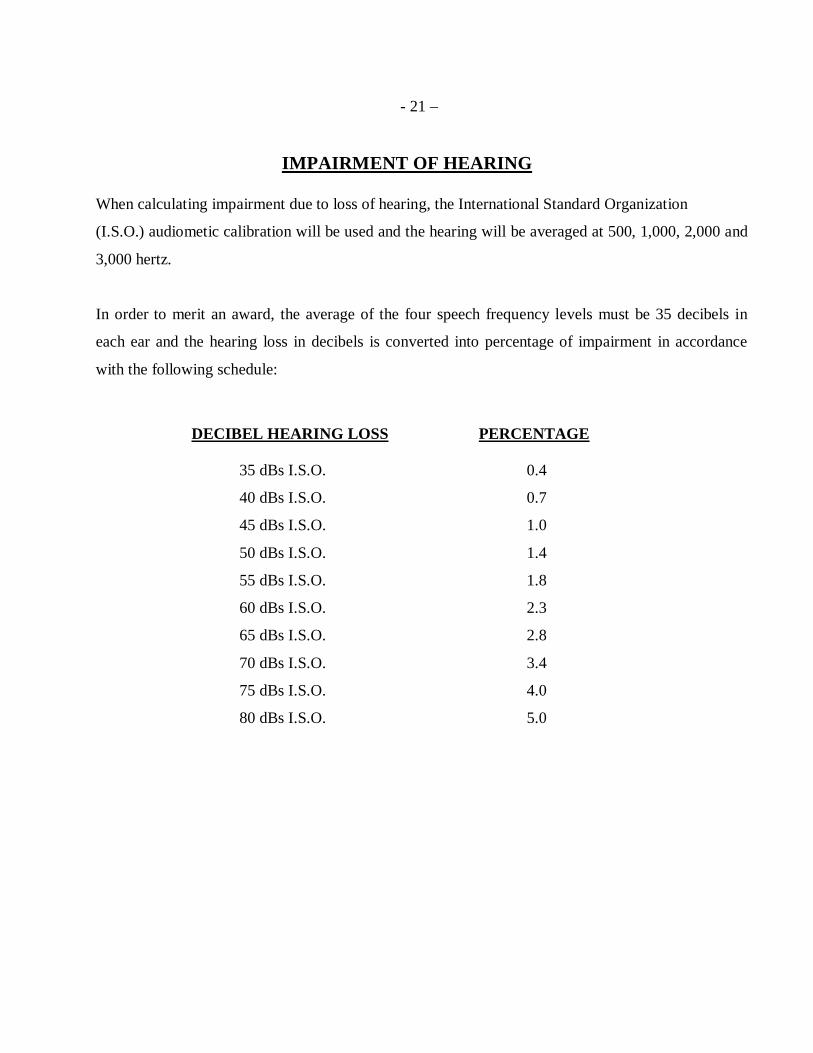
IMPAIRMENT OF HEARING When calculating impairment due to loss of hearing, the International Standard Organization
(I.S.O.) audiometic calibration will be used and the hearing will be averaged at 500, 1,000, 2,000 and
3,000 hertz.
In order to merit an award, the average of the four speech frequency levels must be 35 decibels in
each ear and the hearing loss in decibels is converted into percentage of impairment in accordance
with the following schedule:
DECIBEL HEARING LOSS PERCENTAGE 35 dBs I.S.O. 0.4
40 dBs I.S.O. 0.7
45 dBs I.S.O. 1.0
50 dBs I.S.O. 1.4
55 dBs I.S.O. 1.8
60 dBs I.S.O. 2.3
65 dBs I.S.O. 2.8
70 dBs I.S.O. 3.4
75 dBs I.S.O. 4.0
80 dBs I.S.O. 5.0
- 22 - ENHANCEMENT FACTOR:
In bilateral deafness the poorer ear is rated according to the scale and the better ear is rated
according to the scale, multiplied by five. The sum of the two give the combined rating.
PRESBYCUSIS: In cases where the claimant’s age exceeds 60, deduct .5 decibels for each year. This is to allow
for presbycusis or loss of hearing due to age.
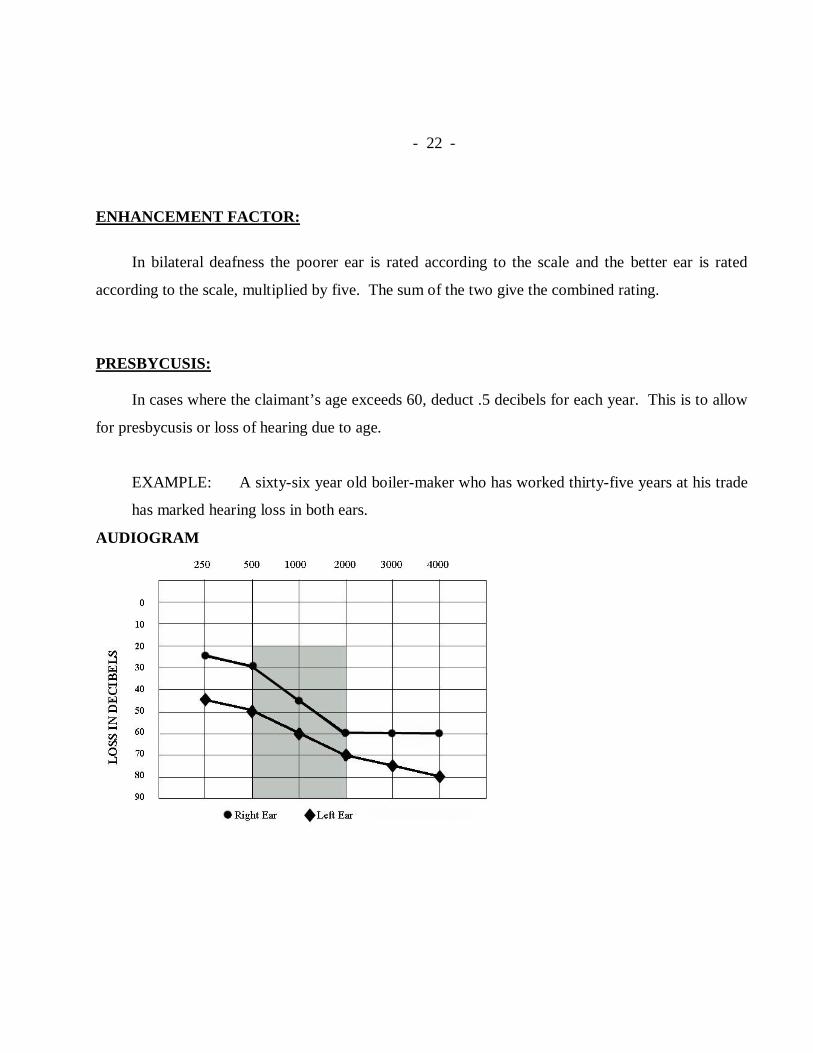
EXAMPLE: A sixty-six year old boiler-maker who has worked thirty-five years at his trade
has marked hearing loss in both ears.
