Embed Size (px)
Citation preview

Ghost Maculopathy: An Artifact on Near-InfraredReflectance and MultiColor Imaging Masquerading
as Chorioretinal Pathology
CLAUDINE E. PANG AND K. BAILEY FREUND
� PURPOSE: To describe the features of an artifact onnear-infrared reflectance andMultiColor imaging, termed‘‘ghost maculopathy,’’ and to illustrate how it maymasquerade as true chorioretinal pathology.� DESIGN: This was a retrospective, observational caseseries.� METHODS: The authors studied 144 eyes of 72 consec-utive patients in a vitreoretinal clinical practice, reviewingmultimodal imaging including color and red-free fundusphotography, fundus autofluorescence (FAF), near-infrared reflectance, MultiColor imaging, and spectral-domain optical coherence tomography (SD OCT).� RESULTS: In 36 of 144 eyes (25%), there was anappearance of a hyper-reflective spot on near-infraredreflectance and MultiColor imaging, located at the mac-ula, nasal or superonasal to the fovea, which did notcorrespond to any apparent lesion on color and red-freefundus photography, FAF, or SD OCT. This spot wastermed the ‘‘ghost image’’ in this phenomenon of ‘‘ghostmaculopathy.’’ The ghost image was present consistentlyon near-infrared reflectance andMultiColor imaging in all36 eyes at every imaging encounter, showing minimal andsubtle variability in its shape and location within eacheye; however, it showed large interindividual variabilityin size, shape, location, and reflectivity between differenteyes. Nine eyes were found to have a similar hyper-reflective spot resembling that in ghost maculopathy,but corresponding SD OCT images were consistentwith diagnoses of choroidal nevus, age-related maculardegeneration, and multifocal choroiditis. All eyes withghost maculopathy were found to be pseudophakic witha posterior chamber intraocular lens.� CONCLUSION: Ghost maculopathy is the phenomenonof an imaging artifact appearing at the macula on near-infrared reflectance and MultiColor imaging that occurspredominantly in pseudophakic patients and may bemistaken for true chorioretinal pathology. Awareness
Accepted for publication Mar 5, 2014.From The Vitreous, Retina, Macula Consultants of New York, New
York, New York (C.E.P., K.B.F.); LuEsther T. Mertz Retinal ResearchCenter, Manhattan Eye, Ear and Throat Hospital, New York, New York(C.E.P., K.B.F.); and Department of Ophthalmology, New YorkUniversity School of Medicine, New York, New York (K.B.F.).
Inquiries to K. Bailey Freund, Vitreous Retina Macula Consultants ofNew York, 460 Park Avenue, Fifth Floor, New York, NY 10022; e-mail:[email protected]
0002-9394/$36.00http://dx.doi.org/10.1016/j.ajo.2014.03.003
� 2014 BY ELSEVIER INC.
of this artifact is prudent to avoid misinterpretationof clinical findings and possible unnecessary over-investigation. (Am J Ophthalmol 2014;-:-–-.� 2014 by Elsevier Inc. All rights reserved.)
