Embed Size (px)
Citation preview
1
GERIATRIC PHARMACOLOGY
DRUGS: AFFECT BOTH WELL-BEING AND WALLET!!!

2
INTRODUCTION
3
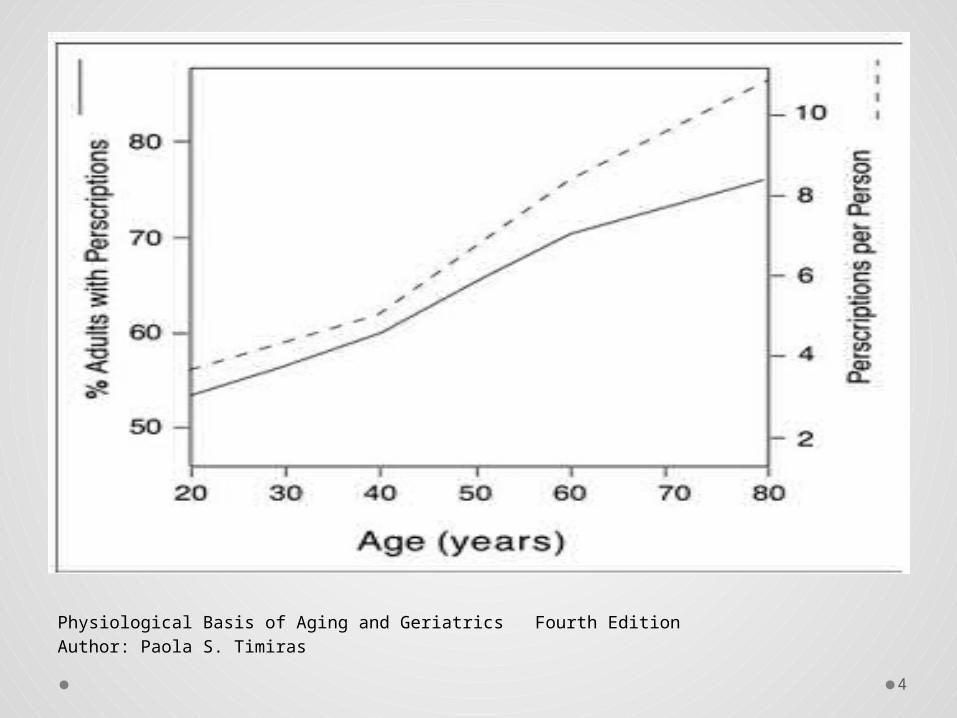
• Elderly population percentage
• Consumption of medications
o ˜- 31 % of total prescribed drugs
o 80-90% elderly consume at least 1 drug/day in
developing countries
JAMA, 2002
• A major public health problem
Public Health Reviews,
2010
4
Physiological Basis of Aging and Geriatrics Fourth EditionAuthor: Paola S. Timiras
5
BURDEN
• Medication related hospital admissions
• Consequences of poly-pharmacy & ADR
• Financial burden:
Economic profile of Indian elderly:
Old age dependency ratio=13.1%
Ministry of Statistics & Program Implementation,
Govt. of India, June 2011
6
DRUGS & BODY INTERACTION
What happens to the drug when it enters the body?
