Embed Size (px)
DESCRIPTION
How to assess the GI system for nursing
Citation preview

GASTROINTESTINAL SYSTEMASSESSMENT

PYRAMID POINTSTechnique for abdominal assessmentAssessment of risk factors associated with
gastrointestinal (GI) disordersPreprocedure and postprocedure
interventions for diagnostic studiesCommon laboratory studies related to the
gastrointestinal tract and their relationship to gastrointestinal disorders

RISK FACTORS OF GI DISORDERSFamily history of GI disordersChronic laxative useTobacco useChronic alcohol useChronic high stress levelsAllergic reactions to food or medications Chronic use of aspirin or nonsteroidal
antiinflammatory drugs (NSAIDs)

RISK FACTORS OF GI DISORDERSLong-term GI conditions such as ulcerative
colitis may predispose to colorectal cancerPrevious abdominal surgery or trauma may
lead to adhesionsNeurological disorders can impair movement,
particularly with chewing and swallowingCardiac, respiratory, and endocrine disorders
may lead to constipationDiabetes mellitus may predispose to oral
candida infections

UPPER GI TRACT STUDY (BARIUM SWALLOW)
From Zakus SM: Clinical procedures for medical assistants, ed. 3, St. Louis, 1995, Mosby.

UPPER GI TRACT STUDY (BARIUM SWALLOW)POSTPROCEDURE
A laxative may be prescribed Instruct the client to increase oral fluids to
help pass the bariumMonitor stools for the passage of barium
(stools will appear chalky white) because barium can cause a bowel obstruction

LOWER GI TRACT STUDY (BARIUM ENEMA)
DESCRIPTIONA fluoroscopic and radiographic examination of
the large intestine after rectal instillation of barium sulfate
May be done with or without air

LOWER GI TRACT STUDY (BARIUM ENEMA)
From Heuman DM, Mills AS, McGuire HH: Gastroenterology, Philadelphia, 1997, W.B. Saunders.

LOWER GI TRACT STUDY (BARIUM ENEMA)PREPROCEDURE
A low-residue diet for 1 to 2 days prior to the test
A clear liquid diet and a laxative the evening before the test
NPO after midnight prior to the day of the testCleansing enemas on the morning of the test

LOWER GI TRACT STUDY (BARIUM ENEMA)POSTPROCEDURE
Instruct the client to increase oral fluids to help pass the barium
Administer a mild laxative as prescribed to facilitate emptying of the barium
Monitor stools for the passage of bariumNotify the physician if a bowel movement does
not occur within 2 days

GASTRIC ANALYSIS
DESCRIPTION The passage of a nasogastric (NG) tube into
the stomach to aspirate gastric contents for the analysis of acidity (pH), appearance, and volume; the entire gastric contents are aspirated and then specimens are collected every 15 minutes for 1 hour
Histamine or pentagastrin may be administered subcutaneously to stimulate gastric secretions; may produce a flushed feeling

GASTRIC ANALYSIS
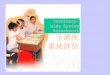
DESCRIPTION Esophageal reflux of gastric acid may be
performed by ambulatory pH monitoring; a probe is placed just above the lower esophageal sphincter, is connected to an external recording device, and provides a computer analysis and graphic display of results

MANOMETRY TUBES AND pH PROBE
From Beare, P. & Myers, J. (1998). Adult health nursing, ed 3, St Louis: Mosby.

GASTRIC ANALYSIS
PREPROCEDUREFasting for 8 to 12 hours prior to the testAvoid tobacco and chewing gum for 6 hours
prior to the testMedications that stimulate gastric secretions
are withheld for 24 to 48 hoursPOSTPROCEDURE
May resume normal activitiesRefrigerate gastric samples if not tested within
4 hours

UPPER GI FIBEROSCOPY
DESCRIPTIONAlso known as esophagogastroduodenoscopy
(EGD)Following sedation, an endoscope is passed
down the esophagus to view the gastric wall, sphincters, and duodenum; tissue specimens can be obtained

ESOPHAGOGASTRODUODENOSCOPY
From Ignatavicius, D. & Workman, M. (2002). Medical-surgical nursing: Critical thinking for collaborative care, ed 4, Philadelphia: W.B. Saunders.