NEAR-INFRARED LIGHT IS WELL SUITED FOR USE IN
imaging the subretinal structures, as it largelyavoids absorption and reflection by the layers of
the neuroretina and penetrates readily to the level of theretinal pigment epithelium (RPE) and choroid.1 Dallowfirst suggested the use of near-infrared in 19742 but gainedlittle support at the time. In 1996, Elsner and associates3
demonstrated near-infrared visibility of subretinal struc-tures in macular degeneration using a confocal scanninglaser ophthalmolscope (SLO). Subsequently, this tech-nique has been extended to polarization-sensitive near-infrared and, only recently, near-infrared reflectanceimaging has been used to capture the appearance ofchoroidal neovascularization (CNV) in age-related macu-lar degeneration (AMD).4–6
The Heidelberg Spectralis (Heidelberg Engineering,Heidelberg, Germany), uses confocal SLO to achievehigh-contrast near-infrared reflectance images and appliesan 830 nm laser source to acquire high-reflectance imagesin the near-infrared. More recently, Heidelberg Engineer-ing has introduced MultiColor scanning laser imagingthat uses multiple laser colors (infrared [820 nm], green[515 nm], and blue [488 nm]) simultaneously to selectivelycapture and display information originating from differentretinal structures. Blue reflectance produces detailedimages of epiretinal membranes, retinal nerve fiber layerthinning, and macular pigment changes. Green laser pro-vides detailed views of retinal vasculature and intraretinallipid exudation, while infrared is useful for identifyingdrusen and RPE.7
It is well known that with near-infrared reflectance andMultiColor imaging, the normal foveal umbo can appear asa hyper-reflective spot;8,9 however, the appearance of otherhyper-reflective imaging artifacts has not been describedpreviously. As experience with these imaging techniquesis relatively new, interpretation of acquired images stillinvolves close examination and clinician experience.This study aims to highlight an artifact, unrelated to thefoveal umbo, that can occur with these imaging techniquesand may masquerade as true chorioretinal pathology.
1ALL RIGHTS RESERVED.

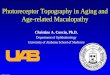
FIGURE 1. Near-infrared reflectance imaging showing the distinct difference between the normal foveal umbo and ghost maculop-athy. (Left) Near-infrared reflectance image showing a hyper-reflective spot at the normal foveal umbo. (Right) Near-infraredreflectance image showing a hyper-reflective artifact, termed ‘‘ghost image’’ (white arrow), superonasal to the fovea.
METHODS
THIS WAS A RETROSPECTIVE, OBSERVATIONAL CASE SERIES
of 72 consecutive patients seen by a single physician(K.B.F.) in a vitreoretinal referral practice located inNew York, New York, USA on 2 typical full-day consulta-tion clinic sessions. Patients with the appearance of ahyper-reflective spot at the macula on near-infrared reflec-tance that was differentiated from the normal hyper-reflectivity seen at the foveal umbo were identified(Figure 1). This spot was termed the ‘‘ghost image’’ inthis phenomenon of ‘‘ghost maculopathy.’’ Medical recordsand multimodal images including color and red-free fundusphotography, fundus autofluorescence (FAF), near-infraredreflectance, MultiColor scanning laser imaging, andspectral-domain optical coherence tomography (SD OCT)were reviewed. FAF, near-infrared reflectance, MultiColorimaging, and SD OCT were obtained with the HeidelbergSpectralis (Heidelberg Engineering, Heidelberg, Germany).Color and red-free fundus photographs were obtained withthe Topcon TRC-50IX (Topcon Corporation, Tokyo,Japan) fundus camera. All images of retrospective clinicvisits up to 4 years of retrospective follow-up were reviewed.This study had Western Institutional Review Boardapproval and was compliant with the Health InsurancePortability and Accountability Act.
RESULTS
IN 36 OF 144 EYES (25%), THERE WAS THE APPEARANCE OF A
hyper-reflective spot on near-infrared reflectance andMultiColor imaging, located at the macula, that did notcorrespond to any apparent lesion on color and red-freefundus photography, FAF, or SD OCT and was thereforegiven the term ‘‘ghost maculopathy.’’ The mean age of
2 AMERICAN JOURNAL OF
the 36 patients with ghost maculopathy was 83 years(52–100 years), 8 (22%) were male and 28 (78%) werefemale. All eyes with ghost maculopathy were found tohave the presence of a posterior chamber intraocular lens(PC-IOL) implanted at the time of cataract surgery.Among the 75 pseudophakic eyes, the prevalence of ghostmaculopathy was 48% (75/144). Of note, ghost maculop-athy was not seen in any of the 69 phakic eyes.The ghost image was present consistently on near-
infrared reflectance and MultiColor imaging in all 36eyes at every imaging encounter but never in FAF or SDOCT (Figure 2). Ghost maculopathy showed large interin-dividual variability in size, shape, location, and reflectivitybetween different eyes. Its appearance ranged from a small,well-circumscribed, circular or oval or crescent-shaped spotto a larger, more diffuse reflectance with indistinct borders.Its location could vary, although it was usually nasal orsuperonasal to the fovea. The ghost image always appearedas hyper-reflective, although its reflectance could vary fromsolid, bright white to a granular or speckled, less intensewhite (Figure 3).Ghost maculopathy showed minimal and subtle vari-
ability in its shape and location within each eye at everyclinic encounter of up to 4 years of follow-up visits(Figure 4). In 2 patients who had cataract surgery withinthe course of their follow-up, the appearance of the ghostimage was observed to occur only after the implantationof the intraocular lens.In an attempt to eliminate the artifact, repeated near-
infrared reflectance images at a single setting with varyingangles of incident light were obtained. This resulted in sub-tle shifts in the location of the lesion (Figure 5). The ghostimage could not be completely eliminated without compro-mising the image quality or resulting in a completeblackened-out fundus image where no details of the funduswere visible.