AUDIOGRAM
- 23 -
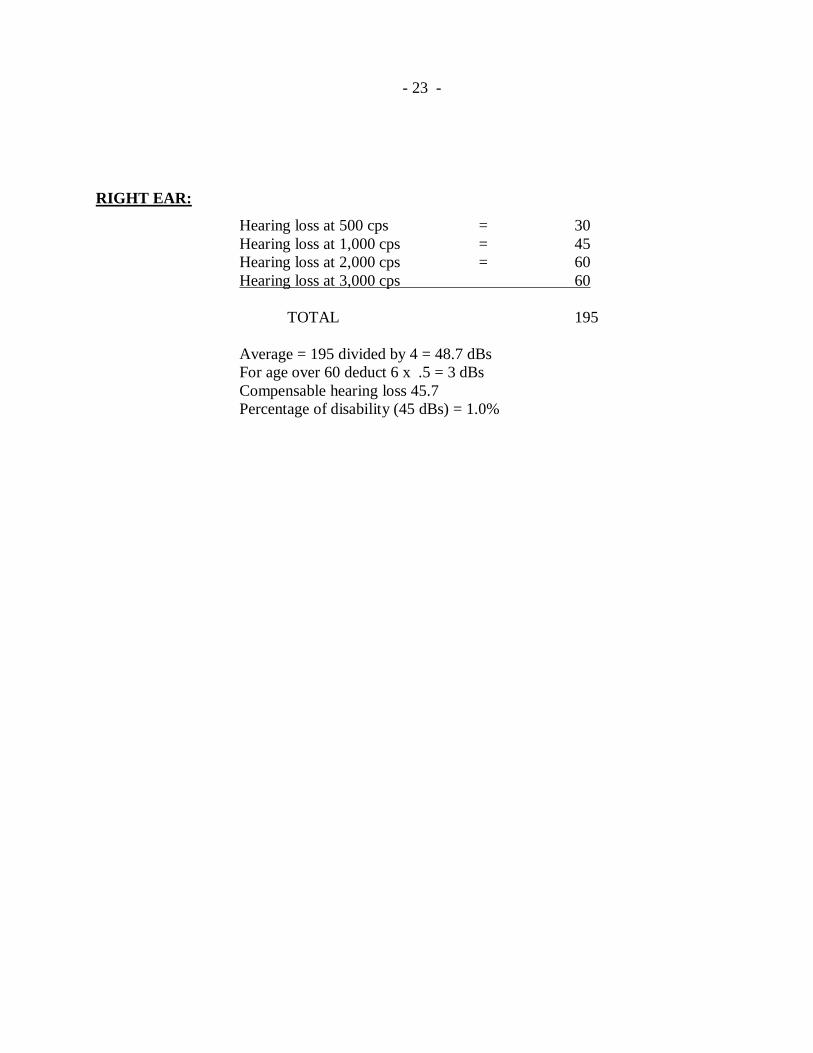
RIGHT EAR:
Hearing loss at 500 cps = 30 Hearing loss at 1,000 cps = 45 Hearing loss at 2,000 cps = 60 Hearing loss at 3,000 cps 60 TOTAL 195 Average = 195 divided by 4 = 48.7 dBs For age over 60 deduct 6 x .5 = 3 dBs Compensable hearing loss 45.7 Percentage of disability (45 dBs) = 1.0%
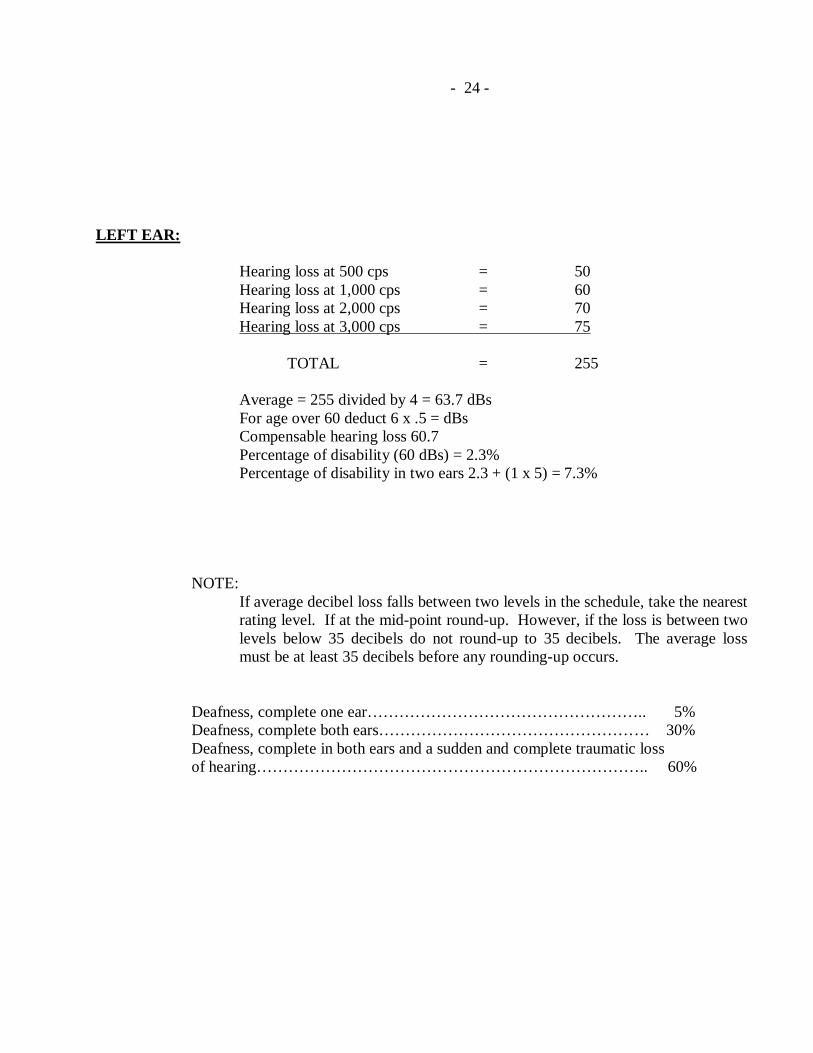
- 24 - LEFT EAR: Hearing loss at 500 cps = 50 Hearing loss at 1,000 cps = 60 Hearing loss at 2,000 cps = 70 Hearing loss at 3,000 cps = 75 TOTAL = 255 Average = 255 divided by 4 = 63.7 dBs For age over 60 deduct 6 x .5 = dBs Compensable hearing loss 60.7 Percentage of disability (60 dBs) = 2.3% Percentage of disability in two ears 2.3 + (1 x 5) = 7.3% NOTE:
If average decibel loss falls between two levels in the schedule, take the nearest rating level. If at the mid-point round-up. However, if the loss is between two levels below 35 decibels do not round-up to 35 decibels. The average loss must be at least 35 decibels before any rounding-up occurs.
