Embed Size (px)
Citation preview

Claire Houston, RN
Giant aneurysm surgery
Overall surgical morbidity and mortali- ty rates have not been uniformly good with standard surgical techniques for giant aneurysms, so a more radical ap- proach using hypothermia and cardiac arrest has been instituted at Stanford University Medical Center in Califor- nia. Hypothermia and elective circula- tory arrest were first used in surgery on such lesions in the early 1960s. This method created a bloodless field, but with the metabolic difficulties, hemor- rhagic complications, and technical problems, the hazards often outweighed the benefits. Cannulation was done by the open chest procedure, which is more traumatic than the femoral artery can- nulation the Stanford team uses.
The technique was abandoned as neurosurgery became more refined and other operative methods developed in the field. Use of the operating micro- scope, controlled hypotension, better neuroanesthesia, and a better under- standing of the time for surgery made the morbidity of aneurysm without car- diac arrest more acceptable. In the meantime, cardiac surgeons continued to use hypothermia and circulatory ar- rest. As a result, their technical ad-
Claire Houston, RN, is a neurosurgical nurs- ing specialist in the operating room at Stan- ford (Calif) University Medical Center. She is a graduate of St Mary’s Hospital School of Nursing, Brooklyn, NY.
vances in pump oxygenators and me- chanical heat exchangers, as well as the availability of multiple clotting factors, have made neurosurgery using these methods far safer. The technique is used, however, only when the conven- tional approach would be unsatisfacto- ry.
An aneurysm forms when a weak arterial wall bulges into a thin-walled sac. As the sac grows under the force of arterial blood pressure, its dome thins and may rupture. Patients who survive the initial rupture are in danger of dying from subsequent hemorrhage un- less the aneurysm is excluded from the cerebral circulation. Giant aneurysms are greater than 2.5 cm in diameter. They are uncommon, occurring in 3% to 5% of patients suffering from intracra- nial aneurysms.2 Only % of the general population have intracranial aneu- rysms.
Giant aneurysms are said usually to present as mass lesions, compared with smaller aneurysms that first appear with symptoms of acute subarachnoid hem~rrhage .~ This, however, has not been the experience a t Stanford. Of thirteen patients with giant aneu- rysms, seven presented with subarach- noid hemorrhage, and one had a fatal subarachnoid hemorrhage during an- giogr aph y.
Surgery cannot be done immediately for patients who have a subarachnoid bleed because of arterial vasospasm and
643 AORN Journal, March 1983. Vol 37, No 4

cerebral edema. Arterial vasospasm is an abnormal narrowing of the large ce- rebral a r t e r i e ~ . ~ Cerebral edema is an increase in the tissue fluid content re- sulting in increased tissue v01ume.~ It is best to delay surgery until the cerebral edema and vasospasm have cleared, as shown by a normal neurological exam or stable neurological deficit and an an- giogram showing no vasospasm.
While waiting to intervene surgi- cally, the staff takes measures to pre- vent further bleeding and resolve cere- bral swelling. Bed rest with sedation and antihypertensive drugs, such as so- dium nitroprusside, methyldopa (Al- domet), reserpine, and chlorothiazide (Diuril), are recommended to keep blood pressure down. The antifibrinolytic agent aminocaproic acid (Amicar) is used to prevent lysis of the clot sealing off the aneurysm. Dexamethasone (De- cadron) may help resolve the cerebral edema, and anticonvulsants are given to prevent seizures. There is no effective medication to treat the vasospasm. Usually, it will resolve one to three weeks after the initial bleed.6
Surgery on a giant aneurysm is diffi- cult. Because of its size and poor visual- ization of surrounding vital structures,
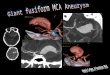
Fig 1. Preoperative CT scans show a 4 cm lefi middle cerebral artery aneurysm with dense adhesions and calcification.
dissection is difficult. Occluding the sac while maintaining the patency of the parent vessel and its branches is an ar- duous task. Although the brain cannot tolerate ischemia for more than a few minutes without damage, hypothermia does help to protect the brain against anoxia.'