--- 2014OPHTHALMOLOGY

FIGURE 2. Multicolor images (with its components) and near-infrared reflectance images showing the appearance of the hyper-reflective ghost image (white arrows) superonasal to the fovea, which does not appear on fundus autofluorescence. (Top left) Multi-color image showing the ghost image superonasal to the fovea. (Top right) Infrared reflectance component showing the ghost image inthe same location as in the multicolor image. (Middle left) Green reflectance component showing the ghost image in the same locationas in the multicolor image. (Middle right) Blue reflectance component showing the ghost image in the same location as in the multi-color image. (Bottom left) Near-infrared reflectance showing the ghost image superonasal to the fovea, in the same location as in themulticolor images. (Bottom right) Fundus autofluorescence showing absence of ghost image.
In 9 eyes, we observed the appearance of a similar hyper-reflective spot resembling the ghost image. However, thesespots corresponded to true pathology seen on SD OCT im-ages and their diagnoses included choroidal nevus, AMD,and multifocal choroiditis (Figures 6, 7 and 8).
VOL. -, NO. - GHOST MACULOPATHY: A
In 4 eyes with AMD, the ghost image was observed inclose proximity to an area of geographic atrophy (GA),which also appeared as hyper-reflective on the near-infrared reflectance image. In all 4 cases, ghost maculop-athy masqueraded as a coalescent area of GA, which led
3N IMAGING ARTIFACT

FIGURE 3. Near-infrared reflectance images showing interindividual variability of size, shape, location, and reflectivity of ghostimage (white arrows). (Left) The ghost image appears as a small punctate, circular, solid, intensely hyper-reflective spot located super-onasal to the fovea. (Middle) The ghost image appears as a medium, oval, granular, and less intense hyper-reflective spot located super-onasal to the fovea. (Right) The ghost image appears as a large, diffuse, speckled, and low-intensity hyper-reflective spot locatedsuperonasal to the fovea. Incidentally, there is drusen located at the fovea resulting in hyper-reflectance, unrelated to the ghost image.
FIGURE 4. Near-infrared reflectance images of 3 consecutive clinic encounters of a 67-year-old female with a history of branchretinal vein occlusion and previous superior sectoral laser photocoagulation, showing subtle changes in shape and location of the ghostimage (white arrows) at each visit. (Left) Near-infrared reflectance image taken at the first clinic visit showing the ghost image locatednasal to the fovea. (Middle) Near-infrared reflectance image taken at the second clinic visit 6 months later showing very subtle changein shape and location of the ghost image. The ghost image is located slightly inferior to that in the prior visit. (Right) Near-infraredreflectance image taken at the third clinic visit 1 year later showing the ghost image with a similar shape and location to that in the firstvisit.
to the region of pathology appearing larger than it actuallywas (Figure 9). In 1 eye with AMD and CNV, the ghostimage appeared in close proximity to the area of CNVand gave the illusion of a larger CNV lesion than in reality(Figure 10).