7
PHASES
Study of what happens to
the drug in the body or
how the body processes
the drug
Study of what the drug
does to the body i.e. what
are the effects of the drug
on the body, both at the
systemic and cellular
levels
PHARMACOKINETICS PHARMACODYNAMICS
• Absorption
• Distribution
• Metabolism
• Elimination
• Intensity
• Peak
• Duration
8
ABSORPTIO
N
Intestinal blood flow
Gastric emptying time
Mucosal cell absorption
area
Altered gastric pH
Lipophilic drugs
Acidic drug
binding
Total body fat,
à-1 glycoprotein
Total body mass, total
water content, albumin
DISTRIBUTIO
N
Drug-drug
interaction
Drug-food
interaction
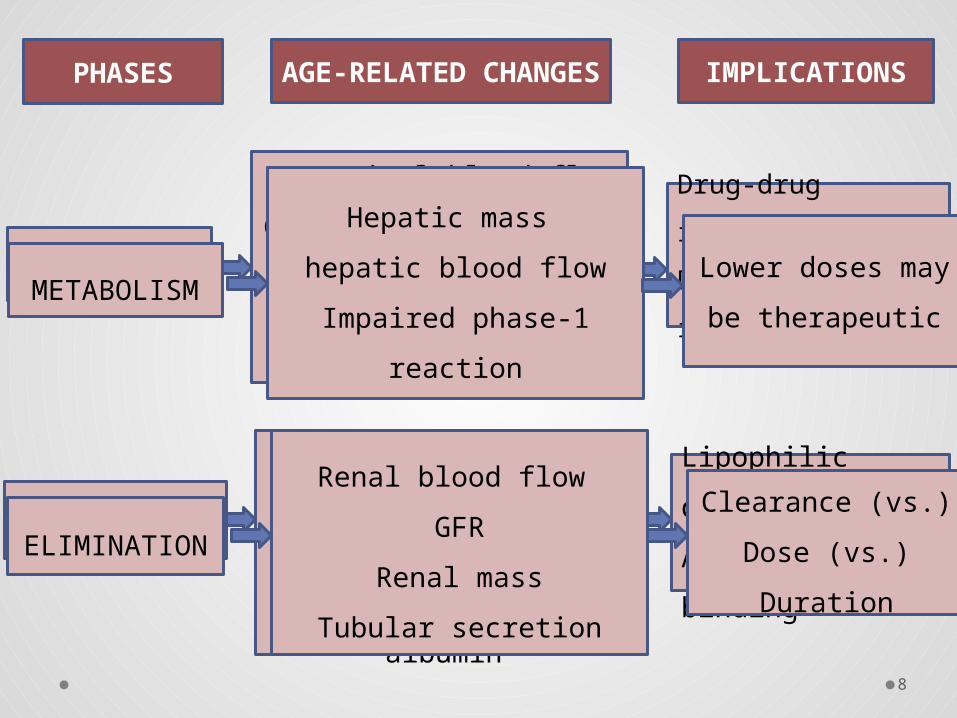
PHASESAGE-RELATED
CHANGESIMPLICATION
S
METABOLIS
M
Hepatic mass
hepatic blood flow
Impaired phase-1
reaction
Lower doses may
be therapeutic
Clearance (vs.)
Dose (vs.)
Duration
Renal blood flow
GFR
Renal mass
Tubular secretion
ELIMINATIO
N

9
PHARMACODYNAMICSAge-related systemic changes:
Homeostatic control
Thermoregulatory mechanisms
Altered cellular responses:
Receptor level
Changes in intra cellular structure and
function
Alterations in the sensitivity to drug
