Embed Size (px)
Citation preview
KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
1
Gestational Diabetes Mellitus: A Current Approach
Jo’s Office
GDM-carbohydrate intolerance of any degree with onset or diagnosis during pregnancy (ADA, 2012) GDM A1-diet controlled GDM A2-insulin requiring

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
2
GDM comprises 90% of all DM in pregnancy Reported rates of GDM 5-14% of all pregnancies-true
incidence unknown due to lack of uniform diagnostic criteria Five to 10% of women with GDM have undiagnosed type 2 DM Women over the age of 20 comprise over half of individuals
with diabetes type 2 diabetes and only 25% know it New diagnostic criteria for GDM will increase incidence to 18%
of all pregnancies Increasing prevalence due to delayed childbearing and obesity
Overweight increases risk factor (RF) by 2.1; obese increases RF
3.6; severely obese increases RF 8.6
NIDDK, NATIONAL DIABETES STATISTICS, 2011
Obesity 26%
Diabetes 9%

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
3
Weekly food expenditure: $341.98
Food expenditure for one week: 387.85 Egyptian Pounds or $68.53

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
4
PORTABLE PHONES
REMOTE CONTROLS
KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
5
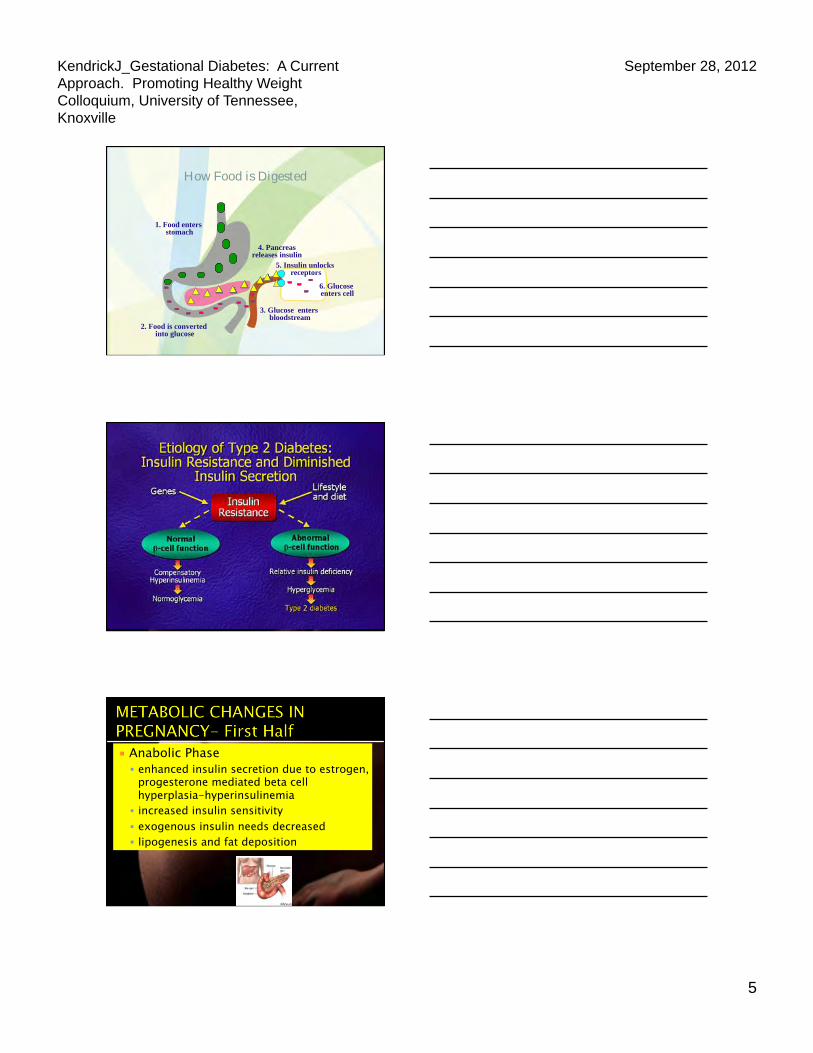
How Food is Digested
1. Food enters stomach
5. Insulin unlocks receptors
4. Pancreas releases insulin
2. Food is converted into glucose
3. Glucose enters bloodstream
6. Glucose enters cell
Anabolic Phase enhanced insulin secretion due to estrogen,
progesterone mediated beta cell hyperplasia-hyperinsulinemia
increased insulin sensitivity exogenous insulin needs decreased lipogenesis and fat deposition

