Embed Size (px)
Citation preview
Getting Started with Audiologic
RehabilitationAudiologic Rehabilitation for Children and Educational
AudiologySPA 6581 – Spring 2015
Lecture Date: 01/06/2015
Topics• Background• Review syllabus and course requirements • Audiology Scope of Practice regarding AR• Neurological Foundations of Listening and Talking • Getting started with Aural Habilitation• The Auditory System• Effects of Hearing Loss on Development of
Speech and Language
A Hybrid• Dually certified by ASHA as a SLP and an AuD• Specific clinical interests include: cochlear
implants, auditory verbal therapy, incorporating speech and audiology, investigating and demonstrating the habilitative aspect of audiology, interdisciplinary teams
• Positions held in speech and audiology: public school systems (elementary through high, total communication programs, oral communication programs), special education schools, group homes, residential facilities, home health, private practice, ALF and SNF, and cochlear implant teams.
Recommended Resource Texts
• Cole, E. B., & Flexer, C. (2007). Children with hearing loss: Developing listening and talking birth to six. San Diego, CA: Plural Publishing, Inc.
• Deconde Johnson, C., & Seaton, J. B. (2012). Educational
audiology handbook. (2nd ed.). Clifton Park, NY: Delmar Cengage Learning.
• Ling, D. (2002). Speech and the hearing-impaired child: Theory and practice. (2nd ed.). Washington, DC: Alexander Graham Bell Association for the Deaf and Hard of Hearing.
• Ling, D., & Ling, A. H. (1978, 1980, 1985). Aural habilitation: The foundations of verbal learning in hearing-impaired children. (3rd ed.). Washington, DC: AG Bell Association for the Deaf, Inc.
“The most debilitating consequence of onset of
hearing loss in childhood is its disruption to learning speech and language.”
-ASHA
What’s the difference?
Habilitation vs. Rehabilitation
Why does the differentiation matter?
How might it aid you?
Audiologic HabilitationAudiologic (Hearing) (Re)Habilitation is the process of
providing training and treatment to improve hearing for those who are hearing impaired.
or
Audiologic/Aural rehabilitation (AR) is an ecological, interactive process that facilitates one’s ability to
minimize or prevent the limitations and restrictions that auditory dysfunctions can impose on well-being and
communication, including interpersonal, psychosocial, educations, and vocational functioning.
AR Today• “…Client-centered rehabilitation model that
promotes successful adherence to treatment recommendations and professional accountability.”
• Each child and family should have an individualized aural (re)habilitation plan. o Who comes up with that plan?
• The scope of practice of AR has expanded such that not all aspects of AR are as likely to be addressed by either an audiologist or a speech-language pathologist as they were 20 years ago.
Routine Aspects of ARExpanded Range and Increased Complexity
• More Recent View: o Assessment measures
o Educational, behavioral, technological, and counseling intervention procedures
o Ongoing client-clinician interaction• Evaluate and monitor
progress
• AR is NOT just limited to: o Speechreading
o Auditory training
o Hearing aid orientation
o 30 day trial period
Focus of AR Services• Training in auditory perception• Improving speech• Developing language• Managing Communication
o Pragmatics
• Managing hearing aids and assistive listening deviceso Making the best use of personal amplification deviceso Exploring assistive deviceso Adjusting to hearing loss
• May incorporate visual cues
Services Depend On…Chronological age
Age of onset of hearing loss
Age at which the hearing loss was diagnosed
Severity/extent of the hearing loss
Type of hearing loss
“Hearing age”
Communication Mode
Others?
Service ModelsIndividualized
Small groups
Combination of both
Therapist/patient dynamic
Therapist/parent/patient dynamic
Members of AR Team
Other Potential Members:• Office Staff• Administrative
Support• Social Worker• Group Home
Managers• Pediatrician• Psychologist• Others?
Primary Members:• The PATIENT and the
FAMILY/Caregivers• Otolaryngologist (ENT)• Audiologist• Speech-Language Pathologi
st• Listening and Spoken
Language Specialist• Hearing Therapist• Early Interventionist• Educators
o Itineranto Mainstreamo Teacher of the Deaf
Quote from the 70sMy how far we’ve come! …or have we?
“People who have all the skills required for work in parent-centered habilitation are rare. Most
specialist teachers of hearing-impaired children have too little knowledge of speech science,
audiology, and counseling; most audiologists have insufficient background in child development,
speech science, language acquisition and education; and most speech pathologists have few, if any, skills relating to audiology, education, and
the speech acquisition problems of hearing-impaired children.”
(Ling & Ling, 1978)
Is Coursework Enough?
The interdisciplinary nature of AR, particularly in the area of pediatrics where speech and language intervention is crucial, supports the need for additional training/coursework beyond the current minimal requirements for certification for either audiology or speech-language pathology!
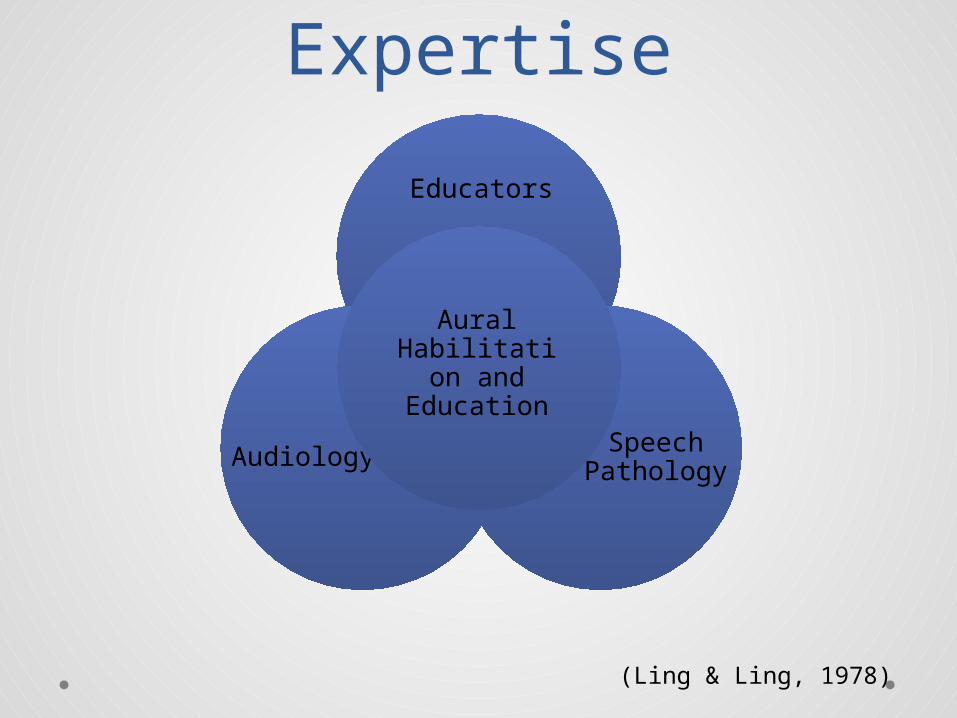
Professional Expertise
Educators
Speech PathologyAudiology
Aural Habilitation
and Education
(Ling & Ling, 1978)
Roles of Professionals• Audiologists and Speech-Language Pathologists
roles may be: o Complementaryo Interrelatedo Overlapping
• Both Audiologists and Speech-Language Pathologists bring specific knowledge and skills to the ongoing facilitative process of AR.
