Embed Size (px)
Citation preview

GFR Normalized to Total Body Water AllowsComparisons across Genders and Body Sizes
Bjørn O. Eriksen,*† Toralf Melsom,*† Ulla D. Mathisen,*† Trond G. Jenssen,†‡
Marit D. Solbu,* and Ingrid Toft*†
*Section of Nephrology, University Hospital of North Norway; †Department of Clinical Medicine, University ofTromsø, Tromsø, Norway; and ‡Oslo University Hospital, Rikshospitalet, Oslo, Norway
ABSTRACTThe normalization of GFR to a standardized body-surface area of 1.73 m2 impedes comparison of GFRacross individuals of different genders, heights, or weights. Ideally, GFR should be normalized to aparameter that best explains variation in GFR. Here, we measured true GFR by iohexol clearance in arepresentative sample of 1627 individuals from the general population who did not have diabetes,cardiovascular disease, or kidney disease. We also estimated total body water (TBW), extracellular fluidvolume, lean body mass, liver volume, metabolic rate, and body-surface area. We compared twomethods of normalizing GFR to these physiologic variables: (1) the conventional method of scaling GFRto each physiologic variable by simple division and (2) a method based on regression of the GFR on eachvariable. TBW explained a higher proportion of the variation in GFR than the other physiologic variables.GFR adjusted for TBW by the regression method exhibited less dependence on gender, height, andweight compared with the other physiologic variables. Thus, adjusting GFR for TBW by the regressionmethod allows direct comparisons between individuals of different genders, weights, and heights. Wepropose that regression-based normalization of GFR to a standardized TBW of 40 L should replace thecurrent practice of normalizing GFR to 1.73 m2 of body-surface area.
J Am Soc Nephrol 22: 1517–1525, 2011. doi: 10.1681/ASN.2010121321
The GFR is arguably one of the most importantparameters in human physiology and plays a fun-damental role in nephrology. In both clinical prac-tice and research, comparisons of GFR between andwithin subjects are of vital importance. BecauseGFR varies with weight and height, it is evident thatGFR comparisons must include some adjustmentfor body size. The traditional adjustment methodhas been to divide GFR by body-surface area (BSA)and to standardize it to 1.73 m2. This was first pro-posed in a study of urea clearance by McIntosh in1928.1
The conventional method has been repeatedlycriticized, and it has been suggested that other phys-iologic variables may be more appropriate for ad-justing GFR than BSA. Peters et al.2 showed thatnormalizing the GFR to the extracellular fluid vol-ume (ECV) was more appropriate for children. Inadults, some studies have concluded that ECV
should replace BSA,2,3 and others have found BSAsuperior or similar to other parameters.4,5 A com-parison among mammals of different sizes has sup-ported the hypothesis that metabolic rate sets thelevel of GFR; thus, some researchers have proposedthat metabolic rate should be used for normaliza-tion.6 Total body water (TBW), height, liver vol-ume, and lean body mass have also been suggestedas candidates for a normalizing factor.4,7 In prac-tice, fluid volumes and metabolic rate are cumber-
Received December 31, 2010. Accepted March 15, 2011.
Published online ahead of print. Publication date available atwww.jasn.org.
Correspondence: Dr. Bjørn Odvar Eriksen, Section of Nephrology,University Hospital of North Norway, 9038 Tromsø, Norway. Phone:47-466-82-780; Fax: 47-776-69-408; E-mail: [email protected].
Copyright © 2011 by the American Society of Nephrology
CLI
NIC
AL
EP
IDE
MIO
LOG
Y
CLINICAL EPIDEMIOLOGY www.jasn.org
J Am Soc Nephrol 22: 1517–1525, 2011 ISSN : 1046-6673/2208-1517 1517

some to measure directly and would have to be estimated withequations based on anthropometric measures.
In normalizing GFR to body size, at least two issues must beconsidered. First, the adjustment must facilitate GFR compar-isons among individuals by reducing differences that arisefrom differences in body size as much as possible. The physio-logic variables that have been suggested as a basis for adjust-ment may differ in their abilities to explain interindividualvariations in GFR. Second, statistically, there are theoreticalproblems associated with adjustments that simply divide GFRby a physiologic variable, e.g. the current practice of dividingGFR by BSA (the ratio method). Specific conditions must bemet to avoid spurious correlations between such ratio variablesand other independent variables.8 This problem was previ-ously pointed out by Tanner in 19499 and illustrated in a sim-ulation study by Lowrie in 1999.10 An alternative method basedon regression analysis has been proposed by Turner andReilly,11 but to date this has received very little attention in thenephrological community.
The normalization of GFR has been studied only in smallstudies of selected subjects or in populations of potential kid-ney donors. Those results may not be valid for the generalpopulation. The purpose of this study was to explore the nor-malization issue in a representative sample of the general pop-ulation drawn from the sixth population-based prospective
survey conducted in Tromsø, Norway (Tromsø 6). In the Re-nal Iohexol Clearance Survey in Tromsø 6 (RENIS-T6), GFRwas measured with a precise method in persons between 50and 62 years without known diabetes, cardiovascular, or renaldisease. Our first aim was to investigate the ability of differentphysiologic variables to explain variations in GFR. Our secondaim was to compare the conventional ratio method and theTurner and Reilly regression method for adjusting GFR by thephysiologic variables that we estimated with functions basedon height and weight.
RESULTS
The RENIS-T6 cohort consisted of a representative sample of1627 subjects aged 50 to 62 years without diabetes, cardiovas-cular disease, or kidney disease from the general population.Table 1 shows the baseline measurements made in the mainpart of the population survey, Tromsø 6, and compares theincluded subjects to all eligible subjects. The statistically signif-icant differences between groups were very small.