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
6
Catabolic Phase diabetogenic state decreased insulin
sensitivity due to anti-insulin placental hormones
Accelerated starvation-fat breakdown/lipolysis
decreased acid buffering capacity
increased risk for DKA dramatically increased
insulin needs
First prenatal visit—all or at risk Fasting plasma glucose (FPG)->126 mg./
dL. Hgb Aic-6.5% Random Plasma Glucose (RPG)->200 mg./
dL.* If FPG is 92-125, considered early GDM If all of the above normal—then
administer 75 gram OGTT at 24-28 weeks
International Association of Diabetes and Pregnancy Study Groups (IADPSG, 2010). Diabetes Care, 33,#3, March 2010.
MEASURE OF GLYCEMIA THRESHOLD
Fasting Plasma Glucose (FPG)
> 126 mg./dL
A1c > 6.5%
Random plasma glucose (RPG)
> 200 mg./dL confirmed*
*Random plasma glucose must be confirmed by FPG or A1c
Accepted by ADA, 2010, Rejected by ACOG, 2011

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
7
Timing Criteria mg./dL mmol/l Fasting plasma glucose
92 5.1
1 hr plasma glucose
180 10.0
2 hr plasma glucose
153 8.5
*One abnormal values constitutes GDM Accepted by ADA, 2010, Rejected by ACOG, 2011
Low risk does not require screening Age < 25 years Pre-pregnancy weight normal (BMI of 25 or less) No known diabetes in first degree relatives Not a member of high risk racial-ethnic group ▪ Hispanic ▪ African American ▪ Native American ▪ Asian
No history of abnormal glucose tolerance No history of poor obstetric outcome
American Diabetes Association; 2008
Requires testing between 24-28 weeks Abnormal pre-pregnancy weight High risk racial ethnic heritage Family history of type 2 diabetes in first
degree relative History of abnormal glucose tolerance test History of poor obstetric outcome History of fetal macrosomia (>4000 grams)
American Diabetes Association; 2008

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
8
Requires testing as soon as pregnancy confirmed: Severe obesity Prior history of GDM or delivery of a
large-for gestational age infant Presence of glycosuria Diagnosis of polycystic ovarian syndrome Strong family history of type 2 diabetes
American Diabetes Association; 2008
50 gram 1 hour oral glucose challenge test (GCT) Positive at 130 mg./dL ( non fasting)*** ▪ Requires step #2---3 hour OGTT ▪ Requires 25% of women to have OGTT
Positive at 140 mg./dL (fasting) *** ▪ Requires 15% to have OGTT but will miss 10%
Diagnostic at 200 mg./dL.
***Berkus, Stern, Mitchell et al. Does fasting interval affect the glucose challenge test? Am J Obstet Gynecol 1990;163: 1282.
Diagnostic 3 hour oral glucose tolerance test 100 gm(OGTT) for high risk population or 75 gram OGTT
Plasma fasting prior to ingestion Diagnostic for GDM at 120 mg./dL.
Testing should be performed after an overnight
fast with no smoking or activity during test.
Diet prior to fast should be unrestricted (150 gms. CHO) for 3 days

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
9
Organization Test type Diagnostic threshold
ACOG (2011) 100 gm 3 h. OGTT 75 gm
National Diabetes Data Group (NDDG) F: >105 1 hr >195, 2 hr.>165 3 hr>145 Carpenter & Coustan F.>95, 1 hr> 180, 2 hr.>155, 3 hr.>140 F> 95, 1 hr>180, 2 hr.>155
WHO (2010): ADA 2010
75 gm OGTT F: >92, 1 hr>180, 2hr >153
Mullholland, Njorge, Mersereau & Williams, 2007. Comparison of guidelines available in the US for diagnosis and management of diabetes Before, during and after pregnancy. Journal of Women’s Health, 16,790-801.
DIABETES
DIABETES
DIABETES
DIABETES
Women with risk factors with normal 3 h OGTT may benefit from repeat testing at 32 weeks1
Macrosomia associated with one abnormal value2
consider nutrition intervention and repeat OGTT 4 weeks later
1. Neiger, Coustan.(1991) The role of repeat glucose tolerance tests in the diagnosis of GDM. Am J Obstet Gynecol,165:787-790.
2. Lindsay, MK., Graves, Klein. (1989). The relationship of one abnormal glucose tolerance test value and pregnancy complications. Obstet Gynecol, 73; 103-6.