Altered therapeutic effects of drug
Example: Hypertension
Age-related changes like:
Reduced baroreceptor function
Reduced peripheral venous tone
Drug: vasodilators
Younger
individuals
response:
tachycardia
Elderly individuals:
No CV response
due to age-related
changes
10
ADVERSE DRUG EVENTS IN ELDERLY
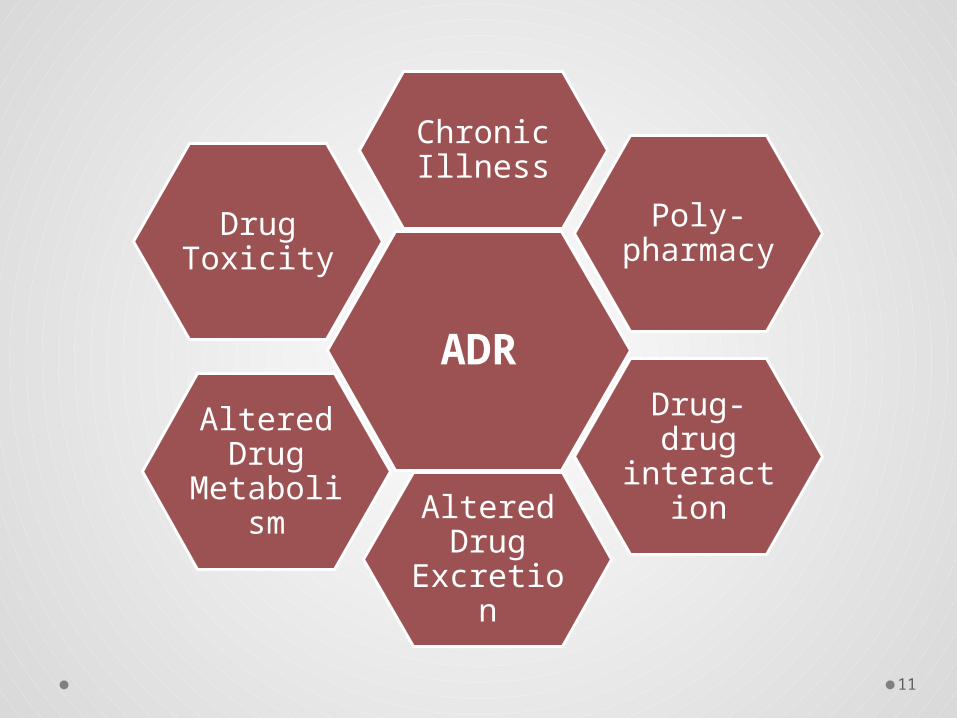
11
ADR
Chronic Illness
Poly-pharmacy
Altered Drug Metabolism
Altered Drug Excretion
Drug-drug interaction
Drug Toxicity
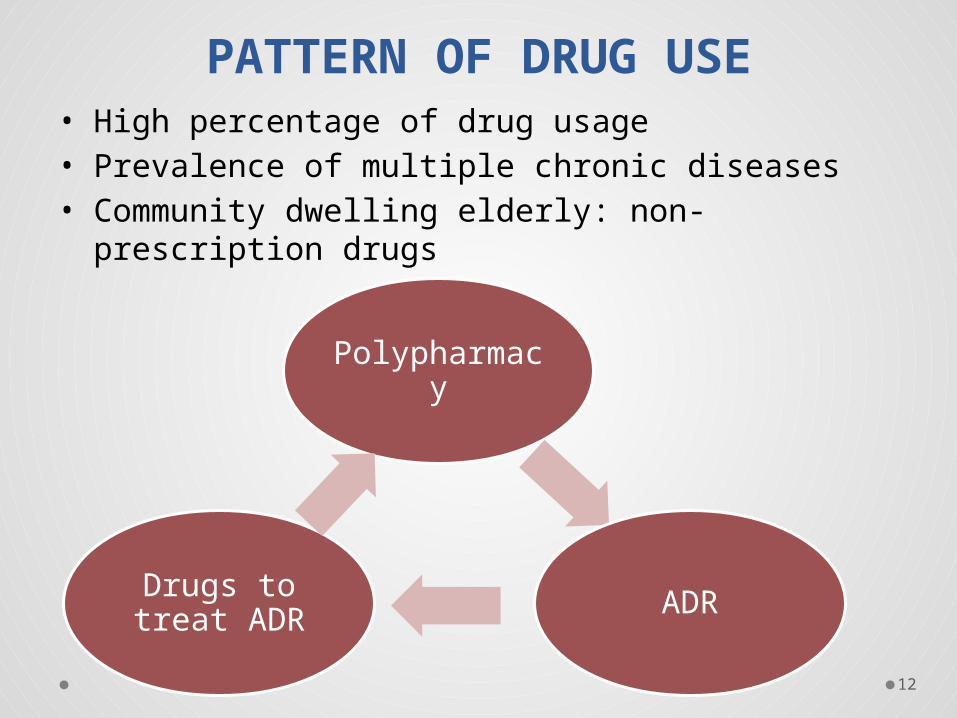
12
PATTERN OF DRUG USE• High percentage of drug usage• Prevalence of multiple chronic diseases • Community dwelling elderly: non-prescription
drugs
Polypharmacy
ADRDrugs to treat ADR
13
REASONS FOR MEDICATION
RELATED PROBLEMS
14
Critical Reviews in Oncology/Hematology, 2009
ALTERED RESPONSES
•Physiological and pathological changes due to aging
•Altered pharmacokinetic and pharmacodynamics response
•Cumulative effects of aging and drugs
•Altered response: longer drug half life
15
MULTIPLE & CHRONIC
DISEASES
• Multiple disease state is defined as the presence of
at least more than one disease conditions that is
commonly found in geriatric population.