To find the best predictor of GFR from gender, age, weight,and height, multiple linear regression analyses were performedwith unadjusted GFR (uGFR) in ml/min as the dependentvariable (Table 2). Age, gender, height, and weight were inde-
Table 1. Study population characteristics compared to all eligible subjects
Women Men
Included (n � 826) Eligible (n � 1542)a Included (n � 801) Eligible (n � 1283)a
Median age (IQR), years 57.5 (53.0 to 61.0) 57.0 (53.0 to 60.0) 57.0 (53.0 to 60.0) 57.0 (53.0 to 60.0)Median height (IQR), cm 164.4 (160.8 to 168.6) 164.4 (160.3 to 168.5) 177.2 (172.9 to 181.1) 177.5 (173.0 to 181.7)Median weight (IQR), kg 70.0 (63.1 to 77.7) 69.0 (62.4 to 77.4) 85.0 (77.4 to 94.0) 84.8 (77.2 to 93.2)Median body-mass index (IQR), kg/m2 25.7 (23.3 to 28.9) 25.6 (23.2 to 28.5) 27.1 (25.0 to 29.6)c 26.9 (24.9 to 29.3)Median body-surface area (IQR), m2 1.77 (1.68 to 1.86)c 1.76 (1.67 to 1.86) 2.02 (1.92 to 2.13) 2.03 (1.92 to 2.13)Median estimated GFR (IQR), ml/min per
1.73 m2 b
89.4 (79.8 to 100.4)c 88.0 (78.2 to 98.8) 91.9 (82.7 to 101.5) 91.7 (82.8 to 101.4)
Median unadjusted measured GFR (IQR),ml/min
90.5 (81.0 to 100.2) 112.2 (100.6 to 123.9)
Median measured GFR (IQR), ml/minper 1.73 m2
87.9 (79.3 to 96.6) 95.9 (86.4 to 104.8)
The values represent the baseline measurements taken in the main part of the sixth population survey in Tromsø. IQR, interquartile range.aMedians and interquartile ranges weighted according to the age stratification of RENIS-T6.bGFR estimated with the recalibrated four-variable Modification of Diet in Renal Disease study equation.cP � 0.05 for difference between included and eligible in age-adjusted quantile regression.
Table 2. Multiple linear regressions of unadjusted glomerular filtration rate (ml/min) on age, gender, body weight, andheight
Independent VariableRegression Coefficient (ml/min) (95% Confidence Interval)
Model 1 Model 2 Model 3
Intercept 133.68 (121.67 to 145.68) 100.79 (89.11 to 112.47) 51.82 (26.68 to 76.96)Gender (female � 0, male � 1) 22.27 (20.69 to 23.85) 14.68 (12.99 to 16.38) 16.43 (14.21 to 18.65)Age, years �0.74 (�0.95 to �0.54) �0.82 (�1.01 to �0.63) �0.67 (�0.87 to �0.46)Body weight, kg 0.51 (0.46 to 0.57)Height, cm 0.47 (0.34 to 0.60)
Root mean square error 16.24 14.95 15.99Coefficient of determination (R2) 0.335 0.437 0.356
CLINICAL EPIDEMIOLOGY www.jasn.org
1518 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1517–1525, 2011

pendently associated with uGFR (P � 0.0001). Because of co-linearity, weight and height were not included in the samemodel. The model that incorporated weight (Model 2) had ahigher coefficient of determination (R2) than the model thatincorporated height (Model 3) (0.437 versus 0.356). All of thepossible interactions between the independent variables weretested. Only the interaction between gender and weight wassignificant (P � 0.004), but its partial R2 was only 0.004. Nononlinear effects were found when the same variables were ex-plored in generalized additive models. When the continuous vari-ables in Model 2 were log-transformed, all of the independentvariables remained statistically significant, and R2 was 0.404.
Physiologic variables were estimated with published equa-tions (Table 3). To explore their ability to explain variation inuGFR, the fit of separate linear regression analyses with uGFRas the dependent variable and each of the physiologic variables
and age as the independent variables were analyzed (Table 4).The analyses were performed both with and without log-trans-formed variables. For the untransformed variables, all of theintercepts were different form zero (P � 0.05), which meansthat uGFR was not strictly proportional to any of the physio-logic variables. For both untransformed and log-transformedvariables, TBW had the highest R2. Although the 95% confi-dence intervals overlapped, these differences in R2 between TBWand each of the other physiologic variables were statistically dif-ferent with the bootstrap method (P � 0.05). Lean body mass andmetabolic rate had R2 values similar to that of TBW. The differ-ences in root-mean-square error exhibited the same pattern as R2.
