Embed Size (px)
Citation preview

Chapter
9Chapter
9Genetics Perspectives in Nursing
LEARNING OBJECTIVESOn completion of this chapter, the learner will be able to:
1. Describe the role of the nurse in integrating genetics in nursingcare.
2. Conduct a genetics-based assessment.3. Identify the common patterns of inheritance of genetic disorders.4. Identify ethical issues in nursing related to genetics.
123
●
●

Nurses must learn to recognize patterns of inheritance whenobtaining family and medical histories and understand when it isappropriate to consider new gene-based testing and treatment op-tions. This chapter offers a foundation for the clinical applica-tions of genetics principles in medical and surgical nursing,outlines the nurse’s role in genetic counseling and evaluation, ad-dresses important ethical issues, and provides genetics resourcesfor nurses and patients.
A Framework for Integrating Genetics Into Nursing PracticeNursing’s unique contribution to genomic medicine is its phi-losophy of holism. Nurses are ideally positioned to incorporategenetics into their assessments, planning, and interventions forpatients at different ages and stages across the lifespan and in allsettings. The holistic view that characterizes nursing takes intoaccount each person’s intellectual, physical, spiritual, social, cul-tural, biopsychologic, ethical, and esthetic experiences while ad-
124 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Human genome discoveries have ushered in a new era ofmedicine, genomic medicine, which recognizes that multiple geneswork in concert with environmental influences to cause disease.Genomic medicine aims to improve predictions about individuals’susceptibility to diseases, the time of onset for those diseases, theirextent and eventual severity, and which treatments or medicationsare likely to be most effective or harmful (Billings, 2000). Already,new gene-based strategies for disease detection, management, andtreatment have been created, allowing health professionals to tailorcare to an individual’s particular genetic make-up.
To meet the challenges of genomic medicine, nurses need to un-derstand the new technologies and treatments of gene-based healthcare. Nurses also must recognize that they are a vital link betweenpatients and health care services; patients often turn to nurses firstwith questions about family history of risk factors, genetics infor-mation, and genetic tests and interpretations. Incorporating ge-netics into nursing means bringing a genetics framework to healthassessments, planning, and interventions that supports identifica-tion of and response to individuals’ changing genetics-relatedhealth needs (Lea, Williams, Jenkins, et al., 2000).
Glossaryallele: any one of two or more alternate
forms of a gene at the same location. Anallele for each gene is inherited from eachparent.
autosome: a single chromosome from any ofthe 22 pairs of chromosomes not involvedin sex determination (XX or XY)
carrier: person who is heterozygous; possess-ing two different alleles of a gene pair
chromosome: microscopic structures in thecell nucleus that contain genetic informa-tion and are constant in number in aspecies (eg, humans have 46 chromosomes)
deoxyribonucleic acid (DNA): the primarygenetic material in humans consisting ofnitrogenous bases, a sugar group, andphosphate combined into a double helix
diploid: the number of chromosomes nor-mally present in somatic cells. For humans,that number is 46.
dominant: a genetic trait that is normallyexpressed when a person has a gene muta-tion on one of a pair of chromosomes andthe “normal” form of the gene is on theother chromosome
genetics: the scientific study of heredity;how specific traits or predispositions aretransmitted from parents to offspring
genome: the total genetic complement of anindividual genotype
genomics: the study of the human genome,including gene sequencing, mapping, andfunction
genotype: the genes and the variationstherein that a person inherits from his orher parents
haploid: the number of chromosomes pre-sent in egg or sperm (gametes); in humans,this is 23
Human Genome Project: an internationalresearch effort aimed at identifying and
characterizing the order of every base inthe human genome
meiosis: the reduction division of diploidegg or sperm (germ cells) resulting inhaploid gametes (having 23 chromosomeseach)
mitosis: cell division occurring in somaticcells that normally results in daughter cellswith the same number of chromosomes—46 (diploid)
monosomy: missing one of a chromosomepair in normally diploid cells (for exam-ple, 45,X females have only one X chro-mosome)
mutation: a heritable alteration in the ge-netic material
nondisjunction: the failure of a chromo-some pair to separate appropriately duringmeiosis, resulting in abnormal chromo-some numbers in reproductive cells(gametes) or cells
nucleotide: a nucleic acid “building block”composed of a nitrogenous base, a five-carbon sugar, and a phosphate group
pedigree: a diagrammatic representation of afamily history
penetrance: the percentage of individualsknown to carry the gene for a trait whoactually manifest the condition. For ex-ample, a trait with 90% penetrance willnot be manifested by 10% of persons pos-sessing the gene.
phenotype: a person’s entire physical, bio-chemical, and physiological makeup, asdetermined by the individual’s genotypeand environmental factors
polymorphism: a genetic variation with twoor more alleles that is maintained in apopulation
population screening: the application of atest or inquiry to a group to determine if
individuals in the group have an increasedlikelihood of a genetic condition or a mu-tation in a specific gene (eg, cholesterolscreening for hypercholesterolemia)
predisposition testing: testing that is usedto determine the likelihood that a healthyperson with or without a family history ofa condition will develop the disorder.Having the gene mutation would indicatethat the person has an increased suscepti-bility to the disorder, but this is not adiagnosis. One example is DNA mutationtesting for hereditary breast/ovariancancer.
prenatal screening: testing that is used toidentify if a fetus is at risk for a birth de-fect such as Down syndrome or spina bi-fida (eg, multiple marker maternal serumscreening in pregnancy)
presymptomatic testing: genetic testingthat is used to determine whether personswith a family history of a disorder, but no current symptoms, have the genemutation. An example of this would beHuntington disease.
recessive: a genetic trait that is expressedonly when a person has two copies of amutant autosomal gene or a single copy ofa mutant X-linked gene in the absence ofanother X chromosome
transcription: the process of transforminginformation from DNA into new strandsof messenger RNA
trisomy: the presence of one extra chromo-some in an otherwise diploid chromosomecomplement—for example, trisomy 21 (Down syndrome)
variable expression: variation in the degreeto which a trait is manifested; clinicalseverity
X-linked: located on the X chromosome

dressing genetics information, gene-based testing, diagnosis, andtreatments. Thus, knowledge about genetics is basic to nursingpractice (Lea, Anderson & Monsen, 1998).
A framework for integrating genetics into nursing practice in-cludes a philosophy of care that recognizes when genetics factorsare playing a role or could play a role in an individual’s health.This means using family history and the results of genetics testseffectively, informing patients about genetics concepts, under-standing the personal and societal impact of genetics informa-tion, and valuing the privacy and confidentiality of geneticsinformation.
A person’s response to genetics information, genetic testing, orconditions may be either disabling or empowering. Genetics in-formation may stigmatize individuals if it affects how they viewthemselves or how others view them. Nurses can help individu-als and families understand the genetic aspect of themselves andlearn how genetic traits and conditions are passed on within fam-ilies and how genetic and environmental factors influence healthand disease (Lea, Anderson & Monsen, 1998; Peters et al., 1999).
Nurses facilitate communication among family members, thehealth care system, and community resources; they offer valuablesupport by virtue of their continuity of care with patients andfamilies. All nurses should be able to recognize when a client isasking a question related to genetics information and shouldknow how to obtain genetics information by gathering familyand health histories and conducting physical and developmental
assessments. Being able to recognize a genetics concern allows thenurse to provide appropriate genetics resources and support toindividuals and families (Lea, Jenkins & Francomano, 1998).
Key to nurses’ genetics framework is the awareness of one’s at-titudes, experience, and assumptions about genetics concepts andhow these are manifested in one’s own practice. Chart 9-1 offersinsights on how nurses can conduct periodic self-assessments.
Genetics ConceptsScientists and philosophers have long speculated about heredityand developed theories to explain how traits are transmitted tooffspring. Developments in technology and research have accel-erated progress in our understanding of genetics, allowingscientists to better understand relatively rare diseases such asphenylketonuria (PKU) or hemophilia that are related to muta-tions of a single gene inherited in families. New technologies andtools allow scientists to characterize inherited metabolic varia-tions that interact over time and lead to common diseases such ascancer, heart disease, and dementia. This transition from geneticsto genomics highlights how our understanding of single genesand their individual functions has evolved to understanding howmultiple genes act and control biologic processes. Most healthconditions are now believed to be the result of a combination ofgenetic and environmental influences and interactions (Billings,2000).
Chapter 9 Genetics Perspectives in Nursing 125
Examining Our Own Attitudes, Experiences, and Assumptions
Self-knowledge is one of the cornerstones to providing quality nursingcare, and as practitioners, our attitudes and experiences have an im-pact on clinical practice. These attitudes emerge from social, cultural,and religious experiences in one’s personal life. Awareness of our ownvalues, beliefs, and cultural perceptions not only is important to thenurse–patient relationship, but it is also the first step in developing agenetics framework.
Periodic self-assessment can help maintain an effective frameworkas nurses update genetics knowledge and practice. Nurses can developan awareness of their own attitudes, experiences, and assumptionsabout genetics concepts by considering the following:
• One’s family’s beliefs or values about health. What are yourfamily, religious, or cultural beliefs about the cause of illness?How have your values or biases influenced your understandingof genetic conditions?
• One’s philosophical, theologic, cultural, and ethical perspectivesrelated to health. How would these attitudes influence your ownuse of genetics information or services? What experiences haveyou had with people from different social, cultural, religious,or ethnic groups? How would you deliver genetics informationto individuals from different social, cultural, or ethnic groups?Can you recognize when personal values or biases may affect orinterfere with the delivery of genetics information?
• One’s level of genetics expertise. Can you recognize the limita-tions of your own genetics experience and know when to referpatients for further genetics work-up?
• One’s experience with birth defects, chronic illnesses, and geneticconditions. Do you have a family member or friend who has agenetic condition or disorder? Has your experience been that
Chart9-1
Chart9-1
genetic disorders are disabling or empowering? Do you view aparent “at fault” for having a baby born with a birth defect orgenetic condition? Do you advocate for fair access and otherrights for individuals who have birth defects, genetic conditions,or other disabilities?
• One’s view of DNA (the most basic concept of who we are, since ourgenetic makeup is unlike that of any other person except an identicaltwin). What are your assumptions about DNA? For example, doyou assume that the genetic component of “the self ” is a defectiveself? As another example, healthy carriers of genetic alterationsthat predispose them to develop certain diseases in the future nowbelong to a new class of “at risk” individuals. A person who is“at risk” is not ill at present, but may not remain well as long asthe “average” person. Is it good to know that you are “at risk”or is this information that should not be identified or revealedbecause of the risk of potential discrimination?
• One’s beliefs about reproductive options. What are your beliefsregarding reproductive options such as prenatal diagnosis andpregnancy termination? How might these influence your careof a patient who holds different beliefs?
• One’s view of genetic testing and engineering. Do you see genetictesting and engineering—the ability to eliminate or enhancecertain traits—as a way to create an “ideal genetic self ”?
• One’s approach to patients with disabilities. How are your atti-tudes made apparent in your practice and practice settings? For example, do you have access to TTY machines and/orinterpreters for those who have hearing impairment? Are yourintake procedures adapted to meet the needs of an individualwith disabilities?
Sources: National Coalition of Health Professional Education in Genetics (2001). Core competencies; http://www.nchpeg.org;Kenan, R. (1996). The at-risk health status and technology: A diagnostic invitation and the gift of knowing. Social Scienceand Medicine, 42(11), 1545–1553; Peters, J. A., Djurdjinovic, L. & Baker, D. (1999). The genetic self: The Human GenomeProject, genetic counseling and family therapy. Families, Systems & Health, 17(1), 5–25.

