Embed Size (px)
Citation preview

[CANCER RESEARCH 47, 5518-5527, November, 1987]
Perspectivesin CancerResearch
Genetics of Cancer Predisposition
Marc F. Hansen and Webster K. Cavenee
Ludwig Institute for Cancer Research (Montreal Branch), Royal Victoria Hospital, Montreal, Quebec, Hi A ¡AlCanada
Formal genetic analysis of cancer engenders several paradoxical situations: (a) although familial instances are well described, most disease occurs as sporadic isolated cases; (b) evenin those cases arising subsequent to inheritance, tumors arefocal in nature rather than affecting all cells of a particulartissue; (c) individuals in those families who exhibit high propensities to malignancy appear to be at risk for broad, butspecific, subsets of cancer. Here we have consolidated evidencefrom familial, epidemiológica!, cytogenetic, and molecular genetic studies which support the notion that cancer is a profoundly genetic disease and which help explain the aforementioned seeming paradoxes. We review approaches and resultsaddressing these questions afforded by molecular biologicaltechnologies and speculate on the nature of genetic lesionsresponsible for predisposition to cancer.
Familial Clustering
The observation of a family with a high proportion of members who developed breast or liver cancer led to the firstproposal in 1866 (1) that familial aggregation of malignancywas due to some inherited aberration within the affected tissuethat allowed tumor development. Similarly, studies of spontaneous mammary tumor formation among inbred strains of miceindicated that predisposition to tumorigenesis behaved in aformal sense as a Mendelian genetic trait (2) such that femalemice whose recent female ancestors had developed breast tumors incurred a much higher risk of developing similar tumorsthan females from strains with non-tumor-bearing ancestors.
Several subsequent studies of human cancer have supportedthese indications of inheritance as a component of the etiology.Analysis of cancer patients from five pedigrees indicated thatimmediate family units tended towards an increased incidenceof disease although the inheritance patterns of their extendedfamilies were not necessarily clear (3). These limited sets oftumor aggregation were termed "cancer fraternities" and were
postulated to arise through the mating of two heterozygouslysusceptible but unaffected parents (3). Analyses of the pedigreesof all cancer patients admitted to the University of Michiganhospital between 1895 and 1913 indicated that 15% of 3,600patients had some familial history of cancer (4). Accuratemultigenerational data from four families were compiled andsusceptibilities to several specific cancer types appeared to betransmitted as autosomal dominant Mendelian traits. The largest of these families was afflicted exclusively by cancers of thedigestive tract and uterus that were predominantly of earlieronset than the general population. The term "cancer family"
was coined to designate this aggregation of specific types oftumors. Subsequent studies of other cancer families suggestedthat many other types of tumors also have a genetically determined component in their etiology (5-9).
The proposal that neoplasia has an inherited sensitivity aspart of the process has a corollary that such genetically markedindividuals should often develop tumors at multiple distinct
Received 6/10/87; revised 8/6/87; accepted 8/10/87.
sites. In fact, as early as 1932 it was possible to document 1,259patients with multiple primary cancers (10), a number that hasbeen extended to well over 30,000 cases to date (11). Suchtumors can be categorized as simply multifocal or multicentricor as different types of cancers in different tissues. One particularly striking example of multicentric neoplasia arose throughcareful gross and microscopic examination of tissues frompatients treated for primary epithelial carcinoma (11); between20 and 93% of all cases showed multiple primary epithelialcancer of shared epithelial surfaces [e.g., lips and skin; kidney,ureter, urethra, and stomach (12); colon (13); liver (11); andbreast (14)]. Although these multiple tumors appeared to beindependent primary events, the level of resolution of histo-pathological analysis was not, of course, fine enough to eliminate the possibility of multiple early métastases.Conversely,many patients who died of a first primary tumor would nothave had the opportunity to develop others, thus making theincidence estimates cited above artificially low. Nonetheless, itis quite clear that the presence of one malignancy in theseindividuals indicates a great likelihood that a second malignancy of similar type has occurred. Thus, predisposition tothese tumor types does not appear to simply reside in a singlecell of a given histological type but rather in many, or even all,such cells.
A second clinical phenomenon suggesting a genetic diathesisof cancer is the occurrence of multiple primary malignanciesarising in different tissues of the same patient. In adults, manytumor associations have been reported (11) to occur at greaterfrequency than would be expected by chance. For instance,breast cancer has been associated with cancers of the colon,larynx, bone, ovaries, salivary gland, and uterus while similarsorts of associations have been reported between other primarycancers. Although the numbers of cancers clinically associatedone with the other appears large, clearly discernible groups canbe ascertained; for example, leukemia appears to be associatedwith cancers of the lung, skin, thyroid, and melanocytes but notwith those cancers associated with breast cancer. These specificassociations may be defining the range of predisposition due toa single defect inherent in those individuals. Alternatively, thesecancer-cancer associations may be merely an artifact of therelative thoroughness with which various cancer types are diagnosed and recorded, the age at which a second malignancybecomes apparent, differential geographic incidence of specificmalignant neoplasias, or even of differential therapies elicitingsubsequent second tumors.
The genetics of a familial inheritance of susceptibility tomultiple primary malignancies is perhaps best documented ina clinical presentation known as "Cancer Family Syndrome"
(15). These families are characterized by the occurrence ofadenocarcinomas of the colon and endometrium in half theoffspring of an affected parent. The risk for development of asecond site primary cancer in an affected member of such afamily is about 50% during the first 18 years after the firstprimary tumor. The predisposition to more than one tumortype in these families is inherited with a probability consistent
5518
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
with a single highly penetrant autosomal dominant Mendeliantrait. Similar families have been identified which appear to besegregating defective genes which predispose to specific groupsof tumors, for example premenopausal breast cancer and osteo-sarcoma.1 Thus, it seems reasonable to postulate that these
families are, in effect, defining the tissue specificities of theaberrant gene they are segregating.
The final example of tumor-tumor associations involves theexamination of second primary tumors arising in children.Clearly, in adults some common tumor types may arise irrespective of a primary tumor and any aberration in geographicdistribution which enhances the frequency of such tumor typeswould strengthen any apparent association. Additionally, manyadult tumors are not readily treatable by current therapies andso such patients would not be expected to live long enough todevelop a second tumor. Tumors of childhood, however, haverecently proven more manageable. They also arise early in lifeso that, if successfully managed, the possibility for developmentof a second site tumor later in life is increased. Several suchchildhood tumor associations have been reported including:Wilms' tumor with hepatoblastoma, mesothelioma, adrenocor-tical carcinoma, and basal cell carcinoma; and Ewing's sarcoma
with adenocarcinoma of the breast, rhabdomyosarcoma, andosteogenic sarcoma (16). The overall frequency of second malignant neoplasm development in survivors of first childhoodtumors is about 15% (17), even though the average incidenceof any of these tumors singly is about 1:10,000 live births. Thus,the specific types of second primary tumors arising in childrenwith a first primary tumor may be indicative of the tissueswhich share a common predisposition to malignancy.
Two clear, and perhaps prototypic, examples of tumor clustering exist which may allow the combination of analyses offamilial manifestation of multiple tumor types as well as thoseof second malignancies in children. The first of these examples,the association of bilateral retinoblastoma and subsequent os-teosarcoma ( 18,19), may represent the best in vivo evidence forcancer genes with less than absolute tissue specificity. Thesecond example is the heritable predisposition to several tumortypes classified as the multiple endocrine neoplasias, types I,II, and III (20-22).
Retinoblastoma is one of a group of childhood tumors towhich predisposition can be inherited as an autosomal dominant trait (23, 24). The inherited form of the disease generallypresents in both eyes whereas the sporadic form presents inonly a single eye (25). Advances in surgical technique andradiotherapy have led to survival rates exceeding 90% forretinoblastoma patients. However, it has been observed (18,19)that patients with bilateral but not unilateral retinoblastomahave a high incidence of the development of independent second-site tumors; of 693 bilateral retinoblastoma cases, 15%developed second primary tumors, about 45% of which wereosteogenic sarcomas (19). Importantly, survivors of nonherita-ble unilateral retinoblastoma appear to have no increased riskfor the development of these second site tumors. Additionalsupport for the idea of a genetic association between these twodisparate tumor types comes from a family in which two half-sibs with bilateral retinoblastoma were fathered by the sameman who subsequently developed osteosarcoma himself (26).