The models with log-transformed variables in Table 4 wereused to create adjusted GFRs according to the regressionmethod of Turner and Reilly.11 Another set of adjusted GFRswas created by simply dividing the uGFR by each of the phys-
Table 3. Equations for estimating physiologic variables
Variable Equation Author(s) Reference
Total body water (L) Watson et al. 20men 2.447 � (0.3362 � weight) � (0.1074 � height) � (0.09516 � age)women �2.097 � (0.2466 � weight) � (0.1069 � height)
Resting energy expenditure(metabolic rate) (kcal/day)
(9.99 � weight) � (6.25 � height) � (4.92 � age) � (166 � gender) � 161 Mifflin et al. 34
Lean body mass (kg) Boer 7men �19.2 � (0.407 � weight) � (0.267 � height)women �48.3 � (0.252 � weight) � (0.473 � height)
Extracellular volume (L) Silva et al. 14men �12.424 � (0.191 � weight) � (0.0957 � height) � (0.025 � age)women �4.027 � (0.167 � weight) � (0.05987 � height)
Liver volume (mL) 722 � (body-surface area)1.176 Johnson et al. 35Body-surface area (m2) 0.007184 � weight0.425 � height0.725 DuBois and DuBois 36Weight is in kilograms, height is in centimeters, and age is in years. Gender is 0 for women and 1 for men. Body-mass index is defined as weight/(height)2
Table 4. Results of linear regressions to determine physiologic factors that influence unadjusted glomerular filtration rateIntercept (95%
Confidence Interval)Regression Coefficient
(95% Confidence Interval)R2 (95% Confidence
Interval)Root Mean Square Error
(95% Confidence Interval)
Glomerular filtration rate (ml/min)total body water, L 71.33 (59.50 to 83.15) 1.79 (1.69 to 1.89) 0.436 (0.397 to 0.473) 14.95 (14.32 to 15.64)metabolic rate, kcal/d 52.70 (40.35 to 65.05) 0.05 (0.05 to 0.06) 0.428 (0.390 to 0.466) 15.06 (14.42 to 15.76)lean body mass, kg 69.37 (57.36 to 81.38) 1.32 (1.24 to 1.39) 0.424 (0.384 to 0.461) 15.11 (14.47 to 15.82)extracellular fluid volume, L 76.48 (64.38 to 88.59) 3.62 (3.40 to 3.84) 0.404 (0.365 to 0.443) 15.38 (14.73 to 16.06)liver volume, mL 47.90 (34.71 to 61.09) 0.06 (0.06 to 0.07) 0.378 (0.339 to 0.417) 15.70 (15.03 to 16.40)body-surface area, m2 30.80 (17.05 to 44.55) 60.09 (56.22 to 63.96) 0.378 (0.339 to 0.417) 15.70 (15.04 to 16.40)body weight, kg 90.08 (77.48 to 102.68) 0.78 (0.72 to 0.83) 0.337 (0.297 to 0.377) 16.22 (15.54 to 16.90)height, cm �60.84 (�82.11 to �39.57) 1.14 (1.05 to 1.24) 0.273 (0.236 to 0.310) 16.98 (16.29 to 17.75)
Log(glomerular filtration rate)log(total body water) 3.776 (3.281 to 4.272) 0.696 (0.654 to 0.739) 0.401 (0.356 to 0.444) 0.159 (0.148 to 0.171)log(metabolic rate) 0.284 (�0.323 to 0.891) 0.765 (0.718 to 0.813) 0.393 (0.347 to 0.436) 0.160 (0.149 to 0.172)log(lean body mass) 3.456 (2.947 to 3.966) 0.716 (0.670 to 0.761) 0.387 (0.340 to 0.431) 0.161 (0.150 to 0.173)log(extracellular fluid volume) 4.431 (3.934 to 4.929) 0.726 (0.678 to 0.773) 0.370 (0.326 to 0.414) 0.163 (0.152 to 0.175)log(liver volume) �0.587 (�1.277 to 0.102) 0.958 (0.891 to 1.024) 0.345 (0.300 to 0.391) 0.166 (0.155 to 0.179)log(body-surface area) 5.715 (5.224 to 6.207) 1.126 (1.048 to 1.204) 0.345 (0.300 to 0.391) 0.166 (0.155 to 0.179)log(body weight) 4.030 (3.496 to 4.564) 0.609 (0.563 to 0.655) 0.310 (0.267 to 0.354) 0.171 (0.160 to 0.182)log(height) �3.906 (�4.955 to �2.858) 1.923 (1.754 to 2.092) 0.252 (0.210 to 0.294) 0.177 (0.167 to 0.190)
Each line represents a separate multiple linear regression of the dependent on the corresponding independent variable. All of the analyses were adjusted forage or log(age) as appropriate. The regression coefficients are given per unit. Natural logarithms were used. Age or log(age) was statistically significant in allthe models (P � 0.0001). The differences in R2 and root-mean-square error between total body water and each of the other physiologic variables for bothtransformed and untransformed variables were tested with the bootstrap method and found statistically significant (P � 0.05). R2 is the coefficient ofdetermination.
CLINICAL EPIDEMIOLOGYwww.jasn.org
J Am Soc Nephrol 22: 1517–1525, 2011 Normalization of GFR 1519

iologic variables (the ratio method). We then determined theeffects of gender and either height or weight on each adjustedGFR variable (Table 5). The adjusted GFR variables were re-gressed on gender and on height or weight in age-adjustedmodels. For the ratio method, all of the adjusted GFR variableswere associated with both gender and either weight orheight (P � 0.05), except metabolic rate, which was not asso-ciated with gender (Model 2). For the Turner and Reilly regres-sion method, all of the adjusted GFR variables were associatedwith both gender and height or weight (P � 0.05), except TBWand lean body mass. Neither TBW nor lean body mass adjust-ments depended on gender or weight (Model 3). For TBW, theregression coefficients for gender and height in Model 4 weresmaller than the corresponding coefficients for the other phys-iologic variables. The regression coefficients in Table 5 werestandardized estimates to facilitate comparison across physio-logic variables.
GFRs normalized to either BSA or TBW by the two methodswere compared according to body-mass index (BMI) for dif-ferent genders (Table 6). In this table, GFR was normalized tothe population means of BSA (1.9 m2) and TBW (39.2 L) to
facilitate comparisons, rather than to a BSA of 1.73 m2 and aTBW of 40 L. GFR adjusted for TBW by the Turner and Reillyregression method did not differ across the BMI categories foreither of the genders. The other adjusted variables varied acrossBMI categories for one or both genders (P � 0.05).
DISCUSSION
When assessing GFR, we want to be able to decide whether aperson has a normal GFR, and if not, to measure the deviationfrom normal. However, the concept of “normality” in physi-ology is no less problematic than in other areas of medicine.Conceivably, more detailed knowledge of renal physiology andhomeostatic mechanisms would reveal constant relationshipsbetween GFR and other physiologic parameters, which wouldhelp settle the issue; however, we are far from attaining thatknowledge. Currently, our best option is to use statisticalmethods to adjust GFR for factors that clearly affect variation.