Basic Areas of Knowledge and Skills:
Audiologists• Basic Communication
Processeso Anatomic and physiologic basis
for normal development and use of speech, language, and hearing
o Physical bases and processes of the production and perception of speech and hearing
o Linguistic and psycholinguistics variables related to the normal development and use of speech, language and hearing
o Dynamics of interpersonal skills, communication effectiveness, and group theory
• General Knowledgeo General psychologyo Human growth and
developmento Psychosocial behavioro Cultural and linguistic
diversityo Biological, physical, and social
scienceso Mathematicso Qualitative and quantitative
research methodologies
Specific Areas of Knowledge and Skills: Audiologists
• Auditory System Function and Disorders• Developmental Status, Cognition, and Sensory
Perception• Audiologic Assessment Procedures• Speech and Language Assessment Procedures• Evaluation and Management of Devices and Technologies for
Individuals with Hearing Impairment• Effects of Hearing Impairment on Functional
Communication• Effects of Hearing Impairment on Psychosocial,
Educational, and Occupational Functioning• AR Case Management• Interdisciplinary Collaboration and Public Advocacy• Hearing Conservation/Acoustic Environments
Basic Areas of Knowledge and Skills:
SLPs• Basic Communication
Processes:o Anatomic and physiologic
bases for the normal development and use of speech, language, and hearing
o Physical bases and processes of the production and perception of speech and hearing
o Linguistic and psycholinguistic variables related to the normal development and use of speech, language, and hearing
o Dynamics of interpersonal skills, communication effectiveness, and group theory
• General Knowledge:o General psychologyo Human growth and
developmento Psychosocial behavioro Cultural and linguistic
diversityo Biological, physical, and social
scienceso Mathematicso Qualitative and quantitative
research methodologies
Specific Areas of Knowledge and Skills: SLPs
• Auditory System Function and Disorders• Developmental Status, Cognition, and Sensory Perception• Audiologic Assessment Procedures• Assessment of Communication Performance• Devices and Technologies for Individuals with
Hearing Loss• Effects of Hearing Loss on Psychosocial,
Educational, and Vocational Functioning• Intervention and Case Management• Interdisciplinary Collaboration and Public Advocacy• Acoustic Environments
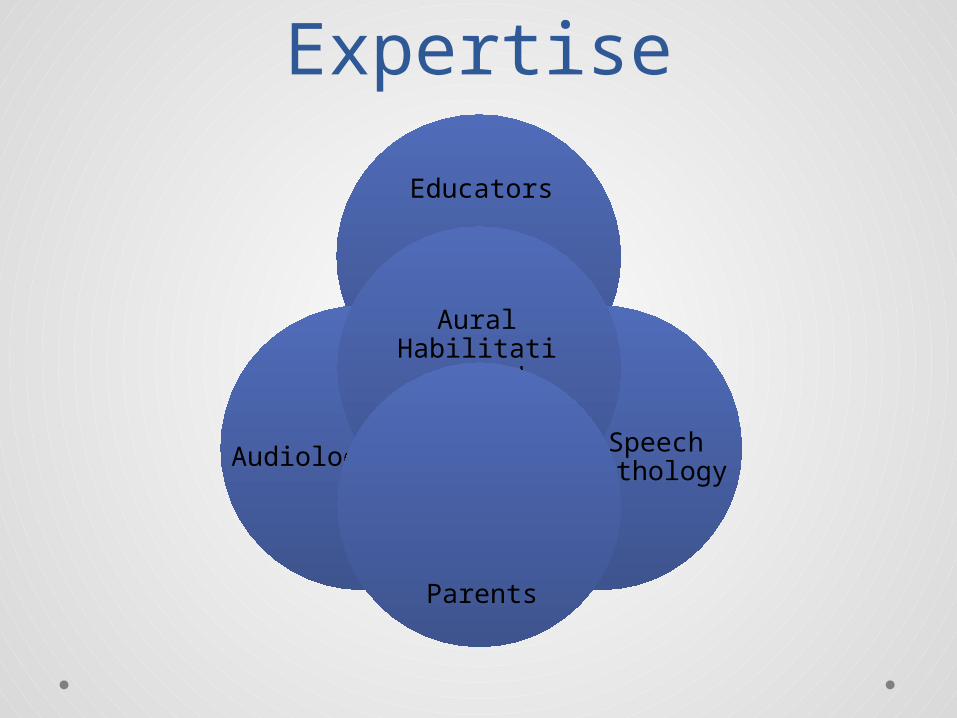
Professional Expertise
Educators
Speech PathologyAudiology
Aural Habilitation
and Education
Parents
Scope of Practice• American Academy of Audiology• American Speech-Language-Hearing Association
• Who is responsible for providing, facilitating, maintaining, and evaluating aural habilitation services? o Teacherso Clinicians
• Audiologists, Speech-Language Pathologists, Listening and Spoken Language Specialists
o Educational Administratorso Parents
• What other services are within the scope of practice of audiology? o Did you know… “Audiologists may perform speech or language screening, or other
screening measures, for the purpose of initial identification and referral of persons with other communication disorders.” AAA 2004(American Academy of Audiology,
2004)(American Speech-Language-Hearing Association, 2004)
Scope of Practice: How prepared are we?• Did you know…
o “Audiologists may perform speech or language screening, or other screening measures, for the purpose of initial identification and referral of persons with other communication disorders.”
o “The audiologist is the professional who provides the full range of audiologic treatment services for persons with impairment of hearing…”
o “The audiologist provides assessment, counseling, and ALL aspects of audiologic treatment including auditory training, rehabilitation…”
o “The audiologist…is a source of information for family members, other professionals, and the general public. Counseling regarding hearing loss, the use of amplification systems, and strategies for improving speech recognition is within the expertise of the audiologist.”
o “The audiologist’s scope includes participation in the development of an Individual Education Plan (IEP) for school-age children or an Individual Family Service Plan (IFSP) for children from birth to 36 months old.”
(American Academy of Audiology, 2004)(American Speech-Language-Hearing Association, 2004)
• A few more…o The audiologist provides counseling regarding the effects of hearing loss on
communication and psycho-social status in personal, social, and vocational arenas.
o The scope of practice for audiologists includes screening for speech, orofacial myofunctional disorders, language, cognitive communication disorders, and/or preferred communication modalities that may affect education, health, development, or communication, and may result in recommendations for rescreening or comprehensive speech-language pathology assessment or in referral for other examinations or services.
o The audiologist is responsible for the provision of comprehensive audiologic rehabilitation services, including management procedures for speech and language habilitation and/or rehabilitation for persons with hearing loss or other auditory dysfunction, including but not exclusive to speechreading, auditory training, communication strategies, manual communication, and counseling for psychosocial adjustment for persons with hearing loss or other auditory dysfunction and their families/caregivers(American Academy of Audiology,
2004)(American Speech-Language-Hearing Association, 2004)
“Most hearing-impaired children can learn to speak and understand spoken language if they are given adequate
opportunity to do so. Adequate opportunity can be provided only if
those concerned with the child’s care – parents, teachers, clinicians, and
administrators – are aware of, and exploit, the conditions that contribute
to verbal learning.”
(Ling & Ling, 1978)
Neurological Foundations:Listening and
Talking
Amazing Brains!• Auditory experience in utero and infants with
normal hearing• “We hear with the brain – the ears are just a way
in.” • How do auditory pathways mature?• Neuroplasticity• Secondary Auditory Association areas in the
cortex• Developmental Synchrony• Invisible Acoustic Filter

Typical Infants• At birth, infants prefer their mother’s speech and
they even prefer songs and stories heard before birth.
• Infants are born with 20 weeks of listening experience.o Cochleae are formed and functional by the 20th week of gestation
• So why do we care so much about early identification of hearing loss? o Experience with sound is available to the infant in uteroo Newborns with hearing loss have already missed what?
• 20 weeks of listening!
“We have time, the baby is only 6 months
old…”• What do you think about that statement?• In the first 6 months of life, babies can discriminate many speech
sounds, even those not heard in their home-spoken language(s). • By the end of the first year, there is a functional reorganization of
the brain to distinguish phonemes specific to language(s) heard daily.
• This neural reorganization improves and tunes the phonetic categories required for the infant’s language and attenuates those phonemic distinctions not required for the infant’s mother tongue.
• Infants use their phonetic categories as the foundation for learning new words. Phonetic distinctions guide new word learning by 17 months of age.
• What does that mean for listening experience in infancy? o It is critical for the development of both speech and language in young children, and a strong
language base is essential for reading.