The second example of familial clustering of multiple tumortypes are the multiple endocrine neoplasias. MEN2 type Iappears to be inherited as an autosomal dominant trait com-
1L. Strong, personal communication.2The abbreviations used are: MEN, multiple endocrine neoplasia; RFLP,
restriction fragment length polymorphism(s).
posed of tumors of the pituitary, parathyroid, adrenal cortex,and pancreas (20). Although each of these tumor types canoccur in a single family, it is rare that any one patient developscancer in more than one or two endocrine glands. It has beensuggested that this constellation of tumors results from defective differentiation of neural crest tissue. MEN type II alsoappears to be inherited as an autosomal dominant trait composed of pheochromocytomas in patients with medullary thyroid carcinoma; other tumors reported in MEN II patientsinclude meningiomas, gliomas, and glioblastomas. MEN typeIII also appears to arise subsequent to an autosomal dominantmutation which results in pheochromocytoma, medullary thyroid carcinoma, and mucosa! neuromas of the conjunctiva,labia, and bucea (21). Several other developmental abnormalities are also often present including pseudoprognathism, enlarged corneal nerves, hypotonia, lax joints, kyphoscoliosis,megacolon, genu valgus, and pes cavus.
Thus, the preceding discussion indicates a strong familialcomponent in the etiology of human cancer. The cited studies,however, cannot address formal models for the mechanisticbasis of this phenomenon.
Epidemiological Modeling
In 1902, Boveri (27) noted that sea urchin eggs fertilized bytwo sperm often underwent abnormal mitotic divisions leadingto loss of chromosomes in the daughter cells and atypical tissuemasses in the gastrula. He also noted that these abnormaltissues appeared physically analogous to the poorly differentiated tissue masses found in tumors and hypothesized thatcancer arose from a cellular aberration that elicited asymmetrical mitotic figures thereby resulting in the loosely defined tissuemass of both the tumor and dispermie sea urchin gastrula.These astute observations and prescient postulations appear toprovide the first support for the notion that tumors representmasses of inherently abnormal cells rather than a stimulationor acceleration of normal cellular growth.
A mechanism whereby cells from presumably normal tissuecould give rise to tumors was proposed in 1916 following theobservation that spontaneous tumors arising in Japanese waltzing mice showed a wide variation in their ability to be transplanted to other mice (28). Since spontaneous tumors from oneisogenic strain could differ in their transplantability to genetically identical host mice, this variation did not seem to bedependent on the genetic background of either the donor or therecipient strain. This characteristic appeared to arise de novoin the tumor and was then capable of horizontal transmissionby implantation of the tumor, a phenomenon termed somaticmutation since it could not be passed genetically to the offspringof parents which developed the disease.
Although this theory was consistent with the behavior oftransplanted tumors in an inbred population, it could notaddress the observed phenomenon of increased susceptibility tocancer with increasing age in humans; if the rate of somaticmutation were constant throughout life, the likelihood of tumorformation would also be expected to remain constant. Thisdiscrepancy could be resolved if, as hypothesized (29), thecorrelation of cancer and increasing age was due, not to an age-related increase in the rate of somatic mutation, but rather toan increase in the size of the population of cells at risk and theconsequent increased stochastic probability that any one cellwould undergo the somatic mutation (or mutations) leading totumor formation. Alternatively, the discrepancy could be dueto the somatic mutation giving rise to a tumor requiring a
5519
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
"latency" period prior to its expression (30). However, analysisof tumors arising subsequent to X-irradiation suggested a latency period of approximately 9 years, a time span that couldnot account for the occurrence of tumors in young children,particularly those apparent prior to the first year of age. Subsequently, epidemiológica! analyses of stomach cancer incidence at different ages (31) led to the proposal that cancer arosenot by one mutation in a single cell, but rather through singlemutations in several adjacent cells. Subcriticai masses of thesemutant cells were postulated to remain dormant until sufficientadjacent cells had undergone mutation to achieve a critical masswhich then cross-fed and subsequently developed into a tumor.
A mathematical treatment of these data suggested that thenumber of cancer cells present in any tissue would be proportional to the age of the tissue raised to the power of one lessthan the number of cells necessary to form a cancer island.Supportive evidence for this formulation was provided by statistical studies of the incidence of deaths due to stomach cancerin American females (31). This analysis appeared particularlyappropriate due to the short interval between diagnosis ofstomach cancer and death, which made the incidence of cancerdeaths an accurate reflection of cancer onset. A graphical comparison of the logarithm of the age at diagnosis and the corresponding logarithm of the death rates indicated a linear relationship with a slope (which is equal to one less than the numberof cells critical to form an island) of 5.7, indicating that thenumber of cells necessary to form a stomach cancer island wasbetween six and seven.
There were, however, several problems that this hypothesiscould not explain. First was the problem of early onset disease,such as childhood tumors, which showed a corresponding relationship requiring far fewer than the six or seven mutant cellsnecessary for an adult stomach cancer island. It was suggestedthat the rapid division of tissues during organismal developmentmight lead to an enhanced susceptibility to mutation and thatthe number of cancer cells necessary to form an island mightalso be fewer in the developing fetus (31). Secondly, this hypothesis could not explain the incidence of carcinogen-inducedcancers in experimental animals since one would predict thatthis cancer incidence should be proportional to the concentration of the carcinogen, raised to the fifth or sixth power.However, experimentally, the proportionality of tumor incidence and concentration of carcinogen vary in arithmetic ratherthan exponential order (32).
Alternative hypotheses to explain the age-dependent increasein cancer incidence were put forth which proposed that a singlesomatic mutation was insufficient to elicit a tumor and thattumors arose from a single cell which underwent multiplesomatic mutations (29, 33). A comparison of the incidence ofcancer deaths and age of diagnosis in 25- to 74-year-old malesin the United States, Great Britain, France, and Norway produced a best fit with a model requiring six independent mutations to produce a tumor, assuming that the rate for eachmutation was constant and equal throughout life (30). Similaranalyses of Welsh cancer deaths corroborated this quantification (34-36). This hypothesis still did not explain the highincidence of childhood cancers, a discrepancy noted by Nordling(29) in his proposal that childhood cancers arise from alteredfetal cells which are inherently more susceptible to mutation.The hypothesis was, however, in agreement with the evidencefrom experimental carcinogenesis in its prediction that theincidence of tumor formation would be directly proportional tothe concentration of carcinogen (32).
This notion of cancer being elicited by multiple mutations in
a single cell gained support through the examination of deathrates for men and women of differing age groups from cancersof the esophagus, stomach, colon, rectum, pancreas, lungs,bladder, prostate, breast, ovary, cervix, and corpus uteri, whichshowed that the first four types clearly increased in incidencewith age (32). Formally, the data were consistent with approximately six to seven intracellular events being required fortumor formation. However, the incidence of cancers of lung,bladder, and prostate in men and lung, breast, ovary, cervix,and corpus uteri in women showed a significant departure frompredicted mortality that was not consistent with this number ofevents. It was suggested that this departure was due to thepresence of factors which increased the likelihood of cancer andthereby biased the incidence rates. For example, the incidenceof lung tumors in the older age groups was lower than in themiddle age groups. Since cigarette smoking had been popularfor less than 50 years, members of the older age groups wereless likely to have indulged in this practice than members ofthe middle age groups. Thus, a reasonable explanation for thedeparture from expected incidence ratios was that the middleage group had been exposed to the mutating effect of cigarettesmoke for a larger proportion of their lives than had the olderage groups.
A refinement of the "one cell, multiple hits" theory proposed
that one effect of a first mutation might be to increase thegrowth rate of the mutated cell (37). One prediction of thishypothesis is that as the tissue proliferates, the proportion ofcells in the tissue which carry the first mutation will increase,thereby enlarging the population of cells at risk for a subsequentmutation. It was reasoned that if the probability of undergoinga first mutation was p, per unit time, if each cell that hadundergone the first mutation gave rise to a clonal populationof cells of ekt at time / after the initial mutation where A:is a
constant, and if the probability of a second mutation in one ofthose cells in which a first mutation has already taken placewasp2i*' per unit time t, then the incidence of a cell undergoing
both mutations at any given time could be mathematicallypredicted by the expression
/ = Np,[l - exp((-p2/k)(exp(Ai - 1)))]
where N is the number of cells in the tissue at risk for the firstmutation (38). As t becomes larger, the expression asymptotically approaches / = Np\.