GENES AND THEIR ROLE IN HUMAN VARIATIONGenes are central components of human health and disease.Work on the Human Genome Project (an international researcheffort to map and sequence the human genome in its entirety) hasshown how basic human genetics is to human development,health, and disease. Knowledge that specific genes are associatedwith specific genetic conditions makes diagnosis possible, even inthe unborn. Research continues to demonstrate how manycommon conditions have genetic causes. Many more associa-tions between genetics, health, and disease will likely be identi-fied as scientists complete and refine human genome mappingand sequencing.
Genes and ChromosomesA person’s unique genetic constitution, called a genotype, ismade up of some 30,000 to 40,000 genes. A person’s phenotype,the observable characteristics of his or her genotype, includesphysical appearance and other biologic, physiologic, and molec-ular traits. Environmental influences modify every individual’sphenotype, even those with a major genetic component.
Human growth, development, and disease occur as a result ofboth genetic and environmental influences and interactions. Thecontribution of genetic factors may be large or small. For exam-ple, in a person with cystic fibrosis or PKU, the genetic contribu-tion is significant. In contrast, the genetic contribution underlyinga person’s response to infection may be less so.
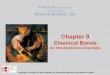
An individual gene is conceptualized as a unit of heredity. Agene is composed of a segment of deoxyribonucleic acid (DNA)that contains a specific set of instructions for making the proteinor proteins needed by body cells for proper functioning. Genesregulate both the types of proteins made and the rate at whichproteins are produced. The structure of the DNA molecule is re-ferred to as the double helix. The essential components of theDNA molecule are sugar-phosphate molecules and pairs of ni-trogenous bases. Each nucleotide contains a sugar (deoxyribose),a phosphate group, and one of four nitrogenous bases: adenine(A), cytosine (C), guanine (G), and thymine (T). DNA is com-posed of two-paired strands, each made up of a number of nu-cleotides. The strands are held together by hydrogen bondsbetween pairs of bases (Fig. 9-1).
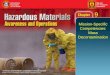
Genes are packaged and arranged in a linear order withinchromosomes, which are located in the cell nucleus. In humans,46 chromosomes occur in pairs in all body cells except oocytes(eggs) and sperm, which each contain only 23 chromosomes.Twenty-two pairs of chromosomes, called autosomes, are thesame in females and males. The 23rd pair is referred to as the sexchromosomes. A female has two X chromosomes, while a malehas one X and one Y chromosome. At conception, each parentnormally gives one chromosome of each pair to his or her chil-dren. As a result, children receive half of their chromosomes fromtheir fathers and half from their mothers (Fig. 9-2).
Careful examination of DNA sequences from many individ-uals shows that these sequences have multiple versions in a pop-ulation. These different versions, or sequence variations, arecalled alleles. Sequences found in many forms are said to be poly-morphic, meaning that there are at least two common forms of aparticular gene.
Cell DivisionThe human body grows and develops through a process of cell di-vision. Mitosis and meiosis, two distinctly different types of celldivision, contribute to these processes.
Mitosis is the process of cell division involved in cell growth,differentiation, and repair. During mitosis, the chromosomes ofeach cell duplicate. The result is two cells, called daughter cells,each containing the same number of chromosomes as the parentcell. The daughter cells are said to be diploid because they con-tain 46 chromosomes in 23 pairs. Mitosis occurs in all cells of thebody except oocytes (eggs) and sperm.
Meiosis, in contrast, occurs only in reproductive cells and isthe process by which oocytes and sperm are formed. Duringmeiosis a reduction in the number of chromosomes takes place,resulting in oocytes or sperm that contain half the usual numberor 23 chromosomes. Oocytes and sperm are referred to as hap-loid because they contain a single copy of each chromosome,compared to the usual two chromosomes in all other body cells.
126 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Cell
Nucleus
Chromosomes
Gene
Chemicalbases
DNAmolecule
FIGURE 9-1 DNA that carries the instructions that allow cells to makeproteins is made up of four chemical bases. Tightly coiled strands of DNAare packaged in units called chromosomes, housed in the cell’s nucleus.Working subunits of DNA are known as genes. From the National Institutesof Health and National Cancer Institute. (1995). Understanding gene testing(NIH Pub. No. 96-3905). Washington, DC: U.S. Department of HumanServices.

During the initial phase of meiosis, paired chromosomes cometogether in preparation for cell division, portions cross over, andan exchange of genetic material occurs. This event, called re-combination, creates greater diversity in the makeup of oocytesand sperm.
During meiosis, a pair of chromosomes may fail to separatecompletely, creating a sperm or oocyte that contains either twocopies or no copy of a particular chromosome. This sporadicevent, called nondisjunction, can lead to either a trisomy or a monosomy. Down syndrome is an example of trisomy. An
individual with Down syndrome has three number 21 chromo-somes. Turner syndrome is an example of monosomy. Girlswho have Turner syndrome usually have a single X chromo-some, causing them to have short stature and infertility (Lash-ley, 1998).
Gene MutationsWithin each cell, many intricate and complex interactions regu-late and express human genes. Gene structure and function, tran-scription and translation, and protein synthesis are all involved.Alterations in gene structure and function and the process of pro-tein synthesis may influence a person’s health. Changes in genestructure, called mutations, permanently change the sequence ofDNA, which in turn can alter the nature and type of proteinsmade (Fig. 9-3).
Some gene mutations have no significant effect on the pro-tein product made, while others cause partial or completechanges. How a protein is altered and its importance to properbody functioning determine the mutation’s impact. Gene mu-tations may occur in hormones or enzymes or important pro-tein products, thereby having significant implications for healthand disease.
Sickle cell anemia is an example of a genetic conditioncaused by a small gene mutation that affects protein structure,producing hemoglobin S. A person who inherits two copies ofthe hemoglobin S gene mutation has the condition sickle cellanemia and experiences the symptoms of severe anemia andthrombotic organ damage resulting from hypoxia (Lashley,1998; Lea, 2000).
Other gene mutations may be larger, such as a deletion (loss),insertion (addition), duplication (multiplication), or rearrange-ment (translocation) of a longer DNA segment. Duchenne mus-cular dystrophy, an inherited form of muscular dystrophy, is anexample of a genetic disorder caused by structural gene mutationssuch as deletions or duplications in the dystrophin gene. Anothertype of gene mutation, called a triplet or trinucleotide repeat,involves the expansion of more than the usual number of a triplet
Chapter 9 Genetics Perspectives in Nursing 127
1 2 3 4 5 6
7 8 9 10 11 12
13 14 15 16 17 18
19 20 21 22 X Y
FIGURE 9-2 Each human cell contains 23 pairs of chromosomes, whichcan be distinguished by size and by unique banding patterns. This set is froma male, since it contains a Y chromosome. Females have two X chromosomes.From the National Institutes of Health and National Cancer Institute.(1995). Understanding gene testing (NIH Pub. No. 96-3905). Washington,DC: U.S. Department of Human Services.
Nucleus
Gene
DNA
DNAbases
mRNA
Cell membrane
Chain ofamino acids
Alteredprotein
Ribosome
FIGURE 9-3 When a gene contains amutation, the protein encoded by thatgene will be abnormal. Some proteinchanges are insignificant, others are dis-abling. From the National Institutes ofHealth and National Cancer Institute.(1995). Understanding gene testing (NIHPub. No. 96-3905). Washington, DC:U.S. Department of Human Services.

repeat sequence within a gene. Myotonic dystrophy, Huntingtondisease, and fragile X syndrome are examples of conditions causedby this type of gene mutation.
Gene mutations may be inherited or acquired. Inherited orgerm-line gene mutations are present in the DNA of all body cellsand are passed on in reproductive cells from parent to child.Germ-line mutations are passed on to all daughter cells whenbody cells replicate (Fig. 9-4). The gene that causes Huntingtondisease is one example of a germ-line mutation.
Spontaneous gene mutations take place in individual oocytesor sperm at the time of conception. These mutations are not in-herited in other family members. A person who carries the new“spontaneous” mutation, however, may pass on the gene muta-tion to his or her children. Achondroplasia, Marfan syndrome,and neurofibromatosis type 1 are examples of genetic conditionsthat may occur in a single family member as a result of sponta-neous mutation.
Acquired mutations take place in somatic cells and involvechanges in DNA that occur after conception, during a person’slifetime. Acquired mutations develop as a result of cumulativechanges in body cells other than reproductive cells (Fig. 9-5). So-matic gene mutations are passed on to the daughter cells derivedfrom that particular cell line.
Gene mutations occur in the human body all the time. Cellshave built-in mechanisms by which they can recognize mutationsin DNA, and in most situations they correct the change before itis passed on by cell division. However, over time, body cells maylose their ability to repair damage from gene mutations, causingan accumulation of genetic changes that may ultimately result indiseases such as cancer and possibly other conditions of aging,such as Alzheimer’s disease (Lashley, 1998).
Genetic VariationSorting out the genetic components of complex conditions (eg,heart disease, diabetes, common cancers, psychiatric disorders)that result from the interaction of environment, lifestyle, and thesmall effects of many genes is ongoing. New studies of genetic
variation in humans are underway to develop a map of commonDNA variants. Genetic variations occur among individuals of allpopulations. Polymorphisms and single nucleotide polymor-phisms (SNPs, pronounced “snips”) are the terms used for com-mon genetic variations that occur most frequently throughoutthe human genome. Some SNPs may contribute directly to a traitor disease expression by altering function. SNPs are becoming in-creasingly important for the discovery of DNA sequence varia-tions that affect biologic function. Such knowledge will allowclinicians to subclassify diseases and adapt therapies to the indi-vidual patient (Collins, 1999; Collins & McKusick, 2001). Forexample, a polymorphism or SNP can alter a protein or enzymeactivity and can thus affect drug efficacy and safety when it oc-curs in proteins that are targets of medication regimens or thatare involved in drug transport or drug metabolism (McCarthy &Hilfiker, 2000; Schafer & Hawkins, 1998).
INHERITANCE PATTERNS IN FAMILIESNursing assessment of patients’ health includes obtaining andrecording family history information. Family history evaluationin the form of a pedigree is a first step in establishing the patternof inheritance. Nurses must become familiar with mendelian pat-terns of inheritance and pedigree construction and analysis to beable to help identify individuals and families who may benefitfrom further genetic counseling, testing and therapeutics (Lea,Jenkins & Francomano, 1998; Lea, 2000).
Mendelian conditions are genetic conditions that are inher-ited in families in fixed proportions among generations. Namedafter Gregor Mendel, mendelian conditions result from gene mu-tations present on one or both chromosomes of a pair. An indi-vidual gene inherited from one or both parents can cause amendelian inherited condition. Mendelian conditions are classi-fied according to their pattern of inheritance in families: auto-somal dominant, autosomal recessive, and X-linked. The termsdominant and recessive refer to the trait, genetic condition, orphenotype, but not to the genes or alleles that cause the observ-able characteristics (Thompson et al., 2001).
128 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Egg Sperm
Fertilized egg
Mutation
ReproductiveBone
PancreasBrain
Body cells of offspring
FIGURE 9-4 Hereditary mutations are carried in theDNA of the reproductive cells. When reproductive cellscontaining mutations combine to produce offspring,the mutation will be present in all of the offspring’sbody cells. From the National Institutes of Health andNational Cancer Institute. (1995). Understanding genetesting (NIH Pub. No. 96-3905). Washington, DC:U.S. Department of Human Services.

Autosomal Dominant InheritanceAutosomal dominant inherited conditions affect female andmale family members equally and follow a vertical pattern ofinheritance in families (Fig. 9-6). An individual who has an au-tosomal dominant inherited condition carries a gene mutationfor that condition on one chromosome of a pair. Each of thatindividual’s offspring has a 50% chance of inheriting the genemutation for the condition and a 50% chance of inheriting thenormal version of the gene. Offspring who do not inherit thegene mutation for the dominant condition will not develop thecondition and do not have an increased chance for having chil-
dren with the same condition (Fig. 9-7). Table 9-1 presentscharacteristics and examples of different patterns of inheritedconditions.
Autosomal dominant inherited conditions often present withvarying degrees of severity among affected family members andpersons. Some individuals with the condition may have signifi-cant symptoms, while others may have only mild ones. This char-acteristic is referred to as variable expression; it results from theinfluences of genetic and environmental factors on clinical pre-sentation.
Another phenomenon observed in autosomal dominant in-heritance is penetrance, the percentage of persons known tohave a particular gene mutation who actually show the trait.Penetrance is observed in conditions such as achondroplasia, inwhich nearly 100% of persons with the gene mutation typicallydisplay traits of the disease. In some conditions, the presence ofa gene mutation does not invariably mean that a person willhave or develop an autosomal inherited condition. For exam-ple, a woman who has the BRCA1 hereditary breast cancer genemutation has a lifetime risk for breast cancer up to 80%, not100%. This quality, known as incomplete penetrance, indicatesthe probability that a given gene will produce disease. In otherwords, a person may inherit the gene mutation that causes anautosomal dominant condition but may not have any of the ob-servable physical or developmental features of that condition.However, these individuals carry the gene mutation and stillhave a 50% chance of passing the gene for the condition to eachof their children. One of the effects of incomplete penetrance isthat the gene appears to “skip” a generation, thus leading to er-rors in interpreting family history and in genetic counseling.Examples of other genetic conditions with incomplete pene-
Chapter 9 Genetics Perspectives in Nursing 129
Normalbone cell
Mutationoccurs
Alteredgene
Alteredbonecells
Normal bonecells
FIGURE 9-5 Acquired mutations develop in DNA during a person’s life-time. If the mutation arises in a body cell, copies of the mutation will exist onlyin the descendants of that particular cell. From the National Institutes ofHealth and National Cancer Institute. (1995). Understanding gene testing (NIHPub. No. 96-3905). Washington, DC: U.S. Department of Human Services.
Affected maleAffected femaleUnaffected maleUnaffected female
I
II
III
FIGURE 9-6 Three-generation pedigree illustrating autosomal dominantinheritance.
Affectedfather
Normalmother
Affecteddaughter
Normalson
Affectedson
Normaldaughter
FIGURE 9-7 In dominant genetic disorders, if one affected parent has adisease-causing allele that dominates its normal counterpart, each child in thefamily has a 50% chance of inheriting the disease allele and the disorder.From the National Institutes of Health and National Cancer Institute.(1995). Understanding gene testing (NIH Pub. No. 96-3905). Washington,DC: U.S. Department of Human Services.