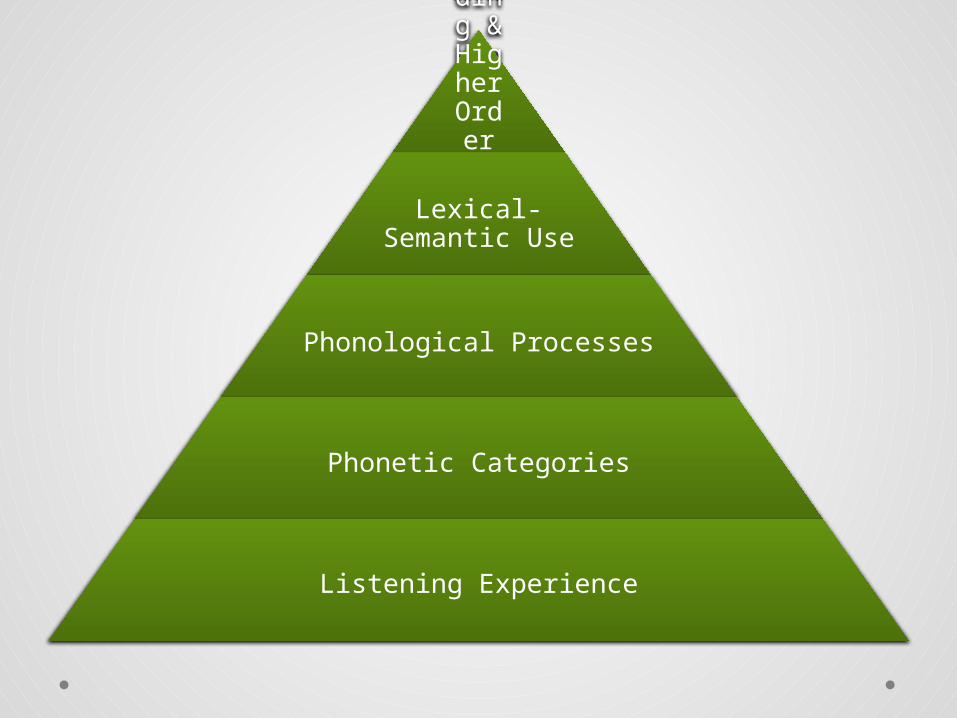
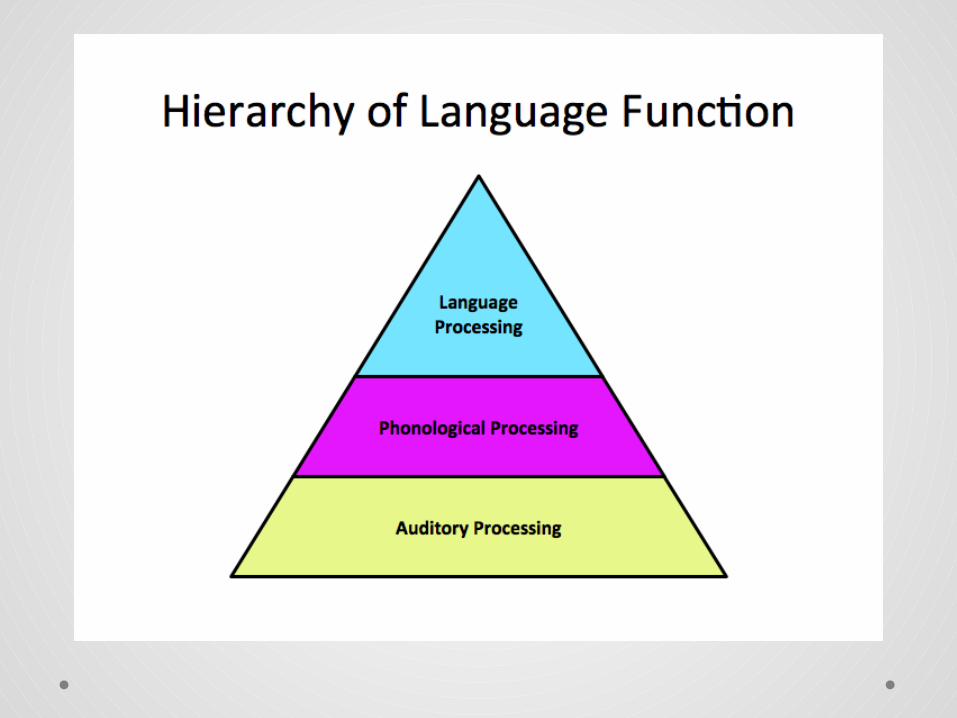
Reading & Higher Order
Language Use
Lexical-Semantic Use
Phonological Processes
Phonetic Categories
Listening Experience
32
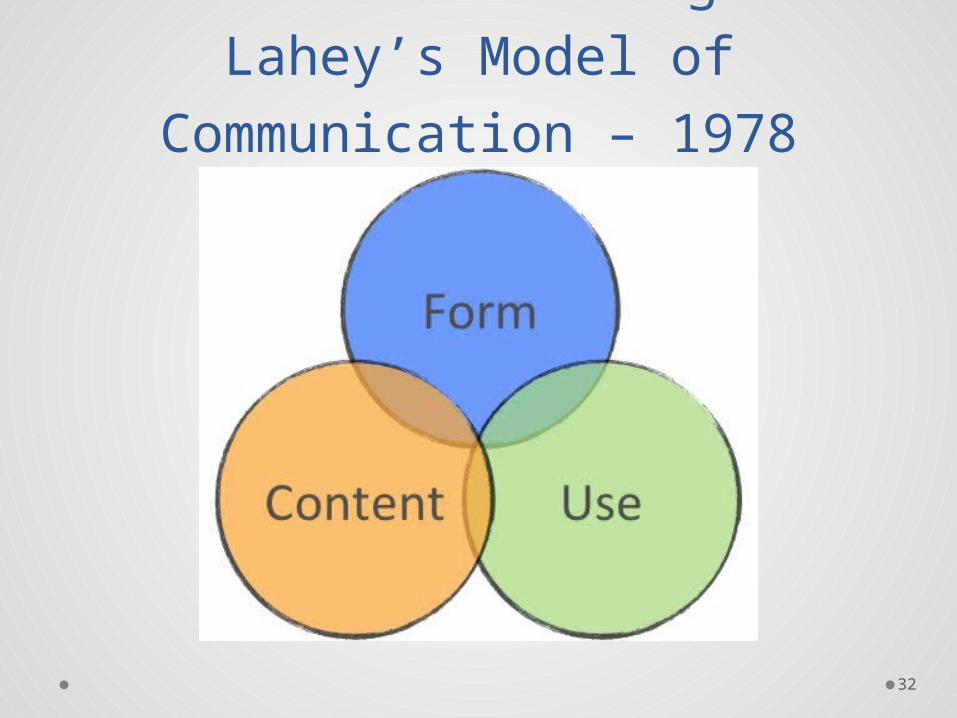
Lois Bloom and Margaret Lahey’s Model of
Communication – 1978
Model of Language• Bloom and Lahey (1978)
o Three aspects of language were identified: • language form (syntax, morphology, and
phonology)• language content (semantics)• language use (pragmatics)
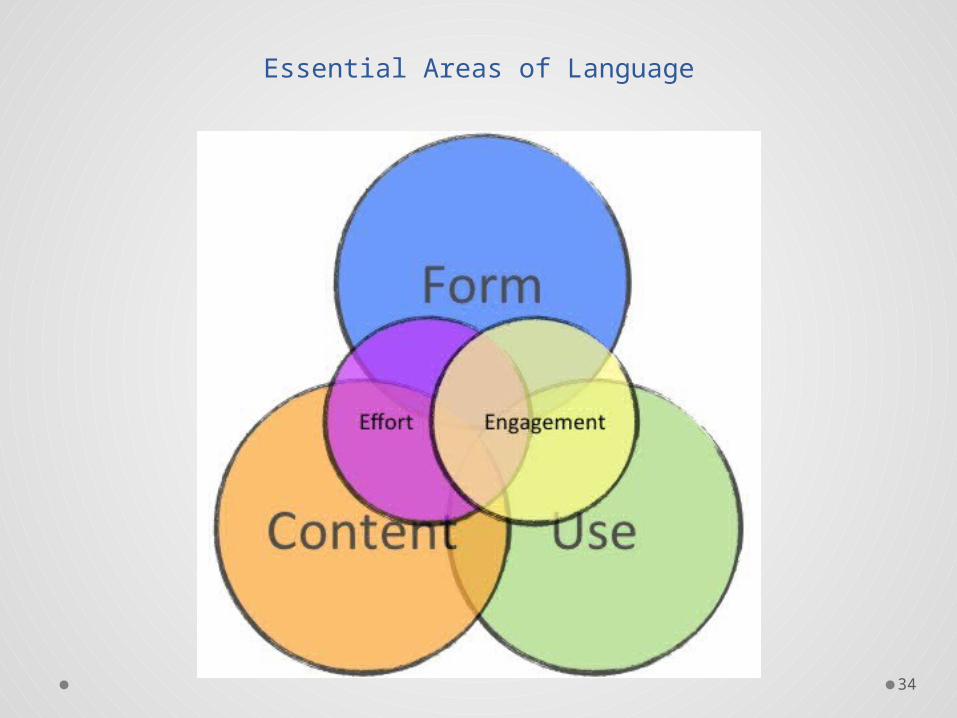
• Lois Bloom and Erin Tinker added the following as factors influencing language development:
• effort• engagement
34
Essential Areas of Language
How Much is Necessary?
• In order to obtain adequate language development, how much listening experience is necessary?
• The first three years of experience put in place a trajectory of vocabulary growth and the foundations of analytic and symbolic competencies that will make a lasting difference to how children perform in later years.
• ALL infants and children require a great deal of listening experience in order to develop age appropriate auditory and spoken language skills.
Importance of Early Identification
• Newborn infant screening programs and Newer technology
o These both allow access to critical auditory brain centers during times of maximum neuroplasticity
o Auditory language enrichment can be provided during critical periods of maximum brain neural plasticity – the first few years of life (Sharma, Dorman, & Spahr, 2002; Sharma et al., 2004; Sharma, Dorman, & Kral, 2005).
Auditory Neural Development
• “We hear with the brain – the ears are just a way in.”
• How do auditory pathways mature?o Full maturation of central auditory pathways is a precondition for the normal development
of speech and language skills in children, whether or not they have a hearing loss
• Neuroplasticityo Brain’s availability and malleability to grow, develop, and alter its structure as a function of
external stimulation. o Why is neuroplasticity important?
• Today’s babies and young children who are born deaf or hard of hearing have incredible possibilities for achieving higher levels of spoken language, reading skills, and academic competencies than were available to most children in previous generations.
• Secondary Auditory Association Areaso Cortical levelo Not fully developed until a child is about 15 years old
• Limited time period of optimal neural plasticity (greatest during the first 3 ½ years of life)
• Studies in brain development show that sensory stimulation of the auditory centers of the brain is critically important, and influences the actual organization of auditory brain pathways.
• Neural imaging has shown that the primary and secondary auditory areas are most active when a child listens and when a child reads.
• Phonological or phonemic awareness, which is the explicit awareness of the speech sound structure of language units, forms the basis for the development of literacy skills.