• Prevalence of multiple chronic diseases
Centers for Disease Control and
Prevention ,2010
16
RESEARCH IN GERIATIC
PHARMOCOLOGY• Lack of clinical trials
• Lack of guidelines for drug dosage and regimen
for elderly
17
DRUG-TAKING BEHAVIOUR
• Self-medication/ Over-the-counter medication
• Adherence to prescribed medication
Factors affecting adherence to medication
Pathological conditions: cognitive decline, arthritis of hand, poor eyesight
Polypharmacy
Side-effects of medications
Financial burden
18
POLYPHARMACY
Definition
Factors
Consequences
Assessing inappropriate drug
Tools to reduce polypharmacy
19
DEFINITION• Lack of clear definition
• Number of drugs
• Older definitions
• Polypharmacy (5-9 medications) and high-level
Polypharmacy (>or=10 medications)
• Inappropriate medication
Br J Clin Pharmacol. 2007
Br J Med Pract. 2008
20
FACTORS LEADING TO POLYPHARMACY
• Clinics in Geriatric Medicine, 2012 May; 28(2): 159-72• Guccione A. Geriatric Physical Therapy, second edition
21
• Patient Related
o Socio-demographics
o patients' conditions.
o patient behavior, such as patient's self
medication with all types of medications
o Medications from relatives etc.
• Physician Related
• Patient Physician Interaction
22
CONSEQUENCES
• Drug-drug interaction leading to adverse drug
reactions
• Decreased compliance
• Increased financial burden
23
TOOLS TO REDUCE
POLYPHARMACY
• Non-pharmacological management should be first line of
action
• Communication between physicians
• Communication between physician and patient
• Regular monitoring
• 3-main points to check in a prescription:
o Number
o Regimen
o Dosage
Merle L et al., Drugs Aging, 2005
24
Medications Related Falls in Elderly
Huang et al., Drug Aging, 2012
25
Factors:
Medications with half life period more
than 24hrs
Polypharmacy: more medications lead to
higher incidence of fall
Wilson,1998Common drugs associated with high
incidences of fall are:
• Anti-hypertensives
• Anti- depressants
• Narcotics & sedative

26
27