DISCUSSION
THE PREVALENCE OF GHOST MACULOPATHY, AN ARTIFACT
seen on near-infrared reflectance and MultiColor imaging
4 AMERICAN JOURNAL OF
in a vitreoretinal referral practice, was approximately25%. Looking only at pseudophakic eyes, almost halfhad ghost maculopathy. We observed that ghost maculop-athy occurred exclusively in pseudophakic patients,which suggests that the hyper-reflective artifact occursbecause of reflections or scatter of near-infrared lightfrom the PC-IOL. It is possible that ghost maculopathymay also occur in patients with anterior chamber intraoc-ular lens (AC-IOL), possibly with a different position inthe macula; however, we did not have any patientswith AC-IOL in this study.
--- 2014OPHTHALMOLOGY

FIGURE 5. Repeated near-infrared reflectance images taken in a single setting by adjusting the angle of the incident light, in anattempt to eliminate the ghost image without blackening out the fundus, showing subtle changes in the size, shape, location, and reflec-tivity of the ghost image (white arrows), although no complete disappearance of the image. (Left) The ghost image is located just nasalto the fovea. (Middle) The ghost image appears inferior to the image in the left. (Right) The ghost image appears superior to the imagein the left but appears more faint and less distinct.
FIGURE 6. Near-infrared reflectance images showing the difficulty in distinguishing ghost maculopathy from choroidal nevus. (Topleft) Near-infrared reflectance image showing a hyper-reflective spot at the nasal juxtafoveal area (white arrow), which appears similarto a ghost image but is actually a choroidal nevus. (Bottom left) Corresponding spectral-domain optical coherence tomography (SDOCT) image through the white line in image above, showing a choroidal nevus causing focal choroidal thickening (double-headedarrow) just nasal to the fovea. (Top middle) Near-infrared reflectance image showing a hyper-reflective ghost image nasal to the fovea(white arrow) that has a similar appearance to a choroidal nevus. (Bottom middle) Corresponding SD OCT image through the whiteline in the image above showing no true pathology. (Top right) Near-infrared reflectance image showing a hyper-reflective spotsuperior to the fovea that resembles a ghost image (white arrow) but is actually a choroidal nevus. (Bottom right) CorrespondingSD OCT image through the white line in the image above showing a hyporeflective lesion in the choroid consistent with a choroidalnevus (white arrowhead).
Ghost maculopathy is seen in near-infrared reflectanceand MultiColor imaging but not on color fundus photog-raphy, red-free photography, or FAF. The total fundusreflectance of near-infrared light is up to 10 times higher
VOL. -, NO. - GHOST MACULOPATHY: A
than that of color and red-free fundus photographs.3 Thismay have contributed to a marked increase in near-infrared light scatter or reflections brought about by thePC-IOL compared to visible light in color and red-free
5N IMAGING ARTIFACT

FIGURE 7. Near-infrared reflectance images showing the similar appearance of the ghost image and geographic atrophy in age-relatedmacular degeneration. (Top left) Near-infrared reflectance image showing ghost image (white arrow), which appears as a bright whitespot with distinct borders. (Bottom left) Corresponding spectral-domain optical coherence tomography (SDOCT) image through thewhite line in the image above, showing no true pathology. (Top middle) Near-infrared reflectance image of a patient with age-relatedmacular degeneration showing a hyper-reflective spot of geographic atrophy that appears bright white with distinct borders locatednasal to the fovea and closely resembles the ghost image (white arrow) in the image on the left. (Bottom middle) CorrespondingSD OCT image through the white line in the image above, showing photoreceptor loss and outer retinal atrophy (white arrowhead),typical of geographic atrophy. (Top right) Near-infrared reflectance image showing a hyper-reflective spot that appears as a brightwhite spot with distinct borders. Although its appearance resembles a ghost image, it is located temporal to the fovea and is thereforeunlikely to be a ghost image. (Bottom right) Corresponding SDOCT image through thewhite line in the image above showing thinningand disruption of the outer retina, photoreceptor layer, and retinal pigment epithelium, consistent with atrophy (white arrowhead).