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
10
Total of 25,505 women in 15 centers in nine countries
Took 9 years and 20 million dollars
75 gm OGTT between 24-32 weeks
Blinded to women with FPG < 105 and 1 or 2 hour PG <200 mg./dL.
Analysis based on assigned glucose category The HAPO Study cooperative Research Group (2008). Hyperglycemia and adversePregnancy outcome. NEJM 358 (19); 1991-2002.
Category Fasting Glucose 1 hr. Glucose 2 hr. Glucose
1 <75 <105 <90
2 75-79 106-132 91-108
3 80-84 133-155 109-125
4 85-89 156-171 126-139
5 90-94 172-193 140-157
6 95-99 194-211 158-177
7 100 or more 212 or more 178 or more
Directly proportional change in outcomes to maternal glucose
Adjusted for confounders of maternal BMI, previous macrosomia and previous GDM
Outcome measures Birth weight Umbilical cord c-peptide (chosen due to stability in
frozen sample) Incidence of cesarean delivery Incidence of neonatal hypoglycemia

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
11
Secondary outcome measures with positive associations(related to 1 and 2 hr. glucose but not fasting) Preeclampsia Shoulder dystocia or birth injury Premature delivery Intensive neonatal care hyperbilirubinemia
The HAPO Study Cooperative Research Group. N Engl J Med 2008;358:1991-2002
Evaluated the HAPO results and published their recommendations for screening and diagnosis of hyperglycemia in pregnancy in Diabetes Care 2010;33: 676-682

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
12
International consensus recommendation for the screening and diagnosis of gestational diabetes 75 gram OGTT, one abnormal value Thresholds: FBS: 92 (8.3%) OR 1 hr.: 180
(5.7%) OR 2 hr: 153 (2.1%) Total: 17.8% Odds ratio of 1.75 FOR PRIMARY
OUTCOMES
Prevalence of GDM will be increased to 17.8 % which more closely reflects the incidence of T2dm/pre dm
Cost/benefit analysis not obtained
Requires the availability of dietitians, diabetes educators and staff for increased surveillance of these pregnancies
Additional costs associated with therapy Number of inductions will be increased and
risk for CS
Requires fasting and morning appt.
Overt DM can be detected and treated and vascular disease assessment obtained during pregnancy, allows postpartum referral, negating need for further testing
Will allow a global data base and true epidemiology and prevalence determined
Treating lower glycemic thresholds may reduce risks for metabolic syndrome/T2DM later
Treating lower thresholds should reduce the risk of adverse outcomes

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
13
Japan Parts of India Germany (with modifications) China (with modifications) Italy Brazil (with modifications)
The American Diabetes Association WHO has reviewed HAPO data and other data and will
publish revised guidelines soon. NIH will hold a consensus conference October 29-31,
2012 and will make independent recommendations that may or may not be the same as IADPSG.
(Boyd Metzger, 2012)
Pre eclampsia/eclampsia HTN and worsening of HTN Urinary tract infections Polyhydramnios Preterm labor/birth Spontaneous abortion Cesarean section Operative delivery
Managing Preexisting Diabetes and Pregnancy, 2008
complication incidence cause Hypoglycemia Hypocalcemia Hypomagnesemia Polycythemia Cardiomyopathy Hyperbilirubinemia Respiratory Distress Syndrome (RDS) Stillbirth
10-25% 50% 33% 5-6% <1% 20-40% 2-6% 2.5-4%
Excessive neonatal insulin secretion Transient hypoparathyroidism Often secondary to hypocalcemia Intrauterine hypoxia Anabolic effect of hyperinsulinemia Increased hemolysis, ineffective erythropoiesis Decreased surfactant production with hyperinsulinemia Polyhydramnios, chronic fetal hypoxia or acidemia
Fraser RA, 2010; Ogata ES, 2008;Hawson JM, 2010;Girling J, 2010

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
14
Cesarean birth Excessive blood loss Infection Wound breakdown
Macrosomia HTN GDM Fetal death Birth defects-NTD Longer hospital
stays Miscarriage
Inability to monitor fetus
Difficult epidural or spinal anesthesia
Higher NICU admissions
Increased deep veinthrombosis
n=323, 1 hr. <130 PP, predicted 28% macrosomia (Institute control prior to 32 weeks) (DIEP, J Obstet Gynecol,164:1991)
1 hr. PP decreases risk of macrosomia from 42% preprandial to 12% (DeVenciana et al. N Engl J Med. 333:1995)
1 hr PP BG< 120 mg./dL eliminates macrosomia (Combs et al. Diabetes Care, 15; 1992)
1 hr. PP BG < 120 decreases risk of neonatal hypocalcemia (Demarini et al. Obstet Gynecol. 823; 1994)
Mean PP BG of <105 significantly correlated to abd. circumference (Paretti et al. Diabetes Care 24;2001)
Significant reduction in LGA and emergent CS in 1 hr. PP testing and pt. preference (Moses et al. Aust NZ J Obstet. Gynecol, 39; 1999)