The aforementioned multiple-step carcinogenesis hypothesesof Muller (33) and Nordling (29) required only that the firstmutation be time independent, and thus their predictions of theincidence of cancer simplified mathematically to this sameasymptotic approach. This suggested that it was possible torequire as few as two mutations to fit the incidence curves, ifthe first mutation led to growth of the mutated cells. In thisway, it was possible to account for the perturbations in thepreviously proposed mathematical models. This formulationcould also account for the latency period between exposure toa mutagenic agent and the appearance of the tumor by considering that a tumorigenic agent induces a first mutation leadingto an increased growth rate and a consequently larger population of vulnerable cells, any one of which could produce neo-plastic growth upon a second mutational event. It could alsoaccount for earlier findings that tumors in murine mammaryglands were surrounded by "hyperplastic nodules" of rapidly
growing cells (2) and for the clinical observation of hyperplasiain premalignant tissues such as intestinal polyps in humans(39). The model would predict that the nodules were composedof cells which had received the first (growth-stimulating) mu-
5520
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
tation but had not undergone the second (tumor-forming) event.The first model (40) to explain the incidence of childhood
malignancies arose from a joint consideration of suggestionsthat tumors arose subsequent to two events (38) and that apremalignant mutation might be inherited but not expresseduntil the cell was exposed to an unfavorable environment (41).This model proposed that latency could be due to a prezygoticmutation, which was not itself oncogenic but which insteadpredisposed the cells to a second somatic alteration underconditions of stress which then gave rise to neoplastic growth(40). This idea did not require that the initial somatic mutationlead to favored growth of the cell but instead postulated thatthe initial mutation was present in all cells of the body by virtueof germline inheritance. Since the likelihood of a second eventoccurring in a previously mutated cell over a long period oftime is essentially independent of the frequency of the secondevent (38), those individuals who inherited the first mutationwould inevitably suffer the second alteration in at least onetarget cell and, consequently, develop cancer. The applicationof this hypothesis to childhood leukemia showed that earlyonset forms of leukemia occurred with kinetics consistent witha single event, suggesting that the first mutation occurredprezygotically, and led to the suggestion that childhood leukemia could be grouped into those that had a prezygotic mutationand thus required further somatic alterations and those that didnot inherit such a mutation but rather required cumulativepostzygotic events for oncogenesis. This hypothesis was extended to leukemias of known familial or environmental origin(42) and the data indicated that inherited mutations couldsubstitute for somatic mutations in all cases where the etiologyof a tumor required multiple postzygotic events. Furthermore,one stated constraint on this model was the requirement forone or more somatic mutations together with other epigeneticevents for onset of the disease; otherwise such a mutationalcombination would probably be prenatali) lethal.
Analysis of solid tumors of childhood has been most fruitfuland has led to specific hypotheses about the number, nature,and relationship between pre- and postzygotic genomic alterations in the process of human cancer (43-47). The data haveindicated the necessity of as few as two mutations in the samecell for the initiation of a tumor; that sporadic and heritableforms of disease were likely to arise by alterations of the samegenetic loci; and that the kinetics of cell renewal in the stagesof tissue differentiation plays a role in determining the frequency and age of onset of various tumor types (43). Theseproposals distill all of the common themes of the aforementioned approaches and, furthermore, overcome most of theirweaknesses. The initial comparison of bilateral and unilateralretinoblastoma cases (44) indicated that the two forms of disease differed significantly in age of onset, number of tumorclones, and heritability. When the ages of diagnosis for the twoforms of the diseases were graphically displayed, bilateral casesappeared to show kinetics requiring a single event, while unilateral cases appeared to require two events in their etiology. Itseemed that these differences were unlikely to be due to mutations at different loci, since unilaterally affected parents couldsometimes give rise to bilaterally affected progeny. It wasproposed that both forms of retinoblastoma occur by sequentialmutations, each of which arises at a rate of 2 x IO"7 per cell
per year; the essential difference between the two forms of thedisease was hypothesized to be the somatic or germinal occurrence of the first mutation. This formulation was entirely consistent with the aforementioned models (38, 40), as well as theclinical evidence, and furthermore made specific predictions
about the mechanism of tumorigenesis in this disease. Similarresults were obtained with a variety of other solid tumors ofchildhood, particularly Wilms' tumor, neuroblastoma, and phe-
ochromocytoma (45, 46). Importantly, the general model (47)could be extended to adult cancers such as breast cancer (48)and medullary thyroid carcinoma (49) with only minor modifications.
Thus, the analyses described in the preceding section haveconverged to provide a mechanistic model which specifies theinvolvement of prezygotic and postzygotic lesions in the genesisof human cancer. They do not address, except in a speculativeway, the biological nature of these lesions.
Somatic Cell Genetics of Tumorigenesis
A great deal of important information concerning the geneticbehavior of cellular transformation has been obtained throughascertainment of the tumorigenicity of somatic fusions betweennormal and tumor cells in vitro (50-54). Early experimentsusing interspecies hybrids between mouse and hamster cellsprovided conflicting data indicating that fusion progeny couldhave either normal or tumorigenic phenotypes (55). Karyotypicanalyses suggested that a major difficulty with this line ofexperimentation was chromosomal instability of the hybrid cellsuch that genetic material of the normal parent in such crosseswas rapidly lost upon passage in culture (55).
More informative and reproducible results were obtainedwhen both normal and tumorigenic parents were derived fromthe same species since these crosses produced relatively stableprogeny. A particularly interesting set of experiments of thistype involved the fusion of normal human fibroblasts withvarious human tumor cell lines (56, 57). In these studies, theprogeny of normal x normal parents were nontumorigenicwhile those of the fusion of similar tumor type were tumorigenic. However, in each instance, progeny of normal x tumorigenic parents were completely nontumorigenic. Furthermore,rare revenants of this latter class were isolated (58) which hadbecome tumorigenic. In these revenants, particular pairs ofchromosomes had been lost. These general results have beencomplemented by an elegant series of studies using Chinesehamster embryo fibroblast cell lines (59). Two possible interpretations of these data are that normal cells express geneproducts the functions of which are to suppress tumorigenicityor that the normal cells were providing a function that had beenlost by the tumor cells which was required for maintenance ofthe normal phenotype. The first, more activist, interpretationis consistent with a model proposed by Comings (60) in whichcells carry genes which encode products which act as repressersof other tumor-causing genes. The second interpretation isconsistent not only with this view but also with the broadernotion that tumorigenicity arises subsequent to the total loss ofsome required cellular function, i.e., by the development ofhomozygosity for recessive mutant alÃelesat some unspecifiedloci. The major difficulties with this line of experimentationare the lack of objective criteria for transformation and tumorigenicity and the extension of information obtained in culturedcell lines to the human neoplastic process. The definition ofsuppression of tumorigenicity is necessarily separated fromcertain aspects of transformation such as anchorage independence, serum requirements, and contact inhibition. These in vitrocriteria for transformation have been suggested (61, 62) to beunnecessary for in vivo tumorigenesis. Similarly, when individual chromosomes are introduced into tumor cells, the resulting
5521
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
phenotype does not resemble normal cells but is, rather, different from either tumor or normal parental cells (63, 64).
Retinoblastoma, a Prototypic Neoplasm
Cytogenetics. Evidence supporting the notion of a geneticbasis of human cancer has been provided through direct cyto-genetic examination of the chromosome numbers and theirarrangement in tumor cells. As the resolution of these analyseshas increased and they have been extended to solid tumors,various chromosomal abnormalities have been described whichappear to be consistent within a tumor type (65). These abnormalities most frequently take the form of deletion of particularportions of the genome or chromosomal interchanges betweenspecific regions of two chromosomes.
Although these aberrations are best documented in lymphoidtumors, several instances have been reproducibly described insolid tumors as well (66, 67). Perhaps one of the clearestexamples is the deletion of the interstitial band q 14 of chromosome 13 in retinoblastoma. Beginning in the early 1960sand 1970s cases have been reported (68-70) with karyotypes ofconstitutional cells showing deletions of the long arm of chromosome 13. Although these deletions were discernible in onlyabout 5% of retinoblastoma patients and the extent of deletionvaried considerably, the smallest overlapping region of aberration was the band 13ql4. Furthermore, analysis of tumor cellsfrom patients with normal constitutional karyotypes indicatedthat about 5% of cases had tumor-specific deletions of chromosome 13, each of which included the ql4 band (71-74).Although striking, the significance of these observations wasunclear for several reasons. First, only a small proportion ofcases carried visible constitutional or somatic deletions. Secondly, in those cases in which a 13ql4 deletion was apparentin all cells, not all retinal cells were neoplastic. Clearly thesealterations were insufficient in and of themselves to elicit disease. Finally, tumor (but not constitutional) karyotypes haveshown several other chromosomal aberrancies in addition todeletion of 13ql4 such as triplication of Iq23-lqter and anisochromosome 6p (74).