Hypothermia and cardiac arrest were first used in neurosurgery at Stanford in November 1978. The surgical tech- nique evolved from that used at the medical center for aortic arch replace- ment.8 In the first case, the patient had a large left middle cerebral artery aneu- rysm that had been operated on twice previously (Fig 1, 2, and 3). His first surgery had been done in 1969 after a subarachnoid hemorrhage, when the aneurysm was wrapped in muslin gauze. At that time, his recovery was uneventful, but he complained of in- creasingly Severe headaches over the next six years.
In 1975, a repeat angiogram demon- strated a larger aneurysm. A second craniotomy was performed, but the sur- geon abandoned the procedure due to dense adhesions surrounding the domi- nant frontal and temporal lobes. Post- operative angiography showed two of
644 AOKN Journal, March 19R3. Vol 37, No 4

Fig 2. A preoperative angiogram of the left middle cerebral artery aneurysm. Note the stretch on the branch due to the size of the aneurysm. Fig 3. Postoperative angiogram of the same aneurysm. Note the curly appearance of the branch now that the aneurysm has been eradicated from the cerebral circulation.
the three middle cerebral branches had been occluded, rendering the patient acutely aphasic and hemiplegic. The pa- tient gradually recovered speech and right-side function but remained inca- pacitated by seizures and headache.
In 1977, the patient came under the care of the Stanford Neurosurgical De- partment. Observation for one year documented progressive incapacitation from seizures, headache, nausea, vomit- ing, dementia, and memory loss. It was felt that another attempt to eradicate the aneurysm was warranted. Because of the size of the aneurysm, now mea- suring 4 cm, and the dense adhesions, the only approach would be through the aneurysm to suture its orifice. Hypo-
thermia with circulatory arrest was nec- essary to do t h k 9
The primary concept of hypothermia is to decrease cellular metabolism and therefore oxygen consumption of the heart and brain during an interruption in circulation. To achieve hypothermia, heat must be lost faster than it is pro- duced. Patients are either cooled by sur- face-induced hypothermia, blood- stream cooling, or a combination of both methods.1°
Preparation for the case started days before the surgery. Neurosurgeons, cardiac surgeons, anesthesiologists, op- erating room nurses, blood bank per- sonnel, and perfusionists collaborated in the planning. Unfortunately, the En-

gineering Department was not in- formed. On the morning of surgery, there was far too much electrical equipment for the number of circuits in the room. At 6 am, a n engineer was routing extension cords up and down the hall to avoid overloading any cir- cuit. Fortunately, surgery went on without delay.
Now there is a schematic drawing of the electrical routing. Following this diagram, someone checks to be sure all necessary equipment is in the room and in working order. Although the neuro- surgery room is large by usual stan- dards, it seems to shrink as equipment is added.
The patient is placed on the operating room bed with a hypothermia-hyper- thermia blanket under him. The blan- ket is not connected to the bath coolant until the patient is asleep. Because of the number of lines and monitors, the bed is positioned so i t will not have to be relocated after induction.
Monitored variables include electro- cardiogram (ECG), arterial pressure, central venous pressure (CVP), expira- tory COz and 02, urine output, and na- sopharyngeal and rectal temperature. Induction of anesthesia is done with narcotics to avoid myocardial depres- sion. Surface cooling is started after the induction of anesthesia to avoid a hy- pertensive response and cardiovascular stress. The blanket is perfused with fluid at 4 "C. We do not pack the patient in ice. The patient is vasodilated using nitroprusside and, if necessary, chlor- promazine to accelerate heat exchange. The nitroprusside also induces hypo- tension, which is necessary when oper- ating on an aneurysm because it reduc- es the pressure in the sac."