Rapid Development in Infants
• What is required to keep up with the rapid brain development in infants? o PROMPT interventiono …remember…not just identification, but INTERVENTION
• Early amplification or implantation stimulates a brain that is in the initial process of organizing itself, and is therefore more receptive to auditory input, resulting in greater auditory capacity. o However, this only provides the access to sound…
Access, Access, Access• Access will allow for experiences, which will allow for
“programming” of those critical and powerful auditory centers of the brain with acoustic detail and will expand children’s abilities to listen and learn spoken language.
• Early and ongoing intervention is essential. NOT JUST IDENTIFICATION. That is just the first step!
• Important neural deficits have been identified in the higher auditory centers of the brain due to prolonged lack of auditory stimulation.
• The auditory context is directly involved in speech perception and language processing in humans.
Neural Maturation• In order for auditory pathways to mature,
acoustic stimulation must occur early and often because normal maturation of central auditory pathways is a precondition for the normal development of speech and language skills in children.
• Audiologists are critical!o Fitting personal devices which allow for accesso Fitting these devices appropriatelyo Direct, repetitive auditory skills instruction as part of an effective
family-based early intervention program is criticalo EXTRA auditory stimulation is necessary
“A brain can only organize itself around
the sensory stimulation that it receives.”
Impact of the Absence of Sound
• The brain reorganizes itself to receive input from other senses, primarily vision. o Cross-Model Reorganization
• This process actually reduces auditory neural capacity.
We can’t just stop at access!
• Hearing vs. Listening
• “We hear with the brain – the ears are just a way in.”
• Hearing is acoustic access to the brain. o Improves the signal-to-noise ratio by managing the environment and
utilizing hearing technology
• Listening is attending to acoustic events with intentionality.
Intervention Models• Developmental
• Remedialo Not in harmony with normal developmento We need to undo the neural organization that the brain has initially
acquired and reorganize the brain around different stimuli. o This model takes longer and has reduced outcomes. Why?
• The child is now neurologically and psychosocially out of synchrony with the typical developmental process.
Cumulative Practice• What is it?
o Each practice opportunity builds on the last one.
• Mastery of any developmental skill depends on cumulative practice.
• Why do we care about this?o The more delayed the age of acquisition of a skill, the farther behind
children are in the amount of cumulative practice they have had to perfect that skill.
• Another way to think of it…Cumulative Auditory Practice.
Cumulative Practice• Other developmental skills (walking, crawling)
o How do they learn these skills? They practice.
• Delayed auditory development leads to delayed language skills which will necessitate using a remedial rather than a developmental paradigm.
Developmental Synchrony
• Humans are programmed to develop specific skills during certain periods of development.
• If those skills can be triggered at the intended time, we will be operating under a developmental and not a remedial program. o That is…skills mastered as close as possible to the time that a child is
biologically intended to do so result in developmental synchrony
• Intervention later in life is out of harmony with the typical developmental process.
Normal Speech and Language
Development
Normal Development• Based on the age by which most monolingual
speaking children will accomplish identified milestones
• All items in a category are not typically mastered until reaching the upper age in the age ranges.
• Why important? o Not just so you know what abnormal development is…o To aid in counseling a family regarding progress
• Other than… “Little Johnny is doing good!”

Normal DevelopmentHearing, Understanding and Talking
Birth to 3 months
4-6 months
7 months to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
4 years to 5 years
(American Speech-Language-Hearing Association, 2012)

Audition
Speech
Language
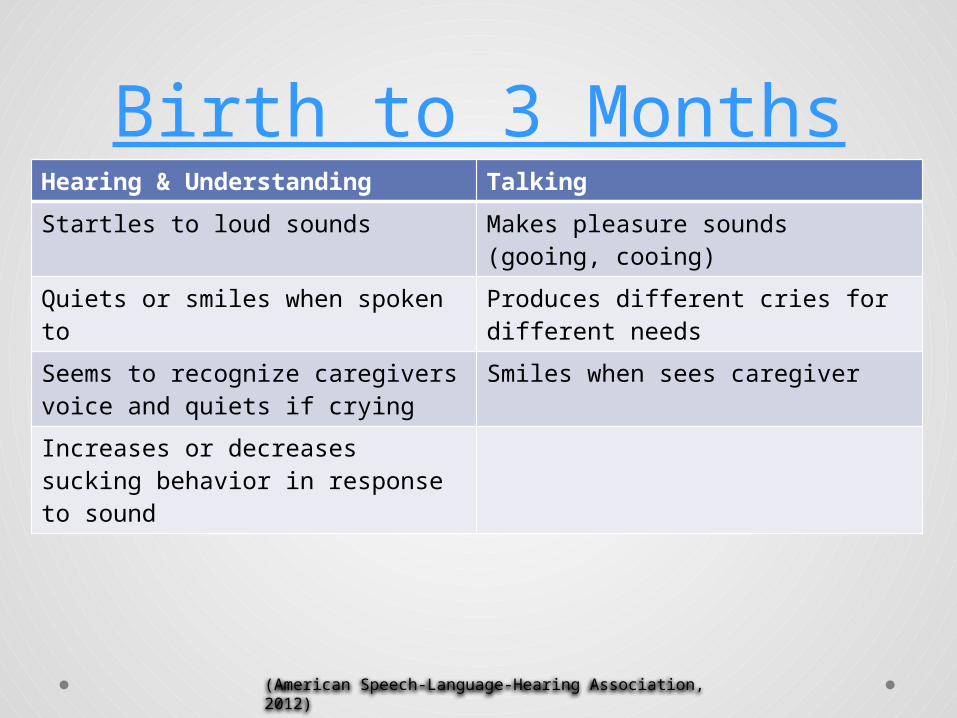
Birth to 3 MonthsHearing & Understanding Talking
Startles to loud sounds Makes pleasure sounds (gooing, cooing)
Quiets or smiles when spoken to Produces different cries for different needs
Seems to recognize caregivers voice and quiets if crying
Smiles when sees caregiver
Increases or decreases sucking behavior in response to sound
(American Speech-Language-Hearing Association, 2012)
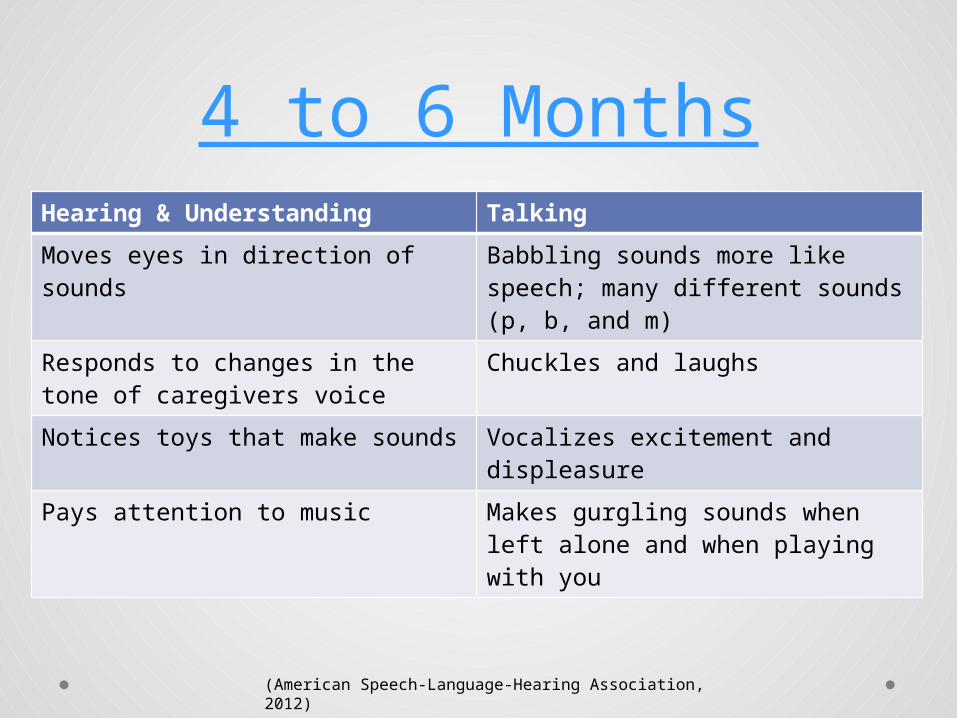
4 to 6 MonthsHearing & Understanding Talking
Moves eyes in direction of sounds Babbling sounds more like speech; many different sounds (p, b, and m)
Responds to changes in the tone of caregivers voice
Chuckles and laughs
Notices toys that make sounds Vocalizes excitement and displeasure
Pays attention to music Makes gurgling sounds when left alone and when playing with you
(American Speech-Language-Hearing Association, 2012)
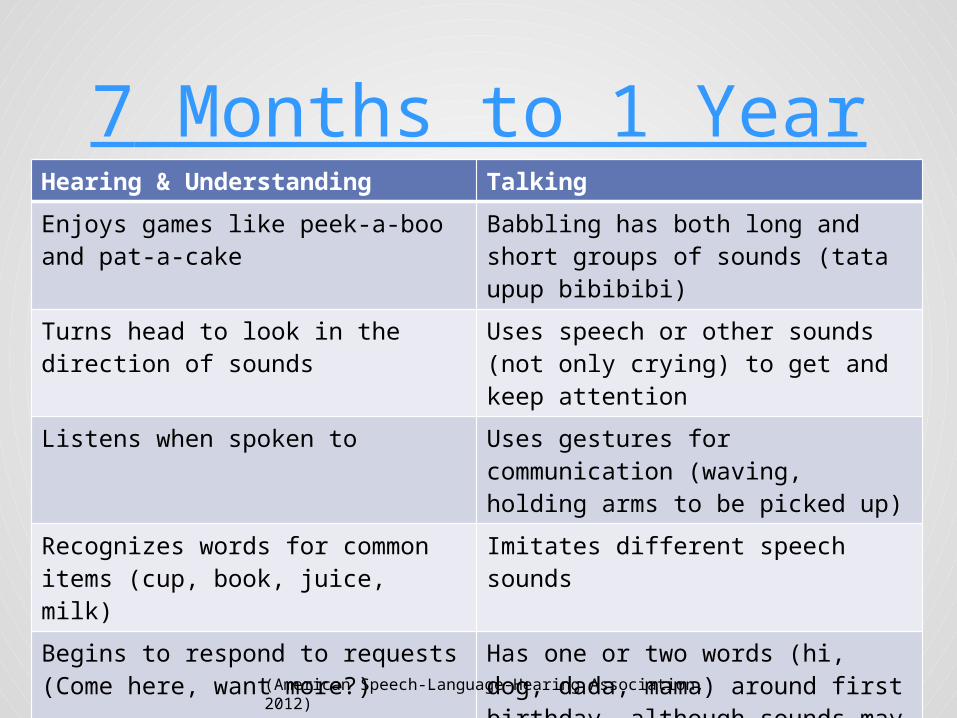
7 Months to 1 YearHearing & Understanding Talking
Enjoys games like peek-a-boo and pat-a-cake
Babbling has both long and short groups of sounds (tata upup bibibibi)
Turns head to look in the direction of sounds
Uses speech or other sounds (not only crying) to get and keep attention
Listens when spoken to Uses gestures for communication (waving, holding arms to be picked up)
Recognizes words for common items (cup, book, juice, milk)
Imitates different speech sounds
Begins to respond to requests (Come here, want more?)