However, these deletion cases have been useful in definingthe region of the genome likely to contain a locus involved inthe genesis of retinoblastoma not only by inference from thephysical map but also by genetic linkage mapping. Activitylevels of esterase D, an enzyme of unknown physiologicalfunction, were shown to be reduced in patients with deletionsof 13ql4 as compared to their karyotypically normal familymembers (75). This enzymatic activity also displayed isozymicforms in the human population so that the cosegregation of aspecific allelic variant with retinoblastoma could be determinedin families (23). In fact, no meiotic recombination events couldbe detected, strongly suggesting that a genetic locus influencingtumor development resided in the 13ql4 region. Additionally,the involvement of this region has been substantiated by theidentification and cytogenetic analysis of a remarkable kindred(24). In this family, both affected and unaffected members weredescribed that carried an interstitial 13ql4 deletion. However,several of the unaffected members also carried a chromosome3 which included an interstitial translocation of this 13ql4region. Thus, all family members who were constitutionallymonosomic for the region developed disease whereas all whowere either disomic or trisomie were spared. These data stronglysuggested that the deletional event predisposed to retinoblastoma, that this region did indeed contain a locus or loci involvedwith tumor development, and that the initial mutation wasunlikely to be acting in a dominant genetic fashion.
The limitations of these sorts of analyses in describing unifying genetic mechanisms are obvious. The first is the relativelysmall proportion of diseased individuals who display cytoge-netically visible chromosomal aberrations. This could be due tothe restricted precision of the analysis but could also be due torandom rearrangements in the process of tumorigenesis. Secondly, the combination of low level analytical resolution withallelic data that relies on enzyme expression can be misleadingas well. One particularly appropriate example of this was areported case of a child with bilateral retinoblastoma (76).Analysis of esterase D activity in blood and fibroblasts fromthis patient indicated about one-half the level of that in thegeneral population. However, cytogenetic analysis of these samecells revealed no observed deletion of chromosome 13. Tumorcells from this child showed an absence of esterase D activityand a single distinguishable chromosome 13. On this basis, itwas concluded that the chromosome 13 in the tumor cellscarried a submicroscopic deletion of 13ql4 that entirely eliminated both the esterase D (ESD) and retinoblastoma (RBI)loci. This proposal would, of course, be consistent with the ideathat the initial deletion mutation in this child was recessive atthe cellular level and was unmasked by chromosome loss of thehomologue carrying the wild type RBI alÃele.However, it isalso possible (and, in light of recent molecular data discussedbelow, likely) that these results could be explained by simultaneous intralocus mutations in the ESD and RBI loci, in whichcase they shed little light on the genetic mechanisms involvedin tumorigenesis. A final example of how this combined determination of esterase D activity or isozymic forms with cytoge-netics can be misleading is illustrated in a study of six cases ofretinoblastoma (77). Each of these patients was constitutionallyheterozygous at the ESD locus (i.e., displayed both electropho-rectic variants) and none had any obvious deletion of theirchromosome 13. The corresponding tumor cells from four ofthese six patients showed only one isoform of esterase D andno deletion in either chromosome 13 homologue. These dataare consistent with mechanisms involving either somatic mu-tation/deletion/inactivation of one alÃeleof the ESD locus,mosaicism for a 13ql4 deletion and clonal expansion of a cellcontaining such an aberration, or somatic loss of one chromosome 13 homologue with duplication of the other resulting intwo chromosomes 13 identical at every locus. The secondpossibility was discounted by examining several individual fi-broblast clones from each patient and establishing that eachexpressed both ESD isozymes. The third possibility was discounted on the basis of cytogenetic examination of fibroblastand tumor cells from one patient, both of which were heterozygous for a chromosome 13 fluorescent-staining satellite sequence. It was proposed therefore that retinoblastoma arose inthese patients through a spread of somatic inactivation fromthe ESD to the RBI locus in a manner analogous to X-chro-mosome inactivation in females. However, molecular geneticanalyses described below indicate that the third mechanismabove, or variations thereof, was extant in these and other cases.
Molecular Genetics. The foregoing discussion raises severalsalient points regarding mechanisms of development of humanneoplasia. It seems likely that cancer is a disease with a geneticbasis; specific chromosomal aberrations appear to be a route toits expression. Single genetic events, even in individuals proneto cancer development by virtue of inheritance, seem to beinsufficient to elicit disease; epidemiológica! and theoreticalconsiderations suggest that, in some cancer types, as few as twogenetic alterations may be required. The behavior of the transformed phenotype in vitro indicates that tumorigenicity may
5522
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
arise through the elimination of tumor suppressor genes andanalysis of the pathology of individuals with familial cancersuggests that those cells with only the initial prezygotic lesionhave no hétérozygotephenotype.
A model was proposed which could account for each of thesepoints and which predicted several specific chromosomal mechanisms capable of unmasking predisposing mutations. Each ofthese chromosomal mechanisms would be expected to be mi-totic and each would have as its net effect the somatic attainment of homozygosity for a mutant alÃeleat a relevant locus.These chromosomal mechanisms included: mitotic nondisjunc-tion with loss of the wild type chromosome, which would resultin hemizygosity at all loci on the chromosome; mitotic nondis-junction with duplication of the mutant chromosome, whichwould result in homozygosity at all loci on the chromosome;mitotic recombination between the chromosomal homologueswith a breakpoint between the tumor locus and the centromere,which would result in heterozygosity at loci in the proximalregion of the chromosome and homozygosity throughout therest of the chromosome, including the tumor locus; or regionalsecond events such as gene conversion, deletion, or point mutation. Sporadic disease could also arise through the appearanceof homozygosity at the tumor locus, the difference being, inthis instance, two somatic events as compared to one germinaland one somatic event in heritable cases (44).
The method that was used to examine these hypotheses (78)relies on the variability of DNA sequences among humanswhich results in inherited differences in restriction endonucle-ase recognition sites. In this approach, segments of the humangenome are isolated in recombinant DNA form and the locihomologous to these probe segments are tested for their encompassing restriction endonuclease recognition sequences whichmay vary among unrelated individuals. Two types of suchvariation have been defined. The first, and most abundant,results from simple base pair changes within the recognitionsite sequence of a particular restriction endonuclease and yieldsalÃelesof longer (when the effect of the mutation is loss of asite) or shorter (when the effect of the mutation is the gain of asite) length. The second type results from the insertion ordeletion of varying numbers of blocks of like DNA sequenceinto or out of the genomic locus. Practically, the net result isthe observation of two alÃelesat the locus encompassing a sitechange (presence or absence of the site) in the first case ornumerous alÃelesat a locus subject to insertion or deletion oflarger segments of DNA. In either case, however, any givenindividual will reveal only two alÃelesat the locus, one from thepaternally derived and one from the maternally derived homologue. In all cases examined to date these types of markers havebeen shown to behave in family studies as would be predictedfor simple Mendelian codominant alÃeles.It is notable thatthese RFLP would be apparent regardless of the tissue originof the DNA sample and also that this type of analysis does notrely on the expression or determination of different proteinisoforms. It is also noteworthy that a RFLP locus is defined bythe probe and the relevant restriction endonuclease; consequently the number of such loci is virtually limitless. Recombinant DNA segments were isolated from human chromosome13, as well as other chromosomes, and used as probes toexamine loci scattered along the chromosome in order to detectchanges in the somatic genotypes of tumors, as compared tothe germline genotypes of the individuals harboring the tumors(78).
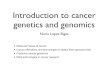
A schematic illustration of the model and its specific experimental predictions is shown in Fig. 1. In this model the hered
itary form of the disease (Fig. 1, left) arises subsequent to theinheritance of a germinal mutation at the RBI locus from themother and is, therefore, present in all somatic and germ cellsof the daughter. The sporadic form (Fig. 1, right) arises subsequent to a somatic mutation at the Rii I locus in a single retinalcell. Any subsequent event that results in hemizygosity orhomozygosity for the mutant alÃele(i.e., mutant at the RBIlocus on both chromosome 13 homologues) will result in atumor clone. Furthermore, these chromosomes are differentially marked by restriction fragment length polymorphisms atthe loci designated A and B that flank the RBI locus. Severalchromosomal mechanisms which could accomplish the somaticattainment of homozygosity for a mutant alÃeleat the RBIlocus are illustrated at the bottom of the figure.