The physiologic variables investigated in this study wereonly able to explain 30 to 45% of the variation in uGFR (Table
Table 5. Comparison of methods for normalizing GFR to a physiologic variable: dependence of the normalized GFRvariables on gender, body weight, and height in regression analyses for each of the physiologic variables
Physiologic variable used asbasis for adjustment by each of
the two methods
Method 1: Glomerular Filtration Rate (ml/min)Adjusted by the Ratio Method
Method 2: Glomerular Filtration Rate (ml/min)Adjusted by the Method of Turner and Reilly11
Model 1 Model 2 Model 3 Model 4
Standardizedregressioncoefficient
PStandardized
regressioncoefficient
PStandardized
regressioncoefficient
PStandardized
regressioncoefficient
P
Total body watergender (female � 0, male � 1) �0.136 �0.0001 �0.105 0.0016 0.047 0.10 0.087 0.01body weight, kg �0.254 �0.0001 �0.045 0.12height, cm �0.227 �0.0001 �0.089 0.01
Metabolic rategender (female � 0, male � 1) �0.027 0.33 0.055 0.1072 0.094 0.001 0.172 �0.0001body weight, kg �0.230 �0.0001 �0.068 0.02height, cm �0.281 �0.0001 �0.159 �0.0001
Lean body massgender (female � 0, male � 1) �0.115 �0.0001 0.077 0.02 0.051 0.07 0.209 �0.0001body weight, kg �0.184 �0.0001 �0.005 0.87height, cm �0.402 �0.0001 �0.225 �0.0001
Extracellular fluid volumegender (female � 0, male � 1) 0.160 �0.0001 0.202 �0.0001 0.252 �0.0001 0.299 �0.0001body weight, kg �0.395 �0.0001 �0.174 �0.0001height, cm �0.345 �0.0001 �0.191 �0.0001
Liver volumegender (female � 0, male � 1) 0.299 �0.0001 0.415 �0.0001 0.307 �0.0001 0.420 �0.0001body weight, kg �0.195 �0.0001 �0.167 �0.0001height, cm �0.304 �0.0001 �0.280 �0.0001
Body-surface areagender (female � 0, male � 1) 0.324 �0.0001 0.430 �0.0001 0.307 �0.0001 0.420 �0.0001body weight, kg �0.096 0.0004 �0.167 �0.0001height, cm �0.219 �0.0001 �0.280 �0.0001
For each physiologic variable, the adjusted variables by each of the two methods were regressed on gender and body weight in Models 1 and 3 and ongender and height in Models 2 and 4. All of the models were adjusted for age. The standardized regression coefficients give the increase as the number ofstandard deviations of the dependent variable per standard deviation of the independent variables.
CLINICAL EPIDEMIOLOGY www.jasn.org
1520 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1517–1525, 2011

4). Some of the residual variation was caused by day-to-day,within-person variability of iohexol-clearance measurements;this measurement has been found to have a coefficient of vari-ation of about 5.5% in other studies,.12,13 In this study, wefound that TBW was superior to BSA and the other physiologicvariables in explaining the variation in uGFR, as expressed byR2 (P � 0.05) (Table 4). In addition to the ECV equation de-veloped by Silva et al.,14 we tested an alternative equation de-veloped by Bird et al.15 that resulted in an even lower R2 (notshown).
The traditional and almost universally used method for ad-justing GFR has been to scale uGFR by simply dividing by avariable, e.g. uGFR/BSA or uGFR/TBW. The problem with thismethod is that it assumes strict proportionality between GFRand the physiologic variable, i.e. it assumes an intercept of zeroin a regression of uGFR on the physiologic variable. We found
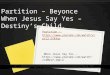
that the intercepts were statistically differentfrom zero for all of the investigated physio-logic variables (upper part of Table 4). As aconsequence, the ratio method assigned in-appropriately-high adjusted GFR values insubjects with, for example, low TBW and in-appropriately-low adjusted GFR values insubjects with high TBW, even when their uG-FRs could be considered normal, relative totheir TBWs (Figure 1). The example in Fig-ure 1 was calculated for the mean age inthe RENIS-T6 cohort. Because age was anindependent predictor of uGFR in theuntransformed analyses, the intercept inFigure 1 varied with age, which made theratio method even more problematic.
It has been argued that the error asso-ciated with the BSA ratio method is toosmall to justify changing the method.16
However, the error may be larger for in-dividuals with atypical body sizes.17 Thealternative method proposed by Turnerand Reilly on the basis of regression anal-ysis overcomes some of the problems as-sociated with the ratio method, because itcompletely removes variation associatedwith the variable used to adjust the GFR.The TBW-regression adjustment of GFRwas less dependent on gender, height,and weight than the other physiologicvariables (Table 5). Moreover, the BSAadjustment depended on one or more ofgender, height, and weight in both theratio and the regression methods.
We modified Turner and Reilly’s methodby using the log-transformed linear regres-sion analyses as the starting point (lower partof Table 4).11 We implemented this trans-formation because the untransformed vari-
ables can give negative values for the adjusted variable whenuGFR is very low. Log-transformed variables avoid this prob-lem because the subtraction of a negative residual is equivalentto division when the antilogarithm is performed. The fits of theuntransformed and transformed models for TBW were notsignificantly different, as estimated by R2 (Table 4). An addi-tional justification for using log transformation was the recog-nition of the general assumption that the error in GFR mea-surement depends on the magnitude of GFR. We also modifiedthe Turner and Reilly method by including an adjustment forlog(age) in the regression. However, the final, simplified equa-tion for the TBW adjustment was independent of age, becausethe age terms canceled out.