FIGURE 8. Near-infrared reflectance images showing the similar appearance of the ghost image and the atrophic spot in multifocalchoroiditis. (Top left) Near-infrared reflectance image showing a ghost image (white arrow) that appears as a small, punctate, brightwhite spot with distinct borders. (Bottom left) Corresponding spectral-domain optical coherence tomography (SD OCT) imagethrough the white line in the image above, showing no true pathology. (Top right) Near-infrared reflectance image showing a punctateatrophic spot (white arrow) in a patient with multifocal choroiditis or punctate inner choroidopathy, which appears as a small, punc-tate, bright white spot with distinct borders and closely resembles the appearance of a ghost image in the image on the left. (Bottomright) Corresponding SD OCT image through the white line in the image above, showing a small area of photoreceptor loss and outerretinal atrophy (white arrowhead) characteristic of an atrophic spot in multifocal choroiditis.
6 --- 2014AMERICAN JOURNAL OF OPHTHALMOLOGY

FIGURE9. Near-infrared reflectance images showing the presence of a ghost image after cataract surgery and the absence of the ghostimage before cataract surgery. (Left) Near-infrared reflectance (NIR) image showing a ghost image (white arrow) in close proximityto the area of geographic atrophy (GA) in a pseudophakic patient with age-related macular degeneration, giving the apparent appear-ance of a larger area of GA than in reality. Notice how the ghost image appears bright white with distinct borders, similar to the GA.(Right) NIR image of the same patient obtained before cataract surgery and implantation of intraocular lens. No ghost image ispresent, revealing the actual size of GA.
FIGURE 10. Near-infrared reflectance images of a patient with age-related macular degeneration, showing how ghost maculopathycan masquerade as a choroidal neovascularization (CNV). (Left) Near-infrared reflectance image showing a ghost image (whitearrow) in close proximity to the CNV, giving the apparent appearance of a larger area of CNV than in reality. (Top right) Correspond-ing spectral-domain optical coherence tomography (SDOCT) image through the white line in the image on the left, at the level of theghost image, showing no true pathology. (Bottom right) Corresponding SDOCT image through the black line in the image on the left,at the level of the neovascular tissue, showing a type 1 (sub–retinal pigment epithelium) CNV lesion (white arrowhead).
fundus photography, resulting in the appearance of theghost image—whereas in FAF imaging, the use of barrierfilters eliminates the appearance of such artifacts owingto reflections of light.
Ghost maculopathy, although created by the presence ofan intraocular lens, was not seen in all pseudophakicpatients. There are likely other factors that determine thepresence or absence of the ghost image. It is known thatthe normal foveal umbo shows an increased near-infraredreflectivity, especially in young individuals, and is broughtabout by the prefoveal inner limiting membrane owing tothe curvature of the retinal surface.8,9 We postulate thatfactors such as curvature of the retinal surface, angle ofincident light, angle of tilt of the intraocular lens, anddegree of posterior capsular opacification may contributeto the appearance and quality of the ghost image,
VOL. -, NO. - GHOST MACULOPATHY: A
including its size, shape, and reflectivity. These variablesmay also account for the large variability in theappearance of the ghost image in different patients.Despite the large interindividual variability seen
between patients, the ghost image appears fairly constantin each individual patient, with very subtle changes notice-able. Owing to the consistent appearance of the ghostimage at every imaging encounter, this hyper-reflectivespot can easily be mistaken for true chorioretinal pathol-ogy, such as choroidal nevus, GA, or CNV in AMD andpunctate atrophic spot in multifocal choroiditis or punctateinner choroidopathy. Hence, interpretation of near-infrared reflectance and MultiColor images requires corre-lation with color and red-free fundus photography, FAF,and SDOCT imaging in order to differentiate ghost macul-opathy from true pathology.
7N IMAGING ARTIFACT

In summary, ghost maculopathy is an imaging artifact innear-infrared reflectance and MultiColor imaging thatappears to occur fairly commonly in pseudophakic patients.