Deafness, complete one ear…………………………………………….. 5% Deafness, complete both ears…………………………………………… 30% Deafness, complete in both ears and a sudden and complete traumatic loss of hearing……………………………………………………………….. 60%
- 25 -
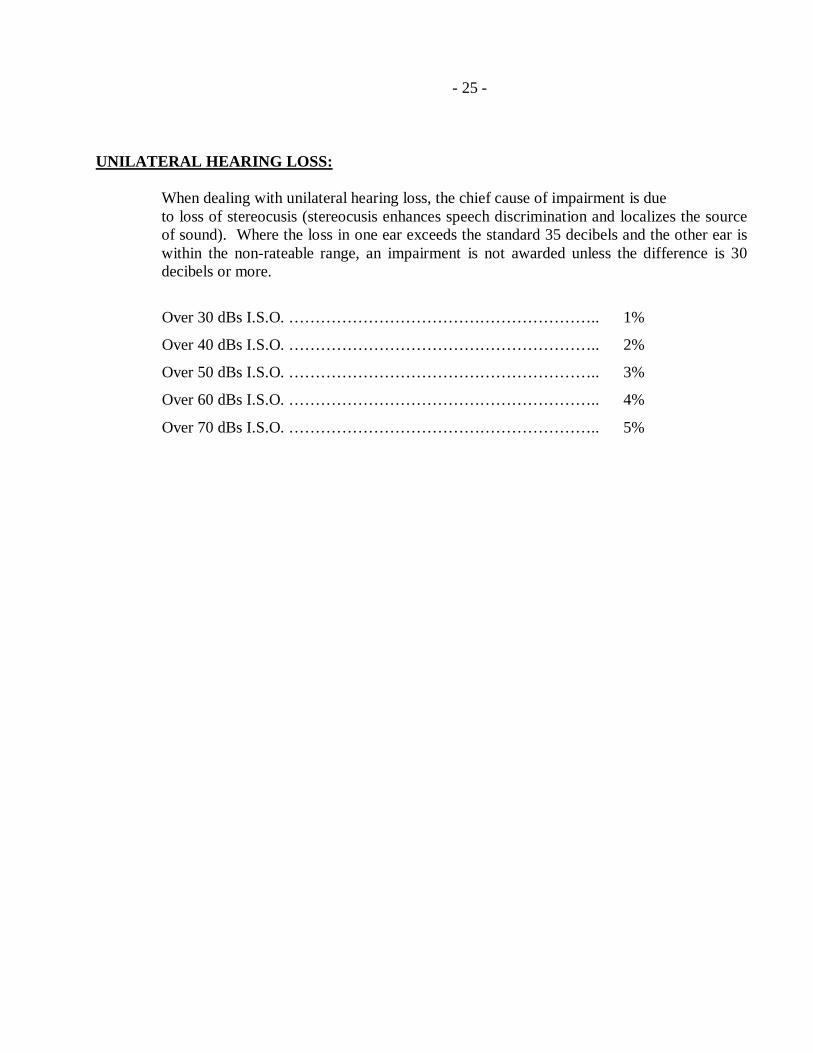
UNILATERAL HEARING LOSS: When dealing with unilateral hearing loss, the chief cause of impairment is due
to loss of stereocusis (stereocusis enhances speech discrimination and localizes the source of sound). Where the loss in one ear exceeds the standard 35 decibels and the other ear is within the non-rateable range, an impairment is not awarded unless the difference is 30 decibels or more.
Over 30 dBs I.S.O. ………………………………………………….. 1%
Over 40 dBs I.S.O. ………………………………………………….. 2%
Over 50 dBs I.S.O. ………………………………………………….. 3%
Over 60 dBs I.S.O. ………………………………………………….. 4%
Over 70 dBs I.S.O. ………………………………………………….. 5%
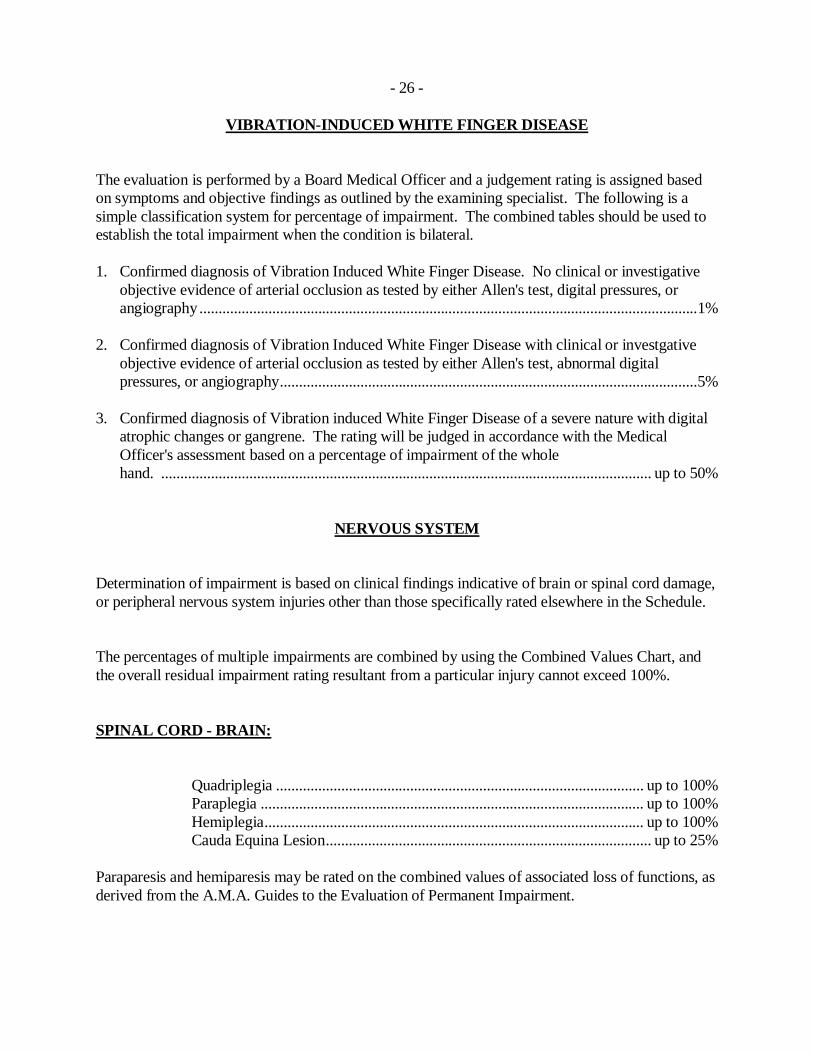
- 26 - VIBRATION-INDUCED WHITE FINGER DISEASE The evaluation is performed by a Board Medical Officer and a judgement rating is assigned based on symptoms and objective findings as outlined by the examining specialist. The following is a simple classification system for percentage of impairment. The combined tables should be used to establish the total impairment when the condition is bilateral. 1. Confirmed diagnosis of Vibration Induced White Finger Disease. No clinical or investigative
objective evidence of arterial occlusion as tested by either Allen's test, digital pressures, or angiography .................................................................................................................................. 1%
2. Confirmed diagnosis of Vibration Induced White Finger Disease with clinical or investgative
objective evidence of arterial occlusion as tested by either Allen's test, abnormal digital pressures, or angiography ............................................................................................................. 5%
3. Confirmed diagnosis of Vibration induced White Finger Disease of a severe nature with digital
atrophic changes or gangrene. The rating will be judged in accordance with the Medical Officer's assessment based on a percentage of impairment of the whole
hand. ................................................................................................................................ up to 50% NERVOUS SYSTEM Determination of impairment is based on clinical findings indicative of brain or spinal cord damage, or peripheral nervous system injuries other than those specifically rated elsewhere in the Schedule. The percentages of multiple impairments are combined by using the Combined Values Chart, and the overall residual impairment rating resultant from a particular injury cannot exceed 100%. SPINAL CORD - BRAIN: Quadriplegia ................................................................................................ up to 100% Paraplegia .................................................................................................... up to 100% Hemiplegia ................................................................................................... up to 100% Cauda Equina Lesion ..................................................................................... up to 25% Paraparesis and hemiparesis may be rated on the combined values of associated loss of functions, as derived from the A.M.A. Guides to the Evaluation of Permanent Impairment.