Has one or two words (hi, dog, dada, mama) around first birthday, although sounds may not be clear
(American Speech-Language-Hearing Association, 2012)
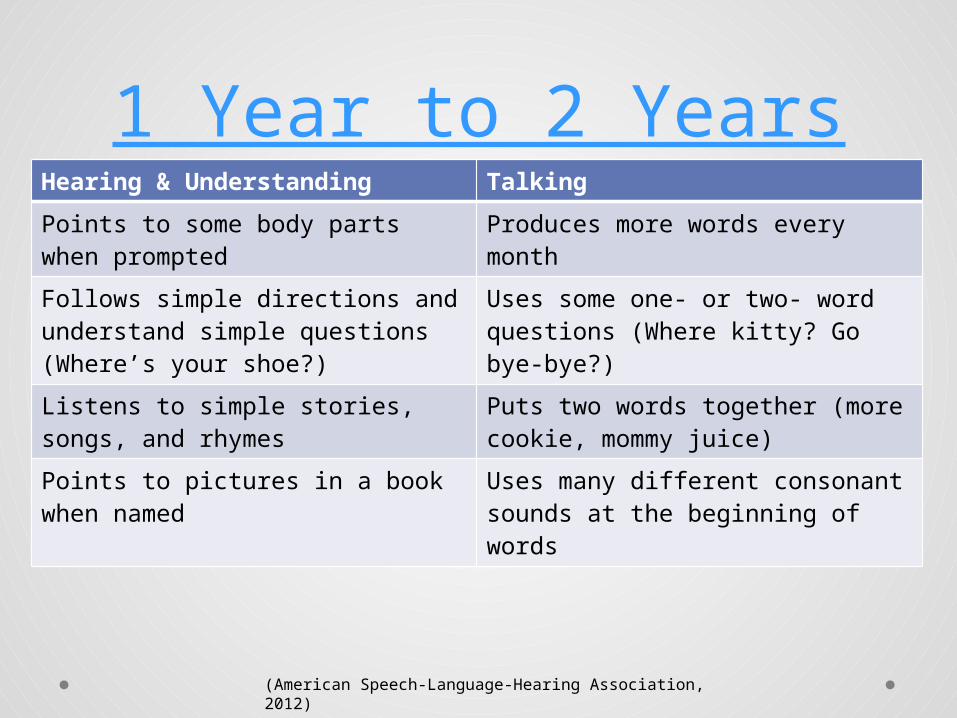
1 Year to 2 YearsHearing & Understanding Talking
Points to some body parts when prompted
Produces more words every month
Follows simple directions and understand simple questions (Where’s your shoe?)
Uses some one- or two- word questions (Where kitty? Go bye-bye?)
Listens to simple stories, songs, and rhymes
Puts two words together (more cookie, mommy juice)
Points to pictures in a book when named
Uses many different consonant sounds at the beginning of words
(American Speech-Language-Hearing Association, 2012)
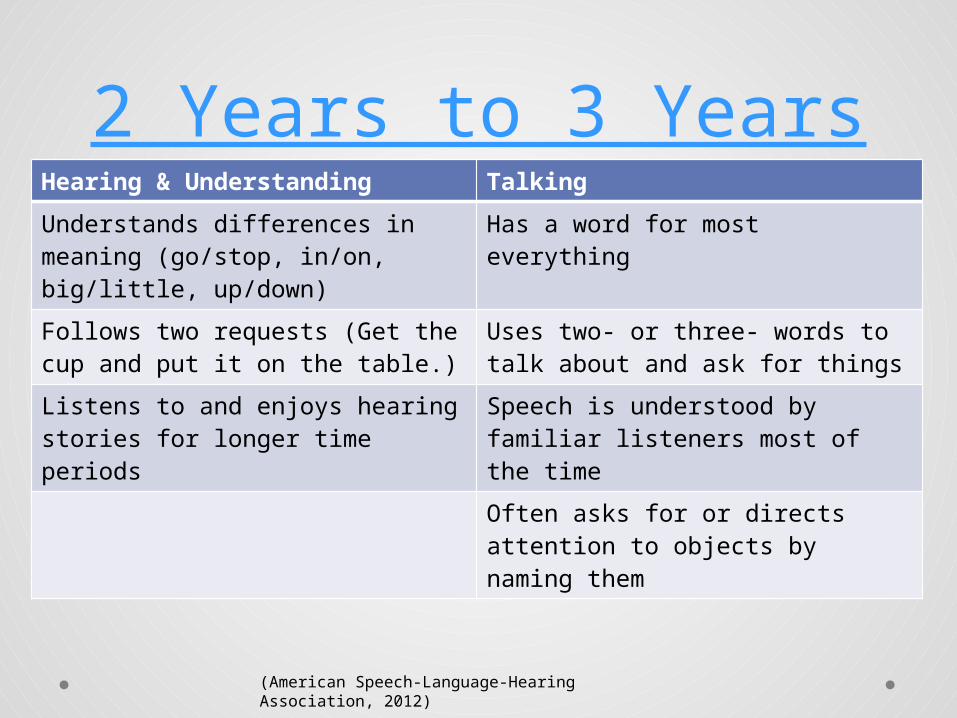
2 Years to 3 YearsHearing & Understanding Talking
Understands differences in meaning (go/stop, in/on, big/little, up/down)
Has a word for most everything
Follows two requests (Get the cup and put it on the table.)