Our findings indicated that using TBW to adjust the uGFRwith the regression method of Turner and Reilly had clear ad-vantages over other methods. Daugirdas et al.4 reached a dif-
Table 6. Comparison of unadjusted and adjusted glomerular filtration ratesaccording to body-mass index and gender
Mean (standard deviation)
Women Men
Unadjusted glomerular filtration rate, ml/min�25 kg/m2 body-mass index 86.5 (13.9)c 105.0 (15.1)c
25 to 30 kg/m2 body-mass index 91.3 (14.1) 111.5 (16.6)�30 kg/m2 body-mass index 96.4 (17.6) 122.1 (18.0)
Total body water, L�25 kg/m2 body-mass index 31.0 (2.1)c 40.7 (3.0)c
25 to 30 kg/m2 body-mass index 33.6 (2.0) 44.7 (3.1)�30 kg/m2 body-mass index 37.5 (3.0) 50.0 (3.7)
Body-surface area, m2
�25 kg/m2 body-mass index 1.69 (0.11)c 1.90 (0.12)c
25 to 30 kg/m2 body-mass index 1.80 (0.10) 2.03 (0.12)�30 kg/m2 body-mass index 1.95 (0.13) 2.18 (0.13)
GFR adjusted to population mean body-surfacearea† by the ratio method, ml/min
�25 kg/m2 body-mass index 98.2 (15.3)c 105.7 (14.9)25 to 30 kg/m2 body-mass index 97.2 (14.8) 105.2 (15.0)�30 kg/m2 body-mass index 94.5 (17.0) 107.2 (15.5)
GFR adjusted to population mean body-surfacearea by the regression method of Turner andReilly, ml/mina
�25 kg/m2 body-mass index 99.8 (15.7)c 105.8 (15.1)25 to 30 kg/m2 body-mass index 98.0 (15.0) 104.4 (15.0)�30 kg/m2 body-mass index 94.3 (17.1) 105.5 (15.4)
GFR adjusted to population mean total bodywater by the ratio method, ml/minb
�25 kg/m2 body-mass index 109.8 (17.1)c 101.4 (14.4)c
25 to 30 kg/m2 body-mass index 106.9 (16.3) 97.9 (14.0)�30 kg/m2 body-mass index 101.1 (18.5) 95.9 (14.0)
GFR adjusted to population mean total bodywater by the regression method of Turnerand Reilly, ml/minb
�25 kg/m2 body-mass index 102.1 (15.8) 102.4 (14.2)25 to 30 kg/m2 body-mass index 101.8 (15.3) 101.8 (14.4)�30 kg/m2 body-mass index 99.6 (17.9) 103.1 (14.6)
aStudy population mean body-surface area was 1.9 m2.bStudy population mean total body water was 39.2 L.cP � 0.05 for differences across body-mass index categories within each gender.
CLINICAL EPIDEMIOLOGYwww.jasn.org
J Am Soc Nephrol 22: 1517–1525, 2011 Normalization of GFR 1521

ferent conclusion in their study of 1551 potential kidney do-nors. BSA and TBW were not analyzed in the regressionmethod of Turner and Reilly, but after adjusting for age andrace, they found that GFR/BSA did not depend on gender, butGFR/TBW was markedly higher in women than men. How-ever, the investigated donor population may not have beenrepresentative of the general population, because the GFR ofthe included women was similar to that of the men (106 versus104 ml/min per 1.73 m2). In contrast, there was a clear genderdifference in BSA-adjusted GFR in this study (Table 1).
In 1952, McCance and Widdowson18 suggested that TBWwas the correct variable for adjusting GFR; however, there is alack of studies on the relationship between GFR and TBW inthe literature. Some authors compared BSA and ECV for ad-justing the GFR. In fact, the uGFR/ECV is a particularly attrac-tive adjustment, because the uGFR/ECV is approximatelyidentical to the slope of the terminal exponential of the plasmaclearance curve after a bolus injection of a filtration marker.19
In contrast to the single-sample method used in this study,uGFR and ECV can be measured in the same procedure, whenGFR is measured by a single-injection, multi-sample method.Visser et al.3 found that GFR/ECV did not depend on gender,BSA, or height in regression analyses but that GFR/BSA de-pended on gender. That study was performed in healthy vol-unteers and potential kidney donors. In contrast, White andStrydom5 found that uGFR/BSA and uGFR/ECV produced es-sentially the same result in 110 patients with uGFRs between 10and 160 ml/min. Peters et al.2 argued that normalization toECV was more appropriate for children than for adults, but
they included patients with reduced GFR. None of those stud-ies considered the regression method of Turner and Reilly as analternative to using the ratio method. The diverging resultsmay have been caused by differences between the investigatedpopulations. To our knowledge, this study is the first to exam-ine this issue in a representative sample from the general pop-ulation.
An important limitation of this study was that it relied onestimates, instead of direct measurements, of the physiologicvariables. The estimates were all on the basis of age, gender,weight, and/or height, and whereas the BSA equation used onlyweight and height, the TBW equation included gender and ageas well. Direct measurement of the physiologic variables, withthe possible exception of ECV, is so complicated and costlythat estimation from anthropometric measures is currently theonly feasible method in clinical practice and epidemiologic re-search. Watson’s equation for TBW has been validated.20,21
When we repeated the analyses with Chumlea’s equation forestimating TBW, the results were very similar to those ob-tained with Watson’s equation (not shown). Nevertheless,some caution should be observed in the conclusion that TBWwas the best variable for the adjustment of GFR. The fits of themodels for TBW, metabolic rate, and lean body mass showedonly small differences, and physiologically, there is a high cor-relation between these variables and ECV. However, TBW,metabolic rate, and lean body mass were clearly different com-pared with BSA for adjusting GFR; this supports the recom-mendations that adjustment by BSA should be abandoned.
Another limitation was that this study only included mid-dle-aged Caucasians. However, age did not influence the ef-fects of gender, height, and weight on uGFR within the studiedage interval because the interactions of these variables with agewere not statistically significant. But although basal physio-logic relationships can be expected to be invariant across ageand ethnicity, our study should be replicated in general popu-lations with other characteristics. Also, our analyses were onthe basis of the assumption that variation in GFR caused bygender, height, and body weight in healthy persons in a repre-sentative sample of the general population is without biologicsignificance. Whereas this assumption is usually made aboutGFR, it is difficult to prove. When investigating effects of vari-ation in GFR, the possibility that the relationship between GFRand body fluid volumes may be different in patient popula-tions, for example as in obese patients, should be kept open.The best approach in such cases may be to use absolute GFR inml/min as an explanatory variable and to adjust for both TBWand ECV.