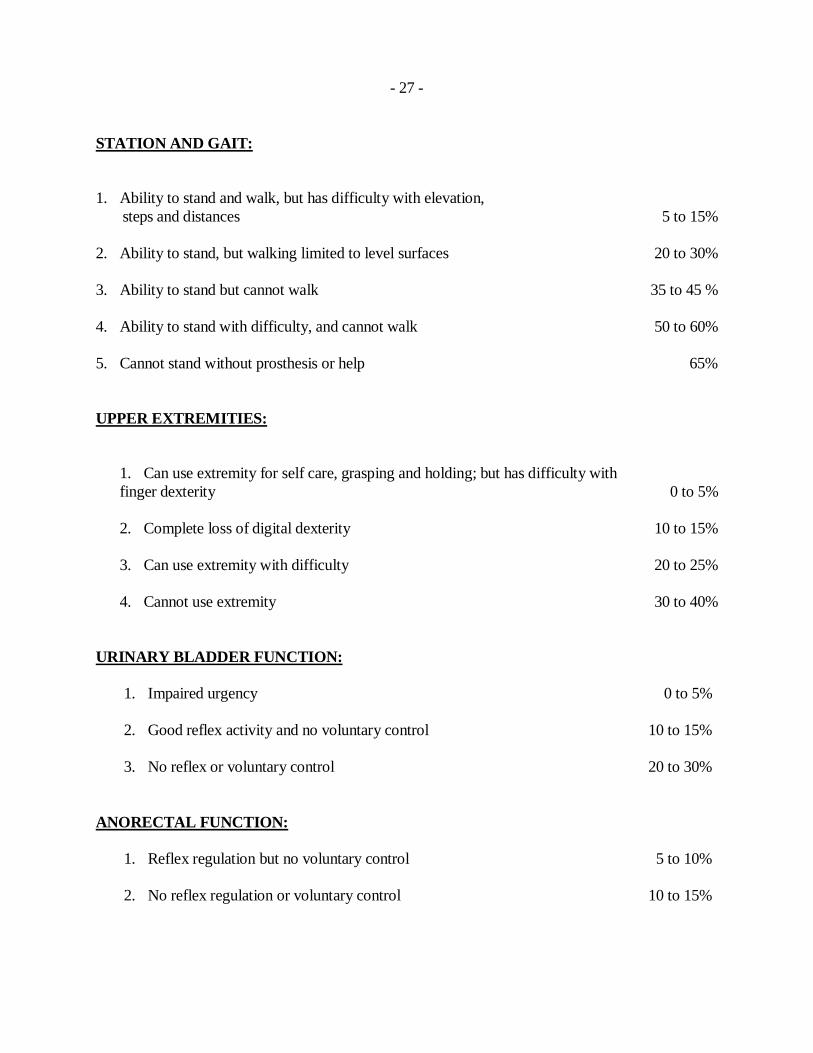
- 27 - STATION AND GAIT: 1. Ability to stand and walk, but has difficulty with elevation, steps and distances 5 to 15% 2. Ability to stand, but walking limited to level surfaces 20 to 30% 3. Ability to stand but cannot walk 35 to 45 % 4. Ability to stand with difficulty, and cannot walk 50 to 60% 5. Cannot stand without prosthesis or help 65% UPPER EXTREMITIES:
1. Can use extremity for self care, grasping and holding; but has difficulty with finger dexterity 0 to 5%
2. Complete loss of digital dexterity 10 to 15%
3. Can use extremity with difficulty 20 to 25%
4. Cannot use extremity 30 to 40%
URINARY BLADDER FUNCTION:
1. Impaired urgency 0 to 5% 2. Good reflex activity and no voluntary control 10 to 15% 3. No reflex or voluntary control 20 to 30%
ANORECTAL FUNCTION:
1. Reflex regulation but no voluntary control 5 to 10% 2. No reflex regulation or voluntary control 10 to 15%
- 28 -
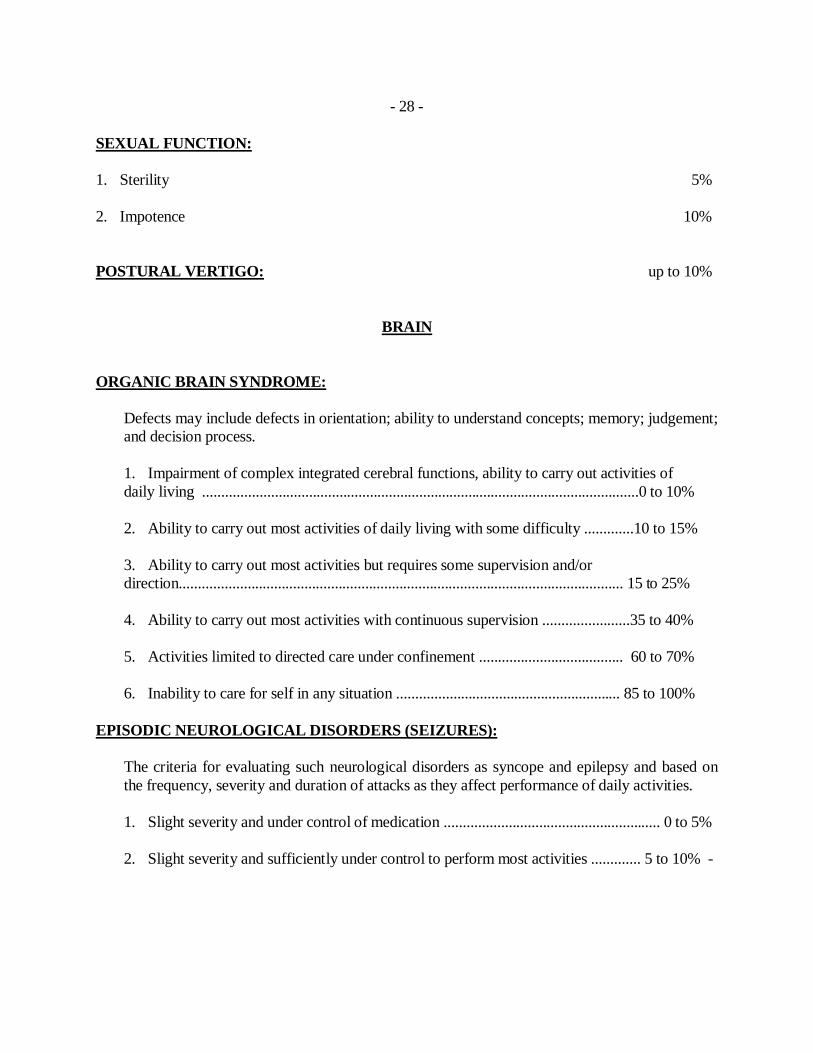
SEXUAL FUNCTION: 1. Sterility 5% 2. Impotence 10% POSTURAL VERTIGO: up to 10%
BRAIN ORGANIC BRAIN SYNDROME:
Defects may include defects in orientation; ability to understand concepts; memory; judgement; and decision process. 1. Impairment of complex integrated cerebral functions, ability to carry out activities of daily living ...................................................................................................................0 to 10% 2. Ability to carry out most activities of daily living with some difficulty .............10 to 15% 3. Ability to carry out most activities but requires some supervision and/or direction..................................................................................................................... 15 to 25% 4. Ability to carry out most activities with continuous supervision .......................35 to 40% 5. Activities limited to directed care under confinement ...................................... 60 to 70% 6. Inability to care for self in any situation ........................................................... 85 to 100%
EPISODIC NEUROLOGICAL DISORDERS (SEIZURES):
The criteria for evaluating such neurological disorders as syncope and epilepsy and based on the frequency, severity and duration of attacks as they affect performance of daily activities. 1. Slight severity and under control of medication ......................................................... 0 to 5% 2. Slight severity and sufficiently under control to perform most activities ............. 5 to 10% -
- 29 -
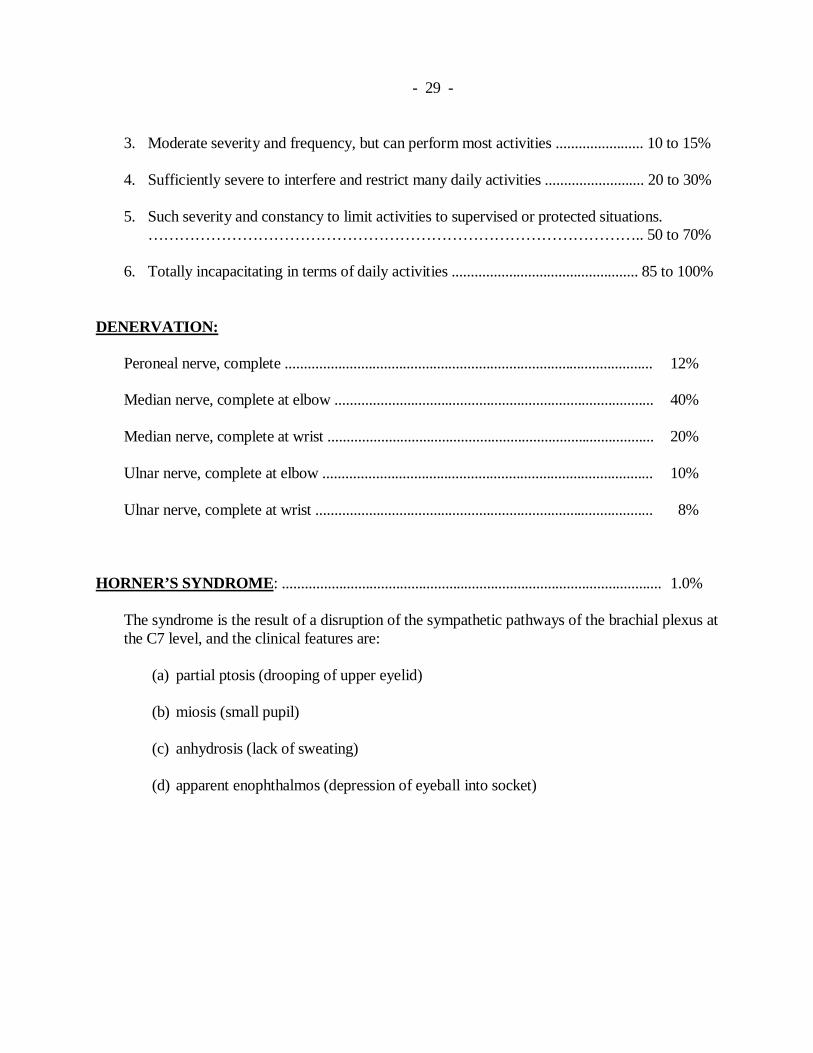
3. Moderate severity and frequency, but can perform most activities ....................... 10 to 15% 4. Sufficiently severe to interfere and restrict many daily activities .......................... 20 to 30% 5. Such severity and constancy to limit activities to supervised or protected situations.