trance include otosclerosis (40%) and retinoblastoma (80%)(Lashley, 1998).
Autosomal Recessive InheritanceThe pattern of inheritance in autosomal recessive inherited con-ditions differs from that of autosomal dominant inherited condi-tions in that it is more horizontal than vertical, with relatives of asingle generation tending to have the condition (Fig. 9-8). Ge-netic conditions inherited in an autosomal recessive pattern arefrequently seen among particular ethnic groups and tend to occurmore often in children of parents who are related by blood, suchas first cousins (see Table 9-1).
In autosomal recessive inheritance, each parent carries a genemutation on one chromosome of the pair and the normal workingcopy of the gene on the other chromosome. The parents are saidto be carriers of the particular gene mutation. Unlike an individ-ual with an autosomal dominant inherited condition, a carrier ofa gene mutation for a recessive inherited condition does not havesymptoms of the genetic condition. When two carrier parents havechildren together, they have (with each of their pregnancies) a 25%chance of having a child who inherits the gene mutation from eachparent and who will have the condition (Fig. 9-9).
X-Linked InheritanceX-linked conditions may be inherited in families in recessive ordominant patterns (see Table 9-1). In both, the gene mutation islocated on the X chromosome. All males inherit an X chromo-some from their mother and a Y chromosome from their father
for a normal sex constitution of 46,XY. Since males have only oneX chromosome, they do not have a counterpart for its genes as dofemales. This means that a gene mutation on their X chromo-some is expressed when present in one copy. A female, on theother hand, inherits one X chromosome from each parent for anormal sex constitution of 46,XX. A female may be a carrier of
130 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Table 9-1 • Patterns of Mendelian Inheritance
CHARACTERISTICS EXAMPLES
Autosomal Dominant Inherited ConditionsVertical transmission in familiesMales and females equally affectedVariable expression among family members and others with
conditionReduced penetrance (in some conditions)Advanced paternal age associated with sporadic cases
Autosomal Recessive Inherited ConditionsHorizontal pattern of transmission seen in familiesMales and females equally affectedAssociated with consanguinity (genetic relatedness)Associated with particular ethnic groups
X-Linked Recessive Inherited ConditionsVertical transmission in familiesMales predominantly affected
Multifactorial Inherited ConditionsOccur as a result of genetic and environmental factors combiningMay recur in familiesInheritance pattern does not demonstrate the characteristic pattern
of inheritance seen with other mendelian inherited conditions
Hereditary breast/ovarian cancer syndromeFamilial hypercholesterolemiaHereditary non-polyposis colorectal cancerHuntington diseaseMarfan syndromeNeurofibromatosis
Cystic fibrosisGalactosemiaPhenylketonuriaSickle cell anemiaTay-Sachs diseaseCanavan disease
Duchenne muscular dystrophyHemophilia A and BWiscott-Aldrich syndromeProtan and Deutran forms of color blindness
Congenital heart defectsCleft lip and/or palateNeural tube defects (anencephaly and spina bifida)Diabetes mellitusOsteoarthritisHigh blood pressure
Adapted from Lea, D. H., Jenkins, J. F., & Francomano, C. A. (1998). Genetics in clinical practice: New directions for nursing and health care.Sudbury, MA: Jones & Bartlett; Lea, D. H. (2002). Genetics. In Maher, A. B., Salmond, S. W., & Pellino, T. A. (Eds.) Orthopaedic nursing.Philadelphia: W. B. Saunders.
I
II
IIIAffected MaleAffected femaleCarrier maleCarrier femaleUnaffected maleUnaffected female
FIGURE 9-8 Three-generation pedigree illustrating autosomal recessiveinheritance.

a gene mutation or affected if the condition results from a gene mu-tation causing a dominant X-linked condition. Either the X chromosome that a female receives from her mother or theX chromosome she receives from her father may be passed on toher sons, and this is a random occurrence.
The most common pattern of X-linked inheritance is that inwhich a female is a carrier for a gene mutation on one of her X chromosomes. This is referred to as X-linked recessive inheri-tance. In X-linked recessive inherited conditions, a female carrierhas a 50% chance to pass on the gene mutation to a son, whowould be affected, or to a daughter, who would be a carrier likeher mother (Fig. 9-10).
Nontraditional Inheritance PatternsAlthough mendelian inherited conditions present with a spe-cific pattern of inheritance in some families, many diseases andtraits do not follow these simple patterns. A variety of factorsinfluence how a gene performs and is expressed. Different mu-tations in the same gene can produce variable symptoms in dif-ferent individuals, as is the case with cystic fibrosis. Differentmutations in several genes can lead to the identical outcome,as observed with Alzheimer’s disease. Some traits involve thesimultaneous mutation in two or more genes. A recently ob-served phenomenon, imprinting, can determine which pair ofgenes (the mother’s or the father’s) will be silenced or activated.This form of inheritance has been observed in Angelman syn-
drome, a severe form of mental retardation and ataxia (Thompsonet al., 2001).
Multifactorial and Complex Genetic ConditionsMany birth defects and common health conditions such as heartdisease, high blood pressure, cancer, osteoarthritis, and diabetesoccur as a result of interactions of multiple gene mutations andenvironmental influences, and thus are called multifactorial orcomplex conditions (see Table 9-1). Multifactorial conditionsmay cluster in families but do not present with the characteristicpattern of inheritance seen in families having mendelian inher-ited conditions (Fig. 9-11). Neural tube defects, such as spina bi-fida and anencephaly, are examples of multifactorial geneticconditions (Chart 9-2).
Chapter 9 Genetics Perspectives in Nursing 131
Carrierfather
Carriermother
Normalson
Carrierson
Carrierdaughter
Affecteddaughter
FIGURE 9-9 In diseases associated with altered recessive genes, bothparents—though disease-free themselves—carry one normal allele and onealtered allele. Each child has one chance in four of inheriting two altered al-leles and developing the disorder; one chance in four of inheriting two nor-mal alleles; and two chances in four of inheriting one normal and one alteredallele, and being a carrier like both parents. From the National Institutes ofHealth and National Cancer Institute. (1995). Understanding gene testing(NIH Pub. No. 96-3905). Washington, DC: U.S. Department of HumanServices.
Affected maleCarrier femaleUnaffected maleNoncarrier female
I
II
III
FIGURE 9-10 Three-generation pedigree illustrating X-linked recessiveinheritance.
I
II
III
Unaffected maleUnaffected femaleAffected male
FIGURE 9-11 Three-generation pedigree illustrating multifactorialconditions.

CHROMOSOMAL DIFFERENCES AND GENETIC CONDITIONSDifferences in the number or structure of chromosomes are amajor cause of birth defects, mental retardation, and malignan-cies. Chromosomal differences are present in approximately 1 inevery 160 live-born infants and are the cause of greater than 50%of all spontaneous first-trimester pregnancy losses (Lashley, 1998;Thompson et al., 2001). Chromosomal differences most com-monly involve an extra or missing chromosome. This is called ane-uploidy. Whenever there is an extra or missing chromosome, thereis always associated mental or physical disability to some degree.
Down syndrome, or trisomy 21, is a common chromosomalcondition that occurs with greater frequency in pregnancies ofwomen who are 35 years or older. A person who has trisomy 21Down syndrome has a complete extra number 21 chromosome,which causes a particular facial appearance and increased risk forcongenital heart defects, thyroid and vision problems, andmental retardation. Other examples of chromosomal differencesinclude trisomy 13 and 18, both more severe than Down syn-drome, and conditions involving extra or missing sex chromo-somes (eg, Turner syndrome, in which females have only one X chromosome instead of the usual two) (Lashley, 1998).
Chromosomal differences may also involve a structural re-arrangement within or between chromosomes. These are lesscommon than chromosomal conditions in which there is an extraor missing chromosome, but occur in 1 in every 500 newborns(Thompson et al., 2001). People who carry “balanced” chromo-some rearrangements have all of their chromosomal material, butit is rearranged. A person who carries a balanced chromosomal re-arrangement has an increased risk for spontaneous pregnancy lossand for having children with an unbalanced chromosomal arrange-ment that may result in physical or mental disabilities. Knowncarriers are therefore offered prenatal counseling and testing.
Chromosome studies may be needed at any age, dependingupon the indication. Two common indications are for confirma-tion of a suspected diagnosis such as Down syndrome, and for a his-tory of two or more unexplained pregnancy losses. Chromosomestudies are accomplished by obtaining a tissue sample (eg, blood,skin, amniotic fluid), preparing and staining the chromosomes,and analyzing them under a microscope. The microscopic study
of chromosomes is called cytogenetics and is an area that israpidly evolving. Today, cytogenetics is used with new molecu-lar techniques such as fluorescent in situ hybridization (FISH),which permits more detailed examination of chromosomes. FISHis useful to detect small abnormalities, including characterizingchromosomal rearrangements (Thompson et al., 2001).
Clinical Applications of GeneticsOne of the most immediate applications of new genetics discov-eries is the development of genetic tests that can be used to detecta trait, diagnose a genetic condition, and identify people whohave a genetic predisposition to a disease such as cancer or heartdisease. Another emerging application is pharmacogenetics. Phar-macogenetics involves the use of genetic testing to identify ge-netic variations that relate to the safety and efficacy of medicationsand gene-based treatments, so that individualized treatment andmanagement plans can be developed. Future applications may in-clude the use of gene chips to map a person’s individual genomefor genetic variations that may lead to disease. Nurses will be in-volved in caring for patients who are undergoing genetic testingand gene-based treatments. Knowledge of the clinical applicationsof modern genetics technologies will prepare nurses to informand support patients, and to provide high-quality genetics-relatedhealth care.
GENETIC TESTINGGenetic tests provide information leading to the diagnosis of in-herited conditions or other conditions with a known genetic con-tribution. Genetic testing involves the use of specific laboratoryanalyses of chromosomes, genes, or gene products (eg, enzymes,proteins) to learn whether a genetic alteration related to a specificdisease or condition is present in an individual. Genetic testingcan be DNA-based, chromosomal or biochemical.
There are several important uses for genetic testing, as identi-fied by the Secretary’s Advisory Committee on Genetic Testing(SACGT, 2000). Prenatal testing includes all three types of ge-netic testing (DNA-based, chromosomal and biochemical) andis widely used for prenatal screening and diagnosis of such con-ditions as Down syndrome. Carrier testing is used to determinecarrier status, helping couples or individuals learn whether theycarry a recessive allele for an inherited condition (eg, cystic fi-brosis, sickle cell anemia, or Tay-Sachs disease) and thus riskpassing it on to their children. Genetic testing is also used widelyin newborn screening, and in the United States is made avail-able for an increasing number of genetic conditions. Two ex-amples are PKU and galactosemia. Diagnostic testing is used todetect the presence or absence of a particular genetic alterationor allele to identify or confirm a diagnosis of a disease or con-dition in an affected individual—for example, myotonic dys-trophy and fragile X syndrome. In the near future, genetic testswill be increasingly used to identify a person’s predisposition todisease and to design specific and individualized treatment andmanagement plans. Examples of current uses of genetic tests areshown in Table 9-2.
Nurses will increasingly participate in genetic testing, espe-cially in the areas of patient education, ensuring informed healthchoices and consent, advocating for privacy and confidentialitywith regard to genetic test results, and assisting patients to un-derstand the complex issues involved in genetic testing (Lea &Williams, 2002).
132 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Neural Tube Defects and Folic Acid
Most neural tube defects are caused by both genetic and environ-mental influences that combine during early embryonic develop-ment, leading to incomplete closure of the neural tube. More rarely,chromosomal abnormalities such as trisomy 18 or prenatal expo-sure to certain medications such as valproic acid are the underlyingcause of neural tube defects.
Research has shown that folic acid taken in the prescribedamount of 4.0 mg daily prior to conception and during the first3 months of pregnancy reduces the recurrence of neural tube de-fects by 70% in women who have had a previously affected preg-nancy. It is now recommended that all women in childbearingyears take folic acid (0.4 mg) daily as part of a multivitamin to de-crease the risk for neural tube defects (Centers for Disease Controland Prevention, 1992; Hall & Solehdin, 1998). Folic acid is rec-ognized as an important environmental element that plays a criti-cal role in fetal development and influences the outcome of geneticsusceptibility to neural tube defects.
Chart9-2
Chart9-2