UPPER GI FIBEROSCOPY
PREPROCEDURENPO for 6 to 12 hours prior to the testA local anesthetic (spray or gargle) is
administered along with midazolam (Versed) IV (provides conscious sedation and relieves anxiety) just before the scope is inserted
Atropine may be administered to reduce secretions, and glucagon may be administered to relax smooth muscle

UPPER GI FIBEROSCOPY
PREPROCEDUREClient is positioned on the left side to facilitate
saliva drainage and to provide easy access of the endoscope
Airway patency is monitored during the test and pulse oximetry is used to monitor oxygen saturation; emergency equipment should be readily available

UPPER GI FIBEROSCOPY
POSTPROCEDURENPO until the gag reflex returns (1 to 2 hours)Monitor for signs of perforation (pain,
bleeding, unusual difficulty swallowing, elevated temperature)
Maintain bed rest for the sedated client until alert
Lozenges, saline gargles, or oral analgesics can relieve minor sore throat after the gag reflex returns

ANOSCOPY, PROCTOSCOPY, AND SIGMOIDOSCOPY
ANOSCOPYUse of a rigid scope to examine the anal canal;
client is placed in the knee-chest position with the back inclined at a 45-degree angle
PROCTOSCOPY AND SIGMOIDOSCOPYUse of a flexible scope to examine the rectum
and sigmoid colon; client is placed on the left side with the right leg bent and placed anteriorly
Biopsies and polypectomies can be performed

ANOSCOPY, PROCTOSCOPY, AND SIGMOIDOSCOPY
PREPROCEDUREEnemas until the returns are clear
POSTPROCEDUREMonitor for rectal bleeding and signs of
perforation

FIBEROPTIC COLONOSCOPYDESCRIPTION
A fiberoptic endoscopy study in which the lining of the large intestine is visually examined; biopsies and polypectomies can be performed
Cardiac and respiratory function is monitored continuously during the test
Performed with the client lying on the left side with the knees drawn up to the chest; position may be changed during the test to facilitate passing of the scope

FIBEROPTIC COLONOSCOPY
From Chabner D: The Language of Medicine, ed. 6, Philadelphia, 2001, W.B. Saunders.

FIBEROPTIC COLONOSCOPYPREPROCEDURE
Adequate cleansing of the colon is necessaryA clear liquid diet is started at noon on the day
before the testConsult with the physician regarding medications
that must be withheld prior to the testClient is NPO after midnight on the day before the
testMidazolam (Versed) IV is administered to provide
sedationGlucagon may be administered to relax smooth
muscle

FIBEROPTIC COLONOSCOPYPOSTPROCEDURE
Provide bed rest until alertMonitor for signs of perforationInstruct the client to report any bleeding to the
physician

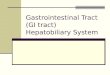
LAPAROSCOPY (PERITONEOSCOPY)DESCRIPTION
Performed with a fiberoscopic laparoscope that allows direct visualization of organs and structures within the abdomen
Biopsies may be obtained

LAPAROSCOPY: PLACEMENT OF TROCARS
From Chabner D: The Language of Medicine, ed. 6, Philadelphia, 2001, W.B. Saunders.

CHOLECYSTOGRAPHY
DESCRIPTIONPerformed to detect gallstones and to assess
the ability of the gallbladder to fill, concentrate its contents, contract, and empty

CHOLECYSTOGRAPHY
PREPROCEDUREAssess allergies to iodine or seafoodContrast agents are administered 10 to 12
hours (evening before) before the testClient is NPO after the contrast agent is
administeredInstruct the client that if a rash, itching, hives,
or difficulty breathing occurs after taking the contrast agent, to report to the emergency room

CHOLECYSTOGRAPHY
POSTPROCEDUREInform the client that dysuria is common
because the contrast agent is excreted in the urine
A normal diet may be resumed (a fatty meal may enhance excretion of the contrast agent)

ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY (ERCP)
DESCRIPTIONExamination of the hepatobiliary system via a
flexible endoscope inserted into the esophagus to the descending duodenum; multiple positions are required during the procedure to pass the endoscope
If medication is administered prior to the procedure, the client is monitored closely for signs of respiratory and central nervous system depression, hypotension, oversedation, and vomiting

ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY (ERCP)
From Beare, P. & Myers, J. (1998). Adult health nursing, ed 3, St Louis: Mosby.

ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY (ERCP)
PREPROCEDUREClient is NPO for several hours prior to the
procedureSedation is administered prior to the
procedure POSTPROCEDURE
Monitor vital signsMonitor for the return of the gag reflexMonitor for signs of perforation or infection

PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAPHY
DESCRIPTIONInvolves the injection of dye directly into the
biliary treeThe hepatic ducts within the liver, the entire
length of the common bile duct, the cystic duct, and the gallbladder are clearly outlined

PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAPHY
From Beare, P. & Myers, J. (1998). Adult health nursing, ed 3, St Louis: Mosby.

PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAPHY
PREPROCEDUREClient is NPOSedating medication is administered
POSTPROCEDUREMonitor vital signsMonitor for signs of bleeding, peritonitis, and
septicemia; report the presence of pain immediately
Administer antibiotics as prescribed to reduce the risk of sepsis

PARACENTESIS
DESCRIPTIONTransabdominal removal of fluid from the
peritoneal cavity for analysis

PARACENTESIS
From Beare, P. & Myers, J. (1998). Adult health nursing, ed 3, St Louis: Mosby.

PARACENTESIS
PREPROCEDUREObtain informed consentVoid prior to the start of procedure to empty
bladder and to move bladder out of the way of the paracentesis needle
Measure abdominal girth, weight, and baseline vital signs
Note that the client is positioned upright on the edge of the bed with the back supported and the feet resting on a stool (Fowler’s position is used for the client confined to bed)

PARACENTESIS
POSTPROCEDURE Monitor vital signsMeasure fluid collected, describe, and recordLabel fluid samples and send to the laboratory
for analysisApply a dry sterile dressing to the insertion
site; monitor site for bleedingMeasure abdominal girth and weight

PARACENTESIS
POSTPROCEDURE Monitor for hypovolemia, electrolyte loss,
mental status changes, or encephalopathyMonitor for hematuria due to bladder traumaInstruct the client to notify the physician if the
urine becomes bloody, pink, or red

LIVER BIOPSY
DESCRIPTIONA needle is inserted through the abdominal
wall to the liver to obtain a tissue sample for biopsy and microscopic examination

LIVER BIOPSY
From Black, J., Hawks, J., & Keene, A. (2001). Medical-surgical nursing: Clinical management for positive outcomes, ed 6, Philadelphia: W.B. Saunders.

LIVER BIOPSY
PREPROCEDUREObtain informed consentAssess results of coagulation tests
(prothrombin time, partial thromboplastin time, platelet count)
Administer a sedative as prescribedNote that the client is placed in the supine or
left lateral position during the procedure to expose the right side of the upper abdomen

LIVER BIOPSY
POSTPROCEDUREAssess vital signs Assess biopsy site for bleedingMonitor for peritonitisMaintain bed rest for several hoursPlace client on the right side with a pillow
under the costal margin to decrease the risk of hemorrhage, and instruct the client to avoid coughing and straining
Instruct the client to avoid heavy lifting and strenuous exercise for 1 week

GI MOTILITY STUDIESRADIONUCLIDE TESTING
Assesses gastric emptying and colonic emptying time
A capsule containing radioactive material is administered to the client and the time it takes for the radioactive material to move through the colon indicates colonic motility
ELECTROGASTROGRAPHYUsed to detect motor or neurological
dysfunction in the stomach; records gastric electrical activity

GI MOTILITY STUDIESESOPHAGEAL MANOMETRY
Detects motility disorders of the esophagus and lower esophageal sphincter
Client is NPO for 8 to 12 hours before the test and medications that affect GI motility are withheld
GASTROINTESTINAL, SMALL INTESTINAL, AND COLONIC MANOMETRY Evaluates delayed gastric emptying and gastric
and intestinal motility disorders; often is an ambulatory outpatient procedure that lasts 24 to 72 hours