………………………………………………………………………………….. 50 to 70% 6. Totally incapacitating in terms of daily activities ................................................. 85 to 100%
DENERVATION:
Peroneal nerve, complete ................................................................................................. 12% Median nerve, complete at elbow .................................................................................... 40% Median nerve, complete at wrist ...................................................................................... 20% Ulnar nerve, complete at elbow ....................................................................................... 10% Ulnar nerve, complete at wrist ......................................................................................... 8%
HORNER’S SYNDROME: .................................................................................................... 1.0%
The syndrome is the result of a disruption of the sympathetic pathways of the brachial plexus at the C7 level, and the clinical features are:
(a) partial ptosis (drooping of upper eyelid) (b) miosis (small pupil) (c) anhydrosis (lack of sweating) (d) apparent enophthalmos (depression of eyeball into socket)
- 30 -
DISFIGUREMENT
When a worker is permanently disfigured as a result of an injury, the Board may determine that
the disfigurement be considered a permanent impairment to which the claimant is entitled to an
award.
Disfigurement is an altered or abnormal appearance. This may be an alteration of color, shape,
or structure, or a combination of these and can also include loss of function due to contractures
as a result of scarring.
The rating for disfigurement is done by the Board’s Medical Department and the degree of
disfigurement is determined on a judgemental basis. The maximum rating for disfigurement, in
extreme cases, is 25%. Typical awards for disfigurement are between 1 and 5%. In order to
maintain consistency in awards for disfigurement, and to make the awards as objective as
possible, Medical staff will make reference to the folio of previous disfigurement awards
established as policy by Board Order No. 67/89 and maintained by the Director of the Benefits
Division as prescribed in Board Order 67/89.
Contractures resulting in loss of function should be considered as for any other cause, and are
applied using the combined values chart.
- 31 -
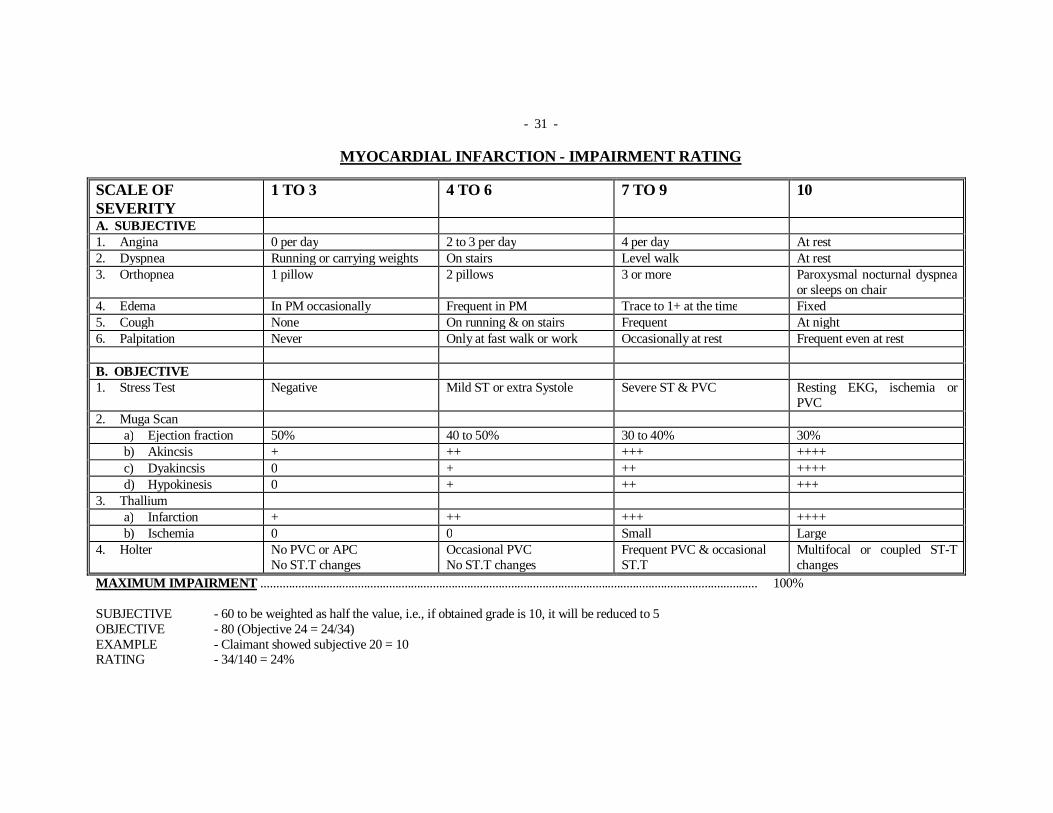
MYOCARDIAL INFARCTION - IMPAIRMENT RATING
SCALE OF SEVERITY
1 TO 3 4 TO 6 7 TO 9 10
A. SUBJECTIVE 1. Angina 0 per day 2 to 3 per day 4 per day At rest 2. Dyspnea Running or carrying weights On stairs Level walk At rest 3. Orthopnea 1 pillow 2 pillows 3 or more Paroxysmal nocturnal dyspnea
or sleeps on chair 4. Edema In PM occasionally Frequent in PM Trace to 1+ at the time Fixed 5. Cough None On running & on stairs Frequent At night 6. Palpitation Never Only at fast walk or work Occasionally at rest Frequent even at rest B. OBJECTIVE 1. Stress Test Negative Mild ST or extra Systole Severe ST & PVC Resting EKG, ischemia or
PVC 2. Muga Scan
a) Ejection fraction 50% 40 to 50% 30 to 40% 30% b) Akincsis + ++ +++ ++++ c) Dyakincsis 0 + ++ ++++ d) Hypokinesis 0 + ++ +++
3. Thallium a) Infarction + ++ +++ ++++ b) Ischemia 0 0 Small Large
4. Holter No PVC or APC No ST.T changes
Occasional PVC No ST.T changes
Frequent PVC & occasional ST.T
Multifocal or coupled ST-T changes
MAXIMUM IMPAIRMENT ............................................................................................................................................................... 100% SUBJECTIVE - 60 to be weighted as half the value, i.e., if obtained grade is 10, it will be reduced to 5 OBJECTIVE - 80 (Objective 24 = 24/34) EXAMPLE - Claimant showed subjective 20 = 10 RATING - 34/140 = 24%
- 32 -
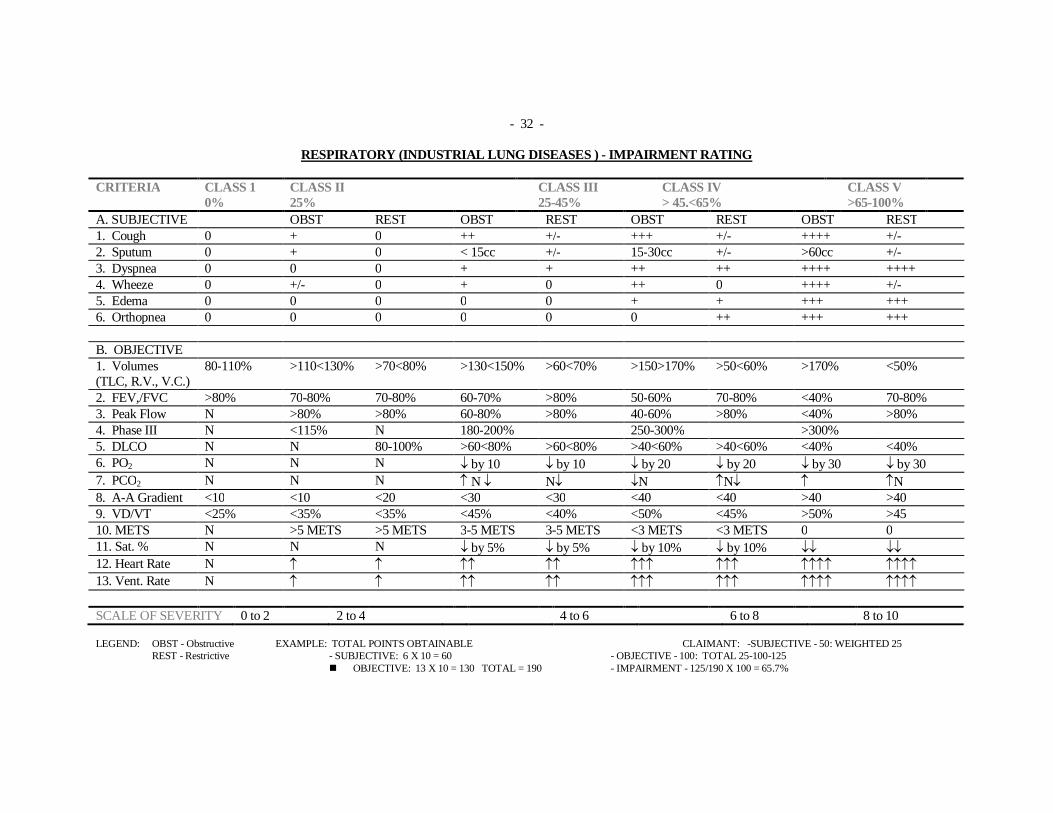