GENETIC SCREENINGGenetic screening, in contrast to genetic testing, is a broader con-cept and applies to testing of populations or groups independentof a positive family history or symptom manifestation. Geneticscreening, as defined in 1975 by the Committee for the Study ofInborn Errors of Metabolism of the National Academy of Sci-ences (SACGT, 2000), has several major aims. One is manage-ment; that is, identifying people with treatable genetic conditionsthat could prove dangerous to their health if left untreated. Anexample of this is screening of newborns. A second aim is to pro-vide reproductive options to people with a high probability ofhaving children with severe, untreatable diseases and for whomgenetic counseling, prenatal diagnosis, and other reproductiveoptions could be helpful and of interest. This is illustrated by thescreening of individuals of Ashkenazi Jewish descent for conditionssuch Tay-Sachs disease and Canavan disease. A third aim is screen-ing pregnant women to detect birth defects such as neural tube de-fects and Down syndrome using multiple marker screening.Genetic screening may also be used for public health purposes todetermine the incidence and prevalence of a birth defect, or to in-vestigate the feasibility and value of new genetic testing methods.
Most commonly genetic screening occurs in prenatal and new-born programs that involve nurses in various roles and settings.However, it is anticipated that genetic screening will expand inthe future to include adult-onset conditions such as cancer, heartdisease, diabetes, and hemochromatosis. Table 9-3 gives exam-ples of genetic screening applications.
In the future, population-based (widespread) genetic screeningwill be applied to help identify people who are predisposed to de-
velop conditions such as breast and colon cancer and heart disease.Nurses will be expected to participate in explaining genetics con-cepts such as risk and genetic predisposition, supporting informedhealth decisions and opportunities for prevention and early inter-vention, and protecting patients’ privacy (Lea & Williams, 2002).
TESTING AND SCREENING FOR ADULT-ONSET CONDITIONSAdult-onset conditions are disorders with a genetic componentthat are manifested in later life. Often symptoms or clinicalmanifestations occur only in late adolescence or adulthood, anddisease is clearly observed to run in families. Some of these con-ditions are attributed to specific genetic mutations followingeither autosomal dominant inheritance or autosomal recessiveinheritance. However, the majority of adult-onset conditions areconsidered to be multifactorial (polygenetic) in nature (eg, heartdisease, diabetes, arthritis). Nursing assessment for adult-onsetconditions is based on the family history and the identification ofdiseases or clinical manifestations associated with adult- onsetconditions. Knowledge of adult-onset conditions and their geneticbasis (ie, mendelian versus multifactorial conditions) influencesthe nursing considerations for genetic testing. Table 9-4 describesadult-onset conditions, their age of onset, pattern of inheritance,genes involved, and testing availability.
If a single gene accounts for an adult-onset condition in asymptomatic individual, diagnostic testing is used to confirm adiagnosis to assist in the plan of care and management. Diagnostictesting for adult-onset conditions is most frequently used withautosomal dominant conditions, such as Huntington disease or
Chapter 9 Genetics Perspectives in Nursing 133
Table 9-2 • Genetic Tests: Examples of Current Uses
PURPOSE OF GENETIC TEST TYPE OF GENETIC TEST
Carrier TestingCystic fibrosisTay-Sachs disease
Canavan diseaseSickle cell anemiaThalassemia
Prenatal Diagnosis—amniocentesis is often per-formed when there is a risk for a chromosomal orgenetic disorder:Risk for Down syndromeRisk for cystic fibrosisRisk for Tay-Sachs disease
Risk for open neural tube defect
DiagnosisDown syndromeFragile X syndromeMyotonic dystrophy
Presymptomatic TestingHuntington diseaseMyotonic dystrophy
Susceptibility TestingHereditary breast/ovarian cancerHereditary non-polyposis colorectal cancer
DNA analysisHexosaminidase A activity testing and DNA
analysisDNA analysisHemoglobin electrophoresisComplete blood count and hemoglobin
electrophoresis
Chromosomal analysisDNA analysisHexosaminidase A activity testing and/or
DNA analysisProtein analysis
Chromosomal analysisDNA analysisDNA analysis
DNA analysisDNA analysis
DNA analysisDNA analysis

Factor V Leiden thrombophilia, and autosomal recessive condi-tions, such as hemochromatosis. In families with known adult-onset conditions or with a confirmed genetic mutation in anaffected family member, presymptomatic testing provides asymp-tomatic individuals with information about having a geneticmutation and about the likelihood of developing the disease.Huntington disease has served as the model for presymptomatictesting because the presence of the genetic mutation predicts dis-ease onset and progression. Although preventive measures are notyet available for Huntington disease, the genetics information en-ables health care providers to develop a clinical, supportive, andpsychological plan of care. Presymptomatic testing is consideredfor families with a known adult-onset condition in which eithera positive or negative result will affect medical management or inwhich earlier treatment of a condition is more beneficial thantreatment at a later stage. Presymptomatic testing is therefore of-fered for several adult-onset conditions, such as cancer, throm-bophilia, and antitrypsin deficiency.
In the absence of a single disease-causing gene, it is thoughtthat multiple genes are related to the onset of most adult diseases.These susceptibility genes modify or influence the developmentand severity of disease. Most susceptibility testing is conducted inthe research setting to identify candidate genes for disease, suchas Alzheimer’s, psychiatric conditions, heart disease, hypertension,and hypercholesterolemia. For some diseases, the interaction ofseveral genes and other environmental or metabolic events affectdisease onset and progression. Susceptibility testing can help todistinguish variations within the same disease or response to treat-ment. For example, no single gene is associated with osteoporo-sis. Several polymorphisms on candidate genes related to thevitamin D receptor, estrogen and androgen receptors, cytokineproduction and its associated stimulation of osteoclasts, and col-lagen type 1-alpha 1 are under study to predict bone mineraldensity and fracture risk. Some susceptibility genes may predicttreatment response. For example, individuals can present withsimilar clinical signs and symptoms of asthma but have differentresponses to treatment. Susceptibility testing can help classify theasthma as sensitive or resistant to treatment with corticosteroids.
Population screening, the use of genetic testing for largegroups or whole populations, to identify late-onset conditions isunder development. Currently population screening is offered insome ethnic groups to identify cancer-predisposing genes. Forexample, Ashkenazi Jewish individuals (Jews of Eastern Europeanorigin) have a greater chance of having inherited a specific geneticmutation in the BRCA1 or BRCA2 genes. Individuals with oneof these BRCA mutations have approximately a 56% risk forbreast cancer, 16% risk for ovarian cancer, and 16% risk for pros-tate cancer by age 70 (Struewing et al., 1997). Therefore, identi-fying one of these mutations allows the patient the options ofcancer screening as well as other medical management such aschemoprevention or prophylactic mastectomy or oophorectomyin carriers. Population screening is being explored for other adult-onset conditions such as type 2 diabetes and hereditary hemo-chromatosis (iron overload disorder). For a test to be consideredfor population screening, there must be: (1) sufficient informa-tion about gene distribution within populations, (2) accurate pre-diction about the development and progression of disease, and(3) appropriate medical management for asymptomatic individ-uals with a mutation (U.S. Preventive Services Task Force, 1996).
Nursing Considerations for Adult-Onset ConditionsNurses must be alert for family histories that indicate multiplegenerations (autosomal dominant inheritance) or multiple siblings(autosomal recessive inheritance) affected with the same condition,or onset of disease earlier than expected in the general population(eg, multiple generations with early-onset hyperlipidemia). Pos-sible adult-onset conditions are discussed with other members ofthe health care team for appropriate resources and referral.
Information about diagnostic testing is often introduced aspart of a diagnostic work-up. The nurse supports the patient inmaking decisions related to genetic testing and provides referralsfor appropriate education and counseling about the adult-onsetcondition prior to genetic testing. The nurse addresses the pa-tient’s questions or concerns about the benefits and limitations of
134 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Table 9-3 • Applications for Genetic Screening
TIMING OF SCREENING PURPOSE EXAMPLES
Preconception screening
Prenatal screening
Newborn screening
For autosomal recessiveinherited geneticconditions that occurwith greater frequencyamong individuals ofcertain ethnic groups
For genetic conditions thatare common and forwhich prenatal diagnosisis available when apregnancy is identified atincreased risk
For genetic conditions forwhich there is specifictreatment
Cystic fibrosis—all couples, but especiallyNorthern European Caucasian, andAshkenazi Jewish
Tay-Sachs disease—Ashkenazi JewishSickle cell anemia—African American,
Puerto Rican, Mediterranean, MiddleEastern
Alpha-thalassemia—Southeast Asian,African American
Neural tube defects—spina bifida,anencephaly
Down syndromeOther chromosomal abnormalities—
trisomy 18
Phenylketonuria (PKU)GalactosemiaHomocystinuriaBiotinidase deficiency

Chapter 9 Genetics Perspectives in Nursing 135
Table 9-4 • Adult-Onset Disorders
GENETICCLINICAL DESCRIPTION AGE OF ONSET INHERITANCE TEST AVAILABILITY
Early-onset familial Alzheimer’s diseaseProgressive dementia, memory failure, personality disturbance, loss
of intellectual functioning associated with cerebral cortical atrophy,beta-amyloid plaque formation and intraneuronal neurofibrillarytangles
Late-onset familial Alzheimer’s diseaseProgressive dementia, cognitive decline
Frontotemporal dementia with parkinsonism—linked tochromosome 17
Dementia and/or parkinsonism. Slowly progressive behavioralchanges, language disturbances and/or extrapyramidal signs andsymptoms, rigidity, bradykinesia, and saccadic eye movements
Huntington diseaseWidespread degenerative brain change with progressive motor loss
both voluntary and involuntary disability, cognitive decline, chorea(involuntary movements) at later stage, psychiatric disturbances
Neuromuscular disordersSpinocerebellar ataxia type 6Slowly progressive cerebellar ataxia, dysarthria, and nystagmus
Spinocerebellar ataxia type 1Ataxia, dysarthria, and bulbar dysfunction
Spinocerebellar ataxia type 2Slow saccadic eye movement, peripheral neuropathy, decreased
deep tendon reflexes, dementiaSpinocerebellar ataxia type 3Progressive cerebellar ataxia and variety of other neurologic
symptoms including dystonic-rigid syndrome, parkinsoniansyndrome or combined dystonia and peripheral neuropathy
Mild myotonic muscular dystrophyCataracts and myotonia or muscle wasting and weakness, frontal
balding, and ECG changes (heart block or arrhythmia), diabetesmellitus in 5% of all cases
Amyotrophic lateral sclerosis (ALS)Progressive loss of motor function with predominantly lower
motor neuron manifestations
Hematologic conditionsHereditary hemochromatosisHigh absorption of iron by GI mucosa resulting in excessive iron
storage in liver, skin, pancreas, heart, joints and testes.Abdominal pain, weakness, lethargy, weight loss are early symptoms.Untreated individuals can present with skin pigmentation,
diabetes mellitus, hepatic fibrosis or cirrhosis, heart failure,dysrhythmias or arthritis.
Factor V Leiden thrombophiliaPoor anticoagulant response to activated protein C with increased
risk for venous thromboembolism and risk for increased fetalloss during pregnancy
Polycystic kidney disease dominantMost common genetic disease in humans. Manifests with renal
cysts, liver cysts, and occasionally intracranial and aortic aneurysmand hypertension. Loss of glomerular filtration can lead to kidneyfailure.
Diabetes mellitus type IIInsulin resistance and impaired glucose tolerance
<60–65 years andoften before 55
>60–65 years
40–60 years
Mean age 35–44 years
Mean age 43–52 years
Mean age 30–40 years
Mean age 30–40 years
Mean age 30s
20–70 years
50–70 years
40–60 in males;after menopausein females
30s; duringpregnancy infemales
Variable onset—allcarriers havedetectable diseaseby ultrasound atage 30
Variable onset—most often >30
A.D.
A.D.
A.D.
A.D.
A.D.
A.D.
A.D.
A.D. with variablepenetrance
Both A.D. andA.R.
A.R.
A.D.
A.D.
M.F.
Presymptomatic
Presymptomatic
Research
Diagnostic andpresymptomatic
Diagnostic andpresymptomatic
Diagnostic andpresymptomatic
Diagnostic andpresymptomatic
Diagnostic andpresymptomatic
Research
Research
Diagnostic andpresymptomatic
Diagnostic andpresymptomatic
Diagnostic andpresymptomatic
Research
(continued)