8 AMERICAN JOURNAL OF
It may be mistaken as true chorioretinal pathology by theobserver, and this study aims to raise greater awareness ofthis phenomenon.
BOTH AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OFInterest. K. Bailey Freund is a consultant for Genentech, Regeneron, Heidelberg Engineering, and Bayer. Claudine E. Pang has no proprietary or commer-cial interest in any of the materials discussed in this article. Funding/support: LuEsther T. Mertz Retinal Research Center, Manhattan Eye, Ear and ThroatHospital, New York and TheMacula Foundation, Inc, NewYork, NewYork. The funding organization had no role in the design or conduct of this research.Author contributions: design and conduct of the study (C.E.P., K.B.F.); collection (C.E.P., K.B.F.), management, analysis, and interpretation of the data(C.E.P., K.B.F.); preparation, review, and approval of the manuscript (C.E.P., K.B.F.).
REFERENCES
1. Theelen T, Hoyng CB, Klevering BJ. Near-infrared subretinalimaging in choroidal neovascularization. In: Holtz FG,Spaide RF, eds. Medical Retina: Focus on Retinal Imaging.Heidelberg: Springer; 2010:77–91.
2. Dallow RL. Color infrared photography of the ocular fundus.Arch Ophthalmol 1974;92(3):254–258.
3. Elsner AE, Burns SA,Weiter JJ, Delori FC. Infrared imaging ofsubretinal structures in the human ocular fundus. Vision Res
1996;36(1):191–205.4. Elsner AE, Weber A, Cheney MC, Vannasdale DA, Miura M.
Imaging polarimetry in patients with neovascular age-relatedmacular degeneration. J Opt Soc Am A Opt Image Sci Vis2007;24(5):1468–1480.
5. Semou O, Guigui B, Tick S, Coscas G, Soubrane G,Souied EH. Infrared features of classic choroidal neovasculari-zation in exudative age-related macular degeneration. Br JOphthalmol 2009;93(2):182–185.
6. Theelen T, Berenschot TT, Hoyng CB, BoonCJ, Klevering BJ.Near-infrared reflectance imaging of neovascular age-relatedmacular degeneraton. Graefes Arch Clin Exp Ophthalmol2009;247(12):1625–1633.
7. Murphy R. Multicolor fundus imaging prepares for debut.Retinal Physician 2012;9:77.
8. Gorrand JM, Alfieri R, Boire JY. Diffusion of the retinal layersof the living human eye. Vision Res 1984;24(9):1097–1106.
9. Gorrand JM, Delori FC. Reflectance and curvature of the innerlimiting membrane at the foveola. J Opt Soc Am A Opt ImageSci Vis 1999;16(6):1229–1237.
--- 2014OPHTHALMOLOGY

Biosketch
Dr Claudine E. Pang is a clinical ophthalmologist specializing in vitreoretinal diseases. She received her medical degree
from the National University of Singapore with Distinction, completed residency training at the Singapore National
Eye Centre and fellowship at the Vitreous Retina Macula Consultants of New York, Manhattan Eye, Ear and Throat
Hospital. She was conferred the Fellowship of the Royal College of Surgeons in Edinburgh (FRSCEd) and College of
Ophthalmologists, Academy of Medicine in Singapore (FAMS). She has interest in macular diseases, vitreomacular
surgery and ophthalmic imaging.
VOL. -, NO. - 8.e1GHOST MACULOPATHY: AN IMAGING ARTIFACT

Biosketch
K. Bailey Freund, MD is a Clinical Professor of Ophthalmology at New York University School of Medicine and a senior
partner at Vitreous Retina Macula Consultants of New York. Dr Freund is on the Editorial Board of the journal Retina. He
has authored over 160 peer-reviewed scientific manuscripts and numerous book chapters. He is a recipient of the Young
Investigator Award from the Macula Society.
8.e2 --- 2014AMERICAN JOURNAL OF OPHTHALMOLOGY