Uses two- or three- words to talk about and ask for things
Listens to and enjoys hearing stories for longer time periods
Speech is understood by familiar listeners most of the time
Often asks for or directs attention to objects by naming them
(American Speech-Language-Hearing Association, 2012)
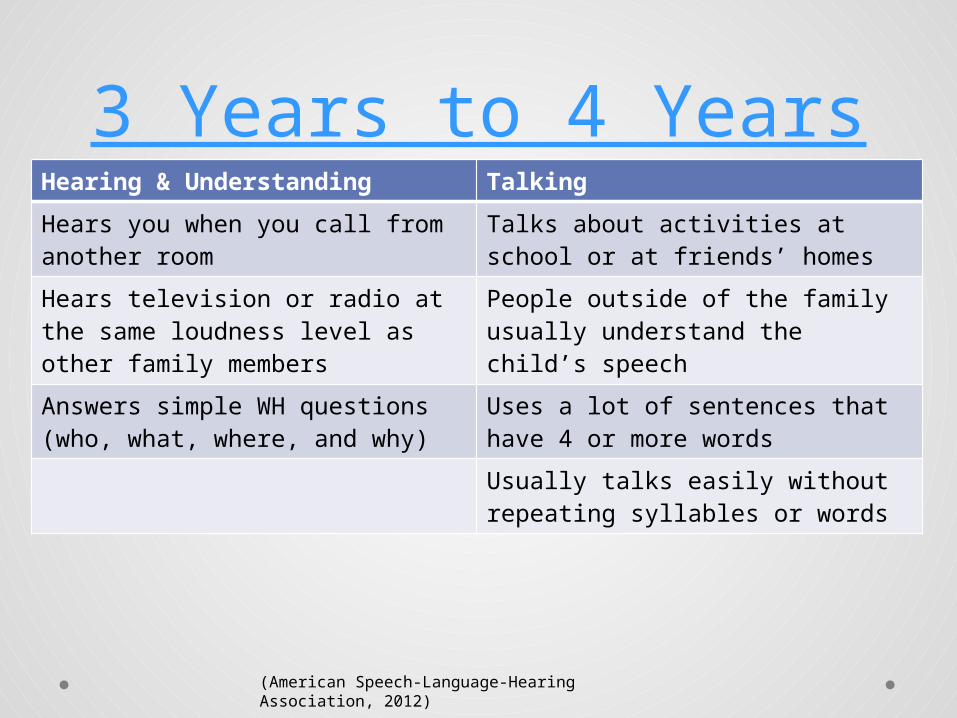
3 Years to 4 YearsHearing & Understanding Talking
Hears you when you call from another room
Talks about activities at school or at friends’ homes
Hears television or radio at the same loudness level as other family members
People outside of the family usually understand the child’s speech
Answers simple WH questions (who, what, where, and why)
Uses a lot of sentences that have 4 or more words
Usually talks easily without repeating syllables or words
(American Speech-Language-Hearing Association, 2012)
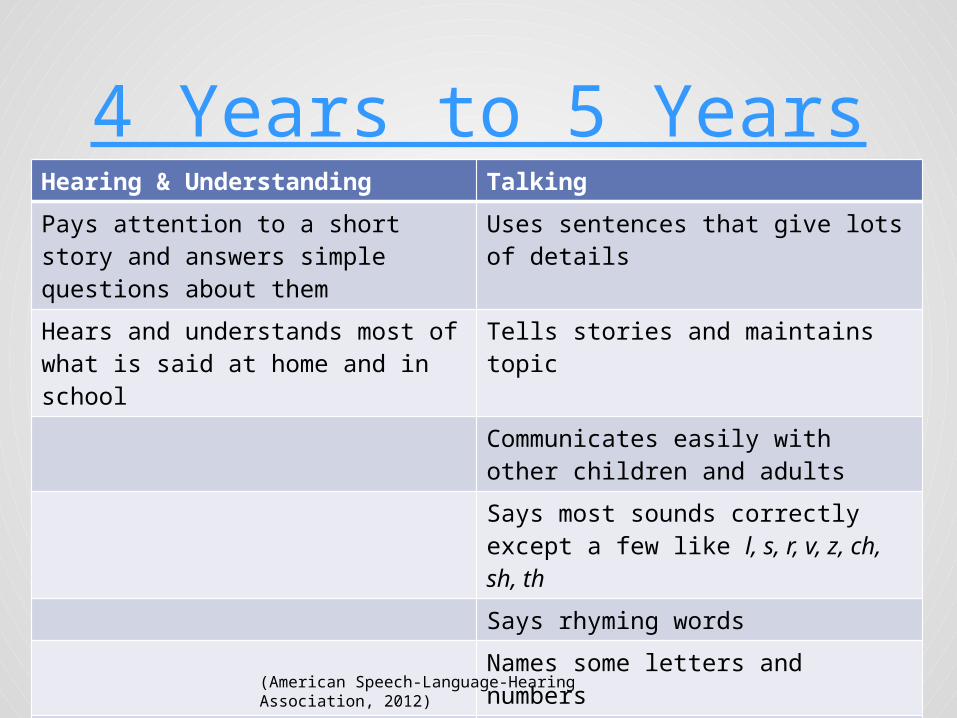
4 Years to 5 YearsHearing & Understanding Talking
Pays attention to a short story and answers simple questions about them
Uses sentences that give lots of details
Hears and understands most of what is said at home and in school
Tells stories and maintains topic
Communicates easily with other children and adults
Says most sounds correctly except a few like l, s, r, v, z, ch, sh, th
Says rhyming words
Names some letters and numbers
Uses the same grammar as the rest of the family
(American Speech-Language-Hearing Association, 2012)
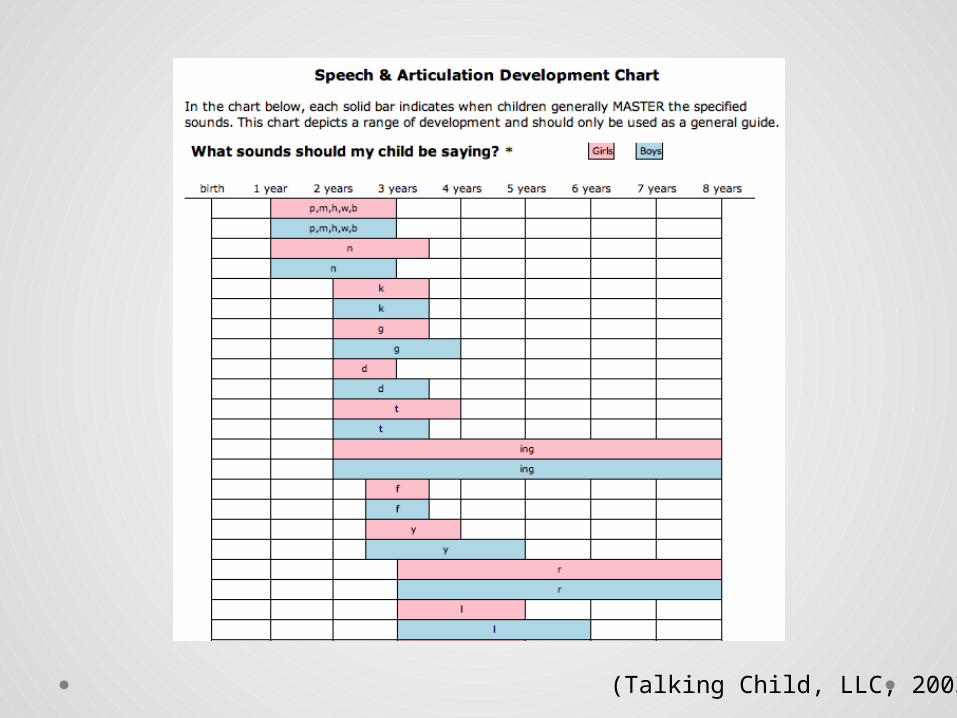
(Talking Child, LLC, 2003)
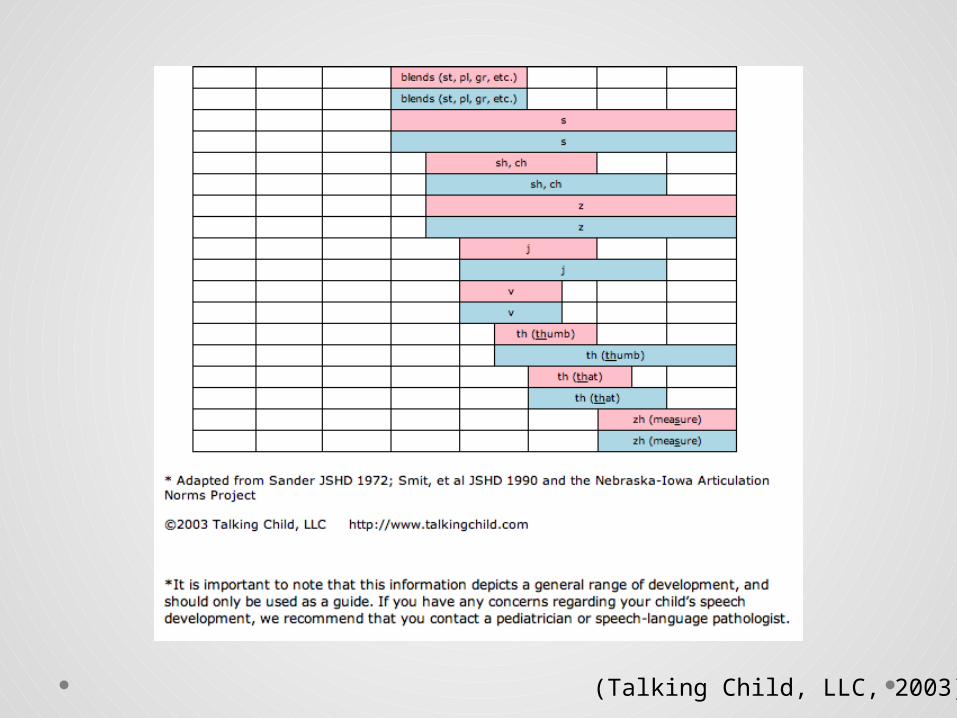
(Talking Child, LLC, 2003)
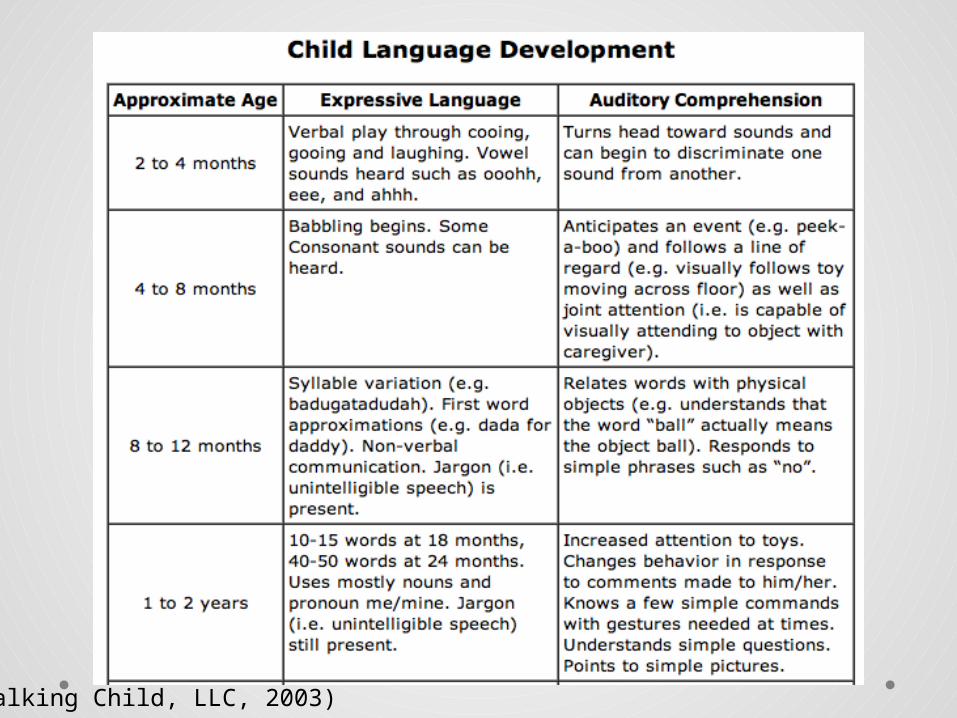
(Talking Child, LLC, 2003)
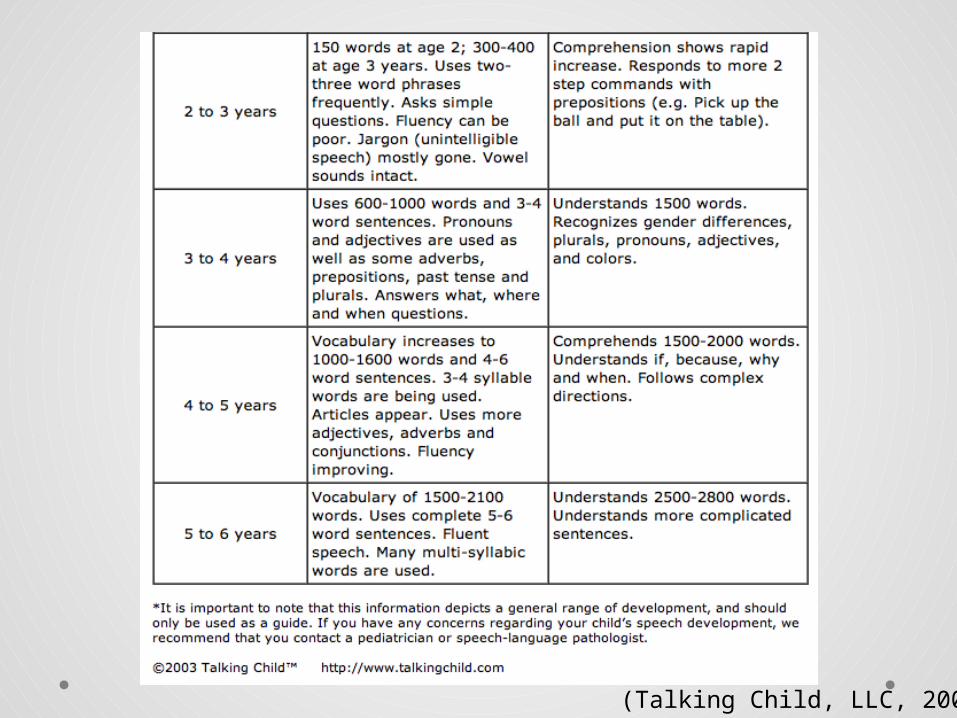
(Talking Child, LLC, 2003)
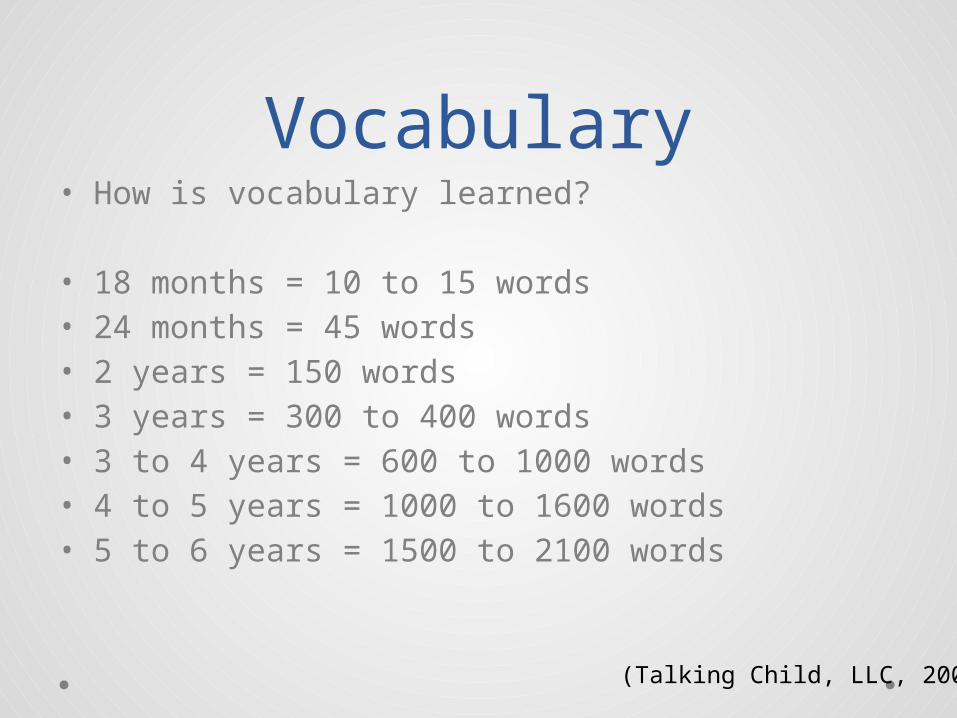
Vocabulary• How is vocabulary learned?
• 18 months = 10 to 15 words• 24 months = 45 words• 2 years = 150 words• 3 years = 300 to 400 words• 3 to 4 years = 600 to 1000 words• 4 to 5 years = 1000 to 1600 words• 5 to 6 years = 1500 to 2100 words
(Talking Child, LLC, 2003)
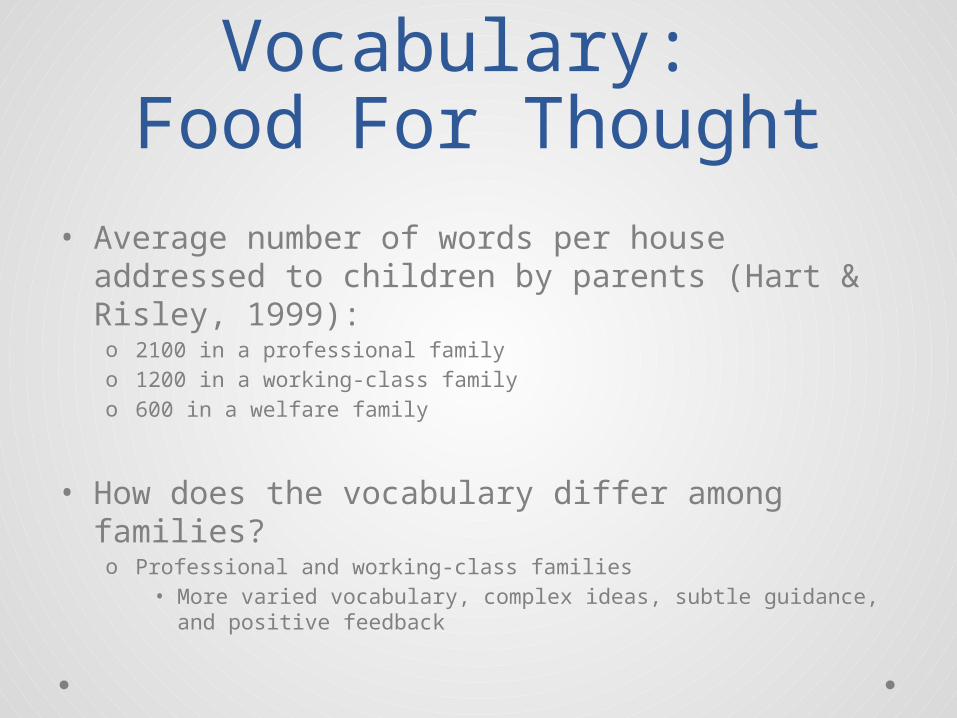
Vocabulary: Food For Thought
• Average number of words per house addressed to children by parents (Hart & Risley, 1999): o 2100 in a professional familyo 1200 in a working-class familyo 600 in a welfare family
• How does the vocabulary differ among families? o Professional and working-class families
• More varied vocabulary, complex ideas, subtle guidance, and positive feedback
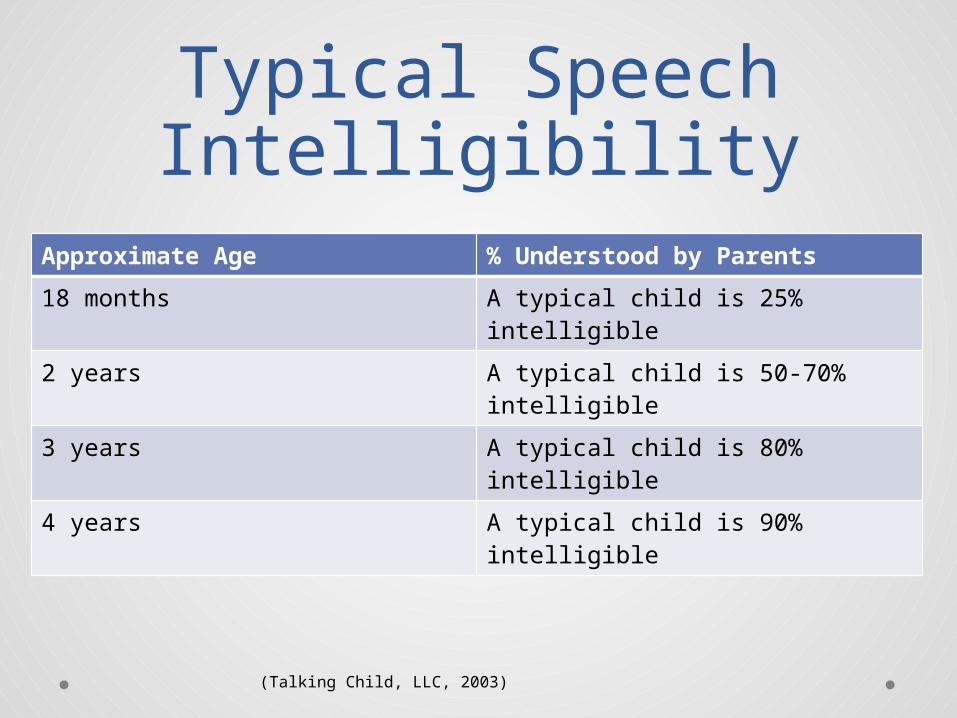