genetic testing for the individual and the impact on the family.When testing is completed, the nurse provides support for in-dividuals newly diagnosed with an adult-onset condition and pro-vides teaching about the meaning and implications of the testresults.
Once a mutation for an adult-onset condition is identified in afamily, at-risk family members can be referred for predispositiontesting. If the patient is found to be the mutation carrier, the nurseprovides the patient with information about the risk to otherfamily members. As part of that discussion, the nurse assures thepatient that his or her test results are private and confidential andwill be shared with others, including family members, only withthe patient’s permission. If the patient is an unaffected family
member, the nurse discusses inheritance and the risk of develop-ing the disease, provides support for the decision-making process,and offers referral for genetics services.
Nursing Care and Interventions in GeneticCounseling and EvaluationThe genetic counseling and evaluation process often involves ad-ditional genetic testing and procedures and subsequent decisionsfor patients and families with regard to reproduction, fertility,testing of children, and management options such as prophylacticsurgery. Genetic counseling and evaluation services are tradition-ally offered at various stages: prenatal or perinatal, newborn or
136 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Table 9-4 • Adult-Onset Disorders (Continued)
GENETICCLINICAL DESCRIPTION AGE OF ONSET INHERITANCE TEST AVAILABILITY
Cardiovascular diseaseFamilial hypercholesterolemia. Elevated LDL levels leading to coro-
nary artery disease, xanthomas and corneal arcus.
HyperlipidemiaElevated low-density lipoproteins and triglycerides associated with
premature coronary disease and peripheral vascular disease
Alpha-1 antitrypsin deficiency60–70% small airway and alveolar wall destruction, emphysema
especially at bases, COPD
Oncology conditions
Multiple endocrine neoplasia (MEN 2a)(Familial medullary thyroid cancer) Medullary thyroid cancer,
pheochromocytoma and parathyroid abnormalities
Breast cancerBRCA1, BRCA2 hereditary breast/ovarian cancerBreast, ovarian, prostate and colon (BRCA1)Breast, ovarian and other cancer (BRCA2)
Hereditary non-polyposis colorectal cancerColorectal, endometrial, bladder, gastric, biliary and renal cell
cancers as well as atypical endometrial hyperplasia and uterineleiomyosarcoma
Li-Fraumeni syndromeSoft tissue sarcoma, breast cancer, leukemia, osteosarcoma,
melanoma, and other cancers, often including colon, pancreas,adrenal cortex and brain
Cowden syndromeBreast, non-medullary (papillary or follicular) thyroid cancer.
Breast fibroadenomas and noncancerous thyroid nodules or goiter. Multiple buccal mucosa papillomas (cobblestone-linepapules), facial trichilemmomas, gastrointestinal polyps.
High arched palate, thickened furrowed tongue, megaloencephalyand pectus excavatum.
40–50 years
30–40 years
35 yr/smoker45 yr/nonsmk
Early adulthood
30–70 years often<50 years
<50 years
Often <40 years
40–50 years forcancer
Teens–20s formucocutaneouslesions
A.R. = autosomal recessive; A.D. = autosomal dominant; M.F. = multifactorial.From Cummings, J. L., Vinters, H. V., Cole, G. M., & Khachaturiar, Z. S. (1998). Alzheimer’s disease: Etiologies, pathophysiology, cogni-tive reserve and treatment opportunities. Neurology, 51(Suppl), 2–17; Dik, M. G., Jonker, C., Comijs, H. C., Bouter, L. M., Twisk, J. W.,van Kamp, G. J., & Deeg, D. J. (2001). Memory complaints and APOE-epsilon4 accelerate cognitive decline in cognitively normal elderly.Neurology, 57(12), 2217–2222; Durr, A., & Brice, A. (2000). Clinical and genetic aspects of spinocerebellar degeneration. Current Opinions inNeurolology, 13(4), 407–413; GeneTests GeneClinics. (2001). Web site: http://www.genetest.org; Larkin, K., & Fardaei, M. (2001). Myotonicdystrophy—a multigene disorder. Brain Research Bulletin 2001, 56(3–4), 389–395; Lindor, N. M., Greene, M. H. and the Mayo Familial CancerProgram. (1998). The concise handbook of familial cancer syndromes. Journal of the National Cancer Institute, 90(14), 1039–1071; McIntyre,E. A., & Walker, M. (2002). Genetics of type 2 diabetes and insulin resistance: Knowledge from human studies. Clinical Endocrinology, 57(3),303–311; Pizzuti, A., Friedman, D. L., & Coskey, C. T. (1993). The myotonic dystrophy gene. Archives of Neurology, 50(11), 1173–1179; Ridker, P. M., Miletich, J. P., Buring, J. E., Ariyo, A. A., Price, D. T., Manson, J. E., & Hill, J. A. (1998). Factor V Leiden mutation as a risk factor for recurrent pregnancy loss. Annals of Internal Medicine, 128(12), 1000–1003; Rogaeva, E. (2002). The solved and unsolved mysteries of the genetics of early-onset Alzheimer’s disease. Neuromolecular Medicine, 2(1), 1–10; Rosso, S. M., & van Swieten, J. C. (2002). Newdevelopments in frontotemporal dementia and parkinsonism linked to chromosome 17. Current Opinions in Neurolology, 15(4), 423–428.
A.D.
M.F. in A.R.fashion
A.D.
A.D.
A.D.
A.D.
A.D.
Research
Diagnostic and research
Diagnostic andpresymptomatic
Diagnostic andpresymptomatic
Predisposition
Predisposition
Predisposition
Predisposition and research
Predisposition and research

neonatal, childhood, adolescence, and adulthood. Nurses haveresponsibilities in each of these areas for assessment and provid-ing psychosocial interventions and accurate information as thefamily members consider their genetic testing and treatment op-tions. In all of these areas, the nurse considers the patient in thecontext of the family.
When individuals or family members are considering genetictesting, whether it is for prenatal, newborn, childhood or adult-onset conditions, the nurse provides accurate information as theyconsider their options. For prenatal testing, this would includeinformation and support for subsequent decisions regarding thepregnancy in the event of a prenatal diagnosis of a genetic condi-tion in the fetus. When a genetic diagnosis such as Down syn-drome or hereditary breast or ovarian cancer is made, families needinformation about the range and severity of potential problems,the proportion of individuals with milder aspects of the condition,management options, support organizations, and current under-standing of the long-term prognosis (Williams & Lea, 2003).
Decision-making support is an important nursing interventionin many genetic counseling situations. Examples include when awoman or couple considers the options regarding termination ofa pregnancy or when individuals are considering presymptomatictesting for conditions such as Huntington disease or predispositiontesting for hereditary cancers. The nurse helps the individual andfamily to acquire information about options, identifies the prosand cons of each option, helps the individual and family to ex-plore their values and beliefs, respects each person’s right to re-ceive or not to receive information, and helps the individual toexplain the decision to others (McCloskey & Bulechek, 2000).
Other essential components of nursing care and genetic coun-seling include teaching and an intervention called “coping en-hancement.” Teaching is needed, for example, when a newgenetic diagnosis is made. The family will need informationabout the range of possible health outcomes in this condition,treatment options, and (in the case of prenatal diagnosis of a ge-netic condition) management options regarding continuing orending the pregnancy. “Coping enhancement” involves “assist-ing a person to adapt to perceived stressors, changes or threatsthat interfere with meeting life demands and roles” (McCloskey& Bulechek, 2000, p. 234). Coping enhancement is essentialthroughout the entire genetic counseling, evaluation, and test-ing process. Indicators of patient knowledge, decision-making,and coping outcomes have been developed ( Johnson, Maas, &Moorhead, 2000), and the nurse can use these indicators whendocumenting nursing care provided to families.
INDIVIDUALIZING GENETIC PROFILESInformation about genes and their variations is helping researchersto identify genetic differences that predispose some individuals orgroups to disease and that affect their responses to treatment. Theuse of individualized genetics information to predict predisposi-tion to common diseases will take considerable time to develop.However, genetic tests for non-disease genes (ie, polymorphismsin detoxifying enzymes, cell or drug receptor variations, or otherinherited polymorphisms related to metabolism) are underway.These genetic tests for individual variations or inherited poly-morphisms are called genetic profiles. One major effort of geneticprofiling is focused on enzyme metabolism. Several polymorphismsrelated to enzyme metabolism have been identified in the cyto-chrome P450 family, long known to affect drug metabolism.There are three subcategories of genetic profiles that describepopulation differences in enzyme metabolism genotypes. These
are based on an individual’s genetic make-up for the metabolismof medications or other exogenous compounds into inactive oractive metabolites (Norton, 2001b).
The field of pharmacogenetics (the study of gene variations indrug response) is rapidly advancing the way nurses will adminis-ter and manage drug treatments. Drug metabolism involves en-zyme activity, controlled by genes, for absorption, distribution,and excretion. A single base change, SNPs (single nucleotidepolymorphisms), in genes activated for enzyme activity can causeeither decreased or increased drug metabolism. Genetic testingfor these SNPs will provide a genetic profile, classifying patientsaccording to their drug metabolism type. The SNP classificationsof drug metabolism are effective metabolizers (having the ex-pected metabolism), poor metabolizers (lacking the ability to me-tabolize effectively), and ultra-rapid or rapid metabolizers (havingextremely rapid metabolism of drug compounds). Poor metaboliz-ers are most likely to have adverse events due to the prolongedbioavailability of the drug, while ultra-rapid metabolizers have in-sufficient drug response. Efficient metabolizers can receive the stan-dard expected drug dosage, whereas poor metabolizers need lowerdoses and ultra-rapid metabolizers need higher doses to obtain atherapeutic effect (Roses, 2000). For example, poor metabolizersof antipsychotic agents are more likely to have oversedationand require dose modification to achieve an expected therapeutic response (Scordo & Spina, 2002).
DNA tests to identify patient-specific genetic profiles will bea treatment priority to assist in planning and evaluating treatmentoutcomes, to prevent adverse effects, and to improve therapies.Nurses therefore will need to know how polymorphisms affect apatient’s susceptibility to disease and treatment response. Under-standing the effect of polymorphisms on protein and enzymefunction and their distribution in specific populations will beneeded for health promotion. Since nurses will provide informa-tion about genetic profiles, they will need to know about the im-pact of genetics on treatment.
Applications of Genetics in Nursing PracticeNursing practice in genetics-related health care blends the prin-ciples of human genetics with nursing care in collaboration withother professionals, including genetics specialists, to foster healthimprovement, maintenance, and restoration. In any practice set-ting, nurses will carry out five main activities in genetics-relatednursing practice: help collect and interpret relevant family andmedical histories; identify patients and families who need furthergenetic evaluation and counseling and refer them to appropriategenetics services; offer genetics information and resources to pa-tients and families; collaborate with genetics specialists; and par-ticipate in the management and coordination of care of patientswith genetic conditions. Genetics-related nursing practice in-cludes the care of patients who have genetics conditions, personswho may be predisposed to develop or pass on genetic conditions,and persons who are seeking genetics information and referral foradditional genetics services (Lea, Williams, Jenkins, et al., 2000).
Nurses support patients and families with genetics-relatedhealth concerns by ensuring that their health choices are informedones and by advocating for the privacy and confidentiality of ge-netics information and for equal access to genetic testing andtreatments. The Scope and Standards of Genetics Clinical NursingPractice, developed by the International Society of Nurses inGenetics (ISONG, 1998) and published by the American NursesAssociation, delineates roles and responsibilities for nurses in pro-viding genetics health care.
Chapter 9 Genetics Perspectives in Nursing 137

GENETICS AND HEALTH ASSESSMENTAssessment of a person’s genetics-related health status is an on-going process. The nurse collects information that can helpidentify individuals and families who have actual or potentialgenetics-related health concerns or who may benefit from furthergenetics information, counseling, testing, and treatment. Thisprocess can begin before conception and continue throughoutthe lifespan. Nurses evaluate family and past medical histories, in-cluding prenatal history, childhood illnesses, developmental his-tory, adult-onset conditions (if adult), past surgeries, treatments,and medications; this information may relate to the genetic con-dition at hand or being considered. (See Chap. 5 for more infor-mation on assessing past medical history.) The nurse also identifiesthe patient’s ethnic background and conducts a physical assess-ment to gather pertinent genetics information. The assessmentalso includes the patient’s culture, spiritual beliefs, and ancestry.Genetics-related health assessment always includes determininga patient’s or family’s understanding of actual or potential healthconcerns related to genetics and understanding how these issuesare communicated within a family (ISONG, 1998; Lea, Jenkins& Francomano, 1998).
Family History AssessmentNurses in any practice setting continuously assess genetic familyhistory to identify the presence of a genetic trait, inherited con-dition, or predisposition. A questionnaire (Chart 9-3) is often usedto identify genetic conditions for which further information, ed-ucation, testing, or treatment can be offered. In consultation andcollaboration with other health care providers and specialists, thenurse can then determine whether further genetic testing andevaluation should be offered for the trait or condition in question.A detailed and accurate family history provides the most com-plete genetics health information. The family history should in-clude at least three generations, as well as information about thecurrent and past health status of all family members, including theage of onset of any illnesses and cause of death and age at death.The nurse also inquires about medical conditions known to havea heritable component and for which genetic testing may be of-fered. The nurse obtains information about the presence of birthdefects, mental retardation, familial traits, or similarly affected fam-ily members (Lashley, 1998; Lea, Jenkins & Francomano, 1998).
The nurse also considers the presence of genetic relatedness(consanguinity) among family members when assessing the riskfor genetic conditions in couples or families. For example, whenobtaining a preconception or prenatal family history, the nurseasks whether the prospective parents have common ancestors (ie,they are first cousins). This is important to know because indi-viduals who share ancestors have more genes in common thanthose who are unrelated, thus increasing their chance for havingchildren with an autosomal recessive inherited condition such ascystic fibrosis. The number of shared genes depends upon the de-gree of relationship. A parent and child, for example, share halfof their genes, while first cousins share one in eight of their genes.Ascertaining genetic relatedness gives the nurse the opportunityto offer additional genetic counseling and evaluation. It may alsoserve as an explanation for families who have a child or individ-ual with a rare autosomal recessive inherited condition (Lea,Jenkins & Francomano, 1998).
When the assessment of family history reveals that the patienthas been adopted, genetics-based health assessment becomesmore challenging. The nurse and health care team should make
all efforts to help the patient obtain as much information as pos-sible about his or her biological parents, including their ethnicbackgrounds.
Questions regarding reproductive history (eg, history of mis-carriage or stillbirth) are included in genetic family history healthassessments to identify possible chromosomal conditions. Thenurse also inquires about any history of family members with in-herited conditions or birth defects; maternal health conditionssuch as type 1 diabetes, seizure disorder, or maternal PKU, whichmay increase the risk for birth defects in children; and exposureto alcohol or other drugs during pregnancy. Maternal age is alsonoted: women who are 35 years or older who are consideringpregnancy and childbearing or who are already pregnant shouldbe offered prenatal diagnosis (eg, testing through amniocentesis)because of the association between advancing maternal age andchromosomal abnormalities such as Down syndrome (Lea, Jenkins& Francomano, 1998).
Ancestry and Ethnicity AssessmentAssessing ancestry and ethnicity helps identify individuals andgroups who could benefit from genetic testing for carrier identi-fication, prenatal diagnosis, and susceptibility testing. For exam-ple, carrier testing for sickle cell anemia is routinely offered toindividuals of African-American heritage, while carrier testing forTay-Sachs disease and Canavan disease is offered to individualsof Ashkenazi Jewish descent. Professional organizations such asthe American College of Obstetrics and Gynecology (ACOG,2001) recommend that relevant racial and ethnic populations beoffered carrier testing. Recently, ACOG and the American Col-lege of Medical Genetics (ACMG) recommended that all cou-ples, particularly those of Northern European and AshkenaziJewish ancestry, be offered carrier screening for cystic fibrosis(ACOG, 2001). Ideally, carrier testing is offered before conceptionto allow persons who are carriers to make reproductive decisions.Prenatal diagnosis is offered and discussed when both partners ofa couple are found to be carriers.
Inquiring about a patient’s ethnic background is also impor-tant when assessing for susceptibilities to adult-onset conditionssuch as hereditary breast or ovarian cancer. For example, a spe-cific BRCA1 cancer-predisposing gene mutation seems to occurmore frequently in women of Ashkenazi Jewish descent. There-fore, asking about ethnicity can help identify persons with an in-creased risk for certain cancer gene mutations (American MedicalAssociation, 2001).
The nurse assesses ancestry and ethnic background to identifyindividuals who may have an underlying genetic condition thatmay affect the safety and efficacy of certain medications ortreatments. For example, glucose-6-phosphate dehydrogenasedeficiency (G6PD) is a common enzyme abnormality that affectsmillions of people throughout the world, especially those ofMediterranean, Southeast Asian, African, Middle Eastern, andNear Eastern origin. G6PD is transmitted as a gene mutation onthe X chromosome. Individuals with a severe deficiency havechronic hemolytic anemia, while others with a milder deficiencydevelop hemolytic anemia upon exposure to peroxide-producingdrugs, infection, exposure to naphthalene in mothballs, or inges-tion of the fava (broad) bean (Lashley, 1998).
Assessment of ancestry and ethnic background is also impor-tant when considering drug metabolism. The ability to metabolizeand eliminate certain medications depends upon acetylation in theliver by the enzyme N-acetyltransferase. Many different versions(polymorphisms) of the gene that codes for N-acetyltransferase
138 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE

exist, and these polymorphisms vary among ethnic groups. Thisis an important consideration, for example, when isoniazid (INH)is prescribed for the treatment of tuberculosis. Patients who arerapid or ultra-rapid metabolizers have a significantly higher riskfor developing isoniazid-induced hepatitis; this is especially truefor persons of Chinese and Japanese descent (Lashley, 1998).
Physical AssessmentPhysical assessment may provide clues that a particular geneticcondition is present in an individual and family. Family historyassessment may offer initial guidance regarding the particular
area for physical assessment. For example, a family history offamilial hypercholesterolemia would alert the nurse to assessfamily members for symptoms of hyperlipidemias (xanthomas,corneal arcus, abdominal pain of unexplained origin). As an-other example, a family history of neurofibromatosis type I, aninherited condition involving tumors of the central nervoussystem, would prompt the nurse to carry out a detailed assess-ment of closely related family members. Skin findings such ascafé-au-lait spots, axillary freckling, or tumors of the skin (neuro-fibromas) would warrant referral for further evaluation, includinggenetic evaluation and counseling (Lea, Jenkins & Francomano,1998).
Chapter 9 Genetics Perspectives in Nursing 139
Primary Genetic Family History Screening Questionnaire
Condition Self Partner Relationship
Birth defect name?___________________ ✓ ✓ _______________________Cancer name?_______________________ ✓ ✓ _______________________High cholesterol ✓ ✓ _______________________Cleft lip/cleft palate ✓ ✓ _______________________Cystic fibrosis (CF) ✓ ✓ _______________________Down syndrome (DS) ✓ ✓ _______________________Fragile X syndrome ✓ ✓ _______________________Gastroschisis (opening in belly at birth) ✓ ✓ _______________________Hearing loss/deafness (not from aging) ✓ ✓ _______________________Heart problem (from birth) ✓ ✓ _______________________Heart disease (early onset) ✓ ✓ _______________________Hemophilia (slow clotting/heavy bleeding) ✓ ✓ _______________________Infant death (before one year of age) ✓ ✓ _______________________Inherited health problems ✓ ✓ _______________________Kidney problems (other than infection) ✓ ✓ _______________________Miscarriages ✓ ✓ _______________________Mental retardation ✓ ✓ _______________________Muscular weakness (muscular dystrophy) ✓ ✓ _______________________Pregnancy termination (due to birth defect) __________ ✓ ✓ _______________________Sickle cell anemia ✓ ✓ _______________________Skin or nerve tumor ✓ ✓ _______________________Spina bifida (opening in spine, at birth) ✓ ✓ _______________________Stillbirths ✓ ✓ _______________________Stroke at an early age (called thrombosis) ✓ ✓ _______________________Thalassemia ✓ ✓ _______________________Visual loss/blindness (not from aging) ✓ ✓ _______________________
Chart9-3
Chart9-3
Question 1If you, yourself, have, or if a family member in either your family or the family of your partner has, or ever hashad, one of the following please circle the check mark under SELF or PARTNER and write in the exact rela-tionship of that person to SELF or PARTNER, i.e., child (born or unborn), partner, sibling, grandparent, cousin,aunt or uncle, niece or nephew.
Note: If you have checked any of these conditions, please talk with your nurse about a genetics referral forcounseling and evaluation.Do you have any other medical problems or issues that are of concern to you?(Please circle one) Yes NoIf you circled Yes, please tell your nurse, who may be able to help you or be able to find appropriate support/helpfor you.Patient name ___________________________________________________________________________Date of birth ___________________________________________________________________________Name of person filling out the form (if different from patient) _____________________________________Relationship to patient ____________________________________________________________________Date form filled out ______________________________________________________________________Nurse name ____________________________________________________________________________Date patient seen ________________________________________________________________________
Courtesy of the Foundation for Blood Research.

When a genetic condition is suspected as a result of a familyhistory or physical assessment, the nurse, in collaboration withthe health care team, may initiate further discussion and evaluation.Providing genetics information, offering and discussing genetictests, and suggesting a referral to a geneticist may be performed(Chart 9-4).
Cultural, Social, and Spiritual AssessmentWhen collecting and discussing genetics information, the nurseneeds to assess the patient’s and family’s cultural, social, and spir-itual orientations. The nurse also needs to consider the patient’sviews about the significance of a genetic condition and its effecton self-concept, as well as the patient’s perception of the role ofgenetics in health and illness, reproduction, and disability. Pa-tients’ social and cultural backgrounds determine their interpre-tations and values about information obtained from genetictesting and evaluation and thus influence their perceptions ofhealth, illness, and risk. Family structure and decision-makingand educational background contribute in the same way (Lea,Jenkins & Francomano, 1998).
Assessing a patient’s beliefs, values, and expectations regard-ing genetic testing and information helps the nurse to provide ap-
propriate information about the specific genetics topic. In somecultures, for example, individuals believe that health means theabsence of symptoms and that the cause of illness is supernatural.Patients with these beliefs may initially reject suggestions forpresymptomatic or carrier testing. However, by including re-sources such as family, cultural, and religious community leaderswhen providing genetics-related health care, the nurse can helpensure that patients receive information in a way that tran-scends social, cultural, and economic barriers (Lea, Jenkins &Francomano, 1998).
Psychosocial AssessmentPsychosocial assessment is an essential nursing component of thegenetics health assessment (Chart 9-5). After conducting an ini-tial psychosocial assessment, the nurse will be aware of the po-tential impact of new genetic information on the patient andfamily and how they may cope with this information.
GENETIC COUNSELING AND EVALUATION SERVICESAs the contribution of genetics to the health–illness continuumis recognized, the process of genetic counseling is expected to be-come a responsibility of all health care professionals in clinicalpractice. Nurses are obvious and natural providers of geneticsservices because they are aware of a patient’s personal and familyhistory. They assess patients’ health and make referrals for spe-cialized diagnosis and treatment. They offer anticipatory guidanceby explaining the purpose and goals of a referral. They collabo-rate with primary care providers and specialists in giving sup-portive and follow-up counseling. They coordinate follow-upand case management.
Genetics ServicesGenetics services provide genetics information, education, andsupport to patients and families with genetics-related healthconcerns. Genetics professionals, including medical geneticists,
140 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Chart 9-5 • ASSESSMENT
Psychosocial Genetic Health Assessment
The nurse assesses:• Educational level and understanding of the genetic condi-
tion or concern in the family.• Desired goals and health outcomes in relation to genetic
condition or concern.• Family rules regarding disclosure of medical information
(eg, some families may not reveal a history of diseases such ascancer or mental illness during the family history assess-ment).
• Family rules, boundaries, and cultural practices as well aspersonal preferences about knowing medical information.
• Past coping mechanisms and social support.• Ability to make an informed decision (eg, is the patient
under stress from family situations, acute or chronic illness,or medications that may impair the ability to make aninformed decision).
Indications for Making a Genetic Referral
Prepregnancy and Prenatal• Maternal age of 35 years or greater at expected time of delivery• Previous child with a chromosome problem• Positive AFP profile screening test• Previous child with a birth defect or family history of birth defects• Pregnancy history of two or more unexplained miscarriages• Maternal conditions such as diabetes, epilepsy, or alcoholism• Exposures to certain medications or drugs during pregnancy• Family history of mental retardation
Pediatric• Positive newborn screening test• One or more major birth defects• Unusual (dysmorphic) facial features• Developmental delay/mental retardation• Suspicion of a metabolic disorder• Unusually tall or short stature, or growth delays• Known chromosomal abnormality
Adult• Mental retardation without a known cause• Unexplained infertility or multiple pregnancy losses• A personal or family history of thrombotic events• Adult-onset conditions such as hemochromatosis, hearing loss,
visual impairment• Family history of an adult-onset neurodegenerative disorder
(eg, Huntington disease)• Features of a genetic condition such as neurofibromatosis (café-
au-lait spots, neurofibromas on the skin), Marfan syndrome(unusually tall stature, dilation of the aortic root), others
Cancer History• A personal or family history of cancer with a known or sus-
pected inherited predisposition (eg, early-onset breast cancer,colon cancer, ovarian cancer, retinoblastoma)
• Several family members affected by cancer• A family member with cancer at an unusually young age• A family member with an unusual type of cancer
Chart9-4
Chart9-4

genetics counselors, and advanced practice nurses in genetics,provide specific genetics services to patients and families who arereferred by their primary health care providers. A team approachis often used by genetics specialists to obtain and interpret com-plex family history information, evaluate and diagnose geneticconditions, interpret and discuss complicated genetic test results,support patients throughout the evaluation process, and offer re-sources for additional professional and family support. Patientsparticipate as team members and decision-makers throughout theprocess. Genetics services encompass an evaluation and commu-nication process by which individuals and their families come tolearn and understand relevant aspects of genetics, to make in-formed health decisions, and to receive support as they integratepersonal and family genetics information into daily living (Lea,Jenkins & Francomano, 1998).
Genetic counseling may take place over an extended periodand may entail more than one counseling session, which may in-clude other family members. This allows patients and families tolearn and understand genetics information, to receive supportand guidance in decision-making, and to obtain comprehensiveand coordinated care if they have specific genetic conditions orconcerns. The components of genetic counseling are outlinedin Chart 9-6. Genetic counseling may be offered at any pointduring the lifespan, although genetic counseling issues are oftenrelevant to the life stage in which counseling is sought. Some ex-amples are presented in Chart 9-7 (Lea, Jenkins & Francomano,1998).
Nursing Role in Genetic CounselingPatients seek genetic counseling for a variety of reasons and at dif-ferent stages of life. Some are seeking preconception or prenatalinformation; others are referred following the birth of a child witha birth defect or suspected genetic condition; still others are seek-ing information for themselves or their families because of thepresence or family history of a genetic condition. Regardless ofthe timing or setting, genetic counseling is offered to all patientswho have questions about genetics and their health. In collabo-ration with the health care team, the nurse considers referring forgenetic counseling any patient in whose family a heritable condi-
tion exists and who asks questions such as, “What are my chancesfor having this condition? Is there a genetic test that will tell me?Is there a genetic treatment or cure? What are my options?” (Lea,Jenkins & Francomano, 1998).
Nurses refer clients, collaborate with genetics specialists, andparticipate in genetic counseling when they carry out the follow-ing activities:
• Provide appropriate genetic information before, during,and in follow-up to genetic counseling
• Help gather relevant family and medical history information• Offer support to patients and families throughout the ge-
netic counseling process• Coordinate genetics-related health care with relevant com-
munity and national support resources
These activities, carried out in collaboration with patientsand families, help ensure that they receive the most benefit fromgenetic counseling (Lea, Jenkins & Francomano, 1998; Lea,Williams, Jenkins, et al., 2000).
RESPECTING PATIENTS’ RIGHTSRespecting the patient’s right to self-determination—that is, sup-porting decisions that reflect the patient’s personal beliefs, values,and interests—is a central principle of how nurses provide genet-ics information and counseling. Genetics specialists and nursesparticipating in genetic counseling make every attempt to respectthe patient’s ability to make autonomous decisions. A first step inproviding such nondirective counseling is recognizing one’s ownvalues (see Chart 9-1) and how communication of genetics in-formation may be influenced by those values.
Confidentiality of genetics information and respect for privacyare other essential principles underlying genetic counseling. Thepatient has the right to have testing without having the results di-vulged to anyone, including insurers or physicians. Some patientspay for testing themselves so that insurers will not learn of thetest; others use a different name for testing to protect their pri-vacy. The Health Insurance Portability and Accountability Act(HIPAA) of 1996 prohibits the use of genetics information to es-tablish insurance eligibility. However, it does not prohibit groupplans from increasing premiums, excluding coverage for a specific
Chapter 9 Genetics Perspectives in Nursing 141