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
15
Organization Capillary Blood Glucose (mg./dL)
ADA, 2010 Fasting 60-99 Peak Postprandial 1 h 100-129 Mean Daily BG <110 A1c <6.0%
AACE (2007) Fasting 60-90 Peak Postprandial 1 hr <120 Initiate Insulin >90 >120 post meals A1c <6.0%
ACOG, 2005 Fasting <95 Premeal <100 Postprandial 1 hr. <140 Postprandial 2 hr. <120 Mean Daily BG 100 A1c <6.0%

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
16
Individualized meal plan based on BMI, height , weight and gestational age
Consider cultural, ethnic, religious influences, schedule and finances
Carbohydrate content divided between meals and snacks 175 grams CHO, 28 gms fiber, 1.1 gm/kg/day
protein (Reader, DM, 2008) Non-nutritive sweeteners approved by FDA in
pregnancy Saccharin, aspartame (except in PKU), acesulfame K,
sucralose neotame-not always recommended Monitor weight gain and loss and tolerance of therapy
Prenatal vitamin with DHA
Calcium 1500 mg/day, folic acid 600mcg/day (dietary or supplements)
Avoid alcohol/smoking
Limit caffeine to 300mg/d, artificial sweeteners 1-2 portions/day
Avoid fish potentially high in mercury
Increase calories after 1st trimester by300kcal/day
Reader, Managing Preexisting Diabetes and Pregnancy, 2008
BMI IOM, 2009 Kiel et al, 2007
Cedergren, 2007
<18.6 28-40 lbs 9-22 lbs
18.6-24.9 25-35 lbs 5 to 22 lbs
>25-29 15-25 lbs <20 lbs
>30 11-20 lbs No more than 13 lbs
30-35 10-15 lbs
>35 0-9 lbs
>40 0-9 lbs wt. loss

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
17
May decrease maternal glucose levels decreasing need for insulin or amount of insulin required
Planned physical activity of 30 minutes daily unless contraindicated, well hydrated with HR less than 150 bpm
Arm exercise in GDM while seated for 10 minutes postmeal reduces BG
May decrease stress and anxiety Summary and Recommendations of Fifth International Workshop
Conference on GDM (2008)
Pregnancy Considerations Risks of moderate-intensity activity done by healthy
pregnant women very low Risks for low birth weight, preterm birth or early pregnancy
loss not increased May reduce risk of pregnancy complications; preeclampsia
and gestational diabetes
Key Guidelines 150 minutes (2 hrs./30 minutes) of moderate intensity
aerobic activity per week for women who are NOT already highly active
Pregnant women who habitually engage in vigorous-intensity aerobic activity may continue
www.health.gov/paguidelines
Avoid doing exercise lying on back after the first trimester
Avoid activities that increase the risk of falling or abdominal trauma Contact or collision sports Horseback riding, downhill
skiing, soccer, basketball

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
18
CONTRAINDICATIONS WARNINGS TO DISCONTINUE
Significant heart or lung dz.
Incompetent cervix Persistent bleeding Preterm labor (PTL) Multiple gestation-PTL Ruptured membranes Pregnancy induced
hypertension
Vaginal bleeding Dyspnea Headache Chest pain Decreased fetal
movement Amniotic fluid leaking Muscle weakness Preterm labor Calf pain or swelling
Day Events Monday (1) Ini3al visit, inser3on of the Con3nuous Glucose Monitoring
System (CGMS), and pedometer placement.
Tuesday (2) Fixed carbohydrate meal for lunch, 30 minutes res3ng, and either 30 minutes of walking on the treadmill or 30 minutes of TV.
Wednesday (3) No visit.
Thursday (4) Fixed carbohydrate meal for lunch, 30 minutes res3ng, and either 30 minutes of walking on the treadmill or 30 minutes of TV.
Friday (5) Final visit and removal of the CGMS
Dawn P. Coe1, Jo M. Kendrick2, Bobby Howard2, David R. Bassett Jr.1, FACSM, Dixie L. Thompson1, FACSM, Scott A. Conger1, and Jennifer D. White1
80 85 90 95
100 105 110 115 120 125 130
Pre-Tr
eatm
ent
Post-
Treatm
ent
2 Hou
rs
3 Hou
rs
4 Hou
rs
5 Hou
rs
6 Hou
rs
Glu
cose
Lev
els
(mg/
dL)
Postprandial Glucose Levels
Walk
Sedentary
Results
Figure 1. Postprandial glucose levels following walking and sedentary condi9ons
*
**
*p<0.001 **p<0.05
KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
19
Pharmacologic Intervention
Insulin only FDA approved treatment for diabetes in pregnancy
Glyburide-second generation sulfonylurea Insulin secretagogue Onset of action 4 hrs lasting 10 hrs. Low placental transfer
Metformin-biguanide
Decreases hepatic conversion of glycogen to glucose Improves peripheral insulin sensitivity Crosses placenta freely
KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
20
Lispro/Aspart, Humulin/Novolin N, Detemir category B
Glargine category C
Algorithm based on weight
Preconception 0.6U/kg/day First Trimester (6w) 0.7U/kg/day Second Trimester(16w) 0.8U/kg/day Third Trimester(26w) 0.9U/kg/day >150%ideal 1.5 to 2U/kg
Basal (50%) and bolus insulin (50%), evaluate BG
Adapted from Jovanovic and Peterson,1982.
Evaluate blood glucose every 1 to 2 weeks based on glycemic control
Serial ultrasound to assess growth after 26-28 weeks
Fetal kick counts at 28 weeks
Begin weekly to twice weekly fetal testing by electronic fetal monitor or ultrasound based on any co-morbidities and level of glycemic control
Deliver at 39 to 40 weeks