Approximately two to three units of the patient's own blood are withdrawn and replaced with four or five liters of chilled normal saline. The purpose is to bring the patient's packed cell volume
to about 20%. Hemodilution is neces- sary to compensate for the rise in blood viscosity with the decreasing tempera- ture, which would otherwise cause red cell sludging and impair perfusion of vital organs. All fluids given after the induction are chilled to assist in the cooling. Since the patient's own blood is given back after rewarming, it escapes the trauma of perfusion and hypother- mia, thus maintaining clotting factors
The patient's skin is prepared from the head to just below the knees. The craniotomy draping is done in conjunc- tion with the cardiovascular draping, but we maintain a field isolated from theirs.
The neurosurgical procedure is begurl immediately, with careful attention to meticulous hemostasis. While the neu- rosurgical team is exposing the lesion., the cardiovascular team exposes the femoral vessels in preparation for can- nulation. Heparin (300 unitdkg) is given after the most surgical exposure that can be done safely is completed. The duration of bypass and the depth of' hypothermia should be the least that protects the patient adequately during surgery.12
Cannulation for cardiopulmonary bypass is performed by inserting a long
Bleeding is a critical problem for the patient.
no 28 catheter in the right femoral vein to the right atrium. A second catheter is placed at the iliac bifurcation via the left femoral vein for venous return. A no 22 vascular catheter is placed in the right femoral artery for arterial return.
6.16 AOKN Journal, March 19x3. Vol 37. No 4

PUMP OXYGENATOR
HEAT EXCHANGER PULSATILE ASSIST DEVICE
L e f t Femoral A r t e r d v J 7 Riaht Atr ium
\
2.5 - 3.5 Flow ( l i t e r s h i n )
Fig 4. Cannulation for extracorporeal circulation is through the femoral artery
The left femoral artery is clamped be- cause the left femoral vein is occluded (Fig 4). Cardiopulmonary bypass is ini- tiated with the patient's temperature at about 28 "C to 30 "C. This is necessary because spontaneous fibrillation of the heart occurs between 23 "C and 27 "C. The patient is then cooled to a target temperature of 17 "C to 20 "C. Cooling occurs a t approximately 0.2 "C per min- ute.I3
The patient is positioned with the head elevated above the level of the heart so that when the pump is stopped and the venous lines opened, the avail- able blood volume is drained into the pump reservoir, markedly reducing the brain bulk and collapsing the aneu- rysm.14 At this point, the neurosurgical pathology is dealt with. If any further dissection around the aneurysm is ne- cessary, i t can be handled relatively
easily because the former mass of the aneurysm has been drained. It is much like a deflated balloon. The anatomy can be clearly seen and the vascular structures identified with the operating microscope. A decision can be made about the best method to obliterate the aneurysm-to open the aneurysm and oversew the orifice or to ligate the base with a ligature, a clip, or a seriesof clips, preserving the parent artery and its branches.
An advantage of this technique is that even if the aneurysm ruptures prematurely, which has happened, a dry field can be achieved as soon as the blood volume can be drained into the pump and the pump turned off. After the aneurysm is obliterated, the pump is restarted, and the surgical field is in- spected to be certain no major arterial bleeders are left unsecured.15 Rewann-
AOKN Journal. March 1983. Vol 37. No 4 1; 17

ing of the patient is begun immediately after a dry field is attained and the neu- rosurgeon is satisfied with the craniot- omy site.
Warming is accomplished without delay by disconnecting the hypothermia blanket from the hypothermia machine when the patient's temperature reaches about 20 "C. This allows us to start warming the water bath early. In addi- tion to the blanket, a Brown-Harrison heat exchanger is used with the prime kept about 10 "C above the patient's blood temperature. Activated coagula- tion times are measured after the hepa- rin is given, after bypass is begun, at every 5 "C during rewarming up to 30 "C, and then as indicated after that.