If the extant mechanism was mitotic nondisjunction with lossof the wild type chromosome, the net result would be hemizygosity for all loci on chromosome 13; a comparison of thenormal and tumor DNA at the two RFLP loci would show acoordinate loss of constitutional heterozygosity. The intensityof hybridization of the remaining alÃeleat each locus in thetumor DNA would be equal to the intensity of hybridization ofeither alÃelein the normal DNA. If the mechanism involvedmitotic nondisjunction and loss of the wild type chromosomefollowed by duplication of the mutant chromosome, analysiswould yield slightly different results. The prediction would becoordinate loss of constitutional heterozygosity at both lociwith the intensity of hybridization of the remaining alÃeleateach locus being twice that of either alÃelein the normal DNA.If the mechanism of loss of the wild-type alÃelewas mitoticrecombination with a breakpoint between the proximal RFLPlocus and Rlil. then genotypic determinations in normal andtumor DNA would be expected to show a loss of constitutionalheterozygosity at the distal RFLP locus. The proximal RFLPlocus, however, would be expected to remain heterozygous. Theintensity of hybridization of the remaining alÃeleat the distallocus would be twice the intensity of either alÃelein the normalDNA, suggesting that there was not simply a deletion of theproximal region of the chromosome. The identified RFLP lociare physically distant from the RBI locus, so other proposedmechanisms leading to loss of the wild-type alÃele,such as geneconversion, point mutation, and small deletion which resultonly in alteration at the RBI locus, would not be detected bythis analysis.
Thirty-three cases of retinoblastoma have been analyzed inthis manner, and the relative distribution of chromosomalevents accomplishing loss of constitutional heterozygosity atthe RBI locus in these tumors is shown in Fig. 1, bottom. Thedata indicated that 24 of these cases arose through mitoticnondisjunction or recombination. Interestingly, several of thetumors which had been reported to undergo somatic inactiva-tion of the region encompassing the ESD and RBI loci (77),when examined at this level of resolution, had instead undergone aberrancies in mitosis. For example, the case which had adistinguishing satellite region (77) had, in fact, arisen throughmitotic recombination (78). Furthermore, these chromosomerearrangements and losses appeared to be specific to chromosome 13 since tested loci on other chromosomes retained heterozygosity in the tumors. Corroboration of these inferenceshas been obtained by examining cases of heritable retinoblastoma (79) and showing that the chromosome 13 homologueretained in the tumor was derived from the affected parent aswould be predicted.
These observations are consistent with all of the lines ofinvestigation discussed above and suggest that chromosomal
5523
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
Heritable
99»
rb
2
2! ¡2
Sporadic
OrOoo 99
2 i ¡2
2
99
: :: ;i iZi i oi i 2
rb
O99
Constitutional
99
Predisposed retinoblast rb
Retinoblastoma
Fig. 1. Chromosomal mechanisms by which an initial predisposing recessive germinal or somatic mutation could be revealed. In a hereditary case (left) the childinherits a chromosome 13 from her affected mother which carries a recessive defect at the RBI locus (designated rb) and so is genotypically re/+ in all of her cells. Aretinoblastoma tumor would occur after the elimination of the dominant wild-type alÃeleat the KHI locus by one of the mechanisms shown at the bottom of the
unmasked by one of the mechanisms shown at the bottom. Reprinted by permission of Elsevier Press from an article by W. Cavenee, A. Koufos and M. Hansen inMutation Research 168: 3-14, 1986.
mechanisms are involved in multistage carcinogenesis and thattheir effects can be to unmask recessive mutations at specificloci. It is noteworthy that, although the unmasking of predisposing mutations at the RBI locus occurs in mechanisticallysimilar ways in sporadic and heritable retinoblastoma cases,only the latter carry the initial mutation in each of their cells.Heritable cases also seem to be at increased risk for the development of second primary tumors, particularly osteogenic sarcoma (18, 19, 26). A testable corollary of the model outlinedabove is that this high propensity is not merely fortuitous but
is genetically determined by the predisposing RBI mutation.This notion of a pathogenetic causality in the clinical association between these two rare tumor types was tested by determining the constitutional and osteosarcoma genotypes at RFLPloci on chromosome 13. The data indicated that osteosarcomasarising in retinoblastoma patients had become specificallyhomozygous around the chromosomal region carrying the RlìIlocus (80). Furthermore, these same chromosomal mechanismseliciting losses of constitutional heterozygosity were observedin sporadic osteosarcomas suggesting a genetic similarity in
5524
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
pathogenetic causality. These findings are of obvious relevanceto the interpretation of human mixed cancer families inasmuchas they suggest differential expression of a single pleiotropicmutation in the etiology of clinically associated cancer of different histológica! types.
This model of chromosomal mechanisms unmasking recessive predisposing mutations has been tested in a variety oftumor types and in each case has been confirmed. The loci forthe associated neoplasms hepatoblastoma, rhabdomyosarcoma,and Wilms' tumor have been mapped to chromosome 11 (81-86) as have those for adrenocortical carcinomas3 and transi
tional cell bladder carcinoma (87). The loci for small cell lungcarcinoma (88) and renal cell carcinoma" have been mapped tochromosome 3p. The low differentiation form of premenopau-sal ductal breast carcinoma appears to arise by similar mechanisms on chromosome 13 (89) whereas meningioma and acoustic neuroma involve chromosome 22 (90, 91).
The importance of these mutations in the process of humantumorigenesis is underscored by three points. First, the examination of any given tumor type with the approaches describedabove indicates that the majority of cases of each have undergone similar chromosomal rearrangements. Secondly, severalgroupings of clinically associated tumors have been found toarise through similar shared mechanisms; these have not beenobserved in nonassociated cancers. Finally, the specificity ofthese chromosomal events is notable, particularly in light of theplethora of chromosomal rearrangements accompanying theneoplastic process (66, 67). Published data obtained from reti-noblastoma (78, 79, 92), osteosarcoma (80, 93), Wilms' tumor
(81-84), hepatoblastoma (85), and acoustic neuroma (90, 91)indicated no nonspecific loss of constitutional heterozygosity.In fact, in unpublished studies from this laboratory, over 300cases of 27 different types of predominantly pediatrie or adolescent tumors have been genotyped at some 45 loci and in only3 instances has apparently random loss of heterozygosity beenobserved. However, it has been reported (94) that such randomlosses do occur in cell lines derived from metastatic adultmelanoma, and some limited nonoverlapping sets of chromosomes do appear to be lost in breast carcinoma (89) andmeningioma (90). The significance of these latter findings is atpresent unclear; in fact other studies of primary uveal melanomas have not shown random chromosomal losses (95).
Molecular Biology: Nature of the Gene Products of These Loci
Several points regarding recessive genes predisposing to tumorigenesis must be considered in any strategy concerned withthe elucidation of their structure and function. First, what isthe biological role of these genes? One possibility is that theproducts of these loci act as suppressors of other transforminggenes (60). This idea would predict a requirement for thecontinuous presence of the gene product to maintain suchsuppression and that the chromosomal events described abovewould suffice to alter or eliminate the suppressing function. Itmight also be reasonable to postulate that the activity of suchsuppressors would be required in any tissue which can betransformed by deregulation of their targets.
Several groups have examined the possibility that the reti-noblastoma gene product is responsible for controlling theexpression of N-/M>-C,a cellular gene that was originally found
to be amplified in human neuroblastomas (96). The mousehomologue has been shown to be under stage-specific regulation
3 Unpublished observations.4 C. Talmadge, personal communication.
during normal murine development and embryogenesis (97).One report suggested that N-myc was deregulated and amplifiedin retinoblastomas as compared to normal fetal or adult retina(98), data which would be consistent with the product of theRBI locus suppressing N-myc expression in normal tissue.However, subsequent analyses (99) indicated that the N-mycgene is normally expressed at high levels in fetal retina to acertain stage and not in adult retina; in retinoblastoma tumors,the level of N-myc expression is comparable to early fetal retina.Furthermore, Squire et al. (99) and we have been unable toconsistently detect N-mye expression in osteosarcomas, a resultwhich is at odds with a suppressing role of the RBI locus. Themost reasonable interpretation of these results is that expression of N-myc in retinoblastomas is merely a reflection of theembryonal nature of these tumors. It is, of course, possible thatthe retinoblastoma gene product functions as a suppressor genebut that its target gene(s) has yet to be identified.