RESPIRATORY (INDUSTRIAL LUNG DISEASES ) - IMPAIRMENT RATING CRITERIA CLASS 1
0% CLASS II 25%
CLASS III 25-45%
CLASS IV > 45.<65%
CLASS V >65-100%
A. SUBJECTIVE OBST REST OBST REST OBST REST OBST REST 1. Cough 0 + 0 ++ +/- +++ +/- ++++ +/- 2. Sputum 0 + 0 < 15cc +/- 15-30cc +/- >60cc +/- 3. Dyspnea 0 0 0 + + ++ ++ ++++ ++++ 4. Wheeze 0 +/- 0 + 0 ++ 0 ++++ +/- 5. Edema 0 0 0 0 0 + + +++ +++ 6. Orthopnea 0 0 0 0 0 0 ++ +++ +++ B. OBJECTIVE 1. Volumes (TLC, R.V., V.C.)
80-110% >110<130% >70<80% >130<150% >60<70% >150>170% >50<60% >170% <50%
2. FEV,/FVC >80% 70-80% 70-80% 60-70% >80% 50-60% 70-80% <40% 70-80% 3. Peak Flow N >80% >80% 60-80% >80% 40-60% >80% <40% >80% 4. Phase III N <115% N 180-200% 250-300% >300% 5. DLCO N N 80-100% >60<80% >60<80% >40<60% >40<60% <40% <40% 6. PO2 N N N by 10 by 10 by 20 by 20 by 30 by 30 7. PCO2 N N N N N N N N 8. A-A Gradient <10 <10 <20 <30 <30 <40 <40 >40 >40 9. VD/VT <25% <35% <35% <45% <40% <50% <45% >50% >45 10. METS N >5 METS >5 METS 3-5 METS 3-5 METS <3 METS <3 METS 0 0 11. Sat. % N N N by 5% by 5% by 10% by 10% 12. Heart Rate N 13. Vent. Rate N SCALE OF SEVERITY 0 to 2 2 to 4 4 to 6 6 to 8 8 to 10 LEGEND: OBST - Obstructive EXAMPLE: TOTAL POINTS OBTAINABLE CLAIMANT: -SUBJECTIVE - 50: WEIGHTED 25 REST - Restrictive - SUBJECTIVE: 6 X 10 = 60 - OBJECTIVE - 100: TOTAL 25-100-125
OBJECTIVE: 13 X 10 = 130 TOTAL = 190 - IMPAIRMENT - 125/190 X 100 = 65.7%
- 33 -
PSYCHOLOGICAL INTRODUCTION:
The psychic functions (mental, affective, adaptive, behavioral) of certain accident victims may be permanently damaged. a) General Impairment Producing Mechanisms
Such impairments are sometimes the direct consequence of a lesion in the central nervous system and therefore entail psychiatric or psychological evaluation which goes beyond the sole assessment of a neurological impairment. In other cases, the impairment reflects a permanent affective dysfunction revealing chronic psychological maladaptation to trauma having temporarily or permanently damaged another part of the body. Impairments of this nature may sometimes result from the interaction of the two impairment producing mechanisms.
b) General Evaluation Criteria
Impairment is assessed by means of a clinical psychiatric or psychological examination. Adequate knowledge of the accident victim’s personality prior to the accident, his complete background and his usual mode of adaptation is necessary for the conducting of a clinical evaluation. The victim’s premorbid level of personal adaptation must be considered in order to determine the degree of functional damage stemming from mental illness caused by an accident. A detailed objective mental examination is essential. The symptomatology must establish a credible, total and coherent syndrome. Impairment of psychic functions must be manifested by changes in the patient’s daily activities and interpersonal relationships and in certain cases must be accompanied by physiopathological signs. Symptoms must be present during a sufficiently long period and, as a rule, must persist despite constant, standard therapy. Additional objective information on the patient’s abnormal mental condition is usually provided by his family and friends and those treating him. A purely subjective syndrome that is difficult to verify rarely indicates severe permanent partial impairment.
- 34 - The clinical evaluation may sometimes be supplemented with a social or psychometric evaluation. Unfavourable social circumstances may influence that accident victim’s rehabilitation and overall prognosis but do not in themselves constitute an impairment of psychic functions. The evaluation must take his motivational aspect into account. Lastly, an impairment assessed by such psychiatric or psychological evaluation is different in its very nature from an impairment caused by the loss of enjoyment of life or of a mutilated organ.