If the patient does not spontaneously defibrillate by the time the temperature reaches 28 "C, the patient is converted with an external shock of 300 watt sec- onds. We are prepared to open the chest if the external shock is not sufficient. So far, this has not been necessary. In fact, most patients have defibrillated spon- taneously just above 27 "C. About five minutes after defibrillation, the blood in the pump is returned to the patient, increasing the blood volume.
Vasodilators are used at this point to improve the blood flow distribution.
Patients recover with relatively few complications.
It usually takes 45 minutes to 1 hour for the patient's temperature to come up to 36 "C. When the temperature reaches 36 "C, bypass is terminated. Protamine sulfate (10 mg/1000 units of the initial heparin dose) is given slowly as de-
cannulation is performed. Then the femoral incisions are closed. At this time, the patient is usually given sir: units of platelets, three units of fresh frozen plasma, two units of the patient's own blood, and two units of Factor IX. complex (Proplex), in that order. Clot- ting studies are imperative.
Although bleeding from the brain is usually minimal, epidural oozing is often copious in spite of the dural tent- ing sutures that are placed at the be- ginning of the case. The dural tenting sutures are placed between the dura and the bone edge. The tension on the dura assists in the control of the epidur- al bleeding. Also, absorbable gelatin sponge and topical thrombin can be used to assist in the control of bleeding. All bleeding can be controlled with the administration of the clotting factors, but the waiting period is often difficult for the neurosurgical team.
Clotting disorders occur in about 68% to 1OO?h of patients during and after a pump run. However, bleeding is a seri- ous problem for the cardiac surgeon in only 2% to 3% of the patients.16 In neurosurgical patients, it is much more critical; they are unable to cope with anything less than absolute intracra- nial hemostasis.
When the craniotomy field is dry, the dura is closed, the bone flap is replaced, and the galea and skin are closed in the usual manner. All patients have an in- tracranial pressure (ICP) monitor in- serted before the end of the case. It is usually inserted through a separate bur hole, preferably on the nondominant side.17 ICP monitoring is essential be- cause an increase in the volume of the brain, vascular volume, or the cerebro- spinal fluid can only be a t the expense of the other two and will cause a precipi- tous increase in the ICP.
Any rise in the ICPmust be dealt with immediately because of the danger of herniation of the brain stem, which
6.1X AORN Journal. March 1983, Vol 37, No 4

Fig 5. A preoperative angiogram of a giant basilar artery aneurysm.
quickly causes irreversible damage to vital structures in the medulla control- ling respirations and cardiac function.'* ICP monitoring is especially critical immediately after surgery because pa- tients usually sleep from 8 to 48 hours postoperatively. Because they do sleep, the conventional neurological checks such as changes in the level of con- sciousness, reaction and size of pupils, movement of extremities, and any change in vital signs are not as valuable as the ICP monitor in caring for these patients. After surgery, all patients go to the intensive care unit (ICU) and re- main there until they are ready to re- turn to the neurosurgical unit. This time varies with each individual. One patient stayed in ICU less than 24 hours, while another stayed almost 2 weeks.
Although our series of patients is small, the results are encouraging. An- giograms of a basilar artery aneurysm are seen in Figs 5 and 6. Of 12 patients and 13 possible procedures, only 11 pro- cedures were done, because 2 patients
Fig 6. A postoperative angiogram of a giant basilar artery aneurysm. Note the series of clips that were applied to occlude the aneurysm sac yet maintain the patency of the basilar artery and its branches.
died before surgery. There has been no operative mortality. One patient had mirror image giant aneurysms of the middle cerebral arteries. Because she bled from the right side, that aneurysm was clipped first. She returned to the hospital two months later, and the left side aneurysm was operated on in an elective procedure, also under hypo- thermic arrest.
There have been two permanent com- plications. One patient had a stroke six months postoperatively with a homon- ymous hemianopsia due to a late thrombosis of the residual sac of aneu- rysm. The second permanent complica- tion, also a homonymous hemianopsia, occurred immediately postoperatively, probably due to coagulation of a small vessel at the time of surgery.