An alternative hypothesis is that the recessive oncogene product plays a direct role in organismal development as a differentiation, cell recognition, or growth arrest factor the absenceof which causes the omission of some signal in the normaldevelopmental program resulting in the continuation of growthin an abnormal fashion. Recently, the isolations of two geneswhich fulfill many of the theoretical criteria for a recessiveoncogene have been reported (100-102). The first of these isthe l(2)gl gene of Drosophila melanogaster. Flies carryinghomozygous recessive mutations of this locus appear to arrestdevelopmentally; they do not pupate but continue larval growth(100). Additionally, in the resultant giant larvae there is autonomous proliferation of neuroectodermal neuroblasts that giverise to transplantable tumor-like growths resembling neuroblastomas. It has been convincingly shown that the excessive larvalgrowth and the neuroblastoma-like tumors are the direct resultof the absence of the l(2)gl gene product because reintroductionof a single copy of l(2)gl by P-element transformation intodefective flies results in both normal development and suppression of the tumor formation (100). The molecular function ofthis gene remains unknown but is an area of intense investigation.
Recently, two groups (101, 102) have reported the isolationof a gene from human chromosome 13ql4 that is expressed asa 4.7-kilobase mRNA. The genomic locus was shown to bealtered from the germline configuration in 4 of 45 retinoblastoma tumors and cell lines as judged by aberrancies uponSouthern analysis. Furthermore, many retinoblastoma and osteosarcoma cell lines express either no mRNA or altered sizetranscripts. These results are, of course, consistent with thegenetic predictions of homozygous loss of function in tumors.Furthermore, this gene appears to be expressed in all normaltissues and all other tumor types examined and at levels suggesting constitutive, perhaps housekeeping, function. DNA sequence analysis reveals little homology with any other knowngene and structural features that are undistinguished. Certainly,the determination of the biological function of this gene is likelyto shed a great deal of light on the molecular mechanism ofhuman carcinogenesis.
Significance
The discovery of genes with heritable recessive alÃelesthatpredispose to cancer has immediate medical relevance. Mostnotable is increased precision in the accuracy of pa-morbidprediction of tumor development in cases of familial retinoblastoma (103). Such predictions of predisposition to disease
5525
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
depend on the ability to detect the chromosomal origin of thepredisposing mutation (79). Identification of the chromosomecarrying the mutation in these linkage-based approaches isindependent of the determination of the primary defect anddepends instead upon flanking RFLP loci which are in informative allelic combinations in the parents and either the parentaltumor or the first affected child (103). Routine prenatal orpremorbid screening of children at risk for retinoblastoma asan adjunct to the earlier application of powerful therapeuticapproaches (104) should dramatically reduce morbidity andmortality in these cases. Furthermore, these methodologiesshould serve as the conceptual basis for their application toother, more common, cancers.
At a more fundamental level, the discovery of loci withrecessive alÃelesthat predispose to cancer may provide aninterface between tumor biology and developmental biology.The normal biological role of these genes and their role inorganismal development remains to be uncovered. It is conceivable that the developmental stage at which an embryonal tumorinitiates may be due to the loss of function of these genesthereby determining the histogenetic basis for tumor structureand behavior. Whether the groups of clinically and pathogenet-ically associated tumors described by these molecular geneticanalyses arise through the inactivation of single loci or throughmultilocus aberration requires the physical and genetic mappingof these heretofore unsuspected genomic regions. In either case,the data which are being rapidly generated promise to providefundamental information of relevance to a wide range of biological and medical specialties. Methodologies which must bedeveloped to analyze the function of these loci and their mutantalÃelespromise to be inventive, novel, and applicable to otherproblems in cancer and developmental biology. Manipulationsof these genes in vivo and in vitro should provide data withwhich to interpret their role in the initiation of human tumors,may allow for the experimental induction (and perhaps reversion) of tumors, and may ultimately allow the distinction between initiating and progressional events (105) in the complexpathway whereby a normal cell becomes malignant.
References
1. Broca. P. P. Traite des Tumeurs. Paris: Asselin, 1866.2. Haaland, M. Spontaneous tumors in mice. Sci. Rep. Invest. Imp. Cancer
Res. Fund, 4: 1-113, 1911.3. Levin. I. The influence of heredity on cancer, a study in eugenics. Z.
Krebsforsch.. //: 547-558, 1912.4. Warthin, A. S. Heredity with reference to carcinoma. Arch. Intern. Med.,
72:546-555, 1913.5. Heinzelman, F. Ãœbereine Krebsfamilie. Ein beitrag zur Frage der Hereditat
des Colonkanzinoms. Helv. Chir. Acta, 31: 316-332, 1964.6. Lynch, H. T. Familial cancer prevalence spanning eight years. Family N.
Arch. Intern. Med., 134:931-938, 1974.7. Lynch, H. T., and Krush, A. J. Heredity and adenocarcinoma of the colon.
Gastroenterology, S3: 517-527, 1967.8. Lynch, H. T., Harris, R. E., Lynch, P. M., Guirgis, H. A., Lynch, J. F., and
Bardawil. W. A. Role of heredity in multiple primary cancer. Cancer(Phila.), 40: 1849-1854. 1977.
9. Li, F. P. Second malignant tumors after cancer in childhood. Cancer(Phila.), 40: 1899-1902, 1977.
10. Warren, S., and Gates, O. Multiple primary malignant tumors. A survey ofthe literature and a statistical study. Am. J. Cancer, 16: 1358-1414. 1983.
11. Moertel, C. G. Multiple primary malignant neoplasms: historical perspectives. Cancer (Phila.), 40: 1786-1792, 1977.
12. Schell, R. F., Dockery, M. B., and Comfort, M. W. Carcinoma of thestomach associated with pernicious anemia. Surg. Gynecol. Obstet., 98:710-720, 1954.
13. Moertel, C. G., Barger, J. A., and Dockety, M. B. Multiple carcinomas ofthe large intestine. A review of the literature and a study of 261 cases.Gastroenterology, 34:85-98, 1958.
14. Dunn, J. E., Bragg, K. V., Sauter, C., and Gardispee, C. Breast cancer riskfollowing a major salivary gland carcinoma. Cancer (Phila.), 29: 1343-1346.
15. Li, F. P., and Fraumeni, J. F. Soft-tissue sarcomas, breast cancers and otherneoplasms. A familial syndrome. Ann. Intern. Med., 71: 747-751. 1969.
16. Lynch, H. T., Krush, A. J.. Mulcahy, G. M., and Reed, W. B. Familialoccurrences of a variety of premalignant disease and uncommon malignantneoplasms. Cancer (Phila.), 38:1474-1479, 1979.
17. Mike, V., Meadows, A. T., and D'Angio, G. J. Incidence of second malig
nant neoplasms in children: results of an international study. Lancet. 2:1326-1331,1982.
18. Kiii-liin. F. D., and Ellsworth, R. M. Pleiotropic effects of the gene forretinoblastoma. J. Med. Genet., //: 244-246, 1974.
19. Abramson, D. H., Ellsworth, R. M.. Kitchin, F. D., and Tung, G. Secondnonocular tumors in retinoblastoma survivors. Are they radiation-induced?Ophthalmology, 91: 1351-1355, 1984.
20. Sipple, J. H. The association of pheochromocytoma with carcinoma of thethyroid gland. Am. J. Med.. 31: 163-166. 1961.
21. Ballard. H. S., Frame, B., and Hartsock, R. J. Familial multiple endocrineadenoma-peptic ulcer complex. Medicine (Baltimore), -I<:481-485. 1964.
22. Schimke, R. N. Genetic aspects of multiple endocrine neoplasia. Annu. Rev.Med., 55:25-31, 1984.
23. Sparkes, R. S., Murphree. A. L., Lingua, R. W.. Sparkes, M. C., Field, L.L., Funderburk, S. J., and Benedict, W. F. Gene for hereditär)'retinoblastoma assigned to human chromosome 13 by linkage to esterase D. Science(Wash. DC), 219: 971-973. 1983.
24. Strong, L. C., Riccardi, V. M.. Ferrell, R. E.. and Sparkes, R. S. Familialretinoblastoma and chromosome 13 deletion transmitted via an insertionaltranslocation. Science (Wash. DC), 213: 1501-1503. 1981.