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
21
Macrosomia (>90percentile) > 4000 gms. (8# 13 oz) incidence-1.4--9% with good
control, 25-42% without normoglycemia (Langer,2004)
Organomegaly-heart, liver Fetal echo r/o hypertrophy with
impaired cardiac function which is associated with fetal death (Leslie 82: Sardesai 01)
excessive fat deposition (shoulders & trunk)
birth trauma-shoulder dystocia, fractured clavicles, brachial plexus injury, asphyxia, and other injuries
intrauterine growth restriction (IUGR) < 10th percentile carries
significant risk for neonatal death (Boulet 06)
incidence 20 %
associated with vasculopathy, HTN, placental insufficiency, decreased renal function, smoking
LONG TERM RISKS RISK REDUCTION
Obesity Insulin resistance Glucose intolerance T2dm GDM (females) HTN Other types of
cardiovascular disease
Parents should be educated regarding long term risks
Encourage breast feeding Encourage healthy diets
and active lifestyle Providers should monitor
growth and development of children

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
22
Consider 39-40 week delivery-well controlled, no comorbidities—earlier with amnio for FLM with worsening vascular disease, poor glycemic control, macrosomia
Continuous fetal heart rate monitoring
Maintain normoglycemia (70-100 mg./dL) to minimize risk of neonatal hypoglycemia Maternal bedside BG monitoring every 1-2 hrs Continuous infusion of insulin/and/or glucose as
indicated May use basal rate on insulin pump and bolus as
indicated
Conway & Catalano, 2008
Insulin resistance dramatically improves immediately after birth GDM resolves Insulin/oral medications require dosage decrease of 50% in
women with prepregnancy diabetes
Breast feeding Requires 500 additional calories Not all oral medications are safe Decreases insulin requirements in type 1 and 2 diabetes Decreases risk of development of type 2 diabetes and obesity in
offspring (Dabelea, 2007; Schaefer-Graf et al, 2006) Decreases risk of transmission of type 1 diabetes (Virtanen &
Knip, 2003)

KendrickJ_Gestational Diabetes: A Current Approach. Promoting Healthy Weight Colloquium, University of Tennessee, Knoxville
September 28, 2012
23
EDUCATION Risk of GDM subsequent pregnancy-30-84% (Kim, Berger &
Chamany, 2007) Lifetime risk of overt diabetes 50-60% (AACE, 2007; Kjos, 2007) Lifestyle modifications and metformin decreases the risk of
development of type 2 diabetes (Ratner et al, Diabetes Prevention Research Group, 2008)
Test every 1 to 3 years and prior to subsequent pregnancy (ADA, 2012)
Preconceptual counseling
75 gram 2 hr. glucose tolerance test 36% obtain f/u testing 32% of physicians order 75 gm Providing written requisition increases testing frequency (Kim,
2007)
Normoglycemia IFG and IGT Diabetes Mellitus FPG <100 FPG between 100-125
mg./dL FPG> 126 mg./dL
2 hr plasma glucose <140
2 hr. plasma glucose 140-199 mg./dL
2 hr. plasma glucose > 200 mg./dL Symptoms of diabetes mellitus and casual plasma glucose >200 mg./dL
Diagnosis must be confirmed on a subsequent day of any of the three methods in the absence of unequivocal hyperglycemia.