condition, or imposing a lifetime cap on benefits. The NationalHuman Genome Research Institute, Policy and Public Affairsand Legislative Activities Branch has a summary of each state’slegislation on employment and insurance discrimination (see theresources list at the end of this chapter).
All genetics specialists, including nurses who participate in thegenetic counseling process and those with access to individuals’genetic information, must honor the patient’s desire for confi-dentiality. Genetics information should be kept from familymembers, insurance companies, employers, and schools if the pa-tient desires, even if keeping the information confidential is dif-ficult. The nurse may want to disclose genetics information tofamily members who could experience significant harm if they donot know such information. However, the patient may have otherviews and may wish to keep this information from the family, re-sulting in an ethical dilemma for both patient and nurse. Thenurse must honor the patient’s wishes while explaining to the pa-tient the potential benefit this information may have to otherfamily members (ISONG, 2002).
PROVIDING PRECOUNSELING INFORMATIONPreparing the patient and family, promoting informed decision-making, and obtaining informed consent are essential in geneticcounseling. The nurse assesses the patient’s capacity and abilityto give voluntary consent. This includes assessment of factors thatmay interfere with informed consent such as hearing and lan-guage deficits, impaired intelligence, and the effects of medica-
tion. The nurse makes sure that the individual’s decision to un-dergo testing is not affected by coercion, persuasion, or manipu-lation. Because information may need to be repeated over time,the nurse offers follow-up discussion as needed (Bove et al.,1997).
The genetics service to which the nurse refers a patient or fam-ily for genetic counseling will ask the nurse to provide back-ground information for evaluation. Genetics specialists need toknow the reason for referral, the patient’s or family’s reason forseeking genetic counseling, and potential genetics-related healthconcerns. The nurse may refer a family with a new diagnosis ofhereditary breast or ovarian cancer, for example, to obtain moreinformation or counseling or to discuss the likelihood of devel-oping the disease and the implications for other family members.The family may have concerns about confidentiality and privacy.Using the nursing assessment, the genetics specialists tailor thegenetic counseling to respond to these concerns.
With the patient’s permission, the nurse may also provide tothe genetics specialists the relevant test results and medical eval-uations. The nurse needs to obtain permission from the patientand, if applicable, from other family members to retrieve, review,and transfer medical records that document the genetic conditionof concern. In some situations, evaluation of more than one fam-ily member may be necessary to establish a diagnosis of a geneticdisorder. The nurse can prepare the family for this assessment byexplaining that the medical information and evaluation are nec-essary to ensure that appropriate information and counseling (in-cluding risk interpretation) are provided.
The nurse will be asked to provide information about theemotional and social status of the patient and family. Geneticsspecialists will want to know the coping skills of a family that hasrecently learned of the diagnosis of a genetic disorder. They willwant to be aware of the types of genetics information beingsought. The nurse helps to identify cultural and other issues thatmay influence how information is provided and by whom. Forpatients with hearing loss, for example, an interpreter’s servicesmay have to be arranged. The genetics professional, after deter-mining these issues with the nurse, prepares for the genetic coun-seling and evaluation with these relevant issues in mind (Lea,Jenkins & Francomano, 1998).
PREPARING THE PATIENT FOR GENETIC EVALUATIONBefore the genetic counseling appointment, the nurse discusseswith the patient and family the type and nature of family historyinformation that will be collected during the consultation. Familyhistory collection and analysis are comprehensive and focus oninformation that may be relevant to the specific genetic concernin question. Although targeted to each genetic counseling situation,such analysis always includes assessment for any other potentiallyinherited conditions for which testing and preventive and treat-ment measures may be offered.
A physical examination performed by the medical geneticistmay be needed to identify specific clinical features that are diag-nostic of a genetic condition. The examination also helps to iden-tify whether additional laboratory tests are needed to clarify thediagnosis of a genetic disorder. The detailed physical examinationgenerally involves assessment of all body systems, with a focus onspecific physical characteristics considered for diagnosis. Thenurse describes the diagnostic evaluations that are part of a ge-netics consultation and explains their purposes (Lashley, 1998;Lea, Jenkins & Francomano, 1998).
142 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE

COMMUNICATING GENETICS INFORMATION TO THE PATIENTAfter the family history and physical examination are completed,the genetics team reviews the information gathered before begin-ning genetic counseling with the patient and family. The genet-ics specialists meet with the patient and family to discuss theirfindings. When information from family and medical historiesand examination confirms the presence of a genetic condition ina family, the genetics specialist discusses with the patient the nat-ural history of the condition, the pattern of inheritance, and theimplications of the genetic condition for reproductive and gen-eral health. When appropriate, the genetic specialists discuss anddescribe relevant testing and management options. The nurse as-sesses the patient’s understanding of the genetic consultation andclarifies information given by the specialists.
PROVIDING SUPPORTThe genetics team provides support throughout the counselingsession and makes every effort to elicit individual and family con-cerns. The genetics specialist uses principles of active listening tointerpret patient concerns and emotions, seek and provide feed-back, and demonstrate understanding of those concerns. Whenneeded, the genetics specialist suggests referral for additionalsocial and emotional support. The genetics specialist discussespertinent patient and family concerns and needs with the nurseand primary health care team so that they can provide additionalsupport and guidance (Lea, Jenkins & Francomano, 1998). Thenurse assesses the patient’s understanding of the informationgiven during the counseling session, clarifies information, an-swers questions, assesses the patient’s reactions, and identifiessupports.
Providing Follow-Up After Genetic EvaluationIn follow-up to genetic evaluation and counseling, the geneticsspecialists prepare a written summary of the evaluation and coun-seling session and, with the patient’s permission, send this sum-mary to the primary health care provider as well as all otherproviders and participants in the patient’s care, as identified bythe family. The consultation summary outlines the results of fam-ily history and physical and laboratory assessments, provides adiscussion of the specific diagnosis (when made), reviews the in-heritance and associated risk of recurrence for the patient andfamily, presents reproductive and general health options, andmakes recommendations for further testing and management.The summary is also sent to the patient and a copy is retained inthe patient’s medical records. The nurse has an important role inreviewing the summary with the patient and family and identify-ing information, education, and counseling for which follow-upgenetic counseling may be useful (Lea, Jenkins & Francomano,1998; Lea & Williams, 2002; Lea & Smith, 2002).
Follow-up genetic counseling is always offered to patients andfamilies, as some may need more time to understand and discussthe specifics of a genetic test or diagnosis or wish to review re-productive options again later when pregnancy is being consid-ered. Follow-up genetic counseling is also offered to clients whenfurther evaluation and counseling of extended family members isrecommended (Lea, Jenkins & Francomano, 1998).
As part of follow-up, nurses can educate patients about whereto find information about genetics issues. Some resources that
provide the most up-to-date and reliable genetics information areavailable on the Internet. Several of these are listed at the end ofthe chapter.
Ethical IssuesWith recent advances in genetics, nurses must consider their re-sponsibilities in handling genetics information and potential eth-ical implications such as informed decision-making, privacy andconfidentiality of genetics information, and access to and justicein health care. The ethical principles of autonomy, fidelity, andveracity are also important (American Nurses Association, 2001).
Ethical questions relating to genetics occur in various settingsand at all levels of nursing practice. At the level of direct patientcare, nurses participate in providing genetics information, test-ing, and gene-based therapeutics. They provide patient care basedon the values of self-determination and personal autonomy. TheAmerican Nurses Association (2001) states that patients shouldbe as fully involved as possible in the planning and implementa-tion of their own health care; to do so, patients need appropriate,accurate, and complete information given at such a level and insuch a form that they and their families can make well-informedpersonal, medical, and reproductive health decisions. Nurses, asthe most accessible health care professionals, are invaluable in theinformed consent process. Nurses can help patients clarify valuesand goals, assess understanding of information, protect the patient’srights, and support their decisions. Nurses can advocate for patientautonomy in health decisions. ISONG’s Position Statement“Informed Decision-Making and Consent” (2000) providessupport and guidance for nurses who are helping patients whoare considering genetic testing.
Nurses need to ensure the privacy and confidentiality of ge-netics information derived from such sources as the family his-tory, genetic tests, and other genetics-based interventions. ManyAmericans are increasingly concerned about threats to their per-sonal privacy. Nurses must be aware of the potential ethical issuesrelated to the privacy and confidentiality of genetics information,including conflicts between an individual’s privacy versus thefamily’s need for genetics information. ISONG’s Position State-ment “Privacy and Confidentiality of Genetic Information”(2002) is a useful resource.
An ethical foundation provides nurses with a holistic frame-work for handling ethical issues with integrity. It also supplies thebasis for communicating genetics information to a patient, to afamily, to other care providers, to community agencies and orga-nizations, and to society as a whole. In addition, it providessupport for nurses facing clinical situations that involve ethicaldilemmas. Principle-based ethics offers moral guidelines thatnurses can use to justify their nursing practice. The emphasis is onethical principles of beneficence (to do good) and non-maleficence(to do no harm), as well as autonomy, justice, fidelity, veracity,to help solve ethical dilemmas that may arise in clinical care.Respect for persons is the ethical principle underlying all nursingcare. With an ethical foundation that is based on these principlesand that incorporates the values of caring, nurses can promote thekind of thoughtful discussions that are useful when patients andfamilies are facing genetics-related health and reproductive deci-sions and consequences (Scanlon & Fibison, 1995; ISONG,2000).
Chapter 9 Genetics Perspectives in Nursing 143