There have been seven transient complications in six patients. One pa- tient had small pulmonary emboli a t about three months postoperatively. This patient had prolonged preopera- tive bedrest and Amicar therapy (24 glday) before surgery. She recovered
AORN Journal . March 1983. Vol 37. No 4 649

without problems following three months of anticoagulation treatment. Another patient developed signs of thrombophlebitis one week postopera- tively. A Greenfield umbrella was in- serted from the femoral vein of the good leg to the vena cava. In one patient, a small asymptomatic intracerebral he- matoma appeared on a computed tomog- raphy scan just under the site of the frontal lobe retractor, but it was re- solved without treatment, and the pa- tient suffered no neurological deficit. Two patients had postoperative ipsilat- era1 third nerve palsy and contralateral hemiparesis. There were also two with mild dysphasia. All of these complica- tions have cleared except for the two patients with the homonymous hemi- anopsia. Three patients have had a hep- arin rebound about three hours postop eratively; these were easily reversed with an additional 5 to 10 cc of prota- mine sulfate.
Hypothermia is not without prob- lems. Bleeding is a major consideration. Although our patients have ranged in age from 32 to 67, we have not had any patients with advanced cardiovascular, renal, or hepatic disease. This has con- tributed to the success of the series. Cer- tainly, patients with any of these dis- eases should be considered for surgery if they have an aneurysm requiring hypo- thermia. They would, however, be at greater risk. It must also be understood that we are treating aneurysms previ- ously thought inoperable in most situa- tions.
We believe that the success of the surgery depends on team work by neu- rosurgeons, cardiac surgeons, anesthe- sia personnel, perfusionists, and nurse specialists. Each person on each team must not only be confident of his or her own ability but must be confident of the other team members as well. No one person or group can be successful with- out the others. It is truly a multidisci-
plinary approach. With better under- standing of the physiology and techni- cal advances, the work of the cardiovas- cular support team, and advances :in neuroanesthesia, patients recover with relatively few complications. [I
Notes 1. G D Silverberg, B A Reitz. A K Ream, “Hypo-
thermia and cardiac arrest in the treatment of giant aneurysms of the cerebral circulation and heman- gioblastoma of the medulla,” Journal of Neurosur- gery 55 (September 1981) 337-346.
2. Silverberg, Reitz. Ream, “Hypothermia and cardiac arrest”; C G Drake et at, “The use of extra- corporeal circulation and profound hypothermia irl the treatment of ruptured intracranial aneurysms,” Journal of Neurosurgery 21 (July 1964) 575-581 ; T P Morley. H W K Barr, “Giant intracranial aneu- rysms: Diagnosis, course and management,” Clin- ical Neurosurgery 16 (1969) 73-94; T Omuma, J Suzuki, “Surgical treatment of giant intracraniaA aneurysms.” Journal of Neurosurgery 51 (Jul,~
3. D Judice, E D Connolly, “Foramen magnum syndrome caused by a giant aneurysm of the poste- rior inferior cerebral artery: Case report,” Neurosur- gery 48 (April 1978) 639-641.
4. P M Pacheco, “Cerebral artery vasospasni and current trends of treatment.” JournalofNeuro- surgical Nursing 11 (September 1979) 171 -172.
5. I Speers, “Cerebral edema,” Journal of Neu- rosurgical Nursing 13 (April 1981) 102-115.
6. Rebecca Gary, “Cerebral vasospasm: Pro- cess, trends and interventions,” Journal of Neuro. surgical Nursing 13 (October 1981) 256-264.
7. R H Patterson, B S Ray, “Profound hypo- thermia for intracranial surgery: Laboratory and clinical experiences with extracorporeal circula- tion by peripheral cannulation.” Annals of Surgery 156 (September 1962) 377-393.
8. R B Griepp, E B Stinson, J F Hollingsworth, “Prosthetic replacement of the aortic arch.” Journar of Thoracic and Cardiovascular Surgery 70 (De- cember 1975) 1051-1063.