The results of our study supported the recommendationthat the practice of using GFR/BSA scaled to 1.73 m2 should beabandoned and should be replaced with a TBW adjustment ofuGFR by the regression method of Turner and Reilly. The re-gression method is somewhat more complicated than the ratiomethod, but uGFR currently requires a computer calculation;thus, the calculations could be automated. In practice, we sug-gest that the measured, unadjusted GFR should be adjusted to
Figure 1. Total body water (TBW) was used to adjust the GFRwith the ratio method. Examples are shown for two patients with25 and 60 L of TBW. The gray circles indicate the GFR and TBWobserved in the RENIS-T6 cohort. The black solid line indicatesthe regression of GFR on TBW at the mean age in the RENIS-T6cohort. Although both the example patients had a normal GFR onthe basis of the regression line, their GFR to TBW ratios aredifferent. For the first patient, a and b indicate the GFR and TBW,respectively. For the second patient, c and d indicate the GFR andTBW, respectively.
CLINICAL EPIDEMIOLOGY www.jasn.org
1522 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1517–1525, 2011

the corresponding GFR in a person with 40 L of TBW (Table 7).This standard individual was chosen because the mean TBW ofmen and women is approximately 40 L.21 The algorithm forcalculating the adjusted variable with this method is given inTable 7. One of the advantages of this method is that whenTBW was used to adjust GFR with the regression method, weobserved almost identical values across gender and BMI cate-gories (Table 6). One of the problems with GFR/BSA has beenthat it assigned inappropriately low values to individuals withhigh BMI, which resulted in potential confounding by BMI instudies of GFR and cardiovascular disease.22
We conclude that using BSA to adjust uGFR, either by theratio method or by the regression method of Turner and Reilly,did not remove dependencies on gender, weight, or height. Wefound that more of the variation in uGFR could be explainedby TBW than by BSA. Furthermore, when TBW estimatedfrom gender, age, height, and weight was used to adjust GFR bythe regression method, the dependencies on gender, weight,and height were removed. Therefore, we propose a new calcu-lation that adjusts the uGFR to a standardized TBW of 40L (GFR40) instead of the current practice of using uGFR/BSAstandardized to a BSA of 1.73 m2.
CONCISE METHODS
SubjectsThe Tromsø Study is a series of population-based prospective surveys
in the municipality of Tromsø, North Norway (current population,
65,000). Our RENIS-T6 cohort was an ancillary part of the sixth
Tromsø study. In the main part of the Tromsø 6 study, a representa-
tive sample of 12,984 adults from the general population participated
between October 2007 and December 2008. The invited population
included a 40% random sample of individuals aged 50 to 59 years and
all individuals aged 60 to 62 years (5464 total subjects in all). A total of
3564 individuals between 50 and 62 years of age completed the main
part of Tromsø 6 (65%). Of these, 739 reported a previous history of
myocardial infarction, angina pectoris, stroke, diabetes mellitus, or
renal disease. The remaining 2825 eligible subjects were invited to
participate in RENIS-T6. Of the 2107 individuals that responded pos-
itively, 12 were excluded because of an allergy to contrast media, io-
dine, or latex; 65 were excluded for other reasons; and 48 did not
appear for their appointments. A total of 1982 subjects remained for
potential inclusion, but only 1632 were investigated, according to a
predefined target. Later, five participants were excluded because the
iohexol-clearance measurements were technical failures. Accord-
ingly, a total of 1627 participants were included in the RENIS-T6
cohort for this study.
This study was approved by the Norwegian Data Inspectorate and
the Regional Ethics Committee of North Norway. All of the subjects
provided written consent.
MeasurementsuGFR was measured as single-sample plasma clearance of iohexol at
the Clinical Research Unit at the University Hospital of North Nor-
way. This method has been validated against gold standard methods
for measuring GFR.23–29 The subjects were instructed to avoid large
meals with meat and nonsteroid anti-inflammatory drugs for 2 days
before the investigation. The measurements were performed after
fasting and abstinence from nicotine. The subjects were reminded to
avoid restricting water intake. A Teflon catheter was placed in an
antecubital vein, and blood was drawn for a null sample and for cre-
atinine measurements. Five milliliters of iohexol (Omnipaque, 300
mg I/ml; Amersham Health, London, UK) was injected, and the sy-
ringe was weighed before and after the injection. The catheter was
flushed with 30 ml of isotonic saline and used for iohexol analysis
samples.27 The optimal time for measuring iohexol concentration af-
ter injection was calculated by Jacobsson’s method on the basis of the
GFR estimated from creatinine.30 To ensure complete distribution of
iohexol in the extracellular fluid volume, the shortest sampling time
was set at 180 minutes. The exact time from injection to sampling was
measured in minutes with a different stop watch for each subject.
The serum iohexol concentration was measured by HPLC, as de-
scribed previously by Nilsson-Ehle.31 The coefficient of variation was
3.0% for the analysis during the study period. The external quality
control was provided by Equalis (Equalis AB, Uppsala, Sweden).
The GFR was calculated with the formulas described by Jacob-
sson.30 Extrarenal iohexol clearance was ignored, in accordance with
the practice of other authors. Further details about the iohexol anal-
ysis and the method for calculating GFR have been described previ-
ously.32
Plasma-creatinine analyses were performed on the Hitachi mod-
ular model with an enzymatic method that has been standardized
against isotope dilution mass spectroscopy (CREA Plus; Roche Diag-
nostics, GmbH, Mannheim, Germany). Estimated GFR was calcu-
lated as ml/min per 1.73 m2 with the recalibrated four-variable Mod-
ification of Diet in Renal Disease equation,33 as follows: 175 �
(creatinine/88.4)�1.154 � age�0.203 � 1.212 (if African Ameri-
can) � 0.742 (if female). Creatinine was expressed in �mol/L.
Statistical MethodsThe comparison of differences between included and eligible persons
in Table 1 was performed with quantile regression adjusted for age.
The medians and interquartile ranges of characteristics of all eligible
persons were weighted according to the age and gender stratifications
of RENIS-T6. The baseline measurements from the main part of
Tromsø 6 were used for these comparisons.