Medication problems that affect the physical
therapist’s workCOMMON DRUG REACTIONS

28
Drug induced ototoxicity
e.g. Aminoglycoside antibiotics cause irreversible deafness -
like gentamicin
loop diuretics - furosemide (lasix)
NSAIDs (aspirin), quinine cause tinnitus is reversible
Drug Induced oculotoxicity
Amantadine - corneal opacities
amiodarone -corneal micro deposits
Anticholinergics,antidepressants, antihistamines: blurred
vision glaucoma
anticonvulsants - diplopia, nystagmus
adrenergic blocker - reduced tears
digoxin - colored halos
Deafness - problem
communicating
visual acuity - problem seeing
demonstration
29
Drug induced Dizziness, Fainting and Weakness
• Cytotoxic agents: treat cancers, arthritis, autoimmune
diseases
• Antihypertensive medications - beta blockers, Ca++
channel blockers, diuretics, ACE inhibitors
Drug Induced drowsiness, anemia, muscle wasting
• Glucocorticoid steroids
• Drugs that cause insomnia - prevent a good night sleep
e.g. caffeine, aminophylline
• Pain medications
• Muscle relaxants
• Antinauseants
• NSAIDs
Problems while performing exercise,and can be
hazardous
remembering
instructions
30
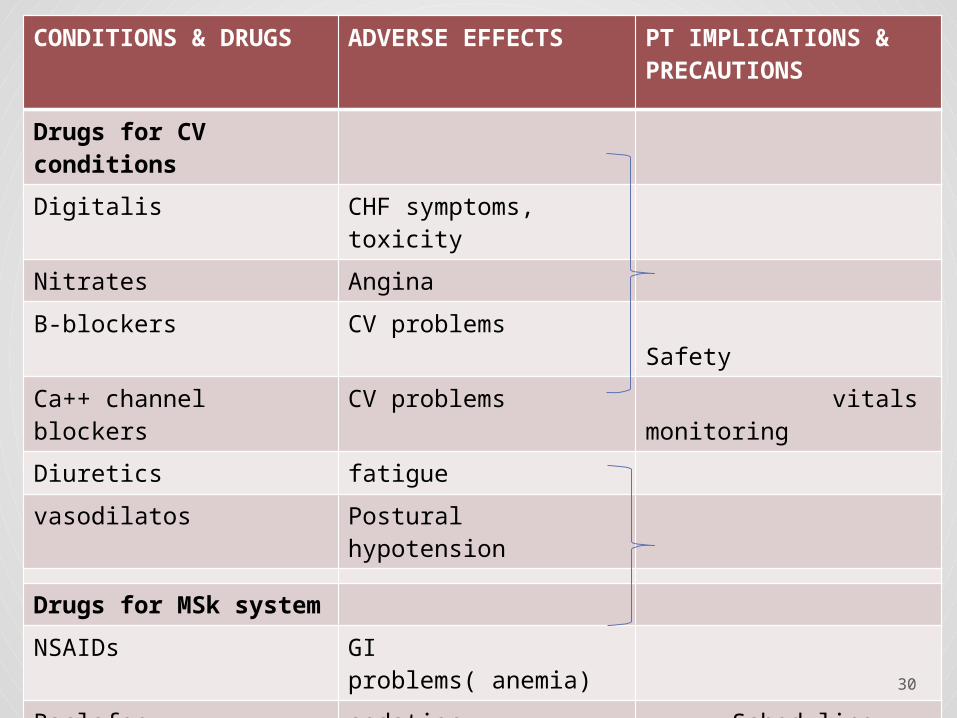
CONDITIONS & DRUGS
ADVERSE EFFECTS PT IMPLICATIONS & PRECAUTIONS
Drugs for CV conditions
Digitalis CHF symptoms, toxicity
Nitrates Angina
B-blockers CV problems Safety
Ca++ channel blockers CV problems vitals monitoring
Diuretics fatigue
vasodilatos Postural hypotension
Drugs for MSk system
NSAIDs GI problems( anemia)
Baclofen sedation Scheduling sessions,
Diazepam sedation vitals monitoring
Narcotics Sedation, OH, GI prob,
Steroids Catabolic effects Electrotherapeutic modalities, Osteoporosis

31
DRUGS COMMON ADVERSE
EFFECTS
PT IMPLICATIONS &
PRECAUTIONS
Anti-
epileptics
Sedation, confusion, GI
problems, skin problems,
other cerebellar signs
like ataxia, etc.
Emergency codes
Co-ordinate sessions
Epilepsy evoking stimulus
Electrotherapeutic modalities
Levadopa Postural hypotension, GI
problems, CV problems,
behavioral changes, etc.