GI MOTILITY STUDIESANORECTAL MANOMETRY
Measures the resting tone and contractibility of the anal sphincters to evaluate the client with chronic constipation or fecal incontinence; phosphosoda or a cleansing enema is administered 1 hour prior to the test
RECTAL SENSORY FUNCTION TESTEvaluates rectal sensory function and
neuropathy to evaluate the client with chronic constipation, diarrhea, or incontinence

DEFECOGRAPHYMeasures anorectal functionThick barium is instilled into the rectum,
fluoroscopy is performed, and the function of the rectum and anal sphincter is visualized while the client attempts to pass the barium
Digital subtraction methods may be used for more rapid imaging and mapping of rectal evacuation
No preparation is required

STOOL SPECIMENSIncludes inspecting the specimen for
consistency and color and testing for occult blood
Tests for fecal urobilinogen, fat, nitrogen, parasites, pathogens, food substances, and other substances; these tests require that the specimen be sent to the laboratory
Random specimens are promptly sent to the laboratory

STOOL SPECIMENSQuantitative 24- to 72-hour collections must
be kept refrigerated until they are taken to the laboratory
Some specimens require that a certain diet be followed or that certain medications be withheld; check agency guidelines regarding specific procedures

HYDROGEN BREATH TEST
Evaluates carbohydrate absorption by determining the amount of hydrogen expelled in the breath after it is produced in the colon and absorbed in the blood
Used to aid in the diagnosis of bacterial overgrowth in the intestine

UREA BREATH TEST
Detects the presence of Helicobacter pylori, the bacteria that causes peptic ulcer disease
The client consumes a capsule of carbon-labeled urea and provides a breath sample 10 to 20 minutes later

UREA BREATH TESTClient is instructed to avoid antibiotics or
bismuth subsalicylate (Pepto-Bismol) for 1 month before the test; sucralfate (Carafate) and omeprazole (Prilosec) for 1 week before the test; and cimetidine (Tagamet), famotidine (Pepcid), ranitidine (Zantac), or nizatidine (Axid) for 24 hours before breath testing
Helicobacter pylori can also be detected by assessing serum antibody levels

LIVER AND PANCREAS LABORATORY STUDIES
ALKALINE PHOSPHATASEReleased during liver damage or biliary
obstructionPROTHROMBIN TIME (PT)
Prolonged with liver damageSERUM AMMONIA
Assesses the ability of the liver to deaminate protein by-products
LIVER ENZYMES (TRANSAMINASE STUDIES)Elevated with liver damage

LIVER AND PANCREAS LABORATORY STUDIESCHOLESTEROL
Increase indicates pancreatitis or biliary obstruction
BILIRUBINIncrease indicates liver damage or biliary
obstruction
AMYLASE AND LIPASEElevations indicate pancreatitis
Refer to module entitled Laboratory Values for information regarding normal liver and pancreas laboratory levels

ABDOMINAL ASSESSMENT
Inspect skin for color, abnormalities, contour, and tautness, and the abdomen for distension
Auscultate for bowel soundsPercuss for air or solidsPalpate for tenderness

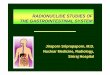
SYSTEMATIC ROUTE FOR ABDOMINAL PERCUSSION
From Beare, P. & Myers, J. (1998). Adult health nursing, ed 3, St Louis: Mosby.

ASSESSMENT FOR BOWEL SOUNDS
Auscultate bowel sounds before percussion and palpation
Normal bowel sounds occur 5 to 30 times a minute or every 5 to 15 seconds
Auscultate in all abdominal quadrantsListen at least 5 minutes in each quadrant
before assuming sounds are absent

QUADRANTS OF THE ABDOMEN
From Black, J., Hawks, J., & Keene, A. (2001). Medical-surgical nursing: Clinical management for positive outcomes, ed 6, Philadelphia: W.B. Saunders.