(c) Groups and Classes of Impairment
Permanent impairment of the accident victim’s psychic functions may result from: chronic brain syndromes psychoses neuroses personality disorders
The history of psychiatric or psychological sequelae, the specific results of the mental examination and supplementary examinations usually allow only one nostologic category to be determined. However, organic brain syndromes may, in particular, be accompanied by and thus include in their clinical picture and evaluation psychotic or neurotic signs or deterioration of the personality. Symptomatic severity is accompanied by repercussions going beyond the accident victim’s mere experience to change his usual activities of daily living and his personal or social efficiency. The accident victim requires constant supervision or therapy, assistance or a particular milieu, and in certain cases even needs to be looked after on a full-time basis for the fulfilment of his basic needs. The diagnosis as to the degree of severity of the impairment affecting the whole person must be specified by applying the general evaluation criteria, by taking the objective effects of the assessed syndrome into consideration, and by referring to the following clauses: Class I: Minor impairment ................................................................... 0 to 15% Class II: Serious impairment ................................................................. 15 to 45% Class III: Extremely serious impairment ................................................ 45% and over
- 35 - Precise quantification in one class may be difficult to achieve, thus the necessity for a comparison with similar cases whose development was followed by the evaluating physician. It may be necessary to wait some time before the final evaluation of the impairment can be carried out. A standard clinical psychiatric or psychological evaluation may not necessarily determine an additional impairment and may be useful only for evaluating the motivation of a patient with an impairment in another system or for establishing that the patient’s potential for a more complete rehabilitation requires further scrutiny before the degree of impairment in the other system is established.
1. CHRONIC BRAIN SYNDROMES:
The syndrome is directly associated with organic brain injury resulting from trauma. Above all, it consists of disturbances of the higher cognitive functions. It is essentially characterized by impairment of orientation, comprehension, memory and of the abilities to learn, anticipate, make decisions and exercise judgement: A supplementary psychometric evaluation may be useful in this case. In addition to these essential signs, the subject may show signs of instability, puerilism, erosion of the importance of moral values, or character disorders. The syndrome is sometimes complicated by psychotic or neurotic reactions in which case they are included in the evaluation. Psychoses or neuroses without organic brain injury will be evaluated separately in their own class. a) Class I
The patient has impairment of the higher cognitive functions but is able to perform most of the activities of daily living, as prior to the accident ..............................................0 to 15%
b) Class II
The patient has impairment of the higher cognitive functions and in some cases exhibits constant or intermittent but recurring psychotic or neurotic symptoms, to such an extent that he requires supervision and direction for several or most of his daily activities .....15 to 45%
- 36 -
c) Class III
The impairment of the higher cognitive functions and the psychological adaptation to the impairment itself are such that the performance of daily activities requires more or less constant care in a protective milieu (home or similar establishment). Patients with extremely severe impairments require help even in meeting their most elementary needs............................................................................................. 45% and over
2. PSYCHOSES:
Psychosis is a severe disturbance of mental function likely to cause more or less considerable impairment, depending on its nature, severity, duration, repercussions, the patient’s history and his reaction to therapeutic measures. It is often advisable to wait two or three years before making the final evaluation of the impairment. The clinical picture may then stabilize and show evidence of permanent impairment. In certain cases basic impairment may be only the more or less strong possibility of relapse. The syndrome is essentially manifested by disturbances in perception, thinking (process, form, content) and behaviour and by abnormalities in emotional control. It is usually accompanied by a lack of self-criticism and often involves abnormal behaviour discernible by those around him. a) Class I
An impairment in this class is manifested by minor and discrete disturbances in perception, thinking, emotional behaviour, but it has little effect on how the patient functions in comparison to his adaptation prior to the accident. Patients who are well controlled by constant psychotropic medication, which allevaites the necessity for rehospitalization, are placed in this class................................................................ 0 to 15%
b) Class II
A psychosis in this class is evident upon mental examination, easily discernible by those around the patient and is reflected in difficulty in social behaviour, odd behaviour and a fairly noticeable reduction in social and personal efficiency. Nevertheless, disorders are not too serious, so the patient can be tolerated in this milieu. The patient’s collaboration is
- 37 -
inconstant, the possibility of intermittent hospitalization is likely and the syndrome is poorly controlled by medication. The patient may require occasional supervision and direction in leading his daily life............................................................................15 to 45%
c) Class III
A psychosis in this class is so severe that the patient manifests disturbances in perception and thinking, and an inability to control his emotions that leads him to behave in a way that is socially intolerable or dangerous to his own well-being. The patient always requires at least part-time supervision and direction so that he can lead his daily life. In more serious cases, he may require a protective milieu or constant care in an establishment, with recurrent hospitalization................................................................................ 45% and over
3. NEUROSES:
Individuals react differently to life’s problems. Some accident victims are prone to adapt neurotically to trauma and its sequelae. Neuroses have no known organic cause. The patient remains lucid and is able to distinguish between external reality and his own subjective experiences. He does not show personality disorganization, but his behaviour may be disturbed within the limits of what is generally acceptable. Neuroses may entail excessive anxiety and phobic, hysterical, obsessive-compulsive, depressive and sometimes even psychosomatic symptoms. Given the strictly subjective nature of neurosis, its great variability, its natural tendency to subside and the motivational context (secondary gains), it is necessary to wait long enough to ensure a strict application of the following general clinical evaluation criteria; previous manner of adaptation, objective repercussions on daily life and relationships, the psychosomatic element, regular continuation of treatment, and social context. a) Class I
i. The neurosis is above all subjective but credible, complete and coherent. It is attended
with minor changes and does not render the victim incapable of adaptive behaviour. There is no reduction in daily activities or in social or personal efficiency ..... 0 to 15%
- 38 - ii. As these impairments do not result from a severe disability, they usually should be
placed in the lowest third of this percentage, specifically from: ...................... 0 to 5%
b) Class II
The symptomatic severity of the neurosis, although usually variable, requires the patient to constantly rely on alleviating therapeutic measures to modify his daily activities, therefore substantially reducing his social and personal efficiency. The neurosis may also entail functional psycho-physiological disorders requiring symptomatic treatment and causing intermittent stoppage of regular activities............................................................ 15 to 45%
c) Class III
i. The neurosis is overpowering and leads to a definite deterioration of personal and social efficiency. Interpersonal relationships undergo considerable and constant changes - isolation or the need of being encouraged and comforted. Daily activities are upset, and the patient needs to be supervised and guided by those around him. Pathological tissue lesions which are more or less reversible may be present with the psychosomatic component. ..................................................................... 45% and over
ii. It is uncommon for a neurotic condition alone to be attended with regression,
deterioration and dependence justifying a percentage higher than the lowest third of this percentage; and impairment should typically be between: .......................45 to 65%
PERSONALITY DISORDERS:
This class mainly concerns character disorders attended with a lack of emotional maturity and expressed as difficulty in interpersonal relationships, poor control of inhibitions, a reduction of tolerance to frustration, excessive egocentricity, inconstancy of efficiency, and fairly serious social maladaptation. In most cases, manifestations of personality disorders existed prior to the accident, and impairment, if any, only increases the pre-existing social maladaptation. The motivational context with respect to temporary demonstrative reactions that are likely to subside after the financially advantageous settlement of the impairment granted must be assessed carefully. A social evaluation in addition to the clinical evaluation may prove useful. Personality changes caused by organic brain syndrome must be evaluated in accordance with the scale provided therefore.