A multiple linear regression analysis was performed with uGFR as
the dependent variable and age, gender, weight, and height as the
Table 7. Method for adjustment of GFR to 40 liters oftotal body water (GFR40)
1. Estimate total body water in liters from Watson’s equationa
men: 2.447 � (0.3362 � weight) � (0.1074 � height) � (0.09516 � age)women: �2.097 � (0.2466 � weight) � (0.1069 � height)
2. Convert the unadjusted GFR to the corresponding GFR in ml/minfor the standard individual with 40 liters of total bodywater (GFR40)b
13.05 � unadjusted GFR � total body water�0.6963
aHeight is entered in centimeters, weight is in kilograms, and age is in years.bTotal body water is entered in L.
CLINICAL EPIDEMIOLOGYwww.jasn.org
J Am Soc Nephrol 22: 1517–1525, 2011 Normalization of GFR 1523

independent variables. All of the possible interactions between the
independent variables were tested. Nonlinear effects of the same vari-
ables were explored in generalized additive models.
Physiologic variables were estimated on the basis of equations
from the literature (Table 3).7,14,20,34 –36 uGFR was regressed on
each variable in separate linear regression analyses. Regressions on
height and body weight were included for comparison. All of the
analyses were adjusted for age. The analyses were performed both
with and without log transformation (natural logarithms) of the
dependent and independent variables. The fit of each model was
judged by root-mean-square error and R2. The bootstrap method
was used to estimate 95% confidence intervals of these statistics
and the differences between fits from 2000 resamples of the origi-
nal observations.37
For each physiologic variable, adjusted GFRs were created by two
methods. In the ratio method, uGFRs were adjusted by dividing by the
physiologic variable, e.g. uGFR/metabolic rate. In the Turner and
Reilly regression method, uGFR was regressed on age and each phys-
iologic variable, with log transformation of the variables.11 For each
subject, the residual from this regression (Figure 2) was added to the
expected log(uGFR) for a person of the same age, with the logarithm
of the physiologic variable set at the population mean. Then the ad-
justed GFR was the antilogarithm, according to the equation: adjusted
GFR � exp[log(uGFR) � (a � b � log(P) � c � log(age)) � (a �
b � log(mean P) � c � log(age))], where P is the physiologic vari-
able, a is the intercept, and b and c are the regression coefficients in the
regression of log(uGFR) on log(P) and log(age). The mean P is the
arithmetic mean of P in the RENIS-T6 cohort. This equation simpli-
fies to: adjusted GFR � exp[log(uGFR) � b � (log(P) � log(mean
P))]; this equation does not depend on age.
Finally, multiple linear regression models were performed to
study how the adjusted GFR created from each physiologic vari-
able by the ratio method and by Turner and Reilly’s regression
method depended on gender, weight, and height. These analyses
were adjusted for age. All of the analyses were performed with SAS,
version 9.2 (SAS Institute, Cary, NC). Statistical significance was
set at P � 0.05.
ACKNOWLEDGMENTS
We thank Britt-Ann Winther Eilertsen, Bjørg Skog Høgset, Saskia van
Heusden, and the rest of the staff at the Clinical Research Unit (Uni-
versity Hospital of North Norway) for performing the study; Harald
Strand and the staff at the Department of Medical Biochemistry (Uni-
versity Hospital of North Norway) for HPLC analyses of iohexol;
Inger Sperstad and Ingrid Dorthea Sandstad (Clinical Research Cen-
tre, University Hospital of North Norway) for database support; and
Tom Wilsgaard, Sriharan Sivasingarajah, and Kurt Jøran Nyland (De-
partment of Community Medicine, University of Tromsø) for iden-
tifying eligible subjects from the Tromsø 6 cohort.
DISCLOSURESNone.
REFERENCES
1. McIntosh JF, Moller E, Van Slyke DD: Studies of urea excretion: III. Theinfluence of body size on urea output. J Clin Invest 6: 467–483, 1928
2. Peters AM, Henderson BL, Lui D: Indexed glomerular filtration rate asa function of age and body size. Clin Sci 98: 439–444, 2000
3. Visser FW, Muntinga JHJ, Dierckx RA, Navis G: Feasibility and impactof the measurement of extracellular fluid volume simultaneous withGFR by I-125-iothalamate. Clin J Am Soc Nephrol 3: 1308–1315, 2008
4. Daugirdas JT, Meyer K, Greene T, Butler RS, Poggio ED: Scaling ofmeasured glomerular filtration rate in kidney donor candidates byanthropometric estimates of body surface area, body water, metabolicrate, or liver size. Clin J Am Soc Nephrol 4: 1575–1583, 2009
Figure 2. Total body water (TBW) was used to adjust GFR withthe regression method of Turner and Reilly. The gray circlesindicate the GFR and TBW observed in the RENIS-T6 cohort. Theblack solid line indicates the regression of log(GFR) on log(TBW)at the mean log(age) in the RENIS-T6 cohort. A: The residuallog(GFR) relative to the regression line is calculated for a subjectwith GFR of 85 ml/min and TBW of 50 L. B: This residual log(GFR)value is subtracted from the expected log(GFR) (on the basis ofthe regression line) for an average patient with a TBW of 40 L.The resulting log(GFR) is converted by taking the antilogarithmto give an adjusted GFR of 73 ml/min. This represents theGFR40 for the subject.