REFERENCES AND SELECTED READINGS
BooksAmerican College of Obstetricians and Gynecologists (ACOG). (2001).
Preconception and prenatal carrier screening for cystic fibrosis: Clinicaland laboratory guidelines. Washington, DC: Author.
American Medical Association. (2001). Identifying and managing hered-itary risk for breast and ovarian cancer. Chicago: Author.
American Nurses Association. (2001). Code for nurses with interpretivestatements. Washington, DC: Author.
Gardiner, R. R. M., & Sutherland, G. R. (1996). Chromosome abnormal-ities and genetic counseling (2d ed.). New York: Oxford University Press.
Hartl, D., & Jones, E. W. (1998). Genetics principles and analysis(4th ed.). Sudbury, MA: Jones & Bartlett Publishing.
ISONG. (1998). Statement on the scope and standards of genetics clinicalnursing practice. Washington, DC: American Nurses Association.
Iowa Intervention Project. (2000). Nursing interventions classification(3rd ed.). St Louis: Mosby.
Iowa Outcomes Project. (2000). Nursing outcomes classification (2d ed.)St. Louis: Mosby.
Johnson, M., Maas, M. L., & Moorhead, S. (Eds.) (2000). Nursinginterventions classification. St. Louis: C.V. Mosby.
Lashley, F. R. (1998). Clinical genetics in nursing practice (2d ed.). NewYork: Springer.
Lea, D. H. (2002). Genetics. In Maher, A. B., Salmond, S. W., & Pellino,T. A. (Eds.) Orthopaedic nursing. Philadelphia: W. B. Saunders.
Lea, D. H., Jenkins, J. F., & Francomano, C. A. (1998). Genetics in clin-ical practice: New directions for nursing and health care. Sudbury, MA:Jones & Bartlett.
Lea, D. H., & Smith, R. S. (2002). Genetics resource guide: A handy ref-erence for public health nurses. Scarborough, ME: Foundation forBlood Research.
McCloskey, J. C. & Bulechek, G. M. (Eds.). (2000). Nursing interventionsclassification (NIC): Iowa Intervention Project (3rd ed.). St. Louis:C. V. Mosby.
National Academy of Science, Committee for the Study of InbornErrors of Metabolism. (1975). Genetic Screening. Washington, DC:National Academy of Sciences.
National Institutes of Health, National Cancer Institute. (1995). Un-derstanding gene testing. Washington, DC: U.S. Department ofHealth and Human Services, NIH Pub. No. 9603905.
Rimoin, D., Connor, J. M., & Pyeritz, R. (2002). Emery-Rimoin prin-ciples and practice of medical genetics (4th ed.). New York: Churchill-Livingstone.
Scanlon, C., & Fibison, W. (1995). Managing genetic information: Im-plications for nursing practice. Washington, DC: American NursesAssociation.
Secretary’s Advisory Committee on Genetic Testing (SACGT). (2000).National Institutes of Health. A public consultation of oversight ofgenetic tests. Bethesda, MD. Available from http://www4.od.nih.gov/oba/sacgt.htm.
Thompson, M. W., McInnes, R. R., & Willard, H. F. (2001). Thomp-son and Thompson’s genetics in medicine (6th ed.). Philadelphia: W. B.Saunders.
U.S. Preventive Services Task Force. (1996). Guide to clinical preventiveservices (2d ed.). Baltimore: Williams & Wilkins.
Williams, J. K., & Lea, D. H. (2003). Genetic issues for perinatal nurses(2d ed.). White Plains, NY: March of Dimes.
JournalsACOG Committee on Genetics. (1996). Screening for Tay-Sachs disease.
International Journal of Gynaecology & Obstetrics, 52(3), 311–312.ACOG Committee on Genetics. (1999). Screening for Canavan disease.
International Journal of Gynaecology & Obstetrics, 65(1), 91–92.ACOG Committee on Genetics. (2001). Genetic screening for hemo-
globinopathies. International Journal of Gynaecology & Obstetrics,74(3), 309–310.
American College of Medical Genetics/American Society of Human Ge-netics Huntington Disease Genetic Testing Working Group. (1998).ACMG/ASHG statement. Laboratory guidelines for Huntingtondisease genetic testing. American Journal of Human Genetics, 62(5),1243–1247.
American Society of Clinical Oncology. (1996). Statement of the Amer-ican Society of Clinical Oncology: Genetic testing for cancer suscep-tibility. Journal of Clinical Oncology, 14(5), 1730–1736.
Anderson, G., Monsen, R. B., Prows, C. A., Tinley, S., & Jenkins, J.(2000). Preparing the nursing profession for participation in a ge-netic paradigm in health care. Nursing Outlook, 48(1), 23–27.
Bartsch, H., Nair, U., Risch, A., et al. (2000). Genetic polymorphism ofCYP genes, alone or in combination, as a risk modifier of tobacco-related cancers. Cancer Epidemiology, Biomarkers and Prevention,9(1), 3–28.
Billings, P. R. (2000). Applying advances in genetic medicine: Where dowe go from here? Healthplan, 41(6), 32–35.
Bove, C. M., Fry, S. T., & MacDonald, D. J. (1997). Presymptomaticand predisposition genetic testing: Ethical and social considerations.Seminars in Oncology Nursing, 13(2), 135–140.
Brookes, A. J. (1999). The essence of SNPs. Gene, 234(2), 177–186.Burke, W. (2002). Genetic testing. New England Journal of Medicine,
347(23), 1867–1875.Burke, W., Thomson, E., Khoury, M. J., et al. (1998). Hereditary he-
mochromatosis: gene discovery and its implications for population-based screening. Journal of American Medical Association, 280(2),172–178.
Centers for Disease Control and Prevention. (1992). Recommendationsfor the use of folic acid to reduce the number of cases of spina bifidaand other neural tube defects. Morbidity and Mortality Weekly Report,41(RR-14), 1–7.
144 Unit 2 BIOPHYSICAL AND PSYCHOSOCIAL CONCEPTS IN NURSING PRACTICE
Critical Thinking Exercises
1. Your patient, age 53, is recovering from a right mastec-tomy. She underwent a left mastectomy for breast cancer atage 45. Her daughter, age 31, expresses concern about herown breast cancer risk, telling you that her sister and mater-nal grandmother have also had breast cancer. What patternof inheritance is suggested in this family? What geneticsinformation would you provide to this woman?
2. A 48-year-old man is admitted to your medical unit witha new diagnosis of liver cancer. He says he is worried abouthis children, an 18-year-old boy and a 15-year-old girl: “I don’t want them to get this, too.” Your nursing assessmentreveals a past history of arthritis and diabetes and a familyhistory of “iron overload” in the patient’s 40-year-old brother.What adult-onset condition does this history suggest? Whatnursing action would you take?
3. Your patient has three daughters, ages 25, 30, and 32,and one son, age 22. He also has four sisters, two of whomwere diagnosed with breast cancer in their early 40s and choseto have BRCA gene mutation testing. Both were found tocarry a BRCA1 gene mutation. The patient’s daughters learnof these results and want to be tested to learn of their status.The patient does not want to be tested and tells the nurse ata routine check-up, “I don’t want to have testing. I have aright not to be tested, and I don’t want to know if I carrythat cancer gene. I care about my daughters, but I am afraidto find out for them.” How might you respond to the pa-tient? What would you say if one of the patient’s daughterscalls you and asks for your help? What are the counselingissues for this daughter that are unique to this situation?
??

Collins, F. S. (1999). Medical and societal consequences of the HumanGenome Project. New England Journal of Medicine, 341(1), 28–37.
Collins, F. S., & McKusick, V. A. (2001). Implications of the HumanGenome Project for medical science. Journal of American MedicalAssociation, 285(5), 540–544.
Cox, N. J., Frigge, M., Nicolae, D. L., et al. (1999). Loci on chromo-somes 2 (NIDDM1) and 15 interact to increase susceptibility to di-abetes in Mexican Americans. Nature Genetics, 21(2), 213–215.
Evans, W. E. & McLeod. (2003). Drug therapy: Pharmacogenomics—Drug disposition, drug targets, and side effects. New England Journalof Medicine, 348(6), 538–549.
Evans, W. E., & Relling, M. V. (1999). Pharmacogenomics: Translat-ing functional genomics into rational therapeutics. Science,286(5439), 487–491
Feetham, S. (1999). Families and the genetic revolution. Implicationsfor primary healthcare, education, and research. Families, Systems &Health, 17(1), 27–43.
FitzGerald, M. G., MacDonald, D. J., Krainer, M., et al. (1996). Germ-line BRCA1 mutations in Jewish and non-Jewish women with early-onset breast cancer. New England Journal of Medicine, 334(3),143–149.
Fleisher, L. K., & Cole, J. (2001). Health insurance portability and ac-countability act is here: What price privacy? Genetics in Medicine,3(4), 286–289.
Ghosh, S., Watanabe, R. M., Valle, T. T., et al. (2000). The Finland-United States Investigation of Non-insulin-dependent Diabetes Mel-litus Genetics (FUSION) Study. I. An autosomal genome scan forgenes that predispose to type 2 diabetes. American Journal of HumanGenetics, 67(5), 1174–1185.
Guttmacher, A. E. & Collins, F. S. (2002). Genomic medicine—a primer.New England Journal of Medicine, 347(19), 1512–1520.
Hall, J., & Solehdin, M. (1998). Folic acid for the prevention of con-genital anomalies. European Journal of Pediatrics, 157, 445–450.
Hanis, C. L., Boerwinkle, E., Chakraborty, R., et al. (1996). A genome-wide search for human non-insulin-dependent (type 2) diabetesgenes reveals a major susceptibility locus on chromosome 2. NatureGenetics, 13(2), 161–166.
ISONG. (2002). Position statement. Privacy and confidentiality of ge-netic information: The role of the nurse. MedSurg Nursing, 11(2),103. Position statement available on-line: http://www.globalreferrals.-com/privacy.htm.
ISONG. (2000). Position statement. Informed decision-making andconsent: The role of nursing. International Society of Nurses in Ge-netics Newsletter, 11(3), 7–8. Position statement available on-line:http://www.globalreferrals.com/consent.htm.
ISONG. (2002). Position statement. Genetic counseling for vulnerablepopulations: The role of nursing. MedSurg Nursing, 11(6), 305.
Khoury, M. J., McCabe, L. L., & McCabe, E. R. B. (2003). Populationscreening in the age of genomic medicine. New England Journal ofMedicine, 348(1), 50–58.
Lea, D. H., Anderson, G., & Monsen, R. B. (1998). A multiplicity ofroles for genetic nursing: Building toward holistic practice. HolisticNursing Practice, 12(3), 77–87.
Lea, D. H. & Williams, J. K. (2002). Genetic testing and screening.American Journal of Nursing, 102(7), 36–50.
Lea, D. H., Williams, J. K., Jenkins, J., Jones, S., & Calzone, K. (2000).Genetic health care: Creating interdisciplinary partnerships withnursing in clinical practice. National Academies of Practice Forum,2(3), 177–186.
Lea, D. H. (2000). A clinician’s primer in human genetics: What nursesneed to know. Nursing Clinics of North America, 35(3), 583–614.
McCarthy, J. J., & Hilfiker, R. (2000). The use of single-nucleotidepolymorphism maps in pharmacogenomics. Nature Biotechnology,18(5), 505–508.
McKinnon, W. C., Baty, B. J., Bennett, R. L., et al. (1997). Predisposi-tion genetic testing for late-onset disorders in adults. A position paperof the National Society of Genetic Counselors. Journal of the Amer-ican Medical Association, 278(15), 1217–1220.
Nebert, D. W., & Dieter, M. Z. (2000). The evolution of drug metab-olism. Pharmacology, 61(3), 124–135.
Norton, R. M. (2001a). Clinical pharmacogenomics: applications inpharmaceutical R&D. Drug Discovery Today, 6(4), 180–185.
Norton, R. M. (2001b). Pharmacogenomics: Pharmacogenomics and individualized drug therapy. Medscape Pharmacotherapy (http://www.medscape.com).
Peters, J. L., Djurdjinovic, L., & Baker, D. (1999). The genetic self: TheHuman Genome Project, genetic counseling and family therapy.Families, Systems & Health, 17(1), 5–25.
Regaldo, A. (1999). Inventing the pharmacogenomics business. Ameri-can Journal of Health Systems Pharmacology, 56(1), 40–50.
Roses, A. (2000). Pharmacogenetics and future drug development anddelivery. Lancet, 355(9212), 1358–1361.
Sachidanandam, R., Weissman, D., Schmidt, S. C., et al. (2001). A mapof human genome sequence variation containing 1.42 million singlenucleotide polymorphisms. Nature, 409(6822), 928–933.
Schafer, A. J., & Hawkins, J. R. (1998). DNA variation and the futureof human genetics. Nature Biotechnology, 16, 33–39.
Scordo, M. G., & Spina, E. (2002). Cytochrome P450 polymorphismsand response to antipsychotic therapy. Pharmacogenomics, 3(2),201–218.
Struewing, J. P., Abeliovich, D., Peretz, T., et al. (1996). The carrier fre-quency of the BRCA1 185delAG mutation is approximately 1 per-cent in Ashkenazi Jewish individuals. Nature Genetics, 12(1),198–200.
Struewing, J. P., Hartge, P., Wacholder, S., et al. (1997). The risk ofcancer associated with specific mutations of BRCA1 and BRCA2among Ashkenazi Jews. New England Journal of Medicine, 336(20),1401–1408.
Weinshilboum, R. (2003). Genomic medicine: Inheritance and drug re-sponse. New England Journal of Medicine, 348(6), 529–537.
RESOURCES AND WEBSITES
Association of Women’s Health, Obstetric and Neonatal Nurses, 2000L. Street, NW, Suite 740, Washington, DC 20036; (202) 261-2400or (800) 673-8499; fax (202) 728-0575; http://www.awhonn.org/resour/POSITION.
Genetic Alliance, Inc., 4301 Connecticut Ave. NW, Suite 404,Washington, DC 20008-2304; (202) 966-5557; e-mail: [email protected]; http://www.geneticalliance.org.
Gene Clinics, University of Washington School of Medicine, 9725Third Avenue NE, Suite 610, Seattle, WA 98115; (206) 221-4674;fax (206) 221-4679; e-mail: [email protected]; http://www.geneclinics.org.
Gene Tests, Children’s Hospital and Regional Medical Center, P.O. Box5371, Seattle, WA 98105-0371; (206) 527-5742; fax (206) 527-5743; e-mail: [email protected].
International Society of Nurses in Genetics, Inc. (ISONG), ExecutiveDirector Eileen Rawnsley, 7 Haskins Road, Hanover, NH 03755;(603) 643-5706; fax (603) 643-3169; e-mail: Eileen.Rawnsley@valleynet; http://www.nursing.creighton.edu/isong/.
National Coalition for Health Professional Education in Genetics(NCHPEG); 2630 W. Joppa Rd., Suite 320, Lutherville, MD21093; (410) 583-0600; http://www.nchpeg.org.
National Organization for Rare Disorders, Inc. (NORD), P.O. Box8923, New Fairfield, CT 06812-8923; (203) 746-6518; fax (203)746-6481; e-mail: [email protected].
National Cancer Institute (NCI), Public Inquiries Office, Building, 31,Room 10A03, 31 Center Drive, MSC 2580, Bethesda, MD 20892-2580; (301) 435-3848; http://www.nci.nih.gov.
Online Mendelian Inheritance in Man (OMIM), National Center forBiotechnology Information, National Library of Medicine, Building38A, Room 8N805, Bethesda, MD 20894; (301) 496-2475; fax(301) 480-9241; http://www.ncbi.nlm.nih.gov/Omim.
Chapter 9 Genetics Perspectives in Nursing 145