- 39 - a) Class I
i. The level of character adjustment usually existing prior to the accident is consistently
worsened and leads to a more pronounced deficiency in social judgement, deterioration of interpersonal relationships, increasing variability of consistency in efficiency, behavioral deviations and the inability to avoid coming into conflict with society or harming oneself. The patient is not capable of adapting to the difficulties of daily life.......................................................................................................................0 to 15%
ii. In general, the impairment should not exceed the lowest third of this percentage . 0 to
5%
b) Class II
The maladaptation is such that the individual shows considerable loss of self-control, is not able to learn from experience and seriously harms himself and those around him in a repeated manner. The lack of social control may have resulted in legal supervision of various kinds. Such psychiatric or psychological impairment, when considered separately, is rarely granted. It must be determined whether or not such objective behavioral deterioration belongs to another impairment class.............................................. 15 to 45%
The following table, taken from the AMA guides, 2nd edition will simplify computation of a psychiatric impairment. When used according to the best clinical judgement of the evaluator it will aid in the evaluation of an individual and it should be used after all diagnostic, clinical, treatment and rehabilitation factors have been explored.
- 40 -
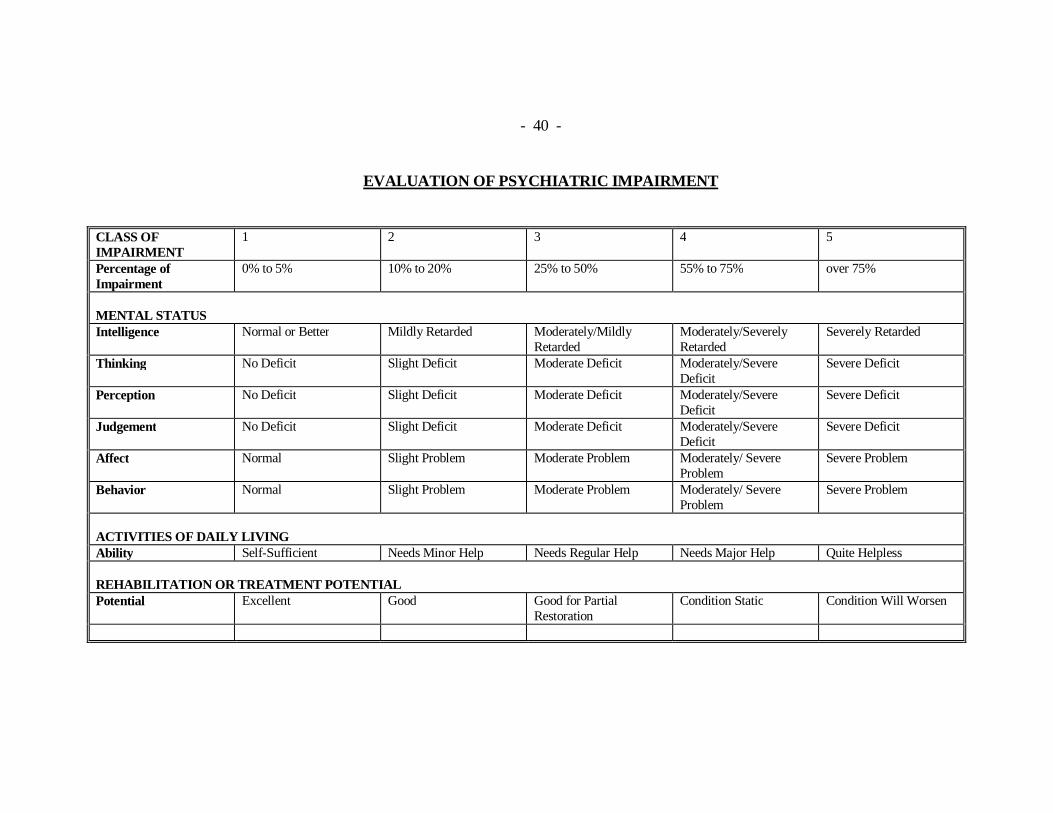
EVALUATION OF PSYCHIATRIC IMPAIRMENT
CLASS OF IMPAIRMENT
1 2 3 4 5
Percentage of Impairment
0% to 5% 10% to 20% 25% to 50% 55% to 75% over 75%
MENTAL STATUS Intelligence Normal or Better Mildly Retarded Moderately/Mildly
Retarded Moderately/Severely Retarded
Severely Retarded
Thinking No Deficit Slight Deficit Moderate Deficit Moderately/Severe Deficit
Severe Deficit
Perception No Deficit Slight Deficit Moderate Deficit Moderately/Severe Deficit
Severe Deficit
Judgement No Deficit Slight Deficit Moderate Deficit Moderately/Severe Deficit
Severe Deficit
Affect Normal Slight Problem Moderate Problem Moderately/ Severe Problem
Severe Problem
Behavior Normal Slight Problem Moderate Problem Moderately/ Severe Problem
Severe Problem
ACTIVITIES OF DAILY LIVING Ability Self-Sufficient Needs Minor Help Needs Regular Help Needs Major Help Quite Helpless REHABILITATION OR TREATMENT POTENTIAL Potential Excellent Good Good for Partial
Restoration Condition Static Condition Will Worsen
- 41 - CANCER The Board of Commissioners, on January 5, 1977, agreed and adopted that gastro-intestinal cancer in asbestos workers be accepted as an industrial disease which under specific conditions is peculiar to and characteristic of a process, trade or occupation involving exposure to asbestos. Furthermore, the Board of Commissioners, on June 14, 1978, agreed and adopted that laryngeal cancer in workers occupationally exposed to asbestos fibre and/or nickel aerosol in specific industrial processes be accepted as an “industrial disease” peculiar to and characteristic of such processes. Inherent to adjudication of such cancer claims is a need to assess and rate residual impairment associated with surgical processes involving the esophagus, stomach, small bowel, colon, rectum, and larynx; including loss of tissue and function. Although rating practices for the variety of problems associated with gastro-intestinal and laryngeal cancer have not been formally addressed, the following criteria has been used to address particular adjudication situations:
Verbal Communication .................................................................................see attached Thyroid Hypofunction ..................................................................................5 to 10% Permanent Tracheostomy (including cosmetic effect) ..................................up to 5%
VERBAL COMMUNICATION CLASS I .............................................................................................................. .. 0%
The worker is able to comprehend and produce speech with adequate speed and clarity of articulation to meet all the daily requirements of communication. There are no problems when dealing with the public, groups or in moderately noisy settings.
- 42 -
CLASS II ............................................................................................................ .. 5%
The worker occasionally experiences difficulty producing or understanding speech and repetition may be required. There may be lack of confidence when having to deal with the public in a professional capacity, and Some phonetic units may be impossible to produce and slight hesitation and slowing of speech pattern is noted, or The worker may sometimes require effort to produce speech of average volume, and voice quality or pitch may be affected. CLASS III ..............................................................................................................10%
The worker can produce or comprehend speech under average conditions and basic communication with strangers presents no problem. The worker experiences some difficulty with communication in group settings or areas of increased noise such as noisy workshops, buses, trains, and restaurants. Speech contains many inaccuracies and is hesitant, interrupted and slow, or The voice tires rapidly and volume fades after a few minutes to become an audible harsh whisper. Communication can be maintained at this level.
CLASS IV ...................................................................................................15 to 20%
The worker experiences considerable difficulty of communication in noisy places. Communication with friends and family usually presents little difficulty but communication with strangers is limited. Speech contains numerous inaccuracies and the need for repetition is frequent, or
- 43 - The worker is able to whisper audibly and communication can be maintained only for brief periods.
CLASS V ......................................................................... 25 to 35% The worker experiences major problems with communication and can barely comprehend or be understood over the telephone. Basic information can be exchanged with friends and family but communication with strangers is extremely difficult or impossible, or The worker essentially has no voice and the needs for everyday communication cannot be satisfied.





