Typical Speech Intelligibility
Approximate Age % Understood by Parents
18 months A typical child is 25% intelligible
2 years A typical child is 50-70% intelligible
3 years A typical child is 80% intelligible
4 years A typical child is 90% intelligible
(Talking Child, LLC, 2003)
“The Invisible Acoustic Filter Effect”
• Hearing loss
• This filter, “distorts, smears, or eliminates incoming sounds, especially sounds from a distance – even a short distance.”
• Hearing is not an isolated activity. Everything else is built upon hearing
• Hearing loss itself is invisible and can be easily ignored or underestimated. o Only the negative effects of hearing loss are visible. o Name some.
“The earlier and more efficiently we can allow a child access to meaningful sound with subsequent direction of the child’s attention to sound, the better opportunity that child will have to develop spoken language, literacy, and academic skills.”
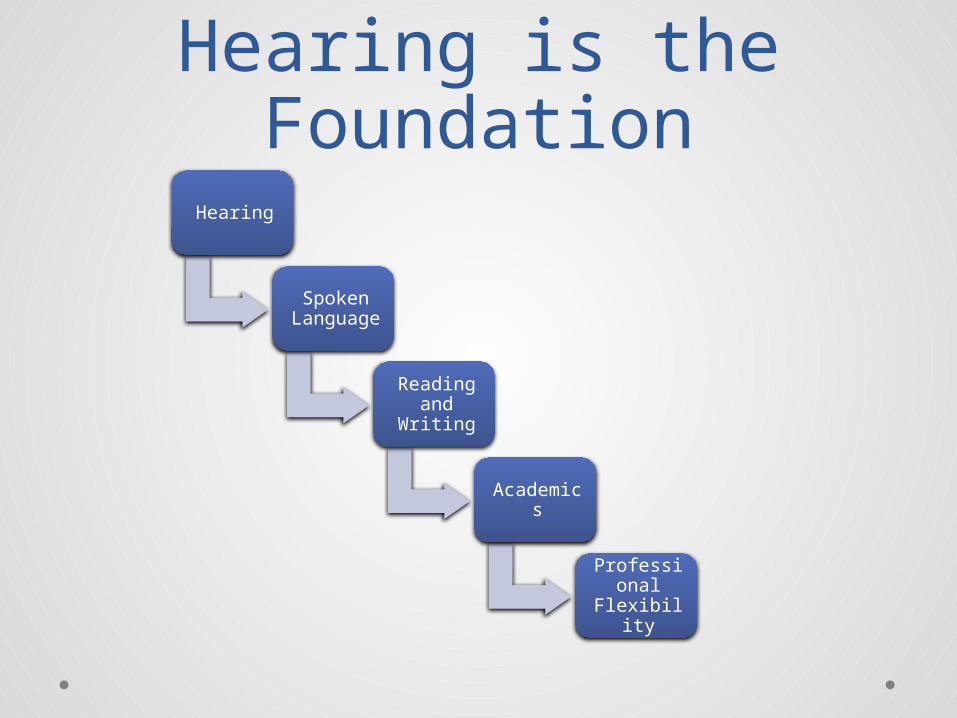
Hearing is the Foundation
Hearing
Spoken Language
Reading and
Writing
Academics
Professional
Flexibility
“What is your vision for your child?”
• Every parent has a vision for their child…even if they haven’t vocalized it yet.
• Why is this important?
• 95% of children with hearing loss are born into hearing and speaking families.
• What will it take to reach that vision the parent has for their child?
Developing Listening and Talking: What it
Takes!• Early identification and intervention • Vigilant and ongoing audiologic management• Immediate and consistent auditory brain access via
technology• Guidance from a professional who is highly
qualified in the development of listening and speaking, through techniques of parent coaching
• Following the professional’s coaching with daily and ongoing formal and informal auditory, language, cognitive, and literacy enrichment.
• Integration and use of auditory strategies into all-day, everyday interactions with the child
“How to Grow Your Baby’s Brain”
• 8. Read aloud• 9. Sing and read
nursery rhymes• 10. Name objects• 11. Describe: sound,
look, and feel• 12. Prepositions• 13. Similar and
Different• 14. Describe sequences• 15. Familiar stories
• 1. Quiet and close• 2. Consistent use of
technology• 3. Device checks and
troubleshooting• 4. FM system• 5. Focus on listening• 6. Joint focus of
attention• 7. Clear speech and
sentences
It’s Not Just About Speech and Language!Hearing Functions• Unconscious Function