Scheduling sessions: ON-
phase
Cardiac pts. : vitals monitoring
Safety
Anti-
depressants
Sedation, confusion, GI
problems, CV problems,
vision, behavioral
changes
Active participation of pts,
schedule sessions
Vitals monitoring, Safety
Anti-
psychotics
Dyskinesia, drug-induced
Parkinson disease,
dystonia, CV problems,
vision
Scheduling sessions
Safety
32
• Monitor adverse reactions due to drugs &
differentiate ADR from symptoms
• Monitoring exercises based on drugs
pharmacokinetics
• Scheduling rehabilitation sessions
• Drug and physiotherapy interactions
• Modifications in case of adverse reaction
• Advice to caregivers
• Compliance to drug regimen
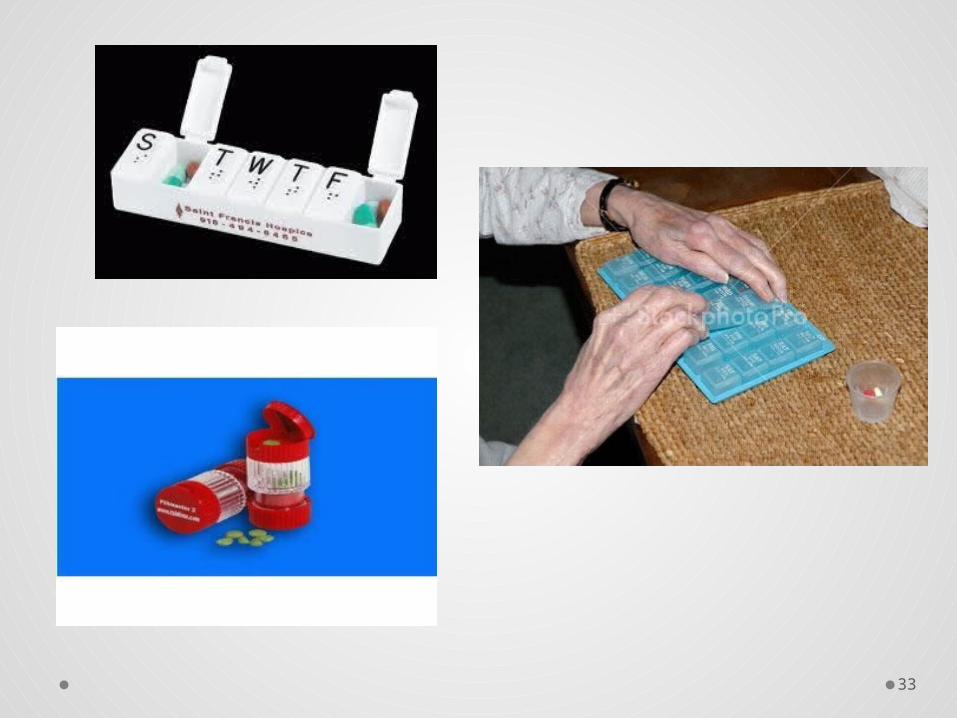
• Pill box for dementia, arthritis patients, etc.
33
34
Conclusion from the evidences:
• Drugs similar as in Lepzig et al., study
• The most commonly used physical performance
measures are:
o Walking speed
o Chair stand
o Grip strength
• Careful assessment and management considering
the drugs
35
REFERENCES
36
• Guccione A. Geriatric Physical Therapy. Second
edition,2000.
• Timiras P. Physiological Basis of Aging and
Geriatrics Fourth Edition, 2007
• Lewis C. and Bottomley J. Geriatric Physical
Therapy A Clinical Approach
• Situation analysis of the elderly in India. Ministry
of Statistics & Program Implementation, Govt. of
India, June 2011
37
• Hanlon JT, Linblad CI, Hajjar E, McCarthy T. Uptade
on Drug- Related Problems in the Elderly. Am J Geri
Pharmathera. 2003; 1(1): 38-43
• Guaraldo L, Cano F, Damasceno G, Rozenfeld S.
Inappropriate medication use among the elderly: a
systematic review of administrative datbases. BMC
Geraitric. 2011,11(79)
• Kirsten KV, Blix HS, Moger TA, Reikvam A,
Polypharmacy as commonly defined is an indicator
of limited value in the assessment of drug-related
problems. Br J Clinc Pharma. 2006; 63(2):187-195