25. Knudson, A. G., and Strong, L. C. Heredity and cancer in man. Prog. Med.Genet., 9: 113-158, 1973.
26. Gordon, H. Family studies in retinoblastoma. Birth Defects, 10: 185-190,1974.
27. Boveri, T. The Origin of Malignant Tumors. Baltimore: Williams & Wil-kins, 1929.
28. Tyzzer, E. E. Tumor Immunity. J. Cancer Res., /: 125-155, 1916.29. Nordling, C. O. A new theory on the cancer-inducing mechanism. Br. J.
Cancer, 7:68-72. 1953.30. Bauer, K. H. Das Krebsproblem. Berlin: Springer-Verlag. 1949.31. Fisher, J. C., and Holloman, J. H. A hypothesis for the origin of cancer.
Cancer (Phila.), 4:916-918, 1951.32. Armitage, P., and Doll, R. The age distribution of cancer and a multistage
theory of cancer. Br. J. Cancer, S: I-12, 1954.33. Muller. H. J. Radiation damage of genetic origin. J. Hered., 39: 357-358,
1948.34. Stocks, P. Cancer of the stomach in the large towns of England and Wales.
1921-39. Br. J. Cancer, 4: 147-157, 1950.35. Stocks, P. Studies of cancer death rates at different ages in England and
Wales in 1921 to 1950. Uterus, breast and lung. Br. J. Cancer, 7: 283-302,1953.
36. Stocks, P. A study of the age curve for cancer of the stomach in connectionwith a theory of the cancer producing mechanism. Br. J. Cancer, 7: 407-417, 1953.
37. Platt, R. Clonal ageing and cancer. Lancet, /: 867, 1955.38. Armitage, R., and Doll, R. A two-stage theory of carcinogenesis in relation
to the age distribution of human cancer. Br. J. Cancer, //: 161-172, 1957.39. Harnden, D. G. In: R. L. Carter (ed.), Precancerous States, pp. 51-53.
Oxford, England: Oxford University Press, 1984.40. Stewart, A. An etiology of childhood malignancies: congenital!) determined
leukaemias. Br. Med. J., /: 452-460, 1961.41. Rous, P., and Kidd, J. G. Conditional neoplasms and subthreshold neoplas-
tic states. A study of tar tumors of rabbits. J. Exp. Med., 73: 365-395,1941.
42. Burch, P. R. J. A biological principle and its converse. Some implicationsfor carcinogenesis. Nature (Lond.), 195: 241-243, 1962.
43. Moolgavkar, S. H., and Knudson, A. G. Mutation and cancer: a model forhuman carcinogenesis. J. Nati. Cancer Inst.. 66: 1037-1052, 1981.
44. Knudson. A. G. Mutation and cancer: statistical study of retinoblastoma.Proc. Nati. Acad. Sci. USA, 68:820-823. 1971.
45. Knudson, A. G., and Strong, L. C. Mutation and cancer: a model for Wilms'tumor of the kidney. J. Nati. Cancer Inst., 48: 313-333, 1972.
46. Knudson, A. G.. and Strong, L. C. Mutation and cancer: neuroblastomaand pheochromocytoma. Am. J. Hum. Genet., 24: 514-524, 1972.
47. Knudson, A. G. Hereditary' cancer, oncogenes. and antioncogenes. CancerRes., 45: 1437-1443, 1985.
48. Moolgavkar, S. H., Day, N. E., and Stevens, R. G. Two-stage model forcarcinogenesis: epidemiology of breast cancer in females. J. Nati. CancerInst., 65: 559-569, 1980.
49. Jackson, C. E., Block, M. A., Greenawald, K. A., and Tashjian, A. H. Thetwo-mutational-event theory in medullary' thyroid cancer. Am. J. Hum.Genet., 31: 704-710, 1979.
50. Harris, H., Miller, O. J., Klein, G., Worst, P., and Tachibana, T. Suppression of malignancy by cell fusion. Nature (Lond.), 223: 363-368, 1969.
51. Klein, G., Bregula, U., Wiener, F.. and Harris, H. The analysis of malignancy by cell fusion. I. Hybrids between tumour cells and L cell derivatives.J. Cell. Sci., «.-659-672, 1971.
52. Harris, H., Wiener, F., and Klein, G. The analysis of malignancy by cellfusion. 3. Hybrids between diploid fibroblast and other tumor cells. J. CellSci.. «.-681-692, 1971.
53. Wiener, F., Fenyo, E. M., Klein, G., and Harris. H. Fusion of tumour cellswith host cells. Nat. New Biol., 238: 155-159. 1972.
5526
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

CANCER GENETICS
54. Wiener, F., Klein, G., and Harris, H. The analysis of malignancy by cellfusion. VI. Hybrids between different tumour cells. J. Cell Sci., 16: 189-198, 1974.
55. Harris, H. The genetic analysis of malignancy. J. Cell. Sci. Suppl., 4: 431-444, 1986.
56. Stanbridge, E. J. Suppression of malignancy in human cells. Nature (Lond.),260: 17-20, 1976.
57. Stanbridge, E. J., Flandermeyer, R. R., Daniels, D. W., and Nelson-Rees,W. A. Specific chromosome loss associated with the expression of tumori-genicity in human cell hybrids. Somat. Cell. Genet., 7:699-712, 1981.
58. Stanbridge, E. J., Der, C. J., Doersen, C.-J., Nishimi, R. Y., Peehl, D. M.,Weissman, B. E., and Wilkinson, J. Human cell hybrids: analysis of transformation and tumorigenicity. Science (Wash. DC), 215: 252-259, 1982.
59. Sager. R. Genetic suppression of tumor formation: a new frontier in cancerresearch. Cancer Res.. 46: 1573-1580, 1986.
60. Comings, D. E. A general theory of carcinogenesis. Proc. Nati. Acad. Sci.USA, 70:3324-3328, 1973.
61. Stiles, C. D., Desmond, W., Sato, G., and Saier, M. H. Failure of humancells transformed by simian virus 40 to form tumors in athymic nude mice.Proc. Nati. Acad. Sci. USA, 72:4971-4975, 1975.
62. Duesberg, P. H. Activated proto-onc genes: sufficient or necessary forcancer? Science (Wash. DC). 228: 669-677, 1985.
63. Srivatsan, E. S., Benedict, W. F.. and Stanbridge, E. J. Implication ofchromosome 11 in the suppression of neoplastic expression in human cellhybrids. Cancer Res., 46:6174-6179. 1986.
64. Saxon. P. J., Srivatsan, E. S., Leipzig, G. V., Sameshima, J. H., andStanbridge, E. J. Selective transfer of individual human chromosomes torecipient cells. Mol. Cell. Biol.. S: 140-146, 1985.
65. Yunis, J. J. The chromosomal basis of human neoplasia. Science (Wash.DC), 221: 227-236, 1983.
66. Sandberg, A. A. The Chromosomes in Human Cancer and Leukemia.Amsterdam: Elsevier/North-Holland Biomedicai Press, 1980.
67. Mitelman. F. Catalogue of Chromosomal Aberrations in Cancer: New York:Alan R. Liss, 1985.
68. Lele. K. P.. Penrose. L. S., and Stallard, H. B. Chromosome deletion in acase of retinoblastoma. Ann. Hum. Genet., 27:171-174, 1963.
69. Orye, E., Delbeke, M. J.. and Vandenabeele. B. Retinoblastoma and longarm deletion at chromosome 13: attempts to define the deleted segment.Clin. Genet.. 5: 457-464, 1974.
70. Francke, U. Retinoblastoma and chromosome 13. Cytogenet. Cell Genet.,16: 131-134. 1976.
71. Balaban-Malenbaum, G., Gilbert, F., Nichols, W. W., Hill. R., Shield, J.,and Meadows, A. J. A deleted chromosome no. 13 in human retinoblastomacells: relevance to tumorigenesis. Cytogenet. Cell Genet., 3: 243-250, 1981.
72. Balaban. G.. Gilbert. F., Nichols, W., Meadows, A. T., and Shield, J.Abnormalities of chromosome'13 in retinoblastoma from individuals withnormal constitutional karyotypes. Cancer Genet. Cytogenet., 6: 213-221,1982.
73. Benedict, W. F.. Banerjee, A., Mark, C., and Murphree, A. L. Non randomchromosomal changes in unilateral retinoblastoma. Cancer Genet. Cytogenet., 10: 311-333, 1983.
74. Squire. J.. Gallic. B. L., and Phillips, R. A. A detailed analysis of chromosomal changes in heritable and nonheritable retinoblastoma. Hum. Genet.,70:291-301, 1985.