9. G D Silverberg et al, “Operative treatment of a giant cerebral artery aneurysm by hypothermia and circulatory arrest: Report of a case,” Neuro- surgery 6 (March 1980) 301 -305.
10. M B Hartley, “Hypothermia,“ AORN Journal 24 (October 1976) 764-769.
11. S J Peerless, C G Drake, Modern Technics in Surgery (Mt Kisco. NY: Futura Publishing Go,
12. Silverberg. Reitz. Ream, “Hypothermia and
13. /bid.
1979) 33-36.
1979) 1-21.
cardiac arrest,” 337-346.
650 AORN Journal, March 198.3, Vol37. No 4

14. Silverberg et al, “Operative treatment of a 17. A K Ream et at, “Epidural measurement of intracranial pressure,” Neurosurgery5 (July 1979)
18. M A Bruya, “Planned periods of rest in the intensive care unit: Nursing care activities and intracranial pressure,” Journal of Neurosurgical Nursmg 13 (August 1981) 184-194.
giant cerebral artery aneurysm,” 301 -305.
cardiac arrest,” 337-346. 16. Silverberg, Reitz, Ream, “Hypothermia and
cardiac arrest,” 337-346; M Moriau et al, “Haemo- stasisdisorders in open heart surgery with extracor- poreal circulation,” VoxSanguinis32 (1 977)41-51.
15. Silverberg, Reitz, Ream, “Hypothermia and 36-43.
Improved technique for breast reconstruction Mastectomy is still the primary treatment for breast tumors. Approximately 15% of these patients subsequently undergo a breast reconstruction procedure.
Choosing the correct procedure for each patient has become more complex as advances in breast construction are made. Women who have had an extensive mastectomy accompanied by poor tolerance to a synthetic silicone prosthesis or infection around the prosthesis, and who have abundant abdominal panniculus, may benefit from using a transverse abdominal island flap for breast reconstruction.
must consider the relative contraindications, timing, and type of procedure, according to Michael Scheflan, MD, assistant professor of plastic surgery at the Medical College of Virginia, Richmond, and his associates. Writing in a recent issue of Contemporary Surgery, Dr Scheflan outlined the circumstances that put patients at high risk. Those with two or more positive axillary nodes and those with distant metastases are high-risk candidates.
Timing of the reconstruction is a controversial issue, but Dr Scheflan suggests that adjuvant chemotherapy and radiation therapy be completed before the reconstruction process begins. If these therapies are not required, a three-month waiting period is preferred to allow for healing and softening of the chest wall scars.
few disadvantages was described by Dr Scheflan. The technique does not use a
In all cases of breast reconstruction, one
A new way to reconstruct the breast with
synthetic silicone prosthesis. Redundant infraumbilical abdominal panniculus is transferred to the chest wall as an island vascularized flap. The advantages of this procedure are the scar is not obvious as it is in the suprapubic area; more subcutaneous tissue areas are available as compared with a latissimus dorsi myocutaneous flap, and the patient does not have to be repositioned, as is required when a latissimus myocutaneous flap is used.
Dr Scheflan said there are two possible disadvantages to this technique. It involves a longer operative time. Also, there is a possibility of a hernia forming below the arcuate line, but this can be avoided by repairing the abdominal wall below the arcuate line.
Past AORN president takes executive position Jean E Davis, RN, president of AORN in 1978-1979, became the executive director of the World Affairs Council in San Diego in October. The council is a nonpartisan organization with 1,200 members. There are meetings held twice a month in which international issues are discussed.
Davis is a graduate of the Hahnemann Medical College and Hospital School of Nursing, Philadelphia. She retired from the US Navy as a commander in 1974. Later, she joined Scripps Clinic and Research Foundation, La Jolla, Calif, to direct and plan a new surgical suite at the Green Hospital. She is now a nurse consultant.
AOKN Journal. March 1983. Vol 37, No 4 65 1