CLINICAL EPIDEMIOLOGY www.jasn.org
1524 Journal of the American Society of Nephrology J Am Soc Nephrol 22: 1517–1525, 2011

5. White AJ, Strydom WJ: Normalization of glomerular-filtration ratemeasurements. Eur J Nucl Med 18: 385–390, 1991
6. Singer MA: Of mice and men and elephants: Metabolic rate setsglomerular filtration rate. Am J Kidney Dis 37: 164–178, 2001
7. Boer P: Estimated lean body-mass as an index for normalization ofbody-Fluid volumes in humans. Am J Physiol 247: F632–F636, 1984
8. Kronmal RA: Spurious correlation and the fallacy of the ratio standardrevisited. J R Stat Soc Ser A Stat Soc 156: 379–392, 1993
9. Tanner JM: Fallacy of per-weight and per-surface area standards, andtheir relation to spurious correlation. J Appl Physiol 2: 1–15, 1949
10. Lowrie EG: Indexing physiological measurements to body size: A com-mon practice that should be changed. Semin Dial 12: S55–S60, 1999
11. Turner ST, Reilly SL: Fallacy of indexing renal and systemic hemody-namic measurements for body surface area. Am J Physiol 268: R978–R988, 1995
12. Tan GD, Lewis AV, James TJ, Altmann P, Taylor RP, Levy JC: Clinicalusefulness of cystatin C for the estimation of glomerular filtration ratein type 1 diabetes: Reproducibility and accuracy compared with stan-dard measures and iohexol clearance. Diabetes Care 25: 2004–2009,2002
13. Gaspari F, Perico N, Matalone M, Signorini O, Azzollini N, Mister M,Remuzzi G: Precision of plasma clearance of iohexol for estimation ofGFR in patients with renal disease. J Am Soc Nephrol 9: 310–313,1998
14. Silva AM, Wang J, Pierson RN, Wang ZM, Spivack J, Allison DB,Heymsfield SB, Sardinha LB, Heshka S: Extracellular water across theadult lifespan: reference values for adults. Physiol Meas 28: 489–502,2007
15. Bird NJ, Henderson BL, Lui D, Ballinger JR, Peters AM: Indexingglomerular filtration rate to suit children. J Nucl Med 44: 1037–1043,2003
16. Geddes CC, Woo YM, Brady S: Glomerular filtration rate: What is therationale and justification of normalizing GFR for body surface area?Nephrol Dial Transplant 23: 4–6, 2008
17. Delanaye P, Mariat C, Cavalier E, Krzesinski JM: Errors induced byindexing glomerular filtration rate for body surface area: Reductio adabsurdum. Nephrol Dial Transplant 24: 3593–3596, 2009
18. Mccance RA, Widdowson EM: The correct physiological basis onwhich to compare infant and adult renal function. Lancet 263: 860–862, 1952
19. Peters AM: The kinetic basis of glomerular filtration rate measurementand new concepts of indexation to body size. Eur J Nucl Med MolImaging 31: 137–149, 2004
20. Watson PE, Watson ID, Batt RD: Total body water volumes for adultmales and females estimated from simple anthropometric measure-ments. Am J Clin Nutr 33: 27–39, 1980
21. Chumlea WC, Guo SS, Zeller CM, Reo NV, Baumgartner RN, Garry PJ,Wang J, Pierson RN, Heymsfield SB, Siervogel RM: Total body waterreference values and prediction equations for adults. Kidney Int 59:2250–2258, 2001
22. Delanaye P, Radermecker RP, Rorive M, Depas G, Krzesinski JM:
Indexing glomerular filtration rate for body surface area in obesepatients is misleading: Concept and example. Nephrol Dial Transplant20: 2024–2028, 2005
23. Brown SC, O’Reilly PH: Iohexol clearance for the determination ofglomerular filtration rate in clinical practice: evidence for a new goldstandard. J Urol 146: 675–679, 1991
24. Sterner G, Frennby B, Mansson S, Nyman U, Van Westen D, Almen T:Determining “true” glomerular filtration rate in healthy adults usinginfusion of inulin and comparing it with values obtained using otherclearance techniques or prediction equations. Scand J Urol Nephrol42: 278–285, 2008
25. Eriksson CG, Kallner A: Glomerular filtration rate: A comparison be-tween Cr-EDTA clearance and a single sample technique with a non-ionic contrast agent. Clin Biochem 24: 261–264, 1991
26. Rydstrom M, Tengstrom B, Cederquist I, Ahlmen J: Measurement ofglomerular filtration rate by single-injection, single-sample tech-niques, using 51Cr-EDTA or iohexol. Scand J Urol Nephrol 29: 135–139, 1995
27. Brandstrom E, Grzegorczyk A, Jacobsson L, Friberg P, Lindahl A,Aurell M: GFR measurement with iohexol and 51Cr-EDTA: A compar-ison of the two favoured GFR markers in Europe. Nephrol Dial Trans-plant 13: 1176–1182, 1998
28. Bird NJ, Peters C, Michell AR, Peters AM: Comparison of GFR mea-surements assessed from single versus multiple samples. Am J KidneyDis 54: 278–288, 2009
29. Stevens LA, Levey AS: Measured GFR as a confirmatory test forestimated GFR. J Am Soc Nephrol 20: 2305–2313, 2009
30. Jacobsson L: A method for the calculation of renal clearance based ona single plasma sample. Clin Physiol 3: 297–305, 1983
31. Nilsson-Ehle P: Iohexol clearance for the determination of glomerularfiltration rate: 15 years’ experience in clinical practice. eJIFCC 13:2006
32. Eriksen BO, Mathisen UD, Melsom T, Ingebretsen OC, Jenssen TG,Njølstad I, Solbu M, Toft I: Cystatin C is not a better estimator of GFRthan plasma creatinine in the general population. Kidney Int 78:1305–1311, 2010
33. Levey AS, Coresh J, Greene T, Stevens LA, Zhang Y, Hendriksen S,Kusek JW, van Lente F for the Chronic Kidney Disease EpidemiologyCollaboration: Using standardized serum creatinine values in the Mod-ification of Diet in Renal Disease study equation for estimating glo-merular filtration rate. Ann Intern Med 145:247–254, 2006
34. Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO: A newpredictive equation for resting energy expenditure in healthy individ-uals. Am J Clin Nutr 51: 241–247, 1990
35. Johnson TN, Tucker GT, Tanner MS, Rostami-Hodjegan A: Changes inliver volume from birth to adulthood: A meta-analysis. Liver Transpl11: 1481–1493, 2005
36. DuBois D, DuBois EF: The measurement of the surface area of man.Arch Intern Med 15: 868–881, 1915
37. Efron B: The Jackknife, the Bootstrap and Other Resampling Plans,Philadelphia, Society for Industrial and Applied Mathematics, 1982
CLINICAL EPIDEMIOLOGYwww.jasn.org
J Am Soc Nephrol 22: 1517–1525, 2011 Normalization of GFR 1525