75. Sparkes, R. S., Sparkes, M. C.. Wilson, M. G., Towner, J. W.. Benedict.W. F., Murphree, A. L., and Yunis, J. J. Regional assignment of genes forhuman esterase D and retinoblastoma to chromosome band 13q 14. Science(Wash. DC), 208: 1042-1044, 1980.
76. Benedict, W. F., Murphree, A. L.. Banerjee, A., Spina, C. A., Sparkes, M.C., and Sparkes, R. S. Patient with chromosome 13 deletion: evidence thatthe retinoblastoma gene is a recessive cancer gene. Science (Wash. DC).2/9:973-975,1983.
77. Godbout, R., Dryja, T. P., Squire. J., Gallie, B. L., and Phillips, R. A.Somatic inactivation of genes on chromosome 13 is a common event inretinoblastoma. Nature (Lond.), 304:451-453. 1983.
78. Cavenee, W. K., Dryja, T. P., Phillips, R. A., Benedict, W. F., Godbout,R.. Gallie, B. L., Murphree, A. L., Strong, L. C., and White, R. Expressionof recessive alÃelesby chromosomal mechanisms in retinoblastoma. Nature(Lond.), 305:779-784, 1983.
79. Cavenee, W. K., Hansen, M. F., Kock, E., Nordenskjold, M., Maumenee,I., Squire, S. A., Phillips, R. A., and Gallie, B. L. Genetic origins ofmutations predisposing to retinoblastoma. Science (Wash. DC), 228: 501-503, 1985.
80. Hansen, M. F., Koufos, A.. Gallie, B. L., Phillips, R. A., Fodstad, O.,Brogger, A., Gedde-Dahl, T., and Cavenee, W. K. Osteosarcoma andretinoblastoma: a shared chromosomal mechanism revealing recessive predisposition. Proc. Nati. Acad. Sci. USA, 82: 6216-6220, 1985.
81. Koufos, A., Hansen, M. F., Lampkin, B. C., Workman, M. L., Copeland,
N. G., Jenkins, N. A., and Cavenee, W. K. Loss of alÃelesat loci on humanchromosome 11 during genesis of Wilms' tumor. Nature (Lond.), 309:170-
172, 1984.82. Orkin, S. H., Goldman, D. S., and Sallan, S. E. Development of homozy-
gosity for chromosome lip markers in Wilms' tumour. Nature (Lond.),309: 172-174, 1984.
83. Reeve. A. E., Housiaux, P. J., Gardner. R. J. M., Chewings, W. E.. Grindley,R. M.. and Millow, L. J. Loss of a Harvey ras alÃelein sporadic Wilms'tumour. Nature (Lond.), 309:174-176, 1984.
84. Fearon, E. R., Vogelstein, B., and Feinberg, A. P. Somatic deletion andduplication of genes on chromosome 11 in Wilms' tumour. Nature (Lond.),309: 176-178, 1984.
85. Koufos, A., Hansen, M. F., Copeland, N. G., Jenkins, N. A., Lampkin, B.C., and Cavenee, W. K. Loss of heterozygosity in three embryonal tumourssuggests a common pathogenetic mechanism. Nature (Lond.), 316: 330-334, 1985.
86. Scrable, H., Witte, D., Wang-Wuu, F., Koufos, A., and Cavenee, W. K.Molecular definition of rhabdomyosarcoma subtypes. Am. J. Hum. Genet.,J9.-A41, 1986.
87. Fearon, E. R.. Feinberg, A. P., Hamilton, S. H., and Vogelstein, B. Loss ofgenes on the short arm of chromosome 11 in bladder cancer. Nature (Lond.),318: 377-380, 1985.
88. Naylor, S. L., Minna, J.. Johnson. B., and Sakaguchi, A. Y. DNA polymorphisms confirm the deletion in the short arm of chromosome 3 in smallcell lung cancer. Am. J. Hum. Genet., 36: 355, 1984.
89. Lundberg, C.. Skoog, L., Cavenee, W. K., and Nordenskjold, M. Loss ofheterozygosity in human ductal breast tumors indicates a recessive mutationon chromosome 13. Proc. Nati. Acad. Sci. USA, 84: 2372-2376, 1987.
90. Seizinger. B. R., Martuza, R. L., and Gusella, J. F. Loss of genes onchromosome 22 in tumourigenesis of human acoustic neuroma. Nature(Lond.), 322:644-647, 1986.
91. Seizinger, B. R., Rouleau, G., Ozelius, L. J., Lane, A. H.. St. George-Hyslop, P., Huson, S., Gusella, J. F., and Moartuza, R. L. Commonpathogenetic mechanism for three tumor types in bilateral acoustic neuro-fibromatosis. Science (Wash. DC), 236: 317-319, 1987.
92. Dryja, T. P., Cavenee, W. K., White, R.. Rapaport, J. M.. Petersen, R.,Albert, D. M., and Bruns, G. A. P. Homozygosity of chromosome 13 inretinoblastoma. N. Engl. J. Med., 310: 550-553, 1984.
93. Dryja, T. P., Rapaport, J. M., Epstein, J., Goorin, A. M., Weichselbaum,R., Koufos, A., and Cavenee, W. K. Chromosome 13 homozygosity inosteosarcoma without retinoblastoma. Am. J. Hum. Genet., 38: 59-66,1986.
94. Dracopoli, N. C.. Houghton, A. N., and Old, L. J. Loss of polymorphicrestriction fragments in malignant tumours. Implications for tumor heterogeneity. Proc. Nati. Acad. Sci. USA. 82: 1470-1474, 1985.
95. Mukai, S., and Dryja. T. P. Loss of alÃelesat polymorphic loci on chromosome 2 in uveal melanoma. Cancer Genet. Cytogenet., 82:45-53, 1986.
96. Schwab, M., Varmus, H. E., Bishop, J. M., Grzeschik, K. H., Naylor, S.L., Sakaguchi, A. Y., Brodeur, G., and Trent, J. Chromosome localizationin normal human cells and neuroblastomas of a gene related to i--ni.iv.Nature (Lond.), 309: 228-291, 1984.
97. Jakobovitz, A., Schwab, M., Bishop, J. M.. and Martin, G. R. Differentialexpression of myc family genes during murine development. Nature (Lond.),318: 188-191, 1985.
98. Lee, W.-H., Murphree, A. L., and Benedict, W. F. Expression and amplification of the \ um gene in primary retinoblastoma. Nature (Lond.), 309:458-460, 1984.
99. Squire, J., Goddard, A. D., Canton, M., Becker. A., Phillips, R. A., andGallie, B. L. Tumour induction by the retinoblastoma mutation is independent of N-myc expression. Nature (Lond.), 322: 555-557, 1986.
100. Mechler, B. M., McGinnis, W., and Gehring, W. J. Molecular cloning oflethal (2) giant larvae, a recessive oncogene of Drosophila melanogasler.EMBO J., 4: 1551-1554, 1985.
101. Friend, S. H., Bernards, R., Rogel, S., Weinberg. R. A., Rapaport, J. M.,Albert, D. M., and Dryja, T. P. A human DNA segment with properties ofthe gene that predisposes to retinoblastoma and osteosarcoma. Nature(Lond.), 323:643-646, 1986.
102. Lee, W.-H., Bookstein, R., Hong, F., Young, L.-H., Shew, J.-Y.. and Lee,E. Y. H. P. Human retinoblastoma susceptibility gene: cloning, identification and sequence. Science (Wash. DC), 235: 1394-1399, 1987.
103. Cavenee, W. K., Murphree, A. L.. Shull, M. M., Benedict, W. F., Sparkes,R. S., Kock, E., and Nordenskjold, M. Prediction of familial predispositionto retinoblastoma. N. Engl. J. Med.. 314: 1201-1207. 1986.
104. Ellsworth, R. M. Treatment of retinoblastoma. In: Transactions of the NewOrleans Academy of Ophthalmology 1986. pp. 55-59. New Orleans: RavenPress. 1986.
105. Klein, G., and Klein, E. Evolution of tumours and the impact of molecularoncology. Nature (Lond.), 315: 190-195, 1985.
5527
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from

1987;47:5518-5527. Cancer Res Marc F. Hansen and Webster K. Cavenee Genetics of Cancer Predisposition
Updated version
http://cancerres.aacrjournals.org/content/47/21/5518.citation
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/47/21/5518.citationTo request permission to re-use all or part of this article, use this link
Research. on November 6, 2020. © 1987 American Association for Cancercancerres.aacrjournals.org Downloaded from