o Most primitive function of hearingo Carries auditory background and sounds that serve to identify a
locationo Own biological sounds
• Signal Warning Functiono Monitoring the environmento Distance hearingo Incidental information
• Can teach a child how to start conversations, make requests, problem solve, negotiate, compromise, joke, tease, and use sarcasm
• Spoken Communication Function
Audiology• How well can you counsel a family?
• The hearing system
• Types of Hearing Tests
• Degrees of Hearing Loss
• Causes of Hearing Loss in Children
• Audiograms
“With the technology and early auditory intervention
available today, a child with a hearing loss can
have the same opportunity as a typically hearing child
to develop spoken language, reading, and
academic skills.”
References• American Academy of Audiology. (2004). Scope of practice . Retrieved from
http://www.audiology.org/resources/documentlibrary/Pages/ScopeofPractice.aspx
• American Speech-Language-Hearing Association. (2012).How does your child hear and talk?. Retrieved from http://www.asha.org/public/speech/development/chart.htm
• American Speech-Language-Hearing Association. (2001). Knowledge and skills required for the practice of audiologic/aural rehabilitation [Knowledge and Skills]. Available from www.asha.org/policy.
• American Speech-Language-Hearing Association. (2004). Scope of practice in audiology [Scope of Practice]. Available from www.asha.org/policy.
• Cole, E. B., & Flexer, C. (2007). Children with hearing loss: Developing listening and talking birth to six. San Diego, CA: Plural Publishing, Inc.
• Deconde Johnson, C., & Seaton, J. B. (2012). Educational audiology handbook. (2nd ed.). Clifton Park, NY: Delmar
Cengage Learning.
• Ling, D. (2002). Speech and the hearing-impaired child: Theory and practice. (2nd ed.). Washington, DC: Alexander Graham Bell Association for the Deaf and Hard of Hearing.
• Ling, D., & Ling, A. H. (1978, 1980, 1985). Aural habilitation: The foundations of verbal learning in hearing-impaired children. (3rd ed.). Washington, DC: AG Bell Association for the Deaf, Inc.
• Talking Child, LLC. (2003). Child language development. Retrieved from http://www.talkingchild.com/chartvocab.aspx
• Talking Child, LLC. (2003). Intelligibility guidelines. Retrieved from http://www.talkingchild.com/chartintel.aspx
• Talking Child, LLC. (2003). Speech and articulation development chart. Retrieved from http://www.talkingchild.